
Product Portfolio - Arthrosurface · • Maintains soft-tissue envelope and native joint mechanics...
15
Product Portfolio International
Transcript of Product Portfolio - Arthrosurface · • Maintains soft-tissue envelope and native joint mechanics...

1
Product PortfolioInternational

3
CONTENTS
Biologics
Pg. 4-5 NanoFx
HemiCAP Resurfacing
Pg. 6-7 Shoulder (25mm, 30mm, 35mm, 40mm, OVO)
Pg. 8-9 Patello Femoral Classic
Pg. 10-11 Patello Femoral Wave
Pg. 12-13 UniCAP (Classic & Small)
Pg. 14-15 Femoral Condyle
Pg. 16-17 Toe DF
Pg. 18-19 Toe Classic
Pg. 20-21 Talus
Pg. 22-23 Hip
Plates & Screws
Pg. 24-25 CheckMATE Arthrodesis System
Additional Information
Pg. 26-27 Key Surgeons & Reference Articles
5
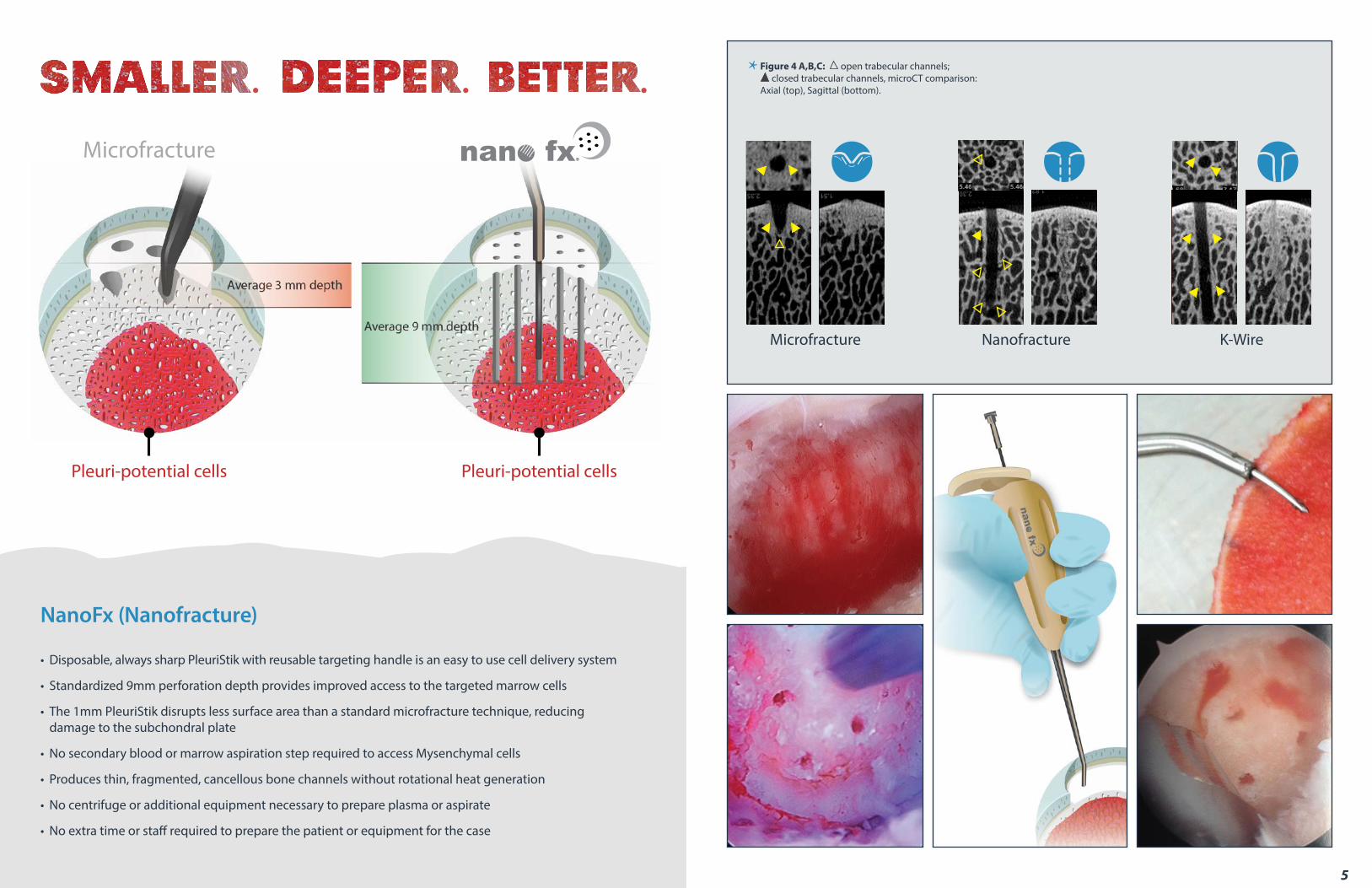
NanoFx (Nanofracture)
• Disposable, always sharp PleuriStik with reusable targeting handle is an easy to use cell delivery system
• Standardized 9mm perforation depth provides improved access to the targeted marrow cells
• The 1mm PleuriStik disrupts less surface area than a standard microfracture technique, reducing damage to the subchondral plate
• No secondary blood or marrow aspiration step required to access Mysenchymal cells
• Produces thin, fragmented, cancellous bone channels without rotational heat generation
• No centrifuge or additional equipment necessary to prepare plasma or aspirate
• No extra time or staff required to prepare the patient or equipment for the case
Microfracture
Pleuri-potential cells Pleuri-potential cells
Figure 4 A,B,C: open trabecular channels; closed trabecular channels, microCT comparison: Axial (top), Sagittal (bottom).
Microfracture Nanofracture K-Wire

