Prothetic Rehabilitation of Edentulous Ridges Following Alveolar Distraction Osteogenesis. Clinical...

of 9
description
distracción osteogenica en un paciente edentulo
Transcript of Prothetic Rehabilitation of Edentulous Ridges Following Alveolar Distraction Osteogenesis. Clinical...
-
Prosthetic Rehabilitation of EdentulousRidges Following Alveolar DistractionOsteogenesis: Clinical Report ofThree CasesGulfem Ergun, DDS, PhD1*Isil Cekic Nagas, DDS, PhD2
Dervis Yilmaz, DDS, PhD3
Mustafa Ozturk, DDS, PhD3
Patients with complete edentulism who have insufficient bone for endosseous dental
implant treatment present a challenge for dental practitioners. Distraction osteogenesis of
the edentulous alveolar ridges is a process for augmentation of atrophic alveolar bone
before dental implant placement. This clinical report describes the use of distraction
osteogenesis and rehabilitation of patients with a fixed or removable implant-supported
prosthesis to treat mandibular defects. Two female patients with segmental alveolar atrophy
at the posterior regions of mandible and one female patient with defect at the anterior
region of mandible were treated using distraction devices. However, lingual tipping of the
distraction vector occurred during the distraction phase in patient 1. The morphology of the
alveolar bone was also analyzed in relation to the planned implant position. After a
consolidation period of 12 weeks on average, radiologic observation suggested that there
was sufficient bone formation for implant installation. In all patients, implant-supported fixed
or removable prosthetic oral rehabilitation was successfully performed, and the clinical and
radiologic findings were satisfactory. After 4 years of follow-up, no functional or esthetic
difficulties with the implants and restorations were noted. These case reports suggest that
although alveolar distraction osteogenesis seems to be an effective technique for
augmenting atrophic alveolar bone for creating bone and soft tissue, complications may
occur after surgical procedures.
Key Words: dental implants, alveolar distraction osteogenesis, implant-supportedprosthesis
INTRODUCTION
After tooth loss caused by any
variety of reasons, alveolar
ridge bone height and width
deficiencies limit the use of
endosseous dental implants.
To reconstruct a full-thickness alveolar de-
1 Department of Prosthodontics, Faculty of Dentistry,Gazi University, Ankara, Turkey.2 School of Dental Technology, Hacettepe University,Ankara, Turkey.3 Department of Oral and Maxillofacial Surgery, Facultyof Dentistry, Gazi University, Ankara, Turkey.* Corresponding author, e-mail: [email protected]: 10.1563/AAID-JOI-D-10-00004
CASE REPORT
Journal of Oral Implantology 183
-
fect, autogenous onlay bone grafts tradition-
ally have been performed.1 However, autog-
enous bone graft has the risk of donor-site
problems with the harvesting of the bone
graft and graft resorption.2,3 Guided bone
regeneration has also been presented as a
reliable solution for correcting atrophic
ridges,4 but this technique may result in
unpredictable bone formation or infection
from membrane exposure.5 To overcome the
problems associated with these techniques,
distraction osteogenesis has evolved as a
promising procedure for alveolar ridge aug-
mentation before implant placement.1
Distraction osteogenesis was originally
created for orthopedic purposes to increase
the length of long bones and was later
applied to the maxillofacial region to correct
severe malformations.4,6 The technique relies
on stretching the bones to achieve length-
ening, to generate new bone, and to correct
deformities in height and width.2,7 This
process also aims to bring the bone to the
exact position needed for subsequent
prosthodontic treatment. This is particularly
important for cases in which an implant-
supported fixed prosthetic denture is planned
and oral implants need to be precisely
installed into the desired position.7
The purpose of this clinical report is to
present the clinical experience in treating
defects of edentulous ridges by means of
intraoral vertical distraction osteogenesis
followed by placement of endosseous im-
plants in the distracted areas.
