Process optimization inProcess optimization in · PDF fileProcess optimization inProcess...
34
Process optimization in Process optimization in Process optimization in hospitals Process optimization in hospitals Ger Koole VU University Amsterdam VU University Amsterdam Eindhoven 25 June 2010 Eindhoven, 25 June 2010
Transcript of Process optimization inProcess optimization in · PDF fileProcess optimization inProcess...

Process optimization inProcess optimization inProcess optimization in hospitals
Process optimization in hospitalspp
Ger KooleVU University AmsterdamVU University Amsterdam
Eindhoven 25 June 2010Eindhoven, 25 June 2010

Personal experiencePersonal experience
Ad i i VU di l t (0 25 ft )Advisor in VU medical center (0.25 fte)– rapid diagnosis (Sonja Z, Berthe v G)– sojourn times emergencies (Annemieke v D)
TrainingsTrainings – LogiZ
eHealth– eHealthResearch– appointment scheduling (Guido K & Paulien O)– bed assignments (Arnoud de B & René B)

Logistics and health careLogistics and health care
“Classical” logistics: drugs, supplies, bed linnen, …,Patient logistics: primary care process
S i ti t i t f th– Service: patient is part of the process– General consensus: health care system is
where manufacturing was in the 70s– Much to win!
Cure ahead of care

Current trend: leanCurrent trend: lean
Focus on what adds valueRemove sources of waste: inventoryRemove sources of waste: inventory, batch processing, transportation, …E i H lthEmerging: eHealth

Diversity in health careDiversity in health care
D t ti t i iDoctors: every patient is unique ad hoc solutionsHowever:– Homogeneous groupsg g p– Heterogeneous restPopular before lean: focused factoriesPopular before lean: focused factories – For homogeneous groups
F l t t b t– For example: cataract, breast cancer– How about the rest?

RandomnessRandomness
Treatments times, patient pathExternal/unavoidable vsExternal/unavoidable vs. Internal/avoidable
E i di t P i– Emergencies according to Poisson process; planned surgery equally variable!
– Operations running late: due to complications but also morning traffic (and are all complications really unavoidable?)

Operations managementOperations management
What needs to change urgently: – daily management of health processy g p– patient orientation
long term implementation of changes– long-term implementation of changes (“borging”)
Less urgent:– advanced planning systemsp g y

Case 1: Clinical wardCase 1: Clinical ward
Arrivals AdmissionsLength of stay (LOS)Number of operational bedsNumber of operational beds
erformance:Bed occupancy refused admissions

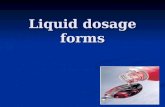
Data analysis yAdmissions per day
Daginstroom VVAT jan - mrt 200678
Acuut Electief
4567 Acuut Electief
23
0
1-ja
n
6-ja
n
11-ja
n
16-ja
n
21-ja
n
26-ja
n
31-ja
n
5-fe
b
10-fe
b
15-fe
b
20-fe
b
25-fe
b
2-m
rt
7-m
rt
12-m
rt
17-m
rt
22-m
rt
27-m
rt
Datum

Data analysisyLOS: hyperexponential distribution
800
900
1000
al li
gduu
r
500
600
700
ot d
at a
anta
gen
200
300
400
500
patië
nten
to da
waargenomen
0
100
200
0 3 7 0 3 7 0 3 7 0 3 7 0 3 7 0 3 7 0
Aan
tal p
g
hyperexponentieel
0
0.83
1.67
2.50
3.33
4.17
5.00
5.83
6.67
7.50
8.33
9.17
10.0
0
10.8
3
11.6
7
12.5
0
13.3
3
14.1
7
15.0
0
Ligduur in dagen VVAT 2006

ModelsModels
Questions:– how to assign beds to specialties?g p– how many beds to take
= how to distribute beds between specialties?= how to distribute beds between specialties?Models required to evaluate changes– simplest model: Erlang B– validated at VUmcvalidated at VUmc

How to assign beds?How to assign beds?
conomies of scale B(s sa) decreasing in s = ec of scaleB(s,sa) decreasing in s ec. of scaleProof: Smith & Whitt 81, analytical
ti f B( )properties of B(.,.)B(s,sa) convex? (s,sa) co eDiminishing returnsNo proof, numerical evidence

MergingMergingTheorem:Theorem:
Compares occupationProof by coupling Smith & Whitt 81Proof by coupling, Smith & Whitt 81Thus: merging wards leads to higher occupancyMerge all wards in case fixed revenue perMerge all wards in case fixed revenue per night

Equal ALOSEqual ALOS
Thus merging minimizes overall blockingThus merging minimizes overall blocking rate in case equal ALOSAlso if ALOS unequal?And how about rates per ward?And how about rates per ward?

