Prognostic value of predischarge exercise stress echocardiography after acute myocardial infarction
7
Prognostic Value of Predischarge Exercise Stress Echocardio raphy After Acute Myocardia Infarction 1 Miauel Quintana, MD, Kai Lindvall, MD, PhD, Lars Rydh, MD, PhD, ” bnd ‘Fredrik Brolund, CT A predischarge exercise test was erformed by 70 patients 7 f 4 days (mean + SD) a tL r acute m ocar- dial infarction (AMI) to determine the short- an J long- term prognostic value of predischarge exercise stress echocardiograph (Ex-Echo) compared with exercise stress electrocar cr iography (Ex-ECG). Two-dimensional echocardiograms were obtained at rest and immedi- atety after exercise; a wall motion score index was obtained both at rest and immediately after exercise. Results of the Ex-Echo were positive in 27 patients (39%), whereas those of Ex-ECG were positive in 34 (49%). The wall motion index after exercise was low- er in patients who died during follow-up (85 vs 98, p = 0.01) and in those with cardiac events, defined as death, nonfatal reinfarction, or revoscularization (88 vs 98, P = 0.005). More patients with a positive Ex-Echo resu t had short-term cardiac events (within 2 weeks) than patients with a negative Ex-Echo (6 (22%) vs 2 [5%1, p = 0.04). The same was true for long-term mor- tality (12 [44%1 vs 3 [7%1, p = 0.0002), reinfarctions (10 [37%1 vs 4 (9%1, p = O.Ol), revascularization pro- cedures (11 [41%1 vs 7 [16%1, = 0.023), and cardiac events (22 [81%1 vs 12 (28%, p <O.OOOl). Survival P time was shorter in patients with positive compared with negative Ex-Echo results (34% difference between groups, 95% confidence interval [Cl] 10% to 58%, = 0.002). The~same applied for cumulative survival ree P from cardiac events (43%, p = 0.001, 95% Cl 9% to 77%). In a multivariate regression analysis, both Ex- Echo and Ex-ECG independently predicted death, death or nonfatal reinfarction, revascularization, and cardiac events. A new-onset wall motion abnormali xl was, however, the strongest variable predicting dea (haz- ards ratio 9.8, 95% Cl 8.5 to 11) and deaths or non- fatal reinfarction (hazards ratio 4.3,95% Cl 3.4 to 5.3). Thus, Ex-Echo is recommended for early risk stratifica- tion after AMI. (Am J Cardiol 1995;76: 1115-l 12 1) R isk stratification, a main goal after acute myocardial infarction (AMI), is usually based on the patient’s clinical characteristics,1,2 the evaluation of residual myo- cardial ischemia,2A and the evaluation of the left ven- tricular function.2s3,5 Residual myocardial ischemia is generally assessed by the patient’s symptoms, and by electrocardiographic changes occurring during ambula- tory electrocardiographic monitoring and during exer- cise stress electrocardiography (Ex-ECG).~‘O Sensitivi- ty and specificity of Ex-ECG in predicting mortality and morbidity after AM1 are, however, 10w.~,~” A good clin- ical evaluation can select high-risk patients after AM1 even before they perform a predischarge exercise test,12 and may explain the low sensitivity of an Ex-ECG test after AMI. Additional noninvasive methods have been used to stratify patients after AMI, such as myocardial scintigraphy, 13-15 radionuclide angiography, 13,16 and more recently, stress echocardiography.17-l9 Short-term and l- year prognoses after AM1 have been studied with exer- cise stress echocardiography (Ex-Echo) in a few stud- ies. 17-19 The value of this technique to predict long-term From ihe Karolinska Institute at the Department of Cardiology, South Hospital and Department of Cardiology, Thorax Division, Karolinska Hospital, Stockholm, Sweden. This study was supported b from the Swedish Heart Lung Foundation, grants Arbetsmar nadens l Forstikrin and Me sbolag [AFA), and Stockholm County Council, Public Health k! lcal Service, Department of Research, Development and Teaching, Stockholm, Sweden. Manuscript received May 1.5, 1995; revised manuscript received and accepted August 16, 1995. Address for reprints: Miguel Quintana, MD, Karolinska Institute at the Section of Cardiology, Department of Internal Medicine, Dan- deryd Hospital, S 182 88 Dandeyd, Stockholm, Sweden. mortality and morbidity still needs further elucidation. This study was conducted to determine the short- and long-term prognostic value of a predischarge Ex-Echo after AMI. METHODS Study population: A group of 203 patients aged ~75 years, admitted to the cardiology ward between January 1989 and February 1990 for AM1 was screened. Of these, 129 (64%) were excluded because of atrial fibrillation, second degree or higher atrioventricular block, valvular heart disease, bundle branch block or intraventricular conduction defects >120 ms, permanent digoxin med- ication, presence of cardiogenic shock, cancer or other unrelated diseases in terminal stages, and unwillingness to participate. Four patients (2%) were excluded because of cardiac events occurring before the exercise test. The study group thus consisted of 70 of these patients (34%). Myocardial infarction was diagnosed clinically and con- timed by electrocardiographic changes and by an increase in creatine kinase to >2 times normal total with an associated increase in the MB isoenzyme levels to >5% of total creatine kinase. The clinical characteristics of the study group are list- ed in Table I. All patients received standard medical care during and after hospitalization. The decision to perform coronary angiography and revascularization was always based on symptoms (postinfarction angina), or on the results of Ex-ECG tests in combination with the pres- ence of refractory effort angina. Physicians in charge of individual patients were aware of the results of Ex-ECG, but not of the results of Ex-Echo. CORONARY ARTERY DISEASE/PROGNOSIS AFTER A./VI WITH STRESS ECHO 1115
