PROgesterone Therapy for Endometrial Cancer Prevention in Obese Women (PROTEC… · CANCER...
13
CANCER PREVENTION RESEARCH | RESEARCH ARTICLE PROgesterone Therapy for Endometrial Cancer Prevention in Obese Women (PROTEC) Trial: A Feasibility Study A C Abigail E. Derbyshire 1 , Jennifer L. Allen 2 , Matthew Gittins 3 , Bhavna Lakhiani 2 , James Bolton 4 , Joseph Shaw 4 , Philip W. Pemberton 5 , Michelle Needham 6 , Michelle L. MacKintosh 1 , Richard J. Edmondson 1,2 , Henry C. Kitchener 2 , and Emma J. Crosbie 1,2 ABSTRACT ◥ Obesity is the major etiologic driver for endometrial cancer. The levonorgestrel intrauterine system (LNG-IUS) reduces the risk of endometrial cancer and its precursor, atypical hyper- plasia. We assessed feasibility and uptake of the LNG-IUS for primary prevention of endometrial cancer in high-risk women and its impact on endometrial tissue biomarkers. Women with class-III obesity [body mass index (BMI) > 40 kg/m 2 ] and histologically normal endometrium were invited to participate in a clinical trial of the LNG-IUS for endometrial protection. Recruitment, successful LNG-IUS insertion, and adherence to trial procedures were recorded. We measured impact of the LNG-IUS on circulating biomarkers of endometrial cancer risk, endometrial proliferation (Ki-67, pAKT, PTEN), endo- metrial hormone receptor status [estrogen receptor and pro- gesterone receptor (PR)], mental wellbeing, and menstrual function. At 6 months, women chose to keep their LNG-IUS or have it removed. In total, 103 women were approached, 54 were offered a participant information sheet, 35 agreed to participate, and 25 received a LNG-IUS. Their median age and BMI were 54 years [interquartile range (IQR) 52–57] and 47 kg/m 2 (IQR 44–51), respectively. Three women (3/35, 9%) were ineligible due to atypical hyperplasia/endometrial cancer on their baseline biopsy. The LNG-IUS was well tolerated and had a positive overall effect on bleeding patterns and mental wellbeing. The LNG-IUS was associated with endometrial morphologic change, reduced Ki-67, and PR expression, but circulating biomarkers of endometrial cancer risk were unchanged. All but one woman (96%) kept her LNG-IUS. The LNG-IUS appears to be acceptable to some women with class-III obesity for primary prevention of endometrial cancer, which could provide a strategy for a prevention trial. Prevention Relevance: Novel strategies are urgently need- ed to prevent the rise in endometrial cancer diagnoses pre- dicted by escalating obesity rates. Here, we show that women with class III obesity are willing to engage in risk reduction with a levonorgestrel intrauterine system, which could provide a strategy for an endometrial cancer prevention trial. Introduction Endometrial cancer is the sixth most common cancer in women, with more than 382,000 new diagnoses and 89,900 deaths recorded globally in 2018 (1). The incidence of endo- metrial cancer is rising sharply in parallel with escalating obesity rates (2). Obesity is the strongest risk factor for the most common histologic subtype, endometrioid (type I) endo- metrial cancer, and its precursor lesion, atypical hyperplasia (3). Such is the strength of the association that approximately 40% of endometrial cancers are thought to be directly attributable to obesity (4), and a marked dose–response relationship bestows higher risk as body mass index (BMI) rises (5). It has been estimated that women with obesity class III (BMI > 40 kg/m 2 ) have a 7-fold increased risk of endometrial cancer compared with normal weight women (BMI 18.5–25 kg/m 2 ; ref. 3). The biological mechanism responsible for this association relates to the endometrial stimulatory effect of adipose-derived estrogen, which is unopposed by progesterone in an ovulatory and postmenopausal women, and augmented by the negative con- sequences of insulin resistance and chronic inflammation (6). Weight loss achieved and sustained through bariatric surgery reduces endometrial cancer risk (7, 8) with measurable impact on circulating biomarkers of adiposity, reproductive hor- mones, and insulin status, accompanied by downregulation of pro-oncogenic signaling pathways in the endometrium (9). 1 Division of Gynaecology, Manchester University NHS Foundation Trust, Manchester Academic Health Science Centre, Manchester, United Kingdom. 2 Division of Cancer Sciences, Faculty of Biology, Medicine and Health, University of Manchester, St Mary’s Hospital, Manchester, United Kingdom. 3 Centre for Biostatistics, School of Health Sciences, University of Manchester, Manchester Academic Health Science Centre, Manchester, United Kingdom. 4 Department of Histopathology, Manchester University NHS Foundation Trust, Manchester Academic Health Science Centre, Manchester, United Kingdom. 5 Department of Clinical Biochemistry, Manchester University NHS Foundation Trust, Manchester Academic Health Science Centre, Manchester, United Kingdom. 6 Sleep Apnoea Service, Salford Royal Hospitals NHS Foundation Trust, Salford, United Kingdom. Note: Supplementary data for this article are available at Cancer Prevention Research Online (http://cancerprevres.aacrjournals.org/). Corresponding Author: Emma J. Crosbie, University of Manchester, 5th Floor Research, St Mary’s Hospital, Oxford Road, Manchester M13 9WL, United Kingdom. Phone: 44-161-701-6942; Fax: 44-161-701-6919; E-mail: [email protected] Cancer Prev Res 2021;14:263–74 doi: 10.1158/1940-6207.CAPR-20-0248 Ó2020 American Association for Cancer Research. AACRJournals.org | 263 Research. on July 2, 2021. © 2021 American Association for Cancer cancerpreventionresearch.aacrjournals.org Downloaded from Published OnlineFirst September 30, 2020; DOI: 10.1158/1940-6207.CAPR-20-0248
Transcript of PROgesterone Therapy for Endometrial Cancer Prevention in Obese Women (PROTEC… · CANCER...
-
CANCER PREVENTION RESEARCH | RESEARCH ARTICLE
PROgesterone Therapy for Endometrial CancerPrevention in Obese Women (PROTEC) Trial:A Feasibility Study A CAbigail E. Derbyshire1, Jennifer L. Allen2, Matthew Gittins3, Bhavna Lakhiani2, James Bolton4,Joseph Shaw4, Philip W. Pemberton5, Michelle Needham6, Michelle L. MacKintosh1,Richard J. Edmondson1,2, Henry C. Kitchener2, and Emma J. Crosbie1,2
ABSTRACT◥
Obesity is the major etiologic driver for endometrial cancer.The levonorgestrel intrauterine system (LNG-IUS) reduces therisk of endometrial cancer and its precursor, atypical hyper-plasia. We assessed feasibility and uptake of the LNG-IUS forprimary prevention of endometrial cancer in high-risk womenand its impact on endometrial tissue biomarkers.Womenwithclass-III obesity [body mass index (BMI) > 40 kg/m2] andhistologically normal endometriumwere invited to participatein a clinical trial of the LNG-IUS for endometrial protection.Recruitment, successful LNG-IUS insertion, and adherence totrial procedures were recorded. We measured impact of theLNG-IUS on circulating biomarkers of endometrial cancerrisk, endometrial proliferation (Ki-67, pAKT, PTEN), endo-metrial hormone receptor status [estrogen receptor and pro-gesterone receptor (PR)], mental wellbeing, and menstrualfunction.At 6months,women chose to keep their LNG-IUSorhave it removed. In total, 103 women were approached, 54were offered a participant information sheet, 35 agreed toparticipate, and 25 received a LNG-IUS. Their median age and
BMI were 54 years [interquartile range (IQR) 52–57] and47 kg/m2 (IQR 44–51), respectively. Three women (3/35, 9%)were ineligible due to atypical hyperplasia/endometrial canceron their baseline biopsy. The LNG-IUS was well tolerated andhad a positive overall effect on bleeding patterns and mentalwellbeing. The LNG-IUS was associated with endometrialmorphologic change, reduced Ki-67, and PR expression, butcirculating biomarkers of endometrial cancer risk wereunchanged. All but one woman (96%) kept her LNG-IUS.The LNG-IUS appears to be acceptable to some women withclass-III obesity for primary prevention of endometrial cancer,which could provide a strategy for a prevention trial.
Prevention Relevance: Novel strategies are urgently need-ed to prevent the rise in endometrial cancer diagnoses pre-dicted by escalating obesity rates. Here, we show that womenwith class III obesity arewilling to engage in risk reductionwitha levonorgestrel intrauterine system, which could provide astrategy for an endometrial cancer prevention trial.