7
Shoulder HemiCAP
• 43 anatomically matched implant convexities to treat a variety of shoulder pathologies
• Focal & Total Arthroplasty: AVN, locked dislocators, traumatic lesions, OA, Cuff Tear Arthropathy, Hill-Sachs
• OVO HemiCAP shape matches humeral head geometry with a 4mm offset
• Clinically proven published peer review data
• Strong & solid screw fixation with minimal bone removal
• Maintains soft-tissue envelope and native joint mechanics
• Preserves skeletal anatomy thereby allowing a future total joint replacement
• Minimally invasive / can be performed on an outpatient basis
“As the outcome scores in this study show, restoring the congruity of the humeral head without altering the soft tissue tension, joint volume, joint height,
version or inclination angle allows improved mobility and function.”
Uribe JW, Botto-van Bemden A, UHZ Sports Medicine Institute, Coral Gables, FLJournal of Shoulder and Elbow Surgery 2009: 1-6

9
Patello Femoral Classic HemiCAP
• Multiple inlay trochlea and patella implants provide an off-the-shelf custom fit
• Strong & solid screw fixation with minimal bone removal
• Reproducible instrumentation and precision milling jigs virtually eliminate overstuffing
• For patients that have isolated PF pathology where a TKR would be too invasive
• The anatomic femoral curvatures and inlay patella are designed to restore a natural moving knee by keeping the joint congruent and ligament structures intact
• May be performed on an outpatient basis
“The results of this study suggest that the limited trochlear resurfacing provides a unique and
favorable alternative to prior implant designs by providing anatomic reapproximation of the
patellofemoral surface and knee contact pressures. Although a challenging problem, limited resurfacing
of the trochlea restores peak pressure, contact area, and peak force to the intact state”
M. Provencher, N. Verma et al. Patellofemoral Kinematic After LimitedResurfacing of the Trochlea. 2009. Journal of Knee Surgery