Unequal ALOSUnequal ALOS
Merged ward has higher blocking probMerged ward has higher blocking prob.Unrealistic numbers

Per ward equal ALOSPer ward, equal ALOS
ICU a s B(s,a) Weighted av.
1 20 20 0.160 130.13
2 8 12 0.05merged 28 32 0 07merged 28 32 0.07
Overall blocking % But blocking % type 2
increasesdecreases
increases

Ward schedulingWard scheduling
How to take advantage of scale…while satisfying rejection constraints?while satisfying rejection constraints?
Answer: dynamic bed assignment

Dynamic policiesDynamic policies
Equal ALOS– DP formulation– Optimality of threshold policies
U l ALOSUnequal ALOS– DP formulation– curse of dimensionality

Bed reservationsBed reservations
“ear marking”single and multi-skilled nursessingle and multi skilled nurses

Case 2: planning of sharedCase 2: planning of shared resources
Queueing at bottleneck resourcesQueueing at bottleneck resourcesQueueing = slot in schedule at later timeDifferent types of patients– different specialties/treatmentsp– urgency
First single t pe q e eFirst: single-type queue

Waiting listsWaiting lists
How to reduce length of waiting lists?Queueing model: Erlang C or M|G|cQueueing model: Erlang C or M|G|c seems logical

Best practiceBest practice
ihi.org: Advanced accessCBO: Werken zonder wachtlijstCBO: Werken zonder wachtlijstUse “lean”: improve process to decrease
i ti d i l t d kservice times and arrival rate and make system stableWork away backlogAfter that no more q e esAfter that: no more queues
“do today’s work today”

PracticePractice
Queues grow again!ReasonsReasons– short queues attract more patients
l k ti t l h– long queues make patients go elsewhereCould have known– queue lengths were stable
contradicts standard queueing models– contradicts standard queueing models

PracticePractice
Avoid more patients to enterRestrict patient poolRestrict patient pool“panel size”not always possible
een, Savin, & Murray, Providing Timely Access to Care: What is the Right Patient Panel Size? Jt Comm J QualWhat is the Right Patient Panel Size?, Jt Comm J Qual Patient Safety, 2007

Shared resourcesShared resources
Resources used by multiple types of patientspUsually further in the chainL ibl t h i tiLess sensible to changes in access timeTypical example: yp ca e a p e– CT or MRI scan

Types of patientsTypes of patients
Not urgent: waiting time order of weeksEmergency: directly/same hourEmergency: directly/same hour– E.g., trauma patient
Urgent: same or next day– E.g., clinical patientg , p
Scheduling methodology: walk-in or slotslk i ibl f h t i ti– walk-in possible for short service times

SlotsSlotsurrent practice:pEvery specialty has its own slots or block of slotsof slotsEmpty slots are filled in few days in advanceadvancesadvantages:Time left beginning or end of blocksNo match demand and supplyNo match demand and supplyOften empty slots

Solution methodSolution method
alk-ins for urgent are feasible?Yes: create walk-in blocks part of the dayYes: create walk in blocks part of the day (on part of the scanners)N l t f t ti tNo: reserve slots for urgent patientsModel for slotsode o s otsCrucial: Can empty slots still be filled?

Modeling slotsModeling slotsUsual approximation: number of urgentUsual approximation: number of urgent patients per day is Poisson distributedWhen empty slots can still be filled: – take “enough” slotsg
When empty slots cannot be filled:i k f i d l t– risk of unoccupied slots
– solution: merge slots of specialties– economies of scale

More advanced slot reservation systems
xample Slots can be given away day beforeSlots can be given away day beforeSlots for same day or day afterReserve uk slots day of the week kWhen more than v slots for day k at endWhen more than vk slots for day k at end k-1: give away until vk
Markov chain model

Case 3: sojourn times at EDCase 3: sojourn times at ED
“mess”: not clear where to startdata analysis on manually collected datadata analysis on manually collected data

4-hour objective4 hour objectiveareful with steering on h-hour norm
: Seddon, Systems thinking in e public sectorp
n an attempt to meet he target four-hour g&E waiting time, atients were ometimes "dumped" in ward without nursing
are”are es Online

Data analysis at EDData analysis at ED
Preliminary conclusions:Preliminary conclusions:– radiology is not to blame– no mgmt related to sojourn times
corresponds to literature

ConclusionConclusion
Health care interesting area for OR/OMDoctors are really interested in OM notDoctors are really interested in OM, not just in outcomesC lt l hCultural changes necessaryHealth care needs to change (budget cuts)ea t ca e eeds to c a ge (budget cuts)