Elements of Professional Nursing Identified by Nursing Experts
Professional Nursing Solutions,
LLCParticipation in the National AHRQ Safety
Program for Antibiotic Stewardship
Presented by Carol Compas, PhD, BSN, RN
November 8, 2019

Introduction to the AHRQ Safety
Program for Improving Antibiotic UseLong-Term Care
AHRQ Safety Program for
Improving Antibiotic Use

Program Support and Target Audience
• Program Support –– This activity is supported by a contract from the
Agency for Healthcare Research and Quality –AHRQ
• Target Audience –– This activity is intended for physicians, physician
assistants, nurse practitioners, registered nurses
and certified nursing assistants.
3
Objectives
1. List the goals of the AHRQ Safety Program for Improving Antibiotic Use
2. Apply the Four Moments of Antibiotic Decision Making
3. Recognize how to adapt the culture of a workplace to improve patient safety
4. Describe the Centers for Medicare and Medicaid Services (CMS) Condition of Participation related to antibiotic stewardship in the long-term care (LTC) setting
5. Describe the timeline of the AHRQ Safety Program
6. State the data requirements for the project and how to upload data on the AHRQ Safety Program website
4

• A quality improvement
collaborative to improve
antibiotic use across
healthcare
• Program targets 3
settings:
– Acute Care
– Long-term Care
– Ambulatory Care
AHRQ Safety Program for Improving Antibiotic Use
5

Integrating Two Important Concepts
• Program which focuses on appropriate use of antibiotics to improve patient outcomes and reduce the development of multi-drug resistant organisms
• Approach to make healthcare safer by improving teamwork and communication among physicians, pharmacists, nurses, and other team members using the science of safety
6
Antibiotic
Stewardship
Culture of
Patient Safety

• Improved safety culture
• Enhanced teamwork and
communication
• Improved antibiotic decision
making
• Reduction in suboptimal
antibiotic usage
• Reduction in Clostridium difficile infections
• Improved compliance with CMS Condition of Participation
Expected Outcomes of Program
7
• Technical assistance for implementing antibiotic stewardship
• Access to experts in patient safety and antibiotic stewardship
– Monthly Webinars
– Monthly office hours with the project team
– An Implementation Adviser for day-to-day troubleshooting
• Ability to network on the regional and national level
Benefits to Participants
8

The Four Moments of Antibiotic Decision Making
9

The Four Moments of Antibiotic Decision Making
1. Does the resident have symptoms that
suggest an infection? Can we try
symptomatic treatment and active
monitoring?
2. What type of infection is it? Have we
collected appropriate cultures and diagnostic
tests before starting antibiotics? What
empiric therapy should we initiate?
3. What duration of antibiotic therapy is needed
for the resident’s diagnosis?
4. It’s been 2-3 days since we started
antibiotics. Re-evaluate the resident and
review results of diagnostic tests. Can we
stop antibiotics? Can we narrow therapy?
10

The Four Moments of Antibiotic Decision Making
1. Does the resident have symptoms that
suggest an infection? Can we try
symptomatic treatment and active
monitoring?
2. What type of infection is it? Have we
collected appropriate cultures and diagnostic
tests before starting antibiotics? What
empiric therapy should we initiate?
3. What duration of antibiotic therapy is needed
for the resident’s diagnosis?
4. It’s been 2-3 days since we started
antibiotics. Re-evaluate the resident and
review results of diagnostic tests. Can we
stop antibiotics? Can we narrow therapy?
11

The Four Moments of Antibiotic Decision Making
1. Does the resident have symptoms that
suggest an infection? Can we try
symptomatic treatment and active
monitoring?
2. What type of infection is it? Have we
collected appropriate cultures and diagnostic
tests before starting antibiotics? What
empiric therapy should we initiate?
3. What duration of antibiotic therapy is needed
for the resident’s diagnosis?
4. It’s been 2-3 days since we started
antibiotics. Re-evaluate the resident and
review results of diagnostic tests. Can we
stop antibiotics? Can we narrow therapy?
12

