
Protective Effect of Telmisartan Against Endothelial...
9
Protective Effect of Telmisartan Against Endothelial Dysfunction After Coronary Drug-Eluting Stent Implantation in Hypertensive Patients Mitsuyasu Terashima, MD,* Hideaki Kaneda, MD,† Kenya Nasu, MD,* Hitoshi Matsuo, MD,* Maoto Habara, MD,* Tsuyoshi Ito, MD,* Nobuyoshi Tanaka, MD,* Sudhir Rathore, MD,* Yoshihisa Kinoshita, MD,* Masashi Kimura, MD,* Mariko Ehara, MD,* Yasuyoshi Suzuki, BS,* Takahiko Suzuki, MD* Toyohashi and Tokyo, Japan Objectives The aim of this prospective, randomized study was to evaluate the effects of telmisar- tan, compared with the calcium-channel blocker amlodipine, on endothelial function after coronary drug-eluting stent (DES) implantation in hypertensive patients. Background DES implantation impairs local endothelial function, which may be associated with fu- ture cardiovascular events. Telmisartan, which has unique peroxisome proliferator-activated-receptor- gamma–mediated effects in addition to its renin-angiotensin system–inhibition effects, has favorable effects on endothelial function. Methods Fifty-one hypertensive patients with coronary artery stenosis but without coronary artery spasm, treated with a sirolimus-eluting stent, were randomly assigned to either the telmisartan (25 cases) or amlodipine (26 cases) treatment groups. At baseline and at 3 months after DES implanta- tion, endothelium-dependent and -independent vasomotion were evaluated by quantitative coro- nary angiography under the condition of medication withdrawal. The mean luminal diameter of a 20-mm coronary segment, beginning 5 mm distal to the stent, was measured before and after infu- sion of intracoronary acetylcholine (10 7 , 10 6 mol/l) and then again after infusion of nitroglycerin. Results Blood pressure was comparable between groups at baseline and after 3 months. Vasocon- striction after acetylcholine infusion at 3 months (impaired endothelial function) was less pro- nounced in the telmisartan group than in the amlodipine group (p 0.0001), although there was no significant difference between the 2 groups before DES implantation. The response to nitroglyc- erin did not differ between groups before or at 3 months after DES implantation. Conclusions Telmisartan, compared with amlodipine, significantly ameliorated endothelial dys- function after DES implantation in terms of vasoconstriction induced by acetylcholine. (J Am Coll Cardiol Intv 2012;5:182–90) © 2012 by the American College of Cardiology Foundation From the *Department of Cardiology, Toyohashi Heart Center, Toyohashi, Japan; and the †Okinaka Memorial Institute for Medical Research, Tokyo, Japan. This study was supported by a grant from Japan Vascular Disease Research Foundation (Kyoto, Japan). The authors have reported that they have no relationships relevant to the contents of this paper to disclose. Manuscript received June 17, 2011; revised manuscript received September 7, 2011, accepted September 28, 2011. JACC: CARDIOVASCULAR INTERVENTIONS VOL. 5, NO. 2, 2012 © 2012 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 1936-8798/$36.00 PUBLISHED BY ELSEVIER INC. DOI: 10.1016/j.jcin.2011.09.022
Transcript of Protective Effect of Telmisartan Against Endothelial...

J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 5 , N O . 2 , 2 0 1 2
© 2 0 1 2 B Y T H E A M E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N D A T I O N I S S N 1 9 3 6 - 8 7 9 8 / $ 3 6 . 0 0
P U B L I S H E D B Y E L S E V I E R I N C . D O I : 1 0 . 1 0 1 6 / j . j c i n . 2 0 1 1 . 0 9 . 0 2 2
Protective Effect of TelmisartanAgainst Endothelial Dysfunction AfterCoronary Drug-Eluting Stent Implantationin Hypertensive Patients
Mitsuyasu Terashima, MD,* Hideaki Kaneda, MD,† Kenya Nasu, MD,*Hitoshi Matsuo, MD,* Maoto Habara, MD,* Tsuyoshi Ito, MD,* Nobuyoshi Tanaka, MD,*Sudhir Rathore, MD,* Yoshihisa Kinoshita, MD,* Masashi Kimura, MD,*Mariko Ehara, MD,* Yasuyoshi Suzuki, BS,* Takahiko Suzuki, MD*
Toyohashi and Tokyo, Japan
Objectives The aim of this prospective, randomized study was to evaluate the effects of telmisar-tan, compared with the calcium-channel blocker amlodipine, on endothelial function after coronarydrug-eluting stent (DES) implantation in hypertensive patients.
Background DES implantation impairs local endothelial function, which may be associated with fu-ture cardiovascular events. Telmisartan, which has unique peroxisome proliferator-activated-receptor-gamma–mediated effects in addition to its renin-angiotensin system–inhibition effects, has favorableeffects on endothelial function.
Methods Fifty-one hypertensive patients with coronary artery stenosis but without coronary arteryspasm, treated with a sirolimus-eluting stent, were randomly assigned to either the telmisartan (25cases) or amlodipine (26 cases) treatment groups. At baseline and at 3 months after DES implanta-tion, endothelium-dependent and -independent vasomotion were evaluated by quantitative coro-nary angiography under the condition of medication withdrawal. The mean luminal diameter of a20-mm coronary segment, beginning 5 mm distal to the stent, was measured before and after infu-sion of intracoronary acetylcholine (10�7, 10�6 mol/l) and then again after infusion of nitroglycerin.
Results Blood pressure was comparable between groups at baseline and after 3 months. Vasocon-striction after acetylcholine infusion at 3 months (impaired endothelial function) was less pro-nounced in the telmisartan group than in the amlodipine group (p � 0.0001), although there wasno significant difference between the 2 groups before DES implantation. The response to nitroglyc-erin did not differ between groups before or at 3 months after DES implantation.
Conclusions Telmisartan, compared with amlodipine, significantly ameliorated endothelial dys-function after DES implantation in terms of vasoconstriction induced by acetylcholine. (J AmColl Cardiol Intv 2012;5:182–90) © 2012 by the American College of Cardiology Foundation
From the *Department of Cardiology, Toyohashi Heart Center, Toyohashi, Japan; and the †Okinaka Memorial Institute forMedical Research, Tokyo, Japan. This study was supported by a grant from Japan Vascular Disease Research Foundation (Kyoto,Japan). The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Manuscript received June 17, 2011; revised manuscript received September 7, 2011, accepted September 28, 2011.
cpItSdlasaa1ma5b8�jtii
(a
Mwsfwtdcowfdi
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S , V O L . 5 , N O . 2 , 2 0 1 2 Terashima et al.
F E B R U A R Y 2 0 1 2 : 1 8 2 – 9 0 Effects of Telmisartan on Endothelial Function
183
Drug-eluting stents (DES) are widely used for the treat-ment of coronary artery disease to reduce both the rate ofrestenosis and the subsequent need for target lesion reinter-vention. Endothelial dysfunction after DES implantation isa concern (1–5), however, and might contribute to thedevelopment of severe adverse cardiac events. Therefore,amelioration of endothelial dysfunction after DES implan-tation might improve prognosis.
Angiotensin-converting enzyme inhibitors and angiotensin-IIreceptor blockers (ARB), which block the renin-angiotensinsystem, are widely used for their organoprotective actions, aswell as for the treatment of hypertension (6). Amongvarious organoprotective actions, renin-angiotensin systemblockers favorably affect endothelial function (7–9). Telmis-artan, an ARB, has unique peroxisome proliferator-activated receptor (PPAR)-gamma–mediated effects in ad-dition to ARB class effects and is expected to improveendothelial function through several mechanisms, includingangiotensin II inhibition with type-1 receptor blockade andinduction of adiponectin via PPAR-gamma–mediated ef-fects (10–12).
