PROMOTINGROMOTING SOCIAL SOCIAL …
71
PROMOTING ROMOTING SOCIAL SOCIAL ENGAGEMENT ENGAGEMENT BY BY UNDERSTANDING UNDERSTANDING, , AND AND ENHANCING ENHANCING, , EMOTIONAL EMOTIONAL RESPONSITIVY RESPONSITIVY IN IN PERSONS PERSONS WHO WHO HAVE HAVE EXPERIENCED EXPERIENCED ABI ABI Presenters: Dawn Good, Ph.D., C. Psych. 1 Julie Baker, M.A., Psych., Ph.D. Candidate 1 Katie Chiappetta, BSc (Hons.) Candidate 1 Angela Dzyundzyak MA Psych Ph D Candidate 1 Angela Dzyundzyak, M.A., Psych., Ph.D. Candidate Stefon van Noordt, BA (Hons.), M.A. Candidate Harnessing the Power 2009 Provincial Acquired Brain Injury Conference Niagara Falls, Ontario Otb 29 2009 1 Neuropsychology Cognitive Research Lab, Brock University, St. Catharines, Ontario October 29, 2009
Transcript of PROMOTINGROMOTING SOCIAL SOCIAL …
PPROMOTINGROMOTING SOCIALSOCIAL ENGAGEMENTENGAGEMENT BYBYUNDERSTANDINGUNDERSTANDING, , ANDAND ENHANCINGENHANCING, , EMOTIONALEMOTIONAL RESPONSITIVYRESPONSITIVY ININ PERSONSPERSONSWHOWHO HAVEHAVE EXPERIENCEDEXPERIENCED ABIABI
Presenters:Dawn Good, Ph.D., C. Psych.1
Julie Baker, M.A., Psych., Ph.D. Candidate1
Katie Chiappetta, BSc (Hons.) Candidate1
Angela Dzyundzyak M A Psych Ph D Candidate1Angela Dzyundzyak, M.A., Psych., Ph.D. CandidateStefon van Noordt, BA (Hons.), M.A. Candidate
Harnessing the Power2009 Provincial Acquired Brain Injury Conference
Niagara Falls, OntarioO t b 29 2009
1Neuropsychology Cognitive Research Lab, Brock University, St. Catharines, Ontario
October 29, 2009
PPSYCHOSYCHOSSOCIALOCIAL OUTCOMESOUTCOMESPPSYCHOSYCHOSSOCIALOCIAL OUTCOMESOUTCOMES& B& BRAINRAIN IINJURYNJURY
Psychosocial outcomes for individuals who have experienced an acquired brain injury (ABI) areexperienced an acquired brain injury (ABI) are more limited relative to age-appropriate cohorts.
While cognitive and physical gains have permitted return to activities and engagement when assessed 10 years later, socioemotional factors continue to influence community integration and quality of life satisfaction ( D P f d &quality of life satisfaction (e.g. Draper, Ponsford, & Schonberger, 2007; Hoofen, Gilboa, Vakil, & Donovick, 2001)
PPSYCHOSYCHOSSOCIALOCIAL OOUTCOMESUTCOMES& B& BRAINRAIN IINJURYNJURY
Individuals and others who know them report
& B& BRAINRAIN IINJURYNJURY
Individuals, and others who know them, report continuing and high rates of depression, anxiety, and loneliness; and successful socialanxiety, and loneliness; and successful social interactions and relationships are compromised as a function of social challenges, not the least of which includes the person’s aggression or anger.
PPSYCHOSYCHOSSOCIALOCIAL OOUTCOMESUTCOMES
O t di d t t th t i di id l i
& B& BRAINRAIN IINJURYNJURYOur studies demonstrate that individuals are, in fact, physiologically underaroused prior to a triggering event and are less able to interprettriggering event and are less able to interpret emotional signals from themselves or others.
As a result, social personality variables of aggression or anger are actually reactive in
t t ‘ t t ’ f b i gnature – not a ‘state’ of being.
Incompatible social responses, or reduced socialIncompatible social responses, or reduced social contact in the community arise, in part, due to a lessened ability to experience emotional responses in one’s self or detect the emotional reactions of others.
PPSYCHOSYCHOSSOCIALOCIAL OOUTCOMESUTCOMES& B& BRAINRAIN IINJURYNJURY
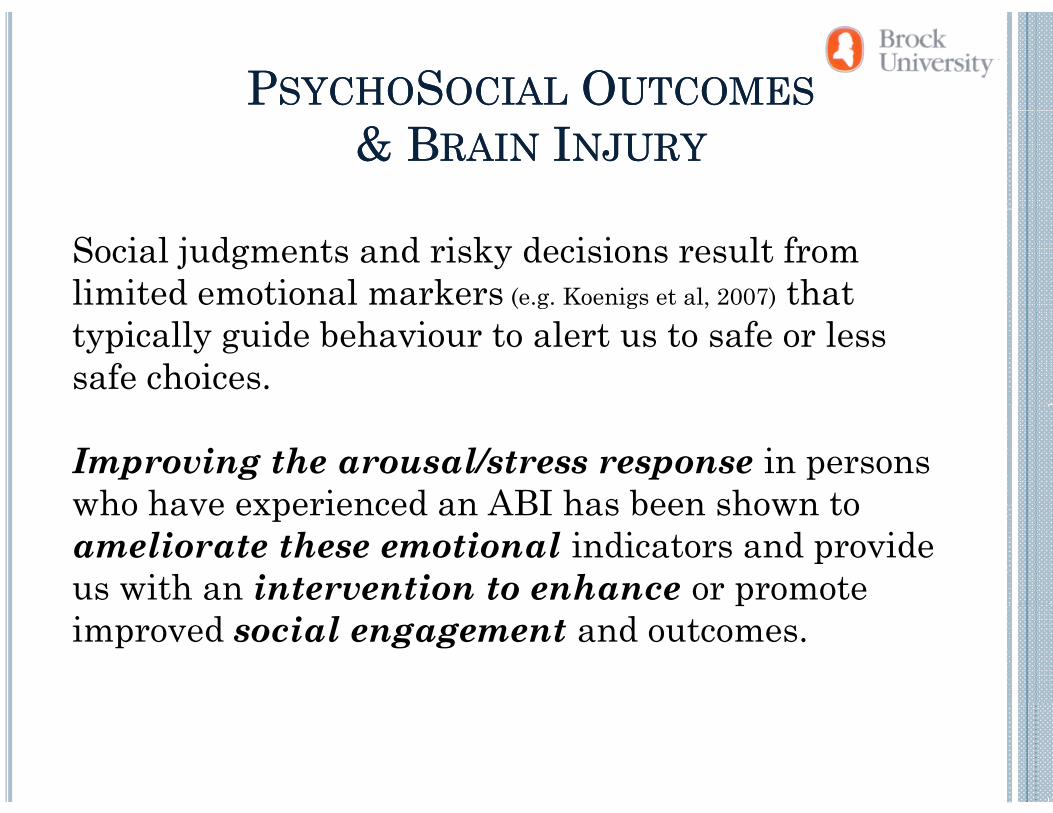
Social judgments and risky decisions result from limited emotional markers (e.g. Koenigs et al, 2007) that ( g g , )
typically guide behaviour to alert us to safe or less safe choices.
Improving the arousal/stress response in persons who have experienced an ABI has been shown towho have experienced an ABI has been shown to ameliorate these emotional indicators and provide us with an intervention to enhance or promote pimproved social engagement and outcomes.
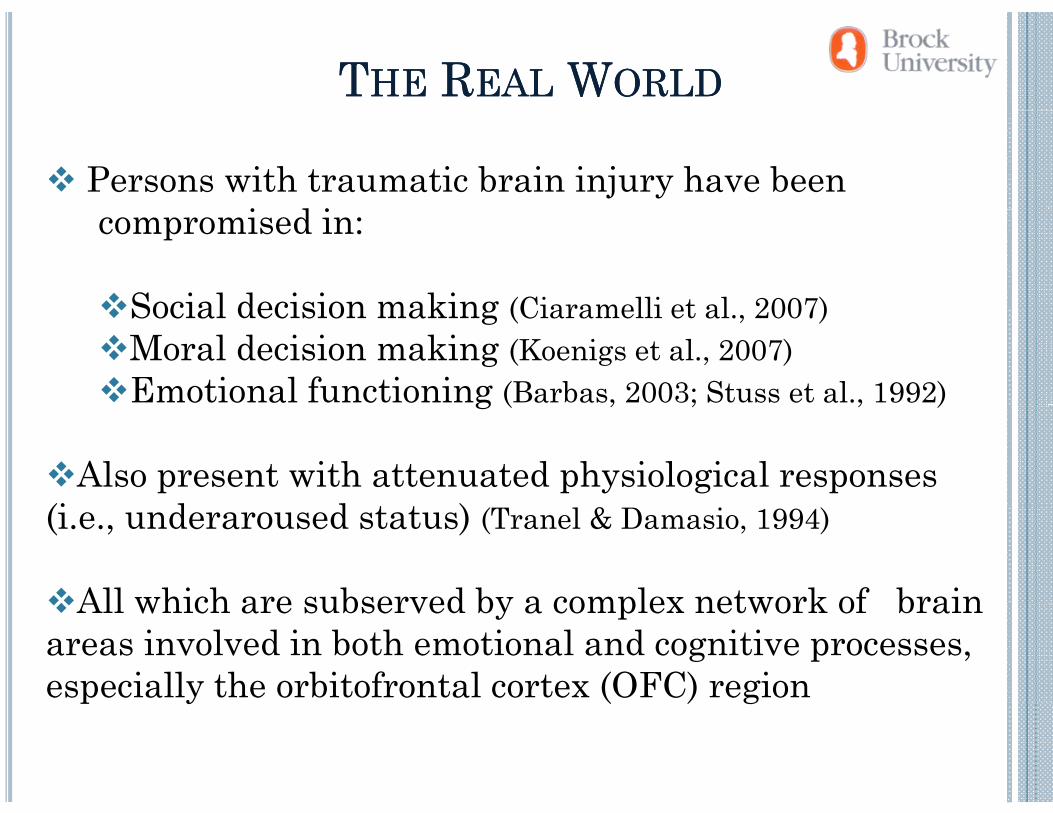
TTHEHE RREALEAL WWORLDORLD
Persons with traumatic brain injury have been i d icompromised in:
Social decision making (Ciaramelli et al 2007)Social decision making (Ciaramelli et al., 2007)Moral decision making (Koenigs et al., 2007)Emotional functioning (Barbas, 2003; Stuss et al., 1992)g ( , ; , )
Also present with attenuated physiological responses (i d d )(i.e., underaroused status) (Tranel & Damasio, 1994)
All which are subserved by a complex network of brainAll which are subserved by a complex network of brain areas involved in both emotional and cognitive processes, especially the orbitofrontal cortex (OFC) regionp y ( ) g
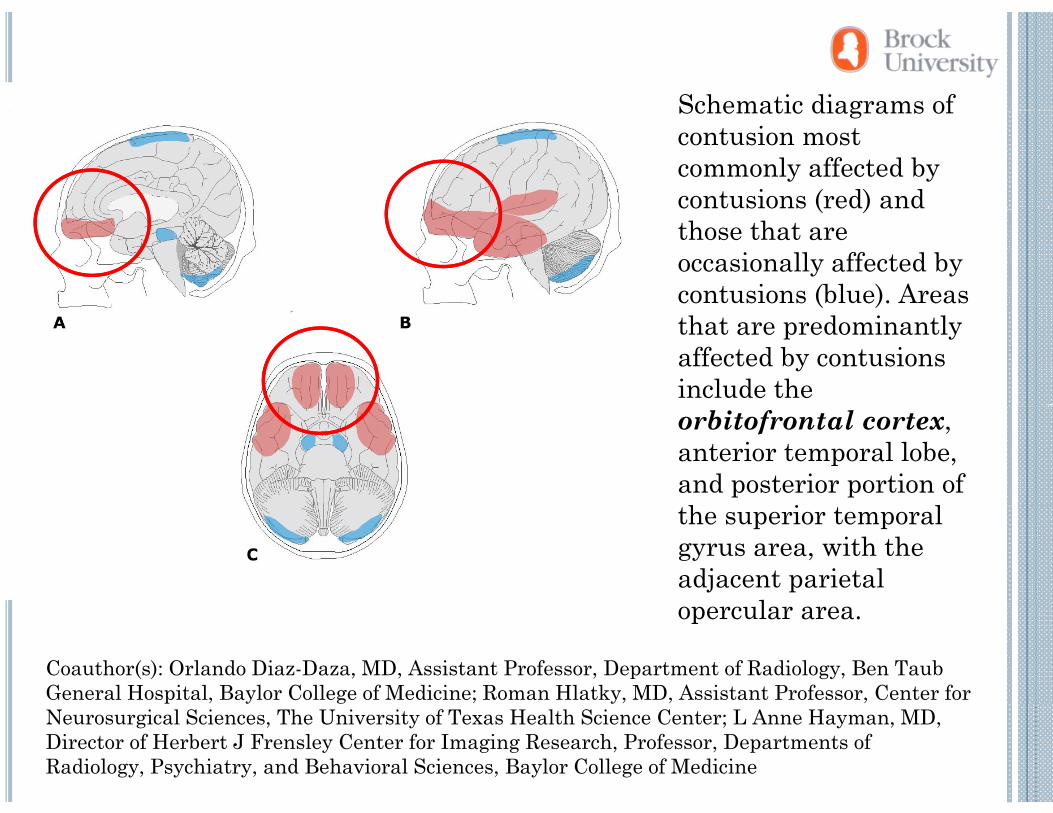
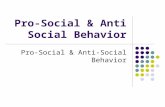
Schematic diagrams ofSchematic diagrams of contusion most commonly affected by contusions (red) and ( )those that are occasionally affected by contusions (blue). Areas ( )that are predominantly affected by contusions include the orbitofrontal cortex, anterior temporal lobe, and posterior portion of h i lthe superior temporal
gyrus area, with the adjacent parietal
l
Coauthor(s): Orlando Diaz-Daza, MD, Assistant Professor, Department of Radiology, Ben TaubGeneral Hospital, Baylor College of Medicine; Roman Hlatky, MD, Assistant Professor, Center for
opercular area.
p , y g ; y, , ,Neurosurgical Sciences, The University of Texas Health Science Center; L Anne Hayman, MD, Director of Herbert J Frensley Center for Imaging Research, Professor, Departments of Radiology, Psychiatry, and Behavioral Sciences, Baylor College of Medicine
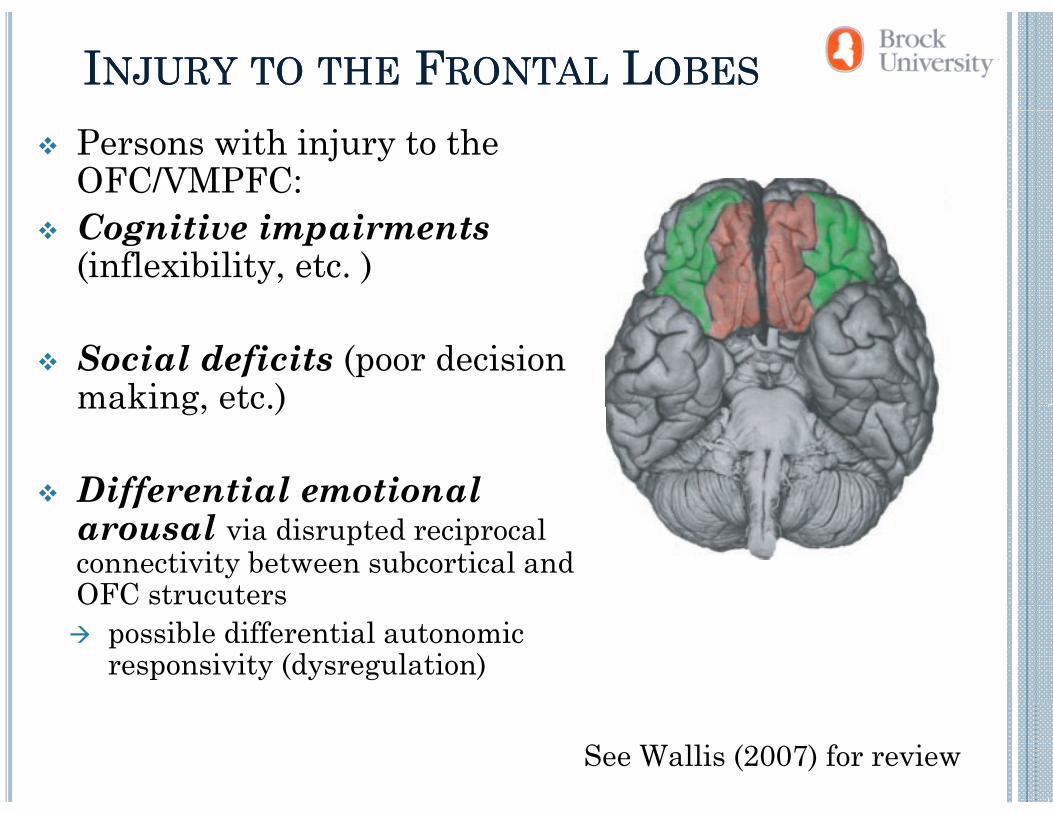
IINJURYNJURY TOTO THETHE FFRONTALRONTAL LLOBESOBES
Persons with injury to the OFC/VMPFC:Cognitive impairments (inflexibility, etc. )
Social deficits (poor decision making, etc.)making, etc.)
Differential emotional ffarousal via disrupted reciprocal connectivity between subcortical and OFC strucutersOFC strucuters
possible differential autonomic responsivity (dysregulation)
See Wallis (2007) for review
PPHYSIOLOGICALHYSIOLOGICAL FFEEDBACKEEDBACK
And these behaviours are likely all reflective of OFC connectivity:y
e.g. limits on decision making may reflect lack of physiological/emotive feedback indicating ‘caution’
i.e. the relationship between
“Gut Reaction”/Arousal and the decision ‘not’ to do somethingg
(Bechara, Damasio, &Damasio, 2000)
CCONSEQUENCESONSEQUENCES OFOF PFCPFC//OFCOFC INJURYINJURY::CCONSEQUENCESONSEQUENCES OFOF PFCPFC//OFCOFC INJURYINJURY: : KNOWINGKNOWING VERSUSVERSUS DOINGDOING
Global intellect intact, but unable to apply social knowledge (e g Phineas Gage - Harlow 1848)knowledge (e.g., Phineas Gage Harlow, 1848).
