Prospective Multicenter Study Preliminary Report P. Witkowski- Coordination Center Dept of Surgery,...
19
Prospective Multicenter Study Prospective Multicenter Study Preliminary Report Preliminary Report P. Witkowski- P. Witkowski- Coordination Center Coordination Center Dept of Surgery, Columbia University, USA Dept of Surgery, Columbia University, USA F. Abbonante F. Abbonante - Dept of Surgery, Catanzaro Hospital, Italy - Dept of Surgery, Catanzaro Hospital, Italy Z. Sledzinski, W. Adamonis, M. Smietanski Z. Sledzinski, W. Adamonis, M. Smietanski - Dept of Surgery, - Dept of Surgery, Medical Univ. of Gdansk, Poland Medical Univ. of Gdansk, Poland I. Fedorov, L. Slavin, D. Slavin I. Fedorov, L. Slavin, D. Slavin - Dept of Surgery, Medical - Dept of Surgery, Medical University of Kazan, Russia University of Kazan, Russia Tension- Free Sutureless Tension- Free Sutureless Sublay Sublay Ventral Hernia Repair Ventral Hernia Repair
-
Upload
nora-holland -
Category
Documents
-
view
223 -
download
3
Transcript of Prospective Multicenter Study Preliminary Report P. Witkowski- Coordination Center Dept of Surgery,...

Prospective Multicenter Study Prospective Multicenter Study Preliminary ReportPreliminary Report
P. Witkowski-P. Witkowski- Coordination Center Coordination CenterDept of Surgery, Columbia University, USADept of Surgery, Columbia University, USA
F. AbbonanteF. Abbonante- Dept of Surgery, Catanzaro Hospital, Italy- Dept of Surgery, Catanzaro Hospital, ItalyZ. Sledzinski, W. Adamonis, M. SmietanskiZ. Sledzinski, W. Adamonis, M. Smietanski- Dept of Surgery, Medical - Dept of Surgery, Medical Univ. of Gdansk, PolandUniv. of Gdansk, PolandI. Fedorov, L. Slavin, D. SlavinI. Fedorov, L. Slavin, D. Slavin- Dept of Surgery, Medical University of - Dept of Surgery, Medical University of Kazan, RussiaKazan, Russia
Tension- Free Sutureless Sublay Tension- Free Sutureless Sublay Ventral Hernia RepairVentral Hernia Repair

1. 1. In ventral hernioplasty sutures preventIn ventral hernioplasty sutures prevent mesh migration mesh migration mesh wrinkling and curlingmesh wrinkling and curling
2. 2. HoweverHowever suturing is:suturing is: time consumingtime consuming often challenging often challenging could create tension in the mesh resulting in could create tension in the mesh resulting in
o postoperative painpostoperative paino complications (1,2) complications (1,2)
BackroundBackround

1.1. There is no need for the mesh suturing in There is no need for the mesh suturing in ventral hernia repair if the mesh is rigid, ventral hernia repair if the mesh is rigid, macroporous, made of monofilament macroporous, made of monofilament polypropylene, and has flat-shape memory. polypropylene, and has flat-shape memory.
2. This mesh will not migrate, wrinkle, or curl 2. This mesh will not migrate, wrinkle, or curl when placed in a closed space even without when placed in a closed space even without suturing to the surrounding tissue (3). suturing to the surrounding tissue (3).
3. This prosthesis prevents hernia recurrence 3. This prosthesis prevents hernia recurrence while laying flat without tension. It is held in while laying flat without tension. It is held in place by intra-abdominal pressure and place by intra-abdominal pressure and connective tissue ingrowth. connective tissue ingrowth.
HypothesisHypothesis

Clinical evaluation of the new Tension- Clinical evaluation of the new Tension-
Free Trabucco Ventral Hernia Repair Free Trabucco Ventral Hernia Repair
technique, which involves the use of rigid technique, which involves the use of rigid
mesh without sutures.mesh without sutures.
AimAim

Prospective Multicenter StudyProspective Multicenter Study
Coordination Center- Columbia University, USACoordination Center- Columbia University, USA
Participating Centers:Participating Centers: Catanzaro Hospital, ItalyCatanzaro Hospital, Italy
Medical University of GdanskMedical University of Gdansk, Poland, Poland
Medical University of Medical University of Kazan, RussiaKazan, Russia
Medical treatmentMedical treatment Preferred- general anesthesiaPreferred- general anesthesia
Antibiotics prophylaxisAntibiotics prophylaxis
Thromboembolic disease prophylaxisThromboembolic disease prophylaxis
The same surgical techniqueThe same surgical technique
Early physical mobilizationEarly physical mobilization

