Product Theater : “Resmetirom for the Treatment of NASH ......F4 Phase 3 MAESTRO-NASH study: F2/F3...
41
Product Theater : “Resmetirom for the Treatment of NASH: Early Data from the Phase 3 MAESTRO Clinical Trials.” Dr. Stephen Harrison, M.D., Medical Director for Pinnacle Clinical Research, San Antonio, Texas, and Visiting Professor of Hepatology, Oxford University, and Principal Investigator of the MAESTRO studies AASLD 2020
Transcript of Product Theater : “Resmetirom for the Treatment of NASH ......F4 Phase 3 MAESTRO-NASH study: F2/F3...
-
Product Theater : “Resmetirom for the Treatment of NASH: Early Data from the Phase 3 MAESTRO Clinical Trials.”
Dr. Stephen Harrison, M.D., Medical Director for Pinnacle Clinical Research, San Antonio, Texas, and Visiting Professor of Hepatology, Oxford University, and Principal Investigator
of the MAESTRO studies
AASLD 2020
-
Conflicts
Advisory Board/Panel: Akero, Altimmune, Arrowhead, Axcella, Blade Therapeutics, Cirius, Civi Biotherma, CLDF, Cymabay, Echosens, Foresite Labs, Galectin, Galmed, Gelesis, Genfit, Gilead, Hepion, Hightide Bio, Histoindex, Indalo, Innovate, Intercept, Madrigal, Medpace, Merck, Metacrine, NGM Bio, Northsea, Novartis, Novo Nordisk, Perspectum, Poxel, Prometic, Ridgeline Therapeutics, Sagiment, Terns, Viking
Consultant: Akero, Altimmune, Axcella, Blade Therapeutics, Cirius, Civi Biopharma, CLDF, Cymabay, Echosens, Enyo, Foresite Labs, Fortress, Galectin, Galmed, Gelesis, Genfit, Gilead, Hepion, Hightide Bio, Histoindex, Indalo, Innovate, Intercept, Kowa, Madrigal, Medpace, Medpace, Merck, Metacrine, NGM Bio, Northsea, Novartis, Novo Nordisk, Perspectum, Poxel, Prometic, Ridgeline Therapeutics, Sagiment, Silverback, Terns, Viking
Principal Investigator of Grant Research: Axcella, BMS, Cirius, Civi Biopharma, Conatus, Cymabay, Enyo, Galectin, Galmed, Genetech, Genfit, Gilead, Hepion, Hightide Bio, Immuron, Intercept, Madrigal, NGM Bio, Northsea, Novartis, Novo Nordisk, Pfizer, Sagiment, Second Genome, Tobira/Allergan, Viking
Stock/Shares (self-managed): Akero, Cirius, Galectin, Genfit, Histoindex, Madrigal, Metacrine, NGM Bio, Northsea
2
-
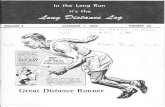
Non-Alcoholic Fatty Liver Disease (NAFLD) Ranges from Simple Steatosis (NAFL) to NASH, a Progressive Form of Liver Disease
3
OUTCOME
◼ NAFLD results from accumulation of excess fat within the liver (steatosis) unrelated to alcohol use
◼ Some patients with NAFLD have NASH (nonalcoholic steatohepatitis)
◼ 25 – 30% of all adults in Western countries have NAFLD
◼ NASH afflicts 3 – 12% of the U.S. population. In certain populations such as diabetics fat in the liver is virtually always NASH.
◼ NAFLD leads to an increased risk of morbidity and mortality from:— Cardiovascular disease (leading cause
of death for NAFLD patients)— Liver-related events
◼ 11% of advanced NASH patients progress to cirrhosis over a 15-year period
Harmful Steatosis
Normal Liver
Lobular inflammation
Ballooning degeneration
Fat Accumulation
NAFLD Spectrum
IsolatedSteatosis
Nonalcoholic Fatty Liver (NAFL)
NASH Fibrosis
NASH Cirrhosis
NASH
DISEASE
INCIDENCE
-
Mechanism of Action: The Importance of Liver THR-β in NASH
4
Lowers LDL-cholesterol Lowers triglycerides Lowers liver fat, potentially reducing
lipotoxicity, NASH
No thyrotoxicosis (THR-α effect)
In humans, thyroid hormone receptor-β (THR-β) agonism:
Sinha and Yen Cell Biosci (2016) 6:46DOI 10.1186/s13578-016-0113-7; Autophagy, 11:8, 1341-1357, DOI: 10.1080/15548627.2015.1061849
Resmetirom (MGL-3196)
◼ THR-β selective liver targeted molecule, once a day oral, with proven safety and efficacy in more than 500 subjects and patients treated
— No exposure outside the liver or activity at the systemic THR-α receptor
◼ Pleiotropic effects in the liver with potential for addressing the underlying metabolic syndrome and hallmark features of NASH: steatosis/lipotoxicity, inflammation, ballooning, fibrosis (both directly and indirectly)
— Reduction of liver fat through breakdown of fatty acids, normalization of mitochondrial and liver function
Thyroid
Gland
Liver
T4➔ T3
T3
Nu
clea
r T
HR
-α, T
HR
-β
Thyroid Hormone Pathway
T4T4
T4, prohormoneT3, active hormone
-
Compound/Indication
Clinical TrialPre-
ClinicalPhase 1 Phase 2 Phase 3 Description
Resmetirom(MGL-3196)
Thyroid Hormone Receptor-β (THR-
β) Agonist
Treatment of Nonalcoholic
Steatohepatitis (NASH)
Phase 2MGL-3196-05NCT02912260
◼ MRI-PDFF, biopsy: positive
• 36 week with 36 week open-label extension
Harrison Lancet. 2019 Nov 30;394(10213):2012-2024.