This prospective, randomized study compared the effects oftelmisartan to a calcium-channel blocker, amlodipine, onendothelial function after DES implantation in hypertensivepatients.
Methods
Study patients. Patients between 20 and 80 years of age withlinically stable angina pectoris and hypertension scheduled forercutaneous coronary intervention (PCI) were enrolled.nclusion criteria were: 1) hypertension defined based onhe criteria put forth in the guidelines of the Japaneseociety of Hypertension or use of an antihypertensiverug; 2) stable angina pectoris with a single de novo stenotic
esion (75% to 90% diameter stenosis) in the native coronaryrtery with a lesion length eligible for treatment with 1 or 2irolimus-eluting stents (SES) (Cypher, Cordis Corp., Mi-mi Lakes, Florida) and with a reference vessel diameter oft least 2.5 mm and �4.0 mm. Exclusion criteria were:) vasospastic angina pectoris; 2) unstable angina pectoris oryocardial infarction within 4 weeks; 3) left main coronary
rtery disease; 4) totally or subtotally occluded lesion;) bifurcation lesion treated with bifurcation stenting; 6)ypass graft lesion; 7) previous PCI for the target vessel;) cardiogenic shock; 9) left ventricular ejection fraction30%; 10) serum creatinine levels �1.5 mg/dl; and 11)
udged by the investigator to be inappropriate for participa-ion in this study. The study protocol was approved by thenstitutional review board, and all patients provided writtennformed consent.Evaluation of endothelial function. Coronary angiographyCAG) to evaluate endothelial function was performed both
t the pre-intervention state and at the 3-month follow-up.edications with potential effects on vasomotor responsesere withheld for at least 48 h before CAG, except for
ublingual nitroglycerin (NTG) as needed. CAG was per-ormed after injection of 2,000 U of heparin, and all drugsere infused through the catheter selectively engaged in the
arget vessel. To evaluate endothelial function, endothelium-ependent and -independent vasomotor responses to intra-oronary infusion of increasing doses of acetylcholine (ACh)r nitrates were assessed. As baseline, physiological salineas infused for 2 min at an infusion rate of 2 ml/min,
ollowed by baseline CAG. Thereafter, the endothelium-ependent vasomotor response was evaluated over a 2-minnfusion of ACh in increasing doses (1.4 and 14 �g/min;
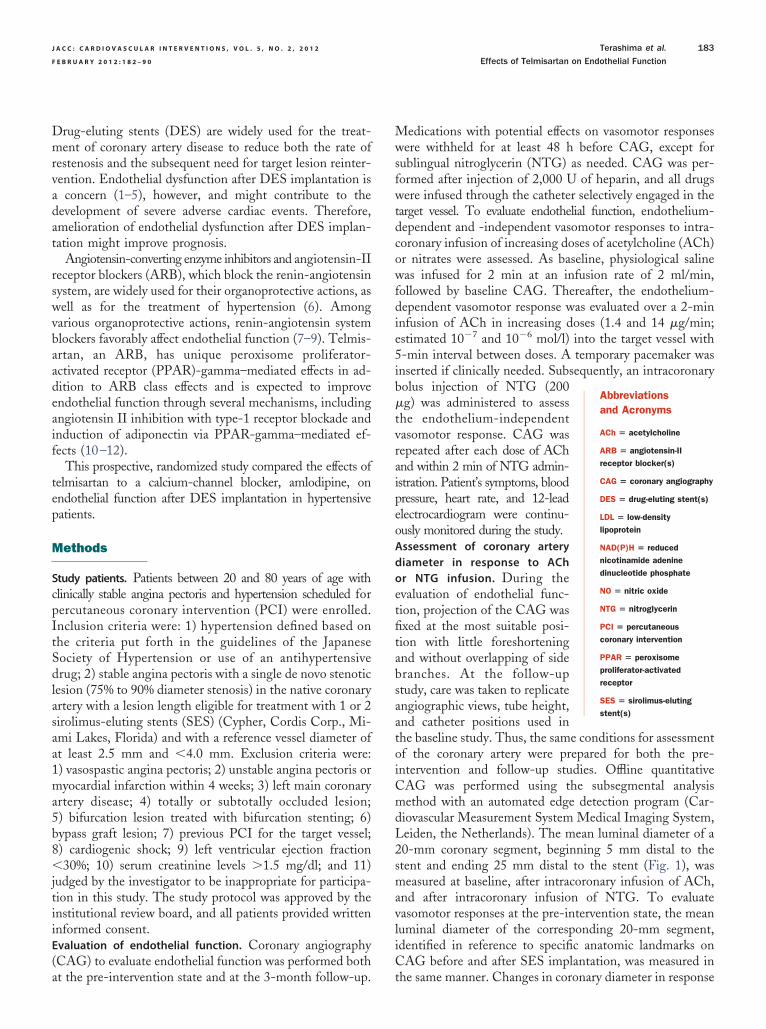
estimated 10�7 and 10�6 mol/l) into the target vessel with5-min interval between doses. A temporary pacemaker wasinserted if clinically needed. Subsequently, an intracoronarybolus injection of NTG (200�g) was administered to assessthe endothelium-independentvasomotor response. CAG wasrepeated after each dose of AChand within 2 min of NTG admin-istration. Patient’s symptoms, bloodpressure, heart rate, and 12-leadelectrocardiogram were continu-ously monitored during the study.Assessment of coronary arterydiameter in response to AChor NTG infusion. During theevaluation of endothelial func-tion, projection of the CAG wasfixed at the most suitable posi-tion with little foreshorteningand without overlapping of sidebranches. At the follow-upstudy, care was taken to replicateangiographic views, tube height,and catheter positions used inthe baseline study. Thus, the same conditions for assessmentof the coronary artery were prepared for both the pre-intervention and follow-up studies. Offline quantitativeCAG was performed using the subsegmental analysismethod with an automated edge detection program (Car-diovascular Measurement System Medical Imaging System,Leiden, the Netherlands). The mean luminal diameter of a20-mm coronary segment, beginning 5 mm distal to thestent and ending 25 mm distal to the stent (Fig. 1), wasmeasured at baseline, after intracoronary infusion of ACh,and after intracoronary infusion of NTG. To evaluatevasomotor responses at the pre-intervention state, the meanluminal diameter of the corresponding 20-mm segment,identified in reference to specific anatomic landmarks onCAG before and after SES implantation, was measured in
Abbreviationsand Acronyms
ACh � acetylcholine
ARB � angiotensin-IIreceptor blocker(s)
CAG � coronary angiography
DES � drug-eluting stent(s)
LDL � low-densitylipoprotein
NAD(P)H � reducednicotinamide adeninedinucleotide phosphate
NO � nitric oxide
NTG � nitroglycerin
PCI � percutaneouscoronary intervention
PPAR � peroxisomeproliferator-activatedreceptor
SES � sirolimus-elutingstent(s)
the same manner. Changes in coron
ary diameter in response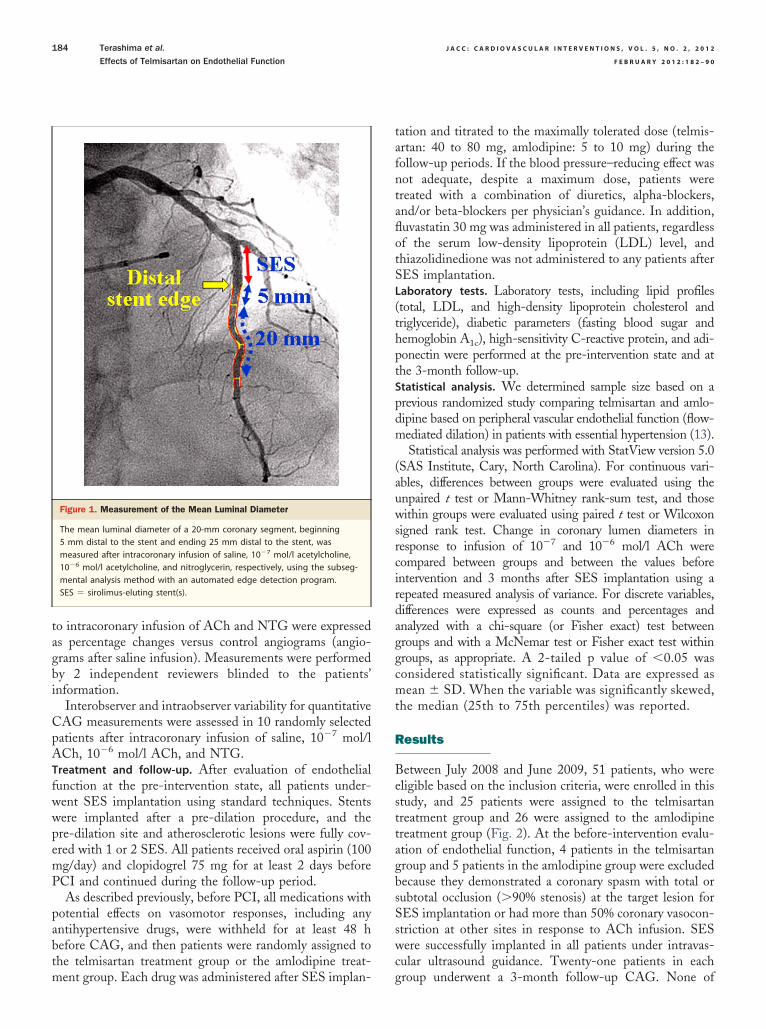
A
(th
cirdagg
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S , V O L . 5 , N O . 2 , 2 0 1 2
F E B R U A R Y 2 0 1 2 : 1 8 2 – 9 0
Terashima et al.
