Prone Positioning Under Anesthesia
32
Prone Positioning Under Anesthesia Aarti Vadhavkar, M.D. CA-2 February 15, 2008
Transcript of Prone Positioning Under Anesthesia

Prone Positioning Under Anesthesia
Aarti Vadhavkar, M.D.CA-2
February 15, 2008

Overview
• Importance of Positioning
• Physiologic Effects
• Support Devices
• Establishing Prone Position
• Complications
2

Positioning Under Anesthesia
• Optimal position: offers maximum anatomical access; yet is physiologically safe for the anesthetized patient.
• Peripheral nerve injury: 2nd most common anesthetic complication represented in the ASA Closed Claims Database1.
• First article in literature on effects of body position on anesthesia published by Dutton2 in1933.
• General anesthesia abolishes normal protective reflexes → significant physiologic and functional hazards for the prone patient.
3
1 Cheney FW et al. Nerve Injury Associated with Anesthesia: A Closed Claims Analysis. Anesthesiology 90: 1062-1069, 19992 Dutton A. The Effects of Posture During Anesthesia. Anesthesia Analgesia 1933; 12:66-74

Physiologic Effects
• Circulatory• ↑ intraabdominal & intrathoracic pressure→ ↓cardiac
output, ↓BP• IVC obstruction → vertebral venous plexus
engorgement → ↑ bleeding, ↑ risk of thrombosis • Head low position: venous congestion of face and neck
→ facial, conjunctival and airway edema• Head high position: risk of venous air embolism
4

Physiologic Effects
5
• Several studies3,4,5 to assess hemodynamic response to prone position• ↓Stroke volume, ↓ Cardiac index
• ↑SVR, ↑PVR
• HR, PAOP, Right atrial pressure: no change
• Recommend invasive hemodynamic monitors in patients with precarious cardiovascular status
3 Backofen JE, Schauble JF. Hemodynamic changes with prone positioning during general anesthesia. Anesthesia Analgesia 1995; 64: 1944 Wadsworth R. et al. The effect of four different surgical prone positions on cardiovascular parameters in healthy volunteers. Anaesthesia. 1996 Sep;51(9):819-225 Sudheer PS et al.. Haemodynamic effects of the prone position: a comparison of propofol total intravenous and inhalation anesthesia. Anaesthesia, 2006 Feb;61(2): 138–141

Physiologic Effects
6
• Respiratory • Cephalad shift of diaphragm, compression abdominal
viscera → ↓ FRC, ↑work of breathing, ↑airway pressures• Ventral supports: improved lung volumes, oxygenation,
and compliance, esp in obese patients6
• Ventilation and perfusion are more uniform in prone position → ↓ V/Q mismatch → Improved oxygenation7
6 Pelosi P. et al: Prone positioning improves pulmonary function in obese patients during general anesthesia. Anesthesia Analgesia 83:578-583, 19967 Nyren S. et al. Pulmonary perfusion is more uniform in the prone than in the supine position: scintigraphy in healthy humans. Journal of Applied Physiology. 1999;86:1135-41.

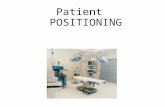
Support Devices – Head & Neck
7
• Surgical pillow/ foam donut, C-shaped face piece, horseshoe head rest, Prone Positioner, Prone View Helmet.
C-Shaped Face Piece
Horseshoe Head Rest Mayfield Tongs
• Mayfield tongs: most stable; recommended in cervical disc disease
Prone Positioner

Support Devices - Ventral
8
• Rolls of tightly packed sheets, bean bags, convex frames (e.g. Wilson frame), pedestal frames (e.g. Relton), special OR tables (e.g. Jackson)
8 Dharmavaram S. et al. Effect of prone positioning systems on hemodynamic and cardiac function during lumbar spine surgery: an echocardiographic study. Spine. 2006 May 20;31(12):1388-93
• Jackson spine table: minimal effects on cardiac function
• Study8 of 51 spine surgery patients to compare different prone positioners.

