Prolotherapy for Golfing Injuries and Pain
7
56 Practical PAIN MANAGEMENT, June 2008 ©2008 PPM Communications, Inc. Reprinted with permission. G olf is a very popular sport in the U.S. and many other countries. This is, in part, from the non-con- tact nature of the sport, allowing many different age groups to play, both older and younger participants. Golf is a sport where high performance and skill are not limited by age. 1 Surveys estimate any- where from 28.7 million 2 to 37 million 3 golfers in the U.S. alone, with golfers’ re- ported annual spending estimated at 24 billion dollars per year on equipment and fees. 4 Despite the low impact nature of the sport, several studies over the years have shown that golf has its share of injuries re- sulting in musculoskeletal pain in the am- ateur as well as the professional golfer. 5-9 Prolotherapy is a non-surgical proce- dure which stimulates repair of muscu- loskeletal injuries. This treatment has re- ceived increased attention over the last few years, and made its way into the sports world, as well as The New York Times which reports: “Unlike many drugs and surgery, prolotherapy has minimal side effects when performed by an experi- enced practitioner…” 10 The purpose of this article is to explore common golf in- juries, contributing factors, diagnosis, prevention and non-surgical treatment options with prolotherapy. Prolotherapy Review Prolotherapy is a method of injection treatment designed to stimulate healing. 11 Many different types of musculoskeletal injuries and pain lend themselves to pro- lotherapy treatment including low back and neck pain, chronic sprains and/or strains, whiplash injuries, tennis and golfer’s elbow, knee, ankle, shoulder or other joint pain, chronic tendonitis/ten- donosis, and musculoskeletal pain relat- ed to osteoarthritis. Prolotherapy works by raising growth factor levels or effective- ness in connective tissue ligaments and tendons to promote repair or growth. 12 Prolotherapy lends itself very well to sports injury and pain because most sports related injuries involve ligaments and ten- dons. Prolotherapy can be used years after the initial pain or problem began, as long as the patient is generally healthy. Significant athletic injuries that hinder a person in playing their sport are almost always ligamentous or tendonous in na- ture, not muscular. 13 This is because liga- ment and tendon tissues have a poor blood supply, as opposed to muscles which have a large blood supply and so that they take longer to heal than other tissues—usually four to six weeks. Since the ligaments are the main stabilizing forces in the joints, these are the struc- tures that take the bulk of the forces while the athlete is playing his/her sport. 14 Un- fortunately, incomplete healing is com- mon after injury to those structures. 15,16 In fact, it has been estimated that the usual best result of a completed connective tis- sue repair process is a return to normal connective tissue length, but only 50% to 60% of pre-injury tensile strength. 17 Over time, and multiple injuries, this can result in laxity and connective tissue insufficien- cy. 18 In repetitive trauma, common in golf related injuries, 19 each individual trauma may be insufficient to provide enough stimulus to prompt complete healing, so that even minor injury may be enough to accumulate damage to the point of initi- ating chronic pain. 20 Prolotherapy works by causing a tem- porary, low grade inflammation at the site of ligament or tendon weakness (fibro-os- seous junction) thus “tricking” the body into initialing a new healing cascade. In- flammation activates fibroblasts to the area, which synthesize precursors to ma- ture collagen, and reinforce connective tissue. 21 This inflammatory stimulus rais- es the level of growth factors to resume or initiate a new connective tissue repair se- quence to complete one which was pre- maturely aborted or never started. 22 Pro- lotherapy is also known as “regenerative injection therapy (RIT),” “non-surgical Prolotherapy by Donna Alderman, DO Prolotherapy for Golfing Injuries and Pain An effective non-surgical treatment option for golf-related injuries, including low back pain, lateral and medial epicondylitis, wrist ligament injuries, shoulder injuries, and other musculoskeletal joint pain. FIGURE 1. The 5 phases of the golf swing. 1. takeaway: from address until the club is horizon- tal; 2. backswing: from horizontal to top of backswing; 3. downswing: from top of backswing until the club is horizontal; 4. acceleration: from horizontal club to impact; and 5. follow- through: from ball contact until end of swing.
description
An effective non-surgical treatment option for golf-related injuries, including low back pain, lateral and medial epicondylitis, wrist ligament injuries, shoulder injuries, and other musculoskeletal joint pain.
Transcript of Prolotherapy for Golfing Injuries and Pain

56 Practical PAIN MANAGEMENT, June 2008©2008 PPM Communications, Inc. Reprinted with permission.
Golf is a very popular sport in theU.S. and many other countries.This is, in part, from the non-con-
tact nature of the sport, allowing manydifferent age groups to play, both olderand younger participants. Golf is a sportwhere high performance and skill are notlimited by age.1 Surveys estimate any-where from 28.7 million2 to 37 million3
golfers in the U.S. alone, with golfers’ re-ported annual spending estimated at 24billion dollars per year on equipment andfees.4 Despite the low impact nature of thesport, several studies over the years haveshown that golf has its share of injuries re-sulting in musculoskeletal pain in the am-ateur as well as the professional golfer.5-9
Prolotherapy is a non-surgical proce-dure which stimulates repair of muscu-loskeletal injuries. This treatment has re-ceived increased attention over the lastfew years, and made its way into the sportsworld, as well as The New York Timeswhich reports: “Unlike many drugs andsurgery, prolotherapy has minimal sideeffects when performed by an experi-enced practitioner…”10 The purpose of
this article is to explore common golf in-juries, contributing factors, diagnosis,prevention and non-surgical treatmentoptions with prolotherapy.
