
Process Mapping - YorOK Website Eii - Annex A... · 1 CITY OF YORK COUNCIL Process Mapping A...
17
1 CITY OF YORK COUNCIL Process Mapping A systems mapping exercise for prevention and early intervention March 2016
-
Upload
trinhkhuong -
Category
Documents
-
view
214 -
download
0
Transcript of Process Mapping - YorOK Website Eii - Annex A... · 1 CITY OF YORK COUNCIL Process Mapping A...

1
CITY OF YORK COUNCIL
Process Mapping A systems mapping exercise for prevention and
early intervention
March 2016

2
1. INTRODUCTION AND EXECUTIVE SUMMARY
The City of York Council is looking to remodel the way in which prevention and early intervention services
operate within the city. A series of process mapping exercises were undertaken with several services from
across the city; this ranged from early years, schools and community and adult services, from voluntary to
statutory focused services. The objective was to establish some learning around the common systems and
practices of a variety of services looking to improve outcomes for children and families at an early intervention
level. The report provides some highlighted findings from the work undertaken and provides
recommendations for developing multi -agency approaches to the new operating model for prevention and
early interventions services in the City.
The review takes on both a case example and systems approach to how families and services interact with the
prevention route map. The collation of findings can be found in diagrammatical form within the report; the
methodology and findings from the exercises can be found in Annex A.
The findings have highlighted two main schools of thought which are reflected throughout the detail below.
The first is related to actual systems and process from which a new operating model for prevention and early
intervention services can learn to build a tangible new process system across city partners.
The second shows how the work has highlighted other key issues which will impact on the success of
developing a new route map for this area of work. Particular messages are related to culture and practice
behaviour, workforce and organisational development , as well as some considerations for strategic
approaches to deploying and commissioning resources to improve outcomes for families in need.
2. RECOMMENDATIONS FOR NEXT STEPS
In order to progress the model further, the following step are recommended:
a) Consolidate the learning from the process mapping with other key learning in shaping the new
operating model, i .e. other engagement feedback, research and other Local Authority area models
b) Identify task and finish groups at various system levels to support the shaping of the operating model
and which accommodate the key elements from the exercise. Decisions will need to be made on :
which actions should be achievable as part of the initial design stages, before the structure is
in place and,
what will remain for the partners and staffing arrangement of the new structure to develop
as part of the operational effectiveness of the model.
3. PROCESS MAP FINDINGS
The visual representation below gives a higher level view of the findings from the exercises and a b road
identification of where partners need to focus to ensure that a more streamlined approach to a new early intervention model.

3
What we found from the mapping.
The ways we behave. What we focus on.
The stages of process from identification, assessment, intervention and exit Patterns and themes identified as
gaps in our approaches Process Map Key:
FAMILY ‘IN’ ASSESSMENT INTERVENTION
OUTCOMES
AND EXIT
START AGAIN?
OUT
Self referred
Because they have to... Data tracking
Single Assessment
Own Agency Tool FEHA
Whole Family
V Individual Need
Domestic Abuse
Parental SMU Mental health and health
‘Toxic Trio’
Show short and long term
changes. What’s really different?
Plan exit from the start
Thresholds –
how can we be
more flexible?
Need to better
manage drift
and anxiety
Needs
coordinated
workforce
development,
commissioning
and resource
Need creative
flexible
solutions
including use
of carrot and
stick
Sequenc e
interventions
and
understand
each agency
outcome
Review of
common
assessments
required reduce
amount and size Timescales –
reduce, be
flexible. Challenge criteria,
extended hours?
Better data
set access
and
proactive
use and
targeting
Engagement and
Compliance Consent difficulties?
No clear evidence of
tangible, measurable
outcomes
The long term
strategy for
complex
families?