Cognitively competent but in vivo decision-makingCognitively competent, but in vivo decision-making impaired (e.g., E.V.R. - Eslinger et al., 1985; Saver et al., 1991).)
Understand problem and possible solutions, but p p ,inability to execute properly (Robertson et al., 2008).
Prevalence of Prevalence of head Injury head Injury Globally 57 million hospitalizations per yearGlobally, 57 million hospitalizations per year
(Langlois et al., 2006)
1/3 sustain injury before 25 (McKinlay et al 2008)1/3 sustain injury before 25 (McKinlay et al., 2008)
70-90% classified as ‘mild’ (Cassidy et al., 2004)
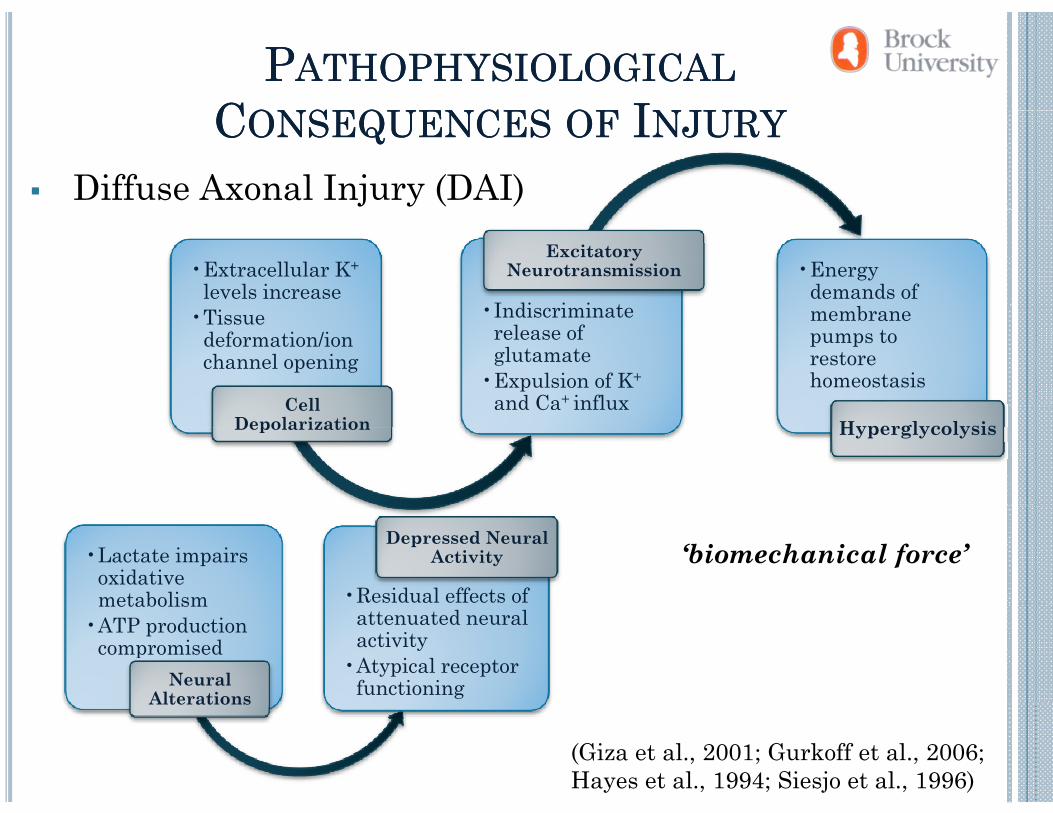
PPATHOPHYSIOLOGICALATHOPHYSIOLOGICALCCONSEQUENCESONSEQUENCES OFOF IINJURYNJURYCCONSEQUENCESONSEQUENCES OFOF IINJURYNJURY
Diffuse Axonal Injury (DAI)
•Extracellular K+
levels increase•Indiscriminate
Excitatory Neurotransmission •Energy
demands of b•Tissue
deformation/ion channel opening
Cell
•Indiscriminate release of glutamate
•Expulsion of K+
and Ca+ influx
membrane pumps to restore homeostasis
Cell Depolarization
and Ca influx Hyperglycolysis
•Lactate impairs oxidative metabolism •Residual effects of
Depressed Neural Activity ‘biomechanical force’
metabolism •ATP production
compromisedNeural
Alterations
attenuated neural activity
•Atypical receptor functioning Alterations
(Giza et al., 2001; Gurkoff et al., 2006; Hayes et al., 1994; Siesjo et al., 1996)
MMILDILD HHEADEAD IINJURYNJURY
Kay et al. (1993): ay e a . ( 993):
physical trauma to the head p yvia biomechanical force sufficient to produce an alteration inalteration in consciousness (e.g., dizziness, dazed, disoriented)
loss of consciousness not required
Previous studies have ev o s s es aveshown the prevalence of MHI in university students yto be ~37% (Chuah et al., 2004; Segalowitz & Lawson, 1995)
Sustained MHI primarily due to:due to:
Accidental fallsSports activitiespMotor Vehicle Collisions(Belanger & Vanderploeg, 2005; Cassidy et al 2004)Cassidy et al., 2004)
MMILDILD HHEADEAD IINJURYNJURY & P& PERSONALITYERSONALITY
Interpersonal relationships rely on personality
MMILDILD HHEADEAD IINJURYNJURY & P& PERSONALITYERSONALITY
Interpersonal relationships rely on personalityPersonality factors:
Socially unacceptable behavioursy pAggressionImpulsivity
Research questionIs mild head injury associated with maladaptive personality characteristics? If yes then which ones?
MHI IMHI INDICATORNDICATOR
Questionnaire:QDemographics
Have you ever had a head injury resulting in an altered state of consciousness (including: vomiting, dizziness, seeing stars, confusion)?
MMILDILD HHEADEAD IINJURYNJURY & P& PERSONALITYERSONALITY
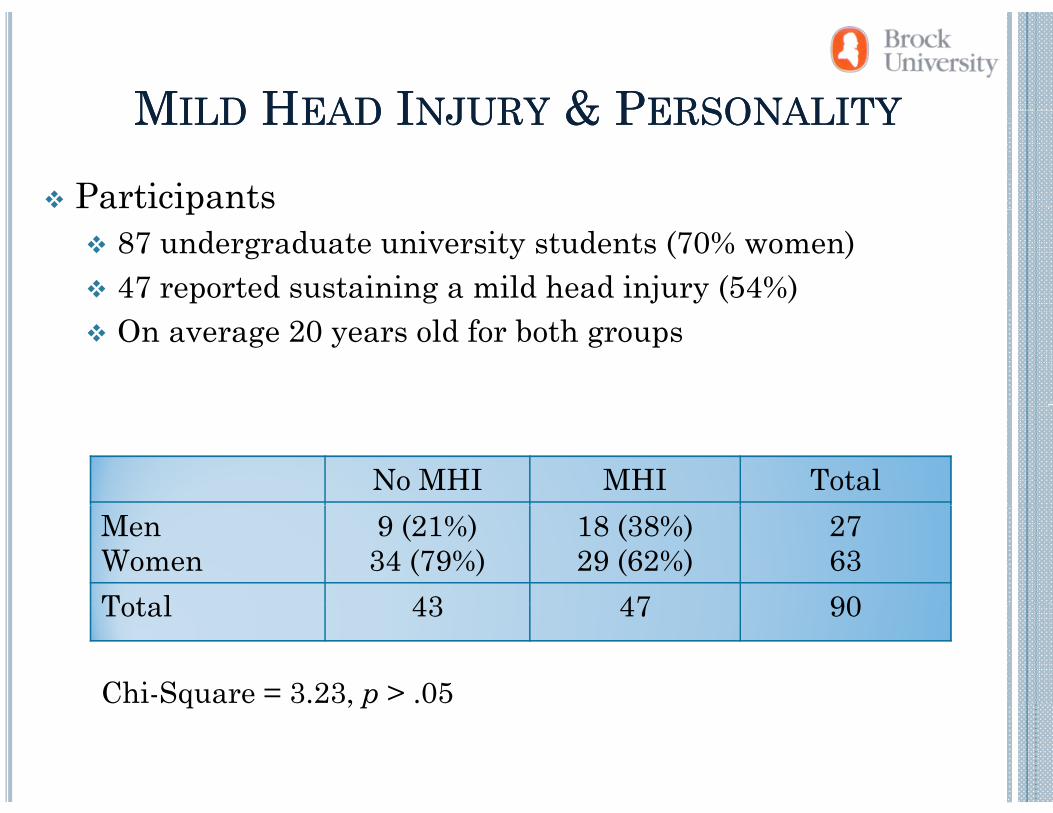
Participants
MMILDILD HHEADEAD IINJURYNJURY & P& PERSONALITYERSONALITY
p87 undergraduate university students (70% women)47 reported sustaining a mild head injury (54%)On average 20 years old for both groups
No MHI MHI TotalMenWomen
9 (21%)34 (79%)
18 (38%)29 (62%)
2763
Total 43 47 90Total 43 47 90
Chi-Square = 3.23, p > .05C Squa e 3. 3, p .05
MMILDILD HHEADEAD IINJURYNJURY & P& PERSONALITYERSONALITY
Personality
MMILDILD HHEADEAD IINJURYNJURY & P& PERSONALITYERSONALITY
yAggression Questionnaire (Buss & Perry, 1992)
Physical aggression, Verbal aggression, Hostility, AngerSRP Checklist (Paulhus et al., in press)
Erratic lifestyle, Socially unacceptable behaviours, Callous affect, Interpersonal manipulationp p
Barratt’s Impulsiveness Scale (Patton, Stanford, & Barratt, 1995)
Attentional impulsivity, Non-planning, DisinhibitionDelay discounting/gratification task (Kirby, Petry, & Bickel, 1999)1999)
MMILDILD HHEADEAD IINJURYNJURY & P& PERSONALITYERSONALITYMMILDILD HHEADEAD IINJURYNJURY & P& PERSONALITYERSONALITY
Executive functionReasoning
CTONI (1996)Cognitive flexibility
T il (DKEFS 2002)Trails (DKEFS, 2002)Sustained attention
NEPSY (NEPSY-2nd Ed., 2007)( , )Working memory
Mental Control (WMS-III, 1997)L b i (WMS III 997)Letter number sequencing (WMS-III, 1997)
MMHIHI ANDAND PPERSONALITYERSONALITY: E: EXPECTATIONSXPECTATIONS
Gender differences
Neurocognitive differences(Executive Functioning)
MHI Status
Personality Differences
MHI status would predict personality differences even after gender and executive functioning differences have b t k i t id tibeen taken into consideration
Higher levels socially unacceptable behaviour and erratic lifestyleHigher levels of reactive aggressiong f ggHigher levels of disinhibition (impulsivity)
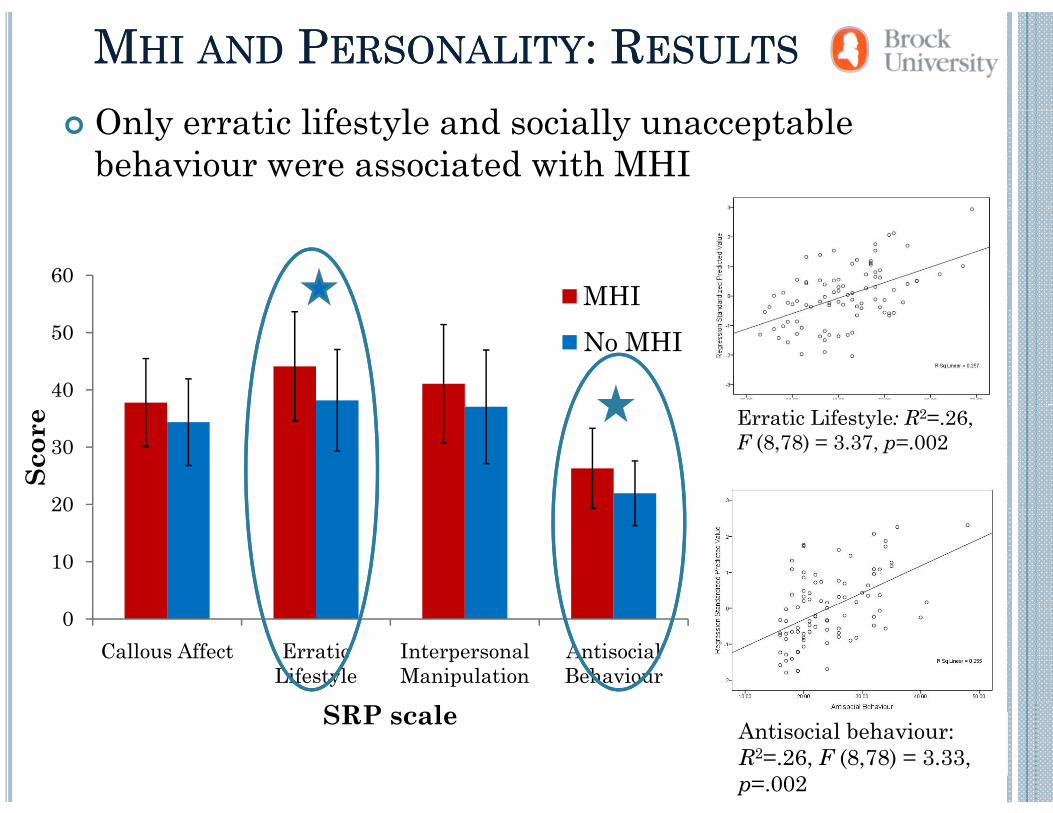
MMHIHI ANDAND PPERSONALITYERSONALITY: R: RESULTSESULTS
O l i lif l d i ll blOnly erratic lifestyle and socially unacceptable behaviour were associated with MHI
60MHI
40
50 No MHI
Erratic Lifestyle: R2=.26,F (8,78) = 3.37, p=.002
20
30
Scor
e
10
20
0Callous Affect Erratic
LifestyleInterpersonal Manipulation
Antisocial Behaviour
Antisocial behaviour: R2=.26, F (8,78) = 3.33, p=.002