IntroductionEndometrial cancer is the sixth most common cancer in
women, with more than 382,000 new diagnoses and 89,900
deaths recorded globally in 2018 (1). The incidence of endo-metrial cancer is rising sharply in parallel with escalatingobesity rates (2). Obesity is the strongest risk factor for themost common histologic subtype, endometrioid (type I) endo-metrial cancer, and its precursor lesion, atypical hyperplasia (3).Such is the strength of the association that approximately 40%of endometrial cancers are thought to be directly attributable toobesity (4), and a marked dose–response relationship bestowshigher risk as body mass index (BMI) rises (5). It has beenestimated that women with obesity class III (BMI > 40 kg/m2)have a 7-fold increased risk of endometrial cancer comparedwith normal weight women (BMI 18.5–25 kg/m2; ref. 3). Thebiological mechanism responsible for this association relates tothe endometrial stimulatory effect of adipose-derived estrogen,which is unopposed by progesterone in an ovulatory andpostmenopausal women, and augmented by the negative con-sequences of insulin resistance and chronic inflammation (6).Weight loss achieved and sustained through bariatric surgeryreduces endometrial cancer risk (7, 8) with measurable impacton circulating biomarkers of adiposity, reproductive hor-mones, and insulin status, accompanied by downregulationof pro-oncogenic signaling pathways in the endometrium (9).
1Division of Gynaecology, Manchester University NHS Foundation Trust,Manchester Academic Health Science Centre, Manchester, United Kingdom.2Division of Cancer Sciences, Faculty of Biology, Medicine and Health, Universityof Manchester, St Mary’s Hospital, Manchester, United Kingdom. 3Centre forBiostatistics, School of Health Sciences, University of Manchester, ManchesterAcademic Health Science Centre, Manchester, United Kingdom. 4Department ofHistopathology, Manchester University NHS Foundation Trust, ManchesterAcademic Health Science Centre, Manchester, United Kingdom. 5Department ofClinical Biochemistry, Manchester University NHS Foundation Trust, ManchesterAcademic Health Science Centre, Manchester, United Kingdom. 6Sleep ApnoeaService, Salford Royal Hospitals NHS Foundation Trust, Salford, United Kingdom.
Note: Supplementary data for this article are available at Cancer PreventionResearch Online (http://cancerprevres.aacrjournals.org/).
Corresponding Author: Emma J. Crosbie, University of Manchester, 5th FloorResearch, St Mary’s Hospital, Oxford Road, Manchester M13 9WL, UnitedKingdom. Phone: 44-161-701-6942; Fax: 44-161-701-6919; E-mail:[email protected]
Cancer Prev Res 2021;14:263–74
doi: 10.1158/1940-6207.CAPR-20-0248
�2020 American Association for Cancer Research.
AACRJournals.org | 263
Research. on July 2, 2021. © 2021 American Association for Cancercancerpreventionresearch.aacrjournals.org Downloaded from
Published OnlineFirst September 30, 2020; DOI: 10.1158/1940-6207.CAPR-20-0248
http://crossmark.crossref.org/dialog/?doi=10.1158/1940-6207.CAPR-20-0248&domain=pdf&date_stamp=2021-1-19http://crossmark.crossref.org/dialog/?doi=10.1158/1940-6207.CAPR-20-0248&domain=pdf&date_stamp=2021-1-19http://cancerpreventionresearch.aacrjournals.org/
-
Bariatric surgery is neither available, appropriate, nor accept-able to everyone with an elevated BMI, however, and cannot berecommended solely for the purpose of primary prevention ofendometrial cancer (10). Dietary caloric restriction can facil-itate weight loss, particularly if accompanied by increased levelsof physical activity, but the amount of weight lost and durationof benefit is considerably lower than following bariatric sur-gery (11). Alternative strategies are therefore urgently neededto provide protection to women at greatest risk of endometrialcancer in order to thwart the explosion in incidence ratespredicted by modeling studies (12, 13).The levonorgestrel intrauterine system (LNG-IUS) delivers
progestin directly to the endometrium, counteracting the stim-ulatory effect of estrogen through stromal decidualization, down-regulation of proliferative signaling pathways, and glandularatrophy (14). Epidemiologic studies have shown ever-users ofthe LNG-IUS have a reduced risk of endometrial cancer (15, 16),and severalmeta-analyses havedemonstrated its effectiveness as atherapeutic agent for women with atypical hyperplasia and low-grade cancers confined to the endometrium (17–19). Despitestrong evidence for its anticancer activity, no previous studieshave investigateduse of the LNG-IUSas a chemopreventive agentfor the primary prevention of obesity-driven endometrial cancer.It is not known whether women with a raised BMI are aware oftheir increased risk of endometrial cancer or whether they wouldbe prepared to engage in risk reduction with a LNG-IUS. Inpreparation for a clinical efficacy study, we measured feasibility,participation rate, and compliance with the LNG-IUS for endo-metrial protection inwomenwith class-III obesity.We studied itsshort-term effects on endometrial morphology, proliferation,and hormone receptor status and on circulating biomarkers ofendometrial cancer risk. Further, we explored the impact of theLNG-IUS on menstrual bleeding patterns, as well as mentalwellbeing, through validated questionnaires.
Materials and MethodsStudy governanceThe study was sponsored by Manchester University NHS
Foundation Trust (MFT) and approved by the Cambridge EastResearch Ethics Committee—(15/EE/0063), Medicine andHealthcare Products Regulatory Authority (MHRA, reference21387/0234/001–0001), and local Research and Developmentdepartments. The trial was prospectively registered on theEuropean (EudraCT number 2014–005610–37) and UK(ISRCTN40940943) clinical trial databases and conducted inaccordance with Good Clinical Practice guidelines and theDeclaration of Helsinki.
Study designThis was a single-arm feasibility study of the LNG-IUS for
endometrial protection in women with class III obesity. Wom-en attended clinic at baseline (screening visit, T0), 2�1months(LNG-IUS inserted in clinic, T1), and 8 �3 months (finalassessment, T2; Fig. 1). Serial assessment of anthropometricmeasures (weight, BMI, andwaist:hip ratio), serumbiomarkers
(hormone status, insulin resistance, and adiposity), endome-trial biomarkers (endometrial morphology, hormone receptorstatus, Ki-67 proliferation index, and pro-proliferation signal-ing molecules), menstrual bleeding patterns, and mental well-being was performed at all time points.
Feasibility, willingness to receive, and compliance withthe LNG-IUSWillingness to receive the LNG-IUS for endometrial pro-
tection was determined as the proportion of eligible womenwho agreed to its insertion. The feasibility of using the LNG-IUS in women with class-III obesity was calculated as theproportion of successful LNG-IUS insertions. Complicationsof insertion, side effects, and adverse events were recorded.At T2 final visit, women chose whether to keep theirLNG-IUS for ongoing endometrial protection or have itremoved. Adherence with repeated endometrial samplingand other trial procedures was recorded. Compliance withthe LNG-IUS was calculated as the proportion of womenwho chose to keep their LNG-IUS.
ParticipantsEligible women were ≥18 years of age with a BMI ≥40 kg/m2
and histologically normal endometrium at baseline. All parti-cipants gave written, informed consent. We advertised thestudy on the University of Manchester and MFT websites,Cancer Research UK and UK ISRCTN clinical trials databases,on socialmedia platforms, and byword ofmouth.We recruitedwomen who approached the research team for participationdirectly and those attending gynecology and sleep apneaoutpatient clinics at MFT and Salford Royal Hospitals NHSFoundation Trust, respectively. Exclusion criteria includedprevious hysterectomy; LNG-IUS or other intrauterine devicewithin the past 6 months; planning pregnancy, pregnant, orbreastfeeding; previous endometrial ablation; congenital oracquired uterine anomaly; history of pelvic inflammatorydisease or genital actinomyces; breast cancer; overdue cervicalscreening or last screen abnormal; immunodeficiency; activelytrying to lose weight; contraindications to LNG-IUS, includingcoagulopathy, liver disease, migraine, raised blood pressure,arterial disease, postpartum endometritis, infected abortionduring the past 3 months or recent trophoblastic disease withpersistently elevated hCG levels; and inability to tolerate endo-metrial sampling/ LNG-IUS insertion as an outpatient.
Medical history and baseline safety checkAt baseline, we recorded last menstrual period (LMP),
menstrual bleeding pattern, and contraceptive use. Postmen-opausal status was defined as LMP occurring >1 year before iffollicle-stimulating hormone (FSH), luteinizing hormone(LH), and estradiol levels were confirmatory; the remainingparticipants were considered premenopausal. A urinary preg-nancy test was performed if indicated. Cervical screening wasoffered in accordancewith theNationalHealth Service CervicalScreening program. High vaginal and endocervical swabs weretaken to exclude active lower genital tract infection. Medical
Derbyshire et al.
Cancer Prev Res; 14(2) February 2021 CANCER PREVENTION RESEARCH264
Research. on July 2, 2021. © 2021 American Association for Cancercancerpreventionresearch.aacrjournals.org Downloaded from
Published OnlineFirst September 30, 2020; DOI: 10.1158/1940-6207.CAPR-20-0248
http://cancerpreventionresearch.aacrjournals.org/
-
historywas documented. Screening bloods, including full bloodcount, urea, and electrolytes and liver function tests were takento confirm medical fitness for participation in the trial.
