7. Analogues intro, 7.1 natural analogues, 7.2 constructed analogues (CA) ,

Professor Ian Holdaway Endocrinologist
Auckland District Health Board

A land of milk and giants – hormone-
secreting pituitary tumours
I M Holdaway, Endocrinologist, Auckland
Acromegaly
Prolactinomas
Cushing’s disease

Acromegaly
The quandary of a rare condition
(prevalence ~ 60-80 per million) which, however, carries serious sequelae if not treated:
- high burden of complications
- major reduction in life expectancy
Once diagnosed, effective treatment is available

What should a GP know about
acromegaly?
• Who to suspect
• How to diagnose it
• Effective treatment is available
(Treatment details and options would not be
considered as core knowledge for family
physicians)

Who should you suspect as
acromegalic?
A. Spot diagnosis on appearance

Who should you suspect as
acromegalic?
B. In those with obstructive sleep apnoea

Who should you suspect as
acromegalic?
C. In those with features of carpal tunnel
syndrome

Who should you suspect as
acromegalic?
D. The challenge – to keep the condition in
mind when seeing those with diabetes,
hypertension, cardiac disease or arthritis

Questions to ask a patient if you
suspect acromegaly
• Does the family think your appearance has
changed? (photos helpful)
• Has your shoe size gone up?
• Have you needed to expand or re-size your
finger rings?
• Are you excessively sleepy in the day? (Epworth
questionnaire)
• Do you sweat excessively?
• Do you have numbness/tingling in the hands?

Why is early diagnosis important?
• Mortality in acromegaly is at least doubled compared with the general population, with 10 or more years of life lost
• Successful treatment reduces mortality to expected levels
• Successful treatment reduces the complications of the disorder
• Delay in diagnosis is an independent risk factor increasing mortality

Mortality in acromegaly from the20 major published series
Ale
xander
(198
0)
Ext
abe
(199
3)
Ben
gtsso
n (198
8)
Abosc
h (199
8)
Hold
away
(200
4)
Bat
es (1
993)
Shim
atsu
(199
8)
Bea
uregar
d (200
3)
Wright (
1970
)
Ben
gtsso
n (199
9)
Sher
lock
(200
9)
Orm
e (1
998)
Trepp (2
005)
Bie
rmas
z (2
004)
Nab
arro
(198
7)
Ayu
k (2
004)
Swea
ringen
(199
9)
Arita
(200
3)
Kau
ppinen
(200
5)
Aro
sio (2
012)
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5O
bserv
ed
-to
-exp
ecte
d m
ort
ali
ty
NZ patients
observed
expected

0
0.2
0.4
0.6
0.8
1
0 5 10 15 20 25 30
Time (years)
Pro
ba
bilit
y
Acromegaly (with 95%
confidence limits)
Normal population
Survival of patients with acromegaly following
treatment (Holdaway et al, 2003) [n=208, 72 deaths]

Cure of acromegaly restores
survival to normal
0
0.2
0.4
0.6
0.8
1
0 5 10 15 20 25 30
Time (Years)
Pro
po
rtio
n S
urv
ivin
g
normal GH & IGF-I
Disorder still
active

Change in age of death of acromegalic individuals in
Auckland over time
20
30
40
50
60
70
80
90
Number of values
Minimum
25% Percentile
Median
75% Percentile
Maximum
Mean
Std. Deviation
Std. Error
Lower 95% CI of mean
Upper 95% CI of mean
Sum
<1/1/2000
68
33.99
52.56
62.70
70.35
86.22
61.57
12.97
1.573
58.43
64.71
4187
>1/1/2000
37
39.56
65.62
74.40
80.45
90.87
71.99
12.02
1.976
67.98
76.00
2664
Table Analyzed
Column A
vs
Column B
Unpaired t test
P value
P value summary
Are means signif. different? (P < 0.05)
One- or two-tailed P value?
t, df
How big is the difference?
Mean ± SEM of column A
Mean ± SEM of column B
Difference between means
95% confidence interval
R squared
F test to compare variances
F,DFn, Dfd
P value
P value summary
Are variances significantly different?
Data 2
<1/1/2000
vs
>1/1/2000
0.0001
***
Yes
Two-tailed
t=4.033 df=103
61.57 ± 1.573 N=68
71.99 ± 1.976 N=37
-10.42 ± 2.584
-15.55 to -5.290
0.1364
1.165, 67, 36
0.6277
ns
No
P<0.0001
Died after1/1/2000
Died before1/1/2000
Ag
e a
t d
eath
(yrs
)