SRP scale
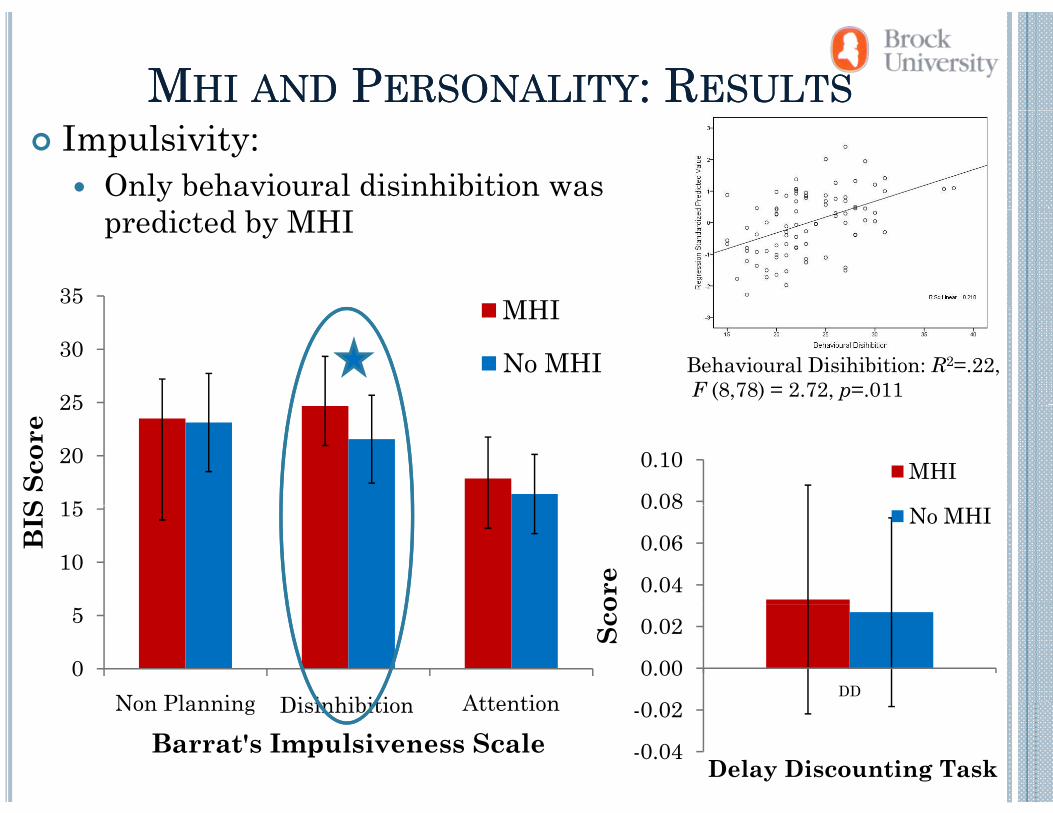
MMHIHI ANDAND PPERSONALITYERSONALITY: R: RESULTSESULTSImpulsivity:
Only behavioural disinhibition was predicted by MHI
35 MHI
25
30MHI
No MHI Behavioural Disihibition: R2=.22,F (8,78) = 2.72, p=.011
0 08
0.10 MHI15
20
25
S Sc
ore
0.04
0.06
0.08
ore
No MHI
10
15
BIS
0 02
0.00
0.02
DD
Sco
0
5
Non Planning Disihbibition AttentionDisinhibition
-0.04
-0.02
Delay Discounting Task
Non Planning Disihbibition Attention
Barrat's Impulsiveness ScaleDisinhibition
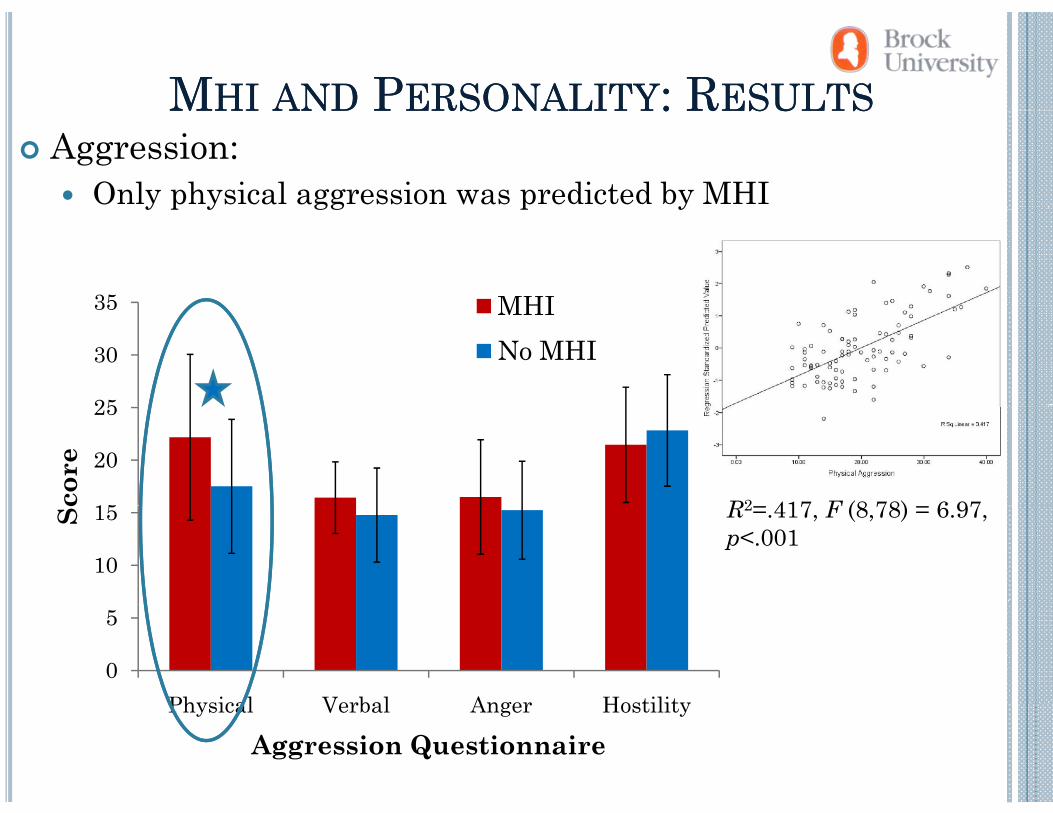
MMHIHI ANDAND PPERSONALITYERSONALITY: R: RESULTSESULTSMMHIHI ANDAND PPERSONALITYERSONALITY: R: RESULTSESULTSAggression:
Only physical aggression was predicted by MHI y p y gg p y
35 MHI
25
30
35 MHINo MHI
15
20
25
core
R2 417 F (8 78) 6 97
10
15Sc R2=.417, F (8,78) = 6.97, p<.001
0
5
Physical Verbal Anger HostilityPhysical Verbal Anger Hostility
Aggression Questionnaire
SS II PP60 No MHI
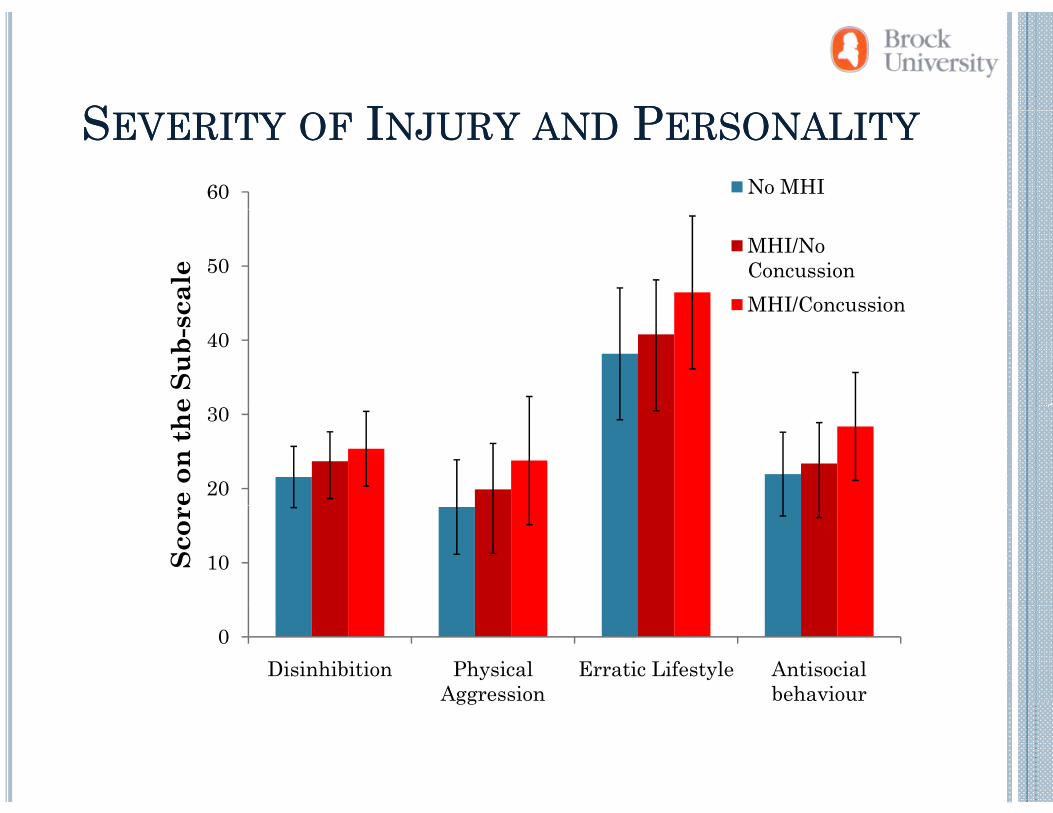
SSEVERITYEVERITY OFOF IINJURYNJURY ANDAND PPERSONALITYERSONALITY
50
cale
MHI/No ConcussionMHI/Concussion
40
e Su
b-sc MHI/Concussion
20
30
e on
the
10Scor
0Disinhibition Physical
AggressionErratic Lifestyle Antisocial
behaviourgg
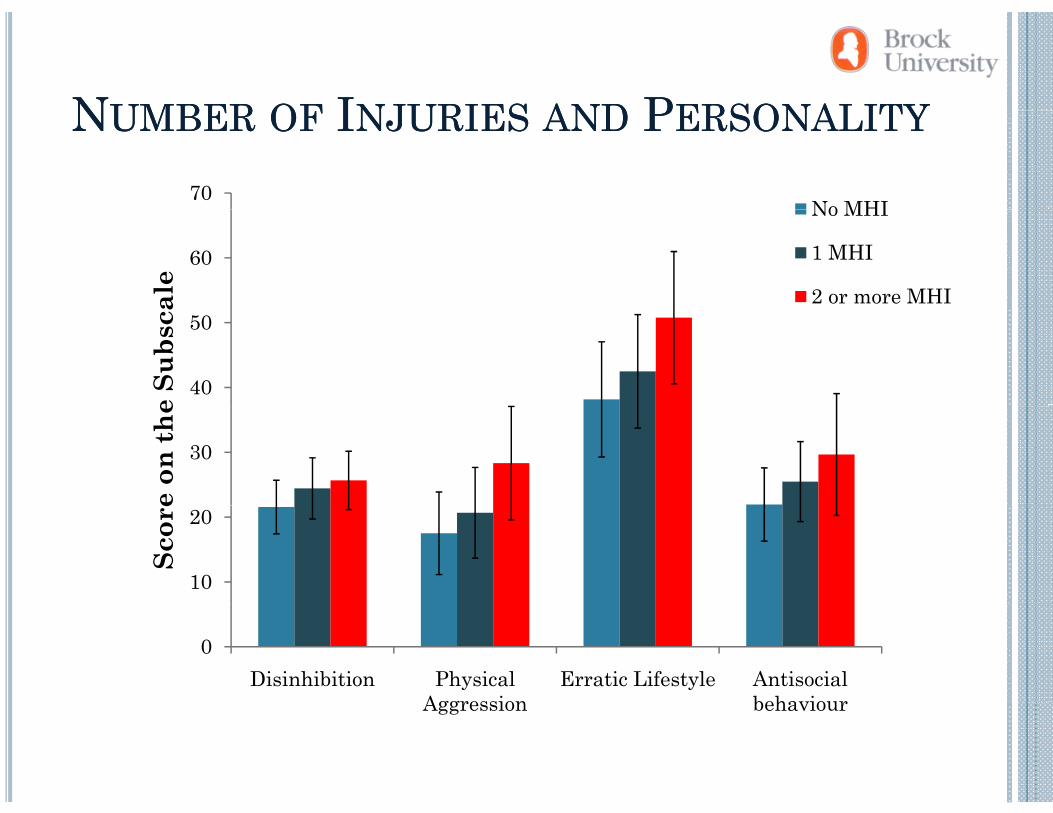
NNUMBERUMBER OFOF IINJURIESNJURIES ANDAND PPERSONALITYERSONALITY
70No MHI
NNUMBERUMBER OFOF IINJURIESNJURIES ANDAND PPERSONALITYERSONALITY
60
ale
No MHI
1 MHI
2 or more MHI
40
50
e Su
bsca
30
e on
the
10
20
Scor
e
0Disinhibition Physical
AggressionErratic Lifestyle Antisocial
behaviourAggression behaviour
MMHIHI ANDAND PPERSONALITYERSONALITY: S: SUMMARYUMMARY
Mild head injury was associated withHigher levels of behavioural disinhibition but not other types of impulsivityHigher levels of physical aggression but not other types ofHigher levels of physical aggression but not other types of aggressionMore socially unacceptable behaviour and erratic lifestyle
Furthermore:Behavioural disihibition was associated with MHI evenBehavioural disihibition was associated with MHI even after lifestyle and socially unacceptable behaviour were taken into consideration (Dzyundzyak, Good, & DeBono,
)2008)
MHIMHI ANDAND PPERSONALITYERSONALITY: S: SOO WWHATHAT??MHI MHI ANDAND PPERSONALITYERSONALITY: S: SOO WWHATHAT? ? Mild head injury is associated with inability to j y ywithhold responses and reactive physical aggression
These effects present as impulsive and aggressive personality characteristics, which in turn have a negative impact on interpersonal relationships
However, these responses are triggered by the environment and, thus, can be anticipated and
t dprevented
Social competence in terms of decision making can be a f i f OFC h hfunction of OFC through:
Arousal Arousal
Social Competence
Social Competence
Trauma or maturationOrbitofrontal
Cortex Orbitofrontal
Cortex
Arousal levels
Injury to the OFC Decision Making
(Yeates et al., 2007)
SSOCIALOCIAL DDECISIONSECISIONS: : MMORALORAL BBEHAVIOURSEHAVIOURS
Previous research demonstrates that persons who have
MMORALORAL BBEHAVIOURSEHAVIOURS
Previous research demonstrates that persons who have incurred a head injury may lack social awareness demonstrated through self-report social problem solving skills (K d ll t l 1997)(Kendall et al., 1997)
Persons who have experienced injury to the VMPFC are more likely to agree with a socially unacceptable choice relative to persons who have not incurred a head injury (Ciaramelli et al., 2007; Koenigs et al., 2007); g , )
Persons who had not incurred a head injury were more reluctant to make decisions that resulted in personalreluctant to make decisions that resulted in personal transgressions compared with impersonal, whereas persons with injury to the VMPFC took equally as long (Ciaramelli et al 2007)al., 2007)
HHYPOTHESESYPOTHESESIndividuals with MHI would rate themselves as
having similar social problem solving skills as i di id l i hindividuals with no MHI
BUTBUT…When individuals with MHI consider social/moral
decisions, we expect their performance to reflect , p pdifferent processes:
Persons with MHI will make lessPersons with MHI will make less socially acceptable choices, and be quicker to do so, compared to no q , pMHI counterparts
MHI IMHI INDICATORNDICATOR
Questionnaire:QDemographics
Have you ever had a head injury resulting in an altered state of consciousness (including: vomiting, dizziness, seeing stars, confusion)?
DDEMOGRAPHICSEMOGRAPHICS
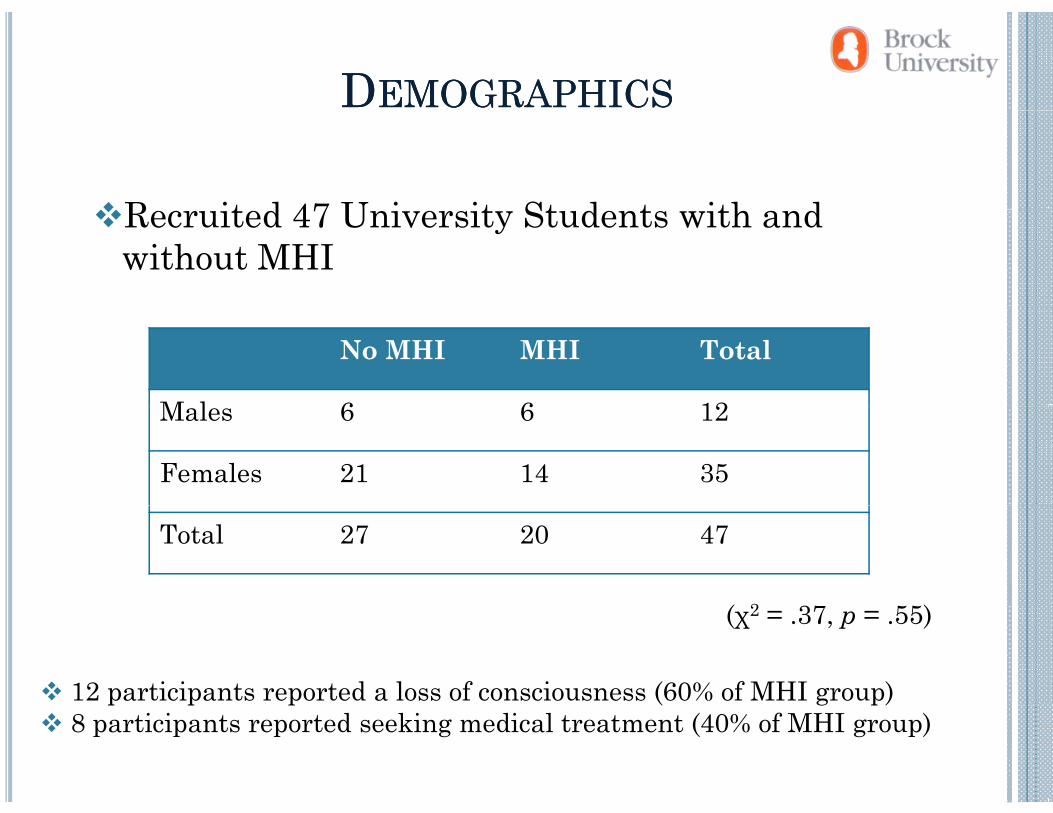
R it d 47 U i it St d t ith dRecruited 47 University Students with andwithout MHI
No MHI MHI Total
M l 6 6 12Males 6 6 12
Females 21 14 35
Total 27 20 47
2(χ2 = .37, p = .55)
12 participants reported a loss of consciousness (60% of MHI group)p p p ( g p)8 participants reported seeking medical treatment (40% of MHI group)
MMEASURESEASURES