LNG-IUS insertionTheMirena LNG-IUS (Bayer plc)was inserted in clinic at T1;
women were advised to take paracetamol and NSAIDs 1 hourbefore insertion, if not contraindicated. The procedure wascarried out on a colposcopy couch using aWinterton speculumunder aseptic conditions, according to the manufacturer’sinstructions. Safety monitoring was by telephone call at 6,
12, and 18 weeks following LNG-IUS insertion. Side effects,adverse events, and complications were recorded. Participantswere advised to attend their General Practitioner for a coilthread check 4 weeks after LNG-IUS insertion.
Anthropometric measurementsHeight was measured using a stadiometer with shoes
removed. Weight was measured using electronic scales follow-ing removal of bulky clothing and BMI derived using theformula kg/m2. Waist to hip ratio was calculated from waist(midpoint between lower margin of last palpable rib and top of
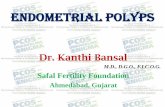
Figure 1.
Study flow chart showing accrual and retention ofparticipants.
PROgesterone Therapy for Endometrial Cancer Prevention
AACRJournals.org Cancer Prev Res; 14(2) February 2021 265
Research. on July 2, 2021. © 2021 American Association for Cancercancerpreventionresearch.aacrjournals.org Downloaded from
Published OnlineFirst September 30, 2020; DOI: 10.1158/1940-6207.CAPR-20-0248
http://cancerpreventionresearch.aacrjournals.org/
-
the iliac crest measured with a tape measure) and hip circum-ference (widest portion of the buttocks).
Blood biomarkersSerum obtained by venepuncture following a 6-hour fast was
used to measure (i) reproductive function (LH; FSH; sexhormone binding globulin, SHBG; testosterone; free androgenindex, FAI; estradiol; progesterone), (ii) insulin resistance[glucose and insulin to derive Homeostasis Model Assessment:Insulin Resistance, HOMA-IR (20); glycosylated hemoglobinA1c, HbA1c), (iii) adiposity (adiponectin, leptin), and (iv)inflammation (C-reactive protein, CRP). With the exceptionof adiponectin and leptin, all analytes were measured usingautomated routine clinical service protocols in the MFT Clin-ical Biochemistry Laboratory. Adiponectin and leptin weremeasured with a DuoSet ELISA development kit (R&DSystems).
Endometrial histopathology and tissue biomarkersEndometrial sampling was performed using a Pipelle
(Carefusion) or MedGyn Endosampler (MedGyn). Premeno-pausal participants were sampled on day 12 �2 of the men-strual cycle, where possible. Endometrial tissue was formalin-fixed, paraffin-embedded, sectioned, and stained with hema-toxylin and eosin. Endometrial morphology was assessed by aconsultant gynecological pathologist. In premenopausal parti-cipants, endometrial morphology and reproductive hormoneprofile was used alongside LMP to determine menstrual cyclephase. Abnormalities were confirmed by a second consultantgynecological pathologist and classified according to WorldHealth Organization guidelines (21, 22).Tissue sections (4 mm) were baked for 30 minutes at 70�C.
The automated Ventana BenchMark Ultra IHC Staining Mod-ule (Ventana Co.) was used with the Ultraview 3, 30 diamino-benzidine (DAB) v3 detection system (Ventana Co.). Tissuesections were deparaffinized and incubated in EZPrep VolumeAdjust (Ventana Co.). A heat-induced antigen retrieval proto-col was carried out using a TRIS–ethylenediamine tetraceticacid–boric acid pH 8 buffer, Cell Conditioner 1 (CC1). Thesections were incubated with ultraviolet inhibitor blocking solu-tion for 4 minutes, followed by an optimized concentration ofantibody (Supplementary Table S1). Sections were then incu-bated with horseradish peroxidase–linked secondary antibody,DAB chromogen, and copper. Counterstain (Hematoxylin II)was applied for 12 minutes before a 4-minute incubation withbluing reagent. Slides were dehydrated through three steps of99% industrial methylated spirits (IMS) and two changes ofXylene. Sections were coverslipped using ClearVue MountXYL (Thermo Scientific). Negative (isotype control) and posi-tive tissue controls were used for quality assurance.The Ki-67 score was the proportion of glandular cells with
positive nuclear staining. TheKi-67 scorewas determined from>1,000 nuclei scored in 3 representative high-powered fields(x20), chosen by the study pathologists; scanty samples werescored in their entirety (23). Estrogen (ER) and progesteronereceptor (PR) staining was assessed by modified H-score (0–
18), the product of area score (proportion of positively stainedtissue, scored 0–6), and intensity of staining score (0 ¼ none,1 ¼ mild, 2 ¼ moderate, and 3 ¼ strong). Phosphorylated (p)AKT staining was scored using the percentage of positivelystained tissue [H¼ (3�% strong staining)þ (2�%moderatestaining) þ (% weak staining)] to account for within tissueheterogeneity (0–300). PTEN status was scored “PTEN null” ifthere were endometrial glands negative for PTEN adjacent topositive stroma. Slides were scored as “PTEN positive” if allendometrial glands expressed PTEN (24). Scoring was per-formed manually by two independent scorers who wereblinded to time point. Discrepant scores (>10% or disagree-ment as to PTEN status) were reviewed and resolved byconsensus agreement.
Menstrual blood loss and mental wellbeing assessmentTwo validated questionnaires, the Hospital Anxiety and
Depression Scale (HADS; refs. 25, 26) and Warwick–Edinburgh Mental Wellbeing Scale (WEMWBS; refs. 27, 28),were completed at baseline and follow-up to determine wheth-er the LNG-IUS had an impact on mental wellbeing. For theHADS, different cutoffs are indicative of a mental healthdisorder, depending on clinical context (26), but lower scoresindicate absent or lower severity of symptoms. For theWEMWBS, the mean score in the general population is 51,with higher scores reflecting improved mental wellbeing (27).Premenopausal participants completed theMenstrual BleedingQuestionnaire (29) at baseline and follow-up.
Sample size considerationsThis was a preliminary study designed to inform recruitment
rates, feasibility of and likely adherence to a clinical efficacy trialof the LNG-IUS for endometrial protection in women withclass-III obesity. We considered that a clinical efficacy trialcould be successfully conducted if >50% of eligible womenagreed to participation, >50% of those eligible had a LNG-IUSsuccessfully fitted, and >75% of women kept their LNG-IUS for>6 months. We also measured LNG-IUS–induced change incirculating and tissue biomarkers to inform intermediarybiomarker endpoints for our definitive study. We did notperform a formal sample size calculation and planned thepragmatic recruitment of 30 to 40 women over a 6- to 12-month recruitment period.
Statistical analysisStatistical analyses were performed using GraphPad Prism
5.0b forMac (GraphPad Software) and SPSS 23.0 forMac (IBMCorp.). Descriptive statistics included mean and SD for nor-mally distributed, and median and interquartile range (IQR)for nonnormally distributed, data. Within-individual changesover time were compared using paired t test and Wilcoxonsigned-rank test for normally distributed and nonnormallydistributed data, respectively. To assess the short-term impactof the LNG-IUS on endometrial proliferation, a mixed effectsregression model was fitted, with Ki-67 score set as the depen-dent variable, time point (baseline set as reference category) as
Derbyshire et al.
Cancer Prev Res; 14(2) February 2021 CANCER PREVENTION RESEARCH266
Research. on July 2, 2021. © 2021 American Association for Cancercancerpreventionresearch.aacrjournals.org Downloaded from
Published OnlineFirst September 30, 2020; DOI: 10.1158/1940-6207.CAPR-20-0248
http://cancerpreventionresearch.aacrjournals.org/
-
the predictor of interest and the covariates baseline Ki-67 score,age, menopausal status (pre/post), smoking (never, ever, cur-rent), type II diabetes mellitus (yes/no) baseline BMI, andbaseline waist:hip ratio. A further analysis was performed thatincluded weight at follow-up, to determine if change in weightwas responsible for change in Ki-67 at outcome. To account forrepeated measures within participants, a random effect inter-cept was included to account for the within subject versusbetween subject variation. To account for possible departuresin normality, a cluster bootstrapping procedure was employedwith 1,000 replications. In an effort to emphasize clinicallyover statistically important effects, data are reported in termsof mean difference effect estimates and 95% confidence inter-vals (CI).