4
4. SYSTEMS AND PROCESS FINDINGS
It is worth distilling the messages from the key points raised by the findings into 3 levels of systems behaviour.
Strategic response – Reflections upon organisational development and behaviour were important in
understanding how leadership throughout partners in the city can support a new way of working. There were
strong messages from all agencies represented that there is an appetite for cultural change and ability to do
things differently, but a sense of watching and waiting for permissions to do this outside of traditional
methods of services delivery. Consideration will be required by agencies external to City of York Council as to
how flexible their resource and decision-making capacity can be to support a more fluid approach to working
with families in a local way.
A particular point of interest is the potential need to join commissioning and strategic thinking around some of
the key issues families are facing; this was particularly evident in issue around the ‘toxic trio’ and a sense of
need to understand the prevalence of the issues for both children’s and adults services and how they respond
in a holistic way. Currently, services have limited interaction across the age ranges to assist better whole family
working.
Within these two messages are a sense of practitioners needing to feel equipped to deal with the issues
families raise and to be able to flex their skills and resources in an informed and permissive way. A focus is
required on what the workforce development strategy and core offer for practitioners across children and
family services will be.
Operational response – The findings support that a different approach to traditional methods of working are
no longer felt to respond to the needs of families, particularly those with more complex and potentially longer -
term need for varying levels of support. Varying degrees of interaction with families are required throughout
the dynamics and life course of the family and some of the ways in which practitioners have identified this
needs to be achieved are reflected in Annex A. This gives some clear foundations which can be built into the
model. Particular focus will need to be in creating flexibilities in multi -agency response to families at threshold
and criteria eligibility levels across children’s , adult and community centred services. There needs to be a
better offer around information sharing, problem solving and less conventional ways of managing resources
which allows for a more pro-active approach to working as well as responding to themes and issues raised
around risk and vulnerability (i.e. CSE, DV) .
Practice response – Practitioners need to have a wider understanding of a family’s journey through an
outcomes approach with partners wherein a shared outcomes framework is developed across children’s,
adults and communities which allows the flexible operational response i dentified above.
As identified within the strategic response, practitioners should expect to develop a skil ls and experience base
which aligns with the needs reflected in local areas and be deployed to tackle issues in whichever identified
way is deemed required. This may be away from the conventional ‘case management’ approach, or thresholds
such as service boundary or criteria such as age; that ‘whole family’ is core business.
KEY ISSUES RAISED
The table below highlights the key points that have been raised through this report and offers some ideas as to
how the new operating model will respond to the findings. As the leadership and management for the new
model is agreed it is expected that these key areas of response are part of the organisational development of
the model.

5
Key points raised How the new model can respond
Not knowing where to go for support or who is
involved
Local Area Teams will provide a significant reduction i n the amount of contact points for services in dealing with
children and families. They will also contain an element of community capacity building giving real -time
information on community and social networks.
Needing flexible, creative, negotiated approaches to
access services quickly and proportionally
At a strategic level , the concept of problem-solving and flexible use of own agency resources needs to be an
agreed and communicated offer.
The Local area Teams will design a multi -agency communication process which will include a process map, family
triage, data intelligence triage from the local demographics, and a system to identify and respond to family or
local area need that is drifting or requires challenge.
Better systematic use of service knowledge and data
systems to identify families and manage progress
Practice processes will start with a more intelligence led approach using data and local knowledge of families to
understand who is in need in the areas, and what level of need they may require. This is intended to be a pro-
active response to identifying families than waiting for them to come to agency attention when issues have
escalated.
The Local Area Team process map will include a route map for intelligence sharing and managing data to identify
and respond to escalating community or behavioural themes (i.e. CSE, DV) as well as individual family concerns.
The size , use and ownership of assessment A review is in progress to align a wide variety of service assessment and planning tools, understand their use and
potential impact and then identify a more flexible range of tools which can support proportionate assessment
practices for a proportionate intervention response. It is envisaged that this work could support a system wide
agreement on what an appropriate assessment, information sharing and planning framework looks like across
partners and thresholds.

6
Key points raised How the new model can respond
Clarifying levels of fair processing and consent to
share information
A privacy impact assessment is being completed as part of the model design. This will include a review of mutli -
agency data and information sharing agreements and practices; this is similalry l inked to the review of
assessment and plannning frameworks and recognition of appropriate tools and formats of communication.
A strategic response to support targeting resources,
workforce development and commissioning towards
the main concern areas identified, particularly the
‘toxic trio’
The model is an opportunity to build an outcomes framework that can deliver strategic messages about the
impact of intervention on the ground. This should inform senior management and commissioning partners to
establish a joined up approach to resourcing and organsiational development.
Having a longer-term strategy for complex families
who come in and out of service support, at whichever
level of intervention.
The Local Area Teams will have an intelligence led approach that should identify the levels of need for families at
any one time. The approach to developing roles as wider than working on a strictly ‘case management’ approach
will mean an ability to flex for family need at any given time. Having an outcomes focussed practice approach
with families as a core offer should also identify with them what they need to maintain levels of independenc e
and what they may need when issues begin to escalate again.
The interface between the Local Area Teams, Children’s and Adults ’ social care is paramount to revising the
current ‘step up/down’ approach from services.
Use of a coordinating approach to help flex and
negotiate about threshold and sanction-related cases
and what they may need.
The model will design processes into the teams which expect managers and staff to use a challenge and support
approach when liaising with families and other agencies to broker what is fully needed for the family or local
area.
The council will look to ensure the workforce development has a core offer element around positive challenge
and outcomes/exit planning with families.