doi: 10.1016/S0140-6736(19)32517-6
Phase 3 MAESTRO-NASHNCT03900429
◼ Treatment of NASH with Fibrosis Stage 2-3
• Serial liver biopsy• 52 week Phase 3; 54
month Phase 4
Phase 3 MAESTRO-NAFLD-1 (presumed NASH) NCT04197479
◼ Treatment of NASH• 52 week• Safety, Lipids and NASH
biomarker and imaging study
• Enrollment of double-blind arms completed
• Open label 100 mg arm; includes NASH cirrhotics
5
Recruiting
Recruiting
Phase 3 NASH Clinical Trials, Ongoing: MAESTRO-NASH and MAESTRO-NAFLD-1
Completed
Madrigal is focused on developing resmetirom for the treatment of NASH
-
Resmetirom Development Path Across the Spectrum of NAFLD/NASH
6
F3
F4 Phase 3 MAESTRO-NASH study: F2/F3 NASH with Metabolic SyndromeNASH Resolution (primary), LDL-C, fibrosis (key secondary); Phase 4 (post-approval): cirrhosis and MACE
F2
F1B
F1
F0
ResmetiromCV Benefits
Fatty liverLDL-CApoBTriglyceridesLp(a)
Phase 3 MAESTRO-NAFLD-1 study:F1-F3 NASH with Metabolic Syndrome diagnosed non-invasively (no liver biopsy requirement)100 mg Open label armEndpoints; Safety, LDL-C, lipids, MRI-PDFF, PRO-C3
2.0 million
3.5 million
6.3 million
3.4 million
1.3 million
NASH/NAFLD Spectrum1
US PatientNumbers
1 Estes et al; Hepatology, Vol. 67, No. 1, 2018 2 Henson Aliment Pharmacol Ther. 2020;51(7):728-736; Clinical Gastroenterology and Hepatology 2020;18:2324–2331.
Total US NAFLD: (NASH plus NAFL)83 million (2015)
Data show that NASH with fibrosis is associated with highest CV risk2
-
Phase 2 NASH Study Design: Randomized, Double-Blind, PBO Controlled
7
◼ Comparator/Arms
— 2:1 Resmetirom to placebo
— 125 patients enrolled in USA, 18 sites
— Resmetirom or placebo, oral, once daily; dose 60-80 mg
◼ Inclusion/Exclusion
— NASH on liver biopsy: NAS≥4 with fibrosis stage 1-3
— ≥10% liver fat on MRI-PDFF
— Includes diabetics, statin therapy, representative NASH population
◼ 36 week extension study (OLE) in 31 patients who completed the Main 36 week study- all received 80 or 100 mg of resmetirom
Open-label Extension (OLE) Study
Screening
MRI-PDFFLiver Biopsy
MRI-PDFFLiver BiopsyMRI-PDFF MRI-PDFFPK
D1 W2 W4 W12 W36 W12 W36OLED1
36 Week Main Study
MRI-PDFF
Harrison Lancet. 2019 Nov 30;394(10213):2012-2024.doi: 10.1016/S0140-6736(19)32517-6
-
◼ Decreases inflammation on biopsy
◼ Continued, sustained decreases in elevated liver enzymes, many reaching normal levels (60% with ALT
-
Resmetirom: Fibrosis, Non-invasive and Liver Biopsy Readouts Phase 2
9
◼ Liver biopsy trend favoring resmetirom for 1-point improvement in fibrosis
— 56% of patients who resolved NASH also resolved fibrosis, 61% of NASH resolvers achieved ≥ 1 point improvement in fibrosis
— Half of F3 patients showed ≥ 1-point improvement in fibrosis, compared to no placebo F3 patients, using Second Harmonic Generation
◼ Statistically significant reductions by resmetirom in multiple fibrosis biomarkers including PRO-C3, ELF, most pronounced in patients with advanced fibrosis at baseline (F2 / F3)
◼ Biomarker of net collagen formation (PRO-C3/C3M) –reduced by resmetirom