-
Upload
miguel-quintana -
Category
Documents
-
view
216 -
download
1
Transcript of Prognostic value of predischarge exercise stress echocardiography after acute myocardial infarction

Prognostic Value of Predischarge Exercise Stress Echocardio raphy After Acute
Myocardia Infarction 1 Miauel Quintana, MD, Kai Lindvall, MD, PhD, Lars Rydh, MD, PhD,
”
bnd ‘Fredrik Brolund, CT
A predischarge exercise test was erformed by 70 patients 7 f 4 days (mean + SD) a tL r acute m ocar- dial infarction (AMI) to determine the short- an J long- term prognostic value of predischarge exercise stress echocardiograph (Ex-Echo) compared with exercise stress electrocar cr iography (Ex-ECG). Two-dimensional echocardiograms were obtained at rest and immedi- atety after exercise; a wall motion score index was obtained both at rest and immediately after exercise. Results of the Ex-Echo were positive in 27 patients (39%), whereas those of Ex-ECG were positive in 34 (49%). The wall motion index after exercise was low- er in patients who died during follow-up (85 vs 98, p = 0.01) and in those with cardiac events, defined as death, nonfatal reinfarction, or revoscularization (88 vs 98,
P = 0.005). More patients with a positive Ex-Echo
resu t had short-term cardiac events (within 2 weeks) than patients with a negative Ex-Echo (6 (22%) vs 2 [5%1, p = 0.04). The same was true for long-term mor-
tality (12 [44%1 vs 3 [7%1, p = 0.0002), reinfarctions (10 [37%1 vs 4 (9%1, p = O.Ol), revascularization pro- cedures (11 [41%1 vs 7 [16%1, = 0.023), and cardiac events (22 [81%1 vs 12 (28%, p <O.OOOl). Survival P time was shorter in patients with positive compared with negative Ex-Echo results (34% difference between groups, 95% confidence interval [Cl] 10% to 58%, = 0.002). The~same applied for cumulative survival ree P from cardiac events (43%, p = 0.001, 95% Cl 9% to 77%). In a multivariate regression analysis, both Ex- Echo and Ex-ECG independently predicted death, death or nonfatal reinfarction, revascularization, and cardiac events. A new-onset wall motion abnormali
xl was,
however, the strongest variable predicting dea (haz- ards ratio 9.8, 95% Cl 8.5 to 11) and deaths or non- fatal reinfarction (hazards ratio 4.3,95% Cl 3.4 to 5.3). Thus, Ex-Echo is recommended for early risk stratifica- tion after AMI.
(Am J Cardiol 1995;76: 1115-l 12 1)
R isk stratification, a main goal after acute myocardial infarction (AMI), is usually based on the patient’s
clinical characteristics,1,2 the evaluation of residual myo- cardial ischemia,2A and the evaluation of the left ven- tricular function.2s3,5 Residual myocardial ischemia is generally assessed by the patient’s symptoms, and by electrocardiographic changes occurring during ambula- tory electrocardiographic monitoring and during exer- cise stress electrocardiography (Ex-ECG).~‘O Sensitivi- ty and specificity of Ex-ECG in predicting mortality and morbidity after AM1 are, however, 10w.~,~” A good clin- ical evaluation can select high-risk patients after AM1 even before they perform a predischarge exercise test,12 and may explain the low sensitivity of an Ex-ECG test after AMI. Additional noninvasive methods have been used to stratify patients after AMI, such as myocardial scintigraphy, 13-15 radionuclide angiography, 13,16 and more recently, stress echocardiography.17-l9 Short-term and l- year prognoses after AM1 have been studied with exer- cise stress echocardiography (Ex-Echo) in a few stud- ies. 17-19 The value of this technique to predict long-term
From ihe Karolinska Institute at the Department of Cardiology, South
Hospital and Department of Cardiology, Thorax Division, Karolinska Hospital, Stockholm, Sweden. This study was supported b from the Swedish Heart Lung Foundation,
grants Arbetsmar nadens l
Forstikrin and Me
sbolag [AFA), and Stockholm County Council, Public Health k! lcal Service, Department of Research, Development and
Teaching, Stockholm, Sweden. Manuscript received May 1.5, 1995; revised manuscript received and accepted August 16, 1995.
Address for reprints: Miguel Quintana, MD, Karolinska Institute at the Section of Cardiology, Department of Internal Medicine, Dan- deryd Hospital, S 182 88 Dandeyd, Stockholm, Sweden.
mortality and morbidity still needs further elucidation. This study was conducted to determine the short- and long-term prognostic value of a predischarge Ex-Echo after AMI.
METHODS Study population: A group of 203 patients aged ~75
years, admitted to the cardiology ward between January 1989 and February 1990 for AM1 was screened. Of these, 129 (64%) were excluded because of atrial fibrillation, second degree or higher atrioventricular block, valvular heart disease, bundle branch block or intraventricular conduction defects >120 ms, permanent digoxin med- ication, presence of cardiogenic shock, cancer or other unrelated diseases in terminal stages, and unwillingness to participate. Four patients (2%) were excluded because of cardiac events occurring before the exercise test. The study group thus consisted of 70 of these patients (34%). Myocardial infarction was diagnosed clinically and con- timed by electrocardiographic changes and by an increase in creatine kinase to >2 times normal total with an associated increase in the MB isoenzyme levels to >5% of total creatine kinase.