CASE REPORTS
This clinical report included three female
patients (mean age of 55 years) with alveolar
defects caused by periodontal disease or
resulting from traumatic tooth loss and
subsequent atrophy of the alveolar ridge
(Figures 1a and b, 2a and b, 3a and b).
Seventy-year-old patient 1 was referred to
our clinic with a complaint of loose and ill-
fitting complete mandibular dentures. Pa-
tient 2, a 55-year-old with a removable
partial denture in the mandible and a
complete denture in the maxilla, was referred
to the clinic because of her concerns about
her appearance, speech, and difficulty in
chewing. Patient 3, a 52-year-old, was referred
to the clinic with a complaint of loose and ill-
fitting complete maxillary and mandibular
dentures.
Informed consent was obtained from
each patient before they participated in the
study. The patients underwent alveolar ridge
distraction using intraoral extraosseous de-
vices (Table). There was no relevant systemic
history for the patients. Distraction was
performed in the mandible of all patients.
In patient 1, segmental atrophy was located
at the anterior region (incisor region). In the
other 2 patients, segmental atrophy was
located at the posterior parts of the mandi-
ble (premolar-molar regions) (Table).
Surgical procedure
The surgical procedures were performed
under local anesthesia in all patients. The
vestibular bone was exposed by a horizontal
paracrestal incision, preserving the crestal
and oral soft tissues for blood supply of the
latter bone segment. Lateral release incision
allowed for buccal mucoperiosteal flap
elevation providing access to the prospec-
tive osteotomy site. Careful subperiosteal
dissection was performed to obtain ade-
quate visibility of underlying bone but to
preserve the lingual or palatal pedicle after
the osteotomy was performed. The outline
of the osteotomy was marked with a fissure
bur before adaptation of the distractor, and
the distraction vector was slightly directed to
the vestibular aspect. The osteotomy was
performed using a reciprocating saw, and
the transport segment was finally mobilized
with an osteotome. After the bone segments
were mobilized, the distractor was then
applied, fixed, and temporarily activated to
Distraction Osteogenesis: Case Reports
184 Vol. XXXVII/Special Issue/2011
-
test for movement of the distracted seg-
ment. Subsequently, the distracted segment
was repositioned to its initial position and
then the surgical incision was sutured with
4/0 silk sutures, leaving part of the distractor
passing through the incision.
The patients were given postoperative
instructions to maintain a liquid or pureed
diet for 1 month and to progress to a soft
diet after that. Antibiotics were prescribed
for a maximum of 10 days (clindamycin 3 3
600 mg), twice a day. The patients were also
provided with an analgesic to be used on an
as-needed basis. Chlorhexidine gluconate
0.12% mouth rinse 15 mL twice daily was
used for 2 weeks postoperatively.
Standard panoramic radiographs were
performed at the first postoperative days
(Figures 1c, 2c, and 3c). After the latency
period (7 days) for initial healing, the
distractors were activated by turning the
screw of the rods at a rate of 1 mm/d in 2
activations for 10 days. The distraction
device was left in position for a 12-week
consolidation period. At the end of this
period, the rod and plates were removed
under local anesthetic. Soft-tissue closure
was once again done in a similar manner
(Figures 2d and 3d).
In patients 2 and 3, the distraction
regenerate was well ossified and stable.
The healing period proceeded without com-
plications. The patients reported no pain or
discomfort and tolerated the procedure well.
However, in patient 1, lingual tipping of the
distraction vector in the anterior mandible
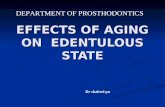
FIGURE 1. (a) Radiograph showing the alveolar deficiency of the patient. (b) Insufficient alveolar crestheight of the patient. (c) Radiograph showing the distracted segment. (d) Ball attachments afterdistraction osteogenesis. (e) Radiograph taken after implant insertion. (f) Intraoral view of the patientat the end of the prosthodontic treatment.