◼ Reduction in fibroscan (kPa), a measure of liver stiffness (fibrosis), in 36 week open-label extension study
NASHFibrosis
Phase 3 NASH study is >90% powered to show a 1-point improvement in fibrosis on biopsy
*Schuppan 2018 https://doi.org/10.1016/j.matbio.2018.04.006
collagenpro-collagen
myofibroblasts
bloodFibrogenesis: PRO-C3, P3NP, hyaluronic acid, TIMP-1Fibrinolysis: C3M
pro-peptide cleavage
-
Non-invasive Biomarkers and Imaging to Follow Patient Response to Resmetirom
10
36 Week OLE Study
W12
36 Week Main Study
W36BL OLE W12 OLE W36BL-E
Res-Res
Pbo-Res
PDFF PDFF PDFF PDFF PDFFBiopsy Biopsy
Biomark Biomark Biomark Biomark Biomark
Dose adjusted to 60 or 80 mg Dose increased to ≥80 or 100 mg
Resmetirom (Res)Placebo (Pbo)
5
10
15
20
25
30
0 12 36 OLE W12 OLE W36
PD
FF
% o
r P
RO
-C3
(n
g/m
l)
Pbo/Res PRO-C3 Res/Res PRO-C3
Pbo/Res PDFF Res/Res PDFF
-2 -2.2-1.8
-3.4
-5
-4
-3
-2
-1
0
p=.006 p=.001 p
-
Secondary Phase 2 Study Analysis: Relationship of MRI-PDFF Response to NASH Biopsy Response
◼ To determine the potential predictive power of liver fat reduction on NASH resolution, data were analyzed from 107 NASH patients (n=34 placebo, n=73 resmetirom) with paired baseline/week 36 liver biopsies (read by two independent blinded central pathologists) and paired baseline/week 12 MRI-PDFFs
— There were 5 placebo (4/5 with >5% weight loss) and 45 resmetirom patients who had at least 30% fat fraction reduction at Week 12 and a paired liver biopsy at Week 36 (PDFF Responders)
◼ Including the MRI-PDFF/biopsy data from both MRI-PDFF responders and non-responders the relationship to a NASH resolution response, NAS component and fibrosis responses were assessed
11
-
Results from Phase 2 Study
12
◼ Primary endpoint achieved, relative reduction in hepatic fat on
MRI-PDFF at Week 12
— Dose dependent 50% reduction of hepatic fat at 80 mg
dose
◼ Key secondary and exploratory endpoints achieved
— Statistically significant reduction and resolution of NASH
as compared with placebo
— Statistically significant reduction in fibrosis biomarkers
— Statistically significant reduction in liver enzymes
— Statistically significant reduction in LDL-cholesterol,
apolipoprotein B, triglycerides and lipoprotein(a)
◼ Safety
— No change in Grade 2 or higher AEs— No safety signals related to mechanism of action
Resmetirom responders with 30% PDFF reduction had higher rates of NASH
resolution (37%) on Week 36 liver biopsy compared to non-responders (4%)1—
hypothesis generating
-10 -14
-36 -40 -39-50 -55
-64
-70
-60
-50
-40
-30
-20
-10
0
All All 60mg 80mg 80-100mg
100 mg
Wk 12 Wk 36 Wk 12 Wk 36 Week 36 Week 36 Week 36 Week 36
Placebo Resmetirom (NASH Phase 2) Resmetirom(Phase 2 Ext)
% R
ela
tive
Red
uciton
in H
ep
atic F
at
Relative Fat Reduction (%)
1Harrison Lancet. 2019 Nov 30;394(10213):2012-2024.doi: 10.1016/S0140-6736(19)32517-6
-
Association of NASH Resolution with Early (Week 12) PDFF Response
◼ The predictive accuracy of PDFF response for NASH resolution was determined by calculating the area under the receiver operating characteristic curve (AUROC) and its 95% confidence intervals (CI)s.
