Proceedings of the and Resources for Occupational · Proceedings of the Workshop-on Needs and...
71
Proceedings of the Workshop on Needs and Resources for Occupational Mortality Data This report contains the proceedings of the Workshop on Needs and Resources for Occupational Mortality Data, January 21-22, 1987. The Workshop was sponsored by the National Center for Health Statistics, the Bureau of Labor Statistics, and the National Institute for Occupational Safety and Health. The use of industry and occupation data from death certificates and the history of coding these data in mortality data bases are reviewed. Options for future occupational motiality data coding are developed and discussed by agency representatives and working groups of Workshop participants. Evaluation of the options include cdteria of timeliness, geographic and occupational coverage and detail, data quality, surveillance capability, cost, and relevance to State and national research. Documents and Committee Reports Series 4, No. 26 DHHS Publication No. (PHS) 88-1463 U.S. Department of Health and Human Services Public Health Service Centers for Disease Control National Center for Health Statistics Hyattsville, Md. August 1988
Transcript of Proceedings of the and Resources for Occupational · Proceedings of the Workshop-on Needs and...

Proceedings of theWorkshop on Needsand Resources forOccupationalMortality DataThis report contains the proceedings of
the Workshop on Needs and Resources
for Occupational Mortality Data, January
21-22, 1987. The Workshop was
sponsored by the National Center for
Health Statistics, the Bureau of Labor
Statistics, and the National Institute for
Occupational Safety and Health. The use
of industry and occupation data from
death certificates and the history of
coding these data in mortality data bases
are reviewed. Options for future
occupational motiality data coding are
developed and discussed by agencyrepresentatives and working groups of
Workshop participants. Evaluation of the
options include cdteria of timeliness,
geographic and occupational coverageand detail, data quality, surveillance
capability, cost, and relevance to State
and national research.
Documents and Committee ReportsSeries 4, No. 26
DHHS Publication No. (PHS) 88-1463
U.S. Department of Health and Human
Services
Public Health ServiceCenters for Disease Control
National Center for Health Statistics
Hyattsville, Md.
August 1988

Copyright information
All material ●ppearing in this report is in the public domain and maybc reproduced or copied without pemtiaaio~ citation aa to source,however, is appreciated.
Suggested citation
National Center for Health Statistic. 1988. Proceedings of theWorkahopon Neadaand Resourcea for Occupational Mortality Data.Vita/ ●nd Health Statistics. Series 4, No. 26. DHHS Pub. No. (PHS)88-1463.
library of Congress Cataloging-in-Publication Dots
Workshop on Noeda and Resources for OccupationalMoRality Dsta (1 987: Washington, D.C.)Proceedings of the Workshop on Needa and Resources
for Occupational Mortality Data, January 21-22, 1987.
(Vital & health statiatica, Series 4, ,Documents andcommittee reports : no. 26) (DHHS publication ;no. (PHS) 88-1463)
Supt. of Doca. no.: HE 20.6209 :4f26Irrcludea bibliographies.“’The workshop was sponsored by the National Center
for Health Statistics, Bureau of Labor Statistic, and
the National Institute for Occupational Safety and
Health.”1. Occupational mortslity-Statistics-Congresses.
2. Death—Proof and certification-Congresses.L National Center for Health Statistics (U. S.)IL United States. Bureau of Labor Statistics.HI. National Institute for Occupational Safety andHealth. IV. Title. V. Series Vital and heslthstatistics. Series 4, Documents and committee repons ;
no. 26. VI. Serie= DHHS publication; no. (PHS) 88-1463.HA37.U1 693 no. 26 362.1 ‘0723 a 88-600196
[H81323.P6] [363.1 ‘12’0723]ISBN 0-6406-0393-2
For sale by the Superintendent of Documents. U.S. Government Printing 0r3ce, Washington, D.C. 20402

National Center for Health Statistics
Manning Feinleib, M.D., Dr.P.H., Director
Robert A. Israel, Deputy Director
Jacob J. Feldman, Ph.D., Associate DiwctorjbrAna@zkand Epiiiemwlogy
Gail F. Fisher, PhJ3.,Asso&te Dihxtor for Planning ondExtmmural l?mgm?ns
Peter L. Hurley, Associute DirectorforVi and HeaZthStatistics Systems
Stephen E. Nieberdirg Associate Dktor for blan~ent
George A. S&m&Associate Diwctor forData Processingand Se?w”ces
Monroe G. Sirken, Ph.D., Asswiate DiYvctoTfor Reseamhand Methodology
Sandra S. Smith, Information O&w
Office of Analysis and Epidemiology
Jacob J. Feldman, Ph.D., Associate Dinxtor
Division of Epidemiology and Health Promotion
Ronald W. Wilsq Director
Patricia M. Golden, S’cialAssistant
Ronald W. Wilson, Acting Chiej Envibunental StudkYBranch
Patricia M. Golden, Actikg Chie$ Health StatusMeasurement Bnmch

Foreword
~“s report includes the proceedings of a Workshopdevoted to the improvement of statistical data related tooccupational safety and health. These activitieswere spon-sored by the three agencies that entered into the formalbipartite Memorandum of Understanding at this Work-shop: the Bureau for Labor Statistic%the National Institutefor Occupational Safety and Health, and the NationalCenter for Health Statistics.
The Workshop was organized by the National Centerfor Health Statistics. Special thanks go to Dr. PatriciaBuffler. Other members of the Workshop planning groupinclude Dr. Bruce (Xhen, Dr. Haq Rosenbe~ and Mr.Jeffrey Maurer km the National Center for Health Statis-tic; Dr. Gilbert Beebe and Dr. Thomas Mason from theNational Cancer Institutq Mr. Harvey Hilaski from theBureau of Labor Statistic and Mr. Todd Frazier from theNational Institute for Occupational Safety and Health. TheWorkshop proceedings were prepared under the directionof Dr. Diane Wagener. Special thanks also are given to
Dr. Jacob Feldman for filling in for Dr. Manning Feinleibwho was suddenly hospitalized the day before the Work-shop. In additioq we particularly appreciate the work ofMs. Jane Schienle from the Bureau of Labor Statistics andMs. Madelyn Lane and Ms. Dorothea Donahue fkom theNational Center for Heiilth Statistics, who took care of themany administrative details of the Workshop.
Finally,the role of the weather must be recognized.Atnoon on the second day, the Workshop came to a prema-ture end because of one of the heaviest snowstorms to hitWashington D.C., in recent years. Therefore, most of thediscuAoxw pos-”ptsj and summary statements in theseproceedings are not from the transcript but from commentsprepared after the Workshop.
Ronald W. Wilson, DirectorDivisionof Epidemiology and Health PromotionOffice of Analysis and EpidemiologyNational Center for Health Statistic
iii

Foreword . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ....m
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
Chapter I. Plenary Session. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Greetings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Needs and resources for occupational mortality data . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Review of activities National Institute for Occupational Safety and Health . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Review of activities Bureau of Labor Statistics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Review of activities and conference objectives:National Center for Health Statistic
Figure 1. U.S. Standard Certificate of Death. . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Tables1. Deaths of men 20-64 years of age of races other than white with work experience, from selected causes of
death, by major occupation group, age, and standardized mortality ratiox United State%1950. . . . . . . . . . . . .2. Observed numbers of deaths and standardized mortality ratios (SMR) for selected occupational groups
exhibitingexcessmortality from malignant and nonmalignant rcspirato~ disease for males aged 20-64 yearxUnited States, 1950 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3. Growth in number of reporting areas adopting uniform occupation and industry coding procedures . . . . . . . .Utah’s experience in building an occupational health surveillanceprogram . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . .
223791113
12
141416
Chapter IL Review of options for producing ~upational mortality data . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17Option No. 1 Existing system: Occupational mortality coding at the National Center for Health Statistics for 20.
States (Annual) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17Option No. 2. 13qxmdingthe existingsystem to all States (Annual) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19Option No. 3. Data for all States in census years only. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
Option No. 4. Subsets of causes or subsets of States (Annual) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21Option No. 5. Mortality followbacksumys . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21Option No. 6. Followup of general population surveysusing the National Death Index . . . . . . . . . . . . . . . . . . . . . . 23Option No. 7. Followup of targeted National Center for Health Statistics surveys. . . . . . . . . . . . . . . . . . . . . . . . . . . 23Option No. 8. Cohort followup of national study groups. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25Option No. 9. Records systems. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26Option No. 10. Use of compressed vital statistics files . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
Table 4. Synopsisof options . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
Chapter III. Working group reports . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28Objectives for working groups . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
Figure 2. Data resources for occupational sumeillancc and research . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28Report from Working Group No. 1 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30Report from Working Group No. 2 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32Report from Working Group No. 3 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Report from Working Group No. 4
34. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36
Discussions. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37Summary of recommendations from participant questionnaires . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44
Chapter IV. Postscriptshorn sponsoring agencies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Postscripfi Bureau of Labor Statistics. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2Postscript: National Institute for Occupational Safety and Health . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47
Figure 3. Sentinel event notifications system for occupational risks (SENSOR):-1987 . . . . . . . . . . . . . . . . . . . . . . . . 48
v

Table 5. Surveillance activities for occupational disease reported by health departments in 50 States, New YorkCity, and Washington, D.C.: 1985 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 48
Postscript: National Center for Health Statistics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50
Appendixes
I. Memorandum of understanding . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52IL Workshop participant questionnaire . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53III. Workshop participants . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59
VI

Proceedings of theWorkshop-on Needs andResources forOccupational MortalityDataa
IntroductionOn January 21, 1987, a Memorandum of Understand-
ing (appendix I) was signed by the Bureau of LaborStatistics (BLS), the National Center for Health Statistics(NCHS), and the National Institute for Occupational Safetyand Health (NIOSH) to work collaboratively in the devel-opment of improved reporting systems and surveillance ofoccupational illness and injuries. The occasion of the sign-ing was used to convene a workshop (January 21-22, 1987,in Washington, D.C.) to explore the needs and resourcesfor occupational mortality data. This volume includes theproceedings of that Workshop.
Surveillance and research in the areas of occupationallyrelated illness and injury are important areas for healthpoliq. According to Langmuir (1976), “good surveillancedoes not necessarily insure the making of the right decisio~but it reduces the chances of making the wrong one.” Mlthree agencies (MS, NCHS, and NIOSH) have been col-lecting data relevant to surveillance and research of occu-pationally related illness and injury. NIOSH has identified aspectrum of Leading Work-Related Diseases and Injuries
‘Workshopsponsored by NationalCenterfor Health Ststisti~ Bureau ofLabor Statistics and National Institute for Ckupstional Safety andHealth.
that necessitates the collection of health data fkom earlysymptoms of disease to clinical illness to death. The devel-opment of a coordinated national strategy to obtain thesedata may require the use of several different complemen-tary data systems.
The purpose of the Workshop was to review the collec-tion and use of data regarding mortality risks by occupationand industry and to develop recommendations regardingfuture direction. A variety of options focusing on datacollected by NCHS and the States were reviewed, and theparticipants then evaluated these options in workinggroups. Evaluations included the following criteriz timeli-ness, geographic and occupational coverage and detail, dataquality, surveillance capability, cost, and relevance to Stateand national research. The working groups then reported tothe Workshop. In addition, a questionnaire for the evalua-tion of each of the options was given to the participants, andthe comments that were returned were reviewed in theseproceedings.
Reference
Langmuir, A. D. 1976.WilliamFam Founder of modem conceptsof surveillance. h. J. Epidetm”ol.5(1):13-18.
1

Chapter 1.Plenary session
Greetings
by Ronald Wilson, Director, Division ofEpidemiology and Health Promotion,National Center for Health Statistics
I would like to weleome you to this first Workshop onNeeds and Resources for Occupational Mortality Data.This Workshop is a collaborative effort among the NationalCenter for Health Statistics (NCHS), the National Institutefor Occupational Safety and Health (NIOSH), and theBureau of Labor Statistics (KS). We hope that it will bethe first of a number of such workshops dealing with issuesrelated to occupation and health. The immediate concernof this Workshop is the issue of the coding of occupationand industry on the death certificate and the fiture of thisactivity at NCHS.
In 19S0, the National Cancer Institute and NIOSHprovided NCHS with the funds to implement coding ofoccupation and industry on death certificates for a limitednumber of States with the hope that this developmentalproject would lead to producing occupational mortalitydata from the death certificates on a routine basis. Laterthis year, NCHS will make available mortality data tapeswith the occupation and industry codes for 16 States thatparticipated in this program during 19SS.
At this Workshop, we want to identify the needscurrent and future use% and resources available for thecontinued inclusion of occupational and industry informa-tion in the mortality data systems of NCHS. We havepartieipanta from the Federal Government, State govem-men~ industry, labor, and academia at this conference. Itis hoped that, with this broad participation, the Workshopwill develop recommendations that will identi& many needsand eoncerna regarding these mortality data.
2

Needs and resources foroccupational mortality data
by BailusWalker, Jr., Ph.D., M.P.H.,(%mmissioner, MassachusettsDepqtrnent ofPublicHeatth
At the outset, allow me to commend the Bureau ofLabor Statistics (BLS), the National Center for HealthStatistics (NCHS), and the National Institute for Occupa-tional Safety and Health (NIOSH) for their continuingefforta to prevent occupational disease and disability. Thedvities of these three Federal ageneies are reinforcingour efforts at the State level. Their teehnical assistan~grant%and other forms of help have enabled us to pursuesigniikant risk management programs, including workereducation, in our States and in local communities.
This is indeed an appropriate time to evaluate theneeds and the resources for developing ocwpational mor-tality data because we are recognizing at more frequentintervals the numerous and complex issues surrounding theidentification and recognition of occupational diseases. Atthe same time, we are constantly reminded that the preven-tion and control of workplace risk rquire that we have inplace comprehensive systems to ‘&ptureoccupational morb-idity and mortality data The development of suck systemscannot proceed very far without sincere Federal and Statecooperation.
I want to offer a State perspective from the vantagepoint of not only my Massachusetts public health portfoliobut also my membership on the National Academy ofSciences and the Institute of Medicine’s Commission forthe Study of the Future of Public Health in the UnitedStates. II& group was established last year by the Instituteof Me&ine to examine a broad range of public healthissues and problems and to make recommendations forfuture positive directions for public health. It has heldpublic hearings and collected a significantvolume of infor-mation.
Even to the most casual observer, it is elesr that wehave made significantprogress in the prevention and con-trol of occupational disease and dysfunctionsince 1910, theyear Alice Hamilton, one of the pioneers in occupationalhealth, was in Brussels attending a conference on occupa-tional disease. At that conference, the Belgium delegatewalked up to her and said, “In the United States, occupa-tional disease prevention and control activities do not infact exist.” According to Hamilton, she could not at thattime find papers published on industrial poisoning. Em-ployers eager to improve conditions in the workplace couldfind ve~ little advice from medical experts at that timebecause little progress had been made in the area ofindustrial hygieneand in the monitoring and sumeillanceofoccupationally related diseases.
The literature is far more complete now, and it pro-vides us with ample evidence that work-related diseasesmust continue to be among our highest public healthpriorities. Indeed, lle 1990 Health Objectivesfor theNatkwx
A Midcourse Review (Public Health Semite, 19S6), pub-lished in late November of last year, underscores the factthat the nearly 104 million men and women who make upthe workforce of the United States sustain an estimated 10million traumatic injuries on the job each year.
It is important at the outset of this Workshop torecognize that when we discuss occupational health andsafety, we are dealing with an expanded universe. In the1%0’s and 1970’s many of us watched the field of healthand safety grow from one that was primarily concernedabout injuries and acute poisonings to one that includedconcern for a broad spectrum of chronic diseasesdysfunctions-most notably, cancer. Today, we eontinu~dconfront mounting evidence of reproductive disorderscaused by workplace exposure% and we are increasinglyaware of clinical and subclinical necrologic dysfunctionscaused by workplace stressors. In addition, occupationalasthma and cumulative trauma disordera must be recog-nized as substantial occupational health problems.
On the horizon, but not yet fully acknowledged in thiscountxy, is the entire realm of stress-related health prob-lems such as peptic uleer~ hypertension, and emotionaldisorders, that can be attributed to working conditions.Thisexpandeduniverse of health problems is exph.incdby a newawareness of longstanding concerns of health and workconditions and by the changing nature of work and work-places.
Indeed, entirely new technologies and materials arebeing rapidly introduced without sufficient regard to theirpotential impact on human health. Fm will debate that thechallenge to prevent work-related diseases is today a sub-stantial one. I submit that sumeilkmee of health conditionsand the workplsee is an essential part of our preventioneffort. We m~ I believe, develop sensitive and timelysumeillance systems to identify work-related health prob-lems for targeting research and for intervention acclivities.
BUL here ag~ l’he 1990 Health Objectivesfor theN&m A MiiicoumeReview (Public Health Sewi~ 19S6)points to deficienciesin the system.For example,one of theobjectiveswas the elimination of occupational heavy metalpoisoning by 1990. Aczmding to the midcourse repo~ nodata are available to messur~ either directly or indirectly,progress toward obtaining this objective. Because no dataare available, it is not posd%le to evaluate the likelihoodthat this objectivewill be reached by 1990.
Another objective stated that .at least one question onlifetime work history and known exposure to hazardoussubstances should be added to all appropriate existinghealth data reporting systems. This objective was notachieved by 19S5. It k however, an important practicalmeasure that is now in effect in many States.
Sumeillsnce must not be limited to the monitoring ofhealth conditions with well-established occupational etiolo-gies. It must also enable us to generate new hypotheses, toident~ new problems, and to develop more effectiveinter-ventions. Omupational illness and injury surveilkumshould provide us with the numbers that we need to justifyour policies and programs and to carry them out.
3

But before we focus on the needs and resources ofomupational mortality dat~ we need to broaden our scopehere to note that there is a necessity to develop a compre-hensive surveillance program utilizing a variety of informa-tion from different data sets.
There are many smveilhmce mechanisms that have yetto be used. This year in Massachusetts, with NIOSH sup-port, we have assembled an interagency task force toidentifj existing data sources that might be employed foroccupational illness, injury, and hazard surveillance at rela-tively low additional costs. We are, for example, evaluatingthe utility of workers’ compensation records, clinical labo-ratory reports, health maintenance organization data bases,and a broad array of data systems on the health of infantsand children and the general population in Massachusetts.We are looking ve~ closely at right-to-know data andpollution data for both indoor and ambient air. We arescrutinizing vmy carefully the regional Occupational Safetyand Health Administration’s data and our own State in-spection reports. And we are exploring the feasibility ofusing the comparatively large number of occupationalhealth clinics in Massachusetts for the surveillance of work-related lung disease and dysfunction.
We have also initiated, with NIOSH support, a pilotprogram to assess the feasibility of occupational diseasereporting by sentinel physicians. It is within this broadcontext that we must evaluate the need and the resourcesavailable for gathering occupational mortality data.
In our enthusiasm for new and innovative sumeilhuxxmechanism% however, we should not underestimate thevalue of death certiikate information. Despite certain inac-curacies and limitations, death certificates remain one ofthe major sources of data on the health status of thepopulation.
In Massachusett& we are fiiding that these certiflxtesare reasonably reliable and that they are accurate as indi-cators of the occurrence of certain diseases that are signif-icant in the context of the health effects of the environment,including occupational environment.
Our experience indicates that death certificates canprovide the information required for defining death iiomspecified causes over time and idcntifjing variations be-tween geographic sections of our State. These analyses aremost helpful in planning and in implementing programs forprevention and control. “
Population-based occupation and industry data arevery difficult to obtain in a timely and inexpensive way.Beeause of thi~ death certificate statements of usual occu-pation and industry would appear to be an attractive solu-tion to this problem. Frazier and Wegman (1979), Frazier(1982), and Beebe (1981) have emphasized the ptentialusefulness of an occupational health surveillance systembased on death certificates. Others have demonstrated thatthe analysis of death certificates is a relatively simple andlow-cost means of generating leads about work-relatedhealth problems.
In Massachusetts, we are currently coding the occupa-tion and industry information contained on our death cer-
tificates and, again with NIOSH support, we are analyzingthese data to identi$ potential work-related health prob-lems. We are concerned about occupational asthma andchronic solvent poisoning and reproductive outcomes. Butwe are also concerned about cancer and acute myocardialinfarction and fatrd injuries—outcomes that we can exploreusing death-certificate data.
Today we should not be debating whether occupationalmortality data can be used, but rather, we should be askingourselves to what extent we should code and analyze avail-able industry and occupation information. Before we cananswer this question, a series of preliminary questionsdirected to the Federal agencies need to be addressed.
● What hadth conditions can be monitomd by death cerh~icates? Given these conditions, what alternative surveil-lance mechanisms an? mwdi/y available? What am thecompanrtive costr?
For example, in Massachusetts, we are currently eval-uating the use of cancer registry data for occupationalcancer surveillance. We know that the diagnostic informa-tion in the cancer registry is more accurate than death-certificate diagnoses, but the occupational information is,thus far, less complete and more highly dependent on themedical community’s inclusion of the occupational data inpatients’ medical histories. Not all States have cancer reg-istries and not all cancer registries include occupationalinformation.
● Am them &oes of industries for which death certificatestae pen+aps the best available souxe of information?
Industries with small workplaces-for example, gasstations and automobile repair shops-are diflicult to studyusing cohort methods.
● What an the i%dtations in the accumqy of death certi~-cate &ata? Am these limitations inherenb or am thempmspect3for imprmementin data qudip?
That iq will the forthcoming 10th Revision of theInternational Cktssification of Diseases enhance diagnosticprecision? Can we improve on the occupational informa-tion being prcAded, for example, by funeral directors?
I am very tempted to ask whether wc have the re-sources to follow up the leads generated by death certificateanalyses, but I hesitate to judge the long-range value of adata system based on the short-run commitments to occu-pational health of some segments of the present adminis-tration.
. What m the alternatives to natbwidg routine codbgand analysis of occupationalmatality data? What awtheu cosfi, including oppo~nity costs?
One alternative that has been proposed is the analysisof data only for years coinciding with the decennial census.Will this approach provide sufficient data to analyze smallindustries concentrated geographically, such as the jewehyindustry in Rhode Island? Who will code this information?Clearly, it does not make much sense to mount coding
4

