Prostate Cancer Early Detection€¦ · PROSTATE CANCER - EARLY DETECTION April 2018 Page 3 of 15...
15
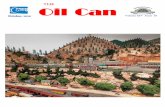
PROSTATE CANCER - EARLY DETECTION April 2018 Page 1 of 15 This map was published by MidCentral District. A printed version of this document is not controlled so may not be up-to-date with the latest clinical information. Prostate Cancer – Early Detection Oncology > Oncology > Prostate cancer Presenting symptoms Notes for MidCentral/ and/or concerns Whanganui Regions Level of understanding and engagement Assessment, Family History, Risk Factors RED FLAGS! URGENT referral to ED Consider differential diagnosis Examination/Testing - PSA, DRE declined - DRE, PSA NO further action Normal PSA and DRE Abnormal PSA Abnormal DRE Check first-degree relative RED FLAGS! Referral to supportive care services Discuss follow up options Treat UTI or Prostatitis if present Refer to Urology Repeat PSA after 6-12 weeks/review results Normal PSA Abnormal PSA Check first-degree relative Referral to supportive care services Refer to Urology Discuss follow up options Care map information Information resources patients and clinicians Updates to this care map Faster Cancer Treatment Targets Hauora Māori Pasifika
Transcript of Prostate Cancer Early Detection€¦ · PROSTATE CANCER - EARLY DETECTION April 2018 Page 3 of 15...
-
PROSTATE CANCER - EARLY DETECTION April 2018 Page 1 of 15
This map was published by MidCentral District. A printed version of this document is not controlled so may not be up-to-date with the latest clinical information.
Prostate Cancer – Early Detection Oncology > Oncology > Prostate cancer
Presenting symptoms Notes for MidCentral/
and/or concerns Whanganui Regions
Level of understanding
and engagement
Assessment, Family
History, Risk Factors
RED FLAGS!
URGENT referral
to ED
Consider differential
diagnosis
Examination/Testing - PSA, DRE declined -
DRE, PSA NO further action
Normal PSA and DRE Abnormal PSA Abnormal DRE
Check first-degree
relative RED FLAGS! Referral to supportive
care services
Discuss follow up
options
Treat UTI or Prostatitis
if present Refer to Urology
Repeat PSA after 6-12
weeks/review results
Normal PSA Abnormal PSA
Check first-degree
relative
Referral to supportive
care services
Refer to Urology Discuss follow up
options
Care map information Information resources
patients and clinicians
Updates to this care
map
Faster Cancer
Treatment Targets
Hauora Māori Pasifika
-
PROSTATE CANCER - EARLY DETECTION April 2018 Page 2 of 15
This map was published by MidCentral District. A printed version of this document is not controlled so may not be up-to-date with the latest clinical information.
1. Faster Cancer Treatment Targets
Faster Cancer Treatment Targets [3]
The Faster Cancer Treatment (FCT) health target builds on the significant improvements that have been made in the quality of
cancer services over recent years. It provides a lens across the whole cancer pathway to ensure people have prompt access to
excellent cancer services.
Faster cancer treatment health target:
• 85 percent of patients receive their first cancer treatment (or other management) within 62 days of being referred with a high
suspicion of cancer and a need to be seen within two weeks by July 2016, increasing to 90 percent by June 2017. [3]
For more information:
• faster cancer treatment programme
References:
3. Faster Cancer Treatment Programme, Ministry of Health.
2.Care map information
In Scope:
Diagnosis and referral to secondary services.
Out of scope:
Treatment in secondary services.
Ministry of Health
Prostate cancer is a significant burden to men’s health. It is now one of the most important problems facing New Zealand men.
In 2013 the Ministry of Health launched a four year Prostate Cancer Awareness and Quality Improvement Programme (AQIP) to
improve outcomes for men with prostate cancer.
General practice plays an important role in helping men make decisions about prostate cancer checks and treatment. Work is under
way to develop guidance, training and tools (including a decision support tool) to help GPs and other health professionals provide
consistent, quality prostate care. [2]
This work includes:
• development of a decision support tool to facilitate discussion and shared decision making between men and GPs (and other
primary care providers)
• enhancements to patient management systems to help primary care services manage men with prostate cancer and track
patients against agreed care plans
• better integration of referral systems within DHBs
• development of content for training and education for GPs and other health professionals
About this pathway: This pathway is based on the Ministry of Health's Prostate Cancer Management and Referral Guidance
document which is a decision support tool to help primary care practitioners provide men and their families/whānau with support
around decision making, it is consistent, culturally appropriate information on prostate cancer testing and treatment.
The guidance document has been endorsed by:
• The Royal New Zealand College of General Practitioners
• The Prostate Cancer Foundation of New Zealand
• The Urological Society of Australia and New Zealand
http://www.health.govt.nz/our-work/diseases-and-conditions/cancer-programme/faster-cancer-treatment-programme
-
PROSTATE CANCER - EARLY DETECTION April 2018 Page 3 of 15
This map was published by MidCentral District. A printed version of this document is not controlled so may not be up-to-date with the latest clinical information.
• The New Zealand Urological Nurses Society
• The New Zealand Society of Pathologists.
