Protecting Ourselves: Practical Skills to Manage … Ourselves John...Protecting Ourselves:...
37
Protecting Ourselves: Practical Skills to Manage Verbal and Physical Aggression Long Term and Continuing Care Association of Manitoba May 2016 Presenter: John Thomas Geriatric Mental Health Consultant
-
Upload
truongcong -
Category
Documents
-
view
214 -
download
0
Transcript of Protecting Ourselves: Practical Skills to Manage … Ourselves John...Protecting Ourselves:...

Protecting Ourselves:Practical Skills to Manage
Verbal and Physical Aggression
Long Term and Continuing Care Association of Manitoba
May 2016
Presenter: John Thomas
Geriatric Mental Health Consultant

Healthcare Time Loss Injuries in Manitoba, 2014
More than 51% of injuries are sustained by registered nurses, nursing aides and patient service associates;
Although more than 55% of time loss injuries were from overexertion and bodily reaction, 7.5% of injuries were due to assaults, violent acts and harassment.
Source: SAFE Work Manitoba, 2015

OBJECTIVES
1. Discuss the experience of verbal aggression among long-term care providers
2. Draw on best practices as a guide for “better” behaviour management and self-protection against verbal aggression
3. Discuss the experience of physical aggression among care providers
4. Demonstrate safe and respectful physical methods of self-protection

Verbal Aggression
Examples of verbal aggression can include, but are not limited to:
Foul language / cursing
Physical insults
Racial slurs
Threats
Accusations of incompetence

The “difficult” resident
Take a moment to think about someone with whom you have worked that was considered to be “difficult” due to episodes of verbal aggression.
What was that like?
In long-term care, these individuals may consume disproportionate staff attention leading to negative attitudes, lowered morale and displaced frustration affecting the care of all residents. (Rosowsky and Smyer, 1999)
Staff often face the dilemma of their conflicting desires to support resident autonomy and enforce the collective good of the facility. (Himelick and Walsh, 2002)

Case ExampleMrs. F S
- 84 year old divorced female living in long-term-care since 2013. She had previously resided in a retirement home for two years prior to her LTC admission
-Medical diagnoses include CVA (2012) with resulting left hemi paresis, Type II diabetes, hypertension
-Mental health diagnoses include a history of depression, mild cognitive impairment and narcissistic personality traits (although there is no formal personality disorder diagnosis on her medical record)
-Social history includes being from a small family, no siblings, a retired Canada customs official, mother of two daughters but otherwise has a limited social network
-Nursing staff reported enduring verbal assaults including rude and vulgar dismissals, racial slurs, accusations of incompetence including belittling comments about caregiver credentials and threats of being reported to higher authorities
-Two frontline care providers cited this resident as why they asked to be transferred to another care team

Management begins with a systematic search for causes...
Possible Causes for Mrs. S’ behaviour
Q2. What are the RISKS and possible causes?
RISKS? Kinship – employee burnout
P - PHYSICAL Pain was queried but well managed using analgesics
I - INTELLECTUAL Query problems with executive functioning and disinhibition due to possible frontal lobe dysfunction
E - EMOTIONAL Query depression but examinations determined it was in remissionNarcissistic personality traits – possible personality disorder?
C - CAPABILITIES Not considered a factor
E - ENVIRONMENT Social context – most care providers were not Jewish and from a visible minority
S – SOCIAL / CULTURAL
Daughter reported her mother could be overtly racistHistory of compromised relationships and limited social support network
Q1. Rude dismissals, racial slurs, accusations of incompetence, belittling, threats usually occurring, but not always, during the provision of care.

When most causes of verbal aggression have been ruled out, can personality be a key contributor?
Indeed!
Personality traits such as dependence, anti-social tendencies and narcissism begin early in the life course (Lee, Brodaty and Draper, 2002).
Although few of our residents will meet criteria for a personality disorder (PD) diagnosis, we look after several who have been labelled as “difficult” and can’t ignore the contribution of personality style. We can borrow from PD best practices to build capacity and assist with managing behaviours while protecting our staff.