MaterialMaterialVentral herniaVentral hernia with defect > 5cmwith defect > 5cm
ItalyItaly PolandPoland RussiaRussia TotalTotal
Number of Number of patientspatients
232317F, 6M17F, 6M
773F, 4M3F, 4M
775F, 2M5F, 2M
373725F, 12M25F, 12M
BMIBMI 31.6± 4.331.6± 4.3 33.3 ± 6.233.3 ± 6.2 35.6 ± 7.535.6 ± 7.5 32.6 ± 5.932.6 ± 5.9
Age (years)Age (years) 64.2 ± 1464.2 ± 14 67.5 ± 1167.5 ± 11 57.8 ± 757.8 ± 7 63 63 ± 12± 12
Incisional Incisional herniahernia
16 16 (70%)(70%) 6 6 (85%)(85%) 4 4 (57%)(57%) 26 26 (70%)(70%)
Primary Primary defect*defect*
7 7 (30%)(30%) 1 1 (15%)(15%) 3 3 (42%)(42%) 11 11 (30%)(30%)
*umbilical or epigastric hernia*umbilical or epigastric hernia
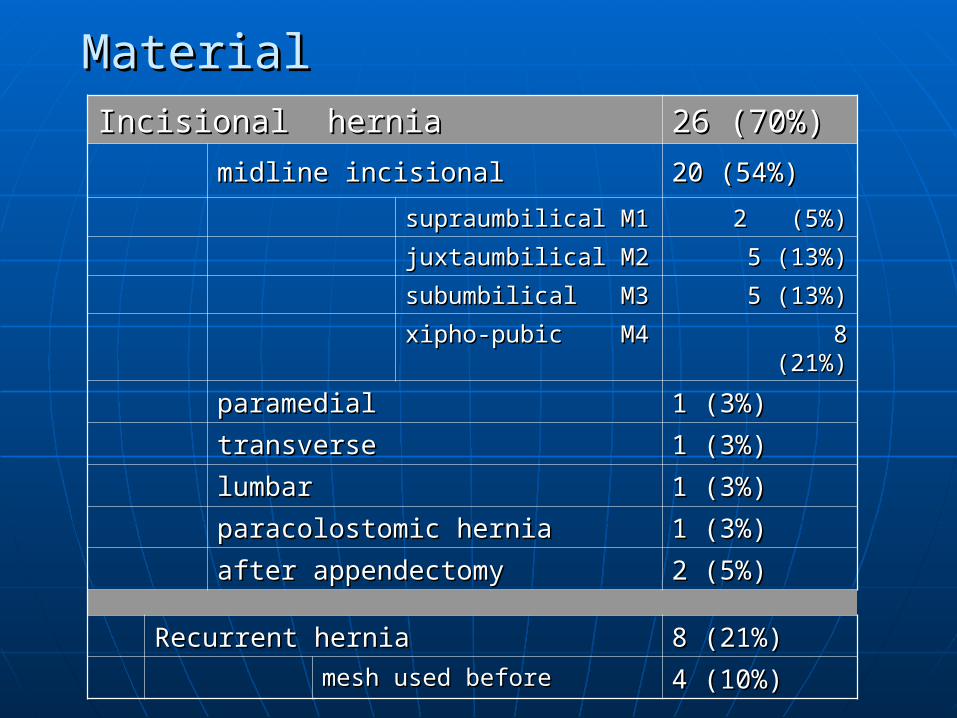
MaterialMaterialIncisional hernia Incisional hernia 26 (70%)26 (70%)
midline incisionalmidline incisional 20 (54%)20 (54%)
supraumbilical M1supraumbilical M1 2 (5%)2 (5%)
juxtaumbilical juxtaumbilical M2M2 5 (13%)5 (13%)
subumbilical M3subumbilical M3 5 (13%)5 (13%)
xipho-pubic M4xipho-pubic M4 8 (21%)8 (21%)
paramedialparamedial 1 (3%)1 (3%)
transversetransverse 1 (3%)1 (3%)
lumbarlumbar 1 (3%)1 (3%)
paracolostomic herniaparacolostomic hernia 1 (3%)1 (3%)
after appendectomyafter appendectomy 2 (5%)2 (5%)
Recurrent herniaRecurrent hernia 8 (21%)8 (21%)
mesh used beforemesh used before 4 (10%)4 (10%)
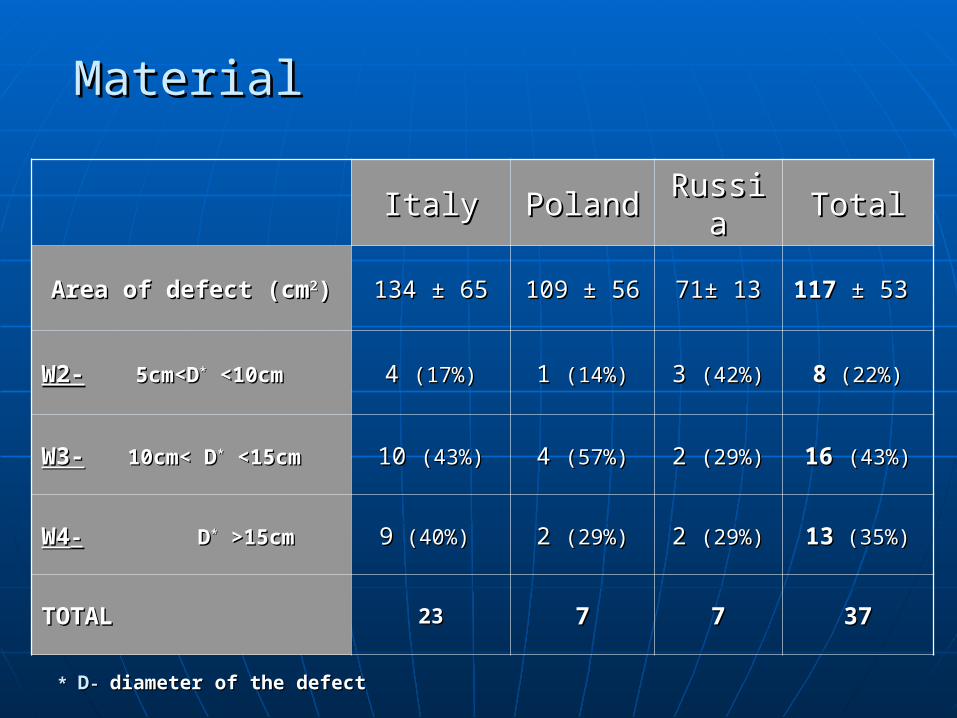
MaterialMaterial
ItalyItaly PolandPoland RussiaRussia TotalTotal
Area of defect (cmArea of defect (cm22)) 134 ± 65134 ± 65 109 ± 56109 ± 56 71± 1371± 13 117 117 ± 53± 53
W2-W2- 5cm<D 5cm<D** <10cm <10cm 4 4 (17%)(17%) 1 1 (14%)(14%) 3 3 (42%)(42%) 88 (22%) (22%)
W3-W3- 10cm< D10cm< D** <15cm <15cm 10 10 (43%)(43%) 4 4 (57%)(57%) 2 2 (29%)(29%) 1616 (43%)(43%)
W4W4-- D D** >15cm >15cm 99 (40%)(40%) 2 2 (29%)(29%) 2 2 (29%)(29%) 1313 (35%) (35%)
TOTALTOTAL 2323 77 77 3737
* * DD- - diameter of the defectdiameter of the defect