capabilities in the States on a sporadic or catch-as-catch-can basis. Can these data be disaggregate back tothe States and used for State-specific studies? We haveapproximately 55,000 deaths per year in Massachuse@,and we estimate that we need, at a very minimunq 3 yearsof occupational mortality data for meaningful analysis.
Another proposed alternative is to select a representa-tive sample of States to provide data for nationwide statis-tic. Most certainly, in choosing only several States, we willlose information on certain geographically concentratedoccupations and industries. Will sample dat% for example, ,provide us with sufficient information to tiamine mortalitypatterns in minority groups? I am constantly appalled bythe inadequacy of health data to provide meaningful infor-mation about minority health-information that will enableus to develop policies and programs designed to addressminority health issues.
● Can we taget tidustries and occupd”ons of interest byfwing on specifi geogmphic locations? And who willdecde what ir “of iittemt?”
How can we make use of NCHS survey data? hesurvey samples large enough to allow for meaningful occu-pational morbidity analysis?
● At thti juncture, can we develop an automated system forcoding occupation and industty information accotiing tothe US. Bureau of the Census classification scheme? Iunderstand that it would be impossible to code 100pexent of the data by compute~ but wouldn’t it bepossible to code a significant percentage?
k our view, an automated coding system would resultin more standardized information and would substantiallyreduce long-term coding costs. Additionally, such a systemcould be applied to multiple data sets used by a variety ofagencies, including many represented here today.
As we consider the prospect of nationwide coding it isinappropriate to envision coding systems based on oldmodels—people in offices shuffling paper forms. It is 1987,we are in the midst of an information processing revolutionwith highly sophisticated technologies. Although previousattempts to automate coding have been limited, perhapsnow wc can move forward. Whatever type of surveillancesystem we consider, though, whether it involves deathcertificates, survey data, clinical data, compensation claims,or health maintenance organization data, we will certainlyneed to code industry and occupation information.
. What are the roles of the vmious Federal agencies andState governments?
Essentially, the options that we are considering requireadditional data gathering and analysis by the Federal Gov-ernment. And yet, I think that the bleak realities we face inFederal budgeting make this somewhat difficult. I would
hope that history would not repeat itself. In the period ofconcern about the Federal deficit, I cannot resist the temp-tation to quote from a letter Alice Hamilton wrote to hersister in 1914 about the inability of the Bureau of LaborStatistics to pay her for her occupational health studies.Hamilton wrote: “They are so poor they cannot make acontract with me for an investigation of rubber, but I meanto do it anyway and trust to their making it in July, the newfiscal year.”
I would hope that Janet Norwood’s Bureau of LaborStatistics is more affluent today than it was when AliceHamilton was on its payroll.
But I think it is important that there be a kind ofcollaboration. States are extremely hesitant to incorporateany additional data components into the Vital StatisticsCooperative Programs until the basic components havebeen adequately funded for all States. ,States, however,need to consider the value of coding occupational informa-tion for their own purposes as opposed to relying onFederal statistics. Our experience in Massachusetts wouldindicate that State-specific information provides more im-mediate direction for State research and intervention ef-forts. Clearly, it has a greater impact on our Statelegislature.
In the last 6 months in Massachusetts, we have hadrequests for occupational mortality data from unions, alarge number of requests from academicians, and an inor-dinate number of requests from health care providers. Wehave used occupational data to elucidate the geographicaldistribution of cancer, which we analyze routinely as part ofour environmental surveillance program.
Clearly, from our experience, there is a user constitu-ency. By providing information and periodic report% weincrease that constituent, and in doing so, we gain supportfor our programs.
In conclusion, let me stress the need for collaborationbetween Federal agencies and the States. I commend thejoint efforts of the agencies represented here today. Ibelieve sincerely that these seminars and workshops areextremely helpful. And I suggest that, until we have abetter, readily available source of information, the use ofoccupational mortality data is an essential component ofany comprehensive effort in occupational medicine.
A 1986 report to Congress by its Committee on Gov-ernment Operations was entitled Occupational Health Haz-ard Swveillance: 72 Years Behind and Counting (U.S.Congress, 1986). The overriding question is not can weafford to code occupational mortality data but can weafford not to?
References
Beebe, G. W. 1981. Record linkage and needed improvements inexisting data resources. Quantificationof OccupationalCancer.Banbwy Report No. 9. Cold Spring Harbor Laboratory.pp. 661-673.
5

Frazier, T. M.: 1982. The use of national and State data systems Public Health Service. 1986. 7he 1990 Health Objectives jbr thefor occupational health .swveilkmce. EnvinmnentaZ Epidenu”o@y, Nadon: A Midcowse Review. Washington: U.S. Governmentedited by P. E. Leaverton. New York Praeger Publ. pp. 121-127. Printing Office.
Frazier, T. M., and D. H. Wegman. 1979. Exploring the use of U.S. Congress. 1986. House of Representatives. Occupationaldeath certificates as a component of an occupational health Health Hazard Surwillance: 72 Years Behind and Counting. Housesurveillance system. Am. J. Public Health 6Ck718-720. report 99-979. Washington: U.S. Government Printing Offk.
*
6
.

Review of activities: Nationalinstitute for Occupational Safetyand Health
by J. DonaldMillar,M.D., Director,NationalInstitutefor OccupationalSafetyand Health
Introduction
It is a real pleasure for me to be here with you for thisWorkshop on Needs and Resources for Occupational Mor-tality Data. I am proud to be associated k tiis wifi Dr.Manning Feinleib and Commissioner Janet Norwm& who,as true leaders in international statistical circles, have doneso much to provide this Nation with sophisticated data onour health and work. Also, I appreciate the kind introduc-tion by my good friend and colleagu~ Ronald Wilson.Among his many duties is service with me on the Subcom-mittee on Environmental Health Risk Assessment of thePublic Health Service Committee to Coordinate Environ-mental Health Related Programs. In the Subcommittee, wegrapple with some tough issues in quantitative risk assess-ment, and we know well the need for sound data.
It is good to be here with many colleagues from theState health and labor departments, where so much of thereal work in statistics is done. When I was serving asDirector of the Bureau of State Services, I heard from Stateoffickds a constant refrain-”We sure wish you Feds wouldget your acts together and give us a consistent message!”Well, the tripartite Memorandum of Understanding amongthe National Center for Health Statistics (NCHS), theBureau of Labor Statistics (BUS), and the National Insti-tute for Occupational Safety and Health (NIOSH) that willbe signed today is aimed’at that very purpose. We are vexyintent on getting our acts together in, as is stated in theMemorand~ “... improving occupational illness and in-jury reporting systems and surveys.”
It is grati@ing to me that the first highly visiile c0lh3b-orative action to be taken by us under terms of the Memo-randum (paragraph II-8) is to bring together our partnersfrom the State& busine~ labor, and academia. & long aswe are getting things coordinated, it makes good sense forus all to do it together. Please note that this Workshopcould be put fonvard as Workshop number one, suggestingit is the first of many. I hope so. It is an important beginningin making utilitarian sense out of a myriad of activities thatare rich in complexity and diversity, but not in unity.
The movement
This meeting and the formal collaboration of NCHS,BLS, and NIOSH result from a growing national movementof people who recognize the need for sound information onthe relationship of occupation and health-or, more pre-cisely, the relationship of occupation to injury, disease,disability, and death. Two congressional hearings on thesubject of the surveillance of occupational disease withinthe last 18 months testify to the strength of this growing
awareness. Until recently, it would have been unthinkablethat a subject so seemingly esoteric and technical wouldhave attracted such congressional attention. For this we areindebted to concerned activisb such as Eric Frumin of theAmalgamated Clothing and Textile Workemj AFL-CIO,who is here today. He and othera have pushed this idea ofoccupational disease suweillance with enthusiq imagi-natio~ and effectiveness.
Dreamscomingtrue
It would please me if this Workshop is seen in theminds of some here as solid evidence of the incipientrealizadon of dreams long nurtured. Within NIOSH, forexample, I think of Todd Frazier, who has labored longhard, and diligently over the past 15 years to encourage,stimulate, and nourish the surveillance of occupationaldiseases and injuries. Todd the seeds you planted havebegun to bear the fruit of national attention.
What NIOSH is doing
Within NIOSH, the surveillamx of occupational dis-ease and injury is now proceeding across the organization.Within five of our seven divisions-in both Cincinnati andMorgantown-there are specMc surveillance programs. Iam proud of all this activity by NIOSH professional%including those in attendance here John Sestito, PatriciaHonchar, Carol Burnett, Robert Mullan, Michael Moll,David Brow and Dennis Bregman. Moreover, Dr. JamesMeli~ whose Division of Surveillance, Hazard Evalua-tions and Field Studies is most visiily associated withsurveillance, will chair a portion of the Workshop.
Last week in Morgantown, we presented our annualProgram Review of NIOSH to Dr. James O. Mason,Director of the Centers for Disease Control (cDC). In myjudgment, it was the best program review by NIOSH since Ifirst got involved with NIOSH as acting director in 1978.Included in the review was a presentation by Dr. Moll ofpreliminary resuks of a new surveillance effort. He pre-sented an analysis of all death certificates for occupationalfatalities during the years 1980-84. Straightforward andfairly simple preliminary analyses revealed striking evi-dence of a hitherto unidentified epidemic of occupationaldeaths among female workers due to homicide in theworkplacq the results also showed that for most States inthis great hmd agriculture is the occupation associated withthe highest rates of occupational mortality. For whateverr-n, I had not expected that. His presentation graphi-cally contirnmd the point made earlier, that there still areimportant “leads””to be had in the collection and analysis ofmortality data.
Because our surveillance activities in NIOSH havebecome so widespread and varied, I recruited Dr. EdwardBaker from Harvard University onto our headquarters’staff as Assistant Director of NIOSH. He is one of theoutstanding young figures in occupational medicine. I gavehim a spedc charge to develop a comprehensive plan forsurveillance activities in NIOSH and asked him to coordi-nate our activities in accord with the plan. That plan was
7

developed, many of you have had input into it, and we aregoing about its implementation,
Surveillance in the national preventionstrategies
As many of you know, because you were there, NIOSHconvened two national symposia on the Prevention of Lead-ing Work-Related Diseases and Injuries, one in Atlanta inMay 1985 and the secxmd in Cincinnati in October 1986.Both were attended by 450-500 of the Nation’s top profes-sionals in occupational safety and health. They came born awide variety of organizational settings. In these symposi~we introduced for discussion and modification, by theseprofessionals, 10 proposed national strategies for prevent-ing each of the 10 Leading Work-Related Diseases andInjuries-one strategy for each entry on the list.
This process has been exhilarating to me personally,and it has given rise to a unprecedentedly broad-basedunderstanding of what needs doing to reduce the burden ofthe Nation’s most important occupational health and safetyproblems. In all of these strategies-each 1 of the 10–theNation’s experts called specifically for epidemiologic sur-veillance of the target conditions. In 9 of the 10 strategk+they also called specifically for environmental smveillanceof the causative agents associated with the condition.
In responding to this ringing endorsement of the needfor better surveillance, we have reinvigorated our notions of.eventually having in this country a comprehensive systemthat wotid result in the reporting of all significant healthproblems associated with occupation. The concept also nowhas a name, SENSOR, which is the acronym for
SentinelEventNotificationSystem, forOccupationalRisks
Many aspects of this concept await full elaboration, butat least we have the dream and a name for it. You will hearmore about it horn Edward Baker.
The big question
With all the national interest generated in surveillanceof occupational health problems, there is now a big andsomewhat scary question posed by our many interestedallies “Now that you have our attention, what are yougoing to do about this thing called surveillance?” It is achallenge we cannot afford to fumble.
Action–The reason for data
In the Statement of Purpose for this meeting there is aquote by Dr. Alexander D. Langmuir, for many years theNation’s premier epidemiologist and Director of the Epide-miology Program, Centers for Disease Control (CDC). Hewas my boss the first 5 years I was in the Public HealthSeAce. In epidemiologicrd circles, he is justifiably calledthe “Father of Disease Surveillance in America.”
Beginning in the early 1950’s, under Dr. Langmuir’sleadership, CDC and its components have pioneered effortafter effort in the suweillance of human health events.These encompass a very wide array from classical infectiousdiseases such as poliomyelitis and influenza to chronicdiseases such as lead poisoning and cardiovascular diseaseto conditions that go beyond the definition of “disease” suchas abortion and sudden intknt death syndrome (SIDS). Indiscussing surveillance, hc often said something akin to thefollowing
Surveillance is done for the sake of action-preventiveintervention if possiile-if not, at least analysis andmeaningful reporting back to those who collected thedata. Unless you are prepared to act on the dat~surveillance is an unconscionable waste of resources.
We in NIOSH are interested in surveilkmce-sudl-lance for the sake of uction, surveillance for the sake ofpmventhfi and sumeillance for the sake of erutiicatt”on, ifpossiile, of at least some occupational diseases and inju-ries. We, all of us here, now have the Nation’s attention tothe need for sumeilhmce of occupational diseases andinjuries. We have a priceless and probably fleeting oppor-tunity to move forward briskly, intelligently, and together.Let’s make the most of it!
8

Review of activities: Bureau ofLabor Statistics
by Janet L Norwood, Ph.D., Commissioner,Bureauof Mm Statistics
Let me first say that I think that occupational safetyand health is probably the most imprtant issue in the labormarket today. Jobs are important. Income is important.And there are a lot of other issues. But if we cannot have asafe and healthy workplace, it really does not matter toworkers what happens otherwise.
Occupational safety and health information is essentialto bringing about a safer and healthier workplace and topreventing the problems Dr. Millar was talking about. Theeconomy today is changing and I believe the changes aregoing to make it harder, not easier, to get good data. Ourwhole industrial economy is being restructured. Our man-ufacturing industries are becoming more efkient by re-moving from production many old, inefficient, and,Perhapq unsafe and unhealthy plants. At the same time,new technology is being put in place, and new substancesare being used in the manufacturing process. We arecreating a large number of jobs. In fact, in the past 49months of reeovery, we have added 12 million new jobs tothe economy in different industries, activities, and occupa-tions than before. We are, in fact, in the midst of change—both industrial and omupational. We need to take thesechanges into account if we are going to be looking at dataon occupational safety and health.
What does this mean to us who are here today? Werecognize the tremendous responsibility to develop infor-mation that can be used to establish public policy, to informour citizens, and, for those who have responsibility to do so,to take preventive action. A number of these issues will bediscussed here today. At the Bureau of Labor Statistic(BLS) we have had a program providing information onsafety and health for a long time. When the OccupationalSafety and Health Act was passed, the Secretary of Labordelegated the statistical requirements of that act to theBureau of Labor Statistics. More than 10 years ago, webegan a system of recordkeeping in establishments and asurvey of business establishments-2S0,000 every year. Wehave a Federal-State cooperative relationship to developconsistent data from business establishments and fromadministrative records. We have also started a series ofwork injury surveys to provide data to the Department ofLabor for regulatory deeisions.
It is now more than 10 years since that work was begun.As in all statistical programs, it is always good to reassesswhere we are. For that reason, we have asked the Commit-tee on National Statistics of the National Academy ofSciences to setup a panel to review this work. We believe,and I am very pleased to tell you that !lxreta~ WilliamBrock agrees, that rec.ordkeeping and data are essential tothe implementation of the Department of Labor’s respon-sibilities. The data systems BLS and the National Centerfor Health Statistics (NCHS) maintain and the work that
the National Institute for Occupational Safety and Health(NIOSH) is doing can help to sensitize both workers andemployers to these needs.
There are problems there can be no question aboutthat. There are problems with almost any statistical pro-gram. Some are harder to solve than others, but what weneed to do is to keep working at them.
We have got to learn more about what causes injuri+Mn_ and fatalities in the workplace. By working to-gether with NCHS and NfOSH, we ean learn and perhapsdevelop a better data base for the population.
Many approaches can be taken to developing data inthe workplace. There are household sumeys, establishmentsurvey% and administrative records. Each data set hasproblems and strengths. In the household survey are% inaddition to the NCHS sponsored surveys, there is the BLSSCurrent Population Sumey that is basically a labor forcesurvey. This survey, conducted for us by the U.S. Bureau ofthe Census is used to collect information on people from60,000 households who work or look for work. It was notdesigned to collect health, safety, or injury information. Thesurveys qxmsored by NCHS are designed to collect healthand injury data. They were not designed to ecdhxt informa-tion on the workplace. We need to experiment in bothsumys to get additional information that will bring thesedata systems together.
We would be remiss if we ignored the fact that theexisting household surveys were created for different pur-poses. There are a number of statistical issues that arisewhen we add questions to a survey. Occupational data arevery difficult to collect. People do not always know whattheir occupation is. I had an interesting experience visitingthe computer-assisted telephone installation of the U.S.Bureau of the Census, where testing on the Current Popu-lation Survey was conducted. I listened to the questioningof the respondents. One after the other, they stumbled onthe questions of industry and occupation, but particxdarly ofoccupation. One respondent, when asked a question aboutindus~ and then about his occupation, said: “I just toldyou I worked in a bank. Why are you asking me myoccupation?” Now we have to recognize as survey special-ists that some improvements need to be made, both forsurvey purposes and also for administrative reeords. Weshould not get earned away with the belief that all we haveto do is take a few questions and add them to the CurrentPopulation Survey or the National Health Interview Sumeyor put some extra codes on the mortally records. It may getus toward a more perfect data system, but it is not going todo it by itself.
I do want to express my admiration for the leadershipthat NCHS has taken in the whole area of cognition andsurvey research. I think Monroe Sirken’s work is an exam-ple for the whole statistical system. It is an area that we atBLS are moving into as rapidly as possible. For the kinds ofissues we are talking about today, cognitive testing istremendously important.
There are other ways of getting data besides householdsurveys. Obviously establishment surveys are one way. At
9

BLS we have found that we get better occupational datafrom business establishments than from household surveys.Our occupational injuries and illnesses survey (interestinglythe only mandatory survey in BLS) is an establishmentsurvey based on a comprehensive rccordkeeping system.We are working hard to improve the data from this survey.But we recognize that problems remain. We have also beenlooking at our other establishment surveys, such as theWage and Industrial Relations Surveys, that may form thebasis for further work. If we could find a way to get theresources, we would like very much to begin collecting datafrom business establishments and then surveying subsam-ples of employees at those establishments to get furtherinformation.
Another area of importance is the full use of adminis-trative records. I am glad to see Fritz Sheuren here. He hasprobably done more than anyone in the statistical area tokeep reminding us about the importance of administrativerecords as a source of data. They reduce the burden onrespondents, and they usually cost less than direct sur-veys—certainly less than household surveys.
Our experience at the Bureau of Labor Statistics sug-gests that a great deal can be done through Federal andState cooperation, We like to think that BLS has developedone of the best Federal and State cooperative programs inthe statistical system. Perhaps NCHS might disagree withus. We have, in the labor market area, tremendously goodrelationships with the States. We are building on thoserelationships in the safe~ and health area. The only way tohave an effective Federal and State cooperative relationshipis to make it truly cooperative. That means that there haveto be two parties to the system. Second, it has to be asystem in which both parties gain. You cannot go out to theStates and say, “You have got to do this because the FederalGovernment wants you to do it.” Even if you pay them forit, the States have to need the data that are collected.
In my experience, I have found the real work to be inthe rest of the country-not here in Washington. The datathat can be used by the States are usually the most practicaldata for administering programs and even for informing thegeneral population. Our job in the Federal Government is
to try to provide leadership, to bring the States together,and to develop quality standards and statistical approachesto have data that can be matched or coordinated for theStates as well as for the Federal Government. The NationalCenter for Health Statistics has a great deal of experiencein working with public health authorities. At BLS we arebeginning to work more and more with public healthauthorities in the States. Our major contacts have been withthe Departments of Labor in the States, in most cases withthe employment security agencies. All of the data collectedby these agencies are extremely important to the Nation asa whole and to its people. Because we believe that theseissues are so important, we are devoting a great deal ofattention this year to a complete reorganization of ourWage-Industrial Relations and Safety and Health Pro-grams. George Stelluto and William Eisenberg are perhapsspending more time with me than they would like, but whenwe are through, we will have moved ahead a great deal.
This really underscores the importance of the work ofthis conference. We were very pleased at the response wegot to the conference that BLS hosted with assistance fromNIOSH and NCHS on issues involving the measurement ofhealth statistics in Albuquerque. We hope to see more andmore of these kinds of cooperative endeavors. The prob-lems are too large to be solved by any single statisticalagency. We have to remember that we are living in a periodof budget austerity, and the challenge is to find ways toaccomplish what we need to do at minimum cost. We haveto get large benefits with small increases in budget. Ibelieve that we can find ways to develop data from house-hold surveys, from business establishments, and from ad-ministrative records. Sampling of administrative records isextremely important because collecting comprehensive datamay not be possible.
We would like to draw from administrative data in amore practical manner to develop estimates for the Statesand the Nation as a whole. We believe that, by workingtogether, we can find ways to develop the information thatis needed to understand the kinds of issues that are facingthis country and to move forward to improve the conditionsin the workplace.
10