The Four Moments of Antibiotic Decision Making
1. Does the resident have symptoms that
suggest an infection? Can we try
symptomatic treatment and active
monitoring?
2. What type of infection is it? Have we
collected appropriate cultures and diagnostic
tests before starting antibiotics? What
empiric therapy should we initiate?
3. What duration of antibiotic therapy is needed
for the resident’s diagnosis?
4. It’s been 2-3 days since we started
antibiotics. Re-evaluate the resident and
review results of diagnostic tests. Can we
stop antibiotics? Can we narrow therapy?
13
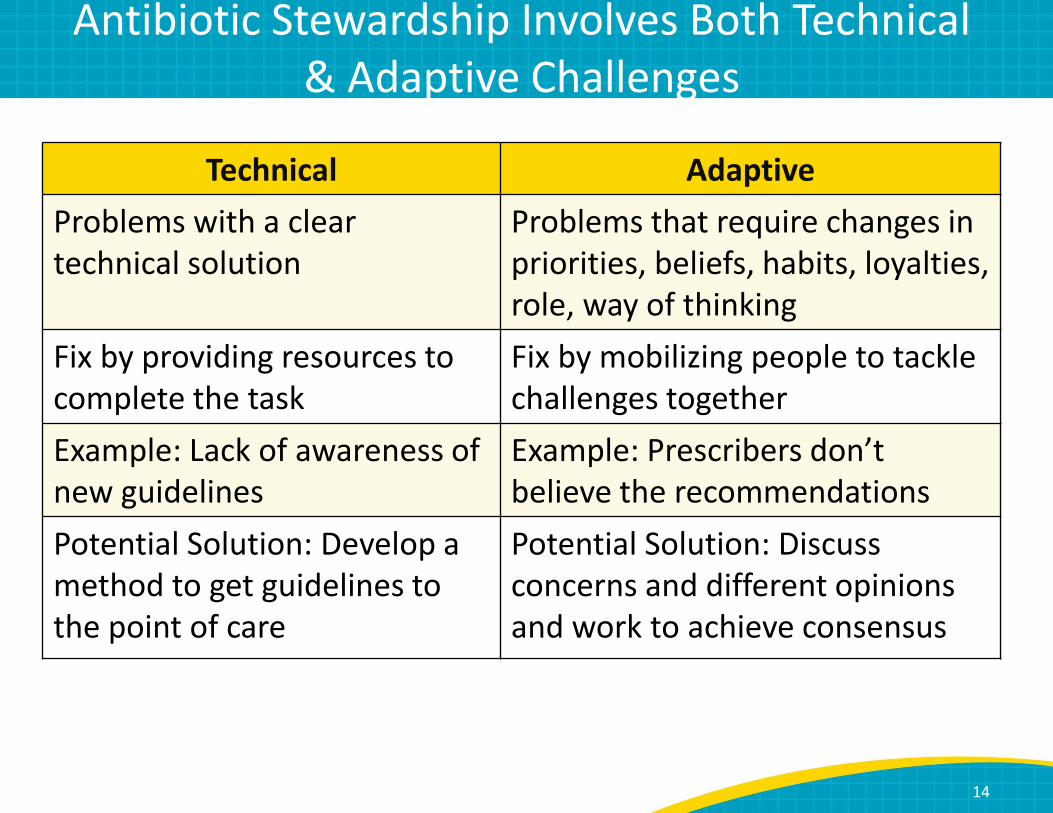
Antibiotic Stewardship Involves Both Technical
& Adaptive Challenges
Technical Adaptive
Problems with a clear
technical solution
Problems that require changes in
priorities, beliefs, habits, loyalties,
role, way of thinking
Fix by providing resources to
complete the task
Fix by mobilizing people to tackle
challenges together
Example: Lack of awareness of
new guidelines
Example: Prescribers don’t believe the recommendations
Potential Solution: Develop a
method to get guidelines to
the point of care
Potential Solution: Discuss
concerns and different opinions
and work to achieve consensus
14

5 Steps for Improving the Culture of Patient Safety
1515
1. Engage leadership for support and collaboration
2. Understanding the science of safety
3. Improve teamwork and communication
4. Recognize current practices that may lead to
patient harm
5. Develop system-based solutions to improve
patient safety