Personality Disorder – Definition
Personality disorders are associated with ways of thinking and feeling about oneself and others that significantly and adversely affect how an individual functions in many aspects of life. They fall within 10 distinct types: paranoid personality disorder, schizoid personality disorder, schizotypal personality disorder, antisocial personality disorder, borderline personality disorder, histrionic personality, narcissistic personality disorder, avoidant personality disorder, dependent personality disorder and obsessive-compulsive personality disorder. (American Psychiatric Association, 2013)

What can we glean from PD literature about looking after people in institutionalized settings?
Embedded in established guidelines is the notion of self-protection. Staff may be vulnerable if the resident is skilled at manipulating the behaviours of others and playing caregivers against each other (Himelick and Walsh, 2002).
There are several themes in the literature:
Team consistency
Establishing clear boundaries
Alternating periods of confrontation (feedback) with periods of support; empathy
Deliberate efforts by the organization to support care providers
(Gibson and Ferrini, 2012)

To Protect our PersonnelOur Focus May Need to Change

Self-Protection
The idea of protecting oneself against verbal attacks and unpleasantries will vary among individuals and situations. Some individuals, based on the circumstances, may elect to do nothing. Nevertheless, an organization can deliberately facilitate a climate of fairness and mutual respect between residents and care personnel.
Elements of self-protection can include:
Providing feedback on a resident’s behaviour to the resident his/herself
Stating that noxious verbalizations are being felt by the care provider
Offering choices
Engaging the resident in collaborative problem solving
(Robinson and Schogt, 2007)

Guidelines for Dealing with Behaviours in Institutionalized Settings(Institut universitaire en santé mentale de Québec, 2012)
DO’s DO NOT’s
•Adopt a calm but firm attitude• Have a consistent and systematic team approach•Establish a team action plan to be implemented by all, in the same way•Identify the benefits to the client who persists withthe unacceptable behavior•Give short, clear instructions on what is expected of the person•Short and precise explanations on what is acceptable and what is not•Inform the person about the possible consequences of their behavior and risks incurred for his/her own safety (e.g. For not receiving care)•Verbally value socially acceptable behavior
•Argue•Ignore the problem or behaviour (this may give implicit authorization for its continuation)•Threaten to punish •Lose patience •Speak loudly
•Use humour; audience is susceptible to misinterpretation and suspicion•Humour can also be perceived as belittling the client’s concerns and/or erode all too important boundaries (McVey, 2010)
Source: Notions de base sur les maladies mentales – Guide pratique d’intervention

Self-Protection Skills Used
Allowing greater personal space
Use of empathy regarding what the client may be feeling, either physically or emotionally
Feedback to the client about her behaviour and how it is affecting the care provider
Providing an alternative or choices
Removal from the care situation if it safe to do so

Mrs. F SSelf-Protection focused interventions
Q3. What (was) the action?
The unit social worker attempted to collaborate with the resident on drafting a behavioural contract. This was met with limited success.
The team decided on a script to be used consistently whenever she was verbally abusive. The message included feedback on her behaviour as well as empathy for any distress (either physical or emotional) she might be feeling at the time.
The unit social worker made deliberate attempts to meet with care providers to give them a chance to debrief about recent experiences and evaluate the plan.
Although there was no significant change in the resident’s behaviour after one month, staff reported feeling better equipped to deal with her verbalizations. Nevertheless, they still endorsed resident transfer to another unit. Burn out cited; interventions came too late?