Effects of Telmisartan on Endothelial Function
184
to intracoronary infusion of ACh and NTG were expressedas percentage changes versus control angiograms (angio-grams after saline infusion). Measurements were performedby 2 independent reviewers blinded to the patients’information.
Interobserver and intraobserver variability for quantitativeCAG measurements were assessed in 10 randomly selectedpatients after intracoronary infusion of saline, 10�7 mol/l
Ch, 10�6 mol/l ACh, and NTG.Treatment and follow-up. After evaluation of endothelialfunction at the pre-intervention state, all patients under-went SES implantation using standard techniques. Stentswere implanted after a pre-dilation procedure, and thepre-dilation site and atherosclerotic lesions were fully cov-ered with 1 or 2 SES. All patients received oral aspirin (100mg/day) and clopidogrel 75 mg for at least 2 days beforePCI and continued during the follow-up period.
As described previously, before PCI, all medications withpotential effects on vasomotor responses, including anyantihypertensive drugs, were withheld for at least 48 hbefore CAG, and then patients were randomly assigned tothe telmisartan treatment group or the amlodipine treat-
Figure 1. Measurement of the Mean Luminal Diameter
The mean luminal diameter of a 20-mm coronary segment, beginning5 mm distal to the stent and ending 25 mm distal to the stent, wasmeasured after intracoronary infusion of saline, 10�7 mol/l acetylcholine,10�6 mol/l acetylcholine, and nitroglycerin, respectively, using the subseg-mental analysis method with an automated edge detection program.SES � sirolimus-eluting stent(s).
ment group. Each drug was administered after SES implan-
tation and titrated to the maximally tolerated dose (telmis-artan: 40 to 80 mg, amlodipine: 5 to 10 mg) during thefollow-up periods. If the blood pressure–reducing effect wasnot adequate, despite a maximum dose, patients weretreated with a combination of diuretics, alpha-blockers,and/or beta-blockers per physician’s guidance. In addition,fluvastatin 30 mg was administered in all patients, regardlessof the serum low-density lipoprotein (LDL) level, andthiazolidinedione was not administered to any patients afterSES implantation.Laboratory tests. Laboratory tests, including lipid profilestotal, LDL, and high-density lipoprotein cholesterol andriglyceride), diabetic parameters (fasting blood sugar andemoglobin A1c), high-sensitivity C-reactive protein, and adi-
ponectin were performed at the pre-intervention state and atthe 3-month follow-up.Statistical analysis. We determined sample size based on aprevious randomized study comparing telmisartan and amlo-dipine based on peripheral vascular endothelial function (flow-mediated dilation) in patients with essential hypertension (13).
Statistical analysis was performed with StatView version 5.0(SAS Institute, Cary, North Carolina). For continuous vari-ables, differences between groups were evaluated using theunpaired t test or Mann-Whitney rank-sum test, and thosewithin groups were evaluated using paired t test or Wilcoxonsigned rank test. Change in coronary lumen diameters inresponse to infusion of 10�7 and 10�6 mol/l ACh wereompared between groups and between the values beforentervention and 3 months after SES implantation using aepeated measured analysis of variance. For discrete variables,ifferences were expressed as counts and percentages andnalyzed with a chi-square (or Fisher exact) test betweenroups and with a McNemar test or Fisher exact test withinroups, as appropriate. A 2-tailed p value of �0.05 was
considered statistically significant. Data are expressed asmean � SD. When the variable was significantly skewed,the median (25th to 75th percentiles) was reported.
Results
Between July 2008 and June 2009, 51 patients, who wereeligible based on the inclusion criteria, were enrolled in thisstudy, and 25 patients were assigned to the telmisartantreatment group and 26 were assigned to the amlodipinetreatment group (Fig. 2). At the before-intervention evalu-ation of endothelial function, 4 patients in the telmisartangroup and 5 patients in the amlodipine group were excludedbecause they demonstrated a coronary spasm with total orsubtotal occlusion (�90% stenosis) at the target lesion forSES implantation or had more than 50% coronary vasocon-striction at other sites in response to ACh infusion. SESwere successfully implanted in all patients under intravas-cular ultrasound guidance. Twenty-one patients in each
group underwent a 3-month follow-up CAG. None of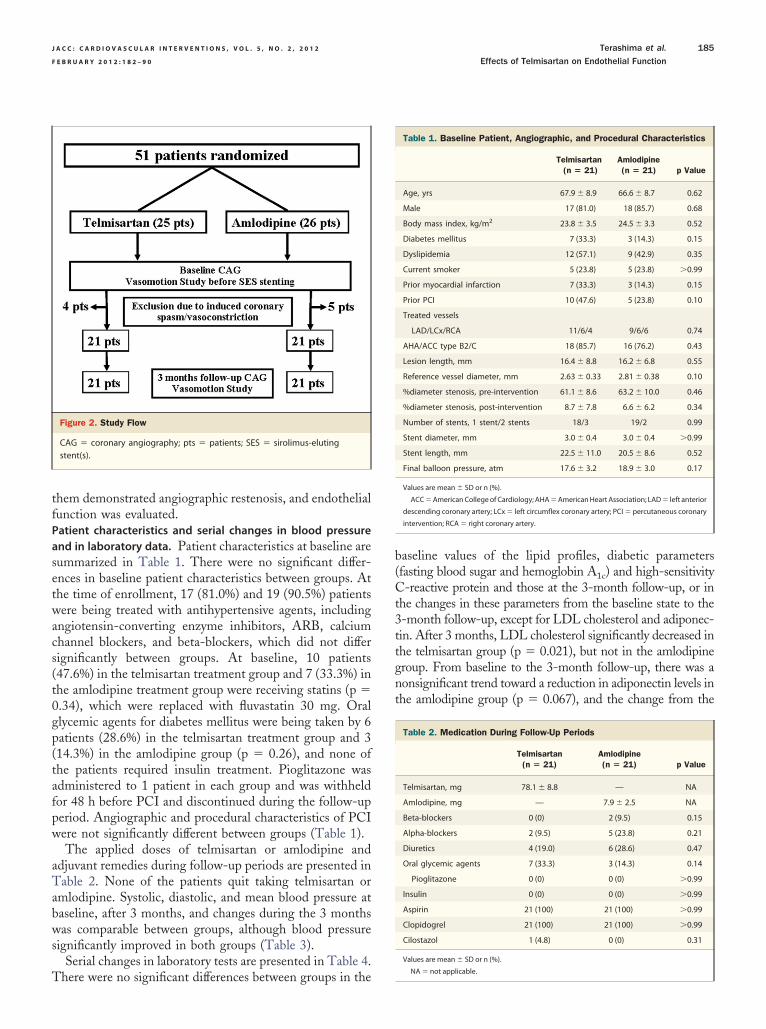
setwacs(t0gp(tafpw
aTabws
T
b(Ct3ttgnt
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S , V O L . 5 , N O . 2 , 2 0 1 2 Terashima et al.