The clinical characteristics of the study group are list- ed in Table I. All patients received standard medical care during and after hospitalization. The decision to perform coronary angiography and revascularization was always based on symptoms (postinfarction angina), or on the results of Ex-ECG tests in combination with the pres- ence of refractory effort angina. Physicians in charge of individual patients were aware of the results of Ex-ECG, but not of the results of Ex-Echo.
CORONARY ARTERY DISEASE/PROGNOSIS AFTER A./VI WITH STRESS ECHO 1115

TABLE I Clinical Characteristics, Pharmacologic Therapy [at discharge), and Outcome During Exercise Stress Echocardiography in 70 Patients With Acute Myocardial Infarction
Exercise Stress
Clinical Echocardiography
Characteristics + (n = 27) - (n = 43) p Value
Age (yr) 62 zi 8 6Oi: 10 NS Maximal CK-MB (pkat/L) 1.8 2 1.3 1.4kl.l NS
Hospitalization time (d) 12.8 + 8.1 8.9 zt 4.0 0.02 Survival time (mo) 21.4 it 11.6 27.1 f 6.0 0.02
Women 11 (41) 3 (7) 0.001
Anterior myocardial 10 (37) 14 (33) NS
infarction Q-wave myocardial 16 (59) 32 (74) NS
infarction Systemic hypertension 13 (48) 13 (30) NS
Previous myocardial 8 (30) 6 (14) NS
infarction Diabetes mellitus 3 111) 4 (91 NS Current smokers 13 (48) 25 (58) NS
Angina pectoris 4 115) 3 (71 NS
Pharmacologic Therapy
Aspirin 24 (89) 39 (91) NS Beta blockers 15 (56) 31 (72) NS
Calcium antagonists 6 (24 10 (23) NS
Diuretics 18 (67) 15 (35) 0.01
Thrombolytics 11 (41) 22 (51) NS Heparin 16 (59) 29 (67) NS
Nitrates 11 (41) 10 (23) NS
Values are expressed ~1s number w) or mean * SD. CK = creatine kinas& isoenzyme; + = positive results; - = negative results
Exercise stress testing: Seventy patients performed a symptom-limited bicycle ergometer exercise stress test 7 f 4 days (mean f SD) after AMI, with 6 standard limb leads and 6 precordial leads. When necessary the elec- trodes’ positions were rearranged to allow satisfactory echocardiographic windows. Electrocardiograms were recorded before exercise, at intervals of 1 minute during exercise, at peak exercise, immediately after recovery, and 2,4,6, and 10 minutes after exercise. The test result was considered positive for ischemia if 21 mm of horizontal
TABLE II Results of Exercise Stress Echocardiography in 70 Patients With Acute Myocardial Infarction I
Variables Measured at Exercise Stress Test
or downsloping ST-segment depression, measured 80 ms after the J point, appeared in 22 consecutive leads, com- pared with the baseline electrocardiogram.
Exercise echocardiography: Two-dimensional echo- cardiograms were obtained, using 2.0 or 3.5 MHz trans- ducers (Aloka SSD 870, Tokyo, Japan). Standard para- sternal long- and short-axis and apical 2- and 4-chamber views were obtained both at rest and immediately after exercise, with the patients in the left lateral decubitus position. Registrations were completed within 2 minutes after end of exercise. All images were recorded on video tapes, and saved in formatted disks using a digital acqui- sition system for quad-screen, side-by-side analysis. The videotapes and the formatted disks were encoded blind for later analysis. In addition, video tapes and disks con- taining exercise stress echocardiograms, performed in 23 age- and sex-matched healthy individuals, were also encoded and mixed with those belonging to the study population. The left ventricle was divided into 16 seg- ments, according to the recommendations of the Amer- ican Society of Echocardiography. The wall motion of each segment was scored between 0 and 125 as follows: hyperkinetic (125), normal (loo), hypokinetic (75), aki- netic (50), dyskinetic (25), or aneurysmal (0), based on visual analysis. 21 A test result &as considered positive when a worsening (in hypokinetic or akinetic segments) or a new-onset wall motion abnormality occurred. The presence of abnormal wall motion at rest alone was not considered a criterion for positivity. A wall motion score index was derived by adding the scores assigned to each segment and dividing the final score with the number of segments analyzed. An Ex-Echo result was considered eligible in the study if at least 12 of 16 segments were interpretable. As with exercise electrocardiograms, echo- cardiograms were blindly analyzed by 2 independent and trained echocardiographers (FB and MQ), who were unaware of the results of exercise electrocardiographic tests and patient outcome. In cases of disagreements, a third interpretation was done by an independent inves- tigator and the majority opinion prevailed.
Follow-up: After hospital discharge, patients were checked at 1,3,6, and 12 months, and then once a year for at least 3 years (mean + SD 36 + 15 months; range 0 to 50. months). Each follow-up visit was performed according to routine procedures. The follow-up was com- plete in all patients. The vital status of
Exercise Stress Echocardiography
+ (n = 27) - (n = 43) p Value
Heart rate at rest (beats/min) 70* 14 67+ 17 Systolic blood pressure at rest (mm Hg) 125 * 17 124 + 18 Diastolic blood pressure at rest (mm Hg) 80 zt 6 80 i: 8 Peak heart rate (beats/min) 117k 18 124 I? 15 Peak systolic pressure (mm Hg) 156 f 34 174228 Peak double product x 1 O-3 18 +5 22 f 4 Maximal workload (W) 89 * 27 115227 Wall motion index-rest 81 f 10 87 f 8 Wall motion index-exercise 832 13 100 * 12 Angina pectoris 4 (151 4 (9) ST-segment depression (STD) 17 (63) 17 (40) Maximal STD [mm) 2.9 zt 1.73 2.44 2 0.95 Maximal STD duration (min) 7.3 f 5.1 6.6 f 5.0
Values we expressed CIS mean * SD or number (%). Symbols as in Table I.
