
Project UPLIFT
21
Project UPLIFT Nancy J. Thompson, Ph.D., M.P.H. Rollins School of Public Health Emory University
description
Project UPLIFT. Nancy J. Thompson, Ph.D., M.P.H. Rollins School of Public Health Emory University. Project UPLIFT. U sing P ractice and L earning to I ncrease F avorable T houghts Delivery of mindfulness-based cognitive therapy by telephone and Internet To people with epilepsy - PowerPoint PPT Presentation
Transcript of Project UPLIFT

Project UPLIFTNancy J. Thompson, Ph.D., M.P.H.
Rollins School of Public HealthEmory University

Project UPLIFTUsing Practice and Learning to Increase
Favorable ThoughtsDelivery of mindfulness-based cognitive
therapy by telephone and InternetTo people with epilepsyMost of the work presented here was funded by
the Centers for Disease Control and Prevention

About Mindfulness-based Cognitive Therapy (MBCT)
• Cognitive Therapy addresses the unrealistic thinking associated with depression.
• Uses verbal techniques to explore the reasoning behind specific attitudes and assumptions.
• Client is taught to recognize, monitor, and record negative thoughts on a daily record.
• CBT focuses on changing thought content while mindfulness changes relationship to the thoughts—see them as passing events that do not necessarily represent a state of reality.
• Mindfulness is important in preventing relapse.
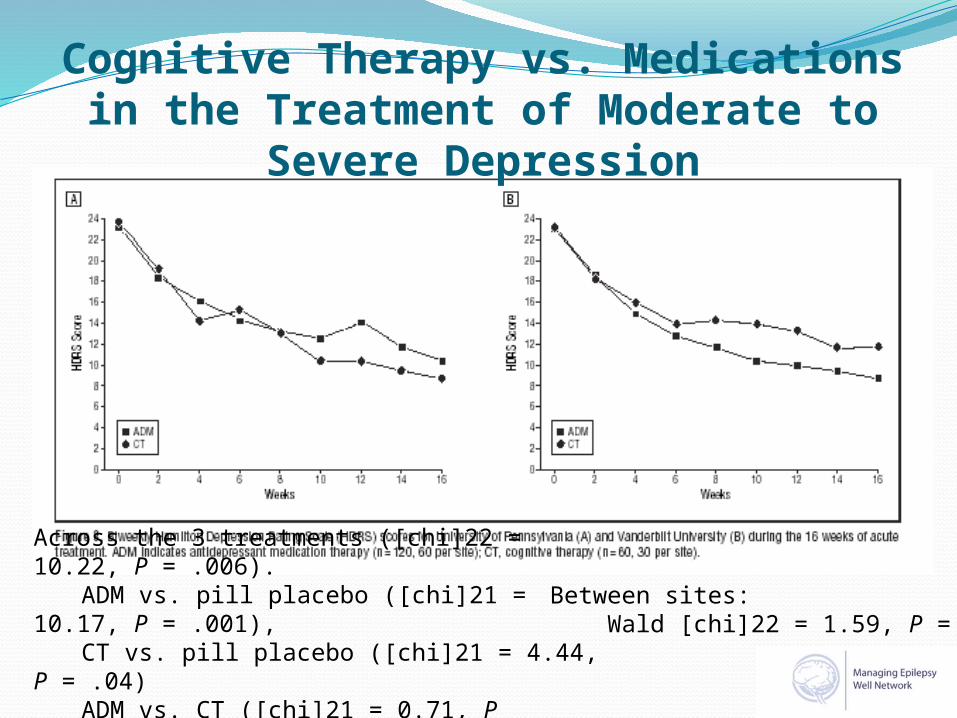
Cognitive Therapy vs. Medications in the Treatment of Moderate to Severe
Depression
Across the 3 treatments ([chi]22 = 10.22, P = .006).
ADM vs. pill placebo ([chi]21 = 10.17, P = .001),
CT vs. pill placebo ([chi]21 = 4.44, P = .04)
ADM vs. CT ([chi]21 = 0.71, P = .40).
Between sites: Wald [chi]22 = 1.59, P = .45

Intent to Treat 4+ Sessions
Follow-up after Mindfulness vs. Treatment as Usual for the Treatment of Depression

Project UPLIFTDelivery of MBCT by Web and Telephone
GroupsPeople with epilepsy randomly assigned to groups
of 7Initially computers and Internet access provided
if neededGroup delivery important for support
surrounding epilepsy Co-Facilitators
Graduate Public Health StudentPerson with epilepsySupervised by a licensed psychologist

Potential Benefits• Cost-effective• Can reach the mobility/transportation
limited• Equal reach to urban and rural• Allows peer support, even with rare
conditions• Potential for anonymity and avoidance
of stigma• Can prevent relapse• Does not require more medication• Mindfulness may improve
attention/cognition