MethodsMethods
ItalyItaly PolandPoland RussiaRussia
Antibiotics Antibiotics prophylacticsprophylactics
Ceftriaxone Ceftriaxone 2.0 g iv 2.0 g iv
Kefzol & Kefzol & MetronidazolMetronidazol Cefazolin 1.0Cefazolin 1.0
Thromboembolic Thromboembolic prophylacticsprophylactics
Fraxiparine Fraxiparine or Clexaneor Clexane
Fraxiparine or Fraxiparine or ClexaneClexane
Elastic Elastic compressioncompression
Type of Type of anesthesiaanesthesia generalgeneral generalgeneral general or general or
spinalspinal
Type of suture Type of suture for posterior for posterior fasciafascia
PDS 1PDS 1 Prolene 0Prolene 0 Vicryl 3-0/ Vicryl 3-0/ Prolene 2-0Prolene 2-0
Type of suture Type of suture for anterior for anterior fasciafascia
PDS 1PDS 1 Prolene 0Prolene 0 Prolene 2-0Prolene 2-0
Surgical techniqueSurgical technique
1. Excision of the hernia sac1. Excision of the hernia sac
2. Closure of the peritoneum and posterior fascia 2. Closure of the peritoneum and posterior fascia with running suture with running suture
3. Placement of rigid mesh in retromuscular position or in 3. Placement of rigid mesh in retromuscular position or in preperitoneal space without suturepreperitoneal space without suture
4. Closure of anterior fascia with running suture4. Closure of anterior fascia with running suture
5. Relaxing incisions of anterior fascia, if necessary5. Relaxing incisions of anterior fascia, if necessary
6. Redon drainage6. Redon drainage