NS NS NS NS
0.02 0.003 0.0002 0.02
<0.0001 NS NS
NS
NS
I
all excluded patients was assessed at the end of the follow-up period. Car- diac events were defined as death, rein- farction (fatal and nonfatal), death or nonfatal reinfarction, revascularization procedures, and the total sum of the first-occurring cardiac events (cardiac events). Short-term cardiac events were those occurring within 2 weeks after index infarction. Coronary angi- ography (29 patients, 41%) and revas- cularization procedures (19 coronary artery bypass surgeries and 1 percuta- neous transluminal coronary angio-
1116 THE AMERICAN JOURNAL OF CARDIOLOGY@ VOL. 76 DECEMBER 1, 1995

TABLE III Exercise Stress Echocardiography and Short- and tong-Term Outcome in 70 Patients With Acute Myocardial Infarction
Exercise Stress
Echocardiography
End Points + (n = 27) - (n = 43) p Value*
Short-term events7 6 (22) 2 (51 0.04 tong-term events
Deaths 12 (44) 3 (7) 0.0002 All reinfarctions 10 (37) 4 (9) 0.01
Fatal reinfarctions 6 (22)* 1 (2) 0.01 Nonfatal reinfarctions 6 (2’4 3 (71 NS
Deaths or reinfarctions 13 (48) 6 (14) 0.001 Revascularizations 11 (41) 7 (161 0.023 Cardiac events 22 (81) 12 (28) <0.0001
Wall Motion Index
Yes-. No p Values
Short-term events7 82+ 18 95 f 14 NS tong-term events
Deaths 85+ 13 98+ 14 0.01 All reinfarctions 88* 15 94* 15 NS
Fatal reinfarctions 84% 13 95* 15 NS Nonfatal reinfarctions 882 17 94k 14 NS
Deaths or reinfarctions 88* 14 95* 14 0.05 Revascularizations 91 f 15 942 15 NS Cardiac events 88 % 14 98+ 14 0.005
*Yates’ corrected chi-square. tFour deaths, 2 coronary bypass surgeries, 2 nonfatal reinfarctions. *Two patients with nonfatal reinfarction developed CI fatal reinfarction later. ~Pearson’s t test. Syt&ols OS in Table I.
plasty, 29%) were performed based on clinical decisions only, according to previously described criteria. Descrip- tions of causes and circumstances of death and the def- inition of a new cardiac e&t have been described else- where.(j
Statistical analysis: Statistical significance was tested using the Yates’ corrected chi-square test or the Fisher’s exact test for discrete variables and the t test for contin- uous and normally distributed variables. Survival analy- sis and the time-dependent cumulative probability for other cardiac events were performed using Kaplan-Meier curves. Statistical difference between 2 groups was test- ed with the log rank test22 (Statistica statistical package, Tulsa, Oklahoma). Multiple regression analysis was cal- culated using the Cox proportional hazards mode1.23 When evaluating cardiac events, only the first cardiac event (in patients with >l event) was considered. A p value of <0.05 was considered statistically significant. Data are presented as mean + SD.
Ethical considerations: This study was approved by the local ethics committee. All the patients received written information and gave informed consent to participation.
RESULTS Clinical characteristics: Table I lists patients’ clinical
characteristics in relation to Ex-Echo findings. Patients with a positive Ex-Echo result had longer hospitaliza- tion periods than patients with a negative Ex-Echo result. More women than men had a positive Ex-Echo result. All other clinical characteristics, and phtiacologic therapy, were similar in patients with positive or nega- tive fix-Echo results, except that more patients taking
r TABLE IV Multivariate Regression Analysis of Clinical Variables,
ST-Segment Depression on Exercise Testing (STD at ExT), and New-Onset Wall Motion on Exercise Stress Echocardiography in 70 Patients With Acute Myocardial Infarction
Variables
New-Onset STD at Diabetes Angina End Points Wall Motion ExT Mellitus Pectoris
Deaths Hazards ratio 9.8 4.7 4.0 - 95% Cl 8.5-l 1 3.4-6 2.6-5.4 - p Value <O.OOl co.05 co.05 NS
Deaths or reinfarctions
Hazards ratio 4.3 2.3 - - 95% Cl 3.4-5.3 1.3-3.3 - - p Value <O.Ol <0.05 NS NS
Revascularizations Hazards ratio 4.7 2.8 - 8.1 95% Cl 3.7-5.7 1.8-3.8 - 7-9.2 p Value <O.Ol co.05 NS co.005
Cardiac events Hazards ratio 6.8 3.2 - 7.8 95% Cl 6-7.5 2.5-3.9 - 6.9-8.7 p Value 10.0001 co.01 NS <O.OOl
0, .--cd-~-- .~&.- -I
diuretics had positive Ex-Echo results than did patients not receiving diuretics.