7
Key points raised How the new model can respond
Be more creative with resource and autonomy to
respond differently.
The Local Area Teams will have identified, individual budgets to allow them to respond in the most appropriate
way to meet the needs of families and communities. Management level job specifications will also include an
expectation on creative and flexible decision making. Agreement on similar approaches across other agencies
involved with children and families will need to be discussed at multi -agency senior management level as the
Local Area Team strategy and model of delivery is realised.
Whilst designing flexibility into the model is required, care must be taken to not allow the model to try and be
“all things to all people” through inconsistencies of when to use flexibility and when to not.
Agencies needing to work to common goals and
identify family progress
A shared outcomes framework needs to be agreed at a senior level across services working with children and
families. Similarly, operational level targets and outputs need to reflect the ability to impact on other agency
objectives. Building this in at a strategic intelligence level should support Local Area Teams having a clear
indication of what overarching goals are expected for the service and how they c ompliment other service areas.
A workforce development opportunity is presented to develop the workforce in a way that places outcomes and
strength based practice at the heart of their approaches. This will be a core offer of the model.
Managing engagement and compliance and how the
‘carrot and stick’ approach might be put to better use
to reengage families.
Reviewing and redesigning approaches to assessment and intervention sequencing with families should include
the concepts of outcomes focused objectives and also support prioritising and consequential actions where
objectives are not met. Similarly, there will need to be an ability to recognise achievement within work with
families to measure progress made against small as well as wider outcomes .

8
ANNEX A – PROCESS MAP FINDINGS – DETAILED REPORT
METHODOLOGY
The exercise was undertaken in two main ways:
CASE LEVEL REVIEW:
Case level examples of early intervention work. 55 case examples were received from 17 service areas as
outlined below:
Children’s Advice Team and Children’s Trust
Unit (4)
Youth Offending Team (3)
Personal Support and Inclusion Service –
Community (3)
Health Visiting Service (4)
Child and Adolescent Mental Health Services
(3)
Housing (4)
SEND (3)
Family Focus (3)
Children’s Centres (3)
Police (6)
Schools (3)
SENDI ASS (3)
Early Years (3)
Personal Support and Inclusion Service -
Castlegate (3)
Connexions (3)
Educational Psychologists (3)
Children’s Social Care (1)