Ergun et al
Journal of Oral Implantology 185
-
occurred during the distraction phase. Then,
5 weeks later, a subsequent osteotomy of
the newly formed bone and transport
segment was performed, and they were
fixed in a labial position with plates and
screws.
Radiographic evaluation
Treatment results of the distraction osteo-
genesis were evaluated by means of pano-
ramic radiographs. The distance between the
upper edge of the lower plate and the
alveolar crest was measured after the dis-
tractor was inserted and at the end of the
distraction period. The difference in the two
heights revealed the vertical distracted bone
gain. The distance between the inferior
margin of the mandible and the alveolar
crest was assessed so that alterations in
bone height could also be observed after
distractor removal. The difference between
the bone height immediately after distrac-
tion and final bone height at the end of
consolidation period represented the bone
relapse.8
The mean gain in the vertical height of
bone obtained immediately after the distrac-
tion procedure was 8.1 mm. However, all
patients had bone relapse after the consol-
idation period (mean bone relapse 5
1.83 mm or 22.6%). After the distraction
period, vertical bone gains of 6.3 mm,
6.4 mm, and 6.1 mm were recorded for
patients 1, 2, and 3, respectively (Table).
Based on the prosthodontic planning,
radiographic splints with tooth setup were
made. The treatment plan consisted of
establishing a correct vertical dimension
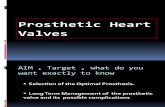
FIGURE 2. (a) Radiograph showing the alveolar deficiency of the patient. (b) Insufficient alveolar crestheight of the patient (left and right side of the mandibula). (c) Radiograph showing the distractedsegments. (d) Left and right distractors with plates screwed to the bone and distraction rod placed. (e)Radiograph taken after prosthodontic treatment. (f) Intraoral view of the patient at the end of theprosthodontic treatment.
Distraction Osteogenesis: Case Reports
186 Vol. XXXVII/Special Issue/2011
-
with a fixed implant. The patients were given
a detailed explanation concerning the pres-
ent state, procedures, and alternative treat-
ment plans, and then informed consent was
obtained from the patients.
In patient 1, treatment with mandibular
implant-supported overdenture prosthesis
retained with ball attachments was planned.
Thus, 2 implants spaced 12 to 16 mm apart
(edge to edge) were placed in the lateral
region to the distracted anterior mandible.
Previously, the patient had needed a vestib-
uloplasty with a cutaneous soft-tissue graft
before loading the implant to obtain ade-
quate vestibular depth and keratinized tissue
around the implants. The abutment connec-
tion was delayed for 6 months after place-
ment of the implant.
In patient 2, fixed mandibular reconstruc-
tion with 6 implants (second molar, first
premolar, canine) with 3 independent fixed
partial dentures (right molar to right premo-
lar, right canine to left canine, left molar to
left premolar) was planned. Similarly, in
patient 3 fixed mandibular reconstruction
with 6 implants (second molar, second
premolar, canine) and 3 independent fixed
partial dentures (right molar to right premo-
lar, right canine to left canine, left molar to
left premolar) was planned. In patients 2
and 3, fixed maxillary reconstruction with 8
implants (second molar, first premolar, ca-
nine, and central incisor) and 4 independent
fixed partial dentures (molar to premolar,
canine to central incisor, bilaterally) was also
planned.
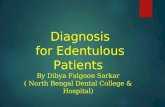
FIGURE 3. (a) Radiograph showing alveolar deficiency of the patient. (b) Initial appearance of the patientwith removable maxillary and mandibular dentures. (c) Radiograph showing the distracted segmentand maxillary implants. (d) Left and right distractors with plates screwed to the bone and distractionrod placed. (e) Radiograph taken after implant insertion. (f) Intraoral view of the patient at the end ofthe prosthodontic treatment.