Cardiac events’ during follow-up: During short-term follow-up, 8 patients had cardiac events: 4 deaths, 2 non- fatal myocardial infarct&s, and 2 bypass surgeries. Dur- ing long-term follow-up, 15 patients died, 18 underwent revascularization, and 14 had a new myocardial infarc- tion. Seven had a fatal reinfarction and 9 had a nonfatal reinfarction (2 patients with’ nonfatal reinfarction devel- oped a fatal reinfarctioh later). A total of 40 cardiac events occurred in 34 of 70 patients. Mortality among nonincluded patients and in the studied group was sim- ilar (33 of 129 [26%] vs 15 of 70 [21%], p = NS).
Exercise stress echocardiography aird clinical out- comes: Table II lists the results of the exercise stress test. In 27 patients (39%), the result of Ex-Echo was consid- ered positive (patients had either worsened segments or new-onset wall motion abnormalities). New-onset wall motion abnormalities were observed in 22 patients (31%). Peak systolic pressure, maximal workload, and double product were significantly higher in patients with nega- tive Ex-Echo results. Patients with a positive Ex-Echo result had lower wall motion indexes at rest and after exercise than did patients with a negative Ex-Echo result.
Relations between Ex-Echo results and cardiac events are listed in Table III. Although the wall motion index’ was significantly lower among patients dying and with cardiac events, this index was similar in patients having a new myocardial infarction and undergoing revascularization. The wall motiori index was also low- er (but not significantly so) in patients with short-term cardiac events (p = 0.08). A positive Ex-Echo result pre- dicted the occurrence of all cardiac events, including short-term events and revascularization procedures. In addition, patients with a positive Ex-Echo result had shorter survival times and shorter cumulative survival free of cardiac events than did patients with a negative Ex-Echo result (Figures 1A to 1D). Univariate regres-
CORONARY ARTERY DISEASE/PROGNOSIS AFTER AM WITH STRESS ECHO 1117

TABLE V Prognostic Value of Exercise Stress Echocardiography (Echo) and Electrocardiography (ECG) in 70 Patients After Acute Myocardial Infarction
Prognostic Deaths Deaths or Reinfarctions Cardiac Events
Value Echo ECG Either Echo ECG Either Echo ECG Either
Sensitivity 80 80 100 68 68 65 68 85 Specificity 73 60 45 58 :.i 86 69 54 PP value 44 35 33 :i 38 36 81 68 64
NP value 93 92 100 86 83 88 72 69 80
Accuracy 74 64 57 71 61 54 73 69 69
cardiac events [Table IV]). Diabetes mellitus predicted the occurrence of death. Revascularization procedures and cardiac events were, as expected, more common in patients with angina pectoris during hospitalization than in patients without angina.
Sensitivity, specificity, predictive val- ue, and accuracy of exercise stress elec- kocardiography and echacardiography:
ECG = positive result from electrocardiography; Echo = positive result from echocardiography; Either = positive result from either echocardiography or electrocardiography; NP = negative predic-
Ex-Echo and Ex-ECG tests had similar
tive; PP = positive predictive. sensitivities to predict deaths, deaths or reinfarctions, and cardiac events (Table V). However, the specificity of Ex-Echo
sion analysis was performed to assess the prognostic val- was higher than that of Ex-ECG to detect those events. ues of all variables included in Table I, including the The positive predictive value, although low for both meth- presence of ST-segment depression and a new-onset wall ods, was higher for Ex-Echo, especially regarding cardiac motion abnormality during exercise test. In multivariate events. The presence of a positive test result, either Ex- regression analysis, among all variables, a new-onset Echo or Ex-ECG, conferred the highest levels of sensi- wall motion abnormality and the presence of ST-seg- tivity to detect deaths (100%) and cardiac events (85%). ment depression on exercise test independently predict- ed mortality and other cardiac events (death or nonfatal
A new-onset wall motion abnormality improved the pos- itive predictive value and the accuracy of Ex-Echo to assess
reinfarction, revascularization, and the occurrence of mortality (55% vs 44% and 82% vs 74%, respectively).
80
60
A. Cumulative Surviving
Patients
s?
Stress-Echo (t) t
Difference between groups: 34% 95% Cl. = 10 to 513 percent
40 17 26 10
100
80
01, 0
I 1 2 3
Follow-up time (years)
B. Cumulative Deaths or Reinfarctions I
$-.-.--------.-.--,-I-----,_- Stress-Echo(-) 1
StresslEcho (t) I
I -
Patients
Difference between groups = 29% 95% Cl. = 4 to 54 percent
24 IO
I 1 2 3
Follow-up time (years)
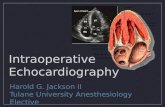
FIGURE 1. Survival times (A) and cumulative survival free of death or reinfarction (B), free of revascularization (C), and free of any cardiac event (0) in 70 patients after acute myocardial infarction. C.I. = confidence interval; Stress-Echo (t) = patients with a positive result after exercise stress echocardiog- raphy (worsened or a new- onset wall motion abnormal- ity); Stress-echo (-) = patients with a negative result after exercise stress echocardiography.
1118 THE AMERICAN JOURNAL OF CARDIOLOGY@ VOL. 76 DECEMBER 1, 1995

Correlation between exercise stress electrocardiog- raphy and echocardiography findings: A poor correlation (R = 0.22, p = 0.057) was found between the results of Ex-Echo and Ex-ECG tests. The concordance between the results of both tests was low (61%, K = 0.22). This correlation was even poorer when ST-segment changes were compared with new-onset wall motion abnormali- ties, occurring in 22 patients (R = 0.20, p = 0.09, con- cordance 60%, K = 0.18).