Reviewof activitiesandconferenceobjectives:NationalCenterfor Heaith Statistics
by Jamb Feldman, Ph.D., Direetor,Office ofAnalysisand Epidemiology,National Centerfor Health Statiatiea
It is a great pleasure for me to welcome our distin-guished speakers and participants to this Workshop onoccupational health statistics. ~s Workshop, a joint effortof the National Center for Health Statistics (NCHS), theBureau of Labor Statistics (BL8), and the National Insti-tute for Occupational Safety and Health (NIOSH), willserve several purposes. The Workshop will identifi gaps inoccupational health statistics that are needed for problemidentification and surveillance. It will help identi~ the roleof participating ageneieq particularly that of the NCHS,which is the Federal agency responsible for collecting gen-eral purpose health statistics An~ finally, the Workshopwill help tG identi~ resources to support this effort.
This Workshop will foeus on occupational mortalitystatisti~ an area in which NCHS and its predecessoragencies have a long history. Our current developmentalactivities are reaching a stage that makes today’s topicparticularly apropos. We are interested in determining howvital statistics data can contribute to the development of anational strategy for occupational mortality surveillanceand research.
Surveillance and research in the areas of oceupationdyrelated illness and injmy are extremely important topics.Indeed, the spectrum of the Leading Work-Related Dis-eases and Injuries identified by NIOSH (Centers for Dis-ease Control, 1983) necessitates the collection of healthdata from early symptoms of disease to ciinieal illness andultimately death. The development of a coordinated na-tional strategy to measure these outcomes may require theuse of several different and complementary data systems.
I will digress briefly to discuss some alternative meth-ods for eolkxting occupational mortality data. A studypublished by Kitagawa and Hauser (1973) linked about300,000 death certificates for the period May throughAugust 1960 with the U.S. Bureau of the Census’ scheduleson April 1 for those individuals. From the U.S. Bureau ofthe Census questionnaire, the current occupation of theindividual could be determined. Because the death certifi-cates and U.S. Bureau of the Census questionnaires repre-sented information for the same population, the mortalityrates could be calculated for different occupational groups.Unfortunately, even with the fairly large sample size, thedata base was not suftkiently large to do analyses onspeeific occupations or on highly specific causes of death.
In an ongoing study jointly sponsored by NCHS, theU.S. Bureau of the Census, and the National Heart, Lungand Blood Institute, a sample of about a million individualswho had been participants in the Current Population Sur-vey for 1978-83 are being tracked through the NationalDeath Index (Rosenberg and Feinleib, 1986). This study
links the Current Population Survey sample with deathreccmis in a prospective fashio~ providing a growing &tabase similar to that of Kitagawa and Hauser (1973).
Mortality as an endpoint has certain methodologiclimitations for studies of occupational health. Death gener-ally occurs late in the etiologicprocess. However, if mor-bidity measures ean be detected at an earlier poin~interventions might be performed. At NCHS we are cur-rently planning our third National Health and NutritionExamination Swey (NHANBS III) in close collaborationwith NIOSH and various other agencies. That survey willhave an occupational component, including assessments ofcentral nervous system and pulmonary functions., In addi-tion, determinations of some trace metal concentrations inblood and urine and, in a nonrandom sample of 20 to59-year-old subject% volatile organic compounds in bloodand pesticide residues in urine will be used as indicators ofexposures to some toxic-ants.Two examination sumeys werecompleted in the 1970’s. The f~st of these surv~NHANES ~ is being followed up in collaboration with theNational Institutes of Health. This will provide informationon the course of occupationally-related diseases and ondiseases that developed after the initial suIvey. Finally, theNational Health Interview Sumy (NHIS) can also be usedfor occupational morbidity analyses. NIOSH has used thesurvey to publish differentials in a variety of conditionsaccording to industry and occupation (Kaminski andSpirtas, 1980). We are trying to improve the measures ofoccupational exposure in that survey. The 1988 NHIS willinclude a special topic section on occupational health devel-oped in collaboration with NIOSH and BLS. This surveywill include questions on longest joh symptoms of backpainor hand discomfor~ work injuries skin eonditionq eye,nose, and throat irritation; and chronic conditions.
In this Workshop, we would like to review the eolkc-tion and use of data regarding mortality risks by occupationand indust~ in order to develop recommendations regard-ing future directions. Of crucial concern to NCHS is thecontinued implementation of coding of indus~ and occu-pation on death certificates. A variety of options that focuson data collected by NCHS and the States will be reviewed.These should be evaluated using criteria such as timeline+geographic and occupational coverage and detail, dataquality, and surveillance capability (that is, sensitivity andspecificity of the compilations of the occupationally relatedmortality data). The issues are
. How many relationships between occupational expo-sure and deaths are discovered based on coded ocq-pational data horn death certificates?
. What proportion of all of the elevated standardizedmortality ratios or proportionate mortality ratios thatare identified turn out to ident@ hazardous situations?
. Could the information have been gotten by othermethods?
We anticipate that, by using existing data that includecoding occupation and industry from death certificates andby implementing new data collection efforts in support of a
11

national strategy for occupational mortality surveillanceand research, the efforts of this Workshop will result in thedevelopment of practical rcmmmendations and priorities.
Statistics compiled from death certificates have beencrucial historically to occupational health studies. Over twocenturies ago, Sir Percival Pott observed the associationbetween the occupation of chimney sweep and an elevatedrisk of scrotal cancer, due to the exposure to soot. Sincethat time, many countries have produced occupationalhealth data fkom death records. Great Britain has the bestrecord; they have produced an occupational mortality sup-plement almost every 10 years for the past century fromvital statistics in combination with their census data. Therecord for the United States is much spottieq we publishednational studies in 1870, 1880, 1890, 1900, 1930, and 1950.
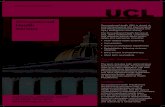
Occupation and industry from information is obtainedfrom the funeral director’s entry on two items on the deathcertificate (figure 1). Figure 1 is the U.S. Standard Certifi-cate of Death that is being recommended by NCHS for use
in the States beginning in 1989. The Standard Certificate ofDeath is revised about every 10 years to reflect changes inthe need for statistical data and to meet changing Statelegal requirements. The Standard Certificate of Death thatwill be used beginning next year differs from that used formany years in the United States; however, the occupationand industry items (12a and 12b) are unchanged from theversion of the death certificate currently in use. Almost allStates use items that are identical or very similar to thoserecommended on the Standard Certificate of Death (Ka-minski et al., 1981). Specifically, the information sought isthe decedent’s usual occupation, that is, the kind of workduring most of his or her working life, and his or her kind ofbusiness or industry.
In the most recent national study for the United Statesby Gurahtick (1962, 1963a, 1963b, 1963c), working withMoriyama and Dom, occupational mortality was estimatedfrom death certificates for over 300,000 male decedents.Table 1 provides illustrative data from this study for males
Table 1. Deaths of men 20-64 years of age of races ether thsn white with work experience, from selected causes of death, by majoroccupation group, ●ge, ●nd standardized mortality ratiox United States, 1950
[Ferrnars and farm tabot’ers]
SLmdeKllrs+d morialny raw
m64 25’59Cause of cbath Tofai m w
Allcausee . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11,689 190 196
Tuberculosis, Cll fCMIS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .001-019 752Syphillsand ttssequelae . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ...020-029
259251 E m
Malignant neoplasm, Including necplasms of tymphatio and hemato@etb thsues. . . ...140-205 889 mMal~MIMpl=mofWti=~Mdp_ . . . . . . . . . . . . . . . . . . . . . ...140-148
10425 74 J’;
Maltgnent neoplasm of stomach . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ...151 225 201MalJgnent neoplasm oflntastlneand rectum . . . . . . . . . . . . . . . . . . . . . . . . . ...152-154 29 72Mallgnant neoplasm of tracheil md of bronchus and lung. . . . . . . . . . . . . . . . ...162.183
8387 49
Mallgnantneoplesm ofprostrafe . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . ...177 100 3::Malignant neoplasm of kidney . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .180 ?!JMaltgnant neoplasm of bladder and ether urhary crgsns
-lJ. . . . . . . . . . . . . . . . . . . . ...181 2
Mallgnent neoplasm of brain andolherparte ofnervoussystem. . . . . . . . . . . . . . . . ...193 12 (’.’ (’)Leukemia andaleukemia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ...204 34
WM@WI=IIC ~ other IWO@SWW63
of tym~k and harnefcpcietk ftseuss . . . .2004K13,205 37 88Diabatesrnelllfus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ...260
7498 143 164
MajOf OCJdbVSSCUbWS* dbeaaea . . . . . . . . . . . . . . . . . . . ..330-334.4CI0-46S.892-594 5,555 187 190
Dlseasaa of cardiovascular system . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .330-334,4clo-4e8 5,170Vascuiar lesions affecting central nervous system , . . . . . . . . . . . . . . . . . . . . . ...330-334 1,472 E ::Dbeasas of ttaaff and rlwurnatk fever . . . . . . . . . . . . . . . . . . . . . . . . . . .400-402,410-443 3,406 m m
Rheurnaficfevarend chronic rheumatic heart cksease . . . . . . . . . . . . . . .4IW402,41O-418 156 118~e~mtk~~d-~,hcludbgcom~d- . . . . . . . . . . . . . . . . . . ...420
1071,184 71
Merbsclerctk heart disease so described . . .73
. . . . . . . . . . . . . . . . . . . . . . ...420.0 245 94Other diaeaseaof comnaryarleries. . . . . . . . . . . . . . . . . . . . . . . . . . ...420.1.420.2
103939
Olhermycoardiel degeneratbn . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ...42269
407 z~rfensbnwtlh heertcflsease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ...440-443 1,066 m !%
Hypafensbn willwut menlbn of heart . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .444-447 151 m mGenera! arlerbsclerosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ..4S0 es 35!
Chrorrio and unspecifbd nephriits end other renal solerosls . . . . . .m
. . . . . . . . . . . ..se2.594 ~
Inftuenraand pneumonki . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ...460.493
—
451Other diseeses otraspiratory system. . . . . . . . . . . . . . . . . . . . . . . . . . . ..470-475.500.527 71 % %Ulcer IX stomach . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ...540 1s0 161Ulcer of duodenum . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Appendices
541 z 88 (’). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34 179
Hemki and Infeatlnal ebskuofbn . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .569,%E 88Cinhoefscfllver . . . . . . . .
300. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 61 % =!B
Acclderlfe . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .E8COE= 1,139 175 179Whneafwork . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 167 108Notwhlleat workand nctetated . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
109972 195
Sukide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .E96S,E97&E979 105Homklde . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .E984,E960-E98S 8% i%— —
SOum Gurdnick iea3a.
%t00rmuonc4con@od
12

U.S. SfANDW
FEs&N7S4AcuELK
INn&%DssI aEEslsssmE
M HASM9Xi
-
ssEosnNImNw oTNEnmc
EEmsnummNIsomLm EAos
aiim
SEEFs!nNlmNoNolNsssmE
Alm3
FIWT.W2SEv. lMS
lDcumx — CERTIFICATEOF DEATH S7A7Em WJMun1.DECEDENTS NAME fftiL~L4@ 2. SEx S. DATE W DSATIE~kov.v=)
6. SOCIAL SECU_ *SER Sa.AOI?-I.UI ltintdmv M ~DfR 1 ‘=S I k UNDER 1 DAY ●.DATEDFmm* 7. :~nll&Arv -d .-m wInMsl MmElm ;Dw : Wwm OSV,YM?I
I I10,MAWALSIAtUS-Mmnid,%%21FRWVINGSFouss 12s. O+CADENT% USUAL 0CCUPA710N ltiWOOF -ESSflNDLISTRY
tinw Mmi8d. ~. InWrc.,hvmdnbnmDwlud (sAuiivI
fGi8wh+ldcFmf2awwa+slmw dwfkiw&cu@ Lu, *.1
I I I
1SS.RESIOHACE-SYA?E lilb. CDUFA?Y 1= m. TOWN,on LocAmoN 12s~ AFADWMGER
)Z* MEINoo OF c4smEmoN Sah FLAcsoFLss?osllx4N /kwat~. OaNmv. m a I.OCATION-CAV e Tmal. SE9W
❑ sulld 13cmmEs0n c1~fmms8Ltc
mtmlkbli a-ih+ddomh,iOsdFysswddm FIL mlnandTxAI”~ . I24. mME OF OEAYN 26. DATE ~DNDWCEO WAD IMalhDw.vur) 26. WAS CAGEFSFWIEO TO MEOICALSXAMINWCOWWR7
Mw- - ID/
27. w~L&wti ~,ww~ti ti_ti&ti. bw~ti&d~tia_umwMw-hek. OrnNIYfAlum. &L OnkmD-rnmdtliu.
niMsDLa7E CAuss mid IunJnare0r9mul + ,. IMuKq h dusll GUSTO m AS A CONSEWENCE OFII I
1
Smwnwiv ELFml-dsbl-n.II mm”. ISA-q 10h’armAm* CFWTOAGRASACONSEWEWEOFI: I
-. Enle Usm!sl.vmo ICAusEinbamub?+utv ~.LiuE Ilil!mod Owms ImdEhshtihlun
GIETOMASACWSEDUE?ECEOFkI
a?ART9. wlumOnmcm! cadnbmamuAwmsmdsmhM1—unNmlwm*m4slh+u -E&16 inFu L - WAS AN AU70UY - m AUTD?SY FwOINos
FE#omso? AVASASISFRW TO.#Ya * MA CGFM.STIONOF CAUSE
OF OEAIH? I% u w
132. REOLSTMR% SIGNAWTE Ss. DAYS wSO a4mm.Dw. Y-
E
Figusu1, U.S. Standmd Csriiibsta of Datls

Table 2. Observed numbars of deaths ●nd standardlzecf mortslity ratios (SMR) for selected occupational groups exhibiting excessmortality from malignant ●nd nonmalignant respiratory disease for males ●ged 20-64 year- Unked Ststes, 1950
A40kwny ilvm mal&tent Mnlmal@nentIBsp&stoly
~ oft~m dksnsa other thanbronchus, and lung kltluenza erldpmwrnnria
Gxl@aibnel group Oaa#s .SMR Deaths Sh4R
aarbers, etc . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Cooks,exeeptprivate hwseholct .,... . . . . . . . . . . . . . . . . . . . . . . . . . . .Machinistsand job setters . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Molders,melal . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Paintets(construatbn)opepetlmngera,end glazier%. . . . . . . . . . . . . . . . . . . .Tmdcabdrivarsendchautfeurs... . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .IAxwers,woodprod uats,elc . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Laborers,primaryrnatslindustries. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Laborers,transpxtatbn equipment. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Operatives,etc., plimelymelsl industrial . . . . . . . . . . . . . . . . . . . . . . . . . . .
9s
1:34
21277
414623077
*151’1651136%27’167‘1ss‘1s611s7!200~145
294166so643620492641
126’195125
%00%3’225154
125s14331195
‘SMRsignlfkdlystow 1~ u P <.01.‘[email protected] 100a!PC .0s.
SOURC13Gurswck,1W3S.
of races other than white whose usual occupation at thetime of their death was farmer or farm laborer. Theunderlined standardized mortality ratios (SMR’S) in the lasttwo columns represent significantly elevated risks for deathdue to specific causes. The set of tables presented in thereport by Guralnick identified specific causes of death aselevated in certain occupations and industries. Table 2 fromthe same study shows another use of these data. SMR’S fornonmalignant respiratory disease (basically chronic ob-structive pulmonary disease) and for malignant neoplasmsof the trachea, bronchus, and lung were highly related, fromwhich it was inferred that nonmalignant respiratory diseasewas probably an earlier indicator that might be used in amorbidity study to identi~ types of exposures.
Since the 1950 study, NCHS has undertaken no full-scxde national study, but a number of States, includingCalifornia, Rhode Island, Wisconsin, Washington, andPennsylvani~ have produced periodic studieq Wisconsinproduces annual data from death certificates. A survey ofStates in 1979, carried out by the Association of VitalRecords and Health StatistiW the voluntary organizationthat represents the interests of State vital registration offi-cials revealed that about a dozen States were codingoccupation and industry on the death certificate. Six ofthese States coded both occupation and industry, five codedoccupation only, and one coded industxy only. However, thedifferent States did not use the same coding system, result-ing in problems of comparability among State studies. Priorto 1979, no national standards or procedures existed forcoding or chissi&ing the cause of death from the deathcertificate.
At the same time, there was a growing interest inenvironmental and health issues. The NCHS (1977) report,“Statistics Needed for Determining the Effects of the Envi-ronment on Health,” discusses many of these interests. Theconvergence of interests and needs resulted in the cobbo-ration of a number of Federal agencies (including NCHS,NIOSH, NCI, and the U.S. Bureau of the Census) and theStates that has resulted in 32 States and the District ofColumbia coding occupation from data on the death certif-icates on a routine and uniform basis. The rapid growth in
14
the number of reporting areas that have adopted uniformcoding procedures for occupation and industry from thedeath certificate is shown in Table 3. The number of Statesthat are providing the data to NCHS is now 20.
Let me brief& summarize our achievements to date.
In 1978, with the U.S. Bureau of the Census andNIOSH, we conducted an evaluation study on thecompleteness of reporting and codability of the occu-pational information on the death certificate. We foundthat over 75 percent of the occupational entries in thesample of 5,000 records were codable (Rosenberg etal., 1979).In 1983, we published a handbook for funeral directorsto promote accurate and complete reporting of occu-pation and industry information on the death certifi-cate.In 19S4, an instruction manual was first produced byNCHS, IWOSH, and the U.S. Bureau of the Census foruniform coding of occupation and industry on thedeath certificates (NCHS, annual).NCHS currently does quality control coding for the 20States that submit coded occupational data to NCHS.In 19SS, we plan to publish the first periodic report onoccupational mortality as a supplement to the-NCHSpublication Monthly VW Statistics Rq.xwt. This willinclude data from about 270,000 deaths in 12 reportingStates.
Tabfe 9. Growth In number of reporting ●reas ●dopting uniformoeeup8tIon ●d Industry oodlng procedures
~dMnrSbwd sraes~
-=$- KHSwhm ~~ ~~M md~ bntwi?vars mms~
lea......... 11 0. . . . . . . . . : 13
;=,. . . . . . . .o
ao 16 51W6, . . . . . . . . 22 19 719s7 . . . . . . . . . 34 w 11

In a word, we have made considerable progress withthe program of occupational mortality data eollectio%which is now institutionalized in two out of eveg threeStates.
NCHShasbeen able to make this progress in large part&rough collaboration with NIOSH and NCIj who haveprovided funding for the fist steps. NCHS is giving a greatdeal of thought to the future of the occupational mortalityprogram. As part of our planning for fd year 1989, weare, in fact, doing a rather full review of this program. It isimperative that any request for new funds to carry forwardthe occupational mortality program must be made onlyafter a careful review of the needs of the States for the datqthe uses to which it will be put, and the various options forits collection. We hope that with your assistance, we eanexplore these issues and provide a solid basis for developingNCHS’ plans for occupational mortality.
References
Centers for Disease Control. 1983. Leadingwork-mkted diseasesand injuries,United States.Modidify and M&afity Weekly Repcm.Vol.32, No. 2.
Guralni~ L. 1962, Mortalityby occupationand industry amongmen 20 to 64 years of a~ United Stat+ 1950. Hral Stathtics—S’cial Repons, Vol. 53, No. 2. WashingtoIXU.S. GovemxnentPrinting Office.
Guralnick, L. 1963a. Mortality by occupation and cause of deathamong men 20 to 64 years of age: United State+ 1950. 14tolStatistics-Special Rep&, Vol. 53, No. 3. WashingtoIXU.S. Gov-ernment Printing Office.
Gumlnic~ L. 1963b. Mortality by industry and cause of deathamong men 20 to 64 years of agex United States, 1950. VilalStatistks-Spcia fRepmts, Vol. 53, No. 4. WashingtorxU.S. Gov-ernment Printing Office.
~ L. 1963c. Mortality by occupation level and cause ofdeath amongmen 20 to 64 years of age United State+ 1950.KralStatistks-Speaaf R- vol.53, No. 5. Washington U.S. Gov-ernmentPrintingOffice.
Kaminski,R,, J. Brocke~ J. Sestito, and T. Frazier. 1981. Occu-pational information on death certificates A survey of Statepraetiees.Anz L Pubfic He& 71(5)KL89.
IG@nski, R, and R spirttm 1980. Ihdwttial Chmctenkics ofPeKons Reptxiing Mdidity Dwing theHealth Intem”ew SurveysC2mduc&d in i?k%U974:An E@onatay Review. DHHS Pub. No.(NIOSH) 80-123.Washington U.S. Government Printing Office.
Kitsgaw E. M., and P. M. Hauser. 1973.DiffmnfiafMomlity inthe United Stores. Cambridge, Mass Harvard UniversityPress.
National Center for Health Statistics. 1977. Statistics needed fordetermining the effects of the environment on health. Report ofthe Tedmical Consultant Panel to the United States NationalCommittee on Vital and Health Statistics. Wtaland Health Starktics. Series 4, No. 20. DHEW Pub. No. (PHS) 79-1457. PublicHealth Serviee.Washington: U.S. Government Printing Office.
National Center for Health Statistics. (Annual). Indumy andOccupation C2xiing for Death Certificates. NCHS IhstrwtionManr@ Par W. HyattsviUe,Md.
Rosenbexg H. M., D. Burnham, R Spirtas, and V. Valdisera.1979.Occupation and industry information horn the &ath eertif-icatex Assessment of the completenem of reporting. StatisticalUses of Ahinisbndve Records w-h Emphasis on Mortality andDisabifi~ l?ese~ edited by De@ B. L., and F. scheluren, U.S.Department of Health, Education, and Welfare, social SecurityAdministration, Officeof Policy,Office of Research and Statistics.Washington U.S. Government Printing Office.
Rosenber& H. M., and M. Feirdeib. 1986. Data bases for theanalysisof socioecmomic differences in mortality in the UnitedStates. Pmceedhgs of the Ztiemadonaf Seminar onSocio—Eeononw“ Aspects of Differential Mcxtafity. Zaraardi,Hungary.
15