F E B R U A R Y 2 0 1 2 : 1 8 2 – 9 0 Effects of Telmisartan on Endothelial Function
185
them demonstrated angiographic restenosis, and endothelialfunction was evaluated.Patient characteristics and serial changes in blood pressureand in laboratory data. Patient characteristics at baseline areummarized in Table 1. There were no significant differ-nces in baseline patient characteristics between groups. Athe time of enrollment, 17 (81.0%) and 19 (90.5%) patientsere being treated with antihypertensive agents, including
ngiotensin-converting enzyme inhibitors, ARB, calciumhannel blockers, and beta-blockers, which did not differignificantly between groups. At baseline, 10 patients47.6%) in the telmisartan treatment group and 7 (33.3%) inhe amlodipine treatment group were receiving statins (p �.34), which were replaced with fluvastatin 30 mg. Orallycemic agents for diabetes mellitus were being taken by 6atients (28.6%) in the telmisartan treatment group and 314.3%) in the amlodipine group (p � 0.26), and none ofhe patients required insulin treatment. Pioglitazone wasdministered to 1 patient in each group and was withheldor 48 h before PCI and discontinued during the follow-uperiod. Angiographic and procedural characteristics of PCIere not significantly different between groups (Table 1).The applied doses of telmisartan or amlodipine and
djuvant remedies during follow-up periods are presented inable 2. None of the patients quit taking telmisartan or
mlodipine. Systolic, diastolic, and mean blood pressure ataseline, after 3 months, and changes during the 3 monthsas comparable between groups, although blood pressure
ignificantly improved in both groups (Table 3).Serial changes in laboratory tests are presented in Table 4.
Figure 2. Study Flow
CAG � coronary angiography; pts � patients; SES � sirolimus-elutingstent(s).
here were no significant differences between groups in the
aseline values of the lipid profiles, diabetic parametersfasting blood sugar and hemoglobin A1c) and high-sensitivity-reactive protein and those at the 3-month follow-up, or in
he changes in these parameters from the baseline state to the-month follow-up, except for LDL cholesterol and adiponec-in. After 3 months, LDL cholesterol significantly decreased inhe telmisartan group (p � 0.021), but not in the amlodipineroup. From baseline to the 3-month follow-up, there was aonsignificant trend toward a reduction in adiponectin levels inhe amlodipine group (p � 0.067), and the change from the
Table 1. Baseline Patient, Angiographic, and Procedural Characteristics
Telmisartan(n � 21)
Amlodipine(n � 21) p Value
Age, yrs 67.9 � 8.9 66.6 � 8.7 0.62
Male 17 (81.0) 18 (85.7) 0.68
Body mass index, kg/m2 23.8 � 3.5 24.5 � 3.3 0.52
Diabetes mellitus 7 (33.3) 3 (14.3) 0.15
Dyslipidemia 12 (57.1) 9 (42.9) 0.35
Current smoker 5 (23.8) 5 (23.8) �0.99
Prior myocardial infarction 7 (33.3) 3 (14.3) 0.15
Prior PCI 10 (47.6) 5 (23.8) 0.10
Treated vessels
LAD/LCx/RCA 11/6/4 9/6/6 0.74
AHA/ACC type B2/C 18 (85.7) 16 (76.2) 0.43
Lesion length, mm 16.4 � 8.8 16.2 � 6.8 0.55
Reference vessel diameter, mm 2.63 � 0.33 2.81 � 0.38 0.10
%diameter stenosis, pre-intervention 61.1 � 8.6 63.2 � 10.0 0.46
%diameter stenosis, post-intervention 8.7 � 7.8 6.6 � 6.2 0.34
Number of stents, 1 stent/2 stents 18/3 19/2 0.99
Stent diameter, mm 3.0 � 0.4 3.0 � 0.4 �0.99
Stent length, mm 22.5 � 11.0 20.5 � 8.6 0.52
Final balloon pressure, atm 17.6 � 3.2 18.9 � 3.0 0.17
Values are mean � SD or n (%).
ACC � American College of Cardiology; AHA � American Heart Association; LAD � left anterior
descending coronary artery; LCx � left circumflex coronary artery; PCI � percutaneous coronary
intervention; RCA � right coronary artery.
Table 2. Medication During Follow-Up Periods
Telmisartan(n � 21)
Amlodipine(n � 21) p Value
Telmisartan, mg 78.1 � 8.8 — NA
Amlodipine, mg — 7.9 � 2.5 NA
Beta-blockers 0 (0) 2 (9.5) 0.15
Alpha-blockers 2 (9.5) 5 (23.8) 0.21
Diuretics 4 (19.0) 6 (28.6) 0.47
Oral glycemic agents 7 (33.3) 3 (14.3) 0.14
Pioglitazone 0 (0) 0 (0) �0.99
Insulin 0 (0) 0 (0) �0.99
Aspirin 21 (100) 21 (100) �0.99
Clopidogrel 21 (100) 21 (100) �0.99
Cilostazol 1 (4.8) 0 (0) 0.31
Values are mean � SD or n (%).
NA � not applicable.
rssl(itil
3cactn
twi
tw
D
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S , V O L . 5 , N O . 2 , 2 0 1 2
F E B R U A R Y 2 0 1 2 : 1 8 2 – 9 0
Terashima et al.
