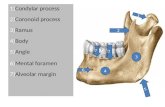
PROF PALANI MS FICS. Paired salivary glands that lie below the mandible on either side. larger...
73
PROF PALANI MS FICS SUBMANDIBULAR SALIVARY GLAND
-
Upload
cornelius-randall -
Category
Documents
-
view
219 -
download
0
Transcript of PROF PALANI MS FICS. Paired salivary glands that lie below the mandible on either side. larger...

PROF PALANI MS FICS
SUBMANDIBULAR SALIVARY GLAND


Paired salivary glands that lie below the mandible on either side.
larger superficial and a smaller deep lobe.
Drained by a single submandibular duct (Wharton’s duct).
It drains into the anterior floor of the mouth at the sublingual papilla.

3 NERVES—Marginal mandibular branch of facial nerve
__hypoglossal nerve __lingual nerve2 MUSCLES__mylohyoid __hyoglossus1 ARTERY __facial artery.
Important anatomical relationships of the submandibular glands





CLINICAL EXAMINATION


most common ectopic salivary tissue is the Stafne bone cyst.
asymptomatic, clearly demarcated radiolucency of the angle of the mandible.
Formed by invagination into the bone on the lingual aspect of the mandible of an ectopic lobe of the juxtaposed submandibular gland.
No treatment required.
Ectopic/aberrant salivary gland tissue


Acute, Chronic or Acute on Chronic.Acute submandibular sialadenitis: - Viral : The paramyxovirus (mumps). - bacterial : secondary to obstruction.
INFLAMMATORY DISORDERS

most common cause is stone formation.Eighty per cent of all salivary stones occur in
the submandibular glands because their secretions are highly viscous.
Eighty per cent of submandibular stones are radio-opaque and can be identified on plain radiography.
OBSTRUCTION AND TRAUMA




SYMPTOMS:Acute painful swelling in the region of the
submandibular gland, precipitated by eating.Swelling occurs rapidly and often resolves
spontaneously over 1–2 hours after the meal is completed—complete obstruction.
Minimal discomfort and swelling, not confined to mealtimes—partial obstruction.

SIGNS:enlarged firm submandibular gland, tender
on bimanual examination.Pus may be visible, draining from the
sublingual papilla.


TREATMENT:DISTAL TO LINGUAL NERVE: -- INTRAORAL APPROACH.PROXIMAL TO LINGUAL NERVE: -- gland excision, stone removal and
duct ligation.


Incision and exposure of glandGland mobilisation.Dissection of the deep lobe and identification
of the lingual nerve.Wound closure.
EXCISION

Incision and exposure of gland
Incision should be marked at least 3–4 cm below the lower border of the mandible to avoid damage to the marginal mandibular branch of the facial nerve.
Superficial veins, including the anterior facial vein, require ligation.

Gland mobilisationintracapsular
dissection - inflammatory
conditionsextracapsular
dissection -tumours.



Important landmark in submandibular gland dissection is the posterior border of the mylohyoid muscle.
The gland is retracted inferiorly, invariably attached to the lingual nerve through parasympathetic secretor motor fibres. Lingual nerve preserved.
Duct ligated and gland excised.
Dissection of the deep lobe and identification of the lingualnerve

Three cranial nerves are at risk during removal of the submandibular gland:
1 The marginal mandibular branch of the facial nerve.
2 The lingual nerve. 3 The hypoglossal nerve.

1. Haematoma;2. wound infection;3. marginal mandibular nerve injury;4. lingual nerve injury;5. hypoglossal nerve injury;6. transection of the nerve to the mylohyoid
muscle producing submental skin anaesthesia.
Complications of submandibular gland excision

Only 50% of submandibular gland tumours are benign, in contrast to 80–90% of parotid gland tumors.
In many circumstances, the swelling cannot, on clinical examination, be differentiated from submandibular lymphadenopathy.
Most salivary neoplasms, even malignant tumours, are often slow-growing, painless swellings.
SUBMANDIBULAR GLAND TUMORS


BENIGN & MALIGNANT NEOPLASMS ACCORDING TO SITE OF ORIGIN
parotid submandibular minor0
10
20
30
40
50
60
70
80
90
75
57
18
25
43
82
benign malignant


MALIGNANT SALIVARY NEOPLASMS
18%
13%
7%
4%
3%
33%
22%
Adenocarcinoma
Malignant mixed
Acinic cell
SCC
Other
Mucoepidemoid
Adenoid cystic

ENVIRONMENTAL : Radiation (ionising & UV radiation).
EBV. Silica dust. Early menarche &
nulliparity. Smoking (Warthin’s
tumor). Diet rich in PUFA
(protective)
GENETIC.
ETIOLOGY

PLEOMORPHIC ADENOMA most common benign tumor of both
major & minor salivary glands.
Peak incidence 4th & 5th decade with slight female preponderance.




Epithelial & modified myoepithelial cells intermingle with a stroma can be mucoid, myxoid, fibrous or chondroid.
Areas of oncocytic metaplasia are common & it can be misdiagnosed as oncocytoma.
Most characteristic appearance of stroma is the formation of mucoid or myxochondroid areas containing scattered epithelial cells with cartilaginous or osseous metaplasia.
MICROSCOPY

Principal clinical problem is recurrence (3.4 % in 5 yrs – 6.8 % in 10 yrs) and malignant progression.
RISK FACTORS FOR RECURRENCE :Variable / Absent capsulation.Intracapsular invasion.Improper excision.