Utah’s experience in building anoccupational health surveillanceprogramby John E. Brockert, Direetor, Bureau ofHealth Statistics, Utah Department of Health
The initial impetus for the development of an occupa-tional health program in Utah occurred in 1978 because ofthe interest of Mark Nichols, M.D., then the Director of theChronic Disease Program. The Chronic Disease Programprovided resources for the manual translation of occupa-tion from the death certificate to a listing of all deaths ofmales 16 through 65 years of age, for the period 1959-68.That experience demonstrated the extensive amount ofwork involved in coding and keying occupation from thedeath certificate. However, the results of that analysis dididentify a population potentially at high risk for myocardialinfarction, employed in the rocket industries located inUtah. These results were reported in a master’s thesis byDr. Nichols.
In 1980 the National Institute for Occupational Safetyand Health (NIOSH) announced the Surveillance Cooper-ative Agreements between NIOSH and the States(SCANS) projects and the staff in the Bureau of HealthStatistics realized they had a great advantage to competefor one of these contracts. The Director of Health Statisticswas eoncemed that Federal funding might be obtainti, andthen after 2 years, the Department would either have to goto the legislature for State funding or drop the program.That concern was expressed to the Administration of theDepartment, and the response was to apply for the contractfunds and worry about additional timding later. The Utahproposal was one of six proposals that were subsequentlyfunded through the first SCANS awards by NIOSH.
The Occupational Health Program efforts by the Bu-reau of Health Statistics were particularly productive dur-ing the next 2 years. We successfully coded the occupationand industry for all death certificates on file from 1957through 1980. This was in excess of 150,000 deaths. Wewere also successful in doing some preliminary coding ofoccupation on the birtheertifieates. Proportionate mortal-ity ratios (PMR’s) were prepared for 85 cause-of-deathcategories and 85 occupation or industry categories. Aseries of technical reports was prepared on coal miners,farm workers, and wood workers in Utah that utilized thePMR’s available from this large resource.
Several meetings were held with interested users fromthe University of Utah, the Rocky Mountain Center forOccupational and Environmental Health, the Utah StateUniversity, the State Industrial Commission, and from Dr.Mark Nichols (now director of a local health department).There was widespread support and encouragement forfurther analysis and publication of occupational healthdata. The report on lung disease mortality in Utah minerswas printed in Utah Science, published by the Utah Agri-cultural Experiment Station at Utah State University. TWOadditional reports were presented, and they are part of theproceedings of two national scientific meeting.
The Department of Health continued to be interestedin the occupational health program and, subsequently,allocated resources to obtain an occupational health epide-miologist. A member of the department staff, RichardJohns, M.D., was assigned to head up the department’sepidemiology programs. He hired Dennis Perrott~ Ph.D.,to work with him as an occupational health epidemiologist.Subsequently, Dr. Johns left employment with the Depart-ment of Health to complete post-doctoral studies in occu-pational health. Dr. Perrotta continued to be active inoccupational health epidemiology with the department untilOctober 1986, when he transferred to a similar program inthe Texas Department of Health. While still in Utah, hewas the recipient of a 1984 NIOSH contract to study theeffect of anesthetic gas on reproductive outmmes of medi-cal personnel.
The Bureau of Health Statistics was also a recipient ofa 1984 NIOSH contract to study occupational injuries inUtah. This contract continued to build on the work that wasalready completed, extending it to include mortality datafor 1981-84. Under this contract, we successfully linked theinjury information from the Industrial Commission withour mortality files. This analysis provides preliminary con-firmation that there were workers who were injury prone.They appeared in the Industrial Commission injury files onmultiple occasions, and they had a higher probability ofbeing linked with the Utah mortality file of deaths due toinjuries than persons who appeared in the injury file onlyonce.
Starting in 1984, Utah was one of the States to contractwith NCHS for the provision of current mortality datacoded for occupation and indust~. That eontraet was toprovide 1985 dat~ and, subsequently, it has been renewedfor 1986 data. We have also been successful in reeentlycompleting the coding for 1984, and we will shortly beproviding NCHS with that data tape.
With funding from the original SCANS contract, Utahhas been developing an automated dictionary of occupationand industry titles and codes. Currently, we have about25,000 linked occupation and industry titles and codes inour automated dictionary. Since 1978, we have keyed theliteral entry for occupation and industry on all death certif-icates. Monthly, the keyed Iiterals are matched with thedictionary. Currently, we are getting a 60-percent match.The balsnee are coded manually by our coding staff. Thecodes are keyed, and the monthly death file is updated. Theautomated dictionary is also updated.
Utah has approximately 800 deaths per month, and it isable to complete the occupation and industry coding andkeying for a total cost of $500.00 per month. This includesall of the activities deseribed above.
I believe the sueeess in the development of the UtahOccupational Health Surveillance Program has been atleast partially the result of our willingness to involve otherparts of the department and other agencies outside thedepartment in our efforts. It is seen as a broad-rangeprogram that will improve the health of Utah’s workers byreducing injuries and illness that are occupationally related.
16

Chapter Il.Review of options forproducing occupationalmortality data
The second session of the Workshop was devoted to areview of 10 options for producing occupational mortalitydata, focusing in particular on the existing system used bythe National Center for Health Statistics (NCHS). Theseoptions (summarized in table 4) were suggested in discus-sions with several Workshop planners and participants inpreparation for the Workshop. They were presented at theWorkshop by representatives of the sponsoring agencies,but they did not necessarily reflect the priorities of thoseagencies.
The session was introduced by John E. Patterson,Director, Division of Vital Statistics (DVS), National Cen-ter for Health Statistics. DVS operates the national vitalstatistics program with the States under an administrativearrangement called the Vital Statistics Cooperative Pro-gram (VSCP). Data from vital records filed in the Statesare sent on data tapes to NCHS for consolidation into thenational vital statistics data base, which includes births,marriages, divorces, fetal deaths, abortions, mid deaths.Beginning in 1984, coded occupational and industry datahave been sent by some States, now numbering 20, toNCHS along with other coded mortality information. Amore detailed description of this program is given later asOption No. 1. Other options that were considered by theindividual working groups and the Workshop as a whole inplenary session are also described. All of the cost estimatesdiscussed in Option Nos. 1-10 are expressed in 1986 dol-lars.
Option No. 1. Existing system:Occupational mortality coding atthe National Center for HealthStatistics for 20 States (Annual)
Presented by Harry M. Rosenberg, NationalCenter for Health Statistics
Description
The purpose of this project, which is a collaborativeactivity of NCHS, the National Institute for OccupationalSafc[y and Health (NIOSH), and the National CancerInstitute (NCI), is to develop a data system—within thecontext of VSCP—that can produce on a routine basisoccupational mortality data from the death certificate.
The death certificate asks for the usual occupation andindustry of the decedent. This information can be readily
coded using the existing coding and classification systemdeveloped jointly by NCHS, NIOSH, and the U.S. Bureauof the Census. The system is based on State utilization ofcommon coding procedures promulgated by NCHS and onState acceptance of NCHS quality control standards forcoding. The system was initiated during 1978-79, when aspecial study was undertaken by the U.S. Bureau of theCensus for NCHS to evaluate the codability from the deathcertificate of the usual occupation and the usual business orindustry of decedent (Rosenberg et al., 1979).
As of 1987, this VSCP approach was well institutional-ized. A total of 32 States and the District of Columbia codethis information from the death certificate, with partialsupport to 11 States from the participating agencies. A totalof 20 of the 32 States are sending their coded data, includ-ing usual industry and occupation, to NCHS for qualitycontrol and for incorporation into the multi-State database, which includes other routinely coded demographicand medical information available for all other deaths inthe coded death records (including underlying and multiplecauses of death). Seed money for this program has beenprimarily available on a reimbursable basis from NIOSHand NCI. The substantial NCI contribution will end withfiscal year 1988, at which time NCHS has indicated that itwill attempt to obtain appropriated funds to continue andexpand the program.
Uses
Occupational information from the death certificate isone of the most accessible, routinely available, and geo-graphically comparable sources of data for measuring oc-cupational health effects over time and across geographicareas. It can be used to identify possible problem areas(geographic or occupational), to generate hypotheses, andto monitor change over time. The usefulness of the vitalstatistics files for occupational health studies has beendemonstrated over the years in the decennial reports ofGreat Britain, in periodic reports for a number of Sta[cs(for example, California, Pennsylvania, Wisconsin, Wash-ington, and Rhode Island), and the United States in 1950.Measures of risk based on the VSCP approach can includestandardized mortality ratios (SMR’S), at least on a decen-nial basis but possibly on an annual basis. In the absence ofpopulation data, measures of relative risk (for example,proportionate mortality ratios, or PMR’s) can be used.
17

Tabfe 4. Synopsis of options
CanCa; analysk
Number of analyWs be done byFederal racorw be 00rre by detailed
Average cost~r number of Stalistlcal detailed i/O causes of ConfiderrtL31ifyOplbn annual cod Ferbdwfy dealh deaths measures codes? death? an issue? Comments
Existklgsystem
Annual f/O coding for all States
f/O codfng fc+ all Stales for yearsafound decennlai sensus
Annual data for subset of causesand/cf Subsd of stares
Mofltdfly Folfowbask Survey
Fdfowup C4NHANES Ill for 10 years
Fofbwup of 3 consecutive yearsC4NHIS fw 10 years
U= Natbnal Infant and MalematHealth Survey
Use Nalbnal Longiiudual Morfalttystudy
Use Annual Survey (BLS)
$B91,000f(NCHS
$294,m)
$3,850,000’(NCHS
$I,450,0(N))
$4.4-7.42mfllkxr(NCHS$4.4-724mlllbn)
Varfabfe
$2&&rr
$wXX3\
S803,0004
$1.30
$0.75
S220-3.70
285,0001285,G00
PMR
PMR
PMR, SMR
PMR
PMR, reles
SMR,
Yes Yes
Yes
Yes
No Provides for small aree analysis for reportingareas Iimlled in coverage
1.
2
3.
4.
5.
6a
b.
7.
8.
9a.
2,000,000/2,000,CO0
Yes
Yes
Selwted 1/0codes
No
No
Yes
No
Yes
Induslryonly
Yes
No Maximizes stahstical power, geographkcoverage, and depth of 1/0 and cause ofdeath analysis
Doss not allow for development of ongoingstale programs
Annual
Pertcensal(for
3 yearsevery 10years)
Annuaf
Every 5yeara
1968-1994,folknved
for 10yeare
3 years,folfowed
for 10yeara
4 yearsuNeyparbd
1979-1961
6J300,000/6,000,1M0
No
Varfabfe No
No
Lower costs, limited analysis depending onprogram design
Analysis for detail dependent on surveydeskgn; no small area analysis
$90
$2,870
$37
$53
$40
$9
$9
$.0GQ3
20,000120,000
No
No28,000/2,600
Yes 12denstve examinalbn findings useful foranalylic sludies and prevalence estimates. .
based
$123,00@ Perhaps330,000/33JIO0
Yes
“i)asad
$132,5006 20,000/1o,ooo
PMR
SMR
Rates,counls
Counls
SMR
Perhaps Yes POlenlial use for reproductive hazardexposures
$2,800,DO07 1,ooo,ooo/55,0Q0
No
Yes
Yea
No
Morlallly differentials by Industty andoccupation for current job and usual industryand occupalbn from dealh carffiicate
Limited by coverage.$2,500,0000 2,800,000employeral
1,562 In1EJ85
Variable/1,179in 10 Slates
k-r1983
31,000,fxro/
Fatalityevent orsource
$2,0C0,0000 Fatalievent or
Limited by coverage and lack of populatbnbase
Excellent for geographic and time trendsurveillance by underlying cause of death
b. Use SDS (8LS)
source
$IO$XKW10.useofcompressedMorirdHyFMe
1986-63 No Yes31 JXX3,000
%cbdss Sfab costs.z~tis m stale chsrgesto NCHS forpurchasingdaeth cerflflcsdas.%s!s stfrltslsd10 owpationsl fxxtion of smey.41m~ em ~ts f~ -paiim corrpnd s4metd $S,00J,OOO d $2S,rXKl NCi ah.
%cbdss S9C0,0W inter+w costs for 3 yearsforcccufdonsl ccmponsrdsndS?30,000 NU mslsfor 10years.%30d onestimatedsurvsycosf of S480,0Wover4 yews foroccupslio+-rslcorqmmnt plus$50,0G0forW =dIng.7ESIiMSlSdccds per deslhbssed on 1972-19SSSSIWr’sS.%udescustsofwccesshofbc4 hfalalsndrro rMalcases.424s forfXocessir@falslCssesare notavailabrssaparar.siyfromnorialslcmes.%tknsted ~sd~ d sacorzderydstacOIlOctiOnC051S.

costs
The projected cost of the program is as follows
. If the program were to continue at the present level (11States), the pass-through funding requirement for FY1989 would be about $176,000.
● If the program were to be expanded to the 20 Statescurrently sending data to NCHS, it would require anestimated $375,000.
These figures represent only the Federal support to theStates for coding their data. The additional cost to NCHSfor processing, analyzing, and publishing these data isestimated to be about $118,000 annually, bringing the totalNCHS cost to $294,000 annually for program continuationat the present level (table 4). For NIOSH, the cost is about$45,000 annually. Further, the States incur a cost estimatedto be about twice that for which NCHS reimburses them.Altogether, then, the per record Federal cost of the existingapproach to fund 11 States is about $1.30. The per recordcost, including the State share, is $2.60. The cost of Statecoding might ultimately be reduced somewhat if automatedcoding of occupation and industV, being investigated by theU.S. Bureau of the Census for the 19Xl Census, proves costeffective.
Advantagesand disadvantages
Option No. 1, the existing system, is on line andworking effectively in 32 States, of which 20 States aresending NCHS data on a routine basis for inclusion on datatapes and reports, the first report of which will be producedin 1988. The data are produced as an integral part of theongoing vital statistics system at the State and Federallevelq neither technical nor administrative problems havebeen encountered that have not been overcome in a routinefashion. Option No. 1 can provide for the full range ofoccupation and cause-of-death detail for areas as small ascounties and for State% a distinct advantage where surveil-lance is sought for detailed occupations and for small@graphic areas. Second, all death certificates within theseStates are covered, not just a sample of deaths. And, third,as a State-based system, this approach can be used by theStates in support of State-administered occupational healthprograms.
An advantage of the State-based approach is thatquestionable information reported on the death certificatecan be queried by the State vital statistics offices, much asother questionable entries are often queried as part of theregular vital statistics program at the State level. Queryingat the national level is no longer possible because theFederal Government is not a repository of actual deathcertificates, which are fikxl in the States, nor does it rou-tinely receive copies of certificates. Increasingly, State vitalstatistics offices are making preceded information availableto NCHS on data tapes. NCHS has copies of only a smallnumber of records that are independently coded eachmonth for quality control purposes, as well as an additional10-percent sample of records used by NCHS to produce
current estimates of mortality by cause of death, publishedin the NCHS Monthly Htal Stah”sticsRepoz
A further advantage of Option No. 1 is that it isrelatively inexpensive per record, even when compared withOption No. 3, which is a special study around the time ofthe decenm”rdcensus.
The disadvantages of the system are related to devel-oping meaningful measures of risk. In particular, the ab-sence of denominator data on a routine and continuingbasis can present a problem. Even with census-based datrqthere are differences between the nature of the occupa-tional information collected through the vital statistics sys-tem and that collected by means of censuses and sumeyxthe death certificate asks for “usual occupation” whereasthe Census asks for “current occupation.” The absence ofannual denominator data means that reliance for measuresof risk has to be placed on frequencies or PMR’s, which inmany cases may serve well. Another disadvantage is thepresent limited number of States that participate. TheseStates may not be representative of the United States as awhole or even of areas with occupational mortality patternsthat merit attention.
Questionsand Answers
During the brief question-and-answer period, the fol-lowing points were made
. The coverage of the ongoing system, with participationof 20 States, includes about 584,000 death records peryear, or 28 percent of all U.S. deaths annually.
● The participating States are coding occupation andindustry on all records that report this information, thatis, there is no arbitrary age cutoff.
● Quality control on medical items and on demographicitems, including occupation and industry, is carried outon a continuous basis by NCHS by coding a sample ofrecords monthly that NCHS receives from the Statesand by comparing the NCHS-assigned codes with thosesent to NCHS by the States. If the State coding doesnot achieve a pre-established level of quality, the batchof records that the sample represents has to be recudedby the State.
Option No. 2. Expanding theexisting system to all States(Annual)
f?resented by Harry M. Rosenberg, NationalCenter for Health Statistics
Description
Option No. 2 is similar to Option No. 1 except thatcoverage would be rapidly expanded to include all 54registration areas (that is, all States, the District ofColumbia, Puerto Rico, Guam, and the Virgin Islands),rather than the estimated 20 States in the program for1987.
19

Uses
Occupational information from the death certificate isone of the most accessible, routinely available, and geo-maphically comparable sources of data for measuring oc-.cupational health effects over time and across geographicareas. It & be used to identify possible problem areas(geographic or occupational), to generate hypotheses, andto monitor changes over time.
costs
The estimated annual Federal support to the Statesunder this approach is $1.2 million. The additional cost tothe Federal Government for processing, analyzing, andpublishing these data is estimated to be about $250,000.Further, the States incur a cost estimated to be about Wicethat for which NCHS reimburses them. The per recordFederal cost is estimated to be about $.75 and $1.90 for thetotal cost (table 4), including the State share.
Advantages and disadvantages
The advantages of national coverage are the ability toproduce national counts of deaths by occupation and indus-try and, in contrast to the 1950 national study (GuralnicR1962, 1963a, 1963b, 1963c), there would be a sufh~ient]ylarge number of cases to provide estimates of occupationalmortality for detailed occupations and causes of death. Alarger data base also would permit occupational mortali~analysis for small geographic areas.
Option No. 2 has all the advantages cited for OptionNo. 1. It is State based, and thus it can tie into occupationalhealth programs at the State level. It can have a queryingcomponent at the State level to improve quality. Further, asa larger data base, it can provide estimates and measures ofgreater statistical reliability and it can provide a samplingframe for followback surveys,
Disadvantages are related to the absence of denomina-tor data except for census years, although some limitedpopulation estimates by occupation and industry are avail-able from the Current Population Survey, conductedmonthly by the U.S. Bureau of the Census. Another disad-vantage of Option No. 2 is the cost, about $1.4 millionannually. However, this cost is not considerable by compar-ison with some other Federal data collection activities.
Questions and answers
A question was raised regarding the quality of theinformation reported on the death certificate. In his answer,Dr. Rosenberg stated that the demographic information onthe decedent is supplied by the funeral director based oninformation from an informant, often a family member.What is known about the quality of this information islargely from special studies, including a 1960 NCHS studythat compared vital record information (excluding occupa-tion and industry) with census information for the sameindividuals (NCHS, 1969). Similar comparisons were madein the 1950 national occupational mortality study producedby the National Office of Vital Statistic& the predecessor
20
agency to NCHS (Guralnick, 1962, 1963a, 1963b, 1963c).In the 1950 study, individual death certificates werematched with census records for the same individuals; andcomparisons were made of the occupation and industry ofthe decedent, as reported on each record. Those resultsshowed a generally good correspondence, despite the dif-ferent types of questions asked on the two sources, but alower match rate on an individual record-by-record basis.Another approach to studying the validity of information onthe death certificate is the followback survey (see OptionNo. 5).
Option No. 3. Data for all States incensus years only
Presented by Harry M. Rosenberg, NationalCenter for Health Statistics
Description
An alternative to the VSCP approach of Option Nos. 1and 2 would be to produce national occupational mortalitydata once every 10 year% the approach used for manydecades in Great Britain. This approach was used in theUnited States for 1950, though the coverage of the U.S.study excluded females. By focusing on the 3-year periodaround the 1990 census (that is, 1989-91), such a studycould take advantage—as did the 1950 study—of denomi-nator information from the 1990 Census of Population. Byadding together the 3 years of mortality data, numeratorinformation would include more cases and would thereforehave greater statistical stability and reliability, which wouldallow for more detailed geographic and occupational anal-ysis than a single calendar year of data. Occupational datafrom the death certificate could be coded either at NCHSby the existing trained coding staff or under contract by theU.S. Bureau of the Census. The latter was done in a 1979NCHS pilot study on the quality of occupational data on thedeath certificate (Rosenberg et al., 1979).
Uses
Occupational information from the death certificate isone of the most accessible, routinely available, and geo-graphically comparable sources of data for measuring oc-cupational health effects across geographic areas. It can beused to identify problem areas (geographic and occupation-al) and to generate hypotheses.
costs
The costs of producing occupational mortali~ dataunder Option No. 3 would be high. Although it wouldappear that the cost would be a simple multiple of theannual cost under Option No. 2, there is an additionalsubstantial cost because, in a once-a-decade study, onecould not depend on States doing the coding as underOption Nos. 1 and 2. It is believed that States would beunwilling and unable to participate in a data program thatoperates for only 1, 2, or 3 years in a decade. States prefer