Ergun et al
Journal of Oral Implantology 187
-
The surgeon used a custom surgical
guide to help place the implants. The
marginal bone of the implants was evaluated
by periapical radiographs. Furthermore, each
radiograph was calibrated using the known
width of the coronal cylinders of the
implants. In total, 6 implants were inserted
in the distracted areas. In addition, 8
implants were inserted in the maxilla of
both patients. The implants were submerged
and uncovered 4 months later for healing
screws and abutments to be inserted.
Prosthetic phase
In patient 1, an implant-retained removable
prosthesis with ball attachments to the
mandible and a complete denture to the
maxilla were planned (Figure 1d). After
removal of the cover screws (ITI, Straumann,
Basel, Switzerland), impression copings (ITI)
with appropriate diameters were placed. The
impression of the alveolar mucosa was made
with a zinc oxide eugenol impression paste
(Cavex, Cavex Holland BV, Haarlem, Nether-
lands). After the dentures were fabricated, ball
attachments were connected to the fixtures in
the mouth. Retentive components were then
placed on the abutment and undercuts were
blocked out. Venting holes were prepared in
the overdenture for expressing excess acrylic
resin. Upon removal of the denture, irregular-
ities and voids in the intaglio surface of the
TABLE
Characteristics of 3 patients who underwent bidirectional alveolar distraction
PatientNo.
Age(Years) Sex
Region ofTooth Loss
and SegmentalAtrophy Distractor
Bone Gain(mm) No. and Type of Implants Placed
1 70 F Mandibularanterior
Intraoral verticalbidirectionaldistractor*
6.3 2 ITI implants:4.1 mm diameter, 10 mm
long2 55 F Mandibular
posteriorIntraoral vertical
bidirectionaldistractor*
6.4 ITI implants
Maxilla: 8 implants:3 implants: 3.8 mm
diameter, 12 mm long3 implants: 4.1 mm
diameter, 12 mm long2 implants: 3.8 mm
diameter, 10 mm longMandible: 6 implants:
4 implants: 4.1 mmdiameter, 12 mm long
1 implant: 3.8 mmdiameter, 10 mm long
1 implant: 4.8 mmdiameter, 12 mm long
3 52 F Mandibularposterior
Intraoral verticalbidirectionaldistractor*
6.1 MIS`
Maxilla: 8 implants:3.75 diameter, 11.5 mm
longMandible: 6 implants:
2 implants: 3.30 diameter,13 mm long
2 implants: 4.20 diameter,11.5 mm long
2 implants: 3.75 diameter,11.5 mm long
*Modus ARS 1.5, Medartis, Basel, Switzerland.Straumann, Basel, Switzerland.`MIS Implant Technologies Ltd, Shlomi, Israel.
Distraction Osteogenesis: Case Reports
188 Vol. XXXVII/Special Issue/2011
-
denture around the attachments were filled in
with additional acrylic resin (Vertex, Vertex-
Dental BV, Zeist, The Netherlands). Excess
acrylic resin was removed; the complete
dentures were polished and inserted in the
maxilla and mandible.
In patient 2, extractions of the existing
mandibular canines were planned because
of mobility and occlusion plane problems.
After these teeth were extracted, a fixed
prosthetic denture in the form of a full-arch
bridge was planned for both jaws. In patient
3, the decision was also made to fabricate a
cement-retained fixed partial denture for
both jaws. After the placement of impression
copings, definitive impressions of the maxil-
lary and mandibular implants were made
using transfer copings and a polyether
impression material (Impregum, 3M Espe,
Seefeld, Germany). The impression copings
were fixed onto the abutment analogs.
Cement-retained prostheses were then com-
pleted on abutment-level models from a
base metal alloy (Master-Tec, Ivoclar Viva-
dent AG, Schaan, Liechtenstein) and porce-
lain (VITA VM 13, VITA Zahnfabrik, Bad
Sackingen, Germany) and cemented to the
abutments.