9
Engagement with the Police Service in this exercise was facilitated through a group session. All other services
contributed case examples either through small discussions or indivi dual completions of case examples.
Service areas were asked to give three case examples including what they perceived to be low,
medium and complex level cases for early intervention. Set questions were asked but were open text
in order to enable practitioners to explore their cases in a meaningful way.
Data was collated from the cases and aggregated.
Strengths to the approach relate to a demonstrati on of clear patterns around cross -organisational
behaviour, regardless of age range and family dynamic. This enables a confident view of processes to
be achieved.
The limitations relate to a qualitative approach to some of the template questions which redu ced
some of the quantitative information available.
MULTI-AGENCY SYSTEM MAPPIN G:
A multi-agency group undertook two sessions of mapping own agency systems and behaviour in line with the
prevention route for early intervention. (session outlines and summary outcomes at Annex B and C). The
following services attended the sessions:
Housing Options
Youth Homeless Prevention
Housing Registrations
Burton Green Primary School
Adult Mental Health
Health Visiting Service
School Nursing Service
Children’s Social Care Referral and
Assessment
Adult Services Commissioning
Children’s Trust and Advice Team
North Yorkshire Police Neighbourhood
Policing
Child and Adolescent Mental Health Services
Child in Need Service
Estate Management
Neighbourhood Enforcement
Representatives from secondary schools, school mental health pilots and adults safeguarding were invited but
unable to attend.
The first session focused on multi-agency discussion of how each service area interfaced with the prevention
route map. A summary of the main themes was then created. The second session focused on elements within
the themes which the group felt needed to be a key part of multi -agency practices going forward.
Strengths of the approach were related to the multi -agency perspectives that were brought to the exercise. All
representatives of the services were of sufficient practitioner or manager level to be able to talk confidently
about their area of expertise and service. All were open and supportive in their discussion of each other’s
approaches to enable a collective view at the end of the work. Similarly, the case examples reflected various
10
perspectives and supported emerging patterns of strengths and issues that the new operating model can
incorporate.
Some limitations to the approach have been around securing all representation needed for a fully rounded
view of the model, particularly from a secondary school and adult social care pers pective at this stage. The
breadth of the systems that the mapping exercise has attempted to explore is also something which means
focusing purely on a process approach and a detailed view of fundamental processes has been difficult to
achieve in a short timescale. This needs to be seen as an ongoing piece of work which would support the
development of the model as it progresses into operational detail. However, there was a general consensus
amongst those involved that there were clearly identifiable patterns regarding process, workforce behaviour
and development that could be seen from all perspectives.
What is clear however is the two exercises have demonstrated a consistent pattern of strengths and areas for
review across agency processes and from which to develop the model further.
SYSTEM ENTRY POINT – ‘FAMILY IN’
FAMILY PROFILE
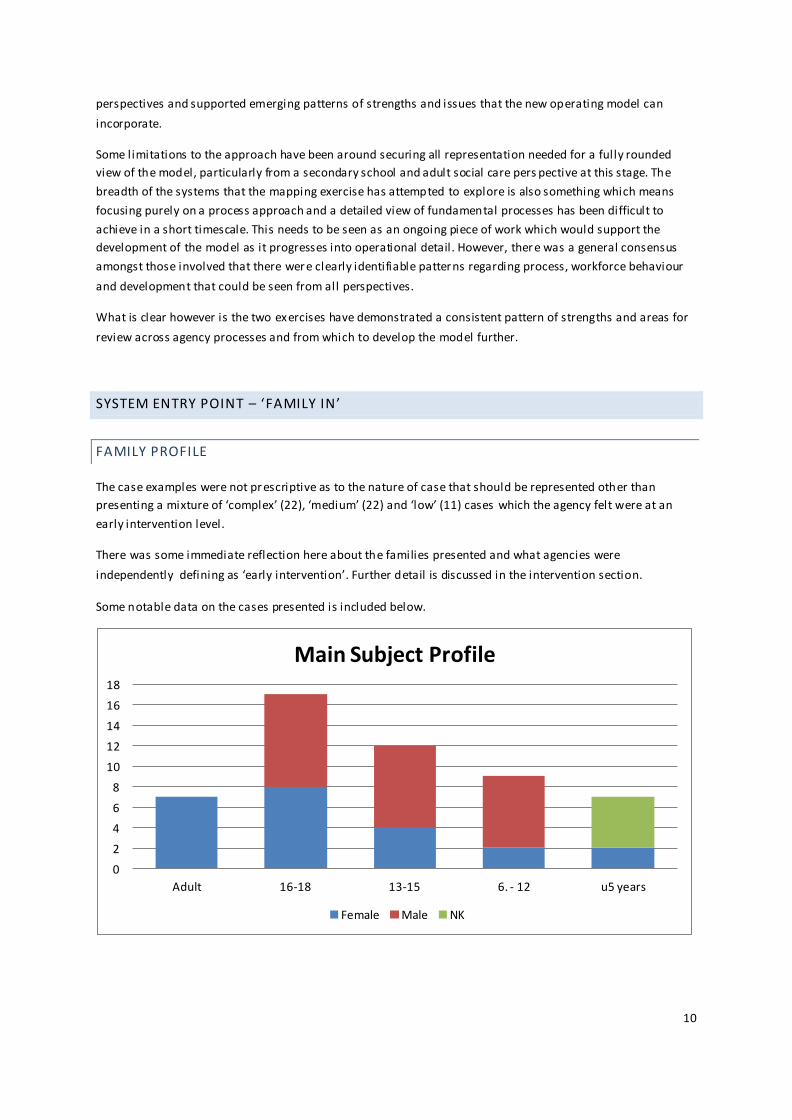
The case examples were not prescriptive as to the nature of case that should be represented other than
presenting a mixture of ‘complex’ (22), ‘medium’ (22) and ‘low’ (11) cases which the agency felt were at an
early intervention level.
There was some immediate reflection here about the families presented and what agencies were
independently defining as ‘early intervention’. Further detail is discussed in the intervention section.
Some notable data on the cases presented is included below.
0
2
4
6
8
10
12
14
16
18
Adult 16-18 13-15 6. - 12 u5 years
Main Subject Profile
Female Male NK