What about the complications of acromegaly –
do they diminish with treatment?
0
10
20
30
40
Acromegaly cured
Acromegalynot cured
New Zealand acromegalics with clinical joint disorders
* p <0.01
% w
ith
jo
int
pro
ble
ms
Prevalence of diabetes in acromegaly(Auckland patients)
0 2 4 6 8 10 12 14 16 18 20
Cured acromegaly
Active acromegaly
NZ population
Acromegaly
Percentage

Not cured
Cured

Cardiac disease in acromegaly
The Auckland experience
1. Cardiac disease at diagnosis = 19%
2. Post-treatment cure, cardiac disease = 7%
3. Post-treatment not cured, cardiac disease = 20%
(p<0.05)

Troublesome symptoms of acromegaly –
prevalence before and after curing the disorder

How can you confirm a diagnosis of
acromegaly?
• Measure the serum IGF-I level – an
elevated level usually indicates growth
hormone excess (cost ~ $25)
• Growth hormone itself is not a good
indicator since it is released in a pulsatile
manner, and single measurements are
difficult to interpret

Pituitary
Liver Bone
Muscle, fat
etc IGF-I
Growth
hormone
Why is IGF-I a good marker of acromegaly?
Because IGF-I is the down-stream mediator of growth
hormone action

Has there been any success with
screening for acromegaly in
General Practice?

Results of screening 17,000 patients from 9
General Practices in Brazil over 6 months in 2010,
using a simple 2-question questionnaire
Rosario & Calsolari, 2012

Screening for acromegaly in 2270 diabetic
patients in a hospital outpatient setting using
serum insulin-like growth factor-I
2270 patients
62 raised serum IGF-I
56 confirmed on second
sample
3 confirmed acromegaly
Rosario 2011

Early detection of acromegaly
• Efforts to screen for the condition to date
are probably not cost effective
• Thus, being alert to the possible diagnosis
remains the key – in NZ most referrals
have been from General Practice

What about treatment?
Until about 20yrs ago surgery and radiotherapy were
the only means of treatment, but only cured ~50% of
patients
The reason? Trans-sphenoidal surgery

Recent developments
• The advent of effective medical (non-surgical)
treatment has meant that the great majority of
acromegalics can now be brought into the “cure”
range of growth hormone and IGF-I
Surgery
Cure (~ 50%)
Not cured
Medical therapy
( ~ 80-90%
overall cure)

Depot octreotide

Growth
hormone
Growth
hormone
Somatostatin
receptor
Action of
somatostatin
analogues such
as octreotide
pituitary
60-70% of
acromegalics
achieve safe
levels of GH
with octreotide
therapy
GH-secreting
cell
somatostatin

Meta-analysis by Freda et al, 2005, n= 612 17 surgical series 1987-2011
Remission of acromegaly with initial surgery
or with LAR octreotide treatment
0
10
20
30
40
50
60
Per
cen
t re
mis
sio
n
wit
h t
reatm
en
t
Surgery LAR octreotide

Shrinkage of GH-secreting macroadenoma
with LAR octreotide therapy
Baseline 6 months 12 months
(Mercado et al 2007)

The land of milk…..
Prolactinomas of the pituitary

When should you think of a
potential prolactin problem?
• Irregular periods or ammenorrhea
• Infertility (men or women)
• Galactorrhea
• Breast discomfort
• Men with low serum testosterone
• Reduced libido