CMS Conditions of Participation
• CMS requires all long-term care facilities to have an Antimicrobial Stewardship Program (ASP)
• An ASP should include—– Written antibiotic use protocols
– A system to monitor antibiotic use with the goal of resident safety
– Measuring and reporting of antibiotic use and resistance data
– Feedback and education to individual prescribers
– Feedback and education to all facility staff
16
2. Medicare and Medicaid Programs; Reform of Requirements for Long-Term Care Facilities. October 2016.
https://www.federalregister.gov/documents/2016/10/04/2016-23503/medicare-and-medicaid-programs-reform-of-requirements-for-
long-term-care-facilities. Accessed July 12, 2018.

CMS Conditions of Participation
• Each facility must designate at least one person as
an Infection Preventionist (IP) who is responsible
for the Infection Prevention and Control
Plan (IPCP).
• The Infection Preventionist must be a member of
the facility’s Quality Assessment and Assurance (QAA) committee and make regular reports.
• The Infection Preventionist must also conduct an
annual review of the Infection Prevention and
Control Plan and update as necessary.
17
2. Medicare and Medicaid Programs; Reform of Requirements for Long-Term Care Facilities. October 2016.
https://www.federalregister.gov/documents/2016/10/04/2016-23503/medicare-and-medicaid-programs-reform-of-requirements-for-
long-term-care-facilities. Accessed July 12, 2018.

Participant Overview
• There will be two groups of participants within the AS program.
– Antibiotic Stewardship team
• A physician
• Either an IP and control nurse OR a pharmacist
• Other members
– Make sure to designate team champions to motivate/encourage sustainable efforts
– Frontline staff
• People who prescribe antibiotics
• People who take care of residents daily
• Even without an AS program, people can use/view the educational material on the program’s website.
18

Introduction and Antibiotic Stewardship Program
Development
December 2018
Antibiotic
Stewardship
Program
Development
Participants
Antimicrobial stewardship team
19
November/
December 2018
Introduction to
the AHRQ Safety
Program for
Improving
Antibiotic Use

Overview of Adaptive Webinars
January 2019
Partnering With a
Senior Executive
January 2019
Improving
Antibiotic Use is a
Patient Safety
Issue
February 2019
Improving Teamwork
and Communication
February 2019
Identifying Targets to
Improve Antibiotic Use
March 2019
Changing the
System to Improve
Patient Safety
January – March 2019
Bi-monthly 25-minute Webinars about adaptive approaches for
cultural change
20
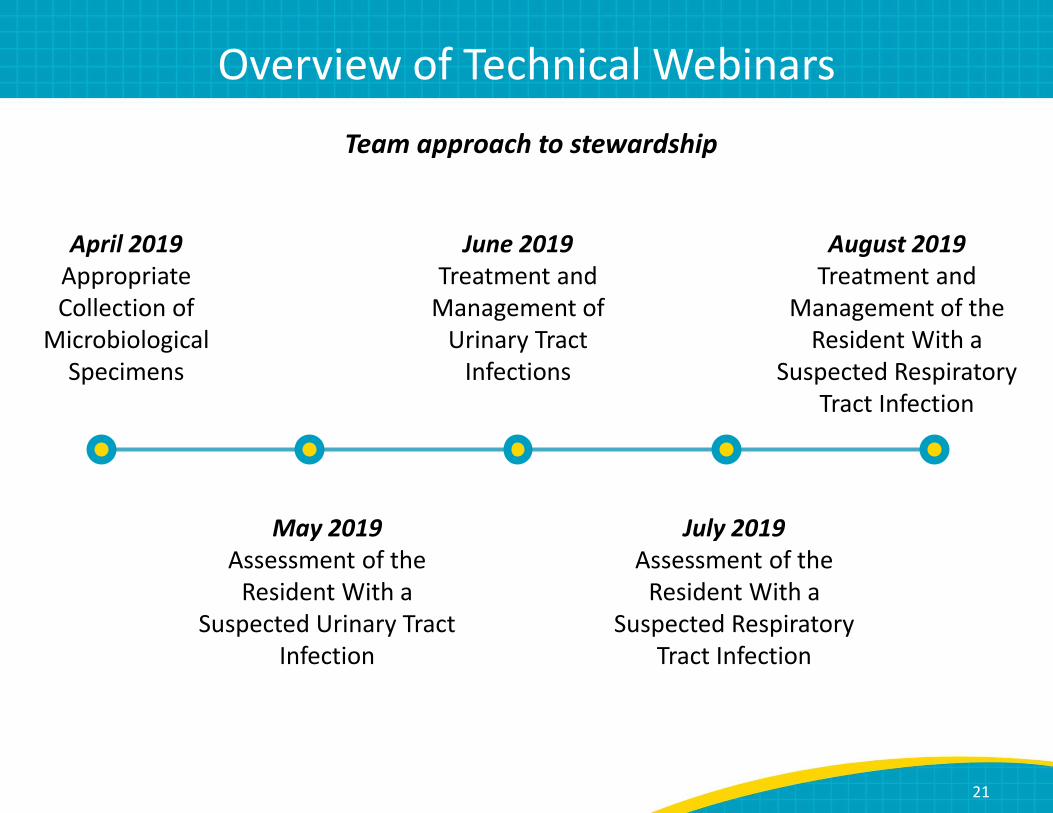
Overview of Technical Webinars
April 2019
Appropriate
Collection of
Microbiological
Specimens
May 2019
Assessment of the
Resident With a
Suspected Urinary Tract
Infection
June 2019
Treatment and
Management of
Urinary Tract
Infections
July 2019
Assessment of the
Resident With a
Suspected Respiratory
Tract Infection
August 2019
Treatment and
Management of the
Resident With a
Suspected Respiratory
Tract Infection
Team approach to stewardship
21