11
Patello Femoral Wave HemiCAP
• Designed to match the complex geometry to the Patello Femoral joint
• Strong & solid screw fixation
• Inlay components preserve the joint by only removing 2-3mm of bone, maintaining future options
• Intraoperative mapping, multiple convexities and trials ensure an anatomic fit
• One tray with simple, reproducible technique and instrumentation
• Maintains existing joint biomechanics thereby allowing normal motion
• May be performed on an outpatient basis
“Patients treated with PFA demonstrated similar results with respect to pain relief, but showed improved function and return to activity when compared with the patients treated with TKA.
Patello-femoral arthroplasty patients also experienced less blood loss, fewer complications, and shorter hospital stay following surgery. Our results indicate that PFA is a less invasive treatment option for patients with isolated PA, yielding early outcomes that compare favorably with TKA.”
Diane L. Dahm, MD. Patellofemoral Arthroplasty Versus Total Knee Arthroplasty in Patients withIsolated Patellofemoral Osteoarthritis. The American Journal of Orthopedics, October 2010
13
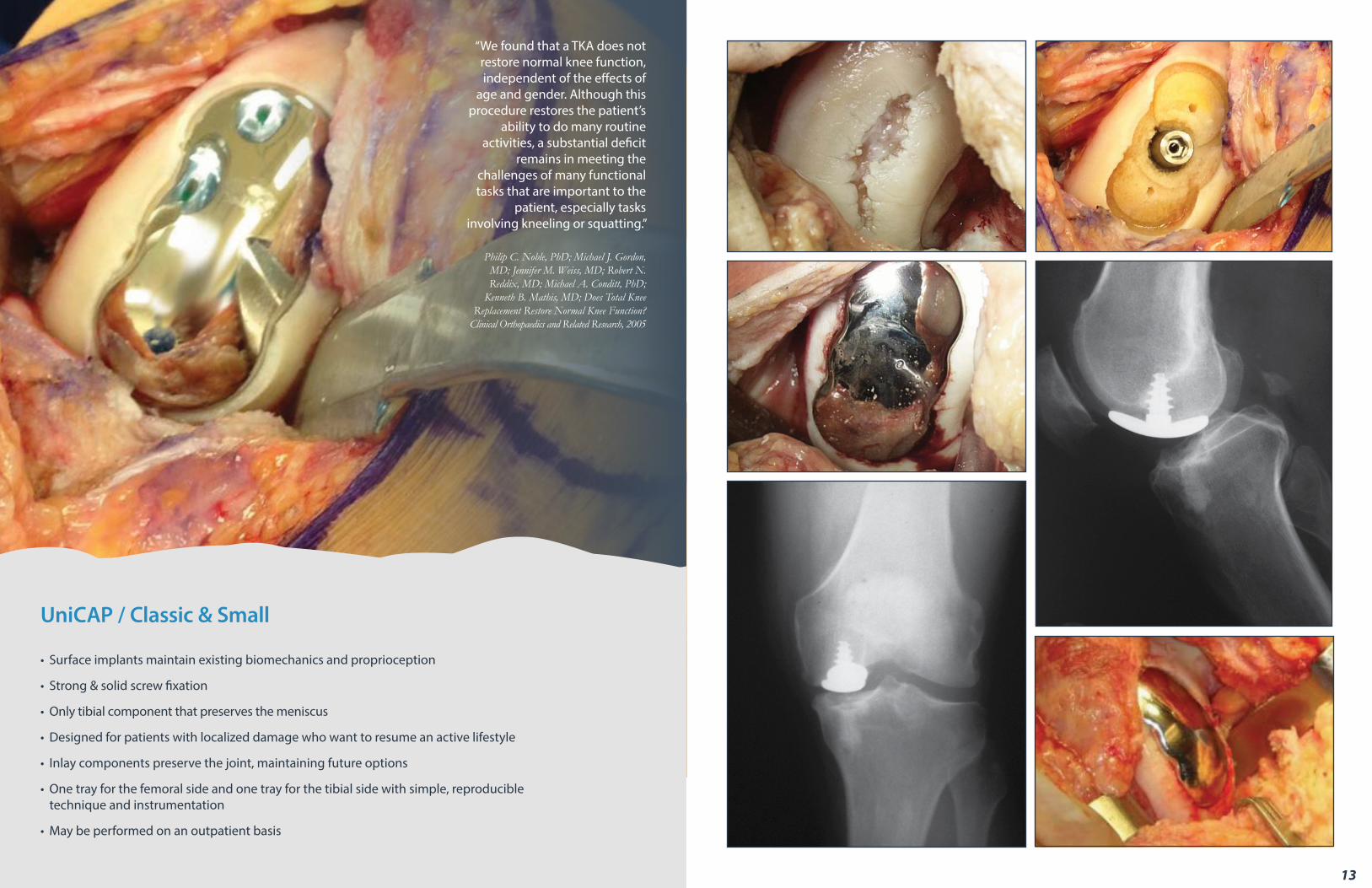
UniCAP / Classic & Small
• Surface implants maintain existing biomechanics and proprioception
• Strong & solid screw fixation
• Only tibial component that preserves the meniscus
• Designed for patients with localized damage who want to resume an active lifestyle
• Inlay components preserve the joint, maintaining future options
• One tray for the femoral side and one tray for the tibial side with simple, reproducible technique and instrumentation
• May be performed on an outpatient basis
“We found that a TKA does not restore normal knee function, independent of the effects of
age and gender. Although this procedure restores the patient’s
ability to do many routine activities, a substantial deficit
remains in meeting the challenges of many functional tasks that are important to the
patient, especially tasks involving kneeling or squatting.”
Philip C. Noble, PhD; Michael J. Gordon, MD; Jennifer M. Weiss, MD; Robert N. Reddix, MD; Michael A. Conditt, PhD;
Kenneth B. Mathis, MD; Does Total Knee Replacement Restore Normal Knee Function?
Clinical Orthopaedics and Related Research, 2005