Moral JudgmentMoral JudgmentDemographicDemographic Social ProblemSocial ProblemMoral Judgment Task• Social
Moral Judgment Task• Social
Demographic Questionnaire • Indicator of
Demographic Questionnaire • Indicator of
Social Problem Solving Inventory
Social Problem Solving Inventory
situation• Presents a
it ti i
situation• Presents a
it ti i
head injury head injury • Describe how they believe they make
• Describe how they believe they makesituation in
which a social dilemma is
situation in which a social dilemma is
they make choices they make choices
requiredrequired
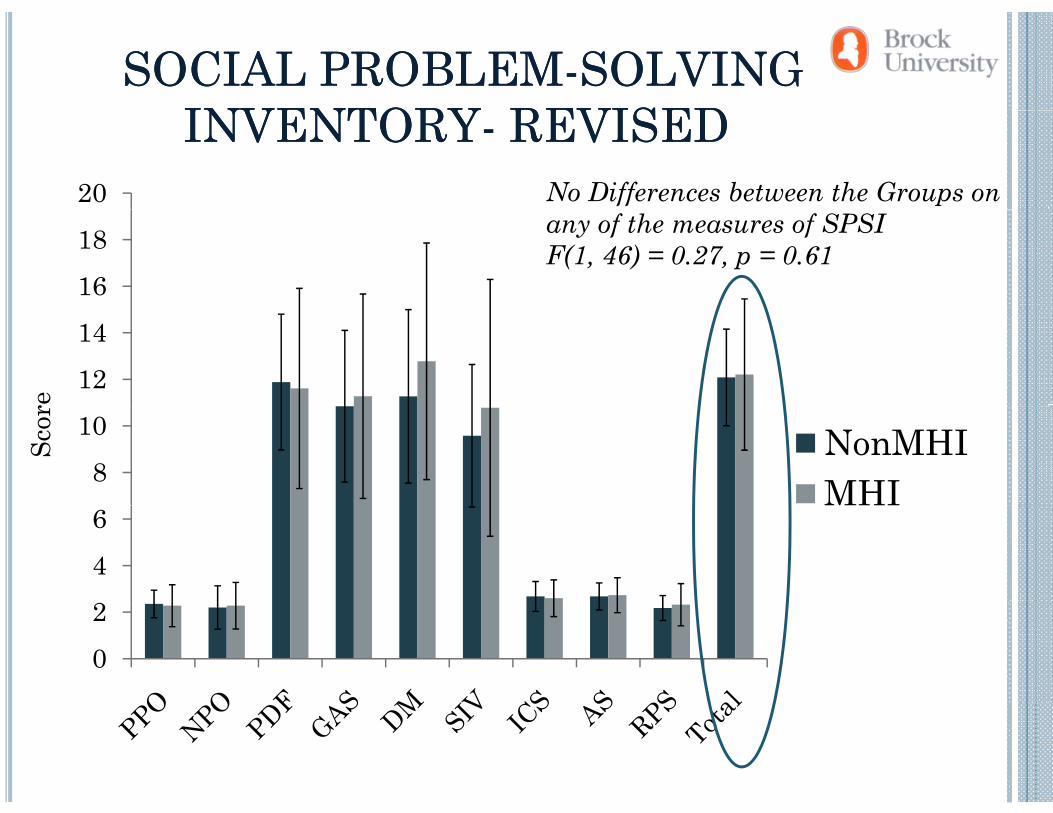
SOCIAL PROBLEMSOCIAL PROBLEM--SOLVING SOLVING INVENTORYINVENTORY REVISEDREVISED
20
INVENTORYINVENTORY-- REVISEDREVISEDNo Differences between the Groups on
1618 any of the measures of SPSI
F(1, 46) = 0.27, p = 0.61
1214
re
810 NonMHI
MHI
Scor
246
02
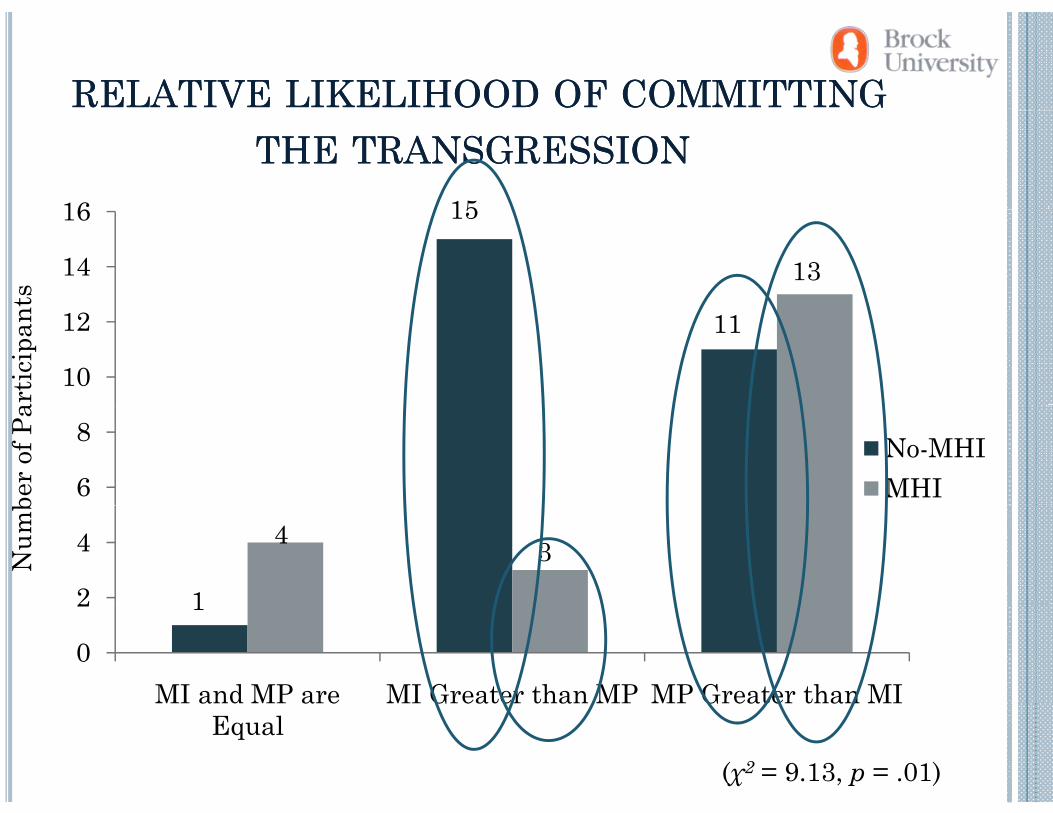
RELATIVERELATIVE LIKELIHOODLIKELIHOOD OFOF COMMITTINGCOMMITTING
16 15
THETHE TRANSGRESSIONTRANSGRESSION
nts
14
16 15
13
artic
ipan
10
12 11
ber o
f Pa
6
8 No-MHIMHI
Num
b
2
4 4 3
1
0
2
MI and MP are MI Greater than MP MP Greater than MI
1
(χ2 = 9.13, p = .01)
MI and MP are Equal
MI Greater than MP MP Greater than MI
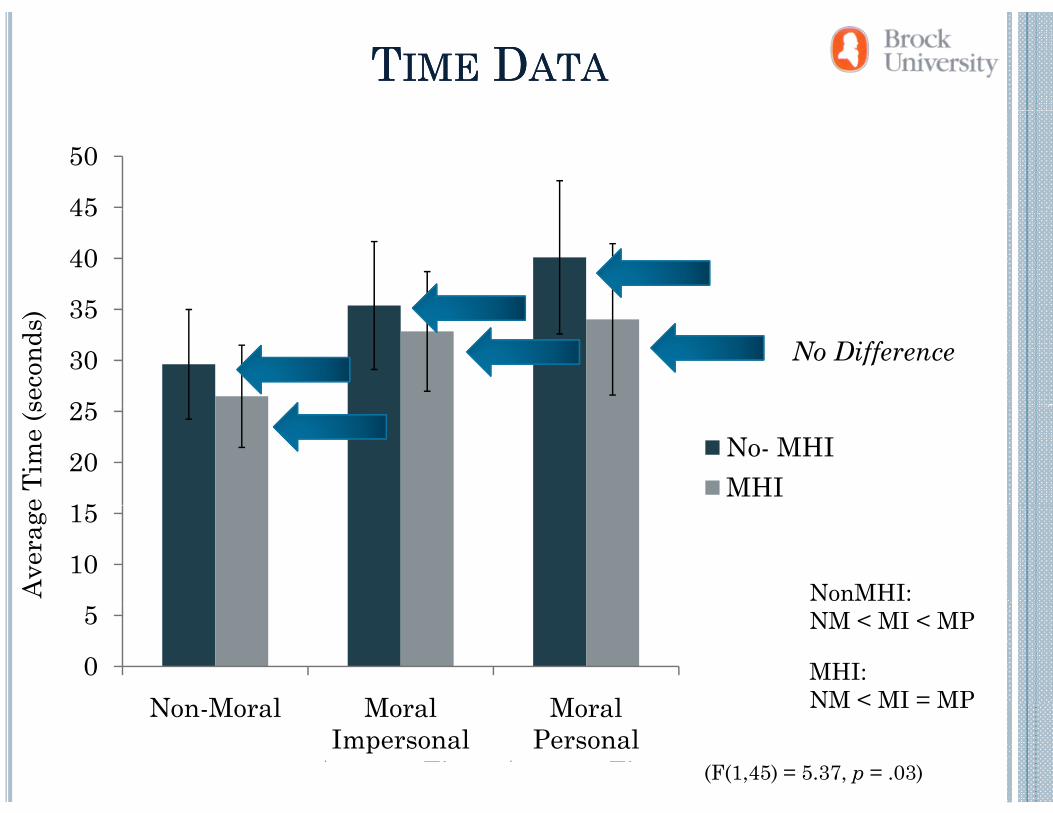
TTIMEIME DDATAATA
45
50
35
40
45
seco
nds)
25
30
35No Difference
e Ti
me
(s
15
20
25No- MHIMHI
NonMHI:Ave
rage
10
15
NM < MI < MP
MHI:NM < MI = MP
0
5
N M l M l M l NM < MI = MP
(F(1,45) = 5.37, p = .03)
Non-Moral Average Time
Moral Impersonal
Average Time
Moral Personal
Average Time
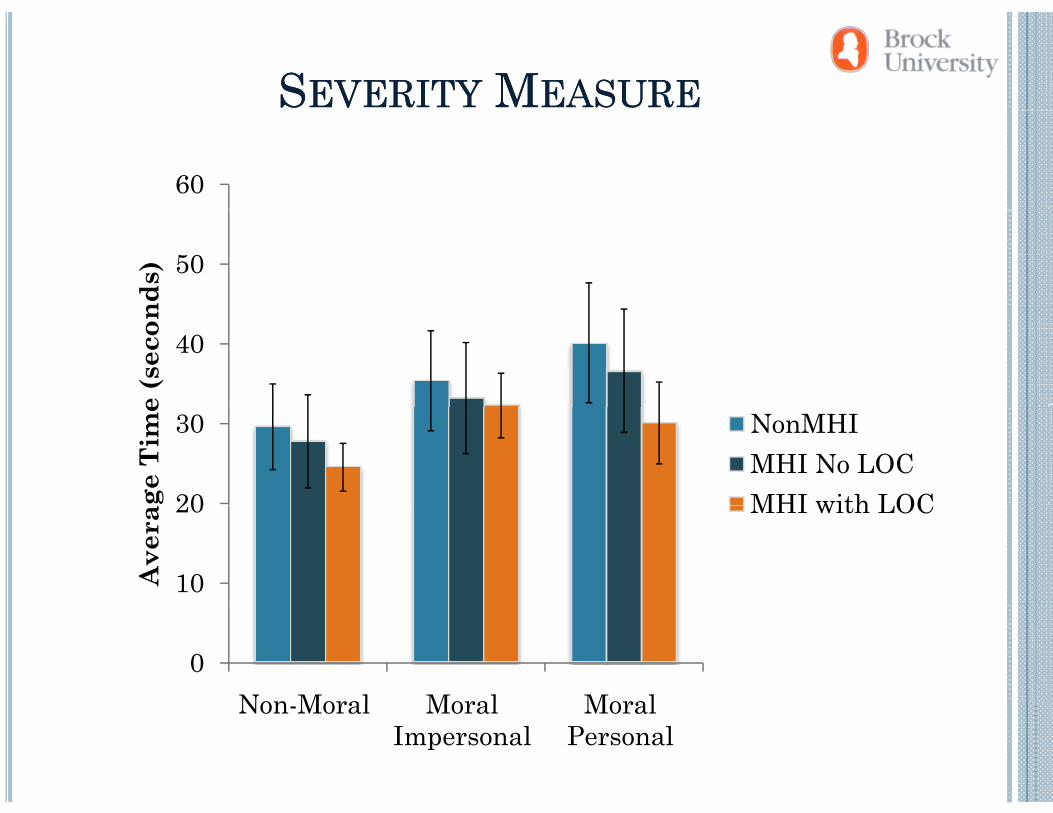
SSEVERITYEVERITY MMEASUREEASURE
60
50
nds)
40
e (s
econ
20
30
ge T
ime
NonMHIMHI No LOC MHI with LOC
10
20
Ave
ra
MHI with LOC
0Non Moral Moral MoralNon-Moral Moral
Impersonal Moral
Personal
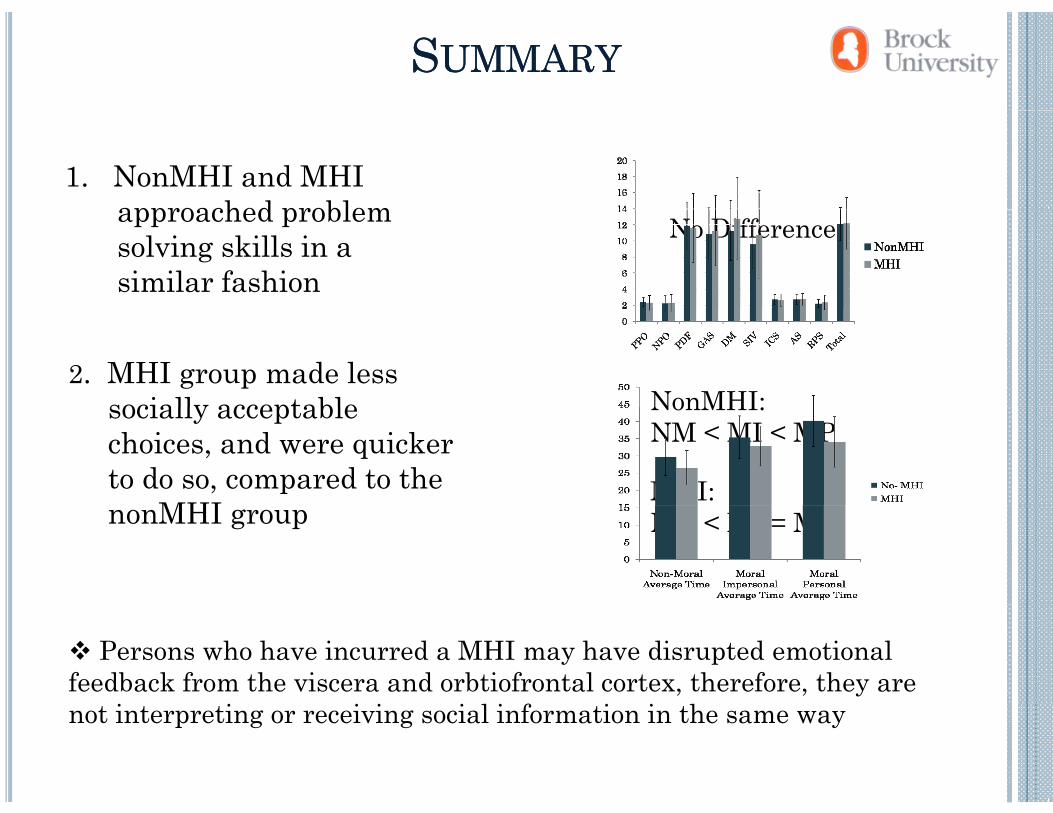
SSUMMARYUMMARY
1. NonMHI and MHI approached problemapproached problem solving skills in a similar fashion
No Difference
2. MHI group made less socially acceptable NonMHI:socially acceptable choices, and were quicker to do so, compared to the
MHI
NonMHI:NM < MI < MP
MHI:nonMHI group NM < MI = MP
Persons who have incurred a MHI may have disrupted emotional feedback from the viscera and orbtiofrontal cortex, therefore, they are not interpreting or receiving social information in the same way
DDECISIONECISION MAKINGMAKING, , EMOTIONALEMOTIONAL,,MARKERSMARKERS ANDAND LEARNINGLEARNING
Emotional feedback to consequences of decisionsEmotional feedback to consequences of decisions signals a discrepancy between one’s expectation and what actually happens (Nieuwenhuis et al., 2004; Oya et al., 2005 S t t l 2009)2005; Santesso et al., 2009)
Affect (valence) associated with an outcome providesAffect (valence) associated with an outcome provides basis for adaptive learning (Bechara, 2004; Rudrauf et al., 2009) – i.e. negative feelings = learn to avoid, or anticipate the negative consequence in future situations
Anticipation of potential future consequences via somatic marker activation (Damasio 1996; Denburg et alsomatic marker activation (Damasio, 1996; Denburg et al., 2007)
CCONSEQUENCESONSEQUENCES OFOF OFC IOFC INJURYNJURY
Have the capacity to emotionally respond to theHave the capacity to emotionally respond to the environment, but have limited activation of anticipatory emotional responses
Limited affective markers compromise emotion precognition in oneself and others (Heberlein et al., 2008; Hopkins et al., 2002; Ietswaart et al., 2008)
Insensitive to the potential of future consequences to decisions (B h t l 1996 2000)decisions (Bechara et al., 1996; 2000)
HHYPOTHESESYPOTHESES
Might those with MHI, even though competent be emotionally
University students with MHI are expected to perform
OO
though competent, be emotionally uninformed when making
decisions?
are expected to perform competently on general cognitive tasksUniversity students with MHI
Do mild head injuries in university students relate to measurable differences in the
University students with MHI are expected to have attenuated physiological responses during the anticipatory stages of d i i kiability to generate and interpret
emotional signals from oneself and others?
decision-makingUniversity students with MHI are expected to be less successful in discriminating facial
How might variable physiological and neuropsychological
h i i fl i l
in discriminating facial expressions of emotionCompromise community reintegration and healthymechanisms influence social
decision making?reintegration and healthy interpersonal relationships
MMETHODSETHODS:: PPARTICIPANTSARTICIPANTS
Study 1 Study 2
OO :: CC
Study 1 Study 2
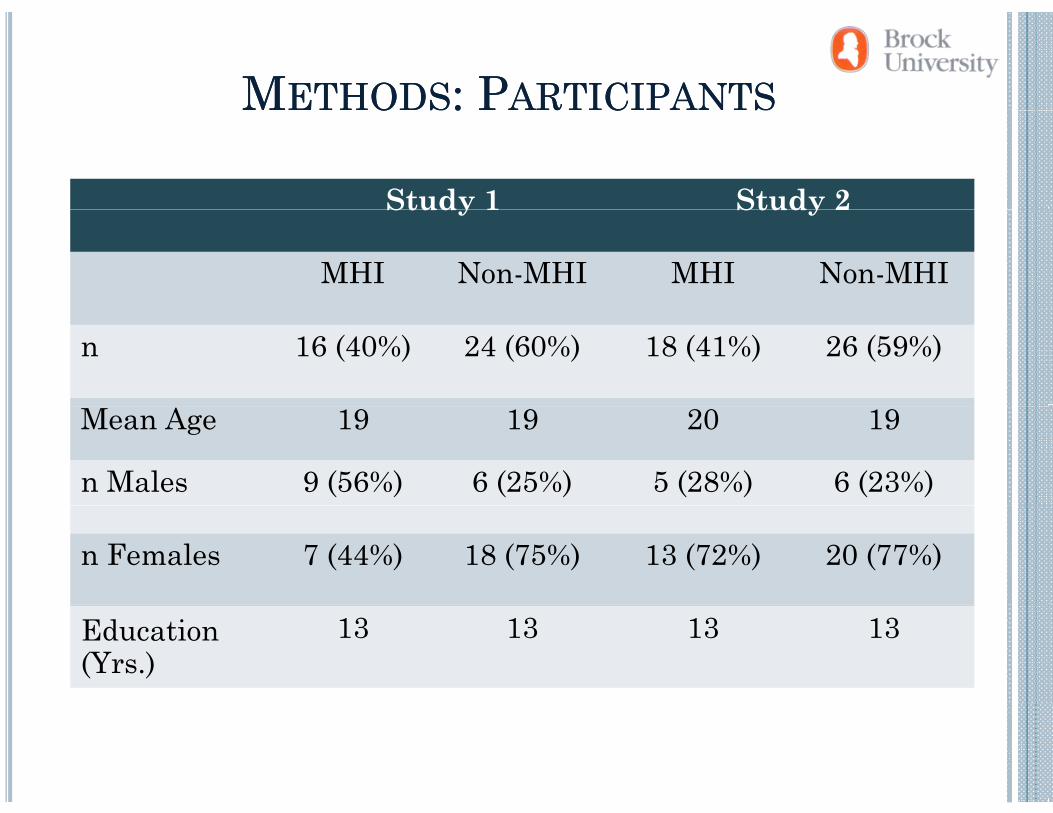
MHI Non-MHI MHI Non-MHI
n 16 (40%) 24 (60%) 18 (41%) 26 (59%)
Mean Age 19 19 20 19
n Males 9 (56%) 6 (25%) 5 (28%) 6 (23%)
n Females 7 (44%) 18 (75%) 13 (72%) 20 (77%)
Education(Yrs.)