Additional Webinars
September 2019
Discussing Infectious
Concerns With Providers
October 2019
Discussing Infectious
Concerns With
Residents and
Caregivers
November 2019
Sustaining Antibiotic
Stewardship Efforts
Webinars about tools for frontline staff to discuss infectious concerns in long-
term care residents with prescribers and concerned family members.
22

Data Collection
23

Data To Be Submitted
24
1. Monthly Dataa. Number of patient days of care
b. Number of days of antibiotic therapy (per 1,000 resident days) for antibiotics commonly used in the LTC setting
c. Number of antibiotic starts (per 1,000 resident days)
d. Number of C. diff LabID events (per 10,000 resident-days)
e. Number of urine cultures (per 1,000 resident days)
2. Team Antibiotic Review Forma. Data does not need to be submitted to the project website
b. Implementation information to be collected by your IA during the monthly check-in call
3. NHSOPS: pre- and post intervention survey on safety culture
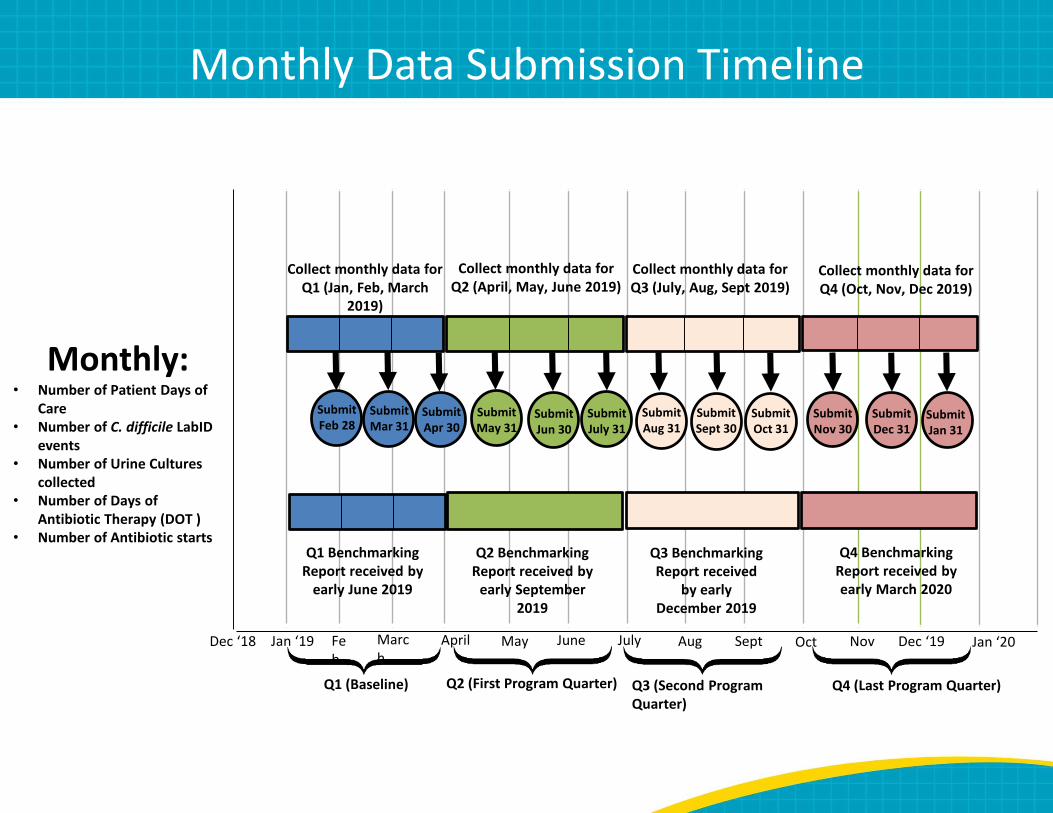
Monthly: • Number of Patient Days of
Care
• Number of C. difficile LabID
events
• Number of Urine Cultures
collected
• Number of Days of
Antibiotic Therapy (DOT )
• Number of Antibiotic starts
Jan ‘19 Marc
hMay July Sept Dec ‘19Dec ‘18 Fe
b
April June Aug Oct Nov
Q1 (Baseline) Q2 (First Program Quarter) Q4 (Last Program Quarter)Q3 (Second Program
Quarter)
Collect monthly data for
Q1 (Jan, Feb, March
2019)
Q1 Benchmarking
Report received by
early June 2019
Submit
Feb 28
Collect monthly data for
Q2 (April, May, June 2019)
Collect monthly data for
Q3 (July, Aug, Sept 2019)
Collect monthly data for
Q4 (Oct, Nov, Dec 2019)
Q2 Benchmarking
Report received by
early September
2019
Q3 Benchmarking
Report received
by early
December 2019
Q4 Benchmarking
Report received by
early March 2020
Submit