11
The sample showed a good range of who agencies were particularly focused upon from within the families
presented. A good mix of gender and age range allowed the exercise to explore processes across multiple
service interfaces.
The family profile of selected cases was also mixed and allowed for some consideration of the issues which
families bring that impact on practitioner knowledge, skill , capacity and interaction.
The way in which families were identified and began working with agencies was mixed although there were
clear reasons identified in the following ways: Self Referral (10), statutory requirement for the service to
engage (9) and through data tracking (4).
Self Referral: Where families trusted a service or individual, regardless of whether they were still eligible to
access the service, they tended to seek out that service or individual to reengage. The identified need for that
family did then not always line up with the service ‘criteria’ or require a long term response from that
practitioner, but provided a gateway of interaction with other services. The case samples related to self -
referral then either required a short-term, flexible response from that service, or support to negotiate working
with another service. This was not always successfully achieved either due to not meeting thresholds or time
delays in responding.
Statutory requirements: this included where engagement for families was either mandatory or a standard
approach, such as Health Visitor checks, school attendance and Youth Offending Team involuntary clients.
The majority of cases (32) identified at least 3-5 agencies involved with the one family, ranging from 1 to 10.
There was no correlation between the number of agencies and the level of identified complexity but some
warning is heeded over the result as agencies may have been involved yet not recorded in the process
feedback. The cases with higher numbers of identified agencies involved were the cases mapped through
specific desktop exercises and ranged from 5-10 agencies involved which was a more accurate representation.
This would suggest that the other cases in the sample had a higher proportion of agencies involved than
recorded for the purposes of this exercise.
There was little indication in case examples that there was a systematic checking of multi -agency data to
ascertain any issues identified for the family or who was known to be involved. Most children’s focused
services showed examples of speaking to the Advice Team for support but there was no evidence of cross
0
5
10
15
20
25 Grandparents
Single parent no identified partner
2 active parents: inc separated or co-habiting
Teen Parents
Father in prison
3+ children in family
children u5 in family
non inhabiting older children
Family Profile

12
agency checking i.e. police, or vice versa. The group discussions identified that for wider community and adult
services, the prevention route map and information services such as the Advice Team were very beneficial but
not widely known. The Family Focus service did demonstrate through their case examples that there had been
full desk top exercises exploring who was involved in the case, and for which individuals in the family.
This fed into a multi -agency coordinated approach for the family. Similarly, the Child in Need Service
demonstrated similar processes of a data and case review using methods such as signs of safety. This led to
identifying a range of options for the family, a recorded defensible decision about the multi -agency approach
and the best course of action at that time.
Key points raised:
Not knowing where to go for support or who is involved
Needing flexible, creative, negotiated approaches to access services quickly and proportionally
Better systematic use of service knowledge and data systems to identify families and manage
progress
ASSESSMENT
TYPE OF ASSESSMENT:
The examples highlighted the use of a Family Early Help Assessment (20), a Social Care Single Assessment (15),
an own agency assessment (13) and in some cases no formal assessment was identified (7).
Discussions with services about the use and benefit of the Family Early Help Assessment were mixed. Issues
with using the tool invariably related to definitions of when to use and confidence in being the Lead
Practitioner. Schools particularly found approaches cumbersome and potentially getting in the way of effective
engagement where other services found them a useful focus, particularly when trying to manage a multitude
of needs across the family dynamic.
FEHAs were predominantly not used by adult related services although Housing staff identified they were
often contributors when invited.
FEHA 36%
None identified 13%
Single Assessment
27%
Own Agency tool 24%
Type of Assessment identified