DISCUSSION In the present study patients with a positive Ex-Echo
result had poor short- and long-term prognoses. Survival times and cumulative survival free of cardiac events were shorter in patients with a positive result, compared with patients with a negative test result. Patients with a poor- er prognosis had, in addition, a lower wall motion index at rest and after exercise than did patients with more favorable prognoses. Few studies17L19 have previously shown the prognostic value of Ex-Echo after AMI. The present study differs considerably from previous inves- tigations in several aspects: (1) A poor outcome was defined by previous investigators18J9 as the sum of all
cardiac events (unstable angina, myocardial infarction, deaths, and need of revascularization), whereas in the present study, each cardiac event was independently assessed. (2) The number of patients included in previ- ous studies was smaller, and the follow-up time was con- siderably shorter. (3) Digital acquisition of echocardio- graphic images for quad-screen side-by-side analysis was used only by Ryan et al.” (4) Timing and protocols for exercise testing were also dilferent. More recently, some studies16,24-27 have confirmed the value of stress echocardiography to correctly assess coronary artery dis- ease and to assess prognosis after AMI. In contrast to ours, all those studies used pharmacologic methods to induce stress.
Wall motion index as a function of left ventricular func- tion-its prognostic value: Left ventricular ejection frac- tion assessed by Ex-Echo in post-AM1 patients has not shown predictive value. 17-19 In the present study, as in the study by Amanullah and LindvalL21 the left ventric- ular function was assessed by measuring wall motion index; patients with poor outcomes had a lower wall motion index during predischarge Ex-Echo. This has been confirmed by Picano et a126 during dipyridamole
FIGURE 1. (continued)
100
80
F :E 60
h
$ 40
20
0
.
c
Difference between groups = 43% 95% Cl. = 9 to 77 percent
Stress-Echo (+) I
Patients
i; 39 13 34 9 21 6 -7 O-
0 1 2 3
C. Cumulative Revascularizations
Patients
Diffrence between groups = 32% 95% Cl. = -6 to 70 percent
z; 39 12 35 8 22 4
1 2 3
Follow-up time (years)
D. Cumulative Cardiac Events
Follow-up time (years)
CORONARY ARTERY DISEASE/PROGNOSIS AFTER AM WITH STRESS ECHO 1119

stress echocardiography in a large-scale study. A global assessment of left ventricular function, based on region- al wall motion index, is a more logical approach than measuring the ejection fraction. The technical difficul- ties and mathematic assumptions that measuring ejec- tion fraction implies are thus avoided.
Additive prognostic value of stress echocardiography: With multiple regression analysis, both Ex-ECG and Ex- Echo independently predicted death and other cardiac events. However, the hazards ratio conferred by a posi- tive Ex-Echo result was higher than that conferred by a positive Ex-ECG test result, and by other clinical vari- ables. Even revascularization procedures that were essentially based upon the results of Ex-ECG tests and on the presence of angina pectoris were best and inde- pendently predicted by a positive Ex-Echo result. This indirectly suggests that a positive Ex-Echo result had a high correlation with the severity of coronary artery dis- ease, which has been reported by others using’ exercise or pharmacologic methods.24,25
The sensitivity of both Ex-ECG and Ex-Echo tests to predict’death, death or nonfatal reinfarction, and car- diac events was similar. The specificity of Ex-Echo in predicting such cardiac events was, however, superior. The high sensitivity of the Ex-ECG test is perhaps explained by the fact that patients performed a high lev- el of exercise (patients achieved 80% of the maximal expected work capacity for sex and age). The relatively high specificity of Ex-ECG test was due to the exclusion of patients with severely abnormal rest ECGs (bundle block, permanent digoxin medication, patients with atri- al fibrillation and valvular heart disease), precluding interpretation for ischemic changes.
The reported sensitivity of Ex-Echo to predict car- diac events after AM1 varies between 63% and SO%.“-i9 Our figures are in accordance with those results. Differ- ences in the reported results are mainly due to technical hints and diverging definitions of an ischemic response during Ex-Echo. A new-onset wall motion abnormality is universally accepted as a marker of transient myocar- dial ischemia.1x24,25 However, the diagnostic value and the clinical significance of the worsening of a preexisting wall motion abnormality are still under debate.17,19,27-2g Recently, Amese et al29 showed that akinesis becoming dyskinesis during dobutamine-atropine stress echocardi- ography represented a “mechanical phenomena” rather than myocardial ischemia. The significance of light or moderate hypokinesia becoming profound hypokinesia or dyskinesia during stress-echo is still unknown.
Poor correlation between electrocardiographic and echo- can&graphic changes: A poor correlation was found be- tween Ex-ECG and Fx-Echo findings during exercise. This phenomenon has been described for electrocardio- graphic changes’and dipyridamole single-photon emission computed tomography l5 electrocardiographic changes and Ex-Echo, l7 and electrocardiographic changes and dipyridamole stress echocardiography. l5 Our findings con- firmed those reported by others15,i7; however, our rate of cardiac events was higher, and ST-segment depression did predict poor outcomes. Mechanisms by which both tests predicted cardiac events may be different.