15
Femoral Condyle HemiCAP
• Restoration of a smooth, continuous load-bearing surface to slow and/or stop further mechanical wear and deterioration of the surrounding joint surfaces
• Strong & solid screw fixation
• A simple, reproducible and less invasive outpatient/ambulatory surgical procedure
• Designed for patients with localized damage who want to resume an active lifestyle
• Inlay components preserve the joint, maintaining future options: “no bridges burned”
• Maintains existing joint biomechanics thereby allowing normal motion
• May be performed on an outpatient basis
Focal femoral condyle resurfacing demonstrated excellent results for pain and function in middle-aged, well selected patients with full thickness cartilage and osteochondral defects. Patient profiling and assessment of confounding factors, in particular mechanical joint alignment; meniscal function; and healthy opposing cartilage surfaces, are important for an individual treatment approach and successful outcomes.
Bollars P, Bosquet M, Vandekerckhove B, Hardeman F, Bellemans J. Knee Surg Sports Traumatol Arthros, 2011, Nov. 11.

17
Toe DF HemiCAP
• Screw based fixation provides an implant construct with proven fixation history
• DF dual implant curvatures improve dorsal role-off and osteophyte regrowth
• Minimal bone removal maintains future options - “No Bridges Burned”
• Proven clinical history with over 20,000 MTP implants
• Bridges the gap between biological therapies and joint fusion
• Maintains existing joint biomechanics thereby allowing normal motion
• May be performed on an outpatient basis
RESULTSPROVEN
The HemiCAPDF has rock solid fixation, a uniquemetatarsal based design and a proven clinical history
with over 20,000 MTP implants. 90°

19
Toe Classic HemiCAP
• Specifically designed for the lesser metatarsals
• Proven screw fixation provides a stable implant
• Minimal bone removal maintains future options - “No Bridges Burned”
• Anatomic “inlay” maintains the length of the 2nd metatarsal
• Resurfacing the metatarsal head with a HemiCAP provides a smooth articulating surface
• Conical shape of the taper post optimizes bone-screw interface
• May be performed on an outpatient basis
“Radiographic evaluation of the HemiCAP prosthesis in 56 patients demonstrated no significant evidence of loosening; it appeared to show superior radiographic results compared to those of other metallic implants using a stemmed design.”
San Giovanni TP. Arthrosurface HemiCAP Resurfacing. Chapter 21. Operative Techniques in Orthopaedic Surgery, 2010

21
Talus HemiCAP
• One implant for 3 surfaces: dome, ridge and medial wall
• Strong & solid screw fixation
• Inlay components restore congruency & maintain existing biomechanics
• Designed for patients with localized damage who want to resume an active lifestyle
• Implant protects subchondral bone and shares load with surrounding tissue
• Minimal bone & tissue removal maintains future options – “No Bridges Burned”
• May be performed on an outpatient basis
“In conclusion, focal resurfacing with a metallic implant appears to hold promise as a means to restore more quasiphysio-logic contact mechanics in ankles with
a large talar osteochondral defect, appreciably reducing biomechanical
aberrations presumed to be responsible for whole-joint cartilage
degeneration.”
Donald D. Anderson, PhD, Yuki Tochigi, MD, PhD, M. James Rudert, PhD, Tanawat Vaseenon, MD, Thomas D. Brown, PhD, and Annunziato Amendola, MD Effect of Implantation Accuracy on Ankle Contact Mechanics with a
Metallic Focal Resurfacing Implant. JBJS. 2010;92:1490-500