Physical Aggression
Examples of physical aggression can include, but are not limited to:Grabs of all sorts
Hits, slaps, kicks, punches
Pinches
Scratches
Hair Pulls
Spitting
Splashing

Physical AggressionSelf-Protection
Despite our best efforts, sometimes situations can escalate to acts of physical aggression from resident to care provider. Countless professionals endure injuries every year.
Most physically aggressive gestures are in the form of grabs and strikes. Despite the dangerous nature of these events, we can protect ourselves in a safe, respectful manner!
The following senior-friendly demonstrations will cover:
The basic grab
The two-handed grab
The seated grab
The two-person containment
Deflecting a strike

DISCLAIMER
The following demonstrations of physical self-protection techniques are for information purposes only. They do not replace formal training in these procedures and should only be used with discretion by session participants.
John Thomas, New Insight and Baycrest accept no liability for the improper use of these techniques.


1. Secure the arm of the client. 2. Locate the gap, open space or weak spot in the
client’s grip.
3. While keeping the arm of the client secure, swiftly move your arm in the direction of the weak spot. To preserve client safety, DO NOT twist or move your arm in any other direction.

When there is no weak spot or open space, target the second weakest part of the client’s grip – the thumb.
Gently grasp the thumb joint knuckle and displace it. Never peel back fingers!

If the client grabs hold of something and won’t let go…
Try offering a meaningful substitute.


1. Without attempting to loosen the client’s grip, reach over with one arm and secure one of the client’s arms.
2. With the client’s arm secure, move your arm in the direction of the weak spot. Do not let go of the client’s arm to maintain control and prevent a strike.3. Use your free hand to secure the client’s other arm and repeat the procedure.

4. If the client’s grab has no open space or weak spot, open the grip by displacing the client’s thumb at the knuckle. Remember, NEVER peel back thumbs or fingers!


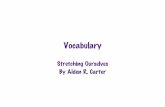
1. Loosen your arm, but keep it straight. Use your free hand to gently secure the client’s arm closest to you.
2. Gently lower your grabbed arm a few centimetres. DO NOT push down on the client’s arm you have secured.
3. While keeping your free hand stable and in the same position, swiftly pop up your grabbed arm. This should create an open space in the client’s grip.4. Move your arm against the weak spot.

For added safety, you can follow the procedure for the basic grab by securing the client’s arm before your final escape!

For Redirection or Provision of Emergency Care

1. Two care providers position themselves on either side of the client. He/She must be ambulatory in order to use this technique.
2. Using the outside hand, gently secure the client’s arm just above his/her wrist. Ensure the client’s arms are straight and at his/her side.

3. Bring your other arm underneath the client’s shoulder and firmly secure your own arm. Remember to ensure the client’s arms are straight.
4. Caregivers can use their hips to keep the client secure. Placing one’s knee behind the client’s thigh can prevent him/her from falling.


“Wipe” Method
1. Once a strike threat is perceived, immediately raise your open hand. It must be flat and firm, as if you were wiping an imaginary surface.
2. Allow your hand to intercept the client’s strike.

3. “Wipe” the strike away. Remove yourself from the client immediately if it is safe to do so. Call for assistance if you need to remain with the client.

SUMMARYTake Home Messages
Client to care provider verbal and physical aggression is an ever present issue that affects the safety, morale and psychological well-being of our care team members
Each situation first warrants a systematic search for causes; PIECES 3-Q template can help us do that
Once all modifiable causes have been explored, acknowledge that personality style might be a key contributor to difficult behaviours
Although management strategies must be individualized, we can transfer principles for working with clients with PDs to the “difficult” clients in long-term care settings
Know when to shift the focus of interventions from behaviour modification to self-protection for the care team (before it’s too late!)
For the ongoing safety and preservation of our valued care providers, something can be done! Ensure that responsive behaviours training includes a self-protection component

ACKNOWLEDGEMENTS
Behavioural Support Resource TeamDownsview Long-Term-Care CentreToronto, ON
Volunteer Services

John Thomas
Geriatric Mental Health Consultant
Toronto, Ontario
(416) 833-1833
E-mail: [email protected]
Web: www.newinsight.ca