Study limitations: A direct assessment of the severity of coronary artery disease and its relationship with stress echocardiography findings could not be established due to the low rate of referrals to coronary angiography. The study was designed to assess the prognosis of patients after AM1 early and noninvasively. As is the case in clin- ical practice, coronary angiograms were performed based on the patient’s clinical symptoms, and not by the designs of the cohort studies or clinical trials. Revascu- larization procedures were not guided by the results of Ex-Echo. However, a positive Fx-Echo result did pre- dict the occurrence of such events, supporting a high cor- relation between Ex-Echo~ test results and severity of coronary artery disease. Thrombolysis did not influence the clinical outcomes or the results of Ex-Echo; the pa- tients were, however, not randomly assigned to specific treatments, and the similarities between groups can be explained just by chance. The study population consist- ed of one third of the screened patients. However, regard- ing mortality, the study’ population and the screened group were similar.
Clinical and econonjc jmpiicatians: Risk stratification by means of predischarge Ex-ECG test only, although highly predictive ih; the present study, has, according to several other studies, a low sensitivity.8-” Klein et a130 showed that exercise-induced ST-segment depression had prognostic value only in patients without pathologic Q waves. In addition, Froelicher et a&l2 in a meta-analy- sis of several studies, showed that exercise-induced ST- segment depression did not give prognostic information.
A predischarge, symptom-limited exercise test per- formed in the early days after AMI is gaining accep- tance. The addition of echocardiography may increase the’safety of this test. In most post-AM1 patients, echo- cardiography is routinely performed. In selected patients, this echocardiogram may’be postponed and performed in connection with exercise testing. This change in rou- tines may result in economic benefits, sparing an initial echocardiogram and avoiding a maximal exercise test 4 to 6 weeks after AMI. Furthermore, in patients with severely abnormal resting electrocardiographic results (precluding the diagnosis of residual ischemia during exercise test), Ex-Echo testing may in part solve this problem. In patients unable or poorly motivated to per- form exercise, pharmacologic stress echocardiography has been shown to be a reasonable altemative.15,26,27
The high accuracy of Ex-Echo to assess every car- diac event and the high positive predictive value of Ex- Echo to assess cardiac events indicates that patients with a positive Ex-Echo should be considered for an early coronary angiography to study the possibility of revas- cularization. The cumulative survival curves separate within the first weeks after infarction (Figure lD), stress- ing the fact that a positive Ex-Echo result should be used as a guide for early intervention. On the other hand, based on the high negative predictive value of Ex-Echo, a negative Ex-Echo result surely reassures a more con- servative approach.
Acknowledgment: We wish to express our thanks to Sven V. Eriksson, MD, PhD, for reviewing this manu-
1120 THE AMERICAN JOURNAL OF CARDIOLOGY@ VOL. 76 DECEMBER 1, 1995

script, and to Carina Hannu, RN, and Anna Pardo, RN, for secretarial assistance.
1. Multicenter Post-Infarction Research Group. Risk stratification and survival after acme myocardial infarction. N Engl J Med 1983;309:331-336. 2. Fioretti P, Brewer RW, Simoons ML, Bos JR, Baardman T, Beelen A, Hugen- holtz PG. Prediction of mortality during the first year after acute myocardial infarc- tion from clinical variables and stress test at hospital discharge. Am J Cardiol 1985;55:1313-1318. 3. Taylor G, Humpries JO, Mellits ED, Pitt B, Dchulza RA, Griffith LX, Achuff SC. Predictors of clinical course, coronary anatomy and left ventricular function after recovery from acute myocardial infarction. Circulation 1980;62:960-970, 4. Nielsen JR, Mickley H, Damsgaard EM, Froland A. Predischarge maxima1 exer- cise test identifies risk for cardiac death in patients with acute myocardial infarc- tion. Am J Cardiol 1990;65:149-153. 5. White HD, Nonis RM, Brown MA, Brandt PW, Whitlock CJ. Left ventricular end-systolic volume as the major determinant of survival after recovery from myo- cardial infarction. Circulation 1987;76:44-51. 6. Quintana M, Lindvall K, Carlens P, Beveglrd S, Brolund F. ST-segment depres- sion on ambulatory electrocardiography in the early in-hospital period after acute myocardial infarction predicts early and late mortality: a short-term and a 3-year follow-up study. C2in Cardiol 1995;18:392-400. 7. Murray DP, Salih M, Tan LB, Deny S, Murray RG, Littler WA. Which exer- cise test variables are of prognostic importance post-myocardial infarctiOn? Inf J Cardiol 1988;20:353-363. 8. Bonaducce D, Petretta M, Labzillo T, Vitagliano G, Bianchi V, Conforti G, Mor- goano G, Arrichiello P. Prevalence and prognostic significance of silent myocar- dial ischaemia detected by exercise test and continuous ECG monitoring after acute myocardial infarction. Eur Heart J 1991;12:186-193. 9. Mickley H, Pless P, Nielssen JR, Beming .I, Miller M. Transient myocardial ischaemia after a first acute myocardial infarction and its relation to clinical char- acteristics, predischarge exercise testing and cardiac events at one-year follow-up. Am J Cardiol 1993;71:139-144. 