23
Hip HemiCAP
• Proven peer reviewed published data
• 6 anatomically matched femoral implant convexities
• Minimal bone removal maintains future options - “No Bridges Burned”
• Focal femoral head resurfacing for traumatic lesions and osteonecrosis
• Inlay placement and proven congruency of the femoral head may avoid premature wear of the acetabulum especially in younger patients
• Minimally invasive procedure can be performed through an anterior approach
“Approximately 5%-18% of all hip arthroplasties are completed on
patients with a primary diagnosis of osteonecrosis. Patients are generally
younger adults age 35 years to 45 years, and risk factors for 75%-90% of cases
include chronic steroid use, alcoholism, smoking, hip trauma including femoral neck fractures and hip dislocations, and
prior hip surgery.”
Anjan P Kaushik, Anusuya Das and Quanjun Cui.World J Orthop. 2012 May 18; 3(5): 49-57.

25
CheckMATE / MTP Arthrodesis System
• Custom low profile elevator to gain exposure of metatarsal head and phalangeal base. Built in templates for sizing purposes
• Interfragmentary Screw Guide eliminates the need for fluoro guidance and eyeballing
• Tack pins eliminate drilling, stabilize the plate and create pilot holes for the screws
• Color coded nubbins for locking and non-locking screws built into the plate are provided pre-assembled and sterile
• Depth gauge is built into the Interfragmentary Screw Guide
• Compression clamp technology built into the plate allows up to 2mm compression across the MTP joint
A low profile, anatomically pre-contoured, super strong anodized plate that combines locking and non-locking screws with an interfragmentary guidance
system to provide maximum stability and a rapid installation.