13 13 13 13
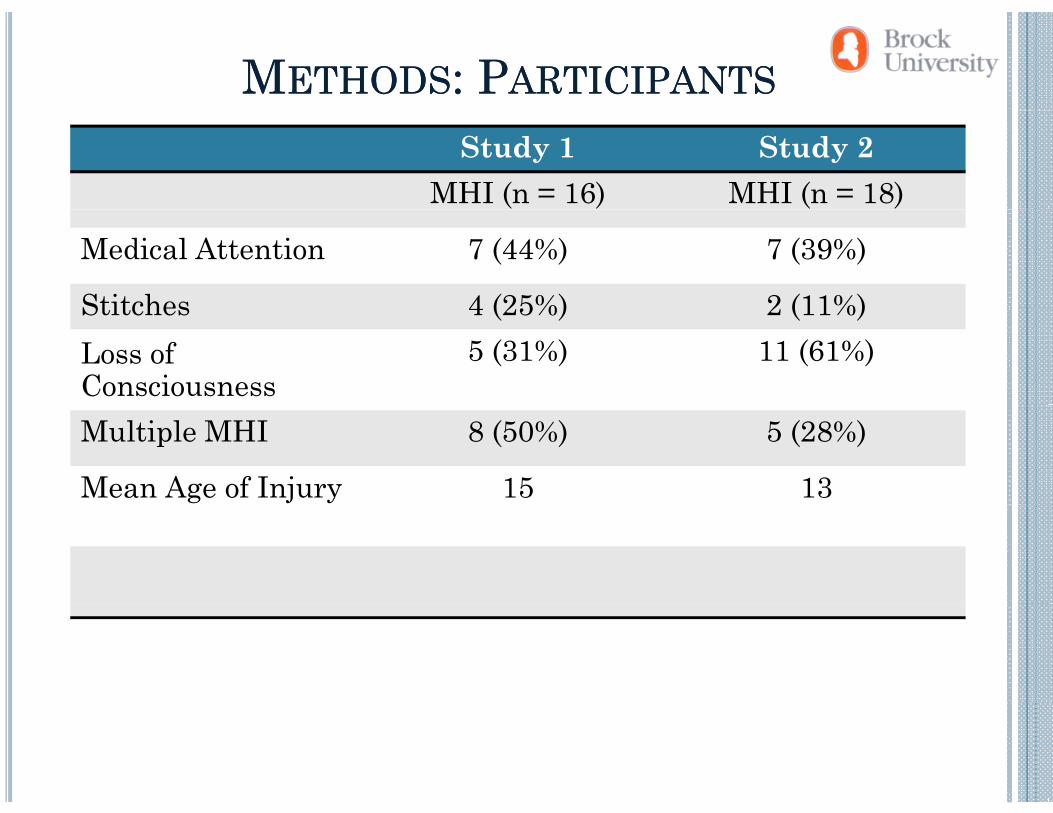
MMETHODSETHODS:: PPARTICIPANTSARTICIPANTSStudy 1 Study 2
MHI (n = 16) MHI (n = 18)
Medical Attention 7 (44%) 7 (39%)
Stitches 4 (25%) 2 (11%)Stitches 4 (25%) 2 (11%)Loss ofConsciousness
5 (31%) 11 (61%)
Multiple MHI 8 (50%) 5 (28%)
Mean Age of Injury 15 13
MMEASURESEASURESNeuropsychological Tasks:
General cognitive abilities:Design Fluency (Delis et al 2001)Design Fluency (Delis et al., 2001).
Behavioural decision-making: A B C DBehavioural decision-making:Iowa Gambling Task (IGT; Bechara, 2007).
Emotion discrimination:Affect Recognition (Korkman et al., 2007).Affect Recognition (Korkman et al., 2007).
ELECTROPHYSIOLOGICALELECTROPHYSIOLOGICAL EQUIPMENTEQUIPMENTELECTROPHYSIOLOGICALELECTROPHYSIOLOGICAL EQUIPMENTEQUIPMENT
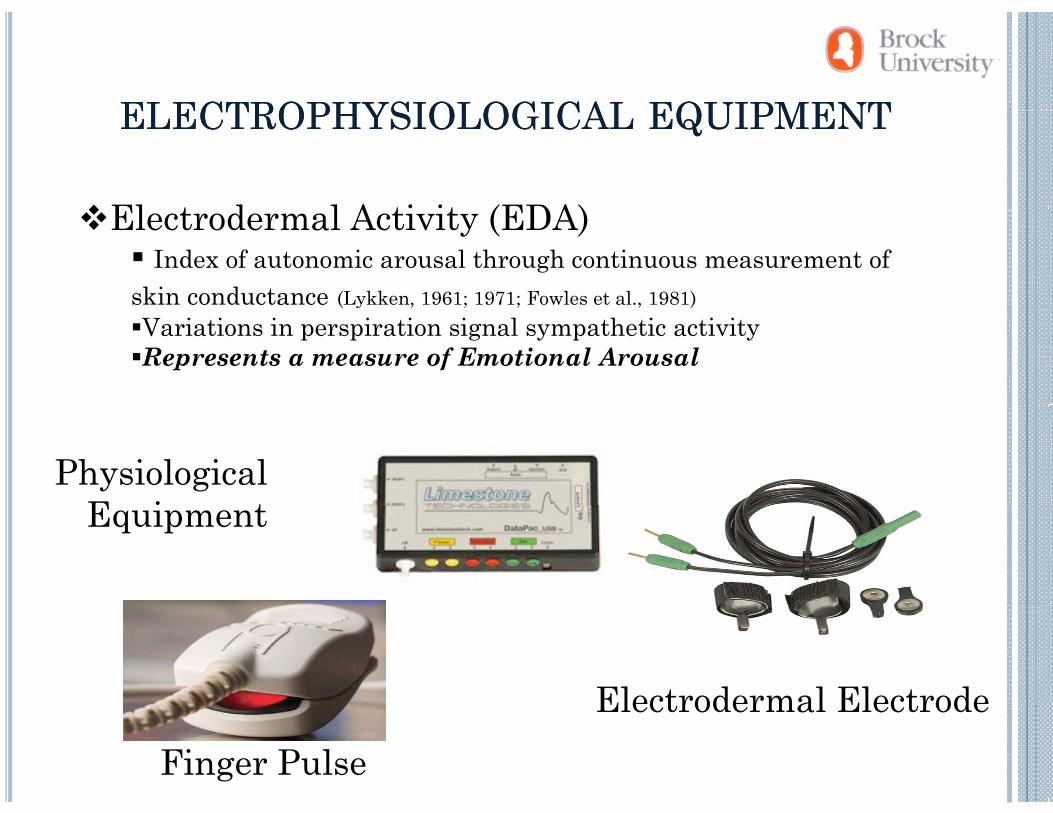
El t d l A ti it (EDA)Electrodermal Activity (EDA)Index of autonomic arousal through continuous measurement of
skin conductance (Lykken, 1961; 1971; Fowles et al., 1981)( y )Variations in perspiration signal sympathetic activityRepresents a measure of Emotional Arousal
Physiological E i tEquipment
Electrodermal ElectrodeFinger Pulse
Electrodermal Electrode
MHI IMHI INDICATORNDICATOR
Questionnaire:QDemographics
Have you ever had a head injury resulting in an altered state of consciousness (including: vomiting, dizziness, seeing stars, confusion)?
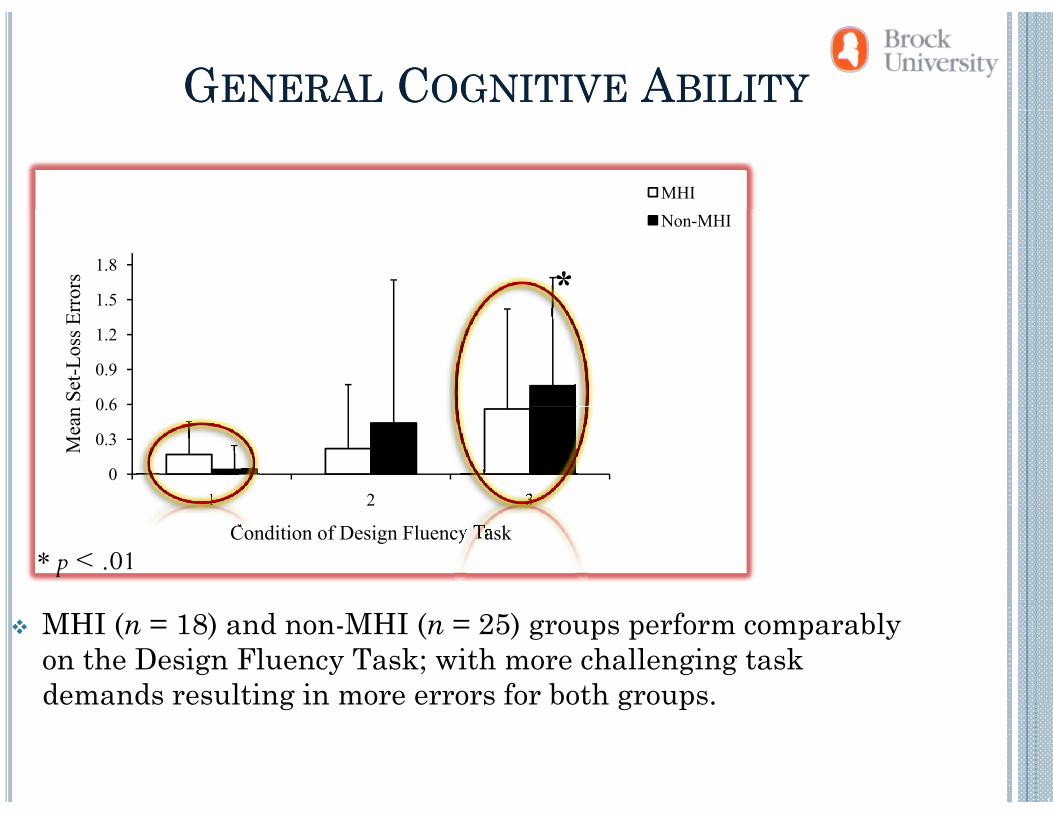
GGENERALENERAL CCOGNITIVEOGNITIVE AABILITYBILITY
MHI
1.5
1.8
rror
s
Non-MHI
*
0 6
0.9
1.2
Set
-Los
s Er
0
0.3
0.6
1 2 3
Mea
n
1 2 3
Condition of Design Fluency Task* p < .01
MHI (n = 18) and non-MHI (n = 25) groups perform comparably on the Design Fluency Task; with more challenging task demands resulting in more errors for both groups.demands resulting in more errors for both groups.
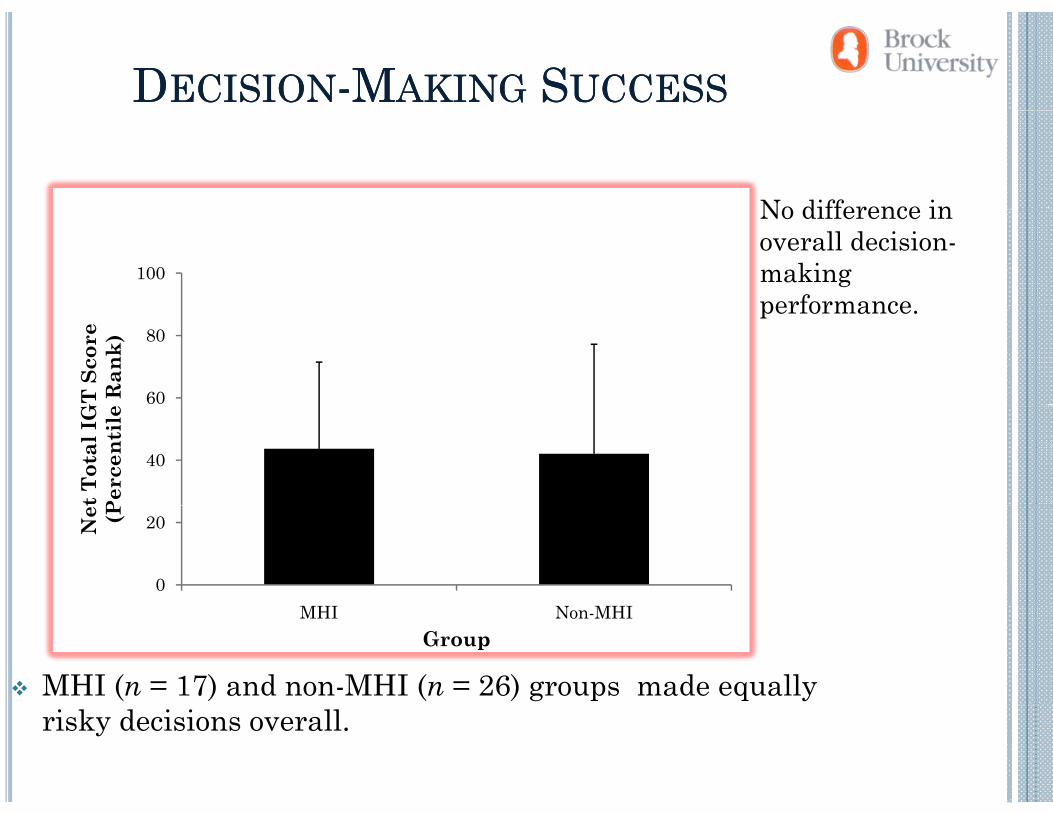
DDECISIONECISION--MMAKINGAKING SSUCCESSUCCESS
No difference in
100
No difference in overall decision-making performance
60
80
GT
Sco
ree
Ran
k)
performance.
40
t Tot
al I
GP
erce
ntil
e
0
20Net (P
MHI Non-MHIGroup
MHI (n = 17) and non-MHI (n = 26) groups made equally risky decisions overall.
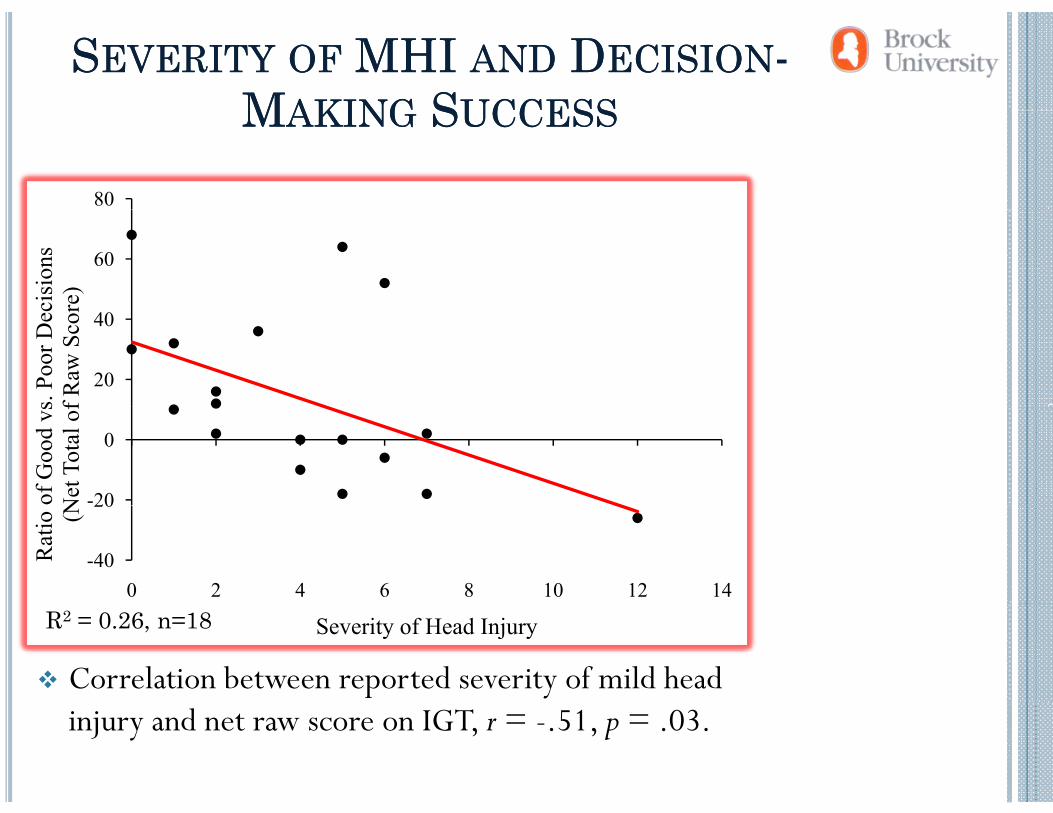
SSEVERITYEVERITY OFOF MHI MHI ANDAND DDECISIONECISION--MMAKINGAKING SSUCCESSUCCESS
80
MMAKINGAKING SSUCCESSUCCESS
60
cisi
ons
re)
20
40
s. Po
or D
ecf R
aw S
cor
-20
0
of G
ood
vsN
et T
otal
of
-40
20
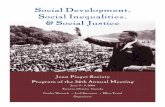
0 2 4 6 8 10 12 14
Rat
io (N
Severity of Head InjuryR2 = 0.26, n=18
Correlation between reported severity of mild head injury and net raw score on IGT, r = -.51, p = .03.
