Process Safety Webinar Series - Part 4
12
Critical Success Factors for Effective Incident Investigation Neil Franklin AECI: Group SHE Manager Process Safety Webinar Series - Part 4 30 September 2021
Transcript of Process Safety Webinar Series - Part 4

Critical Success Factors for Effective
Incident Investigation
Neil Franklin
AECI: Group SHE Manager
Process Safety Webinar Series - Part 4
30 September 2021

2
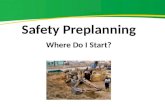
Most common causes of process safety incidents
The Italian Association
of Chemical Engineering
Online at www.aidic.it/cet
In this paper, the contributions of PSM
element to chemical process accident
are studied using major process failures
in the chemical process industry (CPI).
Around 770 major accident cases were
collected and analysed
https://www.aidic.it/cet/17/56/166.pdf
2017
0
3
2
6
11
12
19
17
9
9
6
3
2
0
0 2 4 6 8 10 12 14 16 18 20
Compliance Audits
Emergency PlannIng and Response
Contractors
Hot Work Permit
Training
Employee Participation
Process Hazard Analysis
Operatng Procedures
Mechanical Integrity
MOC
Process Safety Information
Incident investigation
PSSR
Trade Secret
Percentage contribution of PSM Element to 770 incidents
Percentage

3
On this day in history
https://processsafetyintegrity.com/incidents/

4
Recent events in South Africa

5
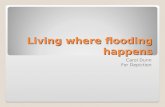
Critical Success Factors
ROLES &
RESPONSIBILITY
2
FIELD
INVESTIGATION
3
ROOT CAUSE
ANALYSIS
4
LEARNING
5
Appointing the
investigation team
Create a detailed
understand of exactly
what happened.
Create a detailed
understand of exactly
why it happened
Ensure the incident
does not repeat
HAVE A DEFINED
PROCESS
1
Define the
expectations and
outcomes

6
Have a defined process, and stick to it.

7
Field Investigation
◇Secure the scene and evidence quickly
◇Make a checklist – assign responsibilities
◇Evidence collection must start immediately BUT
take as long as needed and with repeated views of
the evidence and scene
◇ Look for multiple data sources to confirm a fact in
the sequence of events
◇Appoint one person to collate the evidence
◇Time stamps on photos are critical
Typical evidence collected:
• Interviews
• Photographs, CCTV and any other video
footage
• Process trends
• P&ID’s, MFD’s, Plot plans
• PHA’s, MOC, PSI, Maintenance reports
• Alarm printouts / Logics (Scada/DCS)
• Logbooks, Permit to work, risk assessments
etc.
• Procedures and work instructions
Organisational information
• Structure / vacancies• Training• Overtime

8
Interviews

9
Have agreed techniques – fit for purpose
Incident
description
Direct
cause
Direct
cause
Underlying
cause
Underlying
causeUnderlying
cause
Underlying
cause
Root causeRoot causeRoot causeRoot cause
Why 1
Why 2A
Why 2B
Why 3A
Why 3B
Why 3C
Why 4A
Why 4B
Why 4C
Why 4D
Why 4E
Why 4F
None of these will:
1. Do the field investigation for you;
2. Interview witnesses for you;
3. Select root causes for you;
4. Develop corrective action for you.

10
Identifying the root causes and systemic weaknesses
Preventing repeats can only be done by correcting the absent or failed controls.
Review:
• PHA / Risk Assessments• Maintenance philosophy and
compliance• Procedural accuracy and compliance• Status of drawings and other PSI• Emergency Plan• Audit results
Organisational Factors
• Competency of staff• Correct leading and lagging indicators
being used• Correct performance management• Corrective action effectiveness• Institutionalising of learning

11
Institutionalizing the learning
• Produce a decent report
• Share the learning in the right levels of detail to the right audience
• Hold people accountable to complete actions as part of the learning process
• Audit the implementation of actions
• Don’t rely on memories – engineer the improvements / changes
• Fix the System errors (PHA, Procedures, Training etc.) and audit this
• Conduct incident recall

Thank youAny questions?
12