NB: When using this guidance/pathway, primary care practitioners should be conscious of the disparities that exist in prostate
cancer outcomes for different men, such as for Māori men or men who live in rural areas. For example, Māori men are less likely to
be diagnosed with prostate cancer than non-Māori men, but are 37 percent more likely to die from the disease [1]
References:
1. Prostate Cancer Management and Referral Guidance, Ministry of Health.
2. Prostate Cancer Awareness and Quality Improvement Programme, Ministry of Health.
3.Information resources patients and clinicians
Resources for patients and carers:
• diagnosis and management of prostate cancer nz men
• getting checked for Prostate Cancer, a quick guide for men and their families
• Prostate Cancer Foundation NZ - support groups available nationwide to assist prostate sufferers and their families
• patient resource - what prostate cancer patients really want [4]
• information for you and your family/whānau about your prostate cancer diagnosis and individual treatment programme
Information resources for clinicians.[1]
The benefits and risks of prostate cancer testing and treatment. The role of primary care practitioners is to provide men and their
family and whānau with clear and balanced information about the benefits and risks of prostate cancer testing, so that they can make
an informed decision on whether or not to proceed. The information that men need to make an informed decision is included below.
How primary care practitioners provide this information may need to change depending on each man’s individual needs.
Benefits of prostate cancer testing:
• men and their family and whānau can be reassured that prostate cancer is unlikely to be present if the man’s PSA and DRE are
normal
• if testing indicates that prostate cancer is present, it is likely to be early stage, meaning that the chance of cure is greater
• if a man is found to have localised, low-risk prostate cancer, he has the option of entering an active surveillance programme
• this will allow him to delay or avoid potential treatment-related harms
Risks of prostate cancer testing:
• PSA testing and DRE can produce false positives due to calcifications in the prostate, prostatitis, urinary tract infection, benign
prostatic hypertrophy, recent ejaculation or cycling
• PSA testing can also produce false negatives when the prostate cancer releases no or little PSA
Further information on the benefits and risks for the following:
• prostate biopsy
• curative treatment
• radical prostatectomy
• radiation therapy
Ministry of Health - Prostate Cancer Management and Referral Guidance document. [1]
He Anga Whakaahuru - Supportive Care Framework [5]
Improving the quality of life for those with cancer, their family and whānau through support, rehabilitation and palliative care ........ the
essential services required to meet a person’s physical, social, cultural, emotional, nutritional, informational, psychological, spiritual
and practical needs throughout their experience with cancer.
https://thinkhauorawebsite.blob.core.windows.net/websitepublished/CCP/Resources/General%20Cancer%20docs/Prostate/Patient%20Resources/diagnosis-management-prostate-cancer-nz-men.pdfhttps://thinkhauorawebsite.blob.core.windows.net/websitepublished/CCP/Resources/General%20Cancer%20docs/Prostate/Patient%20Resources/HE2400_Getting-checked-for-prostate-cancer-quick-guide.pdfhttps://prostate.org.nz/support-groups/https://thinkhauorawebsite.blob.core.windows.net/websitepublished/CCP/Resources/General%20Cancer%20docs/Prostate/Patient%20Resources/What-Prostate-Cancer-Patients-Really-Really-Want-2017.pdfhttps://thinkhauorawebsite.blob.core.windows.net/websitepublished/CCP/Resources/General%20Cancer%20docs/Prostate/Patient%20Resources/WDHB%20Individual%20Prostate%20Cancer%20information%20booklet%20-%20draft%20version%202%20(1).pdfhttps://thinkhauorawebsite.blob.core.windows.net/websitepublished/CCP/Resources/General%20Cancer%20docs/Prostate/Benefits%20and%20Risks%20of%20Prostate%20Cancer%20Testing%20and%20Treatment.pdfhttp://www.health.govt.nz/publication/prostate-cancer-management-and-referral-guidance
-
PROSTATE CANCER - EARLY DETECTION April 2018 Page 4 of 15
This map was published by MidCentral District. A printed version of this document is not controlled so may not be up-to-date with the latest clinical information.
Further information on the Standards and Competencies
References:
1. Prostate Cancer Management and Referral Guidance, Ministry of Health.
4. Prostate Cancer Foundation NZ
5. Guidance for Improving Supportive Care for Adults with Cancer in New Zealand, Ministry of Health, 2010.
4.Updates to this care map
Date of publication: October 2017.
Please see the care map’s Provenance for information on references and contributors to this pathway.
5.Hauora Māori
Māori are a diverse people and whilst there is no single Māori identity, it is vital practitioners offer culturally appropriate care when
working with Māori Whānau. It is important for practitioners to have a baseline understanding of the issues surrounding Māori health.