◼ The AUROC was 0.87, the optimal MRI-PDFF reduction with best balance of true positive and false negative rates was 41.5% (p
-
PDFF Responder Analysis: NASH Resolution
◼ Two blinded pathologists (Path A, Path B) independently reviewed the Phase 2 slides
◼ Compared to MRI-PDFF non-responders (=40% p=0.0022
Path A>=30%p
-
Relationship of PDFF Response to Biopsy Component Response
◼ All patients in the study with serial evaluable liver biopsies (baseline and week 36) and PDFFs (baseline and week 12) were included in the analysis
◼ Statistically significant differences were observed between Week 12 PDFF responders(≥30% fat reduction) and non-responders
◼ Improvement and less worsening of all component responses (ballooning, inflammation, steatosis and fibrosis) were observed in PDFF responders
15
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
>=30 PDFFResponse
=30 PDFFResponse
=30 PDFFResponse
=30 PDFFResponse
=30 PDFFResponse
=1 point) Steatosis Ballooning Lob Inf Fibrosis
Improved Unchanged Worse
-
Association of PDFF Response with NASH Resolution and Fibrosis Reduction -Resmetirom
◼ Percentages of patients with NASH resolution
increased with greater PDFF reduction (agreement
between two independent central pathology
readers)
◼ In resmetirom-treated patients with ≥ 50% fat
reduction at Week 12, 64% had NASH resolution
with a component response driven primarily by
ballooning and inflammation
◼ PDFF reduction 30 and 50% at Week 12 was also
associated with
— Fibrosis reduction on subsequent liver biopsy
— Achievement of both endpoints: NASH resolution
and 1 point fibrosis reduction
16
0
10
20
30
40
50
60
70
NASH Resolution(NR)
Fibrosis Reduction Both NR and fibrosisreduction
% R
esp
on
se
>50% PDFF >=30% PDFF MRI-PDFF Non-Responder
Non Responder:
-
Analysis of Patient Reported Outcome in 36 Week Phase 2 NASH Study
◼ In the resmetirom Phase 2 NASH study, Health Related Quality of Life (HRQL) was assessed using self-administered Short Form-36 (SF-36) using 8 domains throughout 36 weeks of treatment and was pre-specified as an exploratory study endpoint
◼ Wilcoxon paired rank sign tests were conducted for SF-36 domains changes from Baseline at Week 36 (completers only) for within-group differences of placebo vs resmetirom, PDFF responder vs Non-responder, sex hormone binding globulin (SHBG) increase 88% vs
-
MRI-PDFF Response at Week 12 Associates with Improved HRQL at Week 36
18
-4
-2
0
2
4
6
8
10
12
14
PhysicalFunctioning Role Physical Bodily Pain General Health Vitality Social Functioning Role Emotional Mental Health
PhysicalComponentSummary
Mental ComponentSummary
HRQL Score Change from Baseline at Week 36
All PDFF Responder
All PDFF Non Responder
MGL-3196 PDFF Responder
PDFF responder : >=30% liver fat reduction on PDFF at Week 12
◼ HRQL score change from baseline at Week 36 for each individual component and summary components, ALL PDFF responders (treatment arms pooled), and resmetirom-treated PDFF responders experienced improvement in health-related scores at Week 36 (PDFF responder >=30% fat reduction at Week 12)
HRQL Change from Baseline at Week 36
-
Comparison of Resmetirom-treated Relative to Placebo
19
Role PhysicalBodily Pain
General HealthVitality
Social Functioning
Physical Component Summary
Mental Component Summary
-10 -5 0 5 10 15
HRQL Change from Baseline at Week 36 for Resmetirom MRI-PDFF Responders
Role Physical
Bodily PainGeneral Health
VitalitySocial Functioning
Physical Component SummaryMental Component Summary
-10 -5 0 5 10 15
HRQL Change from Baseline at Week 36 for Placebo
◼ In line with its safety and tolerability profile, improvements at Week 36 were observed in resmetirom-treated Week 12 PDFF Responders compared to placebo
— Bodily Pain (mean(SE): 9.6(3.4), p=0.045)
— Resmetirom high exposure patients compared to placebo for Bodily Pain (mean(SE): 8.88(3.12), p=0.036) and resmetirom-treated PDFF Responders for Physical Component Summary (mean(SE): 3.35(0.82), p=0.051).