Follow-up and criteria for success
Routine clinical assessments were made 1, 2,
6, and 12 months after prosthetic loading
and then annually with visual and radio-
graphic examinations. Criteria for success
included the following: effective placement
and primary stability of the planned implant,
stability of the implant (lack of mobility),
absence of pain or any subjective sensation
at each visit, lack of peri-implant infection
with suppuration, and lack of continuous
radiolucency around the implant.9 Routine
radiographs consisted of panoramic radio-
graphs taken preoperatively (Figures 1a, 2a,
and 3a), after the distraction osteogenesis
(Figures 1b, 2b, and 3b) and placement of
implants (Figure 3e), at the time of prosthet-
ic loading (Figures 1e and 2e), and annually
thereafter until the end of follow-up. The
initial appearance of the patients (Fig-
ures 1b, 2b, and 3b), the intraoperative view
after distraction osteogenesis (Figures 1d,
2d, and 3d) and final outcome of the
prosthodontic treatment are shown in Fig-
ures 1f, 2f, and 3f.
DISCUSSION
Alveolar distraction osteogenesis has been
considered as an alternative to many other
surgical techniques, such as bone augmenta-
tion for implant-supported oral rehabilitation
of atrophic jaws, alloplastic graft augmenta-
tion, and guided bone regeneration.2,4,8,10,11
Moreover, this technique offers some advan-
tages because it avoids donor-site morbidity
and provides predictable gain of hard and
soft tissues. Further advantages are the low
infection rate and decreased bone resorption.
Moreover, this technique allows the use of
complementary regeneration techniques
when the outcome is not completely satis-
factory.10 Because of these advantages of the
alveolar distraction osteogenesis, the tech-
nique was chosen for this clinical report.
Alveolar distraction osteogenesis also
provides a short bone-consolidation period
before implantation.12 Previous studies re-
ported a mean time of 6 to 8 months after
guided bone regeneration, which is much
longer than the time required after distraction
osteogenesis.12,13 Various consolidation times
have been reported for distraction osteogen-
esis, but 3 to 4 months is typically adequate
for maturation of the distraction regenerate.1
Similarly, in the patients in the present case
report, the consolidation period after alveolar
distraction was 3 months on average. The
advantages of distraction osteogenesis have
been confirmed by the present clinical report.
A number of complications that could
arise with the distraction process include
resorption of the transport segment, difficulty
Ergun et al
Journal of Oral Implantology 189
-
in completing the osteotomy on the lingual
side, excessive length of the threaded rod,
bone fracture, device failure, tipping of the
transport segment, perforation of the mucosa
by the transport segment, and inadequate
length of distraction.10,14 Relapse and long-
term results in alveolar distraction have been
reported in several clinical studies.15,16 The
bone relapse occurs because of scar-tissue
contraction after distraction. A consolidation
period of 3 months is generally accepted to be
sufficient to avoid most of the relapse due to
scar contraction.16 A previous study by Ettl
and colleagues8 reported a mean vertical
bone gain of 6.4 mm and an average bone
relapse of 1.8 mm (21.1%) after a consolida-
tion period of 18 weeks. Furthermore, in
another study, the mean bone gain of
6.5 mm and an average bone relapse of
1.6 mm (25%) after a consolidation period of
810 weeks have been recorded.17 In accord-
ance with the previous studies, in the present
clinical report, after a consolidation period of
12 weeks, a mean bone gain of 6.3 mm and an
average bone relapse of 1.8 mm (22.6%) were
recorded. The bone relapse could be partly
attributed to smoothing of the alveolar crest
prior to insertion of the implants. Eventually,
adjustment of the distraction protocol to
include overcorrection of 1525% may com-
pensate the bone relapse during the consol-
idation period of the distracted alveolar
bone.8,18
Another complication that has frequently
been encountered after distraction osteo-
genesis is the displacement of the transport
segment. In a previous study by Ettl and
colleagues,8 33 complications were observed
in 36 patients. In 15 patients (4 maxilla and
11 mandible), oral displacement of the
transport segment occurred, and corrective
osteotomy of the distracted bone segment
and vestibular augmentation were per-
formed. Accordingly, in the present clinical
report, in patient 1, the vector of distraction
was lingually oriented, resulting in the
regenerated bone being positioned lingual-
ly. To place the implants in the right position,
an additional corrective osteotomy was
performed. An incorrect vector of distraction
could be explained by the tension caused by
surrounding cheek and tongue muscles,
together with the traction of the perioste-
um.8,19 Moreover, the soft-tissue complica-
tion that resulted in a reduced vestibular
sulcus might be the result of inadequate
fixed gingiva formation after surgical proce-
dure. Therefore, a full-thickness vestibular
incision in the lower vestibule might be
useful to prevent these complications.