10. Curie P, Salt&i S. Transient ischaemia after acute myocxdial infarction: rela- tionship to exercise iscliaemia. Eur Heart J 1991;12:395-400. 11. Jereczek M, Andresen D, SchrGder J, VGller H, Briiggemann T, Deutchsmann C, Schriider R. Prognostic value of ischaemia during Halter monitoring and exer- cise testing after acute myocardial infarction. Am J Cardiol 1993;72:8-13. 12. Froelicher VF, Perdue S, Pewen W, Risch M. Application of m&a-analysis using an electronic spread sheet to exercise testing in patients after myocardial infarction. Am J Med 19X7:83:1045-1054. 13. Hung J, Goris ML, Nash E, Kraemer HC, De Busk RF, Berger WI? III, Lew H. Comparative value of maxima1 treadmill testing, exercise thallium myocardial perfusion scintigraphy and exercise radionuclide ventriculography for distinguish- ing high and low-risk patients soon after acute myocardial infarction. Am J Cardi- ol 1984;53:1221-1227. 14. Gibson RS, Watsson DD, Craddock GB, Crampton RS, Kaiser DL, Denny MJ, Belier GA. Prediction of cardiac events after uncomplicated myocardial infarction: a prospective study comparing predischarge exercise thallium-201 scintigraphy and coronary angiography. Circulation 1983;68:321-336. 15. van Daele M, McNeil1 A, Fioretti P, Salustri A, Pozzoli M, El Said M, Reijs A, McFalls E, Slagboom T, Roelandt J. Prognostic value of &pyridamole sestamibi single-photon emission computed tomography and dipyridamole stress echocardi-
ography for new cardiac events after an uncomplicated myocardial infarction. JAm Sot Echocardiogr 1994;7:370-380. 16. Corbett JR, Dehmer GJ, Lewis SE, Woodward W, Henderson E, Parkey RW, Blomqvist CG, Willerson JT. The prognostic value of submaximal exercise testing with radionuclide venticulography before hospital discharge in patients with recent myocardial infarction. Circulation 1981;64:535-544. 17. Ryan T, Armstrong W, O’Donnell 1, Feigenbaum H. Risk stratification after acute myocardial infarction by means of exercise two-dimensional echocardiog- raphy. Am Heart J 1987;114:1305~1316. 18. Applegate RJ, Dell’italia LJ, Crawford MH. Usefulness of two-dimensional echocardiography during low-level exercise testing early after uncomplicated acute myocardial infarction. Am J Cardiol 1987;60:1&14. 19. Jaarsma W, Visser CA, Funke Kupper AJ, Res JCJ, Van Eenige MJ, Roos JP. Usefulness of two-dimensional exercise stress echocardiography shortly after acute myocardial infarction. Am J Cardiol 1986;57:8&90. 20. Schiller N, Shah P, Crawford M, DeMaria A, Devereux R, Feigenbaum H, Gut- segell H, Reichek N, Sahn D, Schnittger I, Silverman N. Recommendations for quan- tification of the left ventricle by two-dimensional echocardiography. American &xi- ety of Echocardiography Committee on Standards, Subcommittee on Quantitation of Two-Dimensional Echocardiograms. JAm Sot Echocardiogr 1989;2:358-367. 21. Amanullah A, Lindvall K. Predischarge exercise echocardiography in patients with unstable angina pectoris who respond to medical treatment. C/in Cardiol1992; 15:417423. 22. Kaplan EL, M&r P. Nonparametric estimation from incomplete observations. J Am Stat Assoc 1958;53:457-481. 23. Christensen E. Multivariate survival analysis using Cox’s regression model. Hepatology 1987;7:134f%1358. 24. Marwick T, Willemart B, D’Hondt AM; Baudhuin T, Wijns W, D&y JM, Melin 1. Selection of the optimal nonexercise stress for the evaluation of ischemic regional myocardial dysfunction and malperfusion. Comparison of dobutamine and adenosine using echocardiography and 99”Tc-MIBI single photon emission com- puted tomography. Circularion 1993;87:345-354. 25. Beleslin B, Ostojic M, Stepanovic J, Djordjevic-Dikic A, Stojkovic S, Nedeljkovic M, Stankovic G, Petrasinovic 2, Gojkovic L, Vasiljevic-Pokrajcic Z, Nedeljkovic M. Stress echocardiography in the detection of myocardial ischemia. Head-to-head comparison of exercise, dobutamine, and dipyridamole tests. Circu- larion 1994;90:1168-1176. 26. Picano E, Landi P, Bolognese L, Chiarandii G, Chiarella F, Seveso G, Sclavo M, Gandolfo N, Previtalli M, Orlandini A, Margaria F, Pirelle S, Magaja OR, Minardi G, Bianchi F, Marini C, Raciti M,.Michelasi C, Severi S, for the EPIC Study Group. Prognostic value of dipyridamole echocardiography early after uncomplicated myo- cardial infarction: a large-scale multicenter trial. Am J Med 1993;95:608-618. 27. Afridi I, Quiiiones M, Zoghbi W, Cheirif B. Dobutamine stress echocardiog- raphy: sensitivity, specificity, and predictive value for future cardiac events. Am Heart J 1994;127:1510-1515. 28. Iliceto S, Galiuto L, Maranguelli V, Rizzon P. Clinical use of stress echocar- diography: factors affecting diagnostic accuracy. Eur Heart J 1994;15:672480. 29. Amex M, Fioretti PM, Come] JH, Postma-Tjoa J, Reijs AEM, Roelandt J. Aki- nesis becoming dyskinesis during high-dose dobutamine stress echocardiography: a marker of myocardial ischemia or a mechanical phenomenon? Am J Cardiol 1994;73:896899. 30. Klein J, Froelicher VF, Detrano R, Dubach P, Yen R. Does the resting elec- trocardiogram after myocardial infarction determine the predictive values of exer- cise-induced ST segment depression? A 2 year follow-up in a veteran population. J Am Cojl Cardiol 1989;14:305-311.
CORONARY ARTERY DISEASE/PROGNOSIS AFTER AMI WITH STRESS ECHO 1121