to operate a continuous system, like the vital recordssystem, m“th constant processing. In contrast, under OptionNo. 3, the coding would have to be handled in an entirelydifferent way, either by contracting coding out to an expe-rienced Federal organization, like the U.S. Bureau of theC&w or to a private organization. This would probablycost more per annum than an establishe~ ongoing Statesystem.
In addition, it would be necessary to purchase deathcertificates from Stat+ an estimated $1.50 to $3.00 perrecord. Therefore, for the estimated 6 million deaths duringtie 3-year period, an additional cost of $9-$18 million forrecords and $4 million for coding would bring the perrecord cost to $2.20 to $3.70 (table 4).
Advantages and disadvantages
The principal advantage of this approach, like that ofOption No. 2, is having a large number of cases for detailedgeographic and occupational mortality analysis. The disad-vantages are that it does not develop a State capacity tocode occupation and industry or to query records that cotddenhance the quality of reporting or promote better report-ing by funeral directors through training. It also abandonsthe idea of occupational surveillance on a continuing basisand the possibility of relating occupational health sumeil-lance at the State kvel with occupational health programsadministered by the States. A formidable obstacle to thisapproach is the cost, which was understated in a recentCongressional report (the Weiss report) that suggested thisas a feasible and desirable option (U.S. Congress, 1986).Under Option Nos. 1 and 2, the States absorb two-thirds ofthe production costs under Option No. 3, they do not.
Option No. 4. Subsets of causes orsubsets of States (Annual)
Presented by Harry M. Rosenberg, NationalCenter for Health Statistics
Description
Under this option, only selected death certificateswould be coded for occupation and indust~. The selectioncould be made on the basis of cause of death, such ascancers or accidents, or on the basis of geographic areas,such as States with cancer registries.
Uses
Occupational information from the death certificate isone of the most accessible, routinely available, and geo-graphically u)mparable sources of data for measuring oc-cupational health effects over time and across geographicareas. It can be used to identify possible problem areas(geographic or occupational), to generate hypotheses, andto monitor changes over time.
costs
The per record costs are estimated to be about thesame as in Option No. 1, unless records have to be pur-chased from the States.
Advantages and disadvantages
The advantage of this approach is cost reductionsroughly in proportion to the reduced number of recordsfrom Option Nos. 1 and 2. However, a major disadvantageof this approach is that it would have to rely on post-stratification. That is the national mortality data wouldhave to be processed annually by NCHS in cooperationwith the States as it does now. After the data are pro-cessed, the sample of remrds, based on cause of death orState, would be selected and separately coded for occupa-tion and industry, either by the States or by a third party. Asa two-stage process, it would be cumbersome comparedwith Option Nos. 1 and 2, where occupation and industryare coded on line with other items. Dr. Walker earlierraised the excellent question of who would decide whichareas would be included among the representative areas.
OptionNo. 5. MortalityfollowbacksurveysPresentedby Gail S. Poe, National Center forHealth Statistics.
Description
The mortality followback survey method is a #owerfulone and can be used to accomplish many objectives. Targetgroups, such as persons dying from certain types of cancer,can be oversampled for epidemiologic investigations. Fur-thermore, historic information can be captured, such aswhether the decedent worked at any time for a particulartype of industry or was exposed to certain types of sub-stances.
NCHS is currently sponsoring a major national follow-back smvey–the 1986 National Mortality Followback Sur-vey (NMFS). In this survey, a sample of 18JO0 deathcertificates of persons aged 25 years and over who died inthe United States in 1986 was selected. A next of kinidentified on the death certificate or some other knowl-edgeable person will serve as the respondent. The survey isdesigned to supplement the information on the death cer-tificate. Additional questions are asked about usual occu-pation, indust~, family income, and education. Othermajor topics are the use of health care resources in the lastyear of life, disability prior to death, and health habits, suchas smoking and drinking alcoholic beverages. The surveyhas a number of sponsors, including NCHS; the HealthCare Financing Administration; the National Cancer Insti-tute; the National Heart, Lung and Blood Institutq theNational Institute of Child Health and Human Develop-ment the Indian Health Servicq the Alcohol, Drug Abuse,and Mental Health Administration, the National Instituteon Aging, and the Veterans Administration.
21

A major purpose of the 1986NMFS was to examinethe reliability of items reported on the death certificate bycomparing these items with the same items reported by thesurvey respondent. Items that will be compared includeage, race, and veteran status. The present survey is alsobeing used to examine the reliability of occupation andindustry reported on death certificates. Considerable de-bate focused on the types of questions to be asked aboutoccupation and industry. Initially, consideration was givento asking adaptations of the questions used on several othermajor national surveys, including the Current PopulationSurvey; but, to save time and to more closely parallel thedeath certificate items, the number of questions on occupa-tion was limited to two. About 5 percent of the originalrespondents are reinterviewed within 2 weeks of the origi-nal interview and asked a set of five additional questions onoccupation and industry related to the job longest held.With two sets of questions, possible comparisons can bemade to the information on the death certificate and to theinformation obtained from the more traditional surveys ofemployment and the labor force, An additional feature ofthe 1986 survey was that the 1986 National Health Inter-view Survey (NHIS) provided information relevant to theestimation of denominator data. The 1986 NHIS includedquestions on the longest held occupation and industry thatcomplement those in the NMFS.
Instead of using the final mortali~ file of all deaths inthe United States as a sampling frame, the 10-percentnational sample of deaths, called the “Current MortalitySample: was used in the 1986 survey. This file is used byNCHS to produce current cause-of-death estimates for theUnited States on a monthly basis, published in the Month/jMta/ Std.stiesReport,in contrast to the final mortality file,which is not available until about 20 months after thecalendar year of occurrence. Past followback surveys haveunderscored the importance of using the most currentmortality file to reach persons familiar with the decedentbecause death is often followed by family dissolution andrelocation that make followup difficult.
With the followback surveys, it is possibleto oversim-ple certain groups who would ordinarily be represented byvery small proportions of national sample. The 1986 survey,for example, included oversampling of younger persons,black persons, American Indians, and persons dying fromselected causes, including ischemic heart disease and se-lected cancers.
The survey is conducted by sending out questionnairesabout 6 to 8 months after the death. If there was noresponse after two mailings of the questionnaires, informa-tion was obtained either by telephone or personal visit. The1986 survey was conducted by the U.S. Bureau of theCensus under contract with NCHS.
The 1986 NMFS contained 158 response items thatrequired approximately 30 minutes to administer. The sam-ple design was totally uncluttered, resulting in increasedinterviewer travel costs for those interviews that cannot beobtained by mail or by telephone.
Uses
Mortality followback surveys can provide informationon industry and occupational exposure and on other vari-ables to supplement cause-of-death information obtainedfrom the death certificate. These surveys can be used forhypothesis-generating or hypothesis-testing studies relatedto risk factors ascertained from responses to the question-naire.
costs
The total field cost includes forms design, interviewingmanagement of data collection, quality control, data keying,and computer edits. For a survey focusing only on occupa-tion and industry, the costs would be approximately $90 percase, assuming 20,000 cases, with a response of at least 90percent over a 5-year period (table 4).
Advantages and disadvantages
Some advantages of the followback technique includethe ability to use extensive questioning to better measuredesired concepts; oversimple certain demographic and oc-cupational groups or causes of death; collect historic infor-mation on a decedent’s work history, for example, ratherthan relying only on a single question of usual occupation;and have probing questions about exposure to hazardoussubstances on the job.
Among the disadvantages of the followback method foroccupational mortality studies are that it is not linked togeneral population surveys; the sample is generally toosmall to provide information for occupational mortalityanalysis unless specifically designed for that purpose; andthe sample is too small for geographic analysis of smallareas. Because of the periodicity and geographic coverageproblems associated with such followback surveys, this isnot a technique for surveillance.
Questions and answers
Discussion after the presentation covered thefollowing
Ms. Poe estimated that response rates of the presentsurvey would be at least 90 percent, based on anunweighed response rate of 89 percent from returns ofthe first quarter.Costs per agency go down when the survey servesmultiple purposes rather than having a single focusbecause of multiple agency sponsorship.Responses on these occupational and industry itemshave been very complete, in contrast to the expressedconcern that incomplete reporting of occupation andindustry would result because an informant, ratherthan the person who is the focus of the questions,responded to the survey.
22

. There was a question as to whether validation ofresponses with information from the Social SecurityAdministration could be done, to which Ms. Poe indi-cated that this might not be possible because of confi-dentiality considerations.
OptionNo. 6. Followupof generalpopulationsurveysusingtheNationalDeath IndexPresented by Bruce Cohen andJeffrey Maurer, National Center for HealthStatistics
Description
TWo major population surveys sponsored by NCHS–the National Health Interview Smvey (NHIS) and theNational Health and Nutrition 12mnination Survey
~)–wdd be used for occupational surveillanceand research. The purpose of NHIS is to provide nationaldata on the incidence of acute illness and injuri~ theprevalence of chronic conditions and impairment% theextent of disability, the utilization of health care servi~and other health-related characteristics. Each calendar yeardata are collected from approximately 50,000 households,yielding about 135,000 persons. In addition to the standardquestions that are asked every year, special questionnaireson current health topics are added each year. For instance,information will be collected during the 1988 survey onlongest job and symptoms of occupationally relatedconditions.
Information is collected during NHANES on a nationalsample through physical examination, clinical and labora-tory tests, and related measurement procedures as well asquestionnaires. Prevalence data are collected for specifi-cally defined diseases or conditions of ill healtly and nor-mative health-related data are collected that show totalpopulation distributions of particular characteristics, suchas visual acuity, pulmonary function, or blood pressure. InNHANESI, 14,407 adultswere examined; the NHANESHI survey (whichwillbegin in 1988) will yield examinationsof approximately 28,000 adults.
Uses
Questions about current and longestjob and symptomsof occupationally related illness (and direct examinationfindings in NHANES) make these surveys potentially use-ful for occupational research. Certainly, they can yieldnormative data for comparison with specific studies per-formed by others. The possibility also exists to link therespondents with later death certificates using the NationalDeath Index (NIX) in order to examine mortality by occu-pation and industry. In fact, searches of mortality recordshave yielded over 2,000 deaths for the NHANES I cohortas part of the NHAN123 I Epidemiologic Followup Study.For these, questions in the followup included occupationlongest held. Other occupational information includes re-sults of rereading x-rays, which have revealed some evi-
dence of asbestosis. For the NHANES IrI study, anestimated 10 percent of the effort will be related to occu-pation.
A possible scenario for using NHIS would be to gatherbasic industry and occupation information on longest jobfor a 3-year period (perhaps supplemented by additionalquestionnaire information) and then follow thii cohortusing the NDI for a lo-year period. Followup of th~ sampleeventually would yield over 30,0(XIdeaths.
Both NHANES and NHIS could be developed toroutinely include longitudinal efforts such as the NHANESI Epidemiologic Followup Study, which is a longitudinalreintewiew with the NHANES I adult cohort originallyexamined from 1971 through 1974. Longitudinal designswould expand the capabilities of these surveys to collectoccupational information. In both instances, the number ofcases would be relatively small for detailed occupation andindustry analysi~ the NHIS would have a larger number ofcases ultimately ascertained by the NIX, but would includeno examination data.
costs
Assuming a 10-year period of followup of NHANESIII using the NIX, resulting in about 2,800 deaths identifiedover that period, the estimated cost (including the examcosts) per ascertained case would be about $2,870 (table 4).An alternative approach would follow up the NHIS samplesat 110,000 a year for 3 consecutive year& this would resultin a larger database, about 33,000 deaths identified over 10years, for analysis and a lower cost, an estimated $37 percase.
Advantages and disadvantages
The advantages of this approach are the availability ofdetailed measures of covariables, symptoms, and examina-tion findings; the potential for questioning indtilduals di-rectly for exposure information and morbidity histo~, andthe potential for longitudinal followup. The disadvantagesinclude small sample sizes that cannot support detailedanalysis and suweillance activities by occupation or industryfor specific causes of death or small geographic areas.
OptionNo. 7. Followupof targetedNationalCenter for HealthStatisticssurveys
Presented by Bruce Cohen, National Centerfor Health Statistics
Description
In addition to the NHIS and NHANES programs,NCHS performs several surveys aimed at specific popula-tions, two of which—the National Survey of Family Growth(NSFG) and the National Maternal and Infant HealthSurvey (NMIHS)-may be useful for occupationalresearch.
23

Cycle IV of the NSFG was scheduled to start in May1987. (Editor’s note The revised date for implementinghis cycle is early 1988.) This sample of approximately12,000women was originally interviewed in the 1986 NHIS.f’he survey will include interviews with a national sample ofwomen 15-44 years of age, regardless of marital status or>regnancy history. They will be interviewed in person. Thenterviews will include the woman’s marital history, preg-lancy history, contraceptive history, data on social and;conomic characteristics, and such risk factors as smoking,.lrinking, pelvic inflammatory disease, and certain sexuallyransmitted diseases.
Information will be collected for the current or most-ecent occupation and industry of employment for the.voman (and her husband if she is married). Occupationallata will be coded according to the 3-digit U.S. Bureau of.he Census classification. Information regarding infertility,reproductive patterns, and birth intervals will be availablehat can be assessed by employment patterns and laborforce participation. The NSFG currently includes somequestions requested by BLS that pertain to employer con-tribution to maternity benefits.
The 1988 NMIHS will be equivalent to the threesurveys that were previously conducted separately—theNational Natality, Fetal Mortality, and Infant MortalityFollowback Surveys-with information collected for threenational samples of vital recorcls: 10,000 live births, 4,000fetal deaths, and 6,000 infant deaths. Thus, a total of 20,000.leliveries will be surveyed to include information obtainedfrom the mothers, hospitals, and medical attendants. It willDe possible to corroborate information obtained on vitalrecords with that obtained by use of a detailed interviewquestionnaire for those States that code industry and occu-pation on their vital records.
NMIHS staff plan to include the followingwork-related items in the 1987 pretest of the 1988 NMIHSquestionnaire: industry and occupation of employment for‘ather at time mother became pregnant (coded to 3-digitU.S. Bureau of the Census codes), including dates of:mployment and average number of hours worked per.veek, and industry and occupation for mother at three time>oints—prior to pregnancy, during pregnancy, and at time~f interview (approximately 5 months after delivery) (codedto 3-digit U.S. Bureau of the Census codes). These data willalso include dates of employment and average number ofhours worked per week. Examination of reproductive haz-ards may be possible with these data.
Other NCHS survey programs, such as the NationalHealth Care Utilization Survey, should be examined fortheir potential usefulness for occupational research.
Uses
These are examples of special surveys that deal withreproductive history and outcomes. Because reproductiveJisorders were identified by NIOSH as one of the 10leading work-related diseases, these data sources should be
examined for their utility to address specific hypothesesand/or generate prevalence estimates of potentially work-related conditions.
costs
The estimated cost for the NMIHS occupationallyrelated component is $480,000. The coding of industry andoccupation will cost an additional $50,000. Therefore, theestimated cost per respondent is $26 and the cost per deathis $53 (table 4).
Advantages and disadvantages
NMIHS includes 4,000 fetal and 6,000 infant deathswith enormous potential to examine occupational risk fac-tors for both parents. The format could provide the oppor-tunity for detailed and specific followback. Among thedisadvantages of the NSFG is that it will likely containinformation on very few deaths if the study population isfollowed with the NDI for subsequent adverse pregnancyoutcomes. The NMIHS has information on a large numberof fetal and infant deaths but not enough for most analysesby detailed occupation and industry or for small geographicareas.
Questions and answers
To the question of whether the information from theNMIHS could use occupational information currently be-ing coded by the States, the reply was that the NMIHSdecedents were infants (without occupations), and the Statecoding was for adult decedents. Unfortunately, no linkagebetween the two sets of records is feasible, but informationon the occupation and industxy of parents could be ob-tained in followback surveys such as the NMIHS to linkoccupational exposures of parents to health outcomes fortheir infants.
Another suggestion that was made was for codingoccupation and industry of the parents on the report of thefetal death or on the birth certificate in those States inwhich data files of matched infant death and live birthrecords are being developed. (Editor’s notti The occupa-tion and industry of both parents are included in the U.S.Standard Report of Fetal Death, but they are only recom-mended for the U.S. Standard Certificate of Live Birth.)That may link enviroflmental and occupational exposures tothe outcomes of pregnancy. Some discussion ensued aboutthe problems associated With linking infant death and livebirth records. NCHS is currently exploring that possibilityin a major multiyear evaluation project. A pilot studyconducted jointly by NCHS and nine States in 1985 and1986 generated a more than 95-percent match rate betweenthese two vital statistics source records, suggesting thatestablishing an ongoing national data base of this type maybe feasible.
24

Option No. 8. Cohort foiiowup ofnationai study groups
Presented by Gilbert Beebe, National CancerInstitute
Description
In recognition of the need for a nationai system ofinformation on occupational mortality, consideration hasbeen given to using administrative record systems andspecial study groups. The decennial census, the CurrentPopulation Suwey (CPS), the Qmtinuous Work HistorySample (CWHS) of the Social Security Administration(SSA), and State unemployment insurance files have allbeen examined as potential sources of information ondifferential mortality associated with employment. Despitestrong encouragement of the National Institutes of Health,the U.S. Bureau of the Census has been unwilling to permitthe use of any part of the decennial census in this waybecause of confidentiality requirements, but has agreed tothe substitution of the Current Population Survey for thepurpose. This has resuited in the National I.mngitudinaiMortality Study, a collaborative undertaking of the NationalHeart, Lung and Blood Institute, the U.S. Bureau of theCensus, and NCHS, with an expanding sample currently at1.2 million individuai$ about 40 pereent of whom havebepn in the labor force.
The CWHS of SSA consists of 1percent of all those inthe social security program since 1937. Beginning in 1957,the file contained a longitudinal history of employment withStandard Industrial Classification (SIC) codes and alsoreasonably complete information on the fact, but not thecause, of death. The National Cancer Institute (NCI) isfunding SSA to obtain cause of death for the period1973-77 in order to test the usefulness of the SIC informa-tion in this file. SSA, the Internal Revenue Semiee (IRS),and NCI have all been interested in the potential value ofthe occupational entries on the IRS Form 1040 and havesupported a project to develop a partially computerizedapproach to Standard Occupational Classification (SOC)coding. One goal is the transfer of IRS occupational data toSSA for the CWHS.
Another source of nationwide data on occupationalmortality is the Dom smoking study of nearly 300,000veterans surveyed in the mid-1950’s. Data through 1970have been published by occupation and by industry, anddata through 1979 are being analyzed now. An additionalpossibility would be to follow up a clearly identified occu-pational population, such as ail members of a particularunion or all employees of a particular company, with theNDI in order to identi~ potential excesses in mortality ifappropriate comparison populations are available.
Uses
Each speciai study cohort presents a different mix ofinformation on demographic characteristics, mortality, in-dustry of employment, and specific occupation, but all of
them provide the basis for erdculating mortality rates withconsistency between numerator and denominator as toemployment coding.
costs
The costs of the National Longitudinal Mortality Studyhave been estimated to be $48 per death for 1973-83samples. Other national studies would have similar costsper death (table 4).
Advantagesand disadvantages
Dr. Beebe discussed the advantages and disadvantagesof Option No. 8 in relation to Option No. 2 (coding deathcertificates annually for all States). He characterized Op-tion No. 2.as the “Cadillac” and as a goai for a data sourceon nationai and local occupational mortality trends andpatterns. Dr. Beebe felt that use at the local level is perhapsan even more important consideration than national use, asstudies by Samuel Milham, for Washington State, havedemonstrated over the years.
The strength of the Current Population Survey (CPS)as a data base for occupational mortality studies, as in theNational Longitudinal Mortality Study, is that it includesinformation on lifestyle as well as occupation. Lifestyledifferences may account for a share of the differentialmortality that now is attributed to occupation. The majordrawback of the CPS is its small size. In addition, toascertain mortali& one has to go through three steps atpresenti (1) use the NDI to identi& the deaths to the CPScohort, (2) purchase copies of the death certificates of theidentified individuals from the States, and (3) code thecause of death from these certificates.
The CWHS has good identi@g information, somedemographic variables, the fact of death, and SIC code forthe industry of the decedent. But it lacks occupationalinformation, and one needs to go through the same steps aswith the CPS to obtain the death certificate from the Statesto codecause of death. A further disadvantage is its smallsample size.
Questionsand answers
A question was asked about the status of a bill de-signed to create “statistical enclaves” (Beebe, 1981). Statis-tical enclaves would allow certain Federal agencies to linkand pool reeords for statistical purposes, overcoming exist-ing restrictions related to confidentiality that either com-pletely or severely limit such information sharing. Dr.Beebe indicated that the legislation was defeated.
It was pointed out that the vital records were notsubject to the Paperwork Reduction Act, implemented bythe U.S. Office of Management and Budget, because vitalrecords are State rather than Federal records but otherdata sources of NCHS are subject to the act.
The information proposed for the 1990 census wasdiscussed. The questions for the 1990 census are likely tobe similar to those in 1980, including asking most recentoccupation if the respondent had worked within the past 5
25