Surgical techniqueSurgical technique
22. Closure of the peritoneum and posterior . Closure of the peritoneum and posterior
fascia with running suturefascia with running suture

Surgical techniqueSurgical techniqueo Mesh must have proper rigidity and flat shape memoryMesh must have proper rigidity and flat shape memory
o Mesh should be macroporous, made of polypropylen and Mesh should be macroporous, made of polypropylen and
significantly larger than defectsignificantly larger than defect
o Test for rigidity- mesh hold in upright position should not bandTest for rigidity- mesh hold in upright position should not band
o Mesh used in the study- Mesh used in the study- Oval Patch (14x 18cm) or Hertra Oval Patch (14x 18cm) or Hertra
O (20x20cm or 30x30cm) (Herniamesh, Italy)O (20x20cm or 30x30cm) (Herniamesh, Italy)

33. . PPlacement of the rigid mesh in preperitoneal lacement of the rigid mesh in preperitoneal
space or retromuscular position without suturingspace or retromuscular position without suturing
Surgical techniqueSurgical technique

Surgical techniqueSurgical technique
4.4. Closure of anterior fascia with running suture Closure of anterior fascia with running suture
5.5. Relaxing incisions, if necessary to reduce tension Relaxing incisions, if necessary to reduce tension

ResultsResults
ItalyItaly PolandPoland RussiaRussia TotalTotal
Area of defect Area of defect (cm(cm22)) 134 ± 65134 ± 65 109 ± 56109 ± 56 71± 1371± 13 117 117 ± 53± 53
Time of Time of operation (min)operation (min) 115 ± 16 115 ± 16 116 ± 54116 ± 54 71 ± 3271 ± 32 106 106 ± 32± 32
Time of mesh Time of mesh implantation*implantation* 23 ± 8 23 ± 8 33 ± 1733 ± 17 21 ± 1521 ± 15 25 25 ± 12± 12
Retromuscular Retromuscular mesh (n) mesh (n) 1717 (74%)(74%) 5 5 (70%)(70%) 4 4 (57%)(57%) 2626 (70%) (70%)
Preperitoneal Preperitoneal mesh (n)mesh (n) 6 6 (26%)(26%) 2 2 (30%)(30%) 3 3 (43%)(43%) 1111 (30%) (30%)
Redon applied Redon applied (n)(n) 23 23 (100%)(100%) 7 7 (100%)(100%) 5 5 (71%)(71%) 3535 (95%) (95%)
* Time of posterior fascia suturing, mesh placement and anterior * Time of posterior fascia suturing, mesh placement and anterior fascia closure. fascia closure.

ResultsResults
ItalyItaly PolandPoland RussiaRussia TotalTotal
*VA S*VA S1 1
median (min- max)median (min- max) 3 (1-8)3 (1-8) 5 (3-6)5 (3-6) 5 (2-6)5 (2-6) 4 (1-8)4 (1-8)
TreatmentTreatment NSAIDNSAID NSAIDNSAID NSAIDNSAID NSAIDNSAID
Duration of Duration of treatment treatment (days)(days)
3 (2- 5)3 (2- 5) 4 (2-6)4 (2-6) 5 (1-6)5 (1-6) 3 (2-6)3 (2-6)
Duration of painDuration of pain(days)(days)
3 (1-5)3 (1-5) 4 (2-6)4 (2-6) 4 (1-5)4 (1-5) 3 (1-6)3 (1-6)
Hospitalization Hospitalization (days)(days)
4 (3-6)4 (3-6) 7 (3-12)7 (3-12) 7 (3-15)7 (3-15) 5 (3- 15)5 (3- 15)
* Pain assessed in Visual Analogue Scale (0-10) on the first day * Pain assessed in Visual Analogue Scale (0-10) on the first day after surgeryafter surgery