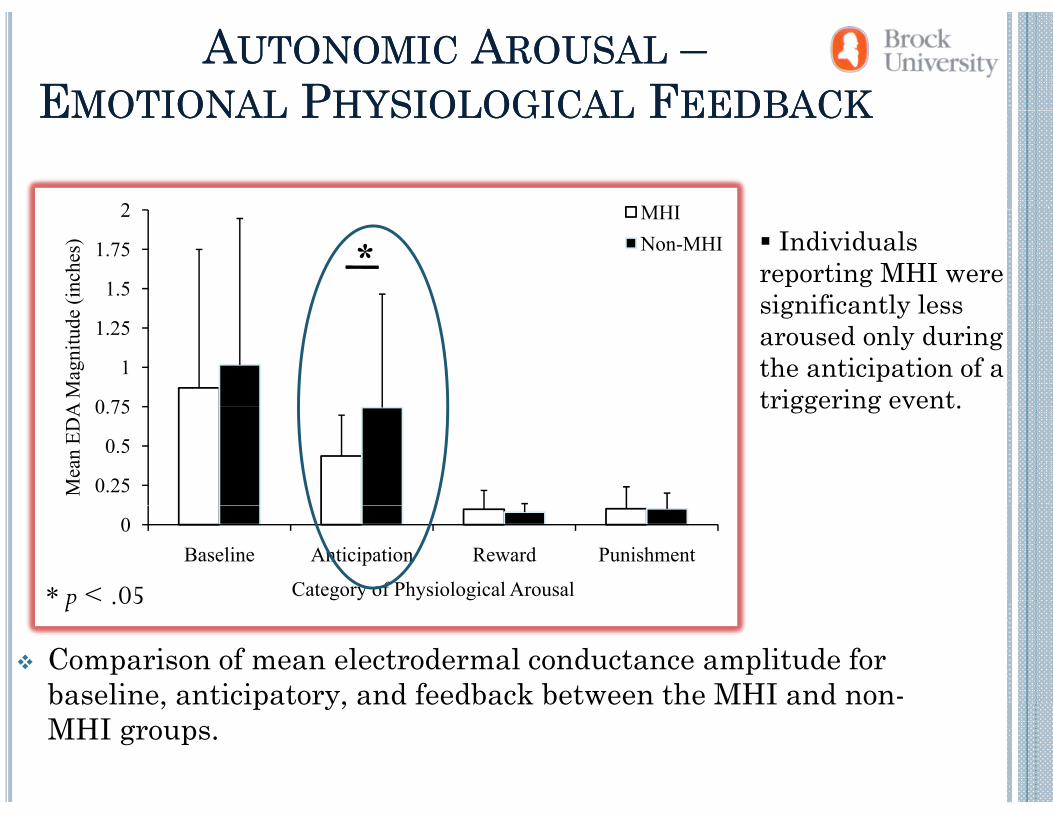
AAUTONOMICUTONOMIC AAROUSALROUSAL ––EEMOTIONALMOTIONAL PPHYSIOLOGICALHYSIOLOGICAL FFEEDBACKEEDBACK
2 MHI
EEMOTIONALMOTIONAL PPHYSIOLOGICALHYSIOLOGICAL FFEEDBACKEEDBACK
1.5
1.75
2
(inch
es)
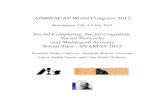
MHINon-MHI* Individuals
reporting MHI were significantly less
0 75
1
1.25
A M
agni
tude
significantly less aroused only during the anticipation of a triggering event.
0.25
0.5
0.75
Mea
n ED
A triggering event.
0Baseline Anticipation Reward Punishment
Category of Physiological Arousal* p < .05
Comparison of mean electrodermal conductance amplitude for baseline, anticipatory, and feedback between the MHI and non-
p .
baseline, anticipatory, and feedback between the MHI and nonMHI groups.
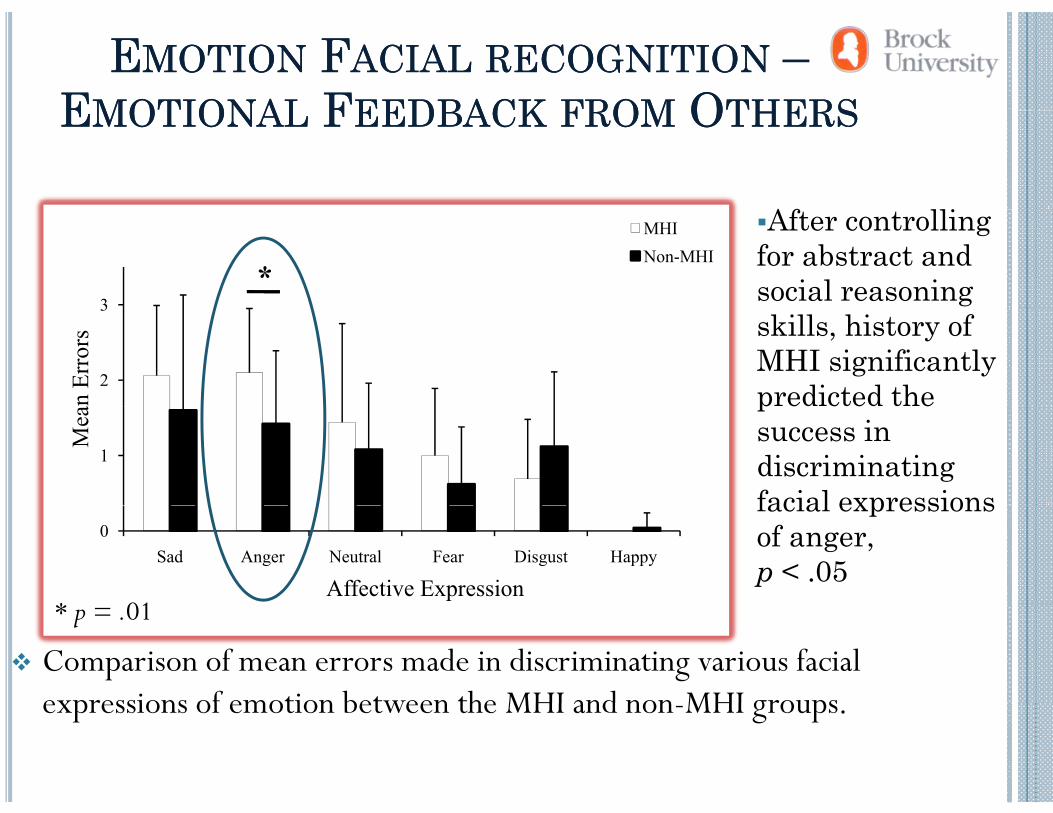
EEMOTIONMOTION FFACIALACIAL RECOGNITIONRECOGNITION ––EEMOTIONALMOTIONAL FFEEDBACKEEDBACK FROMFROM OOTHERSTHERS
Af lli
EEMOTIONALMOTIONAL FFEEDBACKEEDBACK FROMFROM OOTHERSTHERS
3
MHI Non-MHI
After controlling for abstract and social reasoning *
2
3
an E
rror
s skills, history of MHI significantly predicted the
1
Mea
psuccess in discriminating facial expressions
0Sad Anger Neutral Fear Disgust Happy
Affective Expression
facial expressions of anger, p < .05
* 01
Comparison of mean errors made in discriminating various facial expressions of emotion between the MHI and non MHI groups
* p = .01
expressions of emotion between the MHI and non-MHI groups.
SSUMMARYUMMARY OFOF FFINDINGSINDINGS
Intact intellect emotionally responsiveIntact intellect, emotionally responsive
Self-reported MHI severity is marker of underlying metabolic/neural disruptionmetabolic/neural disruption
Limited emotional markers during anticipatory stages of decision makingdecision-making
Individuals with MHI are limited in successful emotional di i i ti ( ti l l i f )discrimination (particularly expressions of anger)
Social decision-making behaviour in the MHI group is t i d b li it ti i i i ti lconstrained by limitations in processing socio-emotional
feedback
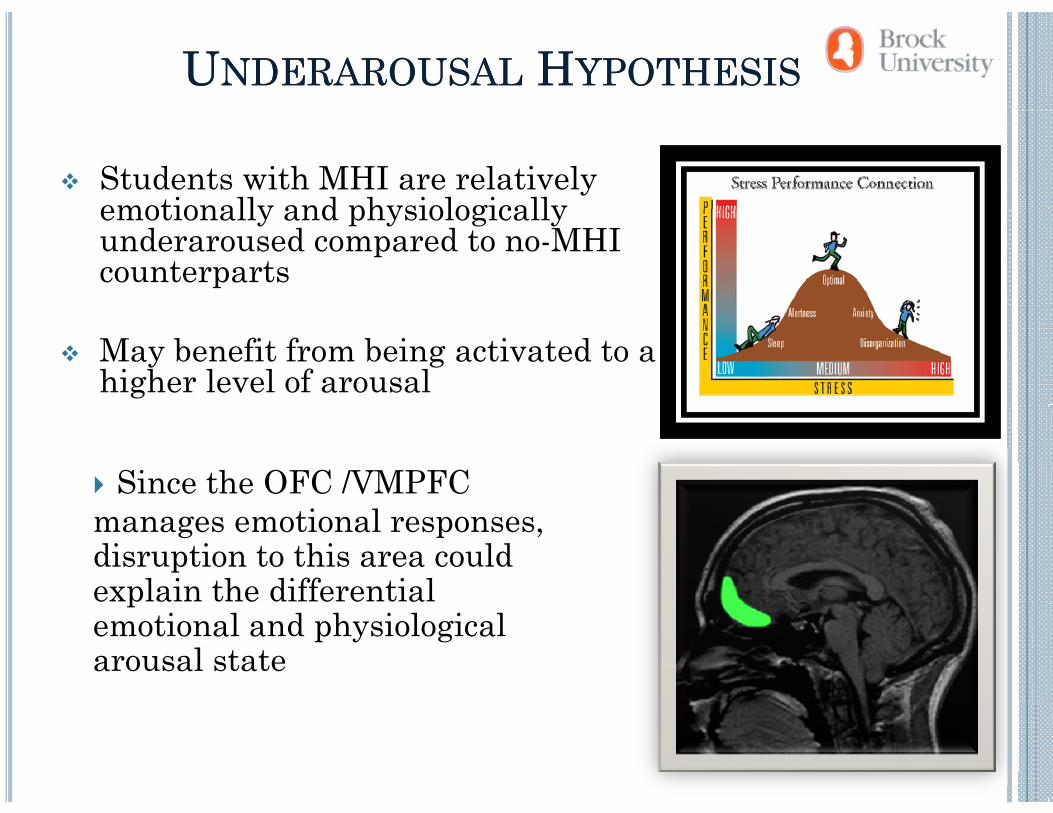
UUNDERAROUSALNDERAROUSAL HHYPOTHESISYPOTHESIS
Students with MHI are relatively emotionally and physiologicallyemotionally and physiologically underaroused compared to no-MHI counterparts
May benefit from being activated to a higher level of arousal
Since the OFC /VMPFC manages emotional responses, disruption to this area could explain the differential pemotional and physiological arousal state
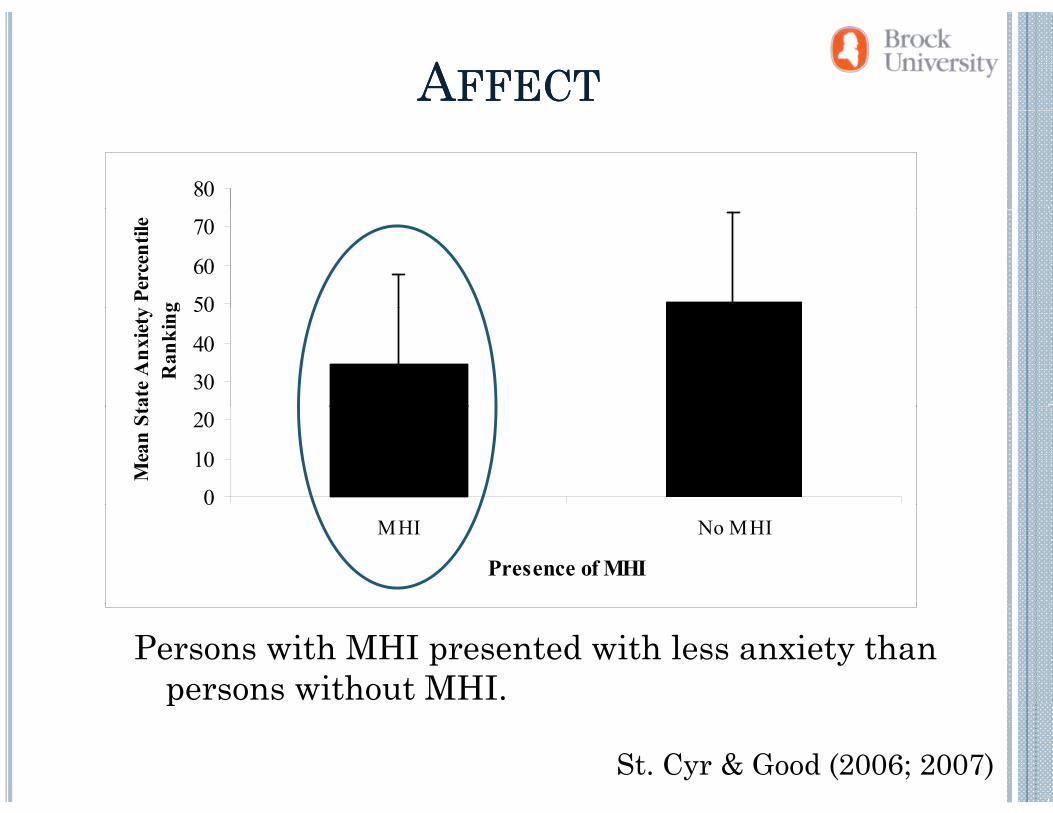
AAFFECTFFECT
80
50
60
70
y Pe
rcen
tile
g
30
40
50
ate
Anx
iety
Ran
king
0
10
20
Mea
n St
MHI No MHI
Presence of MHI
Persons with MHI presented with less anxiety than persons without MHI.p
St. Cyr & Good (2006; 2007)
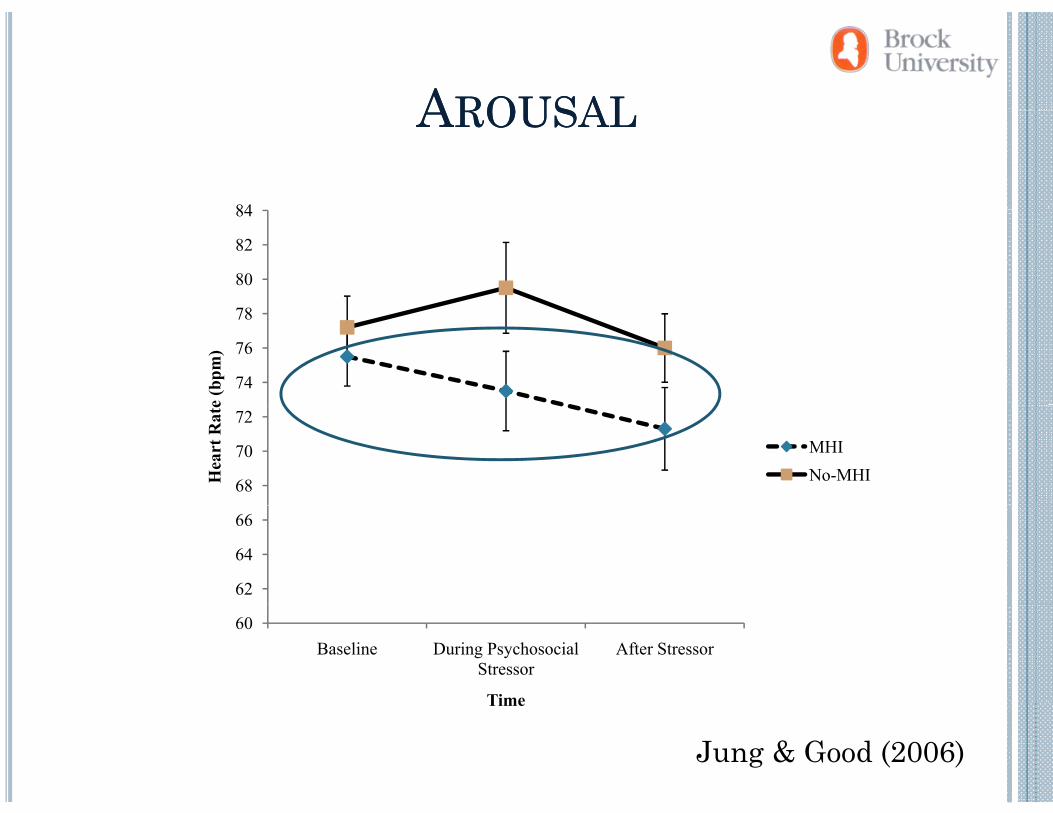
AAROUSALROUSALAAROUSALROUSAL
84
78
80
82
84
74
76
78
e (b
pm)
68
70
72
Hea
rt R
ate
MHINo-MHI
62
64
66
60Baseline During Psychosocial
StressorAfter Stressor
Time
Jung & Good (2006)
Time
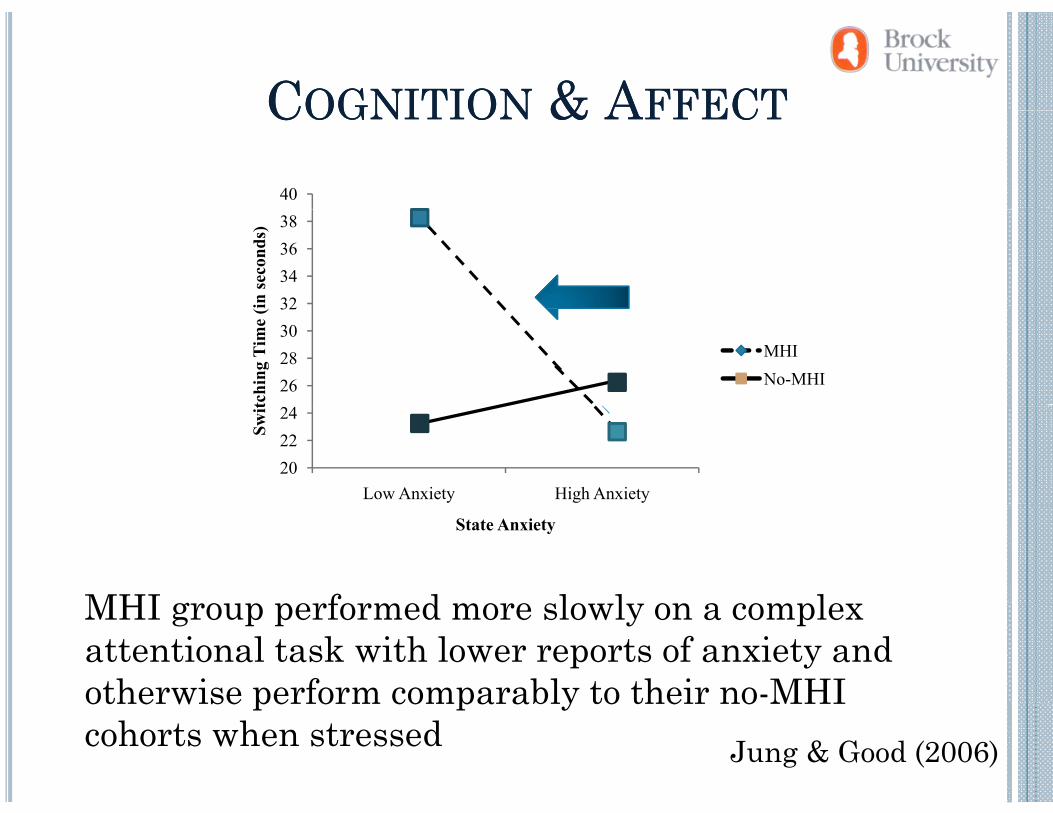
CCOGNITIONOGNITION & A& AFFECTFFECTCCOGNITIONOGNITION & A& AFFECTFFECT
40
32343638
in se
cond
s)
26283032
tchi
ng T
ime
(i
MHINo-MHI
202224
Low Anxiety High Anxiety
Swit
MHI group performed more slowly on a complex
State Anxiety
MHI group performed more slowly on a complex attentional task with lower reports of anxiety and otherwise perform comparably to their no-MHI
Jung & Good (2006)
otherwise perform comparably to their no MHI cohorts when stressed