Prolotherapy ReviewProlotherapy is a method of injectiontreatment designed to stimulate healing.11
Many different types of musculoskeletalinjuries and pain lend themselves to pro-lotherapy treatment including low backand neck pain, chronic sprains and/orstrains, whiplash injuries, tennis andgolfer’s elbow, knee, ankle, shoulder orother joint pain, chronic tendonitis/ten-donosis, and musculoskeletal pain relat-ed to osteoarthritis. Prolotherapy worksby raising growth factor levels or effective-ness in connective tissue ligaments andtendons to promote repair or growth.12
Prolotherapy lends itself very well tosports injury and pain because most sportsrelated injuries involve ligaments and ten-dons. Prolotherapy can be used years afterthe initial pain or problem began, as longas the patient is generally healthy.
Significant athletic injuries that hinder
a person in playing their sport are almostalways ligamentous or tendonous in na-ture, not muscular.13 This is because liga-ment and tendon tissues have a poorblood supply, as opposed to muscleswhich have a large blood supply and sothat they take longer to heal than othertissues—usually four to six weeks. Sincethe ligaments are the main stabilizingforces in the joints, these are the struc-tures that take the bulk of the forces whilethe athlete is playing his/her sport.14 Un-fortunately, incomplete healing is com-mon after injury to those structures.15,16 Infact, it has been estimated that the usualbest result of a completed connective tis-sue repair process is a return to normalconnective tissue length, but only 50% to60% of pre-injury tensile strength.17 Overtime, and multiple injuries, this can resultin laxity and connective tissue insufficien-cy.18 In repetitive trauma, common in golfrelated injuries,19 each individual traumamay be insufficient to provide enoughstimulus to prompt complete healing, sothat even minor injury may be enough toaccumulate damage to the point of initi-ating chronic pain.20
Prolotherapy works by causing a tem-porary, low grade inflammation at the siteof ligament or tendon weakness (fibro-os-seous junction) thus “tricking” the bodyinto initialing a new healing cascade. In-flammation activates fibroblasts to thearea, which synthesize precursors to ma-ture collagen, and reinforce connectivetissue.21 This inflammatory stimulus rais-es the level of growth factors to resume orinitiate a new connective tissue repair se-quence to complete one which was pre-maturely aborted or never started.22 Pro-lotherapy is also known as “regenerativeinjection therapy (RIT),” “non-surgical
Prolotherapy
by Donna Alderman, DO
Prolotherapy for Golfing Injuries and PainAn effective non-surgical treatment option for golf-related injuries, includinglow back pain, lateral and medial epicondylitis, wrist ligament injuries,shoulder injuries, and other musculoskeletal joint pain.
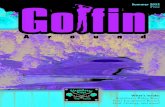
FIGURE 1. The 5 phases of the golf swing. 1. takeaway: from address until the club is horizon-tal; 2. backswing: from horizontal to top of backswing; 3. downswing: from top of backswinguntil the club is horizontal; 4. acceleration: from horizontal club to impact; and 5. follow-through: from ball contact until end of swing.

P r o l o t h e r a p y
tendon, ligament and joint reconstruc-tion” and “growth factor stimulation in-jection therapy.” “Sclerotherapy” is anolder, inaccurate term for prolotherapy,based on the original theory that scar for-mation was the treatment mechanism.However biopsy studies have not demon-strated scar formation with prolotherapyagents currently in use.23 Rather, studieshave shown a proliferation of new, nor-mal, thicker and stronger connective tis-sue after Prolotherapy injections (thus“prolo” for proliferation).24 A typicalcourse is four to six treatments, spacedfrom two to six weeks apart.
Common Injuries in the Amateur andProfessional GolferThe most common injury reported by theamateur and professional golfer alike is inthe low back/lumbar spine/sacroiliac re-gion pain.25-28 This makes sense when look-ing at the powerful rotation and extensionmotion in the golf swing.29 In the profes-sional golfer, the second most commonlyinjured area is the wrist or hand, followedby the shoulder.30,31 For the amateur, thesecond most commonly injured area is theelbow, followed by the wrist or hand, andthen the shoulder.32,33 Overuse is a largecomponent of injury both in the profes-sional and the amateur golfer and, moreoften, the cause of injury than direct trau-ma.34 One study reports 82.6% of all re-ported injuries involve overuse, with morethan 90% of low back injuries attributedto overuse. Only 17.4% of injuries report-ed in that study were attributed to singletrauma events.35 Another report foundthat professional golfers’ injuries oc-
curred primarily from overuse duringpractice (68%) with only 7% during com-petition.36 Wrist injuries occur most com-monly in the lead wrist (left wrist in righthanded golfers). This is also true of shoul-der injuries where 90% of shoulder injuryinvolve the lead shoulder.37,38
The Golf Swing In order to correctly analyze golf injuries,it is important to understand the compo-nents of the golf swing itself. Golfers maygive a history of symptoms that occur onlyduring one specific phase of the swing andan understanding of the swing componentswill help in diagnosis.39 Problems with swingmechanics have been blamed for many ofthe injuries seen in golf,40 especially lowback pain41 and shoulder injuries.42 Theswing requires a coordinated and synchro-nized effort of muscle strength, timing andcoordination on the part of the golfer togenerate clubhead speeds often over 100mph.43 It is no wonder then that many in-juries are reported to occur during the golfswing, most commonly at ball impact, aswell as follow-through and the backswing44,45
(see Figure 1).