years(in the 1970 census, it was asked for respondentshaving worked in the past 10 years). The change reflects thecontinuing pressures on the census to reduce respondentburden.
Option No. 9. Records systems
Presented by William Eisenberg, Bureau ofLabor Statistics, and John Sestito, NationalInstitute for Occupational Safety and Health
Description
The Bureau of Labor Statistics is involved in two majorFederal-State cooperative programs that collect informa-tion on occupational injuries and illness from recordsources the Annual Survey of Occupational Injuries andIllnesses (ASOII) and the Supplementary Data System(SDS), based on State workers’ compensation reports. Theannual survey is a mandatory sample of 280,000 employersconcerning the private sector. Surveyed employers reportall occupational fatalities, illnesses, and injuries, except firstaid cases. The fatality cases that are reported in the surveyare followed back to obtain general causal informationabout the fatal event. Fatality cases are then classified into1 of about 15 different categories, such as highway vehicleaccidents, fires, or electrocutions.
The other general source of information is the Stateworkers’ compensation systems, on which the SDS is based.Information provided in tl]is program includes the industryand occupation of the affected worker, the nature andsource of injury or illness, the part of the body affected, theaccident or exposure type, the associated object of sub-stance, and the sex and age of the worker. Thirty-two Statesprovide this information voluntarily. Of these, 12 Statesprovide information on fatalities. Ten States provide fatalityinformation on “closed cases,” that is, cases that have beensettled. Two States provide information on fatalities on a“current basis: that is, cases for which claims are pendingbut have not yet been closed.
In the past, more traditional approaches to the defini-tion of occupationally related illness and injury have limitedthe utility of workers’ compensation files for studying cer-tain occupational diseases. However, in some cases, legaland legislative initiatives have resulted in the compensationsystem expanding its coverage to other chronic healthconditions.
Uses
The annual survey can provide national and Stateestimates of the numbers and incidence rates of occupa-tional fatalities by general industry and causal categories. Itcan be used for trend analysis and interindustry compari-sons.
The potential exists for followback of workers’ com-pensation files at the State level or through SDS although itmay be more useful for morbidity rather than mortalitysurveillance.
costs
These surveys include morbidity, as well as mortality,records. If the total cost of the surveys were amortized overthe death records only, the costs to maintain these twosurveys is currently about $1,600 (for ASOII) and about$1,700 (for SDS) per death ascertained. The large cost perdeath reflects the fact that a majority of the records pro-cessed in these surveys are not death related.
Advantages and disadvantages
The annual survey has the potential for followback byindustry or source and has detailed industry identification.Although information on the demographic characteristicsof workers is not currently collected, this information isavailable and could be obtained through followback. Inaddition, demographic characteristics for facilities are cal-culated for employers with 11 or more employees. Thesurvey excludes agricultural employers with less than 11employees and the government sector, and it capturesmostly traumatic fatalities due to accidents rather thanchronic illness and may exclude fatal injuries when thedeath occurs in a different calendar year than the injury.
The SDS and workers’ compensation files have excel-lent information on demographic characteristics, on factorsrelating to the event, and detailed industry and occupationinformation. In addition, there is potential for followback atthe State level. SDS files are, however, lirnitcd by inconl-plete coverage of workers, incomplete participation from allState programs, variations in claims processing proccdurcs,and lack of denominator information. The legal nature ofthe system affects its ability to serve occupational healthand mortality surveillance. Being an insurance system,some diseases are not recognized as work-related, and,therefore, are not covered by the system. In addition, theconfidential nature of some of the information containedon workers’ compensation tiles may limit its ability to beused in a record linkage system.
Questions and answers
Among the questions asked of Mr. Eiscnbcrg waswhether his agency had given thought to establishing stud-ies based on the Occupational Safety and Health Admin-istration’s (OSHA) Form 101, which is a supplementalrecord to the establishment survey that includes additionalinformation on the demographic characteristics of the in-jured workers. A pilot study is being developed to test thefeasibility of collecting the information on the OSHA Form101. Also, BLS will explore the use of the standard ICDcodes (the International Classification of Diseases recom-mended by the World Health Organization) that are usedto code morbidity and mortality information.
Mr. Sestito noted that his colleagues in the Morgan-town, West Virginia, office of NIOSH are developing anational fatality registration system, which is an attempt tolink information from the mortality statistics system with
26

information from the workers’ compensation system.Mr. Sest{to feels that there is considerable potential insome of the State information systems, such as workers’compensation, particularly States such as California thatarc beginning to establish compensation funds for certainoccupationally related diseases, such as asbestosis. Thecosts of workers’ compensation is on the order of $22 to$23 billion per year.
Option No. 10. Use of compressedvital statistics files
Presentedby Bruce Cohen, National Centerfor Health Statistics
Description
The detailed vital statistics files can be compressed forrapid, easy use by investigators. An example of this type offile is a county-level national mortality and population filedeveloped at NCHS that spans the years 1968-83, referredto as the Compressed Mortality FiIe (CMF). These files canbe used to identi~ geographic areas with excess mortalityrates that may be related to occupational exposures.
The CMF files are stored on only three reels of tape,hvo for the mortality data and one for the population data.Differential mortality trends can be easily and efficientlyexamined because of the compact nature of this file. AIIearlier version of this system, which covered the years1968-78, was developed by Dr. Alan Gittelsohn (Depart-ment of Biostatistics, Johns Hopkins University School ofHygiene and Public Health) under contract with NCHS.
The compressed vital statistics files are derived fromthe 31 million U.S. microdata death records for this period.The 159-160 byte records were condensed to 23-byterecords by reducing the number of variables included oneach record. The variables included on the condensed fileare county of residence, year of death, race (white versus allother), sex, age group at death (divided into 15 age groups),and underlying cause of death (4-digit ICD code). The 31million records were reduced to 13 million records bycounting records that were identical with respect to thesevariables, and then adding a count field.
The compressed population file is derived from annualestimates for each U.S. county by 5-year age groups, race(white versus all other), and sex. These estimates reflectadjustments based on the 1980 census, and they wereprepared by the U.S. Bureau of the Census with modifica-tions by NCHS, The compressed mortality files and thecorresponding population data from the U.S. Bureau of theCensus are now available as tapes from the National Tech-nical Information Service for $300 for the first 10 years and$900 for the next 5 years.
Uses
This approach would be used to identi~ geographicareas (at the county level or greater) with excess cause-
specitic mortali~ rates that maybe related to occupationalexposures. It would also examine time trends and geo-graphic variations in cause-sprzific and possibly occupa-tionally related mortality.
costs
The costs to develop this data base are minimal be-cause the source data are currently available throughVSCP. The costs for processing and secondary data collec-tion are estimated to be $0.0003 per death (table 4).
Advantages and disadvantages
This approach is simple to use, and it can provideinexpensive, comprehensive cause-of-death informationwith broad geographic coverage over an 18-year span.However, it provides neither industry or occupation infor-mation nor exposure information; it provides only ecolo~”cdatq no individual-level variables are available.
References
Beebe, G. W. 1981.Record linkage and needed improvementsinexisting data resources. Quantification of Occupational CanceZBanbury Report No. 9. Cold Spring Harbor Laboratory.pp. 661-673.
Guralnic~ L. 1962.Mortality by occupation and industry amongmen 20 to 64 yerus of age: United States, 1950. Htal Statistz”cs—Special Repo~8 Vol. 53, No. 2. Washington: U.S. GovernmentPrinting Office.
Guralnic~ L. 1963a. Mortality by occupation and cause of deathamong men 20 to 64 years of a% United States, 1950. HfalStatktics-S’cial Reports, Vol. 53, No. 3. Washington U.S. Gov-ernment Printing Office.
Guralniclq L. 1963b. Mortality by industq and cause of deathamong men 20 to 64 yearn of agti United States, 1950. V7talStatistics+ecial Repents, Vol. 53, No. 4. Washington:U.S. Gov-ernment Printing Office.
Guralnic~ L. 1963c.Mortality by occupation level and cause ofdeath amongmen 20 to 64 yems of age: United States, 1950.J4talStat&tics-Speciaf Repo~, Vol. 53, No. 5. Washington: U.S. Gov-ernment Printing Office.
National Center for Health Statistics, T. Z. Hambright. 1969.Comparability of mm-tat status, race, nativity, and country oforigh on the death certificate and matchingcensus record: UnitedStates, May-August1960. P7taland Health Statktics, Series 2, No.34. PHS Pub. No. 1000.Public Health SeMce. Washington U.S.Government Printing Office.
Rosenbe~ H. M., D. Bumham, R. Spirtas, and V. Valdisera.1979.Occupation and industry information from the death certif-icate: Assessment of the completeness of reporting. StatisticalUses of Administrative Records with Emphasis on Monality andDisability Research, edited by L. Del Bene and F. Scheuren.Washington Social SecurityAdministration.
U.S. Congress. 1986. House of Representatives. OccupationalHeaith Hazard Surveiknce: 72 YearsBehind and Counting. HouseReport 99-979.Washington: U.S. Government Printing Office.
27

Chapter Ill.Working group reports
Objectives for working groups
by Bruce Cohen, Ph.D., Office of Analysis andEpidemiology, National Center for HealthStatistics
There are many data resources that can be used foroccupational surveillance and research as depicted in figure2. This figure is intended to represent the many interlockingparts of a puzzle. The National Institute for OccupationalSafety and Health has several data bases that evaluateexposures and health hazards. The Bureau of Labor Statis-
tics collects information on work-related health events intheir annual survey. Obviously, State government anduniversity-based research play an important role in under-standing the risks. Also, the National Cancer Instituteconducts many industry-wide studies of cancer. In addition,there are studies sponsored by unions and industries. TheNational Toxicology Program performs laboratory researchon toxic agents that are found in the workplace. TheNational Center for Health Statistics (NCHS) has surveysthat address morbidity issues. The central location ofNCHS mortality data in the puzzle is meant to focus ourattention for this Workshop, not to imply that these data
2 C?5 .emWorkers
Compensation
I
NIOSHHealth
?’=jV”
L
Hazard
Evaluations
3
?sw.ti-~
T-
~y
% (+” ‘- n UniversityResearch
u
NCHSMorbidity
w!@Vlw
NationalToxicology
Data Program BLSAnnualsuNeys
NOTE ELS is Bureau of Lnbor Statistics, NCHS ia National Center for Hadth Statistic, NCI ia National Cancer Institute, and NIOSH ia Nauonal lnwtute forOccupational Safety and Health.
Fgure 2. Data Resourms for Occupatia+tal Survoill.ence sandReasmrch
28

areanymore central than other data sources to the overalloccupational health surveillance issue.
The visual display in figure 2 emphasizes severalpoints occupational health surveillance and research are areal puzzle. Further, there are many pieces that provideinformation relevant to the activity. How these pieces fittogether is not being addressed at this Workshop, but thefocus is on how NCHS might assist others in their researchactivities. We all work on different pieces of this puzzle, soI think that it is valuable that we view the NCHS mortalitydata in the context of all of the other pieces of the puzzle.
The first goal of this Workshop is to review the coUec-tion and use of data regarding mortality risk by occupation
and industry. The 10 options that were elucidated do notpreclude consideration of other options or modification ofthe options that were proposed. The second objective is tomake recommendations regarding the implementation ofcoding occupation and industry on death certificates. Cer-tainly, in terms of the needs of NCHS for planning, this isthe key objective. A third objective of the working groups isto discuss recommendations regarding the use of otherNCHS data sources or data from other agencies for occu-pational surveillance. This last objective is a secondary goalof the Workshop.
29

?eport from Woricing Group No. 1
ienry Anderson,W-nsin Diviin ofieaith
~articipants of Working Group No. 1ncluded:
+emy Anderson, RappxteurNisconsin Division of Health
2dward BakerNational Ihstitute for occupational Safety and Health
%aron BlairNational Cancer Institute
?red Blosseroccupational Safety and Health Reporterme Bureau of National Affair% Inc.
3reg BondDow Chemical Company
David BrownNational Institute for occupational Safety and Health
Harvey ChezkowayUniversity of North Carolina
Bruce CohenSational Center for Health Statistic
Gwendolyn DoebbertGditbmia State Health Department
Joseph DuBoiskcupational Safety and Health Administration
Jacob FeldmanNational Center for Health Statistics
John FroinesUniversity of Californi% Los Angeles
Eric Frumin%nerican Clothing and Textile Workers Union
George GayNational Center for Health Statistics
David LilienfeldMt. Sinai School of Medicine
Melvin L. MyersNational Institute for Occupational Safety and Health
Earl PollackNational Academy of Sciences
Charles J. RothwellNorth Carolina State Center for Health Statistics
George StellutoBureau of Labor Statistics
George VanAmburgMichigan State Registrar
Diana ZuckermanU.S. Congress, House of RepresentativesGovernment Operations Committee
Review of options
The approach taken by this working group was totemporarily ignore the options outlined for the group andall of the existing data sets and then ask the question Whatwould we design as a system for a-g occupationallyrelated mortality? Alter that long proc~ the group agreedthat Option No. 2, the annual industry and occupationcoding for all States, represented the ideal situation. If onealready has an existing vital statistics data system, such ascurrently exists in the Vital Statistics program at the Na-tional Center for Health Statistics (NCHS), despite all ofthe problems that anybody can identify, it is worth extend-ing that system to include industry and occupation codingfrom as many of the States as possible on an annual basis.
The group felt that industry and occupation could notbe viewed as a single, isolated entity. They have to beviewed as part of the vital recor@ specifically the mortali~records. Therefore, the other data portions of those recordsshould be considered in the analyses. There is a lot of otherinformation available on the death certificate that is valu-able for the analyses of occupationally related mortali~.
With regard to whether a national data system wasneeds we could come up with no sound arguments for nothaving a national system. Although a national system hasproblems, any system that does not cover the entire countryhas additional problem$ such as incompleteness of dataand limited application to other regions of the county dueto regional characteristics. Another imprtant aspect of anational data system is that problems of bias because ofmigration can be avoided. It was pointed out that, althoughsome people may retire to northern Stat% a substantialproportion of the retired population tends to move towarmer States in the south. Hence, estimates of mortalityfor occupationally related causes at a State or regional levelwould be misleading. The only way to capture informationrelevant to an occupation or indushy category, or to cap-ture information relevant to speciilc industrial settings, is tohave a national system.
Uses of a national data system
The working group summarized some of the importantuses of a national system. At the national level, theseinclude monitoring trends over time in mortality for partic-ular occupations and industries, early identification ofhealth problems, and hypothesis generation. The number ofcauses of death would necessarily have to be focused. Forinstancc, the use of the sentinel health events (occupation-al) (lWtstein et al., 1983) would be key to causes of deathto study. At the State level, one of the key issues would bethe utilization of the data system to target prevention andindustrial hygiene assistance programs. This would also betrue for the Occupational Safety and Health Administra-tion’s sponsored activities.
Key issues in implementing the system
The working group discussed several issues that theyconsidered central to the implementation of a high quality,
30

comprehensive data system. There needs to be nationalleadership and encouragement for this system. Now thatthe three agencies (the Bureau of Labor Statistics, NCHS,and the National Institute for Occupational Safety andHealth) have signed a memorandum of understanding it ishoped that new cooperation will engender greater attentionand provide greater assistance and direction to the States.There is a need to use the information that has alreadybeen collected and publish it so it can be used to inform theStates of the utility of this information. However, the Statesshould be involved in discussions of how the data should beanalyzed and summarized to avoid unilateral decisions bythe Federal Government regarding such aspects as agebrackets and grouping of other coded information.
The working group wished to stress the need to de-velop an automated coding system. This would assist theadditional States to begin the coding and would help reduceescalating costs.
Clearly, the key to the program is quality control. Wefound that everyone seems to have a different definition ofwhat quality control is. However, there was a consensusthat quality control must go beyond simple verification ofthe coded information. There is a need for folIowbackstudies (Option No. 5) to assess the information that iscoded, both for disease and for occupation and industry
information. Option Nos. 6 and 8 would also be useful inassessing data quality.
We felt that Option No. 4 was the best approach forStates in transition to comprehensive coding.
Funding of the program
The working group thought that this program could notbe accomplished by shifting support from ongoing activitiesat NCHS. There needs to be a total increase in the dollarsupport for the whole program because the other aspects ofthe vital statistics program should not be diminished. Wefelt that the best way to fund the program would be as adirect appropriation from Congress. It was felt that theprogram should not be funded on a partial basis. Theimportance of the issues of occupational and industrycoding for death certificates needs to be recognized so thatthis system will be maintained in the future.
References
RutStein,D. D., R. J. Mullan, T. M. Frazier, et al. 1983.Sentinelhealth events (occupational): A basis for physician recognitionand publich health surveillance.Am. J. Public Health 73:1054-1062.
31

Report from Working Group No. 2
Todd Frazier, National Institute foroccupational Safety and Health
Participants of Working Group No. 2included:
Todd Frazier, RapporteurNational Institute for Occupational Safety and Health
Gilbert BeebeNational Cancer Institute
Warren BucklerSocial Security Administration
Km-en M. DeasyNational Institute for Occupational Safety and Health
William EisenbergBureau of Labor Statistics
William FayerweatherE. I. duPont deNemours and Company
Edward HunterNational Center for Health Statistics
Deborah KeimigNational Academy of Sciences
Carl A. KellerNational Institute of Environmental Health Sciences
Barbara KerrNational Center for Health Statistics
Karl KroncbuschOffice of Technology Assessment
Philip LandriganMt. Sinai School of Medicine
Samuel MilhamWashington State Department of Health
Michael MoI1National Institute for Occupational Safety and Health
Robert MullanNational Instilute for Occupational Safely and Health
Patricia PotrzebowskiPennsylvania Division of HealthStatistics and Research
Harry RosenbergNational Center for Health Statistics
Michael SilversteinUnited Auto Workers Health and Safety Department
Elsie StantonNational Center for Health Statistics
Janice WindauBureau of Labor Statistics
Review of options
The consensus of the working group was to concentrateon Option Nos. 1 through 4. Option No. 2, annual coding
for all States, was selected as the goal for the program. Theother three options were viewed as special cases of thepreferred option and represented logical stages in theevolution of a national program.
The working group recognized that fiscal constraintswould affect the speed with which Option No. 2 could beimplemented. It was proposed, therefore, that a modifica-tion of Option No. 4 should be implemented. Specifically, aprogram should be developed that includes industry andoccupation coding in selected States plus demonstrationproject funding designed to increase States’ ability to de-velop occupational disease intervention programs.
Uses of a national data system
The discussion of the group identified three importantuses of this data system: description of trends in occupa-tionally related mortality; hypothesis generating capabilityof mortality data with coded occupation and industry; anduse of sentinel events (preventable deaths due to workinjuries or diseases) that should result in effective interven-tion. At this point, it became clear that there were under-standable, but major, differences in the uses made of themortality data systems by Federal agencies and by theStates. For some users, the purpose of the data is mainlydescriptive for others, the data represent a necessa~ firststep toward intervention.
Issues of data quality, coding, andaccessibilityy
The concept of an information chain in these datasystems includes the flow of information from the attendingphysicians, to the informant, to the funeral director, tonosologists, to epidemiologists. All have a part in providingaeeurate information. The need for raising the awareness ofphysicians to the possible role of workplace hazards wasnoted. The work of the National Institute for OeeupationalSafety and Health (NIOSH) and the National Center forHealth Statistics (NCHS) in publishing the Funeral Direc-tor Handbook was discussed. Mention was made of Dr.Milham’s work developing industry aud occupation codesthat meet specific State needs but remain generally withinthe taxonomy of a national industry and occupation classi-fication system. The role of NIOSH in training nosologiststo code industry and occupation was credited, in part, forthe increase from 6 to 32 States plus the District ofColumbia now making use of the industxy and occupationinformation on death certificates. Surveillance CooperativeAgreements between NIOSH and States (SCANS) and theNIOSH-funded State Capacity Building Agreements alsohelped enhance the value of the death certificate for occu-pational health surveillance.
Key issues in implementing the system
It was recognized that there are different goals, that is,that the needs of the National Center for Health Statistics(NCHS) or the Bureau of Labor Statistics (BLS) to makenational estimates could not necessarily meet other Federal
32

or State Health Department needs. Clearly the currentstatus, Option No. 1, that is, the collection of informationfrom a limited number of States, is necessary but notsufficient.
The group recommended that emphasis be placed onthe development of automated coding of industry andoccupation, that is, keying the literal descriptors from deathcertificates and using the computer to code the industry andoccupation,
Funding of the Program
code occupation and industry on mortality records, there isno assurance that such increases in the NCHS budgetwould be possible. Without an increase, non-NCHS sourceswould have to be sought to support the program. The groupurged NCHS to aggressively seek funding, and also urgedthe National Cancer Institute to continue funding for indus-try and occupation coding beyond fiscal year 1988 if newNCHS appropriations were not forthcoming.
Some concern over current funding plans was dis-cussed. Although NCHS would plan to seek funding to
33