This knowledge can be actualised by (not in any order of priority):
• acknowledging Te Whare Tapa Whā (Māori model of health) when working with Māori Whānau
• asking Māori clients if they would like their Whānau or significant others to be involved in assessment and treatment
• asking Māori clients about any particular cultural beliefs they or their Whānau have that might impact on assessment and
treatment of the particular health issue (Cultural issues)
• consider the importance of whānaungatanga (making meaningful connections) with their Māori client / Whānau
• knowledge of Whānau Ora, Te Ara Whānau Ora and referring to Whānau Ora Navigators where appropriate
• having a historical overview of legislation that has impacted on Māori well-being
For further information:
• Hauora Māori
6.Pasifika
Pacific Cultural Guidelines (Central PHO) 6MB file
Our Pasifika community:
• is a diverse and dynamic population:
• more than 22 nations represented in New Zealand
• each with their own unique culture, language, history, and health status
• share many similarities which we have shared with you here in order to help you work with Pasifika patients more effectively
The main Pacific nations in New Zealand are:
• Samoa, Cook Islands, Fiji, Tonga, Niue, Tokelau and Tuvalu
Acknowledging The FonoFale Model (pasifika model of health) when working with Pasifika peoples and families.
Acknowledging general pacific guidelines when working with Pasifika peoples and families:
https://thinkhauorawebsite.blob.core.windows.net/websitepublished/CCP/Resources/General%20Cancer%20docs/MC/He%20Anga%20Whakaahuru%20Interactive%20PDF%20Final.pdfhttp://apps.centralpho.org.nz/Permalink/MoM/General%20Documents/MoM/Published/Hauora%20Maori%20Forms/Te%20Whare%20Tapa%20Wha.pdfhttp://apps.centralpho.org.nz/Permalink/MoM/General%20Documents/MoM/Published/Hauora%20Maori%20Forms/Cultural%20Issues.pdfhttp://apps.centralpho.org.nz/Permalink/MoM/General%20Documents/MoM/Published/Hauora%20Maori%20Forms/Wh%C4%81naungatanga.pdfhttp://apps.centralpho.org.nz/Permalink/MoM/General%20Documents/MoM/Published/Hauora%20Maori%20Forms/Whanau%20Ora%2C%20Te%20Ara%20Whanau%20Ora%20and%20Navigators.pdfhttps://www.centralpho.org.nz/node/688http://apps.centralpho.org.nz/Permalink/MoM/General%20Documents/MoM/Published/Pacific%20Health%20Forms/Pacific%20Cultural%20Guidelines%20(Central%20PHO).pdfhttp://apps.centralpho.org.nz/Permalink/MoM/General%20Documents/MoM/Published/Pacific%20Health%20Forms/Fonofale%20model.pdf
-
PROSTATE CANCER - EARLY DETECTION April 2018 Page 5 of 15
This map was published by MidCentral District. A printed version of this document is not controlled so may not be up-to-date with the latest clinical information.
• Cultural protocols and greetings
• Building relationships with your pasifika patients
• Involving family support, involving religion, during assessments and in the hospital
• Home visits
• Contact information
Pasifika Health Service
The Pasifika Health Service is a service provided free of charge for:
•all Pasifika people living in Manawatu, Horowhenua, Tararua and Otaki who have long term conditions
• all Pasifika mothers and children aged 0-5 years
• an appointment can be made by the patient, doctor or nurse
• the Pasifika Health Service contact details are:
• Palmerston North Office - 06 354 9107
• Horowhenua Office - 06 367 6433
• more information and referral
Additional resources:
• Ala Mo'ui - Pathways to Pacific Health and Wellbeing 2014-2018
• Primary care for pacific people: a pacific health systems approach
• Tupu Ola Moui: The Pacific Health Chart Book 2004
• Pacific Health resources
• Central PHO Pasifika Health Service
7.Presenting symptoms and/or concerns
NB: Equity - Māori men are less likely to be diagnosed with prostate cancer than non-Māori men, but are 37 percent more likely to
die from the disease [1].
Presenting symptoms and/or concerns
1. Bladder outflow obstruction including:
• urinary frequency
• nocturia
• urgency
• poor flow
• terminal dribbling
• hesitancy
are most commonly due to benign prostatic hypertrophy, but may co-exist with prostate cancer.
2. Bone pain, weight loss, lower back pain, and haematuria are uncommon presentations UNLESS for more advanced /metastatic
prostate cancer.
References:
1. Prostate Cancer Management and Referral Guidance, Ministry of Health.
8. Notes for MidCentral/Whanganui Regions
Notes for MidCentral/Whanganui DHB Regions [3]
We accept the validity of the MOH guideline however, the MCH/WDHB Urologists wish to bring to your attention recent evidence
http://apps.centralpho.org.nz/Permalink/MoM/General%20Documents/MoM/Published/Pacific%20Health%20Forms/Cultural%20Protocols%20and%20Greetings.pdfhttp://apps.centralpho.org.nz/Permalink/MoM/General%20Documents/MoM/Published/Pacific%20Health%20Forms/Building%20relationships%20with%20pacific%20patients.pdfhttp://apps.centralpho.org.nz/Permalink/MoM/General%20Documents/MoM/Published/Pacific%20Health%20Forms/Family%20support_Religion_Healing_Hospital.pdfhttp://apps.centralpho.org.nz/Permalink/MoM/General%20Documents/MoM/Published/Pacific%20Health%20Forms/Home%20visits.pdfhttp://apps.centralpho.org.nz/Permalink/MoM/General%20Documents/MoM/Published/Pacific%20Health%20Forms/Contact%20info.pdfhttp://apps.centralpho.org.nz/Permalink/MoM/General%20Documents/MoM/Published/General%20Cancer%20docs/MC/Pasifika%20Health%20Final%20Pamphlet%202017%20(003)%20(2).pdfhttp://www.health.govt.nz/publication/ala-moui-pathways-pacific-health-and-wellbeing-2010-2014http://www.health.govt.nz/publication/primary-care-pacific-people-pacific-and-health-systems-approachhttp://www.health.govt.nz/publication/tupu-ola-moui-pacific-health-chart-book-2004http://www.health.govt.nz/our-work/populations/pacific-health/pacific-health-resourceshttps://www.centralpho.org.nz/node/480
-
PROSTATE CANCER - EARLY DETECTION April 2018 Page 6 of 15
This map was published by MidCentral District. A printed version of this document is not controlled so may not be up-to-date with the latest clinical information.