Contributing FactorsSince overuse is a large factor in golf in-juries, there is a correlation between play-ing and practice time and injury, with sig-nificantly more injuries in golfers whoplay four or more rounds a week and hitat least 200 balls in one week. Since pro-fessionals spend more time doing boththese activities, it is not a surprise that pro-fessional golfers suffer more injuries thanamateurs despite having a better swing
technique.46 It has also been found thatgolfers who carry their bag on a regularbasis suffer significantly more injuries tothe low back, shoulder, and ankle.47 Thereis also a correlation between stretchingand warming up and injury. Amateurgolfers who warmed up for at least 10 min-utes were found to have less injuries thanthose amateurs that did not warm up priorto practice or play.48 However, eventhough professional golfers routinelystretch, they also spend so much moretime playing that the positive impact ofstretching did not appear to be as muchof a factor as with amateurs.49
Low Back PainAs noted above, low back injuries accountfor the highest percentage of reportedgolfing injuries. The most obvious con-tributing factor for low back injury is poorswing technique and mechanics. This ismore often a problem in the amateurgolfer.50 This is because these golfers tendto have erratic muscle control and do notduplicate the swing with each shot, versusprofessionals who tend to consistently ac-tivate the same muscles each time theyswing.51 Hyperextending the back duringfollow-through is a common problem inamateurs and can result in a low back/sacroiliac ligament injury52 (see Figure 2).Superior swing mechanics in the profes-sional golfer result in increased powergeneration from hips and legs with lessstress on the low back53 (see Figure 3). Pro-lotherapy is very effective in treating lowback pain, sacroiliac injury, sciatica, andeven disc disease because weakening ofthe spinal ligaments precedes disc herni-
FIGURE 2. The golf swing causing injury tothe low back in follow-through.
57Practical PAIN MANAGEMENT, June 2008©2008 PPM Communications, Inc. Reprinted with permission.
FIGURE 3. The golf swing with correct mechanics in follow-through.

P r o l o t h e r a p y
58 Practical PAIN MANAGEMENT, June 2008©2008 PPM Communications, Inc. Reprinted with permission.
ations.54 For a disc to herniate, there mustfirst be a primary ligament weakness anda deteriorating disc.55 While disc problemshave gotten much of the credit for lowback pain, ligament injury is a more im-portant source of back pain.56 In fact, ithas been reported that only 4 percent oflow back pain is due to a herniated disc.57
Prolotherapy strengthens the ligamen-tous tissue around the disc, thus stabiliz-ing and supporting that region. Pro-lotherapy is also very effective for sacroil-iac ligament strain and sciatica (leg paincoming from the back). In fact, it has beenstated that ligament laxity in the sacroili-ac joint is the number one reason for sci-atica and is one of the most common rea-sons for chronic low back pain.58
Elbow Injuries Medial elbow pain, known as medial epi-condylitis, has historically been referred toas “golfers elbow.” However, lateral elbow
pain was found to be more common in theamateur golfer by a 5:1 ratio by one inves-tigator.59 Other investigators found the oc-currence to be equal.60 Both medial andlateral elbow pain is thought to occur as aresult of poor swing mechanics, and aremuch more common in amateurs, withone study showing 25% of amateurs and4% of professionals complaining of thisproblem.61 Medial injuries are thought tooccur as a result of hitting shots “fat” (hit-ting the ground first), or sudden impactloading such as can occur by taking repet-itive strokes that leave large divots.62 Lat-eral injury occurs with over-swinging withthe right hand (in right handed golfers),and repetitive forceful extension of theforearm accompanied by a twisting mo-tion, especially if associated with excessivegripping of the golf club.63 Both of theseproblems increase with age and frequencyof play.64 There are ligamentous and tendi-nous complexes on both the medial and
lateral aspects of theelbow. The medial as-pect of the elbow is sta-bilized by the ulnarcollateral ligament,while the lateral side isstabilized by the radi-al collateral and annu-al ligaments (see Fig-ure 4). The extensortendons attach at thelateral epicondylewhile the flexor ten-dons attach medially.Prolotherapy is an ef-fective treatment forthese ligamentous andtendonous injuries, as
long as there is not a complete rupturepresent. In the case of a complete rupture,surgery may be needed, however this ismuch less common than tendonitis, ten-donosis, or ligamentous sprain.