Effects of Telmisartan on Endothelial Function
186
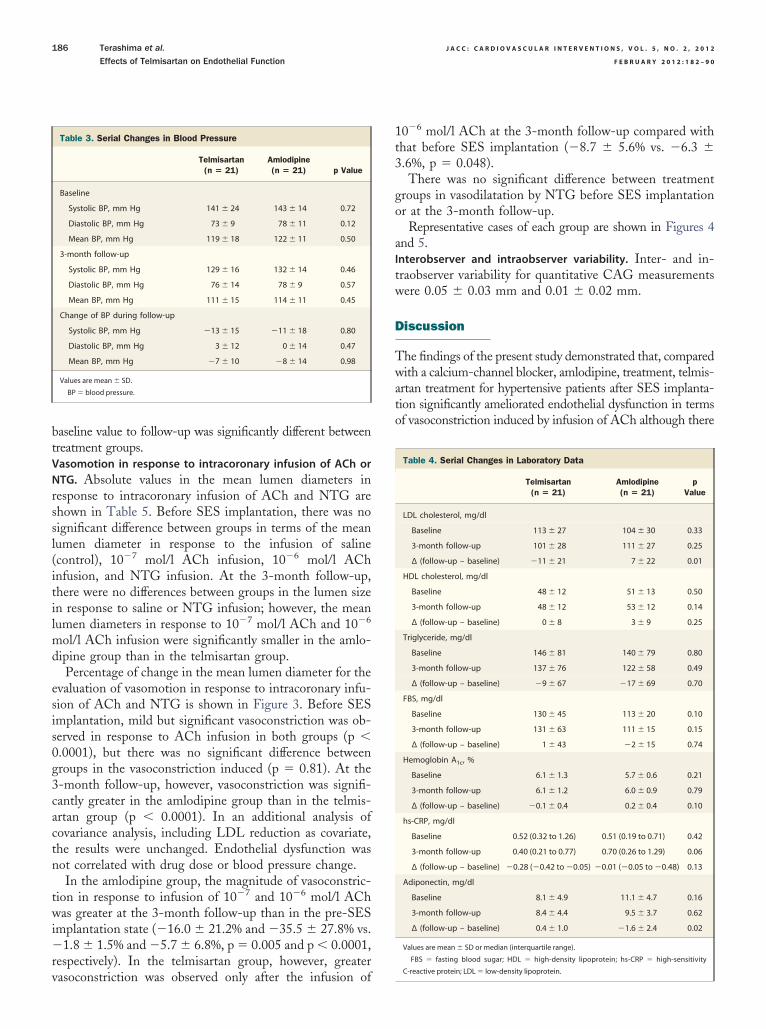
baseline value to follow-up was significantly different betweentreatment groups.Vasomotion in response to intracoronary infusion of ACh orNTG. Absolute values in the mean lumen diameters inesponse to intracoronary infusion of ACh and NTG arehown in Table 5. Before SES implantation, there was noignificant difference between groups in terms of the meanumen diameter in response to the infusion of salinecontrol), 10�7 mol/l ACh infusion, 10�6 mol/l AChnfusion, and NTG infusion. At the 3-month follow-up,here were no differences between groups in the lumen sizen response to saline or NTG infusion; however, the meanumen diameters in response to 10�7 mol/l ACh and 10�6
mol/l ACh infusion were significantly smaller in the amlo-dipine group than in the telmisartan group.
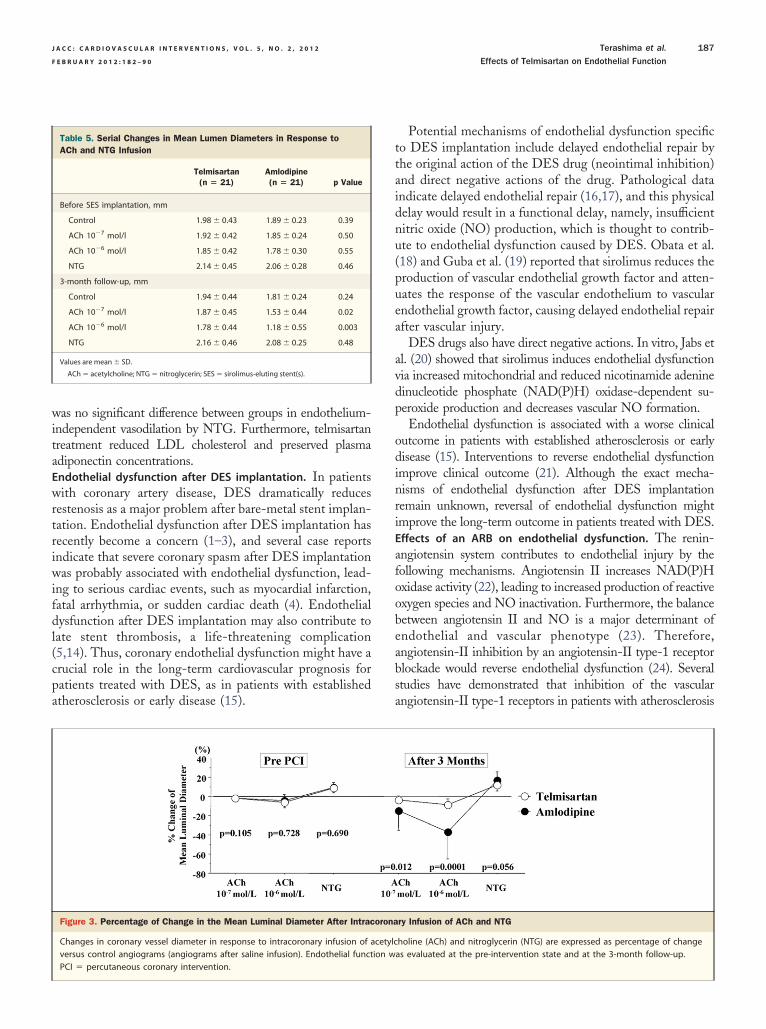
Percentage of change in the mean lumen diameter for theevaluation of vasomotion in response to intracoronary infu-sion of ACh and NTG is shown in Figure 3. Before SESimplantation, mild but significant vasoconstriction was ob-served in response to ACh infusion in both groups (p �0.0001), but there was no significant difference betweengroups in the vasoconstriction induced (p � 0.81). At the-month follow-up, however, vasoconstriction was signifi-antly greater in the amlodipine group than in the telmis-rtan group (p � 0.0001). In an additional analysis ofovariance analysis, including LDL reduction as covariate,he results were unchanged. Endothelial dysfunction wasot correlated with drug dose or blood pressure change.In the amlodipine group, the magnitude of vasoconstric-
ion in response to infusion of 10�7 and 10�6 mol/l AChas greater at the 3-month follow-up than in the pre-SES
mplantation state (�16.0 � 21.2% and �35.5 � 27.8% vs.�1.8 � 1.5% and �5.7 � 6.8%, p � 0.005 and p � 0.0001,respectively). In the telmisartan group, however, greater
Table 3. Serial Changes in Blood Pressure
Telmisartan(n � 21)
Amlodipine(n � 21) p Value
Baseline
Systolic BP, mm Hg 141 � 24 143 � 14 0.72
Diastolic BP, mm Hg 73 � 9 78 � 11 0.12
Mean BP, mm Hg 119 � 18 122 � 11 0.50
3-month follow-up
Systolic BP, mm Hg 129 � 16 132 � 14 0.46
Diastolic BP, mm Hg 76 � 14 78 � 9 0.57
Mean BP, mm Hg 111 � 15 114 � 11 0.45
Change of BP during follow-up
Systolic BP, mm Hg �13 � 15 �11 � 18 0.80
Diastolic BP, mm Hg 3 � 12 0 � 14 0.47
Mean BP, mm Hg �7 � 10 �8 � 14 0.98
Values are mean � SD.
BP � blood pressure.
vasoconstriction was observed only after the infusion of
10�6 mol/l ACh at the 3-month follow-up compared withthat before SES implantation (�8.7 � 5.6% vs. �6.3 �3.6%, p � 0.048).
There was no significant difference between treatmentgroups in vasodilatation by NTG before SES implantationor at the 3-month follow-up.