ResultsStudy populationBetween October 2015 and September 2016, 103 women
were approached, 54 were offered a participant informationsheet, 35 agreed to participate, and 25 received a LNG-IUS(Fig. 1). Forty-nine women (48%) were ineligible to receive theparticipant information sheet for the following reasons: LNG-IUS in situ (n¼ 13); previous hysterectomy (n¼ 12); pendingbariatric surgery (n ¼ 10); social/capacity reasons (n ¼ 7);LNG-IUS contraindicated (n¼ 4), or BMI < 40 kg/m2 (n¼ 3).Nineteen women (35%) declined participation for the follow-ing reasons: none given (n ¼ 8); declined device (n ¼ 3);declined “hassle” (n¼ 3); declined procedures (n¼ 3), or otherreasons (n¼ 2). Thus 35 of 54 (65%) eligible women consentedto the baseline screening assessment, 10 of 35 (29%) eitherfailed screening or withdrew their consent, and 25 of 35 (71%)proceeded to LNG-IUS insertion. Three of the six screenfailures (3/35, 9%) had occult atypical hyperplasia or endome-trial cancer on their baseline biopsy. All four withdrawals (4/35,11%) found baseline endometrial sampling too painful toconsider further procedures. Our final study population com-prised 25 women with a median age and BMI of 54 years (IQR52–57) and 47 kg/m2 (IQR 44–51), respectively (Table 1).There were no significant differences between women whoconsented to participate and women who declined in terms ofage (54 vs. 52 years), BMI (47 vs. 46 kg/m2), or ethnicity/race(all except three were White British). Nine (36%) were pre-menopausal but just 4 had regular menstrual cycles; most wereeither amenorrheic (2/12) or experienced irregular menstrualbleeding (3/12). Four (16%) were using hormone replacementtherapy (3/25, 12%) or oral contraceptives (1/25, 4%) atbaseline, which they continued throughout the trial. All hadat least one comorbidity, most commonly type II diabetes (10/25, 40%), hypertension (15/25, 60%), or asthma (8/25, 32%),and 48% had more than three comorbidities.
Compliance with intervention and study proceduresAll 25 women received the LNG-IUS in clinic without
complication. There were no insertion failures, expulsions,
uterine perforations, or lost devices. One woman (4%) devel-oped mild symptoms of endometritis following LNG-IUSinsertion, which was treated with oral antibiotics. One patientcomplained of pelvic discomfort/mild pain following LNG-IUSinsertion that settled with oral analgesia. Other adverse andserious adverse events, specifically urinary tract infection (1/25,4%), vasculitis (1/25, 4%), sciatica (1/25, 4%), and attemptedsuicide (1/25, 4%), were not thought to be related to the LNG-IUS.Allwomenkept their LNG-IUSuntil theirfinal assessmentwhen one woman (4%) chose to have it removed (“easier nowthan later”); the remaining 24 women (96%) kept their LNG-IUS for ongoing endometrial protection. All 25 women werecompliant with study procedures, including sequential endo-metrial biopsies (all 3 biopsies taken, 25/25).
Endometrial morphology and biomarkersThree of 35 participants (9%) had an incidental finding of
atypical hyperplasia or endometrial cancer on a pre–LNG-IUSbiopsy andwere excluded from the study. All other women hadhistologically normal endometrium at T0 (baseline) and T1(time of LNG-IUS insertion). Many of the samples were scanty.Morphology was consistent with menopausal status and/orreported phase ofmenstrual cycle, as appropriate. At follow-up(T2), all endometrial biopsies showed stromal decidualizationand glandular atrophy, consistent with the progesterone effectassociated with LNG-IUS treatment.
Table 1. Baseline characteristics of the study population.
Median age (IQR), years 54 (52–57)White British, n (%) 24 (96)Median weight (IQR), kg 124 (111–143)Median BMI (IQR), kg/m2 47 (44–51)Median waist:hip ratio (IQR) 0.87 (0.83–0.93)Menopausal status, n (%)
Premenopausal 9 (36)Postmenopausal 16 (64)
Menstrual cycle, n (%)Amenorrheic 2 (8)Regular 4 (16)Irregular 3 (12)
Parity, n (%)0 1 (4)1 6 (24)2 10 (40)3þ 8 (32)
Exogenous hormones, n (%) 4 (16)Polycystic ovary syndrome (PCOS), n (%) 6 (24)Comorbidities, n (%)
Hypertension 15 (60)Type II diabetes mellitus 10 (40)Hypercholesterolemia 5 (20)Gallbladder/liver disease 5 (20)Thromboembolic disease 3 (12)Asthma/COPD 8 (32)Sleep apnea 9 (36)Osteoarthritis 15 (60)Depression/anxiety 8 (32)
PROgesterone Therapy for Endometrial Cancer Prevention
AACRJournals.org Cancer Prev Res; 14(2) February 2021 267
Research. on July 2, 2021. © 2021 American Association for Cancercancerpreventionresearch.aacrjournals.org Downloaded from
Published OnlineFirst September 30, 2020; DOI: 10.1158/1940-6207.CAPR-20-0248
http://cancerpreventionresearch.aacrjournals.org/
-
The LNG-IUS was associated with a significant decrease inendometrial proliferation as assessed by Ki-67 score. ThemeanKi-67 score was 27.1% (SD 23.4) at baseline, 21.8% (SD 14.8) atthe time of LNG-IUS insertion, and 12.7% (SD 10.9) at follow-up. A mixed effects regression model adjusting for withinparticipant clustering, potential confounders, and weightchange between time points is shown in Table 2. Betweenbaseline (T0) and time of LNG-IUS insertion (T1) and betweenbaseline (T0) and follow-up (T2), the change inKi-67 scorewas�5.4% (95%CI,�17.1%, 6.3%) and�14.6% (�25.3%,�3.9%),respectively. These results were consistent across all threemodels, indicating that potential sources of confounding,including change in weight during follow-up, had little effecton Ki-67 score. PR expression decreased with LNG-IUS treat-ment (Table 3). There was no significant change in expressionof the other endometrial biomarkers, estrogen receptor, PTEN,or pAKT. Interestingly, all three women excluded because ofoccult endometrial abnormalities had PTEN-null glands, and afurther 2 of 25 participants in the study had PTEN-null glandsbefore but not after LNG-IUS insertion.
Anthropometric and circulating biomarkers ofendometrial cancer riskOverall, women lost weight during the trial, although this
was not clinically significant [median weight 124.4 kg (IQR111–143), 123.9 kg (IQR 111–142), and 123 kg (IQR 111–144)at T0, T1, and T2, respectively]. There were no clinicallysignificant changes in circulating biomarkers of reproductivefunction, insulin resistance, adiposity, or inflammation acrossthe three time points (Table 3), with the notable exception of
altered serum FSH, LH, and progesterone levels over time,which likely reflect natural reproductive aging in our perimen-opausal cohort.
Menstrual bleeding and mental wellbeingOf the 9 premenopausal participants, 2 (22%) were amen-
orrheic, 4 (44%) had regular, and 3 (33%) irregular menstrualbleeding at baseline. As expected, the 7 women who experi-enced menstrual bleeding reported a significant reduction inblood loss with the LNG-IUS; all but two became amenorrheicaccording to the Menstrual Bleeding Questionnaire. Mentalwellbeing improved with the LNG-IUS according to both theWEMWBS andHADS scales (Table 4). A change in score of 2–3 points is clinically significant, but did not reach statisticalsignificance, most likely because of small numbers.
DiscussionThe PROTEC trial was undertaken to assess the feasibility of
a future clinical efficacy trial of the LNG-IUS for endometrialprotection in women with class-III obesity. In a 12-monthrecruitment period, we approached 103 women, 54 (52%) ofwhommet the inclusion criteria, 35 (65%) agreed to participate,and 25 (71%) proceeded to LNG-IUS insertion. There were noinsertion failures, and all women were fully compliant with allstudy procedures, including an endometrial biopsy at the finalvisit. There were no related serious adverse events but one caseeach of endometritis and postinsertion pain, both recognizedcomplications of LNG-IUS treatment. We observed no detri-mental impact of the LNG-IUS on mental wellbeing and self-
Table 2. Mixed effects regression model reporting change in Ki-67 score over time.
Ki-67 score (number of observations ¼ 71)Factor Category Coef (95% CI)a Coef (95% CI)b Coef (95% CI)c
Time point T0—Baseline (Ref) - - -T1—LNG-IUS �5.27 (�16.9, 6.39) �5.37 (�17.1, 6.33) �5.76 (�17.5, 5.99)T2—Follow-up �14.4 (�25.1, -3.62) �14.6 (�25.3, -3.91) �15.3 (�25.9, �4.58)
Baseline age - 0.69 (�0.50, 1.85) 0.77 (�0.49, 2.04)Baseline weight - �0.26 (�0.90, 0.38) �0.32 (�0.98, 0.33)Baseline BMI - 0.94 (�1.00, 2.82) 1.09 (�0.84, 3.03)Smoker Never (Ref.) - -
Ever - 3.54 (�7.70, 14.8) 3.21 (�8.02, 14.4)Yes - 7.34 (�4.80, 19.5) 7.92 (�4.28, 20.1)
Type II diabetes mellitus No (Ref.) - -Yes - �2.73 (�10.9, 5.49) �2.23 (�10.8, 6.30)
Menopause status Post (Ref.) - -Pre - 5.56 (�3.80, 14.9) 5.42 (�4.16, 15.0)
Change in weight - - �0.41 (�1.50, 0.68)Constant 27.1 (17.8, 36.4) �23.82 (�107, 58.9) �28.5 (�117, 560.0)Random effects (Bootstrapped)Variance constant 7.17E-12 2.38E-11 2.69E-11Variance residuals 285.4 290.3 290.8Intraclass correlation 1.47E-13 8.20E-14 9.25E-14
aMixed model with time of assessment only adjusted for within participant clustering.bMixed model with time of assessment adjusted for within participant clustering and baseline screening characteristics.cMixed model with time of assessment adjusted for within participant clustering, baseline screening characteristics, and change in weight from baseline.