HRQL Change at Week 36 Placebo
HRQL Change at Week 36 Resmetirom PDFF Responders1
1 ≥30% liver fat reduction on Week 12 MRI-PDFF
-
Summary of Patient Reported Outcomes from Phase 2
◼Resmetirom Phase 2 data demonstrated a statistically significant improvement in several components of physical well-being at 36 weeks in patients with ≥ 30% PDFF reduction, including improvements in resmetirom-treated relative to placebo
◼Ongoing Phase 3 MAESTRO-NASH (NCT03900429) and MAESTRO-NAFLD-1 (NCT04197479) studies will assess Improvement in Quality of Life parameters associated with resmetirom treatment
20
-
Phase 3 MAESTRO-NASH Study Design: Randomized, Double-Blind, PBO Controlled: Serial Liver Biopsy Study
21
Comparator/Arms
◼1:1:1 MGL-3196 80, 100 mg , placebo
◼900 F2/F3 patients enrolled in USA, Europe for primary Week 52 analysis, ~200 F1 patients
◼Up to 2000 patients total enrollment for Phase 4 including first 900
◼ >150 centers, world-wide
Key Inclusion/Exclusion
◼Requires 3 metabolic risk factors (Metabolic Syndrome); Fibroscan kPa consistent with F2-F3, CAP≥280
◼NASH on liver biopsy: NAS≥4 with fibrosis stage 1A (up to 3%) 1B, total F1 up to 15%; F3, at least 50%, the rest F2
◼ ≥8% liver fat on MRI-PDFF
Primary Endpoints
◼Resolution of NASH at Week 52 with at least 2 point reduction in NAS
—Key secondary endpoints LDL-C lowering at Week 24, reduction in fibrosis stage Week 52 biopsy
◼Composite liver-related outcome at 54 months [histologic evidence of cirrhosis on biopsy, MELD>=15, hepatic decompensation, liver transplant, all cause mortality]
Outcome Endpoint
Screening
MRI-PDFFLiver BiopsyLDL-C
D1 W16 W24 W52
52 Week Primary Endpoint
Month 54
80 mg
100 mg
Placebo
Ra
nd
om
iza
tio
n
-
AASLD, 2020
22
#1657 ALGORITHM FOR PREDICTING ADVANCED NASH FIBROSIS ON SCREENING BIOPSY IN RESMETIROM PHASE 3 MAESTRO-NASH CLINICAL TRIAL Stephen A. Harrison, Oxford University; Rebecca Taub, Madrigal Pharmaceuticals; Morten A. Karsdal, Nordic Bioscience; John Franc, Madrigal Pharmaceuticals; Mustafa R. Bashir, Department of Radiology, Duke University Medical Center; Jordan Barbone, Madrigal Pharmaceuticals; Guy Neff, Covenant Research, LLC; Nadege T. Gunn, Pinnacle Clinical Research; Sam Moussa, Adobe Gastroenterology
-
MAESTRO-NASH Screening Algorithm
Enrolling NASH fibrosis studies is particularly challenging because most patients at the time of screening do not have a definitive diagnosis of NAFLD (or NASH) and their fibrosis stage is unknown
23
RISK FACTORS for NASH
> Age >50
> BMI >30
> Elevated Liver enzymes (AST >20 U/L, AST/ALT ≥1)
> Type 2 Diabetes
> Hypertension
> Dyslipidemia
> Metabolic Syndrome
> Historical Fibroscan >8.5 kpa, CAP >280 dB/M (Ideally 300)
MAESTRO-NASH 8 Week Screening Process
≥3 Metabolic Risk Factors
FibroscankPa>=8.5CAP>=280
Medicalhistory
LabsMRI-PDFF
≥ 8%Liver Fat
Liver BiopsyNAS≥4All NAS
componentsF2-F3,F1B or
F1A/1C with PRO-C3 ≥14(OR historic liver biopsy)
Randomize
-
Biopsy Success Rate in MAESTRO-NASH
24
◼ ~70% of biopsies met eligibility requirements
◼ ~80% had NASH, some with NASH cirrhosis, or advanced NASH (F2-F3) with NAS14 ng/mL 10.3%
Total Qualifying Biopsies 70.6%
Non-qualifying Biopsies with NASH, F1-F4
NAS, >=3 (
-
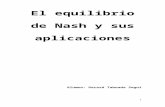
PRO-C3 and Fibroscan Alignment with Baseline Biopsy Fibrosis Stage
◼ When measured in patients with baseline fibroscan kPa≥8.5, PRO-C3 aligned with biopsy F1-F3 NASH fibrosis stages
◼ Fibroscan appeared to be more predictive of NASH cirrhosis than PRO-C3
NOTE: the study only assessed biopsies in patients with biopsy-eligible fibroscanscores (≥8.5)
25
6.1
21.6
10.312.0
15.6
12.8
7.2
29.9
10.7
14.4
18.4
15.3
7.7
24.4
12.714.3
18.6
15.9
7.8
32.8
12.3
15.7
20.8
17.4
6.1
41.1
12.6
17.4
25.0
20.1
9.4
26.0