already incorporated into several other guidelines including:
• EAU Guideline
• Prostate Cancer Foundation of Australia
• NCCN Guideline
There is compelling evidence that men with a PSA level of > 1mcg/L at 40 years of age are at greater risk of clinically
significant or lethal prostate cancer and this cut point identifies a group who might benefit from more intensive screening.
More over, those men with PSA of less than 1 at age 40 but who wish to continue with Prostate Cancer screening can
be screened less frequently (e.g. NCCN recommends intervals of 2-4 yearly).
NB: Thresholds for referral to Urology in the at risk group would be accepted locally with PSA levels lower than the Minstry of
Health recommended level of 4 mcg/L.
Reference
[3] Baseline Prostate-Specific Antigen Testing at a Young Age - Stacy Loeb,H. Ballentine Carter,William J. Catalona,Judd W.
Moul,Fritz H. Schroder. European Urology - Elsevier 2012.
9. Level of understanding and engagement
Apply health literacy principles:
• if English is a second language, ask what the patient understands:
• build on what the patient already knows
• translate medical terminology into lay language (do they have a support person)
• draw diagrams or write key phrases and messages down and give it to the patient to take with them
• provide educational material
• check the patient’s understanding to confirm that they understand the key messages (or confirm with support person if required)
• encourage patient to bring trusted support people to future consultations
Consider other health literacy resources as appropriate:
• interpreter services – Language Line (Nationwide) 0800 656 656 Monday to Friday, 9am to 6pm, and Saturday 9am to 2pm
• local Māori Navigational Services
• local Pasifika Health Services
• LETS PLAN is a resource to help plan your next health care visit. It will help you understand more about your health and
treatment for an illness or injury
Consider barriers to effective care:
Factors that could stop the patient from getting further tests or treatment can include:
• complexity of care pathway not knowing when or where to go next
• cost
• whānau, family and social network dynamics i.e. no whānau support
• family obligations including dependents
• work responsibilities (can't take time off)
• religious beliefs
• locality and geographical access to health and hospital services (travel)
Discuss options of referral to available support services. For more information see the 'consider referral to support services' within
this pathway.
http://www.open.hqsc.govt.nz/assets/Patient-Safety-Week/PR/PLAN-flyer-Oct-2014.pdf
-
PROSTATE CANCER - EARLY DETECTION April 2018 Page 7 of 15
This map was published by MidCentral District. A printed version of this document is not controlled so may not be up-to-date with the latest clinical information.
10. Assessment, Family History, Risk Factors
Risk factors may include:
• age
• family history
• ethnicity
• obesity
• socio-economic factors i.e. health literacy and financial status
• smoking
History:
• a man is defined as having a family history of prostate cancer if he has at least one first-degree relative (father or brother) who
was diagnosed with prostate cancer [1]
• men with a family history of prostate cancer are twice as likely to develop the disease than men without a family history [1]
• if a man has two or more first-degree relatives who were diagnosed with prostate cancer under the age of 65 years, then his
risk increases by 5-11 times (Steinberg et al 1990) [1]
• a small group of men with prostate cancer (about 9 percent) will have the true hereditary form of the disease, which is defined
as three or more affected relatives or at least two relatives who have developed prostate cancer before the age of 55 years
(Steinberg et al 1990; Bratt 2002) [1]
• patients with hereditary prostate cancer usually develop the disease six to seven years earlier than other men, but have about
the same chance of developing a more aggressive form of the disease (Carter et al 1992; Grönberg et al 1996) [1]
References:
1. Prostate Cancer Management and Referral Guidance, Ministry of Health.
11. RED FLAGS!
Red Flag Symptoms:
• Acute neurological symptoms
• Renal failure
• Bone pain
• Macroscopic haematuria (without UTI)
• also see to Note 4 - Red flags of the Prostate Cancer Management and Guidance document for more information [1]
References:
1. Prostate Cancer Management and Referral Guidance, Ministry of Health.
12. Consider differential diagnosis
Lower urinary tract (LUTS) Symptoms
Obstructive:
• poor flow
• hesitancy
• terminal dribbling
Irritative (secondary):
• frequency
https://thinkhauorawebsite.blob.core.windows.net/websitepublished/CCP/Resources/General%20Cancer%20docs/Prostate/Note%204%20Prostate%20Cancer%20Management-%20Referral%20Guidance%20Sept15.pdf
-
PROSTATE CANCER - EARLY DETECTION April 2018 Page 8 of 15
This map was published by MidCentral District. A printed version of this document is not controlled so may not be up-to-date with the latest clinical information.