A variety of intraosseous and extraosse-
ous devices are available for alveolar dis-
traction osteogenesis.20 A previous study by
Wolvius and colleagues18 indicated that the
solution for optimal vector management is
the bidirectional extraosseous alveolar dis-
tractor. The extraosseous devices in the
cases presented here allowed good stability
of both the device and the bone segment
during the distraction and consolidation
periods. Furthermore, the distraction rates
were 1 mm/d, performed in 2 activations for
10 days. A previous study by Walker20
indicated that the greater the frequency of
activation, the more favorable the distraction
regenerate. The distraction rate for the
patient presented in that study was also
1 mm/d, performed in 3 activations.
A major esthetic concern with alveolar
distraction osteogenesis is obtaining a pre-
dictable position of the transosteal portion
of the implant in relation to the newly
generated bone ridge crest.21 However, in
the present clinical report, alveolar distrac-
tion processes were performed in the
posterior part of the mandible in patients 2
and 3. As esthetics is of less concern in the
mandible, no esthetic complications oc-
curred in either case. In addition, in patient
1, satisfactory results from esthetic and
functional standpoints were acquired via
implant-supported removable prosthesis.
Distraction Osteogenesis: Case Reports
190 Vol. XXXVII/Special Issue/2011
-
The decision about when distraction osteo-
genesis can be performed should be based on
the severity of alveolar bone loss. Furthermore,
complications like oral displacement of the
transport vector and inadequate soft-tissue
extensions after distraction may arise. There-
fore, long-term evaluation of a large number of
patients will be necessary to evaluate the
efficacy of this treatment protocol.
CONCLUSIONS
This clinical report has documented the
creation of adequate height and volume of
bone for rehabilitation of the patients with
endosseous implant-supported dental resto-
rations. Although distraction osteogenesis
seems to be a promising method for mandib-
ular reconstruction, it has some limitations.
Bone relapse, displacement of the transport
segment, and soft-tissue complications may
occur after distraction osteogenesis. Thus, the
potential complications and the traction by
muscle forces on the floor of the mouth have
to be considered carefully. Moreover, further
research with more patients is needed to
demonstrate a generalized trend.
REFERENCES
1. Jensen O. Alveolar Distraction Osteogenesis.Chicago, Ill: Quintessence Publishing Co Ltd; 2002.
2. Yalcin S, Ordulu M, Emes Y, Gur H, Aktas I,Caniklioglu C. Alveolar distraction osteogenesis beforeplacement of dental implants. Implant Dent. 2006;15:4852.
3. Cakir-Ozkan N, Eyibilen A, Ozkan F, Ozyurt B,Aslan H. Stereologic analysis of bone produced bydistraction osteogenesis or autogenous bone graftingin mandible. J Craniofac Surg. 2010;21:735740.
4. Chiapasco M, Romeo E, Vogel G. Verticaldistraction osteogenesis of edentulous ridges forimprovement of oral implant positioning: a clinicalreport of preliminary results. Int J Oral MaxillofacImplants. 2001;16:4351.