11.2
13.9
19.8
15.6
0(n = 47)
1A/1Cn = 69
1B(n = 37)
2(n = 125)
3(n = 186)
4(n = 11)
PR
O-C
3 (
ng
/mL
)
0
5
10
15
20
25
30
35
40
45
PRO-C3 by Fibrosis stage
rho = 0.24, p < 0.001
without stage 4: rho = 0.28, p < 0.001
5.3
14.4
8.89.8
11.810.8
5.1
15.6
8.59.911.5
10.0
4.0
15.8
8.910.3
12.211.1
5.3
17.8
9.2
11.1
12.911.7
5.4
23.8
9.8
12.0
15.5
13.8
9.2
35.4
12.2
21.0
34.6
26.7
0(n = 40)
1A/1Cn = 56
1B(n = 32)
2(n = 113)
3(n = 171)
4(n = 9)
TE
(kP
a)
0
5
10
15
20
25
30
35
40
TE by Fibrosis stage
rho = 0.3, p < 0.001
without stage 4: rho = 0.28, p < 0.001
0
10
20
30
40
50
60
0 20 40 60 80
TE
(kP
a)
PRO-C3 (ng/mL)
PRO-C3 and TE
PRO-C3 by Biopsy Fibrosis Stage LSM (fibroscan kPa) by Biopsy Fibrosis Stage
PRO-C3 vs Fibroscan Score
LSM, liver stiffness measure
-
PRO-C3 Alignment with NAS Components
26
6.1
24.0
10.312.3
15.813.4
6.1
31.3
11.8
15.4
19.7
16.6
7.8
42.3
13.9
18.2
25.9
21.3
0(n = 88)
1(n = 232)
2(n = 152)
PR
O-C
3 (
ng
/mL
)
0
5
10
15
20
25
30
35
40
45
rho = 0.34, p < 0.001
6.1
12.19.711.712.112.1
6.1
30.1
10.5
13.9
18.4
15.6
6.1
33.7
13.2
16.6
21.8
18.2
9.9
47.1
13.5
21.9
29.4
24.4
0(n = 13)
1(n = 200)
2(n = 217)
3(n = 41)
PR
O-C
3 (
ng
/mL
)
0
5
10
15
20
25
30
35
40
45
50
rho = 0.29, p < 0.001
PRO-C3 by Biopsy Ballooning PRO-C3 by Biopsy Lobular Inflammation
9.20
12.00
9.20
11.8012.0011.009.30
12.109.8511.7512.0811.23
6.10
24.00
8.9510.70
16.98
13.54
6.10
21.80
10.1511.85
15.5013.31
6.10
26.00
11.10
13.90
17.8015.91
6.10
31.40
12.83
16.45
20.78
17.28
8.10
38.10
13.63
18.05
24.40
20.02
8.80
41.10
14.10
17.90
26.10
21.57
9.90
27.40
12.53
18.75
26.6524.33
0(n = 3)
1(n = 4)
2(n = 24)
3(n = 54)
4(n = 105)
5(n = 124)
6(n = 92)
7(n = 51)
8(n = 14)
PR
O-C
3 (
ng
/mL
)
0
5
10
15
20
25
30
35
40
45
rho = 0.37, p < 0.001
Score:
NAFLD Activity Score (NAS)
PRO-C3 by Biopsy NAS
◼ PRO-C3 levels were significantly correlated with ballooning, lobular inflammation and NAS
◼ Biopsy steatosis score was weakly aligned with PRO-C3
-
Summary: MAESTRO-NASH Enrollment Data
◼ In a large dataset, presence of 3 metabolic risk factors and Fibroscan TE≥8.5kPa predicted biopsy-confirmed NASH in 81% of patients
◼ PRO-C3 is a marker not only of fibrosis stage in NASH but also of the level of NASH activity (inflammation and ballooning) in the NASH liver
— Findings are consistent with recent literature1
◼ In the absence of a liver biopsy, elevated PRO-C3 in the setting of metabolic syndrome (or FIBC3 (PRO-C3 (age, BMI, platelets, T2D)), fibroscan and MRI-PDFF may predict advanced NASH
27
1https://doi.org/10.1016/j.jhepr.2019.06.004
-
Phase 3 MAESTRO-NAFLD-1 (presumed NASH) Study Design: Randomized, Double-Blind, PBO Controlled
Comparator/Arms
◼1:1:1:1 resmetirom 80, 100 mg , placebo, open label 100 mg
◼700 NASH patients enrolled in the USA (~65 sites); 700 patient target exceeded by Sept 2020
Inclusion/Exclusion ◼Requires 3 metabolic risk factors (Metabolic Syndrome)
◼ Fibroscan kPa≥ F1, CAP≥280, except where eligible for MAESTRO-NASH; includes MAESTRO-NASH patients who screen fail at the biopsy stage
◼ ≥8% liver fat on MRI-PDFF
◼Open label arm, >100 patients— NASH patients on 100 mg resmetirom to assess non-invasive measure of safety and efficacy— Open-label treatment of special safety population, e.g. compensated cirrhosis
Endpoints◼Primary safety objective: to evaluate the safety and tolerability of once-daily, oral administration of 80 or 100 mg resmetirom versus
matching placebo as measured by: Incidence of Adverse Events [ Time Frame: 52 weeks ]◼Key efficacy objectives: percent change from baseline in LDL-C; percent change from baseline in ApoB; percent change from baseline in
hepatic fat fraction by MRI-PDFF; percent change from baseline in triglycerides; change in PRO-C3
52 Week Primary Endpoint
28