Shoulder InjuriesThe shoulder is another common area ofinjury for the golfer, with the lead shoul-der (left shoulder in the right handedgolfer) particularly vulnerable to injury.65
Understanding the biomechanics of thegolf swing is especially helpful in diagno-sis of shoulder injuries and sometimesmodifications to the swing can be helpfulin preventing further injury.66 Symptomsof shoulder pain or instability usuallyoccur at the extreme of range of motion(top of backswing or end of follow-through). Those with rotator cuff diseasemay display weakness during initial take-away, leading to poor swing mechanics.Rotator cuff disease and subacromial im-pingement involving the lead shoulderare among the most common problems ingolfers.67 Acromioclavicular joint diseaseis another common problem affecting thispopulation. With acromiclavicular prob-lems, symptoms will usually be experi-enced at the top of the backswing.68
Glenohumeral Instability. The gleno-humeral ligament is a stabilizing ligamentof the anterior portion of the shoulderand is important in the overhead portionof the golf swing. Injury to this ligament—specifically the superior band—predis-poses the shoulder to instability.69 In orderto generate power during the swing,golfers attempt to maximize their shoul-der turn relative to their hip turn.70 Un-fortunately this degree of shoulder rota-tion done repetitively can create micro-trauma on capsular and labral structures,affecting the glenohumeral joint liga-ments, and creating laxity and instabili-ty.71 The patient will complain of pain andinstability at the top of the backswing.
Instability of the glenohumeral liga-ment then leads to rotator cuff injury andsubsequent impingement syndrome72 (seeFigure 5). A simple test for early impinge-ment syndrome is the “Hauser ThumbsDown” test.73 The person holds their armsat 90 degrees to the body with the thumbspointed down to the ground for 2 min-utes. A sensation of a definite weakeningor pain in the shoulder is a positive sign(see Figure 6). A positive test means thatprolotherapy should be considered to cor-rect existing weakness and prevent further
FIGURE 4. Ligaments and tendons of theelbow. Force exerted on the elbow can injureligamentous or tendonous structures.
FIGURE 5. Glenohumeral ligament instabilityleading to impingement syndrome.
FIGURE 6. Hauser Thumbs-Down Test: A person with earlyimpingement of the rotator cuff will not be able to hold this positionwithout experiencing shoulder pain and weakness.

damage to the glenoid labrum.74
SLAP Lesions Biceps Tendonitis/Ten-donosis. Superior labral (SLAP) lesionsalso occur in golfers. These patients com-plain of pain affecting the lead shoulderduring the end of the backswing or begin-ning of the downswing. Sometimes thereare complaints of clicking or catching orsubjective weakness at ball contact duringthe swing. For isolated biceps tendonitis/tendonosis, anterior shoulder pain is mostmarked during the latter part of the fol-low-through phase.75 No definitive studieshave been done on prolotherapy andSLAP lesions, although some clinical ex-perience has demonstrated improvementwith prolotherapy treatment (see Case Re-port 3). Bicipital tendonitis/ tendonosislends itself well to prolotherapy treatmentand this should be tried prior to surgeryunless there is a rupture or detachmentrequiring surgery.
Transverse Humeral Ligament. Oftenforgotten is the small but important trans-verse humeral ligament (THL). The THLis a small ligament holding the long headof the biceps tendon in its groove. It is de-scribed in Gray’s Anatomy as: “a broadband of fibrous tissue passing from thelesser [tuberosity] to the greater tuberos-ity of the humerus, which maintains theposition of the tendon of the long headof the biceps within the bicipital groove”(see Figure 7). With repetitive use and ortrauma, the THL may become stretchedand lax, causing excessive biceps tendonmotion.76 The patient will complain of atwinge-like feeling anteriorly and painduring motions that use the biceps, such
as anterior pain during portions of thegolf swing. Prolotherapy is very effectivein stimulating the repair of this small lig-ament, stabilizing the biceps tendon, andresolving pain.
Adhesive Capsulitis. Adhesive capsuli-tis (frozen shoulder) is another shoulderpresentation that may occur when thegolfer has suffered an injury, then limitedshoulder motion afterwards. This can beparticularly troublesome if it has ad-vanced. However, if caught early, aggres-sive physical therapy to break the adhe-sions and restore range of motion, fol-lowed by prolotherapy on a subsequentvisit for the underlying injured tendon, iseffective. Initially, local anesthetic to theshoulder joint can be used in the officeand manipulation/stretching of the jointdone there to start the process of break-ing the adhesions.77,78 Exercises based onosteopathic muscle energy technique forthis purpose can also be helpful (see Fig-
ure 8). The patient should be instructedto do these exercises two to three timesdaily, and should also be sent for aggres-sive physical therapy to continue mobi-lization of the joint where possible. Fol-lowup visits include reevaluation of rangeof motion, and continued prolotherapytreatments to the underlying injury, withmany patients resolving within the typicalfour to six treatment average.
Wrist and Hand InjuriesThe wrist is a sea of ligaments (see Figure9). These ligaments are injured most typi-cally by hyperextension of the wrist duringthe golf swing and occur most commonlyin the left (leading) wrist or hand. Stabili-ty of the wrist is dependent on the stabili-ty of the wrist ligaments. Overuse or poorwrist control during the swing can cause ex-cessive joint movement leading to wrist lig-ament injury.79 Wrist ligamentous injuriescan be successfully treated with prolother-
P r o l o t h e r a p y
60 Practical PAIN MANAGEMENT, June 2008©2008 PPM Communications, Inc. Reprinted with permission.
Shoulder Range of Motion Exercises
Two people are needed to do this exercise.1. The helper stands to side of the patient and supports the patient’s
arm, which is placed straight ahead. 2. The Helper holds the patient’s arm while the Patient pushes down,
counting to 5 and the Helper supports and resists the motion. 3. Then the Helper lifts the patient’s arm up a little and repeats. 4. Keep going as high as possible.