• nocturia
• urgency
Consider other causes of LUTS:
• UTI
• constipation
• anxiety
• diabetes
• recent radiotherapy or surgery
• medications, most commonly:
• sympathomimetics e.g. pseudoephedrine
• anticholinergics including antihistamines, tricyclic antidepressants, and phenothiazines
• some muscle relaxants e.g. orphenadrine
13. URGENT referral to ED
URGENT presentation to Emergency Department and phone Urologist. Include all relevant information:
• reason for referral
• expectation of referral
• history and co-morbidities
• current management and/or options already pursued
• examination findings
• investigation results
• current medication
• allergies and adverse drug reactions
• any other relevant clinical information
14. Examination/Testing – DRE, PSA
Examination: • a general examination is advised as well as DRE to check for clinical indicators of prostate cancer
• arrange PSA test - Reference to Note 2 - PSA Testing Guidance document [1]
• NB: Include recommended age range if patient is wanting further PSA measurements e.g. 50-69 if family history, start age 40
Consent: [1]
• some men may be reluctant to have a DRE. For Māori and Pasifika men, there may also be a cultural barrier to the procedure
• primary care practitioners should inform these men that not every prostate cancer increases PSA and there is a chance that
they will still have prostate cancer even if their PSA result is normal
• around 20 percent of prostate cancers are diagnosed from an abnormal DRE when the PSA level is normal
• if a man declines a DRE, even after he has been given the above information, it is acceptable to refer him to a urology service
based on two clearly abnormal PSA results
NB: Equity - Men who live in rural or low-decile communities may have restricted access to diagnostic or treatment services,
meaning that they may be more likely to have poorer prostate cancer outcomes than men who do not live in such communities.
Research shows a disparity in PSA testing across New Zealand, with a higher proportion of men being tested in decile 1
communities compared with decile 10 (Gray et al 2005). [1]
References:
https://thinkhauorawebsite.blob.core.windows.net/websitepublished/CCP/Resources/General%20Cancer%20docs/Prostate/PSA%20Testing%20(note%202%20of%20guidance%20document).pdf
-
PROSTATE CANCER - EARLY DETECTION April 2018 Page 9 of 15
This map was published by MidCentral District. A printed version of this document is not controlled so may not be up-to-date with the latest clinical information.
1. Prostate Cancer Management and Referral Guidance, Ministry of Health.
15. PSA, DRE declined – NO further action
If the patient declines testing, no further action is required.
16. Normal PSA and DRE
Normal PSA and DRE.
17. Abnormal PSA
Prostate specific antigen (PSA) testing: [1]
• for more information on abnormal PSA see note 2 of the guidance document
References:
1. Prostate Cancer Management and Referral Guidance, Ministry of Health.
18. Abnormal DRE
Note 3: Digital Rectal Examination (DRE) [1] Most prostate cancers are located in the peripheral zone of the prostate gland
and some can be detected on DRE (Horwich et al 2001).
Prostate cancer may present as a hard, discrete nodule or with asymmetry of the prostate gland.
An enlarged prostate gland is not a good indicator for prostate cancer if the man’s PSA result is normal, as the prostate gland
generally increases in size as men age.
A man with an abnormal DRE should be referred to a urology service. An abnormal DRE indicates the need for a prostate biopsy, as
it can be predictive of more aggressive prostate cancer (Katie et al 2007; Gosselaar et al 2008). Some men may be reluctant to
have a DRE.
References:
1. Prostate Cancer Management and Referral Guidance, Ministry of Health.
19. Check first-degree relative
Check if patient has first-degree relative who was diagnosed with prostate cancer under the age of 65 years.
20. RED FLAGS!
Send urgent referral to ED if:
• PSA is 10 µg/L AND severe back pain AND acute neurological symptoms consistent with spinal cord compression or cauda
equina compression (Note: Where available, refer to a radiation oncology service in the first instance, phone consult with on-call
radiation oncologist)
https://thinkhauorawebsite.blob.core.windows.net/websitepublished/CCP/Resources/General%20Cancer%20docs/Prostate/PSA%20Testing%20(note%202%20of%20guidance%20document).pdf
-
PROSTATE CANCER - EARLY DETECTION April 2018 Page 10 of 15
This map was published by MidCentral District. A printed version of this document is not controlled so may not be up-to-date with the latest clinical information.
Send urgent referral to urology if:
• PSA is 10 µg/L AND renal failure is present (Note: Phone consult with an on-call urologist is recommended)
• PSA is 10 µg/L AND bone pain (new onset, progressive and severe) is present (Note: Phone consult with an on-call urologist
is recommended)
• PSA is 10 µg/L AND macroscopic haematuria is present (Note: Phone consult with an on-call urologist is recommended)
• PSA is 10 µg/L AND prostate feels hard and/or irregular on DRE
21. Referral to supportive care services
He Anga Whakaahuru - Supportive Care Framework [5]
Improving the quality of life for those with cancer, their family and whānau through support, rehabilitation and palliative care - the
essential services required to meet a person’s physical, social, cultural, emotional, nutritional, informational, psychological,
spiritual and practical needs throughout their experience with cancer.