Report from Working Group No. 3
PatriciaHonchar, National InstituteforOccupational Safety and Heafth
Participants of Working Group No. 3included:
PatriciaHonehar, RapporteurNational Institute for Occupational Safety and Health
Faye AzizSocial Security Administration
Patricia BufflerNational Center for Health Statistics
Carol BurnettNational Institute for Occupational Safety and Health
John A. CooperNational Cancer Institute
Deborah DawsonNational Center for Health Statistics
Ralph Frankow@University of Texas, Houston
Frank FrodymaU.S. Department of Labor
Lillian GuralnickConsultant, formerly with National Center for HealthStatistics
AlIan HoskinNational Safety council
Jay LubinNational Cancer Institute
Jeffrey MaurerNational Center for Health Statistics
Dennis PerrottaTexas State Department of Health
Gail PoeNational Center for Health Statistics
John PriebeBureau of the Census
Linda RudolphCalifornia Department of Health Sewices
Alice StarkNew York Department of Health
William StewartJohns Hopkins School of Hygiene
Lacola WashingtonNational Center for Health Statistics
Review of options
The consensus of the working group was for continuedeffort to move toward Option No. 2, the industry andoccupation coding by all States. It was noted that Option
Nos. 1,3, and 4 are included in Option No. 2. The grouppreferred to modi& Option No. 2, however, to be aneventual goal, not a goal for rapid implementation. Rather,the group recommends an aggressive but realistic imple-mentation of Option No. 2.
The group did not review Option Nos. 5 through 10because of time restrictions, not priorities. The group didfeel that there were many important options in this lattergroup and would encourage the careful consideration ofthese options at another time.
Uses of a national data system
The group discussed examples of industry and occupa-tion presented by representatives from several States andfound a wide range of applications. Nonetheless, the issueof development of further uses of the data beyond thecurrently understood potential uses was felt to have a highpriority.
Uses of the data that were identified included trendsurveillance, program and policy evaluation and develop-ment, and hypothesis generation. We feel that consider-ation should be given to providing support and assistance toStates to continue to develop creative uses and evaluationof the indushy and occupation coded mortality data. Thiscould be conducted through demonstration projects tosome states it should also include exploration of use byStates as well as usage for national level analyses.
Issues of data quality, coding, andaccessibility
Because the quality, validity, and accuracy of otherdeath certificate information is relevant in the analyses ofthe industry and occupation data that will be coded, theworking group recommends that filrther attention be givento appropriate estimates of error, or to qualifications of thedat% for all information collected on the death certificate inthe process of reviewing the industry and occupation cod-ing. There should be incentives provided to States to be-come part of the coding system. In most States, the effortrequired to develop industry and occupation coding coulddivert energy, time, and people away from other occupa-tionally related activities.
Key issues in implementing the system
As noted before, the working group felt that an orderly,rapid implementation of the national system is required,There were two distinct approaches suggested for theimplementation of the system. One approach would be toinitiate the coding in one new State at a time. Anotherapproach would be to begin coding with subsets of certifi-cates from all States, with the eventual movement towardcomplete coding in each State. The group did not reach aclear consensus on the relative value of these alternativeapproaches.
The development and sharing of automated coding willbe very important to the implementation of Option No, 2. Ifsuch software were available, the problem noted above of
34

diverting resources away from other occupationally relatedactivities could be minimized.
Questions were raised about the States that are cur-rently not involved in the industry and occupation coding ofdeath certificate information sent to NCHS. &e theseStates using the information? Among the States that docolleet industry and occupation information on the deathcertificate, what are the procedures and what is theirexperience in assessing data quality? The group urged thatall of the States be involved early in the review of theimplementation of a national system.
Funding of the program
The funding issue is related to the relative usefulness ofthe information. The working group recognized that thefunds are limited at the national as well as State levels.Funding of this activity might mean the lack of funds forrelated activities. The group did reeommend that the fund-ing should be a multiagency activity. Involvement of severaIagencies is important both from a teehnical, as well asfinancial, point of view.
35

Reportfrom Working GroupNo. 4
Thomas Mason, National Cancer Institute
Participants of Working Group No. 4inciuded
.Thomaa Mason, RapporteurNational Cancer Institute
Robert BiigradNational Center for Health Statistics
Dennis BregmanNational Institute for OeeupationaiSafety and Health
John E. BroekertUtah Department of Health
Elizabeth DelzellUniversity of Aiabama at Birmingham
Harvey HilaskiBureau of Labor Statistics
Robert IsraelNational Center for Health Statistics
James M. MeliusNational Institute for OeeupationaiSafety and Health
John PattersmNational Center for Health Statistics
Wiiiiam G. PhiiiipsConsultant
David SavitzUniversity of North Carolina
Fritz ScheurenInternal Revenue Sewice
Joseph SchwerhaU.S. Steel Corporation
Thomas ScoppU.S. Bureau of the Census
John SestitoNational Institute for OccupationalSafety and Health
Robert SpirtasNational Cancer Institute
Sabrina SturbaNational Center for Health Statistics
Diane WagenerNational Academy of Sciences
James WeeksUnited Mine Workers of America
Review of options
The working group unanimously a~eed that OptionNo. 2 was the goal to be sought. Any of the other optionswould be compromising the potential utility of the data.Therefore, at this stage of the process, Option No. 2 shouldbe the focus of the program.
Uses of a nationai data system
The first question asked of the working group waswhether anyone felt that we should not persist in codingindustry and occupation on death certificates. No one in thegroup felt that the coding should stop. The group feit thatthe coding should continue not beeause the continuedactivity would facilitate answering important occupationalhealth risk questions but because continued coding wiilstimulate use of the eoliected records and thought onalternative uses of the data. Scientists are opportunist theytake advantage of what is avaiiable. Therefore, it is impor-tant that the coding continue so additional data are avail-able and so continued emphasis ean be focused on the bestway to use industry and occupation data. The group feltthat the other uses for a national data system pale incomparison to the utility of these data to drive the researchfield of occupational health.
Key issues in implementing the system
One of the key i~ues not mentioned by the previousworking group reports is the timely dissemination andreduced cost of obtaining the tapes. The working group feltthat the National Center for Health Statistics (NCHS) has agood reeord in preparing and releasing data and, therefore,NCHS should continue to have the primary responsibility incollecting these data.
Funding of the program
The working group recommended that new fundingsources be sought. In particular, the group noted therelevance of these data to the Agency for Toxic Substancesand Disease Registry (ATSDR). The group felt that thereeent Super Fund reauthorization legislation had broad-ened the mandate of ATSDR to provide for their participa-tion in collecting environmental hazard data to be includedin the registxy. Most of the high-dose exposures to toxicsubstances occur in the workplace. Therefore, industry willprobably be one of the largest users of the registry. Obvi-ousiy, death is an extreme health effeet of exposure, but thecauses of death can give important information regardingthe nature of toxic effects, The working group felt thatATSDR anti other agencies involved in the assessment oftoxic exposures and their effects should be informed aboutthe work that is ongoing at NCHS and the need foradditional funding.
3e

Discussion
by Charles Rothwell, formerly the Director,North Carolina State Center for HealthStatistics
This Occupational Mortality Data Workshop hasbrought together a diverse group of participants fromvarious State and Federal agencies, private industry, andacademia. The Workshop has provided a good forum fordiscussion of wide-ranging efforts relating to the collectionand analysis of health-related industry and occupation(1/0) statistics, The tripartite agreement signed among theBureau of Labor Statistics (BLS), the National Center forHealth Statistics (NCHS), and the National Institute forOccupational Safety and Health (NIOSH) will eneouragejoint ventures in this field and considerable discussion hascentered on the needs for various forms of 1/0 data.However, the primary purpose of the Workshop has beento discuss and then propose the most appropriate optionsthat NCHS should implement to produce occupationalmortality statistics.
The participants have considered 10 options for thecollection of 1/0 data. The first four options related to I/Ocoding on death certificates; the next two options concernedthe use of NCHS surveys for followup in the collection of1/0 data; and the remaining four options related, for themost part, to the use of administrative data collectionsystems, The participants, although representing agenciesof diverse responsibilities, were of one mind in their recom-mendation to NCHS. Both through open discussion and byquestionnaire, they strongly urge NCHS to place primaryemphasis on the collection and utilization of 1/0 coding ondeath certificates, Specifically, they propose that NCHSattempt to establish national coverage of I/O data on deathcertificates while first seeking firm funding for the Statesnow involved in a pilot venture supported by short-termfunding arrangements.
Summary
Although many options were discussed, emphasis hasbeen placed on those alternatives that pertain to existingdata sets of NCHS that utilize NCHS’ strengths. UnlikeNIOSH and other centers in the Centers for DiseaseControl, NCHS has not been involved with development ofState or county level disease surveillance systems. Theprimary role of NCHS has been the creation of nationaldata systems for research of national issues and for produc-ing national estimates to aid in formulating and evaluatingnational policy. The exception to this national focus atNCHS has been the vital statistics system that is a cooper-ative effort at the local, State, and Federal levels. Althoughvital statistics can provide estimates at all three governmen-tal levels, rates can be unstable for small-area estimates ofrare events. Thus, the most prudent use of I/O data derivedfrom death certificates for small-area estimation and sur-
vedlance should be a combmed r~spol]~itil,.i~ L,..>:.. ,.
:.;;.:.
and NCHS. For example, the refinement of the iist ofsentinel health events that are occupationally related(Rutstein et al., 1983) is currently under way by NIOSH.The use of these codes may be the most appropriatemethod for utilization of I/O mortality data for small-areasurveillance.
The appeal of expanding the capabilities of a well-developed and highly utilized data system to serve as theprimary national data system to measure the extcut andimpact of occupationally related disease is considerable.Nevertheless, the utilization of 1/0 information from cIMII1certificatees is not devoid of problems. The quality of thedata is of paramount importance. Da[a quality CALLJILIS
beyond the standardization of coding procedures anti [kverification of State coding. Financial support to States forthe coding and provision of 1/0 data should be prcdic.tt cdon an active State-based query system to resolve ill-dcfineclor improper 1/0 entries. Unfortunately at this time, mosiStates collecting 1/0 information have not enacted a querysystem. The bulk of financial support will be needed mcollect and code these data and assure their timeliness andquali~, however, funding should not be directed solely mStates. At this time, NCHS does not have the ncccssmycapacity to internally support a national 1/0 mortalilysystem. NCHS will need adequate staff to train Slatecoders, to respond to daily questions from States on codingconventions, and to verify State coding in timely fashion.Also, given additional resources, the National Ivlormli[yFollowback Survey could serve as a quality control mecha-nism for cause-of-death information and for 1/0information.
Another concern regarding the development of a na-tional system relates to the appropriate analysis and displayof 1/0 mortality data. Central to this problem is the lack ofdenominator data. States and researchers have used variousmethods to depict differences in mortality outcome forselected occupations and industrial settings. Years of lifelost and mean age at death have been used; yet, thesemeasures may reflect differences in the age distributions ofemployees in selected occupations and not mortality differ-entials. Proportionate mortality ratios and odds ratios havealso been used; however, they may provide an unacceptablelevel of false negative findings. Standardized mortality ra-tios and age-adjusted rates have been used successfully foryears immediately surrounding the census when denomina-tor data are available.
A more intractable, yet related, issue is that cerlainoccupations or industries may attract employees with verydistinct lifestyle attributes and economic pressures. Thus,the measurement of seemingly direct relationships betweenoccupation and mortality and certain diseases may insteadbe the measurement of the relationships of certain diseasesand a select group of people who seek and hold suchemployment. Unfortunately, many such lifestyle factorscannot be handled statistically because data for the factorsare missing. For example, death certificates do not contain
37

smoking history, and it is well known that physicians se-verely underreport cause-ofdeath entities that relate tosmoking. A similar statement can be made about thereporting of alcohol related mortality. Ye~ even with ade-quate cause-of-death reporting it cannot be assumed thatsmoking and the utilization of stimulants and depressantsare uniformly distr]%uted over industry and occupationgroups. Here again, the National Mortality FollowbackSurvey may be of some help. Much analyticwork needs tobe done on the proper methods of data analysis and NCHSshould provide such leadership.
Still another problem relates to the comparability ofcoding that will take place at the State level.The training ofnosologists on standati methods of determining the under-lyingcause of death led to automated means of determiningthe underlying cause. In a similar fashion, NCHS shouldreview efforts at the U.S. Bureau of the Census and at theUtah State Health Department to automate I/O coding.With this as a basis NCHS may then be able to develop anautomated means of coding of I/O data from literal entries.Funding will be needed to develop such a comprehensiveautomated coding system.
Strategy
Even with the problems previously mentioned, themost viable option for NCHS is to seek funding of anational effort to collect I/O data from death certificates.Funding should not be an “all or nothing” proposition.However, if there is no hope for expansion, the money forcontinued funding of pilot States should be placed else-where. Bythemselves the States currently providingdata donot provide enough information for national estimates. Theminimum level of commitment should be for funding ofpilot States as well as neccssmy support functions withinNCHS, coupled with a good chance for future expansiontothe remaining States. If, for whatever reason, this strategydoes not entice funding support, NCHS should re-examinethe options relating to the utilization of linkagesbetween itssurveys and administrative data systemsto provide nationalI/O mortality estimates. Although not recognized by thisWorkshop as the most appropriate set of option% theseother options may generate more funding interest.
The future
Although a national I/O mortality system will takeyears to develop, NCHS should continue to examine futureoptions. The problem of long latency periods from expo-sure to a diagnosed occupationally related disease is wellknown. Now with improved treatment leading to delayedmortality or death due to other causes, mortality databecome even more removed as a measure of a currentexposure problem. Several future possibilities exist.
In 1989, States will begin to collect I/O information onall fetal deaths of greater than 20 weeks’ gestation. Forinfant deaths, a change in procedure could be establishedby States to either collect the I/O data of the mother on all
infant death certificates or to follow back on all infantdeaths for the mother’s I/O information. With the existenceof a national linked birth and infant death file,considerableinformation is available surrounding conditions at birth.Combining I/O data from fetal death certitlcates and linkedbirth and infant death certificates could provide a vexysensitive and low-cost surveillance system for occupationalexposures by women. Such a systemwould not suffer fromthe problem of long latency periods between exposure andoutcome. This project is also of interest because generalmortality I/O data may not be useful for the female popu-lation in the near future. Women have only recently be-come employed in some occupations. The risks of mortalityfor women in these occupational settings can be expectedtobe underestimated. Yet we cannot, even temporarily, turnour backs on measuring the risks of adverse occupationalexposure to women. Measuring reproductive outcome rel-ative to occupational setting should be considered. Thefetal and infant death file is relatively small, and it shouldbe inexpensiveto maintain. There are approximately30,000fetal deaths and 40,(XKlinfant deaths in the United Stateseach year. Even if each State paid $2.00 per record foradditional I/O dat% the cost of data collection would beonly $140,000 per yea~ and internal NCHS su~rt re-quirements beyond the general mortality I/O requirementswould be minimal.
Population-based registries are now being created inmany States. These morbidity registries include birth de-fects, cancer, trauma, and end-stage renal disease patients.Few registries collect I/O data. It would be most helpful ifthe National Committee on Vital and Health Statistic+ aswell as agencies that help support these registries such asthe National Cancer Institute, the Health Care FinancingAdministration, and CDC, would emphasize the utility ofcollectingI/O data.
Many States are creating data bases for health care costcontainment purposes. The agencies responsible for thesedata systemsam seldom found in State health departments.Therefore, the emphasis of these data systems is not pre-ventive health. There is a national organization, the Na-tional Association of Health Data Organizations(N&IDO), that encourages information transfer betweenthese evolvingState systems. Again, the National Commit-tee on Vital and Health Statistics should work with theseState agencies through NAHDO to sponsor discussion ofsuch issues as the collection of ICD E codes, I/O data, andsingle-patient numbers. The data bases are of considerableinterest because they cover such areas as hospital inpatientcare, ambulatory surgical centers, and outpatient services.
Conclusion
The conclusions of the Workshop are specific andheartenin~ yet, the identified challengesare many.There isa clear demand for a national systemto measure the impactand extent of occupationallyrelated disease. There is com-plete agreement where that effort should begin and that itshould not create a new reporting system with substantialreporting burdens. An existing system, the vital statistics
38

system, was selected for this purpose and its viability has Referencesbeen documented through a pilot project with States. Fund- Rut.stein, D. D., R. J. Mullan, T. M. Frazier, et al. 1983. Sentineling will be needed to build capacity at the Federal and Statelevels and research will be needed on analytic issues relating
health events (occupational): A basis for physician recognitionand public health surveillance. Am. J. Public Health 73(9):1054-
to the utilization of this information. 1062.
39

Discussion
by Harry M. Rosenberg, Ph.D., Chief, MortalityStatistics Branch, National Center for HealthStatistics
It has been most grati@ing to have participated in thislandmark Workshop, which is the first systematic andcomprehensive review of alternatives for producing occupa-tional mortality data. I am particularly grateful to Dr.Manning Feinleib, Direetor of the National Center forHealth Statistics (NCHS), for convening this meeting. Dr.Feinleib has sought, and I believe to a large degree re-ceived, a balanced description, critique of options, andrecommendations for producing occupational mortality sta-
tistics. Like many here, I admit to considerable surprise atthe degree of consensus regarding the direction in whichNCHS should proceed in this area that is, that NCHSshould exercise leadership in occupational mortality statis-
through the vital statistics system by
Adding to the existing reporting area of reimbursedStates.Exploring automated coding of occupation and indus-try from the death certificate.Undertaking research in methodologies, measurement,and analysis of occupational mortality.Promoting the quality of reporting occupation andindust~ on death certificates.Seeking appropriated funds for the NCHS budget tosupport State coding.
I would like to use this opportunity to do three thingxtoprovide, for the record, some additional historic perspec-~ive on the program; to raise some new issues and tocomment on the remarks of the rapporteurs and the otherdiscussants.
Some history
The current occupational mortality reporting system isthe outgrowth of one decade of sustained collaborativeeffort by a handful of staff from four Federal agencies, withthe support of the individual participating States, as well asthe Association of Vital Records and Health Statistics.Since 1978, the following Federal agencies have workedtogether with dedication and a high degree of professional-ism to develop a national occupational mortality data basethrough the vital statistics system (Rosenberg et al., 1984):
The U.S. Bureau of the Census has provided standardsfor classifying and coding occupation and industry,developed materials for and carried out training forState and Federal coders, and served as a continuingfocus for coding problem referrals and as a source ofcoding expertise for these items.The National Institute for Occupational Safety andHealth (NIOSH) has provided financial supportthrough funds to NCHS and through demonstrationgrants to the States in the Surveikmce CooperativeAgreements between NIOSH and States (SCANS)
●
c
programs. It has provided assistance to NCHS in manyoperational aspects of the program, including program-ming assisting in developing tabulation lists, and con-ducting training of State coders.The National Cancer Institute (NCI) has assistedNCHS in many aspects of the program and providedthe core funding to the States for fiscal years 1985-88 todemonstrate the feasibility and usefulness of the pro-gram. It is an understatement to say that NCI’S supporthas been crucial in institutionalizing the programwithin the States and at NCHS.The National Center for Health Statistics has adminis-tered the program with the State$ carried out qualityecmtrol on the data received from the States; developedinstructional and training materials; developed, withNIOSH and NCI, tabulation lists for cause of deathand for occupation and industry to be used in presen-tation and publication of these datw and has developedthe publication specifications for the NCHS program.
The occupational mortality program was initiated in1978 with a study to evaluate the codability of the occupa-tion and industxy entries on the death certificate (Rosen-berg et al., 1979). The study, directed by NCHS staff, wascarried out, under an interagen~ agreement, by the U.S.Bureau of the Census. The results demonstrated a highlevel of eodability of these items and established cost andproduction parameters for the coding, which could be usedas a baseline or standard by the States and NCHS.
The status of occupational mortality coding among theStates as of the late 1970’s was documented in a sumycarried out jointly by NIOSH and the association represent-ing State vital registration officials (Kaminski, 1981). Atthat time, only a handful of States were coding these itemsand were using a variety of classification and codingschemes that were neither readily comparable nor amen-able to being organized into a single multi-State data base.
The situation is vastly different today. Over 30 Statesare using a single coding and classification system throughwhich high quality data from 20 States are being routinelytransmitted to NCHS as essentially a component of the vitalstatistics data system.
Principal staff contributing to this deeade-long effortinclude Thomas Scopp and John Priebe from the U.S.Bureau of the Censuq John Sestito, Carol Burnett, andWilliam Crouse from MOSH; Gilbert Beebe and RobertSpirtas from NC~ and Drusilla Bumham, Glenn Flinchum,Jeffrey Maurer, and Harry Rosenberg from NCHS.
Issues
A large number of issues associated with implementingoccupation and industry coding have been identified. Iwould like to comment on a number of those from the pointof view of the program at NCHS that has had a majorresponsibility for this activity.
Institutionalizing the program —There is a consensusamong the working groups that NCHS should move towarda continuous program of coding occupation and industry
40