FIGURE 7. Transverse humeral ligament. Thissmall but important ligament stabilizes theposition of the tendon of the long head of thebiceps within the bicipital groove.
FIGURE 8. Shoulder range of motion exercises.

P r o l o t h e r a p y
61Practical PAIN MANAGEMENT, June 2008©2008 PPM Communications, Inc. Reprinted with permission.
apy. Common areas treated with prolother-apy include the distal radioulnar joint, dor-sal intercarpal ligaments, and ulnar collat-eral ligaments (see Figures 10-12).
Unusual Causes of Wrist or HandPain. While fractures are uncommon, thephysician should consider the possibilityof a hamate fracture (the bone behind thering and little finger) as these type of frac-tures are a golfing specialty.80 Often over-looked, damage to the hook of the hamateis caused by a direct blow from the han-dle of the golf club during a “fat shot” (hit-ting the ground). Patients complain ofvague, deep-seated pain or weak grip.There is local tenderness and pain to re-sisted flexion of the little finger. A carpaltunnel X-ray view or a CT scan is neces-sary to show the fracture radiographical-ly81 and should be ordered if there is a sus-picion of this injury. Surgery is needed toremove the hook bone fragment. To pre-vent these types of fractures, the butt ofthe club should be of appropriate size andlength, extending beyond the palm of theleading hand.82
Clinical EvaluationAs with any physical evaluation, a thor-ough and careful history and exam of thegolfing injury are important in making anaccurate diagnosis. Having the golfer ex-plain during which phase of the swing thesymptoms are worst can be helpful in di-agnosis.83 For example, with shoulder in-juries, pain during the backswing can ex-acerbate subacromial impingement oracromioclavicular issues because of thepositioning of the leading arm (internal-ly rotated, forward flexed and abducted).If pain occurs during the follow-through
where the leading arm is abducted and ex-ternally rotated, a diagnosis of anterior in-stability or biceps tendonitis/osis is sup-ported.84 Before a diagnosis is made, stan-dard orthopedic testing should be done,along with a thorough history of the in-jury, exacerbating or mitigating factors,and review of previous treatments andsuccess of those treatments.
MRI’sMRI’s may sometimes be useful but, as dis-cussed in previous articles, may also bemisleading in diagnosing musculoskeletalpain. As many pain practitioners know, anMRI may show nothing wrong and yet thepatient is still in pain. And, because MRI’smay also show abnormalities not relatedto the patient’s current pain complaint,these MRI findings should always be cor-related to the individual patient’s presen-tation. Many studies have documented thefact that abnormal MRI findings exist inlarge groups of pain-free individuals.85-91 Astudy published in the New England Jour-nal of Medicine showed that out of 98pain-free people, 64% had abnormal backscans.92 Many other studies have alsoshown abnormal neck MRI scans inasymptomatic subjects.93,94 A study of eliteathletes performing repetitive overheadactivity also demonstrates this point. Atthe study’s start, none of the athletes hadany shoulder pain or problems. Yet onMRI, 40% showed partial or full thicknesstears of the rotator cuff, and 20% showedother abnormalities. After five years, noneof the athletes interviewed had any com-plaints or had had any evaluation or treat-ment for shoulder-related problems dur-ing the previous five years. The conclusion
of the study was that an MRI alone shouldnot be used for diagnosis.95
ConclusionProlotherapy is an effective non-surgicaltreatment option for golf related injuries,including low back pain, lateral and me-dial epicondylitis, wrist ligament injuries,shoulder injuries as well as other muscu-loskeletal joint pain. Because many golfrelated injuries are a result of repetitivestrain—where incomplete healing has oc-curred—prolotherapy makes even moresense as a treatment modality to stimulateconnective tissue repair. Prolotherapyshould only be done by a practitioner
Figure 9. Anatomy of the Wrist. A “Sea of Ligaments.”
FIGURE 10. Prolotherapy injection of the dis-tal radioulnar joint.
FIGURE 11. Prolotherapy injection of the dor-sal intercarpal ligaments
FIGURE 12. Prolotherapy injection of theulnar collateral ligament.