Derbyshire et al.
Cancer Prev Res; 14(2) February 2021 CANCER PREVENTION RESEARCH268
Research. on July 2, 2021. © 2021 American Association for Cancercancerpreventionresearch.aacrjournals.org Downloaded from
Published OnlineFirst September 30, 2020; DOI: 10.1158/1940-6207.CAPR-20-0248
http://cancerpreventionresearch.aacrjournals.org/
-
reported menstrual bleeding profiles improved for our pre-menopausal participants. These data suggest that women atgreatest risk of obesity-driven endometrial cancer are willing toengage in risk reduction with a LNG-IUS and that a clinicalefficacy trial could be feasible. Roughly a quarter of womenapproached for the trial had a LNG-IUS inserted, indicating arelatively high proportion of screen failures and noncontinua-tion rate. These findings must be factored in to the design of aclinical efficacy trial.To determine the short-term impact of the LNG-IUS on
biomarkers of endometrial cancer risk, we measured change inanthropometric variables, reproductive hormones, insulinresistance, endometrial morphology, and glandular prolifera-tion status between baseline, 2 months, and 8 months. Aspredicted, we observed stability in these biomarkers prior toLNG-IUS insertion. Short-term treatment with the LNG-IUSwas associated with changes in endometrial morphology,
reduced proliferation, and PR expression; there were no asso-ciated changes to circulating hormone levels, measures ofinsulin resistance, or adiposity. An unexpected finding wasthat women lost an average 2.5 kg in weight during the study;however, this was neither clinically nor statistically significant.Given our conviction that women with class-III obesity are atsufficiently high risk of endometrial cancer that they wouldbenefit from risk-reducing measures, it is striking that 3 of 35(9%) of our participants had an incidental finding of atypicalendometrial hyperplasia or endometrioid endometrial cancerat baseline, requiring hysterectomy. This is consistent with ourprevious study that found 10 of 72 (14%) women with class-IIIobesity referred for weight loss management had occult under-lying endometrial neoplasia (9).Endometrial glands are clonal cell populations that frequent-
ly harbor driver mutations in cancer genes (30). PTEN-nullglands confer a proliferative advantage, predisposing to
Table 3. Changes in anthropometric, blood, and endometrial tissue biomarkers over time.
T0—baseline n ¼ 25 T1—LNG-IUS n ¼ 25 T2—follow-up n ¼ 25Anthropometric measures, mean (SD)
Weight, kg 129.1 (19.2) 128.3 (19.4) 126.7 (19.2)BMI, kg/m2 48.3 (6.3) 48.0 (6.4) 47.5 (6.7)Waist:hip ratio 0.9 (0.07) 0.88 (0.07) 0.87 (0.07)
Blood biomarkers of reproductive function, mean (SD)Estradiol, pmol/L 11.8 (6.6) 9.7 (5.5) 10.1 (6.0)Progesterone, ng/mL 3.1 (2.8) 3.8 (3.8) 1.4 (1.0)Testosterone, nmol/L 7.1 (3.6) 6.3 (3.4) 6.8 (3.7)SHBG, nmol/L 43.6 (28.8) 44.6 (24.7) 41.6 (21.9)FAI 3.1 (2.7) 2.5 (2.2) 2.6 (1.8)LH, IU/L 18.5 (13.1) 17.1 (12.8) 23.3 (16.1)FSH, IU/L 28.8 (23.0) 27.9 (21.7) 35.1 (23.8)
Blood biomarkers of insulin resistance, mean (SD)Glucose, mmol/L 5.5 (0.8) 5.5 (1.0) 5.5 (0.9)Insulin, mU/L 139.0 (122.6) 123.1 (78.8) 124.9 (110.8)HOMA 12.5 (7.1) 28.0 (24.3) 33.8 (34.9)HbA1c, mmol/mol 41.9 (8.2) 41.7 (9.3) 42.2 (9.5)
Blood biomarkers of adiposity, mean (SD)Adiponectin, mg/L 5.6 (13.4) 3.6 (3.7) 3.2 (4.1)Leptin, ng/mL 77.3 (35.2) 82.9 (46.0) 83.4 (41.4)
Blood biomarkers of inflammation, mean (SD)CRP, mg/L 9.0 (4.1) 6.2 (3.3) 7.3 (4.0)
Tissue biomarkers, mean (SD)Ki-67 score (%) 27.1 (23.4) 21.8 (14.8) 12.7 (10.9)pAKT H-score 105.5 (49.9) 89.4 (38.3) 93.1 (40.6)Estrogen receptor (ER) H-score 0.8 (0.1) 0.9 (0.1) 0.8 (0.1)PR H-score 0.8 (0.2) 0.9 (0.1) 0.4 (0.2)Any PTEN-null glands (n, % participants) 2 (8%) 2 (8%) 0 (0%)
Table 4. Changes in mental wellbeing and quality of life over time.
WEMWBS HADS
All participants n ¼ 25 Subset of participantsa n ¼ 17 All participants n ¼ 25 Subset of participantsa n ¼ 17Baseline (T0) Mean score (SD) 45.4 (10.6) 47.3 (10.9) 17.1 (10.4) 12.3 (9.3)Follow-up (T2) Mean score (SD) 47.9 (9.1) 52 (10.9) 14.9 (9.5) 11.4 (8.8)
aAfter excluding women with known depression/anxiety disorder.
PROgesterone Therapy for Endometrial Cancer Prevention
AACRJournals.org Cancer Prev Res; 14(2) February 2021 269
Research. on July 2, 2021. © 2021 American Association for Cancercancerpreventionresearch.aacrjournals.org Downloaded from
Published OnlineFirst September 30, 2020; DOI: 10.1158/1940-6207.CAPR-20-0248
http://cancerpreventionresearch.aacrjournals.org/
-
endometrial carcinogenesis, and have been shown to persistbetween menstrual cycles, but only a small proportion pro-gresses to endometrial cancer (31). We found PTEN-nullglands in all three women with occult endometrial abnormal-ities and in two participants with histologically normalendometrium before, but not after, LNG-IUS insertion. Thisis consistent with the hypothesis that PTEN-null glandsin morphologically normal endometrium represent latentendometrial cancer precursors that regress with LNG-IUStreatment (24).Although the endometrial impact of the LNG-IUS is well
studied (32, 33), this is the first trial to offer the LNG-IUS towomen with class-III obesity for the primary prevention ofendometrial cancer. Confirmation that the expected endome-trial effects of the LNG-IUS are observed in this population isimportant given their defining characteristics, specifically theirclass-III obesity and amenorrhea or irregular menstrual bleed-ing, which distinguish them from regular users of the device. Itis known that Ki-67 score is higher in endometrium harvestedfrom women with obesity compared with that collected fromnormal weight women (34). We considered that the expectedchange in endometrial morphology, a reduction in glandularproliferation as assessed by Ki-67 score, and downregulation ofendometrial progesterone receptors would confirm the utilityof the LNG-IUS at standard doses in this population. We alsoquantified theKi-67 drop at 6months post–LNG-IUS insertionfor the purposes of developing an intermediary molecularendpoint for a definitive trial of the LNG-IUS for endometrialprotection uponwhich a sample size calculation could be based.It is interesting that the 15%Ki-67 drop observed after 6-monthtreatment with the LNG-IUS was similar to that observed afteran average bariatric surgery–induced weight loss of 22 kg at2 months in women with class-III obesity (9). Bariatric surgeryis known to reduce endometrial cancer risk (7, 8, 35), andalthough the mechanisms underlying risk reduction are notfully understood, it is thought that downregulation of endo-metrial pro-proliferative signaling pathways could be impor-tant (9, 36). Ki-67 is only expressed by proliferating cells, ahallmark of cancer; indeed, Ki-67 is known to differentiatebenign from malignant endometrium, with higher Ki-67scores observed in high-grade, advanced stage cancer andcorrelating with poor survival outcomes in this group (37).We considered that a reduction in glandular proliferationin benign peri- and postmenopausal endometrium couldreduce the risk of mutational events that trigger malignanttransformation (10).We have demonstrated proof of principle that some women
at high risk of obesity-driven endometrial cancer are preparedto engage in risk reduction with a LNG-IUS, paving the way fora clinical efficacy trial in this population. Despite concerns thatLNG-IUS insertion would be challenging in the outpatientsetting in postmenopausal women with class-III obesity, wehad no insertion failures, consistent with previous studies (38).Concerns that uterine instrumentation would be unacceptableto women who did not have a gynecological complaint were