Representative cases of each group are shown in Figures 4and 5.Interobserver and intraobserver variability. Inter- and in-raobserver variability for quantitative CAG measurementsere 0.05 � 0.03 mm and 0.01 � 0.02 mm.
iscussion
The findings of the present study demonstrated that, comparedwith a calcium-channel blocker, amlodipine, treatment, telmis-artan treatment for hypertensive patients after SES implanta-tion significantly ameliorated endothelial dysfunction in termsof vasoconstriction induced by infusion of ACh although there
Table 4. Serial Changes in Laboratory Data
Telmisartan(n � 21)
Amlodipine(n � 21)
pValue
LDL cholesterol, mg/dl
Baseline 113 � 27 104 � 30 0.33
3-month follow-up 101 � 28 111 � 27 0.25
∆ (follow-up – baseline) �11 � 21 7 � 22 0.01
HDL cholesterol, mg/dl
Baseline 48 � 12 51 � 13 0.50
3-month follow-up 48 � 12 53 � 12 0.14
∆ (follow-up – baseline) 0 � 8 3 � 9 0.25
Triglyceride, mg/dl
Baseline 146 � 81 140 � 79 0.80
3-month follow-up 137 � 76 122 � 58 0.49
∆ (follow-up – baseline) �9 � 67 �17 � 69 0.70
FBS, mg/dl
Baseline 130 � 45 113 � 20 0.10
3-month follow-up 131 � 63 111 � 15 0.15
∆ (follow-up – baseline) 1 � 43 �2 � 15 0.74
Hemoglobin A1c, %
Baseline 6.1 � 1.3 5.7 � 0.6 0.21
3-month follow-up 6.1 � 1.2 6.0 � 0.9 0.79
∆ (follow-up – baseline) �0.1 � 0.4 0.2 � 0.4 0.10
hs-CRP, mg/dl
Baseline 0.52 (0.32 to 1.26) 0.51 (0.19 to 0.71) 0.42
3-month follow-up 0.40 (0.21 to 0.77) 0.70 (0.26 to 1.29) 0.06
∆ (follow-up – baseline) �0.28 (�0.42 to �0.05) �0.01 (�0.05 to �0.48) 0.13
Adiponectin, mg/dl
Baseline 8.1 � 4.9 11.1 � 4.7 0.16
3-month follow-up 8.4 � 4.4 9.5 � 3.7 0.62
∆ (follow-up – baseline) 0.4 � 1.0 �1.6 � 2.4 0.02
Values are mean � SD or median (interquartile range).
FBS � fasting blood sugar; HDL � high-density lipoprotein; hs-CRP � high-sensitivity
C-reactive protein; LDL � low-density lipoprotein.
wrtriwifdl(cpa
ttaidnu(puea
avdp
odinri
afoobeabsa
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S , V O L . 5 , N O . 2 , 2 0 1 2 Terashima et al.
F E B R U A R Y 2 0 1 2 : 1 8 2 – 9 0 Effects of Telmisartan on Endothelial Function
187
was no significant difference between groups in endothelium-independent vasodilation by NTG. Furthermore, telmisartantreatment reduced LDL cholesterol and preserved plasmaadiponectin concentrations.Endothelial dysfunction after DES implantation. In patients
ith coronary artery disease, DES dramatically reducesestenosis as a major problem after bare-metal stent implan-ation. Endothelial dysfunction after DES implantation hasecently become a concern (1–3), and several case reportsndicate that severe coronary spasm after DES implantationas probably associated with endothelial dysfunction, lead-
ng to serious cardiac events, such as myocardial infarction,atal arrhythmia, or sudden cardiac death (4). Endothelialysfunction after DES implantation may also contribute toate stent thrombosis, a life-threatening complication5,14). Thus, coronary endothelial dysfunction might have arucial role in the long-term cardiovascular prognosis foratients treated with DES, as in patients with establishedtherosclerosis or early disease (15).
Table 5. Serial Changes in Mean Lumen Diameters in Response toACh and NTG Infusion
Telmisartan(n � 21)
Amlodipine(n � 21) p Value
Before SES implantation, mm
Control 1.98 � 0.43 1.89 � 0.23 0.39
ACh 10�7 mol/l 1.92 � 0.42 1.85 � 0.24 0.50
ACh 10�6 mol/l 1.85 � 0.42 1.78 � 0.30 0.55
NTG 2.14 � 0.45 2.06 � 0.28 0.46
3-month follow-up, mm
Control 1.94 � 0.44 1.81 � 0.24 0.24
ACh 10�7 mol/l 1.87 � 0.45 1.53 � 0.44 0.02
ACh 10�6 mol/l 1.78 � 0.44 1.18 � 0.55 0.003
NTG 2.16 � 0.46 2.08 � 0.25 0.48
Values are mean � SD.
ACh � acetylcholine; NTG � nitroglycerin; SES � sirolimus-eluting stent(s).
Figure 3. Percentage of Change in the Mean Luminal Diameter After Intrac
Changes in coronary vessel diameter in response to intracoronary infusion of aversus control angiograms (angiograms after saline infusion). Endothelial funct
PCI � percutaneous coronary intervention.Potential mechanisms of endothelial dysfunction specifico DES implantation include delayed endothelial repair byhe original action of the DES drug (neointimal inhibition)nd direct negative actions of the drug. Pathological datandicate delayed endothelial repair (16,17), and this physicalelay would result in a functional delay, namely, insufficientitric oxide (NO) production, which is thought to contrib-te to endothelial dysfunction caused by DES. Obata et al.18) and Guba et al. (19) reported that sirolimus reduces theroduction of vascular endothelial growth factor and atten-ates the response of the vascular endothelium to vascularndothelial growth factor, causing delayed endothelial repairfter vascular injury.
DES drugs also have direct negative actions. In vitro, Jabs etl. (20) showed that sirolimus induces endothelial dysfunctionia increased mitochondrial and reduced nicotinamide adenineinucleotide phosphate (NAD(P)H) oxidase-dependent su-eroxide production and decreases vascular NO formation.Endothelial dysfunction is associated with a worse clinical
utcome in patients with established atherosclerosis or earlyisease (15). Interventions to reverse endothelial dysfunction
mprove clinical outcome (21). Although the exact mecha-isms of endothelial dysfunction after DES implantationemain unknown, reversal of endothelial dysfunction mightmprove the long-term outcome in patients treated with DES.Effects of an ARB on endothelial dysfunction. The renin-ngiotensin system contributes to endothelial injury by theollowing mechanisms. Angiotensin II increases NAD(P)Hxidase activity (22), leading to increased production of reactivexygen species and NO inactivation. Furthermore, the balanceetween angiotensin II and NO is a major determinant ofndothelial and vascular phenotype (23). Therefore,ngiotensin-II inhibition by an angiotensin-II type-1 receptorlockade would reverse endothelial dysfunction (24). Severaltudies have demonstrated that inhibition of the vascularngiotensin-II type-1 receptors in patients with atherosclerosis
ry Infusion of ACh and NTG
holine (ACh) and nitroglycerin (NTG) are expressed as percentage of changeas evaluated at the pre-intervention state and at the 3-month follow-up.
orona
cetylcion w
ig
eous
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S , V O L . 5 , N O . 2 , 2 0 1 2
F E B R U A R Y 2 0 1 2 : 1 8 2 – 9 0
Terashima et al.
Effects of Telmisartan on Endothelial Function
188
improves coronary and peripheral vasomotion (7–9). Angio-tensin receptor blockers also appear to reduce endothelialmarkers of inflammation and oxidative stress (25).