A “Real-life” NASH Study with Non-invasive Monitoring of Patient Response
Screening
MRI-PDFFFibroscanLDL-C (lipids)
D1 W16 W24 W52
80 mg
100 mg
Placebo
Ra
nd
om
iza
tio
n
Extension
100 mg Open Label
-
#1707 TREATMENT WITH RESMETIROM IN PHASE 3 MAESTRO-NAFLD-1 NASH STUDY OPEN LABEL ARM: EFFECTS ON BIOMARKERS AND IMAGING
◼ An exploratory evaluation of safety, imaging and biomarkers was conducted in patients enrolled in the open label 100 mg active treatment arm of MAESTRO-NAFLD-1
◼ Typically ~20% of the overall NASH population are on thyroxine for the treatment of hypothyroidism. Thyroxine has equal activity at the thyroid receptor alpha and beta receptors
— In order to assess the effects of resmetirom in NASH patients on thyroxine, a subgroup of the open label arm included patients on stable thyroxine (patients on thyroxine are also enrolled in the double-blind arms)
— More females were on thyroxine as a percentage of enrolled open label patients (49.4% versus 19.4% male)
◼ Data analysis — Group included open label patients that had completed at least 16 weeks of dosing— MRI-PDFFs and MREs were assessed in patients who had both baseline and Week 16 MRI-PDFFs and MREs
29
Dr. Stephen A Harrison, Pinnacle Clinical Research, Dr. Naim Alkhouri, Arizona Liver Health, Dr. Rebecca A. Taub, Madrigal Pharmaceuticals, Dr. Guy Neff, Covenant Research, LLC, Dr. Seth J Baum, Excel Medical Clinical Trials and
Dr. Mustafa R Bashir, Department of Radiology, Duke University Medical Center AASLD 2020
-
Baseline Characteristics
◼ Demographics include— Mean age 55.7,— female 71%,— BMI 36.2,— diabetes 41%,— hypertension 64%, — dyslipidemia >70%, — hypothyroid 41%— mean ASCVD score 11.1%
◼ Fibroscan (kPa 7.4) and mean MRI-PDFF 18% are consistent with, on average, F2-stage NASH
— Comparatively, MAESTRO-NASH fibroscan mean is consistent with F3
30
ParameterMean age, years (SD) 55.7(11.3)
Male, n (%) 36(29%)Female, n (%) 87(71%)
Hispanic/Latino, n (%) 32(26%)
Mean Body weight (SD) (kg) 99.3(19.8)BMI mean (SD) (kg/m2) 36.2(6.2)Hypertension, n (%) 79(64%)Hypothyroid#, n (%) 50(41%)
T2D, n (%) 50(41%)T2D Yrs since diagnosis mean (SD) 10.1(7.5)ASCVD score mean (SD) 11.1%(11.7%)
Fibroscan TE mean (SD) (kPa) 7.4(2.9)Fibroscan CAP mean (SD) 341(35.0)
MRI-PDFF mean (SD) (%FF) 18.0%(6.9%)MRE mean (SD) (kPa) 2.67(0.73)
PRO-C3 mean (SD) (ng/ml) 12.8(5.6)HbA1c mean (SD) (%) 6.3(1.0)
HOMA-IR mean (SD) 8.9(8.9)
Statin use (n, %) 56(46%)GLP-1s (n, %) 15(12.2%)SGLT2s (n, %) 16(13.0%)
Other lab parameters, mean (SD)
MELD 7.0(1.6)
NAFLD fibrosis score -1.2(1.3)
Fib-4 0.99(0.50)
Total Cholesterol mean (SD) (mg/dL) 190.2(49.2)
TG mean (SD) (mg/dL) 186.9(85.5)
Lp(a) mean (SD) (nmol/L) 46.1(64.3)
ApoB mean (SD) (mg/dL) 102.9(29.6)
LDL-C mean (SD) (mg/dL) 117.7(42.5)
HDL-C mean (SD) (mg/dL) 44.2(11.9)
ALT (IU/L) 36.6(23.7)
AST (IU/L) 25.5(12.4)
GGT (IU/L) 44.1(46.5)
CK (IU/L) 121.2(111.6)
ALP (IU/L) 83.6(26.5)
Total bilirubin (mg/dL) 0.55(0.21)
Direct bilirubin (mg/dL) 0.10(0.04)
Platelet count 263(67)Albumin (g/dL) 4.3(0.3)
INR 1.1(0.3)
CDT (%) 1.62(0.23)
-
Week 16 MRI-PDFF (%) and MRE (kPa) Changes from Baseline
◼ MRI-PDFF reduction of 53% fat fraction overall, and MRE (-0.34) were observed at Week 16
◼ MRE, unlike other elastography techniques, provides a stiffness map (elastogram)
— The volume of liver parenchyma assessed with a single slice of MRE is about 250 cm31
— Shear wave elastography (20 cm3), point shear wave elastography (0.5–1.0 cm3), transient elastography (4 cm3), and nearly 500 times that of a liver biopsy (10–50 mm3 or < 0.05 cm3)
31
All SHBG (high)
MRI-PDFF (%)
Baseline (%) 17.6 17.9
Relative % Change -53% -62%
p-value
-
MRI-PDFF Subgroups
◼ PDFF reduction of ≥60% was observed in subgroups: stable GLP-1 (no weight loss), ≥5% weight loss, or high SHBG response