Session # Topic
1 Monitoring Thoughts
2 Challenging and Changing Thoughts
3 Coping and Relaxing4 Attention and Mindfulness5 The Present as a Calm Place6 Thoughts as Changeable and
Impermanent7 Pleasure and Reinforcement8 Relapse Action Plans
Project UPLIFT8 Sessions (1 hour by phone)
Noting Challenging/Changing Impermanent
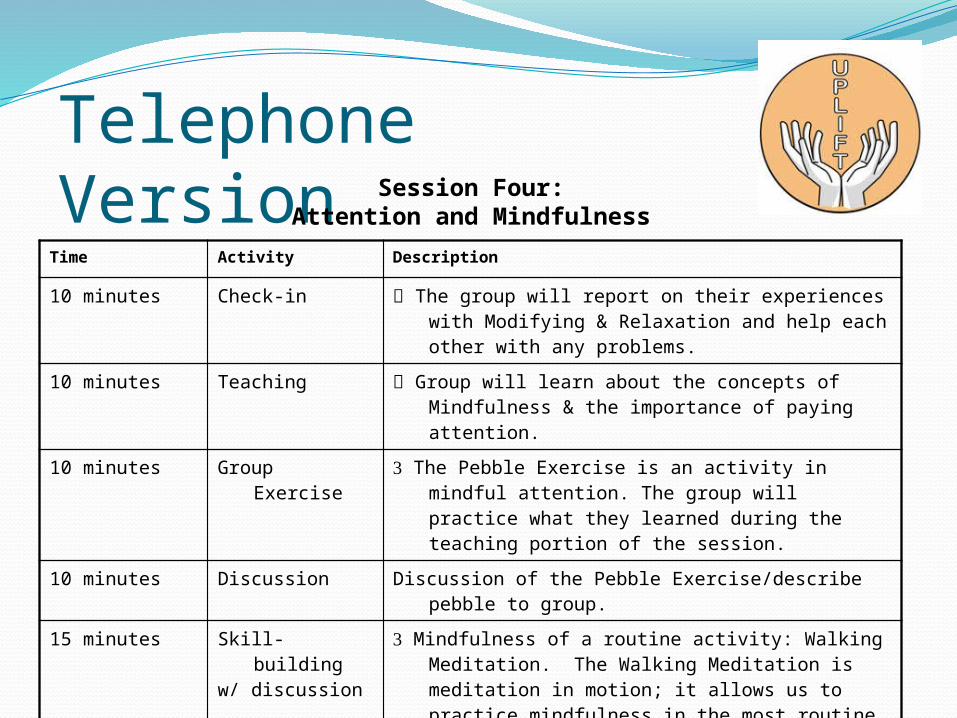
Telephone Version
Time Activity Description
10 minutes Check-in The group will report on their experiences with Modifying & Relaxation and help each other with any problems.
10 minutes Teaching Group will learn about the concepts of Mindfulness & the importance of paying attention.
10 minutes Group Exercise The Pebble Exercise is an activity in mindful attention. The group will practice what they learned during the teaching portion of the session.
10 minutes Discussion Discussion of the Pebble Exercise/describe pebble to group.
15 minutes Skill-buildingw/ discussion
Mindfulness of a routine activity: Walking Meditation. The Walking Meditation is meditation in motion; it allows us to practice mindfulness in the most routine of activities.
5 minutes Review & Homework
Homework: Monitoring with Modification and Practicing Mindfulness of Routine Activities 3 times during the week.
Session Four:Attention and Mindfulness

Web Version Session One:Monitoring Thoughts

Formative Evaluation Focus GroupsImportance of Group
“Medical professionals can tell you the what, the why, the diagnosis, but in a group of people with epilepsy, there’s camaraderie and you can see what other people go through.”
“Being in a group with other people with epilepsy is like sharing with your close friends. You realize that everyone has their insecurities and you feel more safe.”
Response to Activities “If I could learn to modify my thoughts, that
would be practical.” “The good thing about doing mindfulness of
sounds and thoughts is that you can do it anywhere.”