July 31
Submit
Oct 31
Submit
Jan 31
Jan ‘20
Submit
Mar 31
Submit
Apr 30Submit
Jun 30
Submit
May 31
Submit
Sept 30
Submit
Aug 31
Submit
Dec 31
Submit
Nov 30
Monthly Data Submission Timeline

Monthly Data Collection FormNPI [enter NPI here]
Long-Term Care Facility Name
Contact Name
Contact Email
Contact Telephone Number
Reporting Month
Number of Patient Days of Care
Number of C. difficile LabID events
Number of urine cultures collected
Days of Antibiotic Therapy (DOT)
[enter aggregate # of days residents were
administered each antibiotic below in the
reporting month. If no resident was administered a
particular antibiotic, enter "0" for that row]
# Antibiotic Starts
[enter # of antibiotic starts for each antibiotic below in the
reporting month. If there were no antibiotic starts for a particular
antibiotic, enter "0" for that row]
AMOXICILLIN (Amoxil)
AMOXICILLIN/CLAVULANATE
(Augmentin)
AMPICILLIN/SULBACTAM (Unasyn)
AZITHROMYCIN (Zithromax)
CEFADROXIL (Duricef)
CEFDINIR (Omnicef)
CEFIXIME (Suprax)
CEFPODOXIME (Vantin)
CEFTRIAXONE (Rocephin)
CEFUROXIME (Ceftin)
CEPHALEXIN (Keflex)
CIPROFLOXACIN (Cipro)
CLINDAMYCIN (Cleocin)
DOXYCYCLINE (Vibramycin)
ERTAPENEM (Invanz)
FOSFOMYCIN (Monurol)
LEVOFLOXACIN (Levaquin)
LINEZOLID (Zyvox)
MEROPENEM (Merrem)
METRONIDAZOLE (Flagyl)
MOXIFLOXACIN (Avelox)
NITROFURANTOIN (Macrobid)
PIPERACILLIN/TAZOBACTAM (Zosyn)
SULFAMETHOXAZOLE/TRIMETHOPRIM
(Bactrim, Septra)
VANCOMYCIN Intravenous (Vancocin)
VANCOMYCIN Oral (Vancocin)
[enter # urine cultures collected in the reporting month]
[the sum of each daily census (number residents in the facility each day) for the entire reporting month]
[enter facility name here]
[enter telephone number here]
[enter # C. difficile LabID events for the reporting month]
[enter email here]
[enter name here]
[enter reporting month]
26