13
INFORMATION SHARING AND CONSENT:
The case examples demonstrated a general pattern of agencies working together as a routine practice. The
main response to the question ‘what helped…’ was met with a consistent response about creative and regular
multi-agency working. This was described at varying levels in terms of being able to discuss issues through to
fully multi-agency coordinated working.
The group exercise again reflected a general culture and desire to share information and work with families to
achieve this. There was some confusion over a couple of areas around consent and data sharing:
a) When a family does not consent and there is not an escalating concern, what do you do?
b) What some services interpreted as sharing information so that there could be an effective response,
this was not actually the case, leading to no response and no agency feedback. An example was the
police community support officers expectation that they send a referral to Children’s Social Care
regarding a family using the form ‘on the system’. Feedback was that this had to be done on
numerous occasions with limited response until a safeguarding assessment was finally done. There
was some investigation then required as to what PCSOs thought they were sending in and what
Children’s Social Care was actually receiving, which tempered the a gency response (i.e. a referral or
an information form?)
c) PCSOs identified that they effectively worked with the Community Safety Unit where information was
shared about the previous 24 hours police responses and then triaged for effec tive support from a
range of services for the ‘medium to high’ concerning incidents and target of vulnerable people.
Information was fed to PCSOs regarding the less ‘concerning’ incidents but this in turn does not
appear to filter to other agencies. A good example is feedback from the Health Visiting Service about
domestic abuse call out information not reaching their service regarding children under 5 years.
IDENTIFIED CONCERNS:
The primary issues identified by practitioners as the main reason for contact with their service are identified
below. The main initial concern was around school readiness, behaviour, attendance or attainment (31),
followed by concern for the child’s behaviour (24), especially where they were older.
Related to u5
19%
Behaviour/risk/ criminality
24% Health or
mental health 13%
School or learning
31%
Housing 13%
Primary Concern

14
As the relationship with the family was better unders tood, services were able to identify other issues arising
within the family. This was either as part of leading the assessment or the practitioner being part of a wider
multi-agency plan to tackle the full range of issues for the family.
Practitioners were describing a third of the cases involving levels of family violence (35), as well as health or
mental health issues. What appears an apparent gap in process then, is how able practitioners were to clearly
identify and work with these issues and their causes, or gain support to do so. Links to IDAS and some mental
health services were apparent and valued. However, when looking at what potentially hindered progress in
cases (albeit a small number of observations), practitioners identified:
delay in responding, services not responding in a timely fashion that worked with the motivation and
needs of the family. Particular examples were CAMHS, Social Care and Adult Mental Health Services
Having to re-refer
Family member/unit not meeting service ‘criteria’ and falling through gaps
no capacity within services to support and therefore ultimately being 'bounced' back to services,
increasing anxiety.
The issues identified by practitioners within the question ‘what other issues did you uncover?’ have a clear lin k
to the ‘toxic trio’: domestic abuse, substance misuse and parental mental health. These issues are particularly
research proven to have a significantly negative impact on families leading to long-term poor outcomes from a
very early age. The ‘trio’ were then evident in 90% of the case sample, that was identified from the responses
given. Reflecting on the workforce, service criteria and responses from the exercise, a further focus is needed
to ensure confidence, targeted resourcing and appropriate workforce development around these areas to
ensure that a proprtionate response at an early intervention level can manage the anxiety that these issues
bring. Ultimately, the case examples were showing that these cases were more likely to be escalated to
statutory services but without this creating any further resource or response. Certainly in the question ‘what
did you do? Who did you work with?’ and ‘was there a positive resolution’, there was little demonstrable
impact in these three key areas from that agency’s response.
Key points raised:
The size , use and ownership of assessments
Clarifying levels of fair processing and consent to share information
Domestic Abuse
35%
Health/mental health 34%
Substance misuse
21%
School/learning need 10%
Secondary Concern