1. Jäger M, Begg MJ, Krauspe R. Partial hemi-resurfacing of the hip joint--a new approach to treat local osteochondral defects? Biomed Tech (Berl). 2006;51(5-6):371-6. Review.2. Van Stralen RA, Haverkamp D, Van Bergen CJ, Eijer H. Partial resurfacing with varus osteotomy for an osteochondral defect of the femoral head. Hip Int. 2009 Jan-Mar;19(1):67-70.3. Mahmud T, Naudie DD. Partial hip reaurfacing for an osteochondral defect of the humeral head. JBS Case Connector 2012: 2(2):1-6.4. Kirker-Head CA, Van Sickle DC, Ek SW, McCool JC. Safety of, and biological and functional response to, a novel metallic implant for the management of focal full-thickness cartilage defects: Preliminary assessment in an animal model out to 1 year. J Orthop Res. 2006 May;24(5):1095-108.5. Becher C, Huber R, Thermann H, Paessler HH, Skrbensky G. Effects of a contoured articular prosthetic device on tibiofemoral peak contact pressure: a biomechanical study. Knee Surg Sports Traumatol Arthrosc. 2008 Jan;16(1):56-63.6. Becher C, Huber R, Thermann H, Tibesku CO, von Skrbensky G. Tibiofemoral contact mechanics with a femoral resurfacing prosthesis and a non-functional meniscus. Clin Biomech (Bristol, Avon). 2009 Jun 25.7. Becher C, Huber R, Thermann H, Ezechieli L, Ostermeier S, Wellmann M, von Skrbensky G. Effects of a surface matching articular resurfacing device on tibiofemoral contact pressure: results from continuous dynamic flexion-extension cycles. Arch Orthop Trauma Surg. 2011 Mar;131(3):413-9.8. Becher C, Kalbe C, Thermann H, Paessler HH, Laprell H, Kaiser T, Fechner A, Bartsch S, Windhagen H, Ostermeier S. Minimum 5-year results of focal articular prosthetic resurfacing for the treatment of full-thickness articular cartilage defects in the knee. Arch Orthop Trauma Surg. 2011 Aug;131(8):1135-43.9. Bollars P, Bosquet M, Vandekerckhove B, Hardeman F, Bellemans J. Prosthetic inlay resurfacing for the treatment of focal, full thickness cartilage defects of the femoral condyle: a bridge between biologics and conventional arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2011 Nov 11.10. Cannon A, Stolley M, Wolf B, Amendola A. Patellofemoral resurfacing arthroplasty: literature review and description of a novel technique. Iowa Orthop J. 2008;28:42-8. Review.11. Davidson PA, Rivenburgh D. Focal anatomic patellofemoral inlay resurfacing: theoretic basis, surgical technique, and case reports. Orthop Clin North Am. 2008 Jul;39(3):337-46, vi.12. Provencher M, Ghodadra N, Verma N, Cole BJ, Zaire S, Shewman E, Bach B. Patellofemoral Kinematics After Limited Resurfacing of the Trochlea. J Knee Surg. 2009;22:310-31613. Scalise J, Miniaci A, Iannotti JP. Resurfacing Arthroplasty of the Humerus: Indications, Surgical Technique, and Clinical Results. Techniques in Shoulder and Elbow Surgery 8(3):152–160, 200714. Dawson CK, Rolf RH, Holovacs T. Management of localized humeral head defects in the athlete. Oper Tech Sports Med 2008 16:14-20.
15. Scalise J, Miniaci A, Iannotti JP. Resurfacing Arthroplasty of the Humerus: Indications, Surgical Technique, and Clinical Results. Current Orthopaedic Practice 19(4): 443-450,200816. Uribe JW, Botto-van Bemden A. Partial humeral head resurfacing for osteonecrosis. J Shoulder Elbow Surg. 2009 Sep-Oct;18(5):711-6. Epub 2009 Jan 30.17. Moros C, Ahmad CS. Partial humeral head resurfacing and Latarjet coracoid transfer for treatment of recurrent anterior glenohumeral instability. Orthopedics. 2009 Aug;32(8).18. Grondin P, Leith J. Case series: Combined large Hill-Sachs and bony Bankart lesions treated by Latarjet and partial humeral head resurfacing: a report of 2 cases. Can J Surg. 2009 Jun;52(3):249-54.19. Anakwenze OA, Hosalkar H, Huffman GR. Case reports: two cases of glenohumeral chondrolysis after intraarticular pain pumps. Clin Orthop Relat Res. 2010 Sep;468(9):2545-9. Epub 2010 Jan 29.20. Eleftheriou K, Al-Hadithy N, Joshi V, Rossouw D. Use of a partial humeral head resurfacing system for management of an osseous mechanical block to glenohumeral joint range of movement secondary to proximal humeral fracture malunion. Int J Shoulder Surg 2011;5:17-2021. Adalberto Visco, Luis Alfredo Gómez Vieira, Felipe Borges Gonçalves, Luis Filipe Daneu Fernandes, Murilo Cunha Rafael dos Santos, Nivaldo Souza Cardozo Filho, Nicolas Gerardo Gómez Cordero. Surface arthroplasty for treating primary and/or secondary shoulder osteoarthrosis by means of the HemiCAP-Arthrosurface® system. Rev Bras Ortop. 