P r o l o t h e r a p y
62 Practical PAIN MANAGEMENT, June 2008©2008 PPM Communications, Inc. Reprinted with permission.
CASE REPORT 148-year-old male complaining of low back and neck pain.He is an avid golfer and has been playing a lot recently. Hisback pain has been an issue over the years and tends tocome and go, with occasional flares. The last low back flareoccurred while playing golf while “hardly bent over and thenstarted to have extreme pain” in this low back. The pain haspersisted. Regarding his neck, he was dragging his golfclubs recently and felt his hand tingling with right-sidedneck and trapezius pain. An MRI of this cervical spineshowed a ruptured disc. The neck tingling has gotten a littlebetter but he is still bothered by neck pain and stiffness. Past Medical History (PMH): No surgeries, no major ill-
nesses.Review of Systems (ROS): No other complaints.Medications: Levothryoxine, Vitorin, NiaspanExam: Vital signs: Temp 98.0, Blood pressure: 124/70,
Height 6’1”, Weight 214, Pulse 66, Pulse oximetry 97% O2.Gait antalgic, lumbar forward flexion 80 degrees, extension10 degrees. Straight leg raising negative bilaterally. Tenderto palpation at PSIA, ilillumbar and sacroiliac ligaments bi-laterally. Cervical ranged of motion: right 50 degrees, left40 degrees, restricted extension, flexion within normal lim-its, ear to shoulder 20 degrees bilaterally. Tenderness ofcervical interspinous ligaments. Negative for muscularweakness or neurological signs in arms bilaterally.
Findings: Degenerative disc disease lumbar and cervicalspine; lumbosacral sprain-strain, chronic; cervicothoraicsprain-strain, chronic.
Treatment and Outcome: The patient underwent a courseof prolotherapy treatments, first to the lumbosacral spine,then to the cerviothoraic spine. After 4 treatments to thelumbosacral spine and sacro-iliac ligaments, the patientreports 95% improvement and is back to golfing. After 3treatments to the cerviothoraic spine the patient reports95% improvement. Motion testing shows increase in bothlumbar and cervical range of motion.
CASE REPORT 260-year-old left-handed male complaining of right shoulderpain on and off for the past five years. He has been a golferfor many years, however he first noticed the pain while tak-ing luggage off a train and also during weight training. In thepast, his shoulder pain would go away but this time it haspersisted. It has exacerbated to the point of waking him upat night and he has begun to feel it while playing golf duringthe follow-through phase of his swing.PMH: No major illnesses or surgeries.ROS: No other complaints.Medications: None.Exam: Vital signs: Temp 98.4, Blood pressure 100/60;
height 5’8-3/4; weight 184; pulse 76; pulse oximetry 96%.Right shoulder abduction to 150 degrees and slightly“sticky”. Postive active compression test at 0 and 30 (bi-ceps and rotator cuff). Tenderness to palpation atsupraspinatous anteriorly and at transverse humeral liga-ment. No xrays or MRI’s to review.
Findings: (1) Rotator cuff tendonitis/tendonosis with devel-oping adhesive capsulitis; and (2) sprain of transversehumeral ligament.
Treatment and Outcome: Patient began prolotherapy treat-ment to right shoulder. He was also educated on shoulderexercises to increase range of motion and advised to dothem three times daily. After three prolotherapy treatmentshe reports 90% improvement, and no pain while golfing.Range of motion was tested and back to abduction of 180degrees.
CASE REPORT 3(Note: this patient is not a golfer but noted here because ofSLAP lesion improvement after treatment.)
62-year-old male complaining of left shoulder pain, aggra-vated after a fall. Pain was so severe at one point he couldhardly move the shoulder and it became frozen. He hasbeen undergoing physical therapy and improved his rangeof motion by 80%, but still feels some restriction, and alsocontinual pain in the shoulder which he describes as beinglike “a toothache.” He has seen several other physicians in-cluding a neurologist and orthopedic surgeon. Neck originwas considered but ruled out. Patient complains of severelimitations of activities of daily living secondary to pain andrestricted range of motion in this shoulder.PMH: No surgeries, elevated cholesterol controlled with
diet, no major illneses.ROS: No other complaints.Exam: Vital signs: Temp 97.8, Blood Pressure 108/64,
Height 6’3”, Weight 188, Pulse 89, Pulse oximetry 98%O2. Left shoulder exam shows abduction 160 degrees.Positive active compression test (biceps positive). Tender-ness at ACJ. Apley scratch restricted at upper pole. Re-striction with internal rotation.
MRI of left shoulder: (1) No rotator cuff tear; (2) Slap le-sion; (3) Downsloping acromion, type 3; (4) Arthrosis ofthe acromioclavicular joint; (5) Impingement; (6) Anteriorrotator interval capsulitis and sprain; (7) Anterior and pos-terior capsulitis and sprain; (8) Fluid in the shoulder joint;(9) Fluid in the subscapularis bursa; (10) 2mm cyst vs.varicose vein of the glenoid notch; (11) Two 2mm cysts inthe humeral head which are considered to be benign sim-ple cysts.
Findings: (1) Left shoulder adhesive capsulitis, resolvingwith physical therapy; (2) Bicipital/rotator cufftendonitis/tendinosis; (3) SLAP lesion; and (4) Degenera-tive joint disease left shoulder.
Treatment and Outcome: The patient continued with hiscourse of physical therapy and concurrently underwent acourse of prolotherapy treatments. After 5 prolotheapytreatments, he reports restoration of range of motion, nopain, and overall rates his improvement at 95%. Range ofmotion was tested and found to be normal. MRI was sub-sequently repeated and as follows:
Followup MRI: Normal signal intensity and size of supra-spinatous muscle and tendon. Infraspinatus, subscapu-laris and teres minor muscles reveal no tear or sprain.There is no subacromial or subdeltoid buras effusion andsuperior and inferior glenoid labrum are instact. Thehumeral head is smooth but there is type 3 acromioclavic-ular joint spurring causing mild acute supraspinatousmuscle impingement; no tear or additional abnormalities.