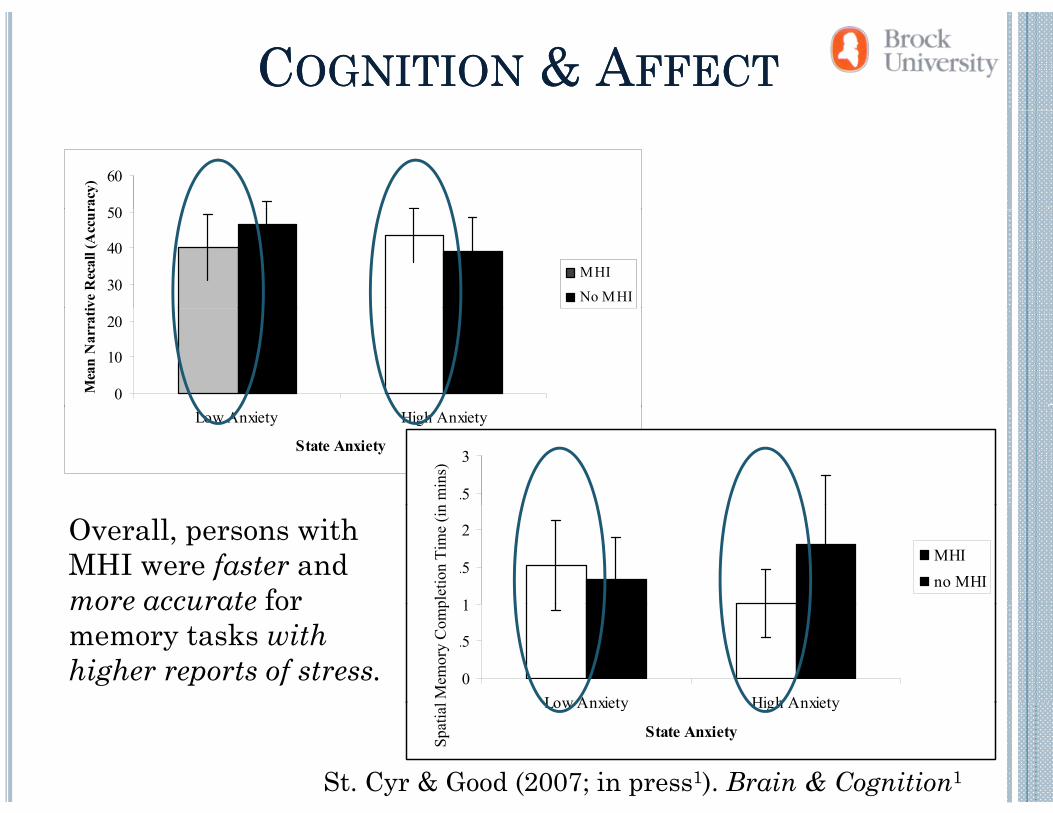
CCOGNITIONOGNITION & A& AFFECTFFECT
50
60
racy
)
30
40
50
ive
Rec
all (
Acc
ur
MHI
No MHI
0
10
20
Mea
n N
arra
ti
Low Anxiety High Anxiety
State Anxiety
2.5
3n
min
s)
Overall, persons with MHI were faster and more accurate for 1
1.5
2
me
(in m
inut
es)
MHIno MHI
plet
ion
Tim
e (in
more accurate for memory tasks with higher reports of stress. 0
0.5
1
Low Anxiety High Anxiety
Tim
Mem
ory
Com
p
St. Cyr & Good (2007; in press1). Brain & Cognition1
Low Anxiety High Anxiety
State AnxietySpat
ial
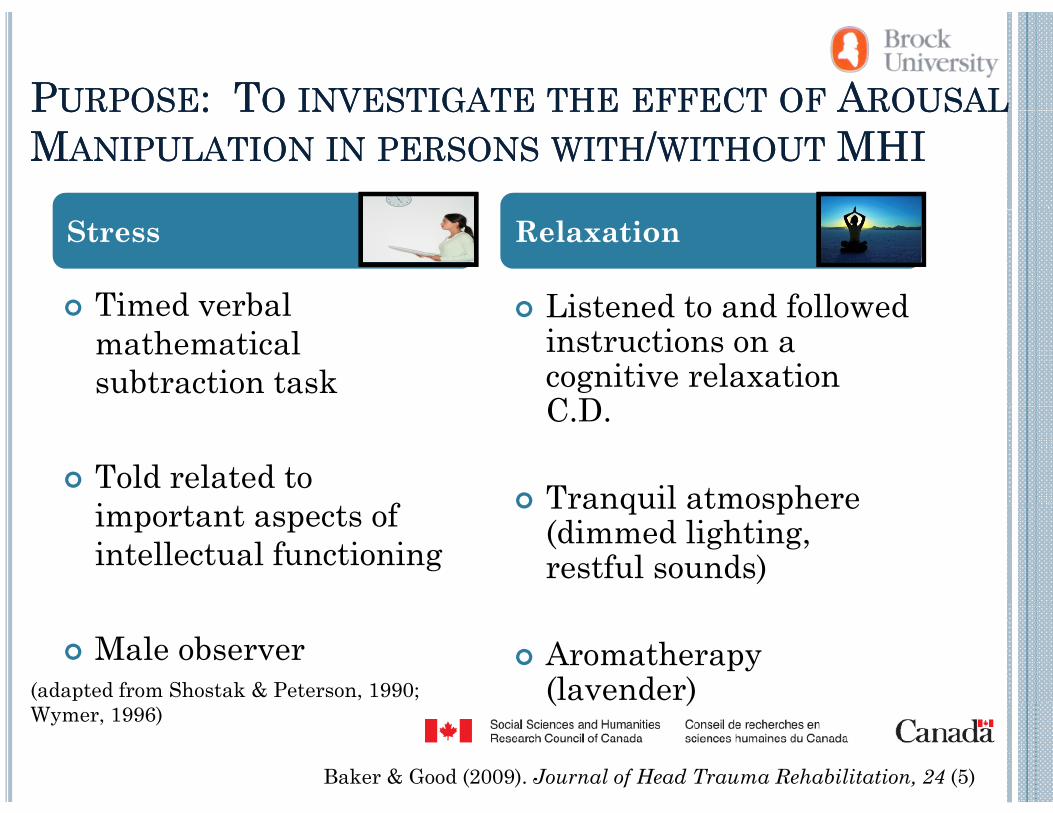
PPURPOSEURPOSE: T: TOO INVESTIGATEINVESTIGATE THETHE EFFECTEFFECT OFOF AAROUSALROUSALPPURPOSEURPOSE: T: TOO INVESTIGATEINVESTIGATE THETHE EFFECTEFFECT OFOF AAROUSALROUSALMMANIPULATIONANIPULATION ININ PERSONSPERSONS WITHWITH//WITHOUTWITHOUT MHIMHI
Timed verbal Listened to and followed
Stress Relaxation
Timed verbal mathematical subtraction task
Listened to and followed instructions on a cognitive relaxation C D
Told related to i f
C.D.
Tranquil atmosphereimportant aspects of intellectual functioning
Tranquil atmosphere (dimmed lighting, restful sounds)
Male observer Aromatherapy (lavender)(adapted from Shostak & Peterson, 1990; ( )
Wymer, 1996)
Baker & Good (2009). Journal of Head Trauma Rehabilitation, 24 (5)
MHI IMHI INDICATORNDICATOR
Questionnaire:QDemographics
Have you ever had a head injury resulting in an altered state of consciousness (including: vomiting, dizziness, seeing stars, confusion)?
MMEASURESEASURESMMEASURESEASURES•• QuestionnairesQuestionnaires •• Arousal State MeasuresArousal State MeasuresQuestionnairesQuestionnaires
• Demographic information
Arousal State MeasuresArousal State Measures
• Electrophysiological Measures re: MHI History (Kay et al., 1993)
• PCSC (Gouvier et al 1992)
• EDA, HR, respiration (sympathetic activation)
PCSC (Gouvier et al., 1992)
• Verbal self-report of arousal state
•• Cognitive MeasuresCognitive Measures
M• Everyday life Stress (adapted
from Holmes & Rahe, 1967)State Trait Anxiety Inventory
• Memory • Planning/abstract
reasoningA i • State-Trait Anxiety Inventory
(Speilberger, 1983)• Attention• Subtests from: WMS-III,
WAIS-III, DKEFS and NEPSY IINEPSY-II
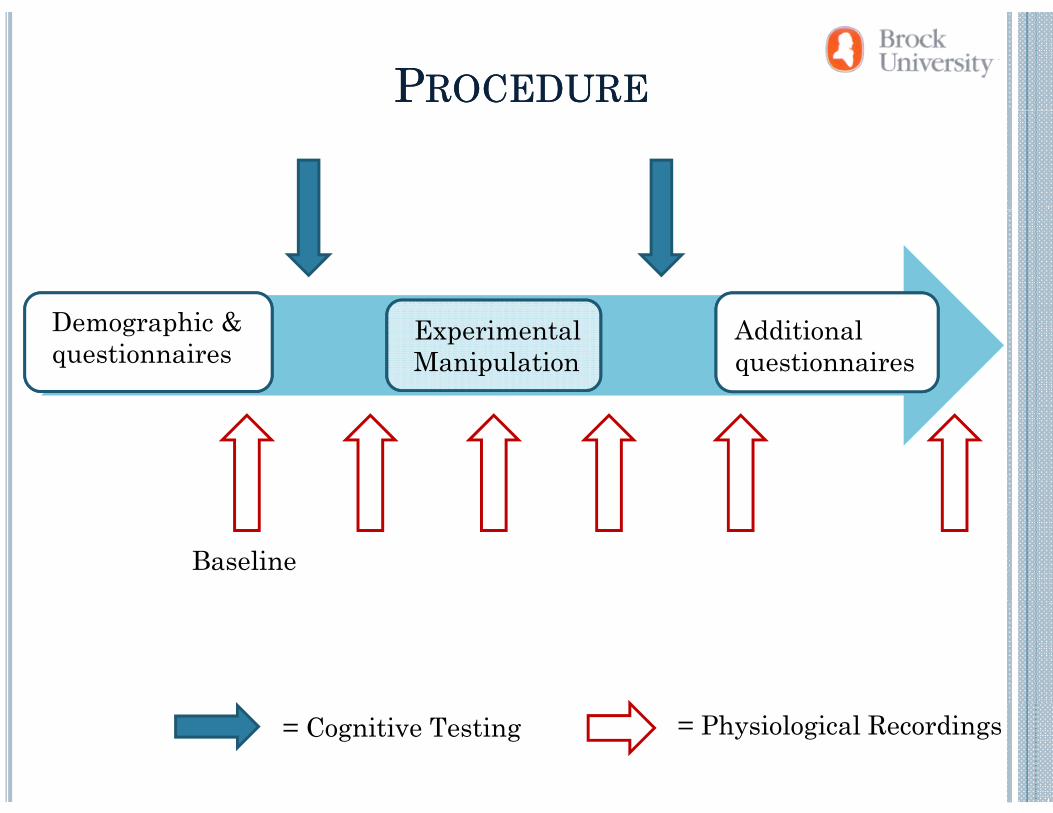
PPROCEDUREROCEDURE
Experimental Manipulation
Demographic & questionnaires
Additional questionnaires
Baseline
= Physiological Recordings= Cognitive Testing
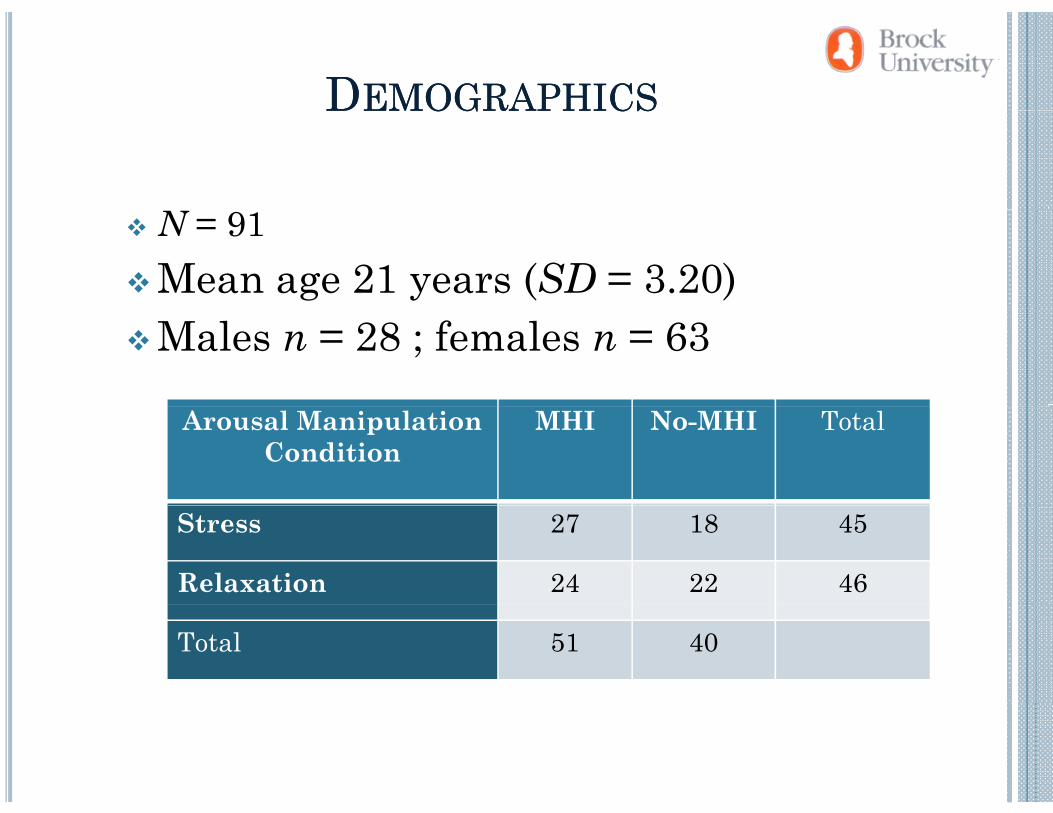
DDEMOGRAPHICSEMOGRAPHICSDDEMOGRAPHICSEMOGRAPHICS
N = 91 Mean age 21 years (SD = 3.20)Males n = 28 ; females n = 63
Arousal Manipulation Condition
MHI No-MHI Total
Stress 27 18 45
Relaxation 24 22 46
Total 51 40
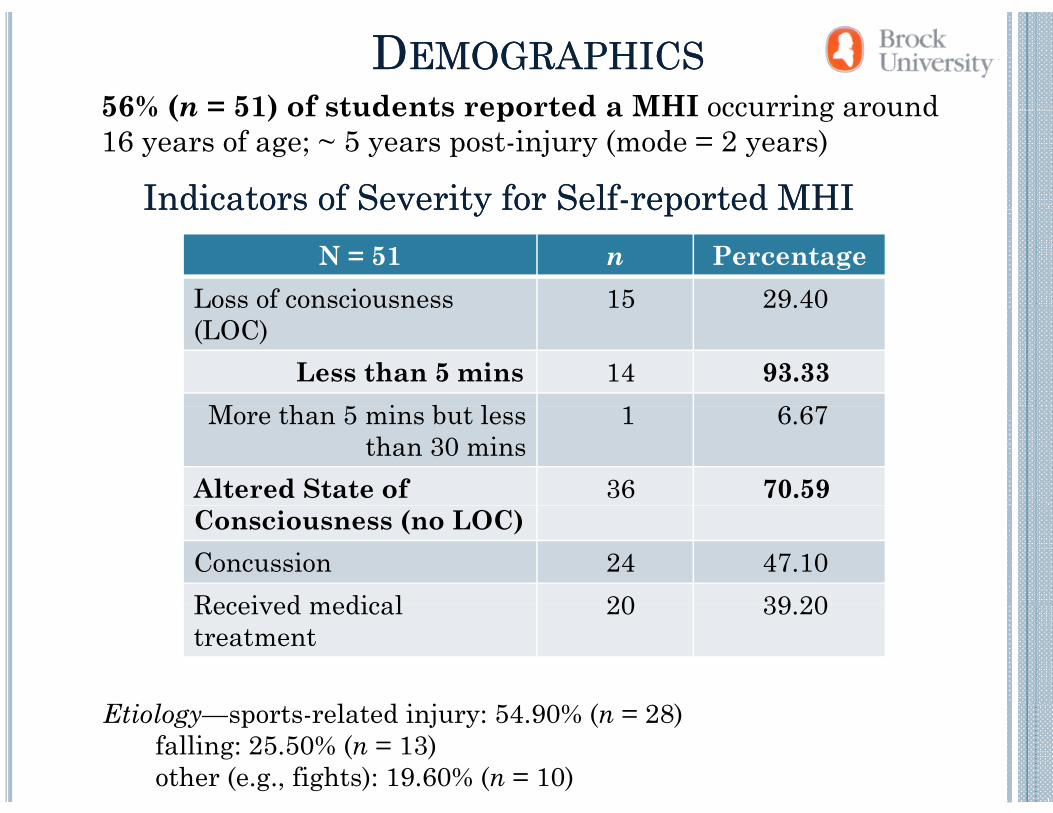
DDEMOGRAPHICSEMOGRAPHICS56% (n = 51) of students reported a MHI occurring around56% (n = 51) of students reported a MHI occurring around 16 years of age; ~ 5 years post-injury (mode = 2 years)
Indicators of Severity for SelfIndicators of Severity for Self--reported MHIreported MHIN = 51 n Percentage
Loss of consciousness 15 29.40
Indicators of Severity for SelfIndicators of Severity for Self reported MHIreported MHI
(LOC)Less than 5 mins 14 93.33
M h 5 i b l 1 6 67More than 5 mins but less than 30 mins
1 6.67
Altered State of 36 70.59Consciousness (no LOC)Concussion 24 47.10Received medical 20 39 20Received medical treatment
20 39.20
Etiology—sports-related injury: 54.90% (n = 28) falling: 25.50% (n = 13)other (e.g., fights): 19.60% (n = 10)