5. Fukuda M, Iino M, Ohnuki T, Nagai H, TakahashiT. Vertical alveolar distraction osteogenesis withcomplications in a reconstructed mandible. J OralImplantol. 2003;29:185188.
6. Urbani G, Lombardo G, Santi E, Consolo U.Distraction osteogenesis to achieve mandibular vertical
bone regeneration: a case report. Int J PeriodonticsRestorative Dent. 1999;19:321331.
7. Iizuka T, Hallermann W, Seto I, Smolka W, SmolkaK, Bosshardt DD. Bi-directional distraction osteogenesisof the alveolar bone using an extraosseous device. ClinOral Implants Res. 2005;16:700707.
8. Ettl T, Gerlach T, Schusselbauer T, Gosau M,Reichert TE, Driemel O. Bone resorption and complica-tions in alveolar distraction osteogenesis. Clin OralInvest. 2010;15:481489.
9. Demarosi F, Leghissa GC, Sardella A, Lodi G,Carrassi A. Localised maxillary ridge expansion withsimultaneous implant placement: a case series. Br J OralMaxillofac Surg. 2009;47:535540.
10. Sant S, Jagtap A. Alveolar distraction osteogen-esis: revive and restore the native bone. J Prosthodont.2009;18:694697.
11. Bulut E, Muglali M, Celebi N, Bekcioglu B.Horizontal alveolar distraction of the mandibular canineregions for implant placement. J Craniofac Surg.2010;21:830832.
12. Chiapasco M, Romeo E, Casentini P, RimondiniL. Alveolar distraction osteogenesis vs. vertical guidedbone regeneration for the correction of verticallydeficient edentulous ridges: a 1-3-year prospectivestudy on humans. Clin Oral Implants Res. 2004;15:8295.
13. Chiapasco M, Abati S, Romeo E, Vogel G.Clinical outcome of autogenous bone blocks or guidedbone regeneration with e-PTFE membranes for thereconstruction of narrow edentulous ridges. Clin OralImplants Res. 1999;10:278288.
14. Mazzonetto R, Allais M, Maurette PE, MoreiraRW. A retrospective study of the potential complica-tions during alveolar distraction osteogenesis in 55patients. Int J Oral Maxillofac Surg. 2007;36:610.
15. Koudstaal MJ, Poort LJ, van der Wal KGH,Wolvius EB, Prahl-Andersen B, Schulten AJM. Surgicalassisted rapid maxillary expansion: a review of theliterature. Int J Oral Maxillofac Surg. 2005;34:709714.
16. Koudstaal MJ, Wolvius EB, Schulten AJ, HopWC, van der Wal KG. Stability, tipping and relapse ofbone-borne versus tooth-borne surgically assistedrapid maxillary expansion; a prospective randomizedpatient trial. Int J Oral Maxillofac Surg. 2009;38:308315.
17. Jensen OT, Cockrell R, Kuhike L, Reed C.Anterior maxillary alveolar distraction osteogenesis: aprospective 5-year clinical study. Int J Oral MaxillofacImplants. 2002;17:5268.
18. Wolvius EB, Scholtemeijer M, Weijland M, HopWC, van der Wal KG. Complications and relapse inalveolar distraction osteogenesis in partially edentulouspatients. Int J Oral Maxillofac Surg. 2007;36:700705.
19. Saulacic N, Zix J, Iizuka T. Complication ratesand associated factors in alveolar distraction osteogen-esis: a comprehensive review. Int J Oral Maxillofac Surg.2009;38:210217.
20. Walker DA. Mandibular distraction osteogene-sis for endosseous dental implants. J Can Dent Assoc.2005;71:171175.
21. Dinse WE, Burnett RR. Anterior maxillaryrestoration using distraction osteogenesis and im-plants: a clinical report. J Prosthet Dent. 2008;100:250253.
Ergun et al
Journal of Oral Implantology 191