CASE REPORTS

P r o l o t h e r a p y
64 Practical PAIN MANAGEMENT, June 2008©2008 PPM Communications, Inc. Reprinted with permission.
64
trained in the procedure and any physi-cian interested in learning the procedureshould seek out appropriate instruction.Otherwise, the practitioner should referto a physician thoroughly trained in theprocedure. Prolotherapy can be a very ef-fective option for the golfer who wants toplay at peak levels unencumbered by mus-culoskeletal pain. n
Donna Alderman, DO is a graduate of West-ern University of Health Sciences, College ofOsteopathic Medicine of the Pacific, inPomona, California, with undergraduate de-gree from Cornell University in Ithaca, NY. Shehas extensive training in Prolotherapy and hasbeen using Prolotherapy in her practice for tenyears. Dr. Alderman is the Medical Director ofHemwall Family Medical Centers in Califor-nia and can be reached through her websitewww.prolotherapy.com. In 2008, she authoredthe book Free Yourself from Chronic Pain andSports Injuries (ISBN 9780981524207)published by Family Doctor Press, Glendale,California, available at familydoctorpress.com
References1. Kim D, Millett P, Warner J, and Jobe F. Shoulder In-juries in Golf. Am J Sports Med. 2004. 32(5):1324.2. National Golf Foundation. 2007 study.www.ngf.org/cgi/faqa.asp. Accessed 6/9/08.3. Beckwith R. The Golf 20/20 Industry Report for2001. Saint Augustine, Fla. World Golf Foundation.2002.4. National Golf Foundation commonly asked ques-tions. www.ngf.org/cgi/faqa.asp. Accessed 6/9/08.5. Batt ME. Golfing injuries: An overview. Sports Med.1993. 16:64.6. McHardy A, Pollard H, and Luo K. One-Year Fol-low-up Study on Golf Injuries in Australian AmateurGolfers. Am J Sports Med. 2007. 35(8):1354.7. Ibid. ref 1.8. Stockard A. Elbow Injuries in Golf. JAOA. 2001.101(9):509.9. Gosheger G, Liem D, Ludwig K, et al. Injuries andOveruse Syndromes in Golf. Am J Sports Med. 2003.31(3):438.10. Brody J. Injections to Kick-Start Tissue Repair.The New York Times. August 7, 2007. Personal HealthSection, p D8. 11. Hackett GS, Hemwall GA, and Montgomery GA.Ligament and Tendon Relaxation Treated by Prolother-apy. (1956 First Edition Charles C. Thomas, Publish-er), Fifth Edition Gustav A. Hemwall. Institute in BasicLife Principles. Oak Brook, IL. 1991.12. Reeves KD. Prolotherapy: Basic Science, ClinicalStudies, and Technique. In Lennard TA (Ed) Pain Pro-cedures in Clinical Practice, 2nd Ed. Hanley and Bel-fus. Philadelphia. 2000. pp 172-190.13. Hauser R and Hauser M. Prolo Your Sports In-juries Away. Beulah Land Press. Oak Park, IL. 2001. p741.14. Ibid. ref 13.15. Ibid. ref 13.16. Browner B. Skeletal Trauma, Volume 1. WB Saun-ders. Philadelphia, PA. 1992:87-88.17. Andriacchi T, Sabiston P, DeHaven K, et al. Liga-ment: Injury and Repair. Acta Rheum Scand. 1956.2:109-116.