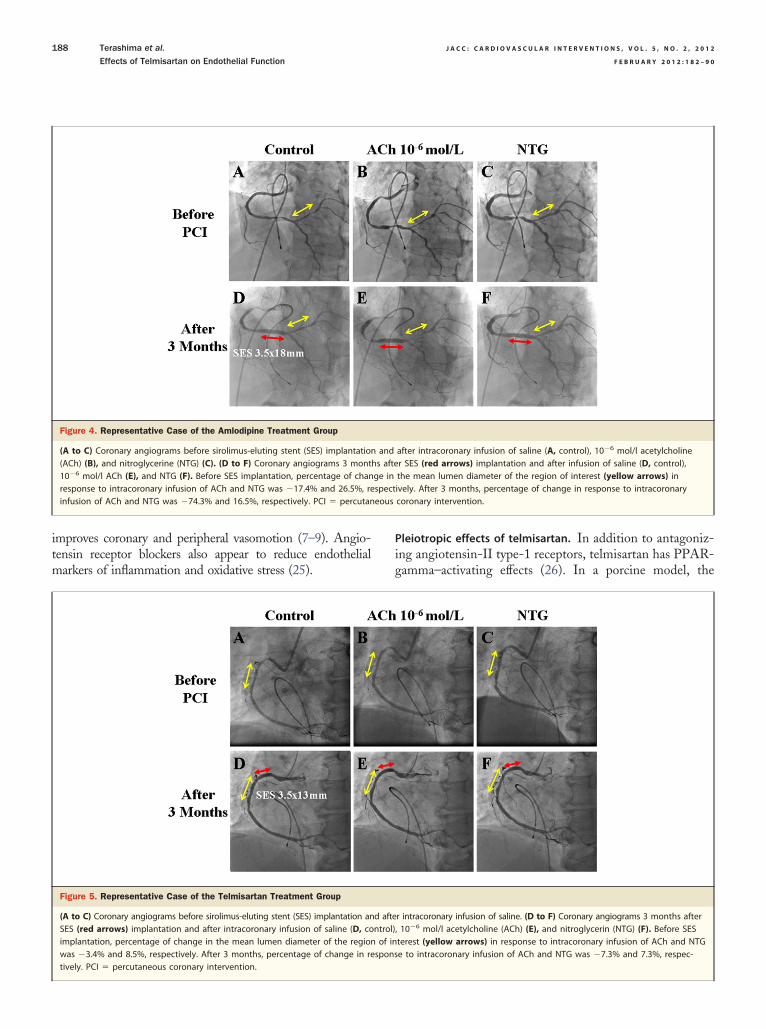
Figure 4. Representative Case of the Amlodipine Treatment Group
(A to C) Coronary angiograms before sirolimus-eluting stent (SES) implantation(ACh) (B), and nitroglycerine (NTG) (C). (D to F) Coronary angiograms 3 mont10�6 mol/l ACh (E), and NTG (F). Before SES implantation, percentage of chanresponse to intracoronary infusion of ACh and NTG was �17.4% and 26.5%, reinfusion of ACh and NTG was �74.3% and 16.5%, respectively. PCI � percutan
Figure 5. Representative Case of the Telmisartan Treatment Group
(A to C) Coronary angiograms before sirolimus-eluting stent (SES) implantation anSES (red arrows) implantation and after intracoronary infusion of saline (D, coimplantation, percentage of change in the mean lumen diameter of the regionwas �3.4% and 8.5%, respectively. After 3 months, percentage of change in re
tively. PCI � percutaneous coronary intervention.Pleiotropic effects of telmisartan. In addition to antagoniz-ng angiotensin-II type-1 receptors, telmisartan has PPAR-amma–activating effects (26). In a porcine model, the
after intracoronary infusion of saline (A, control), 10�6 mol/l acetylcholiner SES (red arrows) implantation and after infusion of saline (D, control),the mean lumen diameter of the region of interest (yellow arrows) inively. After 3 months, percentage of change in response to intracoronarycoronary intervention.
r intracoronary infusion of saline. (D to F) Coronary angiograms 3 months after, 10�6 mol/l acetylcholine (ACh) (E), and nitroglycerin (NTG) (F). Before SESterest (yellow arrows) in response to intracoronary infusion of ACh and NTGe to intracoronary infusion of ACh and NTG was �7.3% and 7.3%, respec-
andhs aftege inspect
d aftentrol)of inspons

J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S , V O L . 5 , N O . 2 , 2 0 1 2 Terashima et al.
F E B R U A R Y 2 0 1 2 : 1 8 2 – 9 0 Effects of Telmisartan on Endothelial Function
189
combination of candesartan and pioglitazone (a PPAR-gamma agonist) more effectively restored endothelial func-tion after SES implantation than candesartan monotherapydid (27). Because PPAR-gamma activation inhibits theexpression of inflammatory genes, the effect on endothelialfunction could potentially be mediated by an improvementin inflammation (28). Moreover, the inhibitory effects ofsirolimus on circulating endothelial progenitor cells wouldbe associated with delayed reendothelialization after SESimplantation. The benefits of PPAR-gamma agonists onthe endothelial progenitor cell endothelialization capacitywould improve endothelial dysfunction (29).
Telmisartan induces adiponectin protein expression inadipocytes at a post-transcriptional level via its PPAR-gamma–activating effect, leading to an increase in adiponec-tin plasma levels (30). Adiponectin is an adipocyte-specificplasma protein with anti-inflammatory, antiatherogenic,and antidiabetic properties (31), and it improves vascularendothelial function via several mechanisms, including en-hanced NO production by increased endothelial NO syn-thase activity and suppressed superoxide generation inendothelial cells through an NAD(P)H oxidase-linkedmechanism (32,33). In the present study, serum adiponectinconcentrations decreased in the amlodipine group, but notin the telmisartan group, during follow-up.
Further, serum LDL-cholesterol levels were significantlydecreased in the telmisartan treatment group but not in theamlodipine treatment group. Telmisartan effectively reducesLDL-cholesterol levels by different mechanisms than statins(34). Telmisartan may accelerate reverse cholesterol trans-port from nonhepatic peripheral cells to the liver, therebylowering LDL cholesterol. Furthermore, telmisartan mightinhibit intestinal cholesterol absorption via its PPAR-gamma–activating effect.
Thus, PPAR-gamma–mediated effects of telmisartanmight confer vascular protection through several mecha-nisms after SES implantation.Comparison between telmisartan and amlodipine in ameliorationof endothelial dysfunction after DES. Amlodipine improvesendothelial function and has antioxidant properties (35). Inthe present study, however, telmisartan treatment inducedsignificantly stronger amelioration of endothelial dysfunc-tion after DES implantation than amlodipine treatment did.Consistent with our results, a recent randomized studydemonstrated that, compared with the calcium-channelblocker amlodipine, telmisartan treatment improves endo-thelial function (flow-mediated dilation) in peripheral ves-sels in hypertensive patients (13).Study limitations. The present study was a single-centerstudy with a small sample size. The lesions involved inthe study were limited to a single stenosis suitable fortreatment with 1 or 2 SES. In addition, the present studyfocused on the first-generation DES (SES), although
second-generation DES are commonly used in currentpractice. Further studies are needed to examine whetherthis study finding is applicable to other DES, especiallysecond-generation DES.
Furthermore, the results of the present study are onlypreliminary; a larger number of subjects and a longerfollow-up for clinical outcomes are crucial to confirm theefficacy of telmisartan treatment for hypertensive patientswith DES implantation.
Conclusions
In this group of hypertensive patients, compared with treat-ment with a calcium-channel blocker, telmisartan treatmentsignificantly ameliorated endothelial dysfunction in terms ofACh-induced vasoconstriction after DES implantation.
AcknowledgmentsThe authors thank Masahisa Tsuzuki of Toyohashi HeartCenter (Toyohashi, Japan) and Satoru Hashimoto ofTCROSS Co. Ltd. (Tokyo, Japan) for their kind help.
Reprint requests and correspondence: Dr. Mitsuyasu Tera-shima, Department of Cardiology, Toyohashi Heart Center,21-1 Gobudori, Oyama-cho, Toyohashi 441-8530, Japan.E-mail: [email protected].
REFERENCES
1. Hofma SH, van der Giessen WJ, van Dalen BM, et al. Indication oflong-term endothelial dysfunction after sirolimus-eluting stent implan-tation. Eur Heart J 2006;27:166–70.
2. Shin DI, Seung KB, Kim PJ, et al. Long-term coronary endothelialfunction after zotarolimus-eluting stent implantation: a 9 monthcomparison between zotarolimus-eluting and sirolimus-eluting stents.Int Heart J 2008;49:639–52.
3. Kim JW, Seo HS, Park JH, et al. A prospective, randomized, 6-monthcomparison of the coronary vasomotor response associated with azotarolimus- versus a sirolimus-eluting stent: differential recovery ofcoronary endothelial dysfunction. J Am Coll Cardiol 2009;53:1653–9.