also unsubstantiated, with 32 of 35 (91%) participants con-senting to and undergoing three sequential biopsies, withoutcomplication. Further, we found the LNG-IUS was not asso-ciatedwith a detrimental impact onmental wellbeing using twovalidated questionnaires, with even some suggestion that men-tal wellbeing improved during the trial, possibly due toimproved menstrual bleeding profiles and peace of mindregarding endometrial health; indeed 24 of 25 (96%) partici-pants chose to keep their LNG-IUS at the end of the trial forongoing endometrial protection. A short-term study of thiskind cannot confirm that women will be compliant with theLNG-IUS in the medium to long-term, however. Nor can ithelp define the optimal duration of a clinical efficacy trial. Wedid not deliberately target perimenopausal women for trialparticipation, although long-term use of the LNG-IUS in aclinical efficacy trial would ideally avoid women whose com-pliance could be compromised by future pregnancy plans. Thesingle-center nature of this research is a limitation of the study,because we cannot necessarily extrapolate feasibility of ourapproach to other centers, countries, or healthcare settings. Thelack of racial and ethnic diversity in our study populationprecludes any insight into the acceptability and uptake of theLNG-IUS for uterine protection in non-White British women.We do not know whether women would consent to random-ization to a no intervention arm, which would be the idealclinical efficacy trial design, and would certainly affect feasi-bility of the definitive study. Furthermore, our biomarkerfindings should be interpreted with caution given the smallsample size and marked heterogeneity of participating womenwith respect to age, menopausal status, and use of exogenoushormones at baseline.Although invasive, the advantage of the LNG-IUS is that it
releases a continuous supply of levonorgestrel directly to theendometrium, avoiding the peaks and troughs observed withoral administration and eliminating compliance issues (39).Apart from insertion problems, there are few contraindicationsto its use, at least partly because systemic concentrations of thedrug are much lower than those achieved with oral adminis-tration (40). Serum levonorgestrel levels are 20-fold lower inLNG-IUS users than levonorgestrel-containing combined oralcontraceptive pill users, for example (41). There is an inversecorrelation between serum levonorgestrel concentrationsand BMI (42), suggesting even lower systemic levels in ourpopulation. A further advantage of the LNG-IUS for thisindication is that it would be expected to eradicate or treatlatent endometrial cancer precursors, atypical hyperplasia,and occult obesity-driven endometrial cancer, as previouslydemonstrated (24, 17–19). Regression of established endome-trial abnormalities takes 6 to 12 months or longer and is morelikely in the case of atypical hyperplasia (approximately 90%complete response rate) than early stage endometrial cancer(67% complete response rate; ref. 43). There are currently novalidated biomarkers that predict LNG-IUS response to estab-lished disease (44), although some show promise (45, 46),mandating careful assessment of any new bleeding that
Derbyshire et al.
Cancer Prev Res; 14(2) February 2021 CANCER PREVENTION RESEARCH270
Research. on July 2, 2021. © 2021 American Association for Cancercancerpreventionresearch.aacrjournals.org Downloaded from
Published OnlineFirst September 30, 2020; DOI: 10.1158/1940-6207.CAPR-20-0248
http://cancerpreventionresearch.aacrjournals.org/
-
develops following device-induced amenorrhea (47) in anendometrial cancer prevention trial.Overall, we found the LNG-IUS to be safe and well-
tolerated, with no unacceptable side effects in our studypopulation. This is particularly important if the LNG-IUS isbeing used for endometrial protection rather than an estab-lished clinical indication, and should be a focus of futurework. There is no evidence that the LNG-IUS increases therisk of cardiometabolic disorders in obese women (48), but arecent systematic review found LNG-IUS users have a mod-estly increased breast cancer risk [OR ¼ 1.16 (95% CI, 1.06–1.28), I2 ¼ 78%, P < 0.01], although most of the includedstudies failed to adjust for BMI (49). Clearly this is animportant area for further research. The LNG-IUS mayprevent the endometrial consequences of excess adiposity,but it does not address the cardiovascular or metabolicsequelae of obesity and competing risks for death.In summary, identifying women at greatest risk of endome-
trial cancer and developing evidence-based prevention strat-egies are important given the escalating rates of obesity andassociated emerging epidemic of endometrial cancer across theworld (50). The LNG-IUSmay be an effective deterrent againstobesity-driven endometrial cancer and offer endometrial pro-tection for those at highest risk. It reduces risk in the generalpopulation by 50% during and for at least 5 years afterdiscontinuation of its use (16), and as such is likely to be acost-effective prevention strategy for women with class-IIIobesity (51). Here, we demonstrate that a LNG-IUS is accept-able to some women with class-III obesity and that a clinicalefficacy trial would be feasible. The specifics of trial designrequire careful consideration because a large cohort withsufficient follow-up will be challenging and expensive toachieve. Minimizing trial size, duration of follow-up, and costis an important goal for women, researchers, and funders ofsuch a trial. Although endometrial cancer risk is high inwomenwith class-III obesity, absolute risk is modulated by reproduc-tive, metabolic, and genetic factors (13, 52), as well as com-peting risks for death. More sophisticated risk predictionmodels, calibrated for clinical use, must now be developed toestablish the optimal prevention trial target population, max-imize the benefits of participation, and reduce unnecessaryharms (53).
Authors’ DisclosuresR.J. Edmondson reports personal fees from Astra Zeneca, personal fees
from Arquer Diagnostics, and grants from Tesaro Inc. outside the sub-mittedwork.H.C.Kitchener reports grants fromWilliamWalterWill Trustand grants fromCentral Manchester Foundation Trust during the conductof the study. No disclosures were reported by the other authors.
Authors’ ContributionsA.E. Derbyshire: Data curation, formal analysis, investigation, writing-
original draft, writing-review and editing. J.L. Allen:Data curation, writing-review and editing.M.Gittins: Formal analysis, supervision, writing-reviewand editing. B. Lakhiani: Data curation, writing-review and editing.J. Bolton: Data curation, formal analysis, writing-review and editing.J. Shaw: Formal analysis, writing-review and editing. P.W. Pemberton:Data curation, writing-review and editing. M. Needham: Data curation,supervision, writing-review and editing. M.L. MacKintosh: Supervision,writing-review and editing. R.J. Edmondson: Supervision, writing-reviewand editing. H.C. Kitchener: Conceptualization, resources, supervision,funding acquisition, writing-original draft, writing-review and editing.E.J. Crosbie: Conceptualization, resources, supervision, fundingacquisition,methodology, writing-original draft, writing-review and editing.
AcknowledgmentsWe would like to thank the women who participated in this study. We
are grateful to all the clinical staff involved in their carewhohelped facilitaterecruitment, especially Samantha Johnson and Bryan Wilson. We wouldparticularly like to thank Linsey Nelson, who contributed to study set-up,and Tina Pritchard, who supported patient recruitment, provided nursingcare, and helped with administrative tasks. We are grateful to the inde-pendent members of the Trial Steering Committee, Professor SudhaSundar, ProfessorMartin Rutter, Professor Steve Roberts, and Anne Lowryfor providing study oversight.
A.E. Derbyshire was a Manchester University NHS Foundation TrustClinical Research Fellow and E.J. Crosbie an NIHR Clinician Scientist(NIHR-CS-012–009), and their work was supported through the NIHRManchester Biomedical Research Centre (IS-BRC-1215–20007) and theWilliam Walter Will Trust. This article presents independent researchfunded by the NIHR. The views expressed are those of the authors and notnecessarily those of the NHS, NIHR, or the Department of Health.
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
ReceivedMay 18, 2020; revised August 22, 2020; accepted September 16,2020; published first September 30, 2020.
References1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global
cancer statistics 2018: GLOBOCAN estimates of incidence and mor-tality worldwide for 36 cancers in 185 countries. CA Cancer J Clin2018;68:394–424.
2. Crosbie EJ,Morrison J. The emerging epidemic of endometrial cancer:time to take action. Cochrane Database Syst Rev 2014;12:ED000095.
3. Setiawan VW, Yang HP, Pike MC, McCann SE, Yu H, Xiang YB, et al.Type I and II endometrial cancers: have they different risk factors?J Clin Oncol 2013;31:2607–18.
4. Arnold M, Pandeya N, Byrnes G, Renehan AG, Stevens GA, Ezzati M,et al. Global burden of cancer attributable to high body-mass index in2012: a population-based study. Lancet Oncol 2015;16:36–46.
5. Crosbie EJ, Zwahlen M, Kitchener HC, Egger M, Renehan AG. Bodymass index, sex hormone-related states and endometrial cancer risk: ameta-analysis. Cancer Epidemiol Biomarkers Prev 2010;19:3119–30.