Support Devices
• Limited comparative studies: skewed,
inconclusive
• Choice based on patient’s physique, available
equipment, requirements of surgical procedure
9

Establishing Prone Position
• Adequate anesthetic depth and muscle relaxation• Monitoring leads, IV lines, catheters: secure and
sufficiently long to sustain position change• Anesthesiologist manages head and airway• ETT disconnected briefly; reconnected after turn• Acceptable ventilation assured, all monitors
rechecked and secured
10

Establishing Prone Position
• Head• Check for migrated monitoring wires, IV lines
underneath• Eyes
• Padded, taped shut• Lubricants: controversial
• Ears• Check for compression, folding of pinna
11

Establishing Prone Position
12
• Neck• Assess ROM of C-spine
& shoulders in pre-op visit
• Rule out cervical spine arthritis, thoracic outlet syndrome, cerebrovascular disease .

Establishing Prone Position
13
• Arms• Padded armboards• Arms abducted, flexed at
elbows• <90⁰ arm abduction
• relieves tension on shoulder muscles
• ↓compression of axillary neurovascular bundle by humeral head
• Protective padding: Ulnar nerve at cubital tunnel, radial nerve in spiral groove of humerus
• Check for full pulses at wrists

Establishing Prone Position
14
• Torso• Ventral longitudinal supports to relieve chest and
abdominal wall compression
• Breasts• Positioned medially and checked for compression
• Genitalia• Pillow placed over caudal end of longitudinal supports
• Knees, Toes• Flexed and padded, esp in prone kneeling position• Pillow to support ankles off table surface

Establishing Prone Position
159 Martin JT and Warner MA (eds). Positioning in Anesthesia and Surgery (3 rd edition) . WB Saunders, PA 1997.

Complications
16
• Peripheral neuropathies • Nerve entrapment
syndromes e.g. carpal tunnel
• Diabetes mellitus• Osteoarthritis,
Rheumatoid arthritis • Pre-existing decubiti• Venous stasis• Previous traumatic injury,
fractures
Risk Factors• Advanced age• Alcohol abuse• Malnutrition• Vitamin deficiencies• Corticosteroid use• Contractures• Morbid obesity• Hypothyroidism• Renal disease

Complications
17
• Airway• Accidental extubation• Obstruction of ETT
bloody secretions/ sputum plugs
• Facial, Airway edema• Prolonged head low
position, ↑ crystalloid infusion
• Problems with extubation

Complications
18
• Accentuation of pre-existing trauma
• Multiple skeletal injuries may be further exacerbated
during positioning
• Neck injury
• Excessive lateral torsion or hyperflexion → Post-op
pain, cervical nerve root or vascular compression

Case Report
• 40/M w/h/o C-spine whiplash injury s/p C4-5-6 discectomy underwent excision of soft tissue mass in prone position ↓GA 10
• C-spine stabilization, awake fiber optic intubation, horseshoe head rest
• PACU: c/o dizziness, headache, painful numbness of right face, slurred speech and myoclonic spasms of left side extremities
• MRA: Rt vertebral artery stenosis → lateral medullary syndrome
• Causes: excessive rotation or extension of head during positioning, hypoperfusion under GA → exacerbated vertebral arterial insufficiency.
19
10 Chu YC et al. Lateral Medullary Syndrome after Prone Position for General Surgery. Anesthesia Analgesia. 2002 Nov;95(5):1451-3

Injuries: Skin & Soft Tissue
20
• Key factors: amount and duration of pressure
• High risk areas: face, breasts, genitalia & bony
prominences e.g. malar regions, chin, iliac crests, knees,
toes
• Uncontrollable factors e.g. duration of surgery may
override protective measures → pressure injury