MALIGNANT SUBMANDIBULAR GLAND TUMOR

MC malignant tumor of salivary gland..
Low grade : predominance of mucous secreting cells with well differentiated epidermoid cells.
High grade : few or no mucous producing cells and poorly differentiated epidermoid cells.
MUCOEPIDERMOIDCARCINOMA

ADENOID CYSTIC CARCINOMA 15 % of salivary neoplasms. 2nd most common malignant tumor of
salivary glands. MC malignant tumor in submandibular, sublingual & minor salivary glands.
Peak incidence 5th & 6ht decade.MC site : oral cavity (50%) sinonasal tract (18%)

5 – 11 % of malignant tumors of salivary glands.
Presents at a younger age.Affects women > men.Arises MC in parotid.MICROSCOPY : cells with basophilic
cytoplasm associated with lymphoid infiltrate.Subtypes : solid, microcystic, papillary cystic
& follicular
ACINIC CELLCARCINOMA

Represents malignancy with both epithelial & mesenchymal elements.
3 – 12 % of salivary gland tumors.Carcinoma ex pleomorphic adenoma -
arising from pre exsisting pleomorphic adenoma. Malignant & metastatic components are epithelial in origin.
De novo malignant mixed tumor (CARCINOSARCOMA) :
with malignant features of both epithelial and mesenchymal components
MALIGNANT MIXED TUMOR

Con………………. malignant transformation occurs in 3 – 4 % of
all benign mixed tumors.Risk of malignant transformation of
pleomorphic adenoma increases with duration of disease. ( 1.5% within 5 yrs -
9.5% within 15 yrs).Features of malignancy in pleomorphic
adenomaNecrosis, calcification, hemorrhage and
excessive hyalinization.

Clinical features of malignant submandibular tumours
1. Rapid enlargement of the swelling.2. Induration and/or ulceration of the
overlying skin.3. Cervical node enlargement.
4. Ipsilateral weakness / numbness of tongue.
5. Fixity to mandible.

FNAC [ sensitivity : 85 – 99 % specificity : 96 – 100% ]
Open surgical biopsy is contraindicated.Trucut biopsy-inoperable tumor -lymphoma.
INVESTIGATIONS

CT better for identifying bone destruction of mandible .
MRI is better to detect - bone marrow involvement.
- perineural spread. - parapharyngeal
space involv.
OTHERS : PET scan, color doppler sonography.


PRIMARY TUMOR (T) :
Tx primary tumor cannot be assessedT0 no evidence of primary tumorT1 tumor <2cms without extraparenchymal extensionT2 tumor >2cms but not >4cms without extraparenchymal exten.T3 tumor >4cms and / or extraparenchymal extension.T4 tumor invades skin, mandible.
STAGING

REGIONAL LYMPH NODES (N)Nx nodes cannot be assessed N0 no nodal metastasisN1 single ipsilateral LN <3cmsN2a single ipsilateral LN >3cms but <6cmsN2b multiple ipsilateral LN <6cmsN2c bilateral / contralateral LN < 6cms.N3 LN >6cms

METASTASIS :Mx distant metastasis cannot be assessedM0 no distant metastasisM1 distant metastasis

STAGE I T1,2 N0 M0
STAGE II T3 N0 M0
STAGE III T1,2 N1 M0
STAGE IV T4 N0 M0 T3,4 N1 M0 ANY T N2 M0 ANY T N3 M0 ANY T ANY N M1
STAGE GROUPING

SURGERY
RADIOTHERAPY
CHEMOTHERAPY
TREATMENT

Tumours, surgical excision with a cuff of normal tissue is the goal.
suprahyoid neck dissection, preserving the marginal mandibular branch of the facial nerve, lingual nerve and hypoglossal nerves.
In cases of overt malignancy, modified neck dissection or radical neck dissection is appropriate.
SURGERY FOR TUMORS

suprahyoid neck dissection





RADIATION THERAPY
RECURRENT ESIDUAL
ERFACTORY

ADENOMA T1 – T2 MALIG LOW GRADE
T3 – T4 TUM. HIGH GRADE CLOSE MARGIN DEEP LOBE PERINEURAL SPREAD INTRAVASCULAR INV N+
NO RT
GIVE RT

RADIOTHERAPY
TELE THERAPY + / - BRACHYTHERAPY
DOSE 50-70 Gy
NERVE GRAFT IS NOT C/I FOR RT
RT TO IPSILATERAL NECK

RADIATION THERAPY COMPLICATIONS :
Severe xerostomia Sensory neural hearing loss Osteo necrosis of mandible.

CHEMOTHERAPY
NO ROLE IN ADJV. SET.USED SPARINGLY IN METS
UNRESECTABLE
DRUGS ADR PLAT 5-FU

FACTOR INFLUENCING SURVIVAL
Stage. Histology & grade. Site. Lymph node metastasis. Surgical margins Perineural spread. Dedifferentiation. (detrimental outcome)

BIOLOGICAL MARKERS
TUMOR SUPPRESSOR GENES & ONCOGENESPOOR PROGNOSTIC INDICATORS :
point mutation of TP 53 tumor suppressor gene
activation of c-myc & ras p 21 proto oncogene
low p 27 tumor suppressor gene expression
over expression of c-erb b2amplification of Her-2 / Neu
expressionDNA PLOIDY
aneuploidy poor prognostic indicator

TUMOR MARKERS MEC – MUC 1, MUC 4, MUC 5AC, MUC 5BSAG (salivary agglutinin)MASPIN CEA – glandular & highly diff. squamous cell ca.LACTOFERRIN – glandular tumorsAMYLASE – ACCPREKERATIN & VIMENTIN – pleomorphic adenoma

EFFECT OF STAGE ON SURVIVAL
94
50
18
81
40
10
73
33
00
102030405060708090
100
10 yr 15 yr 20 yr
SU
RV
IVA
L %
STAGE I
STAGE II
STAGE III & IV

THANK YOU