6. Calle EE, Kaaks R. Overweight, obesity and cancer: epidemiologicalevidence and proposed mechanisms. Nat Rev Cancer 2004;4:579–91.
7. Ward KK, Roncancio AM, Shah NR, Davis MA, Saenz CC, McHaleMT, et al. Bariatric surgery decreases the risk of uterine malignancy.Gynecol Oncol 2014;133:63–6.
8. Anveden A, Taube M, Peltonen M, Jacobson P, Andersson-AssarssonJC, Sjoholm K, et al. Long-term incidence of female specific cancerafter bariatric surgery or usual care in the Swedish Obese SubjectsStudy. Gynecol Oncol 2017;145:224–9.
PROgesterone Therapy for Endometrial Cancer Prevention
AACRJournals.org Cancer Prev Res; 14(2) February 2021 271
Research. on July 2, 2021. © 2021 American Association for Cancercancerpreventionresearch.aacrjournals.org Downloaded from
Published OnlineFirst September 30, 2020; DOI: 10.1158/1940-6207.CAPR-20-0248
http://cancerpreventionresearch.aacrjournals.org/
-
9. MacKintoshML, Derbyshire AE,McVey RJ, Bolton J, Nickkho-AmiryM, Higgins CL, et al. The impact of obesity and bariatric surgery oncirculating and tissue biomarkers of endometrial cancer risk. Int JCancer 2019;144:641–650.
10. MacKintosh ML, Crosbie EJ. Obesity-driven endometrial cancer: isweight loss the answer? BJOG 2013;120:791–4.
11. Bischoff SC, Damms-Machado A, Betz C, Herpertz S, Legenbauer T,L€ow T, et al. Multicenter evaluation of an interdisciplinary 52-weekweight loss program for obesity with regard to body weight, comorbid-ities and quality of life - a prospective study. Int J Obes 2012;36:614–24.
12. Rahib L, Smith BD, Aizenberg R, Rosenzweig AB, Fleshman JM,Matrisian LM. Projecting cancer incidence and deaths to 2030: theunexpected burden of thyroid, liver, and pancreas cancers in theUnited States. Cancer Res 2014;74:2913–21.
13. Kitson S, Evans DG, Crosbie EJ. Identifying high risk women forendometrial cancer prevention strategies: proposal of endometrialcancer risk prediction model. Cancer Prev Res 2017;10:1–13.
14. Bahamondes L, Valeria Bahamondes M, Shulman LP. Non-contraceptive benefits of hormonal and intrauterine reversible con-traceptive methods. Hum Reprod Update 2015;21:640–51.
15. Jareid M, Thalabard JC, Aarflot M, Bovelstad HM, Lund E, Braaten T.Levonorgestrel-releasing intrauterine system use is associated with adecreased risk of ovarian and endometrial cancer, without increasedrisk of breast cancer. results from the NOWAC study. Gynecol Oncol2018;149:127–32.
16. Soini T, Hurskainen R, Grenman S,Maenpaa J, Paavonen J, Pukkala E.Cancer risk in women using the levonorgestrel-releasing intrauterinesystem in Finland. Obstet Gynecol 2014;124:292–9.
17. Wan Y-L, Holland C. The efficacy of levonorgestrel intrauterinesystems for endometrial protection: a systematic review. Climacteric2011;14:622–32.
18. Gunderson CC, Fader AN, Carson KA, Bristow RE. Oncologic andreproductive outcomes with progestin therapy in women with endo-metrial hyperplasia and grade 1 adenocarcinoma: a systematic review.Gynecol Oncol 2012;125:477–82.
19. Yuk JS, Song JY, Lee JH, Park WI, Ahn HS, Kim HJ. Levonorgestrel-releasing intrauterine systems versus oral cyclic medroxyprogesteroneacetate in endometrial hyperplasia therapy: a meta-analysis. Ann SurgOncol 2017;24:1322–1329.
20. Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF,Turner RC. Homeostasis model assessment: insulin resistance andbeta-cell function from fasting plasma glucose and insulin concentra-tions in man. Diabetologia 1985;28:412–9.
21. Emons G, Beckmann MW, Schmidt D, Mallmann PUterus commis-sion of the Gynecological Oncology Working Group (AGO).New WHO classification of endometrial hyperplasias. GeburtshilfeFrauenheilkd 2015;75:135–6.
22. Kurman RJ, Carcangiu ML, Young RH, Herrington CS.WHO classification of tumours of female reproductive organs. 4thed. Lyon: IARC; 2014.
23. Dowsett M, Nielsen TO, A’Hern R, Bartlett J, Coombes RC, Cuzick J,et al. Assessment of Ki67 in breast cancer: recommendations from theinternational ki67 in breast cancer working group. JNCI J Natl CancerInst 2011;103:1656–64.
24. �rbo A, Rise CE, Mutter GL. Regression of latent endometrial pre-cancers by progestin infiltrated intrauterine device. Cancer Res 2006;66:5613–7.
25. Zigmond AS, Snaith RP. The hospital anxiety and depression scale.Acta Psychiatr Scand 1983;67:361–70.
26. Bjelland I, Dahl AA, Tangen T, Neckelmann D. The validity of thehospital anxiety and depression scale an updated literaturereview2002;52:69–77.
27. Tennant R, Hiller L, Fishwick R, Platt S, Joseph S, Weich S, et al.The Warwick-Edinburgh mental well-being scale (WEMWBS):
development and UK validation. Health Qual Life Outcomes2007;5:63.
28. Putz R, O’Hara K, Taggart F, Stewart-Brown S. Using WEMWBS tomeasure the impact of your work on mental wellbeing: a practice-based user guide2012. Available from: https://www.corc.uk.net/media/1244/wemwbs_practitioneruserguide.pdf.
29. MattesonKA, ScottDM,RakerCA,ClarkMA.Themenstrual bleedingquestionnaire: development and validation of a comprehensivepatient-reported outcome instrument for heavy menstrual bleeding.BJOG 2015;122:681–9.
30. Moore L, Leongamornlert D, Coorens THH, Sanders MA, Ellis P,Dentro SC, et al. The mutational landscape of normal human endo-metrial epithelium. Nature 2020;580:640–6.
31. Monte NM, Webster KA, Neuberg D, Dressler GR, Mutter GL. Jointloss of PAX2 and PTEN expression in endometrial precancers andcancer. Cancer Res 2010;70:6225–32.
32. Guttinger A, Critchley HO. Endometrial effects of intrauterine levo-norgestrel. Contraception 2007;75:S93--8.
33. Dinh A, Sriprasert I, Williams AR, Archer DF. A review of theendometrial histologic effects of progestins and progesterone receptormodulators in reproductive age women. Contraception 2015;91:360–7.
34. Villavicencio A, Aguilar G, Argu€uello G, D€unner C, Gabler F, Soto E,et al. The effect of overweight and obesity on proliferation andactivation of AKT and ERK in human endometria. Gynecol Oncol2010;117:96–102.
35. Zhang K, Luo Y, Dai H, Deng Z. Effects of bariatric surgery on cancerrisk: evidence from meta-analysis. Obes Surg 2020;30:1265--72.
36. Argenta P, Svendsen C, Elishaev E, Gloyeske N, Geller MA, EdwardsRP, et al. Hormone receptor expression patterns in the endometriumof asymptomatic morbidly obese women before and after bariatricsurgery. Gynecol Oncol 2014;133:78–82.
37. Kitson S, Sivalingam VN, Bolton J, McVey R, Nickkho-Amiry M,Powell ME, et al. Ki-67 in endometrial cancer: scoring optimizationand prognostic relevance for window studies. Mod Pathol 2017;30:459–68.
38. Saito-Tom LY, Soon RA, Harris SC, Salcedo J, Kaneshiro BE.Levonorgestrel intrauterine device use in overweight and obesewomen. Hawaii J Med Public Health 2015;74:369–74.
39. Nilsson CG. Tissue concentrations of levonorgestrel in women using alevonorgestrel-releasing IUD. Clin Endocrinol (Oxf) 1982;529–36.
40. Apter D, Gemzell-Danielsson K, Hauck B, Rosen K, Zurth C.Pharmacokinetics of two low-dose levonorgestrel-releasing intra-uterine systems and effects on ovulation rate and cervical function:pooled analyses of phase II and III studies. Fertil Steril 2014;101:1656–62.e4.
41. Mirena Annotated CCDS 2014, Bayer AG, Berlin, Germany, 11thFebruary 2014. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2014/021225Orig1s033.pdf.
42. Seeber B, Ziehr SC, Gschlieber A, Moser C, Mattle V, Seger C, et al.Quantitative levonorgestrel plasma level measurements in patientswith regular and prolonged use of the levonorgestrel-releasing intra-uterine system. Contraception 2012;86:345–9.