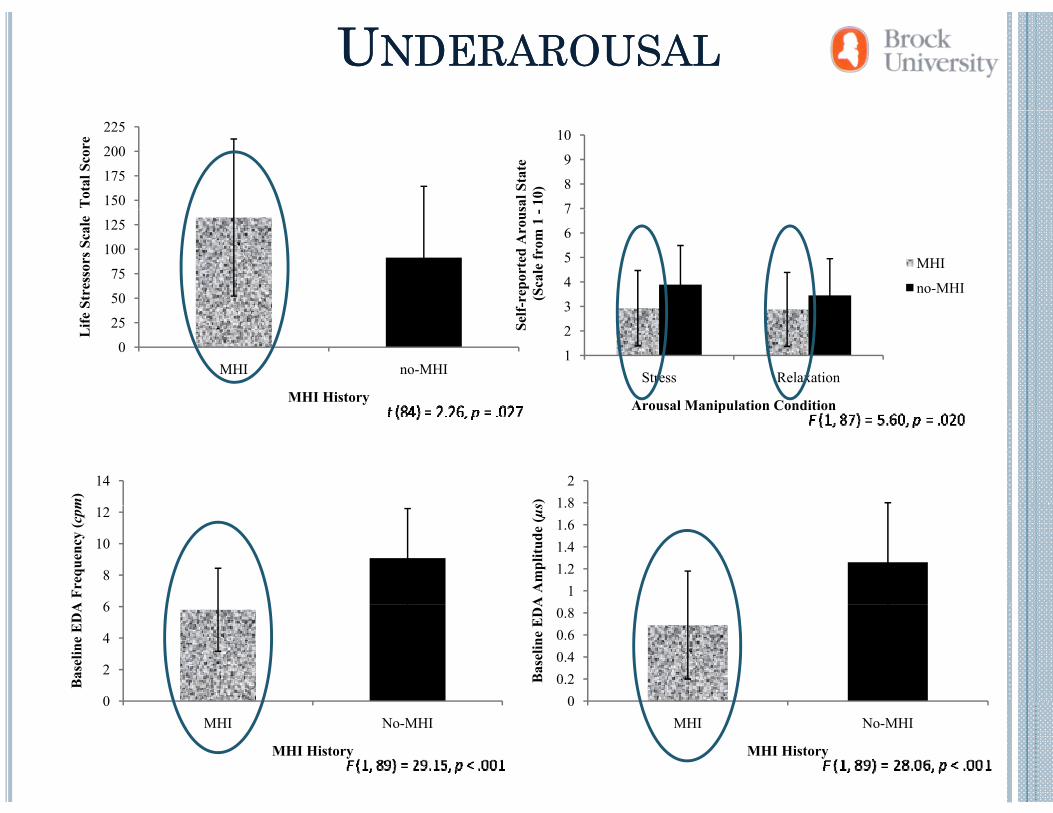
UUNDERAROUSALNDERAROUSAL
7
8
9
10
sal S
tate
10)
150
175
200
225
Tot
al S
core
3
4
5
6
7
f-re
port
ed A
rous
(Sca
le fr
om 1
-
MHI
no-MHI50
75
100
125
Stre
ssor
s Sca
le
1
2
3
Stress Relaxation
Self
Arousal Manipulation Condition
0
25
MHI no-MHI
Life
MHI History Arousal Manipulation Condition
14
m) 1 8
2
s)
6
8
10
12
A F
requ
ency
(cpm
11.21.41.61.8
A A
mpl
itude
(µs
0
2
4
6
Bas
elin
e E
DA
00.20.40.60.8
Bas
elin
e E
DA
0MHI No-MHI
MHI History
0MHI No-MHI
MHI History
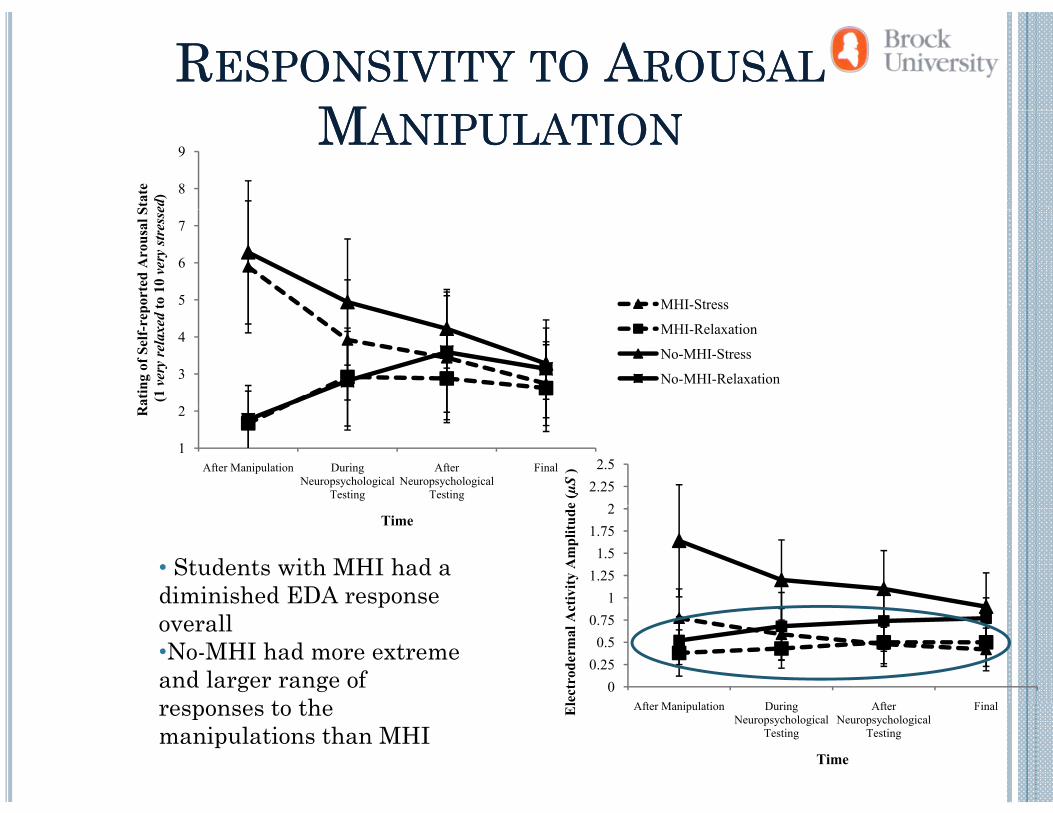
RRESPONSIVITYESPONSIVITY TOTO AAROUSALROUSALMMMMANIPULATIONANIPULATION
8
9St
ate
ed)
5
6
7
port
ed A
rous
al S
to 1
0 ve
rystr
esse
MHI-Stress
2
3
4
Rat
ing
of S
elf-
rep
(1 v
ery
rela
xed
t MHI Stress
MHI-Relaxation
No-MHI-Stress
No-MHI-Relaxation
1
2
After Manipulation During Neuropsychological
Testing
After Neuropsychological
Testing
Final
R
22.25
2.5
e (µ
S)
Time
11.25
1.51.75
2
tivity
Am
plitu
de• Students with MHI had a diminished EDA response
00.25
0.50.75
Af M i l i D i Af Fi llect
rode
rmal
Actp
overall•No-MHI had more extreme and larger range of
t th After Manipulation During Neuropsychological
Testing
After Neuropsychological
Testing
FinalEl
Time
responses to the manipulations than MHI
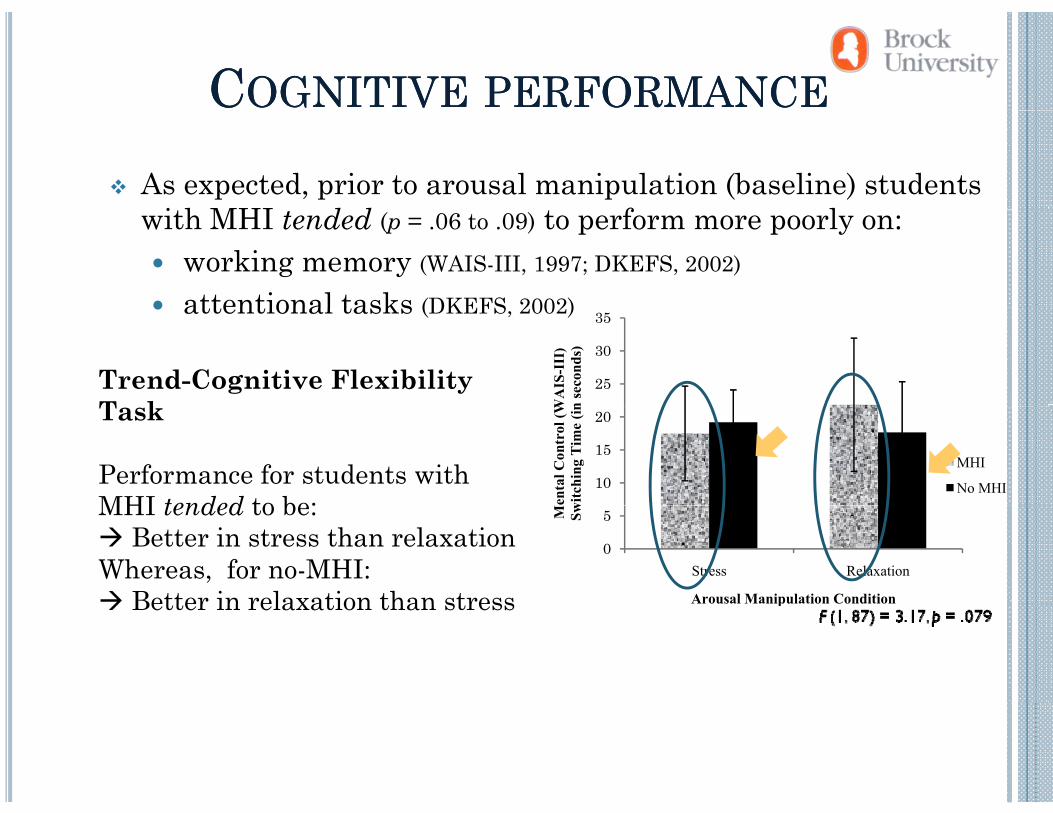
CCOGNITIVEOGNITIVE PERFORMANCEPERFORMANCE
As expected, prior to arousal manipulation (baseline) students i h MHI d d f lwith MHI tended (p = .06 to .09) to perform more poorly on:
working memory (WAIS-III, 1997; DKEFS, 2002)
attentional tasks (DKEFS 2002)attentional tasks (DKEFS, 2002)
25
30
35
WA
IS-I
II)
n se
cond
s)
Trend-Cognitive Flexibility T k
10
15
20
Men
tal C
ontr
ol (W
witc
hing
Tim
e (in
MHI
No MHI
Task
Performance for students with MHI tended to be:
0
5
Stress RelaxationM Sw
Arousal Manipulation Condition
MHI tended to be:Better in stress than relaxation
Whereas, for no-MHI:Better in relaxation than stress pBetter in relaxation than stress
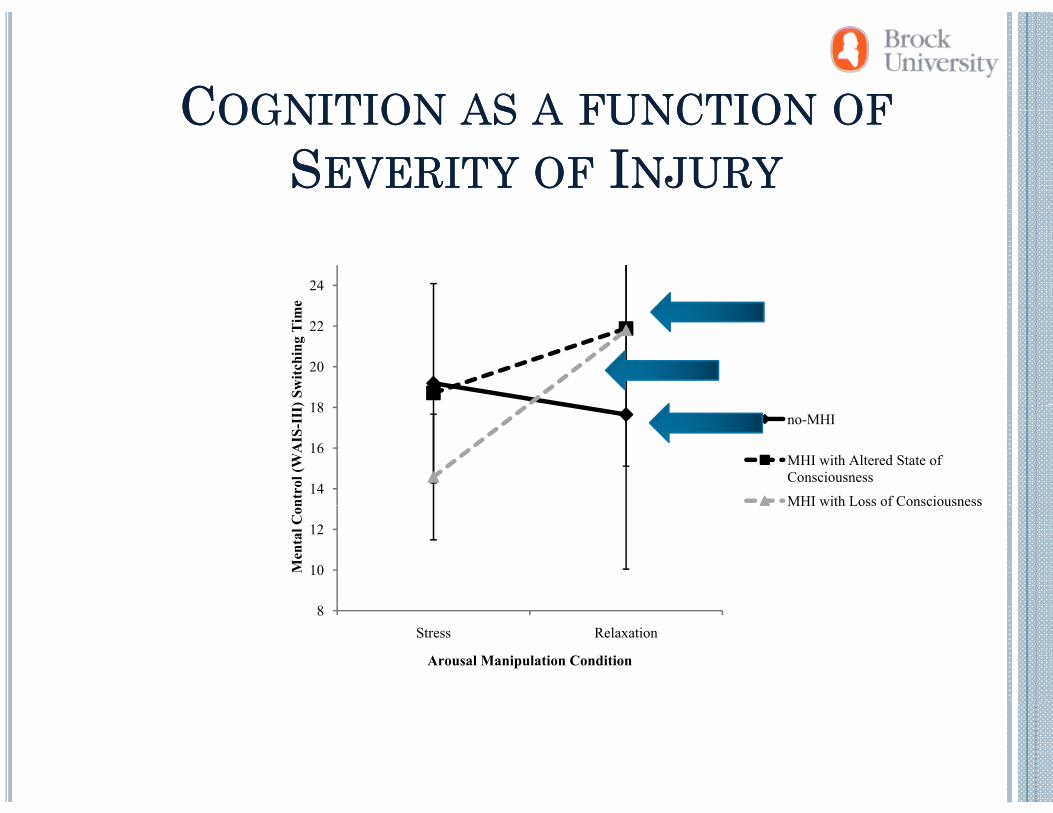
CCOGNITIONOGNITION ASAS AA FUNCTIONFUNCTION OFOFCCOGNITIONOGNITION ASAS AA FUNCTIONFUNCTION OFOFSSEVERITYEVERITY OFOF IINJURYNJURY
24m
e
18
20
22
) Sw
itchi
ng T
im
14
16
18
ntro
l (W
AIS
-III no-MHI
MHI with Altered State of Consciousness
MHI with Loss of Consciousness
10
12
Men
tal C
on MHI with Loss of Consciousness
8Stress Relaxation
Arousal Manipulation Condition
SSUMMARYUMMARY & C& CONCLUSIONSONCLUSIONS
Even individuals with mild head trauma present with a profile similar to that of persons with moderate-to-
TBIsevere TBIunderaroused (emotionally & physiologically)increased reports of life stressorspless responsive to stressors in their environmentadvantaged by increasing their arousal
Suggestive of long-lasting effects of neural disruptionMay indicate subtle disruption to OFC/VMPFC as this y pregion has been implicated in the modulation of autonomic responses (e.g., Tranel & Damasio, 1994)
THANK YOU!
A d Th k ll f h d i h NCR l b!
CONTACTING US…
And Thanks to all of the students in the NCR lab!
Email dawn good@brocku ca (Dr Dawn Good)[email protected] (Dr. Dawn Good)
Website - Neuropsychology Cognitive Research Lab –Website Neuropsychology Cognitive Research Lab Koffler Family Trauma Research Centre in the Lifespan Development Research Institute at Brock U i it ( b k )University (www.brocku.ca)
htt // b k / h/ g iti /i dhttp://www.psyc.brocku.ca/research/neurocognitive/index.html