2011;46(3):288-9222. Lenarz C, Shishani Y, Gobezie R. Surface Replacement: The Hemicap Solution. Semin Arthro, 2011,22:10-1323. Hammond G, Tibone JE, McGarry MH, Jun BJ, Lee TQ. Biomechanical comparison of anatomic humeral head resurfacing and hemiarthroplasty in functional glenohumeral positions. J Bone Joint Surg Am. 2012 Jan 4;94(1):68-76.24. Seitz WH, Miniaci A. vascular necrosis of the humeral head: Hemi-Cap, cap or stemmed solution? Semin Arthoplasty 23(2):60-67,201225. Anderson D, Tochigi Y, Rudert J, Vaseenon T, Bron T, Amendola A. Effect of Implantation Accuracy on Ankle Contact Mechanics with a Metallic Focal Resurfacing Implant. JBJS Am, 2010 June, 1490-150026. van Bergen CJ, Zengerink M, Blankevoort L, van Sterkenburg MN, van Oldenrijk J, van Dijk CN. Novel metallic implantation technique for osteochondral defects of the medial talar dome. Acta Orthop. 2010 Aug;81(4):495-502.27. Ooij B, Kaas L, Reilingh ML, van Dijk CM. Osteochondral defects of the talus: surgical treatment and rehabilitation. Archivio di Ortopedia e Reumatologia. 2010, Volume 121, Number 4, Pages 17-1828. van Bergen CJ, Reilingh ML, van Dijk CN. Tertiary osteochondral defect of the talus treated by a novel contoured metal implant. Knee Surg Sports Traumatol Arthrosc. 2011 Jun;19(6):999-1003.
Selected References
27
29. Reilingh ML, van Bergen CJ, van Dijk CN. Novel Metal Implantation Technique for Osteochondral Defects of the Medial Talar Dome. Techniques in Foot & Ankle Surgery: March 2012 - Volume 11 - Issue 1 - p 45–4930. van Bergen CJAA, Reiling ML, van Dijk CN. Novel metal implantatio technique for secondary osteochondral defects of the medil talar dome- one year resuts of a prospective study. Fuß & Sprunggelenk 10 (2012) 130-13731. Burks JB. Implant arthroplasty of the first metatarsalphalangeal joint. Clin Podiatr Med Surg. 2006 Oct;23(4):725-31, vi.32. Hasselman C, Shields N. Resurfacing of the First Metatarsal Head in the Treatment of Hallux Rigidus. Techniques in Foot & Ankle Surgery 7(1):31–40, 200833. Carpenter B, Smith J, Motley T, Garrett A. Surgical Treatment of Hallux Rigidus Using a Metatarsal Head Resurfacing Implant: Mid-term Follow-up. J Foot Ankle Surg. 2010 July - August;49(4):321-325.34. Aslan H, C İtak M, Baş EG, Duman E, Aydın E, Ateş Y. Early results of HemiCAP® resurfacing implant. Acta Orthop Traumatol Turc. 2012;45(7):17-21.35. Kline AJ, Hasselman CT. Metatarsal Head Resurfacing for Advanced Hallux Rigidus. Foot Ankle Int. 2013 Feb 13.36. Benthien JP, Behrens P. Reviewing subchondral cartilage surgery: considerations for standardised and outcome predictable cartilage remodelling : A technical note. Int Orthop. 2013 Nov;37(11):2139-45.
37. McNickle AG, L’Heureux DR, Provencher MT, Romeo AA, Cole BJ. Postsurgical glenohumeral arthritis in young adults. Am J Sports Med. 2009 Sep;37(9):1784-9138. Bushnell BD, Creighton RA, Herring MM. The bony apprehension test for instability of the shouder: a prospective pilot analysis. Arthrscopy 2008, 24(9): 974-982.39. Elser F, Braun S, Dewing CB, Millett PJ. Glenohumeral joint preservation: current options for managing articular cartilage lesions in young, active patients. Arthroscopy. 2010 May;26(5):685-96. Review. 40. Paul J, Buchmann S, Beitzel K, Solovyova O, Imhoff AB. Posterior shoulder dislocation: systematic review and treatment algorithm. Arthroscopy. 2011 Nov;27(11): 1562-72. Epub 2011 Sep 1.41. Brennan SA, Devitt BM, O’Neill CJ, Nicholson P. Focal femoral condyle resurfacing. Bone Joint J. 2013 Mar;95-B(3):301-4.42. Provencher MT, Barker JU, Strauss EJ, Frank RM, Romeo AA, Matsen Iii FA, Cole BJ. Glenohumeral arthritis in the young adult. Instr Course Lect. 2011;60:137-53.43. Burgess DL, McGrath MS, Bonutti PM, Marker DR, Delanois RE, Mont MA. Shoulder resurfacing. J Bone Joint Surg Am. 2009 May;91(5):1228-38.44. Gomoll AH, Madry H, Knutsen G, van Dijk N, Seil R, Brittberg M, Kon E. The subchondral bone in articular cartilage repair: current problems in the surgical man agement. Knee Surg Sports Traumatol Arthrosc. 2010 Apr;18(4):434-47. Epub 2010 Feb 4. Review.
Cumulative Number of Published & Documented References
2005
4
2006 2007 2008 2009 2010 2011 2012 2013
1420
36
57
86
112
141151
20
40
60
80
100
120
140
160

28 Forge Parkway • Franklin, MA 020381 508 520 3003
fax: 1 508 528 4604
For more information, visit our website:www.arthrosurface.com
This pamphlet and information is intended for markets where regulatory approval has been granted.
PN 0025-1006 REV A
These products are covered by one or more of U.S. Patent Nos. 6,520,964; 6,610,067; 6,679,917; 7,163,541; 7,029,479 and other patents pending.NanoFx®, HemiCAP®, UniCAP®, CheckMATE®, Pinit are trademarks of Arthrosurface, Inc. U.S. © 2013
Arthrosurface, Inc. All rights reserved. Printed in U.S.A.
Individual results may vary and not all patients will return to the same activity level.For additional product information, including indications, contraindications, warnings, precautions
and potential adverse effects, please visit www.arthrosurface.com


