But, not all prolactin excess is
pathological….. Physiologic hyperprolactinaemia:
• Venepuncture stress (1.5-2x upper limit of normal)
• Other stress (up to 2x uln)
• Pregnancy (up to 4x uln or higher)
• Lactation ( “ “ “ “ )
• Macroprolactinaemia (innocent, usually detected by laboratory)
Medications:
• Oestrogen –containing OCPs
• Occaisonally progestins (depot provera)
• Dopamine antagonists (e.g. risperidone etc)

Physical signs relevant to hyperprolactinaemia:
1.Galactorrhea
2. Montgomery tubercule hypertrophy
3. Any signs of hypogonadism?
(reduced testicular volumes etc)

Important pathological causes of an
elevated serum prolactin
• Pituitary microprolactinoma (levels usually
1000-8000 mIU/L)
• Pituitary macroprolactinoma (levels high,
usually 10,000 – 100,000 mIU/L)
Tricky prolactin levels: • Venepuncture stress (if suspected can sample via iv line at rest)
• Don’t forget medication effects
• Rare issues (hypothyroidism, renal impairment, fits etc)
• Pituitary stalk pressure from a non-functioning adenoma or similar

microadenoma
Pituitary MRI scan
showing a
microprolactinoma

Pituitary macroprolactinoma
causing visual field defects

Pituitary stalk pressure
Occurs when the pituitary stalk is distorted or compressed by a large
non-functioning pituitary adenoma.
The usual inhibitory control of prolactin secretion by dopamine coming
down the pituitary portal vessels is interrupted → raised prolactin
(about 600-3000mIU/L i.e.similar to a microprolactinoma)

Treatment of prolactin excess
• Dopamine is the physiologic inhibitor of
prolactin, so long-acting dopamine
analogues give prolonged suppression of
prolactin production
- bromocryptine
- cabergoline
• Prolactin excess has been facetiously
termed “cabergoline deficiency”

cabergoline
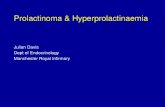
Cabergoline is also very effective at shrinking
prolactinomas

Effect of treatment with cabergoline on tumour volume
in previously untreated patients with prolactinomas
Colao et al, 2000

Dramatic shrinkage of the pituitary

The land of milk, giants, and centrally
obese patients with striae and facial
plethora……
Pituitary –based Cushing’s
syndrome
(“Cushing’s disease”)

When should you suspect
Cushing’s syndrome?
• Patient appearance
• Diabetics, hypertensives, osteoporotics
with “extra” (cushingoid) features
• Simple obesity unlikely to be due to
Cushing’s syndrome

Clinical clues for Cushings:
• Central fat distribution with slim limbs
• Skin changes (acne, skin thinning,
bruising, active striae, hirsuitism)
• Facial plethora
• Lymphoedema
• Proximal myopathy
• Above features in those with hypertension/
diabetes/ hypokalaemia/ osteoporosis

Cushinoid fat distribution and body habitus


Testing for
thinning of the
skin

How can you screen for Cushing's
syndrome?
• Best test = overnight dexamethasone
suppression test (1mg dexamethasone taken at 11pm followed by a blood
cortisol at the local laboratory 9am the next morning)
Normal = plasma cortisol <50nmol/l
“Grey zone” = 50-135nmol/l
• Next option = 24hr urine cortisol (<380nmol/24hr)
• Or spot bedtime urine cortisol <12nmol/mmol creatinine

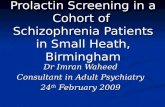
Effect of
treatment of
Cushing’s
disease on
complications of
the disorder

Further testing and treatment
• Can be difficult to distinguish between pituitary-based Cushing’s syndrome (Cushing’s disease) and ectopic ACTH syndrome
• Usual cause of Cushing's disease is a small ACTH-secreting pituitary adenoma, can be difficult to see on scan
• Treatment is by pituitary surgery. Bilateral adrenalectomy less favoured but is curative. Some medical options also available in difficult cases (ketoconazole, metyrapone etc)

Pituitary Cushing’s disease

Survival of patients
with Cushing’s
syndrome is
decreased compared
with the matched
general population
SMR cured = 2.3
SMR not cured = 5.7