Facility Information
• Facility information – 10-digit NPI number
– Facility name (same as used during registration)
– Contact name, email, and telephone number
• Reporting month and days of care– Reporting month (drop down menu)
– Number of patient days of care
27
NPI [enter NPI here]
Long-Term Care Facility Name
Contact Name
Contact Email
Contact Telephone Number
Reporting Month
Number of Patient Days of Care [the sum of each daily census (number residents in the facility each day) for the entire reporting month]
[enter facility name here]
[enter telephone number here]
[enter email here]
[enter name here]
[enter reporting month]

C. difficile Lab Events and Urine Cultures
• Record any positive C. difficile LabID events
• Contact contracted microbiology lab for this information- usually easily accessible.
• Data is concordant with current NHSN requirements.– If you are already working with a QIN/QIO on collecting this data, consider
asking them to help navigate
• Monthly number of urine cultures collected
• Record all urine cultures collected, not simply positive urine cultures
• This information can often be obtained from your contracted microbiology lab or can be a part of monthly QA review.
28
Number of C. difficile LabID events
Number of urine cultures collected [enter # urine cultures collected in the reporting month]
[enter # C. difficile LabID events for the reporting month]

Antibiotic Use
1. Days of antibiotic therapy
2. Antibiotic starts
29
Two measures of
monthly antibiotic use
(by antibiotic)
30
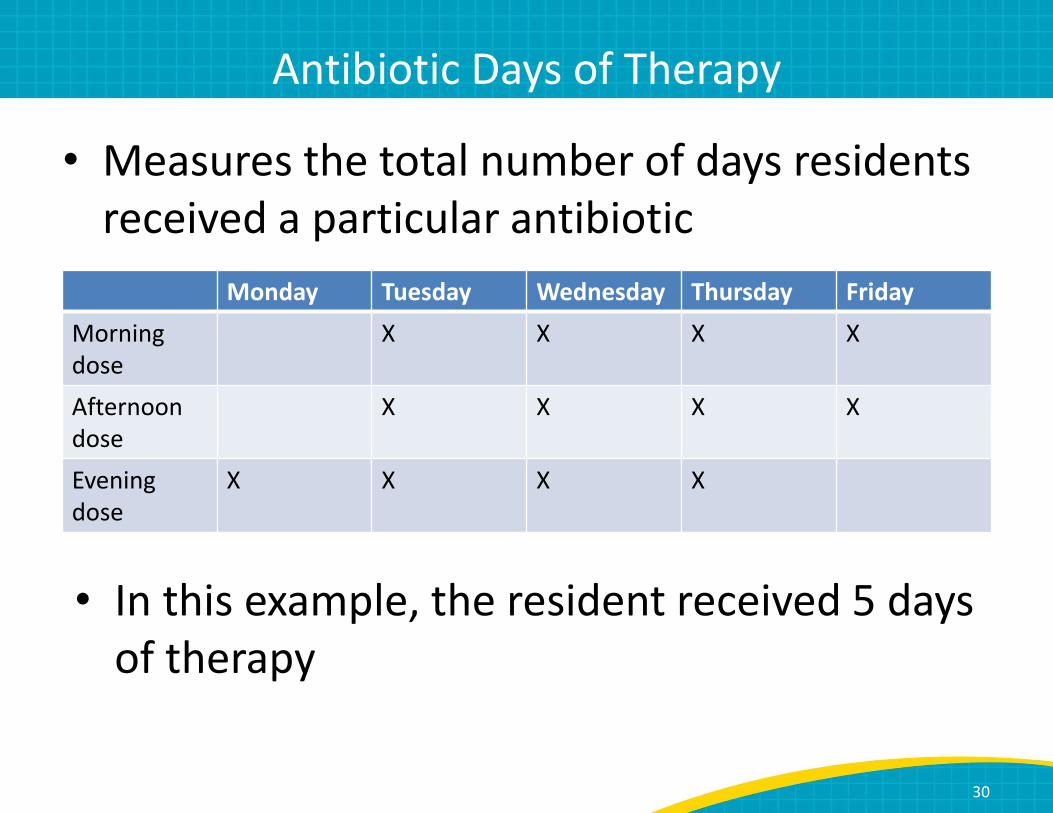
Antibiotic Days of Therapy
• Measures the total number of days residents
received a particular antibiotic
Monday Tuesday Wednesday Thursday Friday
Morning
dose
X X X X
Afternoon
dose
X X X X
Evening
dose
X X X X
• In this example, the resident received 5 days
of therapy
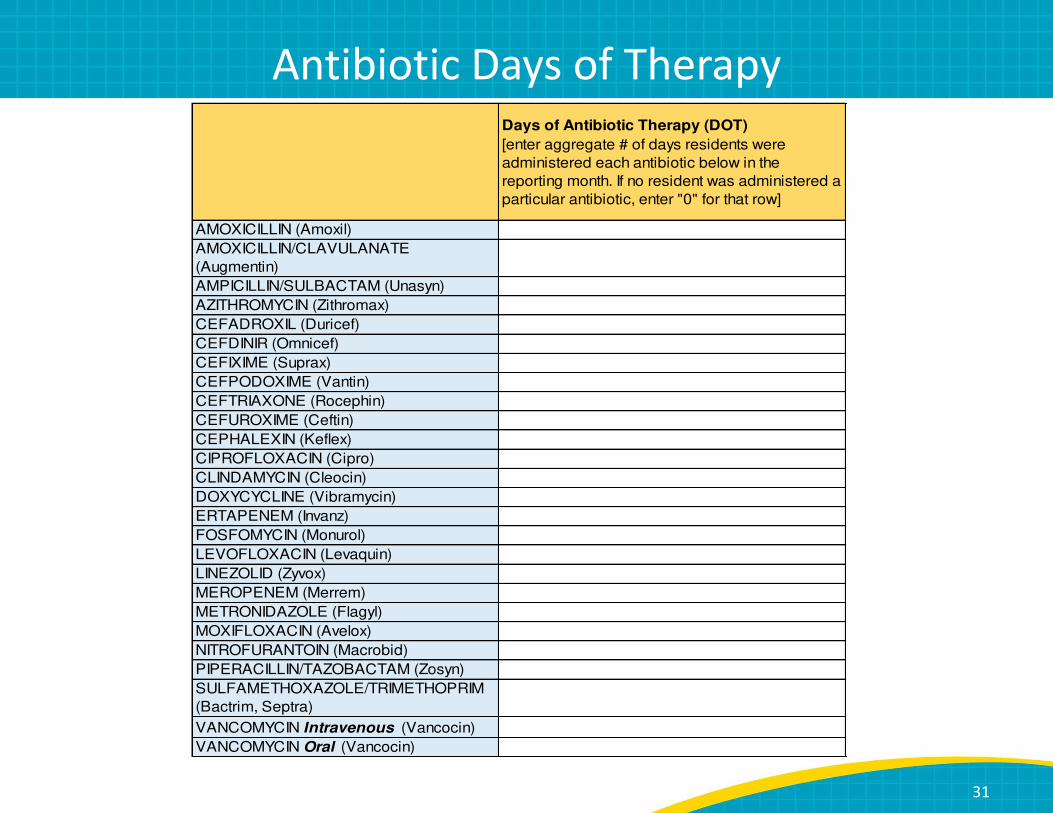
Antibiotic Days of TherapyDays of Antibiotic Therapy (DOT)
[enter aggregate # of days residents were
administered each antibiotic below in the
reporting month. If no resident was administered a
particular antibiotic, enter "0" for that row]
AMOXICILLIN (Amoxil)
AMOXICILLIN/CLAVULANATE
(Augmentin)
AMPICILLIN/SULBACTAM (Unasyn)
AZITHROMYCIN (Zithromax)
CEFADROXIL (Duricef)
CEFDINIR (Omnicef)
CEFIXIME (Suprax)
CEFPODOXIME (Vantin)
CEFTRIAXONE (Rocephin)
CEFUROXIME (Ceftin)
CEPHALEXIN (Keflex)
CIPROFLOXACIN (Cipro)
CLINDAMYCIN (Cleocin)
DOXYCYCLINE (Vibramycin)
ERTAPENEM (Invanz)
FOSFOMYCIN (Monurol)
LEVOFLOXACIN (Levaquin)
LINEZOLID (Zyvox)
MEROPENEM (Merrem)
METRONIDAZOLE (Flagyl)
MOXIFLOXACIN (Avelox)
NITROFURANTOIN (Macrobid)
PIPERACILLIN/TAZOBACTAM (Zosyn)
SULFAMETHOXAZOLE/TRIMETHOPRIM
(Bactrim, Septra)
VANCOMYCIN Intravenous (Vancocin)
VANCOMYCIN Oral (Vancocin)
31