Further information on the Standards and Competencies
Support Services:
1. Community Cancer Nurses Community-based cancer support service is provided to:
• anyone with a possible, probable or definite diagnosis of cancer and are enrolled with a PHO and/or is a resident in the PHO
area
Māori Community Cancer Coordinators - community-based Māori cancer support services:
• Te Wakahuia (Palmerston North, Manawatu) Phone: 06 3573400
• Best Care Whakapai Hauora (Palmerston North)06 3536385 Ext 773
• Te Rānanga o Raukawa (Otaki, Horowhenua) Phone: 06 3688679
• Te Kete Hauora (Tararua) Phone: 06 3746860
• referral form
2. Pae Ora Māori Health Service:
• kaupapa Māori community and hospital based navigation service
• referral form and contact details
3. Cancer Society:
• for additional support services phone the cancer information nurses on the Cancer Information Helpline 0800 226 2374
4. Central Region Cancer Services Directory:
The directory provides a list of cancer support services available across MidCentral, Whanganui and Hawke's Bay including:
• ethnic and cultural
• accommodation
• disability support
• government health services
• medication
• legal advice 5. Social Workers Oncology
• We can support you and your family/whānau as you come to terms with your diagnosis and the impact it may have in your day-
to-day life, now and in the future
• for more information and contact details
6. Cancer Psychology Service (Massey): Te Ara Whatumanawa. We work with people and their whānau/family at all stages of the
cancer journey, from diagnosis to treatment and beyond.
• free service
• 06 3505180
• referral form
7. Regional Cancer Treatment Service (RCTS):
https://thinkhauorawebsite.blob.core.windows.net/websitepublished/CCP/Resources/General%20Cancer%20docs/MC/He%20Anga%20Whakaahuru%20Interactive%20PDF%20Final.pdfhttps://thinkhauorawebsite.blob.core.windows.net/websitepublished/CCP/Resources/General%20Cancer%20docs/MC/Community%20Cancer%20Support%20Nurse%20Brochure.pdfhttps://thinkhauorawebsite.blob.core.windows.net/websitepublished/CCP/Resources/General%20Cancer%20docs/MC/2016%20MAORI%20CANCER%20COORDINATOR%20Referral.pdfhttps://thinkhauorawebsite.blob.core.windows.net/websitepublished/CCP/Resources/General%20Cancer%20docs/MC/Pae%20Ora%20Maori%20Health%20Service%20Referral.pdfhttp://www.centralcancernetwork.org.nz/page/pageid/2145862571https://thinkhauorawebsite.blob.core.windows.net/websitepublished/CCP/Resources/General%20Cancer%20docs/MC/Cancer%20Social%20Workers%20Oncology.pdfhttps://thinkhauorawebsite.blob.core.windows.net/websitepublished/CCP/Resources/General%20Cancer%20docs/MC/CPS%20brochure.pdfhttps://thinkhauorawebsite.blob.core.windows.net/websitepublished/CCP/Resources/General%20Cancer%20docs/MC/CPS%20Referral%20Form%20April%2016.pdf
-
PROSTATE CANCER - EARLY DETECTION April 2018 Page 11 of 15
This map was published by MidCentral District. A printed version of this document is not controlled so may not be up-to-date with the latest clinical information.
Cancer treatment services are provided to patients in Taranaki, Whanganui, Tarawhiti, Hawkes Bay and MidCentral District Health
Boards by the Regional Cancer Treatment Service (RCTS):
• for more information go to website
Reference: He Anga Whakaahuru - Supportive Care Framework [5]
22. Treat UTI or Prostatitis if present
Treat UTI or Prostatitis if present.
23. Refer to Urology
Include relevant information:
• reason for referral
• expectation of referral
• history and co-morbidities
• current management and/or options already pursued
• examination findings
• investigation results
• current medication
• allergies and adverse drug reactions
• any other relevant clinical information
• for more information on referral criteria see note 6 of the guidance document [1]
References:
1. Prostate Cancer Management and Referral Guidance, Ministry of Health.
24. Discuss follow up options
Follow-up options after a normal PSA and DRE: [1]
• see note 5 of the guidance document for more information
References:
1. Prostate Cancer Management and Referral Guidance, Ministry of Health.
25. Repeat PSA after 6-12 weeks/review results
Repeat PSA after 6-12 weeks/review results.
26. Normal PSA
Normal PSA.
27. Abnormal PSA
http://www.midcentraldhb.govt.nz/HealthServices/RCTS/Pages/default.aspxhttps://thinkhauorawebsite.blob.core.windows.net/websitepublished/CCP/Resources/General%20Cancer%20docs/Prostate/Prostate%20Cancer%20Management-%20Referral%20Guidance%20Note%206.pdfhttps://thinkhauorawebsite.blob.core.windows.net/websitepublished/CCP/Resources/General%20Cancer%20docs/Prostate/Prostate%20Cancer%20Management-%20Referral%20Guidance%20Note%205.pdf
-
PROSTATE CANCER - EARLY DETECTION April 2018 Page 12 of 15
This map was published by MidCentral District. A printed version of this document is not controlled so may not be up-to-date with the latest clinical information.