Case Report
• 44/M ASA–I underwent revision of right lower extremity scar in prone position ↓GA11 . H/o multiple LE surgeries in prone position. No known allergies.
• PronePositioner used, uneventful operative course• POD#1: Red rash over face , took Benadryl. • POD#2: To ER with c/o facial, lip and orbital swelling and
itching. Treated with prednisone and Benadryl• Allergy/Immunology Consult: Allergic contact dermatitis
from sensitization to urethane foam in PronePositioner during his previous surgeries.
21
11 Jericho BG and Skaria GP. Contact Dermatitis After the Use of the PronePositioner Anesthesia Analgesia 2003,97(6):1706-8

Injuries: Eye
22
• Corneal abrasions• Orbital edema• Postoperative visual loss ( POVL)
• Rare; unclear etiology• ASA Closed Claims Project 12 : management of
anesthesiologists frequently implicated• ASA Professional Liability Committee created the
POVL Registry 13 in 1999
12 ASA Closed Claims Project http://www.asaclosedclaims.org/13 American Society of Anesthesiologists Task Force on Perioperative Blindness: Practice advisory for perioperative visual loss associated with spine surgery: a report by the American Society

POVL Registry
23
SPINE 72%
MISC. 10%ORTHO. 4%
VASCULAR 5%
CARDIAC 9%
Distribution of cases from the ASA POVL Registry
• Goal: Identify risk factors associated with POVL• Retrospective analysis of patients who reported visual loss
< 7 days postop
PION 60%AION 20%
Unknow
n
9%
CR
AO
11%
Distribution of 93 ophthalmic lesions associated with POVL after spine surgery

POVL
24
Ischemic Optic Neuropathy (ION)
Central Retinal Artery Occlusion (CRAO)
Etiology Intraop ↓ BPProlonged surgery↑ Blood loss↑ Crystalloid infusion
Direct external pressureEmboli
Mechanism IschemiaOrbital edema → stretch and compression of ON
↓Ocular perfusion pressure
Clinical Features
PainlessBilateral↓Light perception↓ Visual fields
PainlessUnilateralPeriorbital swelling or ecchymosis

Injuries: Nerves
• Mechanisms• ↑ stretch, compression → ischemia• Occur despite adequate protection1,12 → other factors?
• Prone patient• Supraorbital, facial, mandibular nerves• Brachial plexus and its peripheral components
25
1 Cheney FW et al. Nerve Injury Associated with Anesthesia: A Closed Claims Analysis. Anesthesiology 1999. 90: 1062-1069.12 ASA Closed Claims Project http://www.asaclosedclaims.org/

Injuries: Brachial Plexus
269 Martin JT and Warner MA (eds). Positioning in Anesthesia and Surgery (3 rd edition) . WB Saunders, PA 1997.

Complications
• Other
• Compartment syndrome, Rhabdomyolysis
• Venous air embolism
• Visceral ischemia: pancreatitis
• Undiagnosed space occupying lesions
27

Case Report
• 60/F underwent decompression laminectomy T11-L1 for invasive tumor ↓GA in prone position14
• Prolonged surgery, ↑ blood loss• 9 hrs: ↓BP → pulseless V tachycardia: VAE ?• Field flooded with NS, ventilated with 100% O2
• Open surgical wound, bleeding, protruding surgical metalwork
• Defibrillator paddles placed in right axilla and left apex → 200J DC shock → Sinus rhythm
28
14 Brown J. et al. Cardiac arrest during surgery and ventilation in the prone position: a case report and systematic review. Resuscitation 2001. 50(2) : 233-238
How does one manage cardiac arrest in a prone patient?