Antibiotic Starts
• Count number of new antibiotics courses
started in the facility in each month
• New admissions on antibiotics should be
included as a new antibiotic start
– This is to capture total antibiotic usage,
including what is prescribed from
surrounding acute care facilities
32

Antibiotic Starts# Antibiotic Starts
[enter # of antibiotic starts for each antibiotic below in the
reporting month. If there were no antibiotic starts for a particular
antibiotic, enter "0" for that row]
AMOXICILLIN (Amoxil)
AMOXICILLIN/CLAVULANATE
(Augmentin)
AMPICILLIN/SULBACTAM (Unasyn)
AZITHROMYCIN (Zithromax)
CEFADROXIL (Duricef)
CEFDINIR (Omnicef)
CEFIXIME (Suprax)
CEFPODOXIME (Vantin)
CEFTRIAXONE (Rocephin)
CEFUROXIME (Ceftin)
CEPHALEXIN (Keflex)
CIPROFLOXACIN (Cipro)
CLINDAMYCIN (Cleocin)
DOXYCYCLINE (Vibramycin)
ERTAPENEM (Invanz)
FOSFOMYCIN (Monurol)
LEVOFLOXACIN (Levaquin)
LINEZOLID (Zyvox)
MEROPENEM (Merrem)
METRONIDAZOLE (Flagyl)
MOXIFLOXACIN (Avelox)
NITROFURANTOIN (Macrobid)
PIPERACILLIN/TAZOBACTAM (Zosyn)
SULFAMETHOXAZOLE/TRIMETHOPRIM
(Bactrim, Septra)
VANCOMYCIN Intravenous (Vancocin)
VANCOMYCIN Oral (Vancocin)
33

References
1. Heifetz R, Grashow A, Linsky M. The practice of adaptive leadership: tools and
tactics for changing your organization and the world, 1st ed. Boston, MA:
Harvard Business Review Press; 2009.
2. Medicare and Medicaid Programs; Reform of Requirements for Long-Term
Care Facilities. October 2016.
https://www.federalregister.gov/documents/2016/10/04/2016-
23503/medicare-and-medicaid-programs-reform-of-requirements-for-long-
term-care-facilities. Accessed July 12, 2018.

Thank You for Your Time
• Please collaborate with your long term care
providers on all things quality
• There is untapped talent in Nursing Homes
• Contact Information:
• Cell (501) 520-5244