If second PSA result is abnormal - obtain informed consent and refer to Urology.
Prostate specific antigen (PSA) testing: [1]
• for more information on abnormal PSA see note 2 of the guidance document
References:
1. Prostate Cancer Management and Referral Guidance, Ministry of Health.
28. Referral to supportive care services
He Anga Whakaahuru - Supportive Care Framework [5]
Improving the quality of life for those with cancer, their family and whānau through support, rehabilitation and palliative care - the
essential services required to meet a person’s physical, social, cultural, emotional, nutritional, informational, psychological,
spiritual and practical needs throughout their experience with cancer.
Further information on the Standards and Competencies
Support Services:
1. Community Cancer Nurses Community-based cancer support service is provided to:
• anyone with a possible, probable or definite diagnosis of cancer and are enrolled with a PHO and/or is a resident in the PHO
area
Māori Community Cancer Coordinators - community-based Māori cancer support services:
• Te Wakahuia (Palmerston North, Manawatu) Phone: 06 3573400
• Best Care Whakapai Hauora (Palmerston North)06 3536385 Ext 773
• Te Rānanga o Raukawa (Otaki, Horowhenua) Phone: 06 3688679
• Te Kete Hauora (Tararua)Phone: 06 3746860
• referral form
2. Pae Ora Māori Health Service:
• kaupapa Māori community and hospital-based navigation service
• referral form and contact details
3. Cancer Society:
• for additional support services phone the cancer information nurses on the Cancer Information Helpline 0800 226 237
4. Central Region Cancer Services Directory:
The directory provides a list of cancer support services available across MidCentral, Whanganui and Hawke's Bay including:
• ethnic and cultural
• accommodation
• disability support
• government health services
• medication
• legal advice
5. Social Workers Oncology
• We can support you and your family/whānau as you come to terms with your diagnosis and the impact it may have in your day-
to-day life, now and in the future
• for more information and contact details
6. Cancer Psychology Service (Massey): Te Ara Whatumanawa. We work with people and their whānau/family at all stages of the
cancer journey, from diagnosis to treatment and beyond.
• free service
• 06 3505180
• referral form
https://thinkhauorawebsite.blob.core.windows.net/websitepublished/CCP/Resources/General%20Cancer%20docs/Prostate/PSA%20Testing%20(note%202%20of%20guidance%20document).pdfhttps://thinkhauorawebsite.blob.core.windows.net/websitepublished/CCP/Resources/General%20Cancer%20docs/MC/He%20Anga%20Whakaahuru%20Interactive%20PDF%20Final.pdfhttps://thinkhauorawebsite.blob.core.windows.net/websitepublished/CCP/Resources/General%20Cancer%20docs/MC/Community%20Cancer%20Support%20Nurse%20Brochure.pdfhttps://thinkhauorawebsite.blob.core.windows.net/websitepublished/CCP/Resources/General%20Cancer%20docs/MC/2016%20MAORI%20CANCER%20COORDINATOR%20Referral.pdfhttps://thinkhauorawebsite.blob.core.windows.net/websitepublished/CCP/Resources/General%20Cancer%20docs/MC/Pae%20Ora%20Maori%20Health%20Service%20Referral.pdfhttp://www.centralcancernetwork.org.nz/page/pageid/2145862571https://thinkhauorawebsite.blob.core.windows.net/websitepublished/CCP/Resources/General%20Cancer%20docs/MC/Cancer%20Social%20Workers%20Oncology.pdfhttps://thinkhauorawebsite.blob.core.windows.net/websitepublished/CCP/Resources/General%20Cancer%20docs/MC/CPS%20brochure.pdfhttps://thinkhauorawebsite.blob.core.windows.net/websitepublished/CCP/Resources/General%20Cancer%20docs/MC/CPS%20Referral%20Form%20April%2016.pdf
-
PROSTATE CANCER - EARLY DETECTION April 2018 Page 13 of 15
This map was published by MidCentral District. A printed version of this document is not controlled so may not be up-to-date with the latest clinical information.
7. Regional Cancer Treatment Service (RCTS):
Cancer treatment services are provided to patients in Taranaki, Whanganui, Tarawhiti, Hawkes Bay and MidCentral District Health
Boards by the Regional Cancer Treatment Service (RCTS):
• for more information go to website
29. Check first-degree relative
Check if man has first-degree relative who was diagnosed with prostate cancer under the age of 65 years.