4. Brott BC, Anayiotos AS, Chapman GD, Anderson PG, Hillegass WB.Severe, diffuse coronary artery spasm after drug-eluting stent placement.J Invasive Cardiol 2006;18:584–92.
5. Togni M, Windecker S, Cocchia R, et al. Sirolimus-eluting stentsassociated with paradoxic coronary vasoconstriction. J Am Coll Cardiol2005;46:231–6.
6. Yusuf S, Teo KK, Pogue J, et al., for the ONTARGET Investigators.Telmisartan, ramipril, or both in patients at high risk for vascularevents. N Engl J Med 2008;358:1547–59.
7. Prasad A, Halcox JP, Waclawiw MA, Quyyumi AA. Angiotensin type1 receptor antagonism reverses abnormal coronary vasomotion inatherosclerosis. J Am Coll Cardiol 2001;38:1089–95.
8. Hornig B, Kohler C, Schlink D, Tatge H, Drexler H. AT1-receptorantagonism improves endothelial function in coronary artery disease bya bradykinin/B2-receptor-dependent mechanism. Hypertension 2003;41:1092–5.
9. Ceriello A, Assaloni R, Da Ros R, et al. Effect of atorvastatin andirbesartan, alone and in combination, on postprandial endothelialdysfunction, oxidative stress, and inflammation in type 2 diabeticpatients. Circulation 2005;111:2518–24.
10. Scalera F, Martens-Lobenhoffer J, Bukowska A, Lendeckel U, TägerM, Bode-Böger SM. Effect of telmisartan on nitric oxide—
asymmetrical dimethylarginine system: role of angiotensin II type 1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S , V O L . 5 , N O . 2 , 2 0 1 2
F E B R U A R Y 2 0 1 2 : 1 8 2 – 9 0
Terashima et al.
Effects of Telmisartan on Endothelial Function
190
receptor gamma and peroxisome proliferator activated receptor gammasignaling during endothelial aging. Hypertension 2008;51:696–703.
1. Ikejima H, Imanishi T, Tsujioka H, et al. Effects of telmisartan, aunique angiotensin receptor blocker with selective peroxisomeproliferator-activated receptor-gamma-modulating activity, on nitricoxide bioavailability and atherosclerotic change. J Hypertens 2008;26:964–72.
2. Yuen CY, Wong WT, Tian XY, et al. Telmisartan inhibits vasocon-striction via PPAR-gamma-dependent expression and activation ofendothelial nitric oxide synthase. Cardiovasc Res 2011;90:122–9.
3. Morimoto S, Yano Y, Maki K, Sawada K. Renal and vascularprotective effects of telmisartan in patients with essential hypertension.Hypertens Res 2006;29:567–72.
4. Pendyala LK, Yin X, Li J, Chen JP, Chronos N, Hou D. Thefirst-generation drug-eluting stents and coronary endothelial dysfunc-tion. J Am Coll Cardiol Intv 2009;2:1169–77.
5. Deanfield JE, Halcox JP, Rabelink TJ. Endothelial function anddysfunction: testing and clinical relevance. Circulation 2007;115:1285–95.
6. Joner M, Finn AV, Farb A, et al. Pathology of drug-eluting stents inhumans: delayed healing and late thrombotic risk. J Am Coll Cardiol2006;48:193–202.
7. Lüscher TF, Steffel J, Eberli FR, et al. Drug-eluting stent and coronarythrombosis: biological mechanisms and clinical implications. Circula-tion 2007;115:1051–8.
8. Obata JE, Kitta Y, Takano H, et al. Sirolimus-eluting stent implan-tation aggravates endothelial vasomotor dysfunction in the infarct-related coronary artery in patients with acute myocardial infarction.J Am Coll Cardiol 2007;50:1305–9.
9. Guba M, von Breitenbuch P, Steinbauer M, et al. Rapamycin inhibitsprimary and metastatic tumor growth by antiangiogenesis: involvementof vascular endothelial growth factor. Nat Med 2002;8:128–35.
0. Jabs A, Göbel S, Wenzel P, et al. Sirolimus-induced vascular dysfunc-tion: increased mitochondrial and nicotinamide adenosine dinucleotidephosphate oxidase-dependent superoxide production and decreasedvascular nitric oxide formation. J Am Coll Cardiol 2008;51:2130–8.
1. Yasue H, Mizuno Y, Harada E, et al., for the SCAST Investigators.Effects of a 3-hydroxy-3-methylglutaryl coenzyme A reductase inhib-itor, fluvastatin, on coronary spasm after withdrawal of calcium-channel blockers. J Am Coll Cardiol 2008;51:1742–8.
2. Griendling KK, Minieri CA, Ollerenshaw JD, Alexander RW. Ang-
iotensin II stimulates NADH and NADPH oxidase activity in culturedvascular smooth muscle cells. Circ Res 1994;74:1141–8.3. Gibbons GH. Cardioprotective mechanisms of ACE inhibition: theangiotensin II-nitric oxide balance. Drugs 1997;54 Suppl 5:1–11.
4. Prasad A, Tupas-Habib T, Schenke WH, et al. Acute and chronicangiotensin-1 receptor antagonism reverses endothelial dysfunction inatherosclerosis. Circulation 2000;101:2349–54.
5. Widlansky ME, Gokce N, Keaney JF Jr., Vita JA. The clinicalimplications of endothelial dysfunction. J Am Coll Cardiol 2003;42:1149–60.
6. Schupp M, Janke J, Clasen R, Unger T, Kintscher U. Angiotensin type1 receptor blockers induce peroxisome proliferator-activated receptor-gamma activity. Circulation 2004;109:2054–7.
7. Dohi T, Miyauchi K, Iesaki T, et al. Candesartan with pioglitazoneprotects against endothelial dysfunction and inflammatory responses inporcine coronary arteries implanted with sirolimus-eluting stents. CircJ 2011;75:1098–106.
8. Barbier O, Torra IP, Duguay Y, et al. Pleiotropic actions of peroxisomeproliferator-activated receptors in lipid metabolism and atherosclerosis.Arterioscler Thromb Vasc Biol 2002;22:717–26.
9. Honda A, Matsuura K, Fukushima N, Tsurumi Y, Kasanuki H,Hagiwara N. Telmisartan induces proliferation of human endothelialprogenitor cells via PPAR-gamma-dependent PI3K/Akt pathway.Atherosclerosis 2009;205:376–84.
0. Clasen R, Schupp M, Foryst-Ludwig A, et al. PPAR-gamma-activating angiotensin type-1 receptor blockers induce adiponectin.Hypertension 2005;46:137–43.
1. Barseghian A, Gawande D, Bajaj M. Adiponectin and vulnerableatherosclerotic plaques. J Am Coll Cardiol 2011;57:761–70.
2. Chen H, Montagnani M, Funahashi T, Shimomura I, Quon MJ.Adiponectin stimulates production of nitric oxide in vascular endothe-lial cells. J Biol Chem 2003;278:45021–6.
3. Motoshima H, Wu X, Mahadev K, Goldstein BJ. Adiponectinsuppresses proliferation and superoxide generation and enhances eNOSactivity in endothelial cells treated with oxidized LDL. BiochemBiophys Res Commun 2004;315:264–71.
4. Inoue T, Node K. Telmisartan as a metabolic sartan for targetingvascular failure. Expert Opin Pharmacother 2008;9:1397–406.
5. Zhang X, Hintze TH. Amlodipine releases nitric oxide from caninecoronary microvessels: an unexpected mechanism of action of a calciumchannel-blocking agent. Circulation 1998;97:576–80.
Key Words: acetylcholine � angiotensin-II receptor blocker �
drug-eluting stent(s) � endothelial function � vasoconstriction.

