ResultsResults
ItalyItaly PolandPoland RussiaRussia TotalTotalEarly complicationsEarly complications
Wound Wound hematoma hematoma 00 00 1 1 (15%)(15%) 1 1 (3%)(3%)
Seroma & Seroma & aspirationaspiration 00 1 1 (15%)(15%) 00 1 1 (3%)(3%)
Wound Wound revisionrevision 00 1 1 (15%)(15%) 1 1 (15%)(15%) 2 2 (6%)(6%)
Follow up- 2 weeks after surgeryFollow up- 2 weeks after surgery
*VAS *VAS 1 (0-3)1 (0-3) 1 (0-4)1 (0-4) 1 (0-3)1 (0-3) 1 (0-4)1 (0-4)
Return to Return to normal home normal home
activity activity 1 weeks1 weeks 1 week1 week 1 week1 week 1 week1 week
* Pain assessed according to Visual Analogue Scale (0-10)* Pain assessed according to Visual Analogue Scale (0-10)
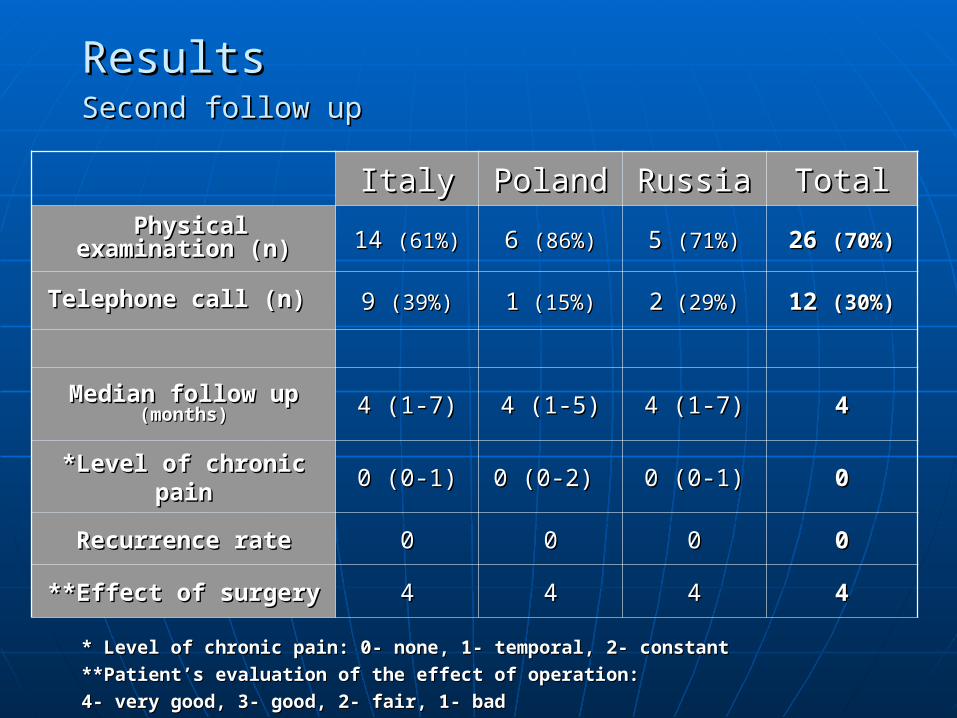
ResultsResultsSecond follow upSecond follow up
ItalyItaly PolandPoland RussiaRussia TotalTotal Physical Physical
examination (n)examination (n) 14 14 (61%)(61%) 6 6 (86%)(86%) 5 5 (71%)(71%) 26 26 (70%)(70%)
Telephone call (n) Telephone call (n) 9 9 (39%)(39%) 11 (15%) (15%) 22 (29%) (29%) 12 12 (30%)(30%)
Median follow up Median follow up (months)(months) 4 (1-7)4 (1-7) 4 (1-5)4 (1-5) 4 (1-7)4 (1-7) 44
*Level of chronic *Level of chronic painpain 0 (0-1)0 (0-1) 0 (0-2) 0 (0-2) 0 (0-1)0 (0-1) 00
Recurrence rateRecurrence rate 00 00 00 00
**Effect of surgery **Effect of surgery 44 44 44 44
* Level of chronic pain: 0- none, 1- temporal, 2- constant* Level of chronic pain: 0- none, 1- temporal, 2- constant
**Patient’s evaluation of the effect of operation: **Patient’s evaluation of the effect of operation:
4- very good, 3- good, 2- fair, 1- bad4- very good, 3- good, 2- fair, 1- bad
ConclusionsConclusions
1. Preliminary results of the study showed that 1. Preliminary results of the study showed that implantation of rigid mesh with flat shape implantation of rigid mesh with flat shape memory using the Sutureless Sublay Techniquememory using the Sutureless Sublay Technique is safe and effective in the treatment of ventral is safe and effective in the treatment of ventral abdominal hernias.abdominal hernias.
2. This technique allows surgeons to save work 2. This technique allows surgeons to save work and time of the operation and patients are able and time of the operation and patients are able to fast recover with low level of postoperative to fast recover with low level of postoperative pain after procedure. pain after procedure.