43. Westin SN, Fellman B, Sun CC, Broaddus RR, Woodall ML, Pal N,et al. Prospective phase ii trial of levonorgestrel intrauterine device:non-surgical approach for complex atypical hyperplasia and earlyendometrial cancer. Am J Obstet Gynecol 2020;S0002-9378(20)30861-9.
44. Derbyshire AE, Ryan N, Crosbie EJ. Biomarkers needed to predictprogestin response in endometrial cancer. BJOG 2017;124:1584.
45. Travaglino A, Raffone A, Saccone G, Insabato L, Mollo A, De PlacidoG, et al. Immunohistochemical predictive markers of response toconservative treatment of endometrial hyperplasia and early endo-metrial cancer: a systematic review. Acta Obstet Gynecol Scand 2019;98:1086–99.
Cancer Prev Res; 14(2) February 2021 CANCER PREVENTION RESEARCH272
Derbyshire et al.
Research. on July 2, 2021. © 2021 American Association for Cancercancerpreventionresearch.aacrjournals.org Downloaded from
Published OnlineFirst September 30, 2020; DOI: 10.1158/1940-6207.CAPR-20-0248
https://www.corc.uk.net/media/1244/wemwbs_practitioneruserguide.pdfhttps://www.corc.uk.net/media/1244/wemwbs_practitioneruserguide.pdfhttps://www.corc.uk.net/media/1244/wemwbs_practitioneruserguide.pdfhttps://www.accessdata.fda.gov/drugsatfda_docs/nda/2014/021225Orig1s033.pdfhttps://www.accessdata.fda.gov/drugsatfda_docs/nda/2014/021225Orig1s033.pdfhttps://www.accessdata.fda.gov/drugsatfda_docs/nda/2014/021225Orig1s033.pdfhttp://cancerpreventionresearch.aacrjournals.org/
-
46. Behrouzi R, RyanNAJ, Barr CE,DerbyshireAE,WanYL,Maskell Z, et al.Baseline serum HE4 but not tissue HE4 expression predicts response tothe levonorgestrel-releasing intrauterine system in atypical hyperplasiaand early stage endometrial cancer. Cancers (Basel) 2020;12:276.
47. Barr CE, Crosbie EJ. The mirena coil is a suitable treatment of early-stage endometrial cancer in obese women: for: careful selection andmonitoring is key. BJOG 2020;127:1001.
48. Bender NM, Segall-Gutierrez P, Najera SO, Stanczyk FZ, Montoro M,Mishell DR Jr. Effects of progestin-only long-acting contraception onmetabolic markers in obese women. Contraception 2013;88:418–25.
49. Conz L, Mota BS, Bahamondes L, D�oria MT, Derchain SFM, Rieira R,et al. Levonorgestrel-releasing intrauterine system and breast cancerrisk: A systematic review and meta-analysis. Acta Obstet GynecolScand 2020;99:970–82.
50. Wan YL, Beverley-Stevenson R, Carlisle D, Clarke S, Edmondson RJ,Glover S, et al. Working together to shape the endometrial cancerresearch agenda: the top ten unanswered research questions.Gynecol Oncol 2016;143:287–93.
51. Dottino JA, Hasselblad V, Secord AA, Myers ER, Chino J, HavrileskyLJ. Levonorgestrel intrauterine device as an endometrial cancer pre-vention strategy in obese women: a cost-effectiveness analysis.Obstet Gynecol 2016;128:747–53.
52. Bafligil C, Thompson DJ, Lophatananon A, et al. Association betweengenetic polymorphisms and endometrial cancer risk: a systematicreview. J Med Genet 2020;57:591–600.
53. O’Mara TA, Crosbie EJ. Polygenic risk score opportunities for earlydetection and prevention strategies in endometrial cancer. Br J Cancer2020 Jul 6. doi: 10.1038/s41416-020-0959-7.
AACRJournals.org Cancer Prev Res; 14(2) February 2021 273
PROgesterone Therapy for Endometrial Cancer Prevention
Research. on July 2, 2021. © 2021 American Association for Cancercancerpreventionresearch.aacrjournals.org Downloaded from
Published OnlineFirst September 30, 2020; DOI: 10.1158/1940-6207.CAPR-20-0248
http://cancerpreventionresearch.aacrjournals.org/
-
Research. on July 2, 2021. © 2021 American Association for Cancercancerpreventionresearch.aacrjournals.org Downloaded from
Published OnlineFirst September 30, 2020; DOI: 10.1158/1940-6207.CAPR-20-0248
http://cancerpreventionresearch.aacrjournals.org/
-
2021;14:263-274. Published OnlineFirst September 30, 2020.Cancer Prev Res Abigail E. Derbyshire, Jennifer L. Allen, Matthew Gittins, et al. Obese Women (PROTEC) Trial: A Feasibility StudyPROgesterone Therapy for Endometrial Cancer Prevention in
Updated version
10.1158/1940-6207.CAPR-20-0248doi:
Access the most recent version of this article at:
Material
Supplementary
1
http://cancerpreventionresearch.aacrjournals.org/content/suppl/2020/09/30/1940-6207.CAPR-20-0248.DCAccess the most recent supplemental material at:
Cited articles
http://cancerpreventionresearch.aacrjournals.org/content/14/2/263.full#ref-list-1
This article cites 46 articles, 7 of which you can access for free at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerpreventionresearch.aacrjournals.org/content/14/2/263To request permission to re-use all or part of this article, use this link
Research. on July 2, 2021. © 2021 American Association for Cancercancerpreventionresearch.aacrjournals.org Downloaded from
Published OnlineFirst September 30, 2020; DOI: 10.1158/1940-6207.CAPR-20-0248
http://cancerpreventionresearch.aacrjournals.org/lookup/doi/10.1158/1940-6207.CAPR-20-0248http://cancerpreventionresearch.aacrjournals.org/content/suppl/2020/09/30/1940-6207.CAPR-20-0248.DC1http://cancerpreventionresearch.aacrjournals.org/content/suppl/2020/09/30/1940-6207.CAPR-20-0248.DC1http://cancerpreventionresearch.aacrjournals.org/content/14/2/263.full#ref-list-1http://cancerpreventionresearch.aacrjournals.org/cgi/alertsmailto:[email protected]://cancerpreventionresearch.aacrjournals.org/content/14/2/263http://cancerpreventionresearch.aacrjournals.org/
/ColorImageDict > /JPEG2000ColorACSImageDict > /JPEG2000ColorImageDict > /AntiAliasGrayImages false /CropGrayImages false /GrayImageMinResolution 200 /GrayImageMinResolutionPolicy /Warning /DownsampleGrayImages true /GrayImageDownsampleType /Bicubic /GrayImageResolution 300 /GrayImageDepth -1 /GrayImageMinDownsampleDepth 2 /GrayImageDownsampleThreshold 1.50000 /EncodeGrayImages true /GrayImageFilter /DCTEncode /AutoFilterGrayImages true /GrayImageAutoFilterStrategy /JPEG /GrayACSImageDict > /GrayImageDict > /JPEG2000GrayACSImageDict > /JPEG2000GrayImageDict > /AntiAliasMonoImages false /CropMonoImages false /MonoImageMinResolution 600 /MonoImageMinResolutionPolicy /Warning /DownsampleMonoImages true /MonoImageDownsampleType /Bicubic /MonoImageResolution 900 /MonoImageDepth -1 /MonoImageDownsampleThreshold 1.50000 /EncodeMonoImages true /MonoImageFilter /CCITTFaxEncode /MonoImageDict > /AllowPSXObjects false /CheckCompliance [ /None ] /PDFX1aCheck false /PDFX3Check false /PDFXCompliantPDFOnly false /PDFXNoTrimBoxError true /PDFXTrimBoxToMediaBoxOffset [ 0.00000 0.00000 0.00000 0.00000 ] /PDFXSetBleedBoxToMediaBox true /PDFXBleedBoxToTrimBoxOffset [ 0.00000 0.00000 0.00000 0.00000 ] /PDFXOutputIntentProfile (None) /PDFXOutputConditionIdentifier () /PDFXOutputCondition () /PDFXRegistryName () /PDFXTrapped /False
/CreateJDFFile false /Description > /Namespace [ (Adobe) (Common) (1.0) ] /OtherNamespaces [ > /FormElements false /GenerateStructure false /IncludeBookmarks false /IncludeHyperlinks false /IncludeInteractive false /IncludeLayers false /IncludeProfiles false /MarksOffset 18 /MarksWeight 0.250000 /MultimediaHandling /UseObjectSettings /Namespace [ (Adobe) (CreativeSuite) (2.0) ] /PDFXOutputIntentProfileSelector /NA /PageMarksFile /RomanDefault /PreserveEditing true /UntaggedCMYKHandling /LeaveUntagged /UntaggedRGBHandling /LeaveUntagged /UseDocumentBleed false >> > ]>> setdistillerparams> setpagedevice