Design—Outcome Evaluation
Stratum 1: Pretest 6-8 wk phone Interim as usual Follow-up
Stratum 2: Pretest 6-8 wk Web Interim as usual Follow-up
Stratum 3: Pretest as usual Interim 6-8 wk phone Follow-up
Stratum 4: Pretest as usual Interim 6-8 wk Web Follow-up
Baseline Week 8 Week 16
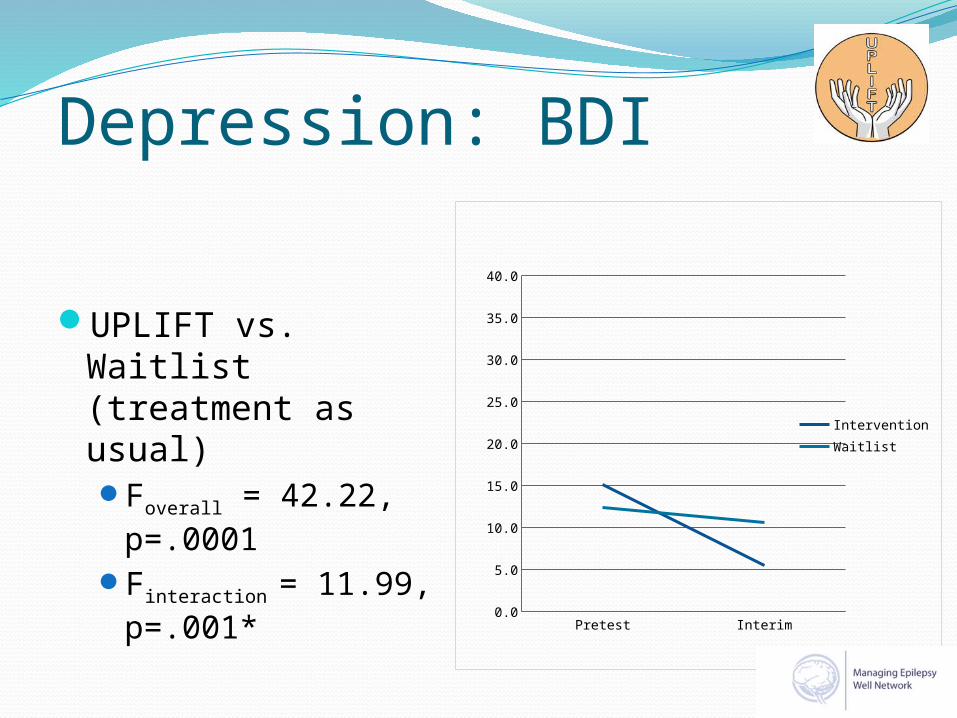
Depression: BDI
UPLIFT vs. Waitlist (treatment as usual)Foverall = 42.22,
p=.0001Finteraction = 11.99,
p=.001*
Pretest Interim0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
40.0
InterventionWaitlist

Depression: BDI By Intervention Type
• Phone vs. Web vs. Waitlist (treatment as usual)Foverall = 41.65,
p=.0001Finteraction = 5.93,
p=.006*Pretest Interim
0
5
10
15
20
25
30
35
40
BDI
Phone TxWeb TxWaitlist

No difference with Major Depressive Disorder or not (F1,35= 1.21, p = 0.279)
MaintenanceMeasure Time Intervention Treatment
-as-Usual Waitlist
F df p-value
BDI Pretest
Interim
Posttest
14.5
4.6
5.7
13.4
10.8
8.3
0.121
7.541
1.124
1,30
1,30
1,30
0.730
0.010*0.297

Knowledge/Skills & Self-Efficacy
Measure Time Intervention TAU Waitlist Finteraction
df 1,37
P-value
Knowledge/Skills
PretestInterim
122.5136.3
123.5126.0
4.75 0.036*
Depression Coping
Self-Efficacy
PretestInterim
67.775.5
72.472.9
3.59 0.066

Quality of LifeMeasure Time Intervention Tx As Usual
Waitlist
Finteraction
df 1,37P-value
Satisfaction with Life
PretestInterim
18.221.0
18.318.0
3.029 0.0901
Mental Health QOL
PretestInterim
59.380.9
65.483.6
0.123 0.727
Physical Health QOL
PretestInterim
68.978.9
76.280.8
0.496 0.486
1.05<p<.10

SummaryEffective in:
Reducing depressive symptoms and teaching knowledge and skills associated with reducing depression Intervention group showed significant improvement
compared to the waitlist Equally effective for those with and without MDD Reduction in depressive symptoms maintained
Approaching significance for Satisfaction with Life and Depression Coping Self-Efficacy
DeliveryBoth phone and web were significantly more
effective in reducing depression than waitlist condition

Participants’ Comments“I told my therapist I think I like this way a lot
better…I’ve always went and talked to somebody versus learning to work through things just using my own mindset.”
“The project had great value. I'm thankful that I was able to participate. I got a lot out of the exercises and coping skills.”
“The program was very helpful and that surprised me. I printed everything out and recorded the meditations onto my MP3 player.”
“The program helped me more than the antidepressants I've been on for years.”
“Thank you for helping me because I have been depressed and now I can cope.”

Potential Benefits• Cost-effective• Reaches the mobility limited• Equal reach to urban and rural• Can form groups even with rare
conditions• Potential for anonymity and
avoidance of stigma• Prevent relapse

Project UPLIFTNext Phase~$1 million Challenge GrantUPLIFT for PreventionParticipants in MEW network states
- Georgia- Michigan- Texas- Washington


