30. Refer to Urology
Include relevant information:
• reason for referral
• expectation of referral
• history and co-morbidities
• current management and/or options already pursued
• examination findings
• investigation results
• current medication
• allergies and adverse drug reactions
• any other relevant clinical information
• for more information on referral criteria see note 6 of the guidance document[1]
References:
1. Prostate Cancer Management and Referral Guidance, Ministry of Health.
31. Discuss follow up options
Follow-up options after a normal PSA [1]
• see note 5 of the guidance document for more information
References:
1. Prostate Cancer Management and Referral Guidance, Ministry of Health.
http://www.midcentraldhb.govt.nz/HealthServices/RCTS/Pages/default.aspxhttps://thinkhauorawebsite.blob.core.windows.net/websitepublished/CCP/Resources/General%20Cancer%20docs/Prostate/Prostate%20Cancer%20Management-%20Referral%20Guidance%20Note%206.pdfhttps://thinkhauorawebsite.blob.core.windows.net/websitepublished/CCP/Resources/General%20Cancer%20docs/Prostate/Prostate%20Cancer%20Management-%20Referral%20Guidance%20Note%205.pdf
-
PROSTATE CANCER - EARLY DETECTION April 2018 Page 14 of 15
This map was published by MidCentral District. A printed version of this document is not controlled so may not be up-to-date with the latest clinical information.
Prostate Cancer – Early Detection
Provenance Certificate
Overview
Overview | Editorial methodology | References | Contributors | Disclaimers
This document describes the provenance of the Sub-region Districts (MidCentral, Whanganui and Hawke’s Bay District Health Boards) Prostate Cancer Pathway.
The purpose of implementing cancer pathways in our Districts is to:
• Reduce barriers so that all people with cancer are able to access the same quality care within the same timeframes, irrespective of their ethnicity, gender, locality or socio-economic status
• Achieve the faster cancer treatment (FCT) health target – 85% of patient receive their first cancer treatment (or other management) within 62 days of being referred with a high suspicion of cancer and a need to be seen within two weeks by July 2016, increasing to 90% by June 2017
• Implement the national tumour standards of service provision, developed as part of the FCT programme, to support the delivery of standardised quality care for all people with cancer
o NB: There are currently no Tumour Standards for Prostate Cancer
• Improve equity along the cancer pathway
• Clarify expectations across providers
• Improve communications and follow up care for cancer patients
To cite this pathway, use the following format:
Map of Medicine/Central Region View/Oncology/Prostate Cancer Suspected
Editorial methodology This care map was based on high-quality information and known Best Practice guidelines from New Zealand and around the world including Map of medicine editorial methodology. It has been checked by individuals with front-line clinical experience (see Contributors section of this document).
Map of Medicine pathways are constantly updated in response to new evidence. Continuous evidence searching means that pathways can be updated rapidly in response to any change in the information landscape. Indexed and grey literature is monitored for new evidence, and feedback is collected from users year-round. The information is triaged so that important changes to the information landscape are incorporated into the pathways through the quarterly publication cycle.
References
This care map has been developed according to the Map of Medicine editorial methodology. The content of this care map is based on high-quality guidelines and practice-based knowledge provided by contributors with front-line clinical experience. This sub-region version of the evidence-based, practice- informed care map has been peer-reviewed by stakeholder groups and the CCP Programme Clinical Lead.
-
PROSTATE CANCER - EARLY DETECTION April 2018 Page 15 of 15
This map was published by MidCentral District. A printed version of this document is not controlled so may not be up-to-date with the latest clinical information.
1. Prostate Cancer Management and Referral Guidance, Ministry of Health.
2. Prostate Cancer Awareness and Quality Improvement Programme, Ministry of Health.
3. Faster Cancer Treatment Programme, Ministry of Health.
4. Prostate Cancer Foundation NZ.
Contributors
MidCentral DHB’s Collaborative Clinical Pathway editors and facilitators worked with clinical stakeholders such as front-line clinicians and pharmacists to gather practice-based knowledge for its care maps.
The following individuals have contributed to this care map:
• David Mason, Urologist, Hawke’s Bay DHB (Secondary Care Clinical Lead)
• Lorraine Cox, Clinical Nurse Specialist Urology, Whanganui DHB
• Catherine Parata, Nurse Practitioner Candidate, Horowhenua Community Practice
• Lucy Keedle, Community Cancer Nurse, Central Primary Health Organisation/Clinical Nurse Specialist, Women’s Health, MidCentral DHB
• John McMenamin, General Practitioner, Wicksteed Medical Centre, Whanganui (Primary Care Clinical Lead)
• Trish White, Nurse Practitioner, Urology, Hawke’s Bay DHB
• Ray Jackson, Project Director, Collaborative Clinical Pathways (Facilitator)
• Eve Williams, Project Assistant, Collaborative Clinical Pathways (Editor)
The following individuals have contributed to this localised MidCentral Region care map:
• Lucy Keedle, Community Cancer Nurse, Central Primary Health Organisation/Clinical Nurse Specialist, Women’s Health, MidCentral DHB (Primary Care Clinical Lead)
• Quinten King, Urologist, MidCentral DHB (Secondary Care Clinical Lead)
• Ray Jackson, Project Director, Collaborative Clinical Pathways (Facilitator/Editor)
Disclaimers
Clinical Board Central PHO, MidCentral DHB It is not the function of the Clinical Board Central PHO, MidCentral DHB to substitute for the role of the clinician, but to support the clinician in enabling access to know-how and knowledge. Users of the Map of Medicine are therefore urged to use their own professional judgement to ensure that the patient receives the best possible care. Whilst reasonable efforts have been made to ensure the accuracy of the information on this online clinical knowledge resource, we cannot guarantee its correctness and completeness. The information on the Map of Medicine is subject to change and we cannot guarantee that it is up-to-date.