15
A strategic response to support targeting resources, workforce development and commissioning
towards the main concern areas identified, particularly the ‘toxic trio’
INTERVENTION
THRESHOLDS:
31 cases were identified as having either current or recent involvement with Children’s Social Care Child
Protection or Child In Need services. It is interesting that these ca ses were being presented as cases
practitioners felt they were dealing with at an early help level when they had already crossed the statutory
threshold. 17 cases had no known or recent involvement. Some of these were acknowledged by practitioners
as having had historical contact with higher level services and a new concern was beginning to emerge in
raising a young child who was now growing older i.e. one particular child was not known to higher level
services, yet within the last 5-10 years, the children in the family had significant involvement across YOT, Police
and Children’s Social Care and the level of need appeared to have remained, particularly around domestic
abuse responses and adult mental health issues. They continue to refuse voluntary services . The point appears
to be that the family will escalate into higher cost services soon if an appropriate response or strategy to their
situation isn’t forthcoming.
A level of the current children’s social care child protection cases had evidenced a multitude of services
involved at an early help level with several previous ‘referrals’ to social care for a formal assessment. The term
‘referral’ is something which needs further exploration as what practitioners may consider a ‘referral’ was
often taken by social care as ‘information giving’, which would not receive a statutory response from a
safeguarding assessment team.
7 cases were escalated to the Referral and Assessment team but the majority of these were then sent back to
early intervention level with recommendations to continue coordinated work at that level. This appeared to
occur where anxieties were high about the family, the family was not getting access to services perceived to be
needed (i.e. adult mental health provision) or where they had disengaged and the single assessment was used
as a means of bringing the family back into support.
Similarly in group discussion, service representatives talked about how there was sometimes a pressure to
sanction families due to the nature of their service when a wider picture of need was presenting. Practitioners
felt that there was potentially a better way of sequencing approaches that helped to use potential statutory or
sanction based response to review engagement and better understand what is causing fami ly’s disengagement
for a variety of angles.
Responses regarding what hindered progress in cases was minimal. However, this was mainly related to: delay in responding,
services not responding in a timely fashion that worked with the motivation and needs of the
family. Particular examples were CAMHS, Social Care and Adult Mental Health Services, particularly around timescales
for engagement and assessment. Similar there were comments about families not meeting thresholds and being 'bounced' back to services.
A very small number of responses identified practitioners perspective that creative examples of working were
evident. Some comments related to being able to flex approaches and use different resources because
managers were able, or willing to do things a bit differently. Relationships between services also appeared to
affect the ability to be flexible in response both at early intervention and interfacing with statutory levels.

16
WHOLE FAMILY OR INDIVIDUAL INTERVENTIONS:
Whether the case example identified that there was whole family working, or whether the work was focused
on an individual was split (28/27 of 55)
Individual person-centred intervention was more likely to be evident where the child was older (late teens)
and focused on the needs and behaviours of the chil d specifically. This was also apparent where the child was
very young (l ikely under 2 years old) and work was focused more on parenting and meeting the child’s basic
needs to improve the child's progress.
The older young person examples clearly indicated that young people were often known to services prior and
were reintroducing themselves for advice and support for a variety of needs. The usual presentation was
regarding Education, Training and Employment (EET) and Housing. This does raise an interesting point in terms
of how these young people, particularly of high need, exit services. Targeting individuals aged 16+ through
pursuing the ‘unknown destinations’ for EET provision is one way of proactively engaging older young people
and something which needs to be considered as part of a wider outcomes framework and intell igence led
approach
The benefit of co-location was identified in both the case examples and group exercises. Practitioners felt that
being physically close to other practitioners allowed for quicker information sharing, a flexible ‘referral’
approach and also a better insight into local knowledge, what was happening for the families in their local
area. One practitioner in the group sessions described how extended family members used their access to
local facilities to consider how they could access support for other family members, and that this was also
ways families gained trust in agencies, knowing workers knew their communities.
Key points raised:
Having a longer-term strategy for complex families who come in and out of service support, at
whichever level of intervention.
Use of a coordinating approach to help flex and negotiate about threshold and sanction-related
cases and what they may need.
Be more creative with resource and autonomy to respond differently.
OUTCOMES
The case example exercise asked practitioners to identify positive outcomes for the family. Examples of
'measurable outcome' (17) include improved school attendance or attainment , reduction in offending, child
gained weight. Mainly, responses were about focussing on continued engagement (23) but l imited in a clear
focus as to what had been achieved for the family. Group feedback would support that practitioners often feel
that just getting a family on board can be an achievement. However, the group also identified that a lack of
clarity as to what the goals were to be achieved with the family, and from the family’s perspective, was also a
factor.

17
Key points raised:
Agencies needing to work to common goals and identify family progress
Managing engagement and compliance and how the ‘carrot and stick’ approach might be put to
better use to reengage families.
Identified, measurable
outcome
35% Better agency engagement
48%
Disengaged 17%
Identifying Outcomes


