Core Competencies• Patient Care: provided medical care to patient discussed• Medical Knowledge: reviewed current literature regarding
physiologic effects, support devices, complications and management of prone positioning under anesthesia
• Practice-based learning and improvement: assimilated scientific evidence pertinent to this case; provided reflective practice for future improvement in patient care
• Interpersonal and Communication skills: discussed the complication with the patient and neurosurgical team
• Professionalism: showed respect and accountability to the patient and provided follow-up care to the patient
• Systems-based practice: coordinated care between Neurosurgical, Anesthesia and Dermatology services.
29

Reflective Practice
• In addition to risks inherent with general
anesthesia, it might have been prudent to discuss
complications associated with positioning in
informed consent
• Earlier detection could have resulted in faster
healing of lesions.
30

References1. Cheney FW, Domino KB, Caplan RA, Posner KL Nerve Injury Associated with Anesthesia: A Closed Claims
Analysis. Anesthesiology 1999. 90: 1062-1069.
2. Dutton Adena The Effects of Posture During Anesthesia. Anesthesia Analgesia 1933. 12:66-74
3. Backofen JE, Schauble JF. Hemodynamic changes with prone positioning during general anesthesia. Anesthesia Analgesia 1995. 64: 194
4. Wadsworth R. et al. The effect of four different surgical prone positions on cardiovascular parameters in healthy volunteers. Anesthesia 1996. Sep;51(9):819-22
5. Sudheer PS et al.. Haemodynamic effects of the prone position: a comparison of propofol total intravenous and inhalation anesthesia. Anesthesia 2006. Feb;61(2): 138–141
6. Pelosi P. et al: The prone position during general anesthesia minimally affects respiratory mechanics while improving FRC and increasing oxygen tension. Anesthesia Analgesia 1995. 80:955,
7. Nyren S. et al. Pulmonary perfusion is more uniform in the prone than in the supine position: scintigraphy in healthy humans. Journal of Applied Physiology. 1999;86:1135-41.
8. Dharmavaram S. et al. Effect of prone positioning systems on hemodynamic and cardiac function during lumbar spine surgery: an echocardiographic study. Spine 2006. May 20;31(12):1388-93
9. Martin JT and Warner MA (eds). Positioning in Anesthesia and Surgery (3rd edition) . WB Saunders, PA 1997.
10. Chu YC et al. Lateral Medullary Syndrome after Prone Position for General Surgery. Anesthesia Analgesia 2002 .Nov;95(5):1451-3
11. Jericho BG and Skaria GP. Contact Dermatitis After the Use of the PronePositioner. Anesthesia Analgesia 2003,97(6):1706-8.
31

References12. ASA Closed Claims Project http://www.asaclosedclaims.org/
13. American Society of Anesthesiologists Task Force on Perioperative Blindness: Practice advisory for perioperative visual loss associated with spine surgery: a report by the American Society of Anesthesiologists Task Force on Perioperative Blindness Anesthesiology 2006. 104:1319–1328.
14. Brown J. et al. Cardiac arrest during surgery and ventilation in the prone position: a case report and systematic review. Resuscitation 2001. 50(2) : 233-238 Atwater BI et al. Pressure on the face while in the prone position: Prone View™ versus Prone Positioner™. Journal of Clinical Anesthesia 2004. Mar;16(2):111-6.
15. Baig MN et al. Vision loss after spine surgery: review of the literature and recommendations. Neurosurgery Focus 2007. 23(5):E1.
16. Chen SH et al. Paraplegia by acute cervical disc protrusion after lumbar spine surgery. Chang Gung Medical Journal 2005..Apr;28(4):254-7.
17. Palmon SC, et al. The effect of the prone position on pulmonary mechanics is frame-dependent. Anesthesia Analgesia 1998. Nov;87(5):1175-80.
18. Rehder K. et al. Regional intrapulmonary gas distribution in awake and anesthetized-paralyzed prone man. Journal of Applied Physiology 1978. 45:528.
19. Kaneko K. et al. Regional distribution of ventilation and perfusion as a function of body position. Journal of Applied Physiology 1966. 21:767–777.
20. Manna EM et al. The effect of prone position on respiratory mechanics during spinal surgery. Middle East Journal of Anesthesiology 2005. Oct;18(3):623-30
32