18. Ibid. ref 12.19. Ibid. ref 9.20. Ibid. ref 9.21. Ibid. ref 9.22. Ibid. ref 12.23. Ibid. ref 12.24. Reeves KD. Prolotherapy: Present and Future Ap-plications in Soft-Tissue Pain and Disability. InjectionTechniques: Principles and Practice. Physical Medi-cine and Rehabilitation Clinics of North America. No-vember. 1995. (6)4:917-923.25. Ibid. ref 9.26. Ibid. ref 6.27. McHardy, A. and Pollard, H. Lower Back Pain inGolfers: a Review of the Literature. J Chiro Med.2005. Vol 4(3):135. 28. Ibid. ref 13.29. American Orthopaedic Society for Sports Medi-cine Sports Tips. Golf Injuries. 2008. 30. Ibid. ref 9.31. McCarroll JR and Gloe TG. Professional golfersand the price they pay. Phys Sportsmed. 1982.10:54.32. McCarroll JR. The frequency of golf injuries. ClinSports Med. 1996. 15:1.33. Theriault G and Lachance P. Golf injuries: anoverview. Sports Med. 1998. 26:43.34. Wadsworth LT. When golf hurts: musculoskeleltalproblems common to golfers. Curr Sports Med Rep.Dec 2007. 6(6):362.35. Ibid. ref 9.36. Ibid. ref 5.37. Mallon WJ. Golf. In: Hawkins RJ and MisamoreGW, eds. Shoulder Injuries in the Athlete: Surgical Re-pair and Rehabilitation. Churchill Livingstone. NewYork. 1996.38. Pink M, Jobe FW, and Perry J. Electromyographicanalysis of the shoulder during the golf swing. Am JSports Med. 1990. 18:137-140.39. Ibid. ref 1.40. Ibid. ref 29.41. Ibid. ref 27.42. Ibid. ref 1.43. Ibid. ref 42.44. Ibid. ref 6.45. Ibid. ref 44.46. Ibid. ref 9.47. Ibid. ref 9.48. Ibid. ref 9.49. Ibid. ref 9.50. Ibid. ref 34.51. Ibid. ref 50.52. Ibid. ref 1353. Ibid, ref 13; p 531.54. Alpers BJ. The problem of sciatica. Medical Clin-ics of North America. 1953. 37:503.55. Hackett GS, Hemwall GA, and Montgomery GA.Ligament and Tendon Relaxation Treated by Prolother-apy, 5th Ed. Institute in Basic Life Principles. OakBrook, IL. 1991. (commenting on work of NewmanPH. p 9).56. Ombregt L, Bisschop P, and ter Veer HJ. A Sys-tem of Orthopaedic Medicine, 2nd Ed. Churchill Liv-ingstone. 2003. p775.57. Hills EC and Wieting JM, et al, eds. MechanicalLow Back Pain. Updated 21 November 2004. avail-able from http://www.emedicine.com/pmr/topic73.htm. Accessed 6/9/08.58. Schwarzer A. The sacroiliac joint in chronic lowback pain. Spine. 1995. 20:31-37.59. McCarrol JR, Retig AC, and Shellbourne KD. In-juries in the amateur golfer. The Physician and SportsMedicine. 1990. 18:122.
60. Ibid. ref 5.61. Kohn HS. Prevention and treatment of elbow in-juries in golf. Clin Sports Med. 1996. 15:65.62. Ibid. ref 61.63. Ibid. ref 8.64. Ibid. ref 29.65. Ibid. ref 1.66. Ibid. ref 65.67. Ibid. ref 1.68. Ibid. ref 67.69. Turkel S. Stabilizing mechanisms preventing ante-rior dislocation of the glenohumeral joint. The Journalof Bone and Joint Surgery. 1981. 63A:1208.70. Burden AM, Grimshaw PN, and Wallace ES. Hipand shoulder rotations during the golf swing of sub-10 handicap players. J Sports Ci. 1998. 16:165.71. Jobe FW and Schwab DM. Golf for the matureathlete. Clin Sports Med. 1991. 10:269.72. Ibid. ref 13; p 527.73. Ibid. ref 13; p 668.74. Ibid, ref 13; p 670.75. Ibid. ref 1.76. Prolotherapy in Sports Medicine, presented by Dr.Donna Alderman at Annual Conference of AmericanCollege of Osteopathic Sclerotherapeutic Pain Man-agement. Phoenix, Arizona. April 2008. 77. Ibid. ref 11.78. Ibid. ref 76. 79. Chao EYS, Tamai K, Cahalan TD, et al. Biome-chanics of the golf swing as related to club handledesign. Biomechanics in Sports: A 1987 Update,1987 DE-Vol 13/BED-vol 6:107-111. 80. Gupta A, Risitano G, Crawford R, et al. Fracturesof the hook of the hamate. Injury. 1989. 20 (5):284-286. 81. Bowen TL. Injuries of the hamate bone. Hand.1973. 5:235-238. 82. Ibid. ref 79. 83. Ibid. ref 1.84. Ibid. ref 83.85. Ibid. ref 56.86. MacRae DL. Asymptomatic intervertebral discprotrusion. Acta Radiologica. 1956. pp 46-49.87. Hitselberger WE and Whitten RM. Abnormal myel-ograms in asymptomatic patients. Journal of Neuro-surgery. 1968. 28:204.88. Wiesel SW, et al. A study of computer-assisted to-mography:1. The incidence of positive CAT scans inan asymptomatic group of patients. Spine. 1984.9:549-551.89. Powell MC. et al. Prevalence of lumbar disc de-generation observed by magnetic resonance insymptomless woman. Lancet. 1986. 13:1366-1367.90. Boden SD, et al. Abnormal magnetic resonancescans of the lumbar spine in asymptomatic subjects.Journal of Bone and Joint Surgery. 1990. 72A:503-408.91. Kaplan PA. MR imaging of the normal shoulder:variants and pitfalls. Radiology. 1992. 184:519-524.92. Deyo R. Magnetic resonance imaging of the lum-bar spine—terrific test or tar baby? New EnglandJournal of Medicine. 1994. 331:115-116. 93. Matsumoto M, et al. MRI of the cervical interverte-bral discs in asymptomatic subjects. Journal of Boneand Joint Surgery (Br). 1998. 80(1):19-24.94. Humphreys SC, et al. Reliability of magnetic res-onance imaging in predicting disc material posteriorto the posterior longitudinal ligament in the cervicalspine, A prospective study. Spine. 1998.23(22):2468-2471.95. Connor PM, et al. Magnetic resonance imagineof the asymptomatic shoulder of overhead athletes:A 5 Year followup study. Am J Sports Med 2003.31:724-727.