◼ Factors that mildly decreased PDFF response included diabetes, thyroxine treatment, low baseline MRI-PDFF or low SHBG response
32
Week 16 MRI-PDFF Relative % Change from Baseline)
-
◼ At weeks 12-24, decreases from baseline in ALT, AST, GGT occurred to the normal range in most patients; statistically significant reductions in inflammatory and fibrosis biomarkers PRO-C3, hsCRP and reverse T3 were observed
◼ Liver enzyme and biomarker responses were consistent with Phase 2 data
33
Inflammatory and Fibrosis Biomarker Responses
Biomarker* Baseline SDPost-
Baseline* SD CFB P valueALT (BL >34 U/L) 58.3 47.4 38.9 16.1 -17.7 26 U/L) 39.3 12.2 31.8 11.3 -6.9 0.0060GGT (BL >30 U/L) 70.2 58.3 54.6 47.8 -16.2 0.0015Adiponectin (ug/mL) 5.0 3.5 5.9 1.6 0.9
-
Reduction in Lipids and Lipoproteins
◼ LDL-C, apolipoprotein-B (-24%), triglycerides (23%), and lipoprotein(a) (-27%)) were statistically significantly reduced (p
-
Safety
◼ Resmetirom was well-tolerated with loose stools lasting
-
Summary
◼ In this 52 week Phase 3 open label study, NASH patients identified using non-invasive imaging and biomarkers were treated with resmetirom 100 mg and demonstrated rapid reduction in hepatic fat, liver stiffness on MRE, fibrosis and inflammation biomarkers and atherogenic lipids after 16 weeks of treatment
◼ Safety was supportive of an 100 mg dose of resmetirom, including in patients on thyroxine
◼ Assessments of serial non-invasive biomarkers potentially supports the use of non-invasive tests to monitor individual NASH patient response to resmetirom treatment
36
-
BACKUP
37
-
Monitoring Individual Patient Response to Treatment
◼ The magnitude of SHBG increase (16 weeks, mean % increase (132% (84%)) was significantly correlated with reductions in liver enzymes, MRI-PDFF, LDL-C and other lipids
◼ Taken together, serial non-invasive biomarkers and imaging tests may have the potential to monitor individual patient resmetirom response to treatment
38
-
PDFF Response, Biopsy and Non-invasive Tests
◼ All NAS component changes showed a relationship to PDFF response
◼ High correlation R2~0.4 between steatosis change on biopsy and PDFF response at both Weeks 12 and 36, p
-
Phase 2: Another Important Non-invasive Measure of Efficacy- Robust Lipid Lowering
Significant sustained lowering effect in multiple atherogenic lipids
40
Lipids (% Change from Baseline)
Resmetirom compared with placebo; all analyses and cutoffs were prespecified; based on prespecified mITT; placebo n=39; Resmetirom n=79 (LOCF)
-22.3-27.6
-36 -36.8 -36.5
-50
-40
-30
-20
-10
0
LDL-C(BL>100)
ApoB (LDLBL>100)
TGs Lp(a)(BL>=10)
ApoCIII
p
-
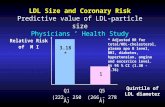
120
32
47
0
10
20
30
40
50
All F3
p=0.03 p=0.05
% b
iop
sie
s
Placebo MGL-3196
Week 36: Change in Fibrosis Score on Liver Biopsy
41
◼ Second Harmonic Generation (SHG) microscopy provides automated fully quantitative assessment of fibrosis on liver biopsy slides based on unique architectural features of collagen
◼ SHG score was generated and aligned with the pathologist baseline score (baseline, r=0.76), (left panel), blinded to treatment code
◼ Using SHG, resmetirom treated compared with placebo showed a statistically significant ≥1-pt reduction in fibrosis score at Week 36. Based on pathology score, fibrosis was reduced by ≥ 1 point in 29% of resmetirom treated patients vs. 23% in placebo
≥1 pt reduction in fibrosis on liver biopsy (SHG)
Pathologist Score
SHG
(q
fib
rosi
s)
https://doi.org/10.1371/journal.pone.0199166Week 36 pathology scores and treatment code were not provided to SHG readers.
3
2
1
0
SHG Score
0 1A 1B 2 30.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
https://doi.org/10.1371/journal.pone.0199166