from the death certificate at the State level through the vitalstatistics system. To achieve this requires predictable, sta-ble, and adequate funding and staff for the States andNCHS. It must be emphasized, however, that this supporthas to be for not only the occupational mortality program,but also for the basic vital statistics program to whichoccupation and industry coding are being added. Occupa-tional data from the death certificate is of little value if theother data from the death certificate—such as cause ofdeath, age, race, sex, and place of residence—are notavailable or of good quality.
The advantages of Option No. 2 are not only that it iseconomically competitive with other options that have beendiscussed but that it draws on the strengths of State andnational vital statistics activities, which have been institu-tionalized for over 50 years, Vital statistics programs, whichexist in all of the States, provide an administrativeframework for ensuring uniform procedures, equitablereimbursement, quality control, data processing, and con-tact with data providers. These programs are also adapt-able, which is essential in a statistical system, as concepts,classifications, and data requirements change over time. Inthe vital statistics system, changes in data production areinstitutionalized through the annual issuance of instructionmanuals to each State for coding and processing vitalstatistics data and through the decennial revision of thestandard certificates and reports.
Funding strotcgies—Principal funding support for theNCHS occupational mortality program was made on ademonstration basis by NCI only through fiscal year 1988.The funding strategy to continue the program that appearsto have emerged from this Workshop is a proposal thatNCHS pursue a multi-pronged approach with the ultimateobjective of implementing Option No. 2 for an ongoingnational program involving the vital statistics systems of allStates.
The multi-pronged strategy would involve simulta-neously exploring several potential sources: (1) expandedfunding from NCI on a demonstration basis (2) fundingfrom the Agency for Toxic Substances and Disease Regis-try; and (3) funding through direct appropriation to NCHS.Clearly, the last of these is preferable to institutionalize thisactivity as an enduring and integral component of thenational vital stat istics program. I agree with the suggestionof Mr. Rothwell that a review of the program in 5 to 10years would be desirable to ensure that the value andutilization of the data for surveillance and analysis warrantsthe expenditure.
I believe that we must approach the issue of resourcesin terms of both adequacy and stability. AM]ough I agreethat the magnitude of resources required for implementingOption No. 2 are quite modest compared with otherfederally supported activities, it should be noted that anoccupational mortality coding program budgeted at $1
million annually would be a nontrivial change in the NCHSbudget, which is about $50 million annually.
If the occupational mortality program is implementedeven at a slightly expanded level from the 11-13 currently
funded States, NCHS must also be provided with the staffand budget resources for processing the greater volume ofdata, and, importantly, for the analyses of these data. Withassistance of other knowledgeable agencies such as NIOSHand NCI, it is crucial that NCHS demonstrate how thesedata can be used at the national and subnational levels toshow associations between occupation and cause of death.
Demonstration projects—Demonstration projects sup-ported by grants to the States can develop creative ways toproduce, analyze, and use the data in support of occupa-tional health activities at the State level. There may beadvantages to having such grants administered by programagencies, such as NIOSH and NCI.
Automated coding—The possibilities of automated cod-ing should be explored as part of a continuing occupationalmortality statistics program. NCHS already has experienceimplementing a pilot project in several States for an auto-mated system for encoding of cause of death from the deathcertificate with the goal of ultimately having the capabilityto automatically convert English language entries directlyinto codes of the International Classification of Diseases. Itis clear that the required internal dictionary in such asystem must accommodate a large number of entries in-cluding synonyms and misspellings. The system will stillrequire a manual component to awommodate the entriesthat cannot be automatically handled. It is unlikely that anautomatic system can completely replace experienced cod-ers for complex data items, such as cause of death andoccupation and industry.
The U.S. Bureau of the Census is developing a systemof this type for automatically coding occupation and indus-try in preparation for the 1990 census. In earlier discus-sions, U.S. Bureau of the Census staff indicated that,although the system is likely to work for a substantialproportion of cases, perhaps 50-70 percent, a large remain-ing number may still have to be manually coded. Perhaps,over time, this residual will be diminished. I strongly agreethat automated occupational mortality coding should beexplored by NCHS, possibly using l-percent evaluationfunds.
Mecwrement problems-The Workshop did not widelydiscuss measurement problems; but these should be notedand be explored thoroughly in an ongoing program. Briefly,measures of mortality risk usually have a numerator repre-senting the occurrence of an event over a stated period oftime, along with a denominator representing a populationat risk to experience the event. The problem for occupa-tional mortality statistics is the paucity of routinely availableinformation on the denominator. Because denominatordata are often not readily available, occupational mortalityanalyses must be carried out in terms of numerators only,that is, using proportional mortality analysis. The growingliterature on numerator analysis needs to be tapped andexplored to make effective use of occupational mortalitydata (e.g., Kupper et al. 1978).
Data quaMy-NCHS is cognizant of concerns in thisarea and is addressing these in several ways, beginning withreporting and extending through data processing to data
. 41

analysis. It is recognized that occupational mortality datacan be no better than the information reported on the deathcertificate. Thus, efforts must be directed by State vitalstatistics offices to funeral directors to provide occupationand industry of decedents in sufficient detail and validity tobe useful for analysis. To facilitate this, NCHS has workedwith NIOSH to produce a handbook that provides funeraldirectors with guidelines on reporting occupation and in-dustry of decedents (NCHS, 1983).
It has been suggested by Rothwell and others thatadditional efforts need to be made to improve the quality ofoccupational mortality data. In particular, it is suggestedthat States que~ incomplete and imprecise I/O informationreported on death certificates. This is an excellent idea, andit should be part of a national strategy to improve thequality of this information repted through the vital statis-tics system. For other items on the death certificate, NCHShas developed a set of guidelines for State querying ofdemographic items on vital recmls (NCHS, 1982). Full andsustained querying and training programs at the State levelwill be costly but they are crucial to improving the qualityof occupational information on vital records.
A firther suggestion is using followback surveys toassess the validity and reliability of occupational informa-tion on death certificates. NCHS is undertaking such aneffort by including a number of occupation questions on the1986 National Mortality Followback Survey.
Data use—National leadership in this program hasbeen emphasized in the discussions of several groups. Thiswould take several forms, including producing reports thatcan serve as models to the States for data analyses and datadissemination. It would include standardized tabulationlists, and it would recommend analytical methods. Accept-ed, standardized measures and analytical approaches areneeded in an area where, because of potentially sensitiveimplications, absence of ambiguity in measurement andanalysis is essential. A program at the national level wouldinvestigate measurement methodologies examine issues ofquality, reliability, and validity of reported information;develop resource materials for States to train funeral direc-tors on reporting these items and for querying incompleteor ambiguous entries on death records; and identi& re-sources to States for demonstration activities, includingdata use in support of occupational health programs.
Reseaxh oppo~nities—I would like to elaborate on apoint made by Dr. Anderson regarding the nature ofoccupational information from the mortality data system; Icall it the “baby bath syndrome” or “statistical myopia.” Itis the unfortunate tendency to denigrate not only occupa-tional information but vital statistics information moregenerally because of known and obvious data imperfectionsand limitations. The challenge to all of us is to exploit thisaccessible, highly standardized data set.
Statisticians and epidemiologists working in the area ofoccupational health, accustomed to working with special-ized surveys or with study cohort data, have to recognizeand to creatively overcome the limitations of the vital
statistics data base, which reflects a data collection instru-ment—the death certificate-that serves both legal andstatistical purposes. The vital statistics system is groundednot in a survey statistician’s constructs but rather in thelegal and statistical needs of State health departments.Problems of occupational mortality data identified in thisWorkshop can provide a research agenda for occupationalmortality. Among the areas to be explored are
● The absence of denominator data for some years.● The difference between occupation elicited on the
death record (“usual” occupation) and on census andU.S. Bureau of the Census sumeys (“current” occupa-tion).
. The lag between time of exposure to an occupationalhazard and related onset of death, especially for somecancers.
. The problem of migration for subnational areas, whichmay contaminate observed geographical associationsbetween occupation and mortality.
● The problem of confounding variables that may par-tially account for relationships between occupation andcause of death.
These problems, I would maintain, constitute a re-search agenda for this data base, and should not impede theproduction and use of occupational data reported on thedeath certificate.
Conclusion
The Workshop has provided, I believe, a balanced andthorough appraisal of issues associated with options forproducing occupational mortality data. Broad consensushas emerged, I believe, on an approach to provide continu-ous, detailed, and high-quality occupational mortality datathrough the existing national vital statistics system; a desireto support NCHS in obtaining appropriated funds for thispurpcxxy and a recommendation for leadership at the Fed-eral level, through research, analysis, and demonstrationactivities. The Workshop clearly can serve as the basis for amajor, sustained national thrust to develop a data base foroccupational health by exploiting existing information re-ported routinely on the death certificate of every State.
References
Kaminski,R., J. Brockert, J. Sestito, and T. Frazier. 1981. Occu-pational information on death certificates A survey of Statepractices.Ant. J. Public Health 71(5):52S-526.
Kupper, L. L., A. J. McMichael,J. J. Symons, and B. M. Most.1978. On the utility of proportional mortality analysis.J. ChronicDiseases 15:15-22,
National Center for Health Statistics. 1982.Guidelines for imple-menting field and que~ programs for registration of births anddeaths, 1983.NCHS Insbuction Manual, Part 18. Hyattsville,Md.
National Gmter for Health Statistics. 1983.Guidelines for Report-ing Occupation and Indu.my on Death Certificates. Hyattsville,Md.
42

Rosenberg, H. M., D. Bumham, R. Spirtas, and V. Valdisera. Rosenberg, H. M., J. Sestito, J. Maurer, et al. 1984. Occupation1979. Occupation and industry information from the death and industry coding from the death certificate: The recent NCHS-certificate: Assessment of the completeness of reporting. Smtkti- NIOSH experience. Paper presented to the Washington Statisticalcal Uses of Admhukirztive Recoin%With Emphasis on Motialhy and Society, Washington, D.C.Disability Reseamh, edited by L. Del Bene, and F. Scheuren.Washington: Social Security Administration.
43

Summary of recommendationsfrom participant questionnaires
Questionnaires were given to the 46 participants whodid not represent the Bureau of Labor Statistics (BLS), theNational Center for H.@th Statistics (NCHS), the NationalInstitute for Occupational Safety and Health (NIOSH), orthe National Cancer Institute (NCI). (See appendix II for acopy of the questionnaire.) Thirty-seven participants com-pleted and returned their questionnaires. The form di-rected participants to weight the 10 options by indicatingwhether they agreed or disagreed with the implementationof each option. The following is a summary of the re-sponses. These are not necessarily an unbiased sample ofthe opinions of the participants. Further, the discussion ofthe results includes interpretations by NCHS staff mem-bers.
Option Nos. 1 through 4. Occupation andindustry coding from death certificates
It is difficult to assess the industry and occupation(1/0) coding Option Nos. 1 through 4 independently be-cause many of the responses obviously considered theseoptions as one issue. The overwhelming number of respon-dents strongly agreed (36/37) with Option No. 2 (annualcoding of industry and occupation for all States). Manyrespondents identified this option as the ultimate goal ofthe system, rather than a strategy for immediate implemen-tation.
Those who strongly agreed with Option Nos. 1 (thecurrent system) and 4 (annual coding for a subset of Statesor causes) felt that these options were the most practicalapproach for current implementation but should be ex-panded to include all jurisdictions willing to participate.Th~~e were several alternatives for implementing OptionNo, 4.
. Bring States into the system as they are ready.
. Sample causes of death that may be occupationallyrelated.
. Sample certificates from all States for industry andoccupation coding.
● Sample death certificates by industry.
Those respondents who recommended implementationof the reporting system during census years only (OptionNo. 3) viewed it as a subset of Option No. 2 (full implemen-tation) and suggested major pericensal reports based onannually generated data.
Many respondent comments highlighted two importantfoci of I/O coding frosm death certificates. First, a nationalsystem is needed for surveillance, for providing impetus tothe States, developing methodologies of analysis and pre-sentation, and for guaranteeing quality and comparabilityof the data collected in the different registration areas. Thesecond focus is at the State level for developing interventionstrategies for the prevention of occupational morbidity andmortality. As one respondent summarized: “We currentlyhave no good baseline data on the magnitude of occupa-
44
tional illness in the U.S. (existing data being very poor withregard to chronic disease). State-based data are critical toState occupational health programs—for program and pol-icy planning, prioritizing of resources, and trend surveil-lance.”
Fifteen respondents (41percent) recommended thatautomated coding of industry and occupation be explored.Several participants also suggested that a quality assuranceprogram must be built into the system. Other suggestionsincluded the following
. Link 1/0 codes to specific occupational exposures,
. Establish a committee to develop a list of reasons that1/0 coding should be done.
. Fund State demonstration projects emphasizing the useof the data.
. Request continued funding from NCI.● Request funding from the Agency for Toxic Substance
and Disease Registry (ATSDR).. Request funding from Congress.
One respondent summarized several of the issues con-cerning coding death certificates as follows
Funding for the basic Vital Statistics Cooperative Pro-gram must be established before adding new compo-nents and processes.There is a need to include sufficient funding for qualitycontrol that includes followup to check the accuracy ofthe data reported.NCHS needs to develop an automated coding processso States can electronically record the literal entries forindustry and occupation.NCHS needs to provide leadership on how to present1/0 data in tabular and graphic displays.NIOSH and BLS should work with States on how tointerpret and use 1/0 specific mortality data.
Option No. 5. Mortality followback surveys
Many respondents endorsed the use of mortality fol-Iowback surveys as a valuable supplemental approach toOption Nos. 1 through 4. Although these surveys wouldhave the problem of a limited sample size, the surveys coulddirect analytic research efforts, provide extremely impor-tant information on the quality of the data collected ondeath certificates, and obtain information on covariates forspecific hypothesis testing. It was felt that the followbackstudies could not provide State-level data or generate na-tional estimates.
Option Nos. 6 and 7. Using NHANES,NHIS, or other NCHS surveys with theNational Death Index
In general, the comments on these options listed manyproblems of this approach, for instance, sample size andtime constraints. This approach should not be considered asan alternative to Option Nos. 1 through 4. However, as anad hoc basis to test certain hypotheses, the availability ofcovariate information from these data sets may make con-

sideration of mortality followup worthwhile. The problemsof the sample sizes available for specific occupation orindustxy analyses and the length of time it would take togenerate an appropriate number of deaths make theseapproaches less desirable.
Those responding to this option felt that it was impor-tant to include occupational data on the National Healthand Nutrition Examination Survey (NHANES) and theNational Health Interview Survey (NHIS). Many partici-pants left this section blank or emphasized its potentialcontribution for morbidity analyses rather than mortalityresearch. Several respondents mentioned that NCHS datashould be examined for investigating reproductive hazards.
Option No. 8. Use of the NationalLongitudinal Mortality Study (NLMS), theContinuous Work History Sample (CWHS),or Internal Revenue Service (IRS) RecordFollowup with the NDI
Many participants did not respond to these issues.Those that did indicated that these efforts certainly shouldnot distract from implementing an 1/0 coding option fromdeath certificates. Some responses were positive for usingNLMS or CWHS. Several participants raised concernsabout the availability of data for analysis. Concerns werealso raised about the quality of the occupational informa-tion available from IRS tax forms.
Option No. 9. Use of BLS Annual Surveyof injuries and illnesses (ASOII) or theSupplementary Data System (SDS) forOccupational Mortality Surveillance
Many concerns were raised about the completeness ofcoverage and the quality of these data. The annual survey
was seen as more valuable for the industries it covers andcould possibly by useful for surveillance of injuries.
Option No. 10. Use of the compressedvital statistics files
Comments ranged from “inappropriate” to “very valu-able” for identi~ing excess cause-specific mortality andmapping. Several persons commented on the value anduses of ecologic data for surveillance.
Other suggestions
Below is a list of options useful for occupational mor-tality surveillance identified on the evaluation forms:
●
●
●
●
●
●
●
●
●
●
●
●
Large sample of U.S. Bureau of the Census long forms.Data linkage “like the Swedes,” that is, the U.S Bureauof the Census linked with cancer incidence data andmortality information supplemented by followbackstudies.Use of the National Hospital Discharge Survey.Incorporation of Medical Examiners’ data for E-codedeaths into Option No. 2.Need to link mortality data with exposure informationfrom the Occupational Safety and Health Administra-tion (OSHA).Modify NDI to include cause of death.Facilitate use of IRS address file.Encourage record linkage and followup studies fordeath certificates, coroner’s reports, OSHA inspec-tions, NIOSH investigations, and workers’ compensa-tion claims.Use end-stage renal disease program data.Set aside money for State demonstration projects.Code 1/0 on NCI’S Surveillance, Epidemiology, andEnd Results cancer registry data.Use OSHA forms for research and surveillance.
45

Chapter IV.Postscripts fromsponsoring agencies
Postscript Bureau of LaborStatistics
by VWliamEisenberg,Associate Commissionerfor Occupational Safety and Health Statistics,Bureau of Labor Statistics
We, at the Bureau of Labor Statistics (BLS), are deeplycommitted to improving occupational injury, illness, andfatality statisti~ and we heartily support interagency ef-fort$ such as this Workshop, that are directed to the sameend. We are particularly happy to be here at this firstgathering under the tripartite agreement.
In the occupational illness are% BLS sponsored asymposium on various aspects of obtaining occupationalillnessdata (U.S. Department of Labor, 1985).This sympo-sium brought together officials and professional staff fromState departments of labor and State departments of health,from the National Center for Health Statistics, the NationalInstitute for Occupational Safety and Health, BLS, and theOccupational Safety and Health Administration, as well asrepresentatives of labor, business, and academia. As aresult of that symposium, a BLS-State health departmentcommittee was established to focus on ways to improvehealth and safety statistics, including fatalities.
In an effort to improve our statistics program overall,we contracted with the National Academy of Sciences for
SDexpert panel study of our data series, with fatalities amajor emphasis, to help fashion SD effective statisticalprogram for sumeillance and prevention (National Re-search Council, 1987).
As regards occupational fatalities BLS recognizesthat,if the death certificate system is to become a primarysource of this information, the quality of the industry andoccupation reporting on death certificates and the stan-dardization of industry and occupation coding are funda-mental requisites. We also recognize that, if it is to becomea viable system a common definition for “at work” fatali-ties is necessary as well as the participation of all States inthe program.
In closing I would like to express our thanks to theNational Center for Health Statistics for sponsoring thisconference, which focuses on such an important area inoccupational health and safety, and we look forward toother promising collaborative efforts under our tripartiteagreement.
ReferencesNationalResearchCouncil.1987.Counting Injurz”esand illnessesin the Workplace: Rvposats fm a Better System. WashingtonNationalAcademyPress.
U.S. Departmentof Labor, Bureau of Labor Statistics.1985.Tonwu% Impmved Measurement and Repom”ng of OccupationalIllness and Disease. $mposium Proceedings. Washington:U.S.Departmentof Labor.

Postscript: National Institute forOccupational Safety and Health
by Edward L. Baker, M.D., M.P.H., DeputyDirector, National Institute for OccupationalSafety and Health
This Workshop was important for many reasons. First,it provided an important opportunity to discuss the meritsof several options for the use of death certificates insurveillance of occupational illness and injury. Second, itprovided an opportunity for continued interaction of occu-pational health professionals interested in surveillance sys-tems. Finally, it represented an affirmation of theopportunity to improve surveillance data for occupationaldisorders. In response to this opportunity, the NationalInstitute for Occupational Safety and Health (NIOSH) iscommitted to a cxmtinued, coordinated involvement de-signed to evaluate the utility of existing approaches tosurveillance and to develop new surveillance systems. Cen-tral to this reassessment is the necessity of linking sumeil-lanee efforts with intervention programs to protect thehealth of individual workers. In this regard, I would like toreview NIOSH plans for the future.
NIOSH is committed to the development of an occu-pational health-hazard-illness-injury coding system, survey,and surveillance capability (PHS, 1986). A variety of ap-proaches are recommended along with a proposed revisionof the initial objeetive, to read: “By 1990, using the surveil-lance systems initiated by 1985, injury, illness, and mortalitytrends should be depicted for at least 10 to 15 hazards, and10 to 15 new priorities should be generated annually forpossible epidemiologic or toxicologic research.”
NIOSH injury surveillance data that are based on theBureau of Labor Statistics’ (BLS) annual survey differ fromthe results obtained from the National Electronic InjurySurveillance System sample of work-related injuries seen inemergency rooms. The reasons for these differences needto be understood. High-risk jobs need to be identified.Effective intervention pro@ams must be implemented.These steps will require the combined efforts of Federalagencies (NIOSH, BLS, the National Center for HealthStatistics (NCHS), the National Cancer Institute (NCI), theOccupational Safety and Health Administration (OSHA),and the Mining Safety and Health Administration) andState departments of health and labor. The precedent setfor Federal and State collaboration by the tripartite effortsduring this meeting points the way toward meaningful nextsteps.
Trend analysis for disease and mortality can be basedon the current efforts to adapt NCHS surveys, NHANESand NHIS, for use in occupational disease surveillance.Mortality trends for a subset of States currently part of theSurveillance Cooperative Agreements between NIOSH andthe States (SCANS) and Capacity Building States programand, eventually, for all States (the consensus of opinion atthe Workshop) form another component of the desiredsurveillance program.
The proposal made by Dr. Millar for SENSOR isdesigned to enlist medical care providers in the effort toidentitj selected occupational disorders for further re-search and intervention. The concept of sentinel physiciansalong with the effort initiated by NIOSH in 1983 to makeuse of sentinel health events (Rutstein et al., 1983) providesa means of getting primary care providers to “. . . routinelyelicit occupational health exposures as a part of patienthistory . . . “ (PHS, 1986).
Clearly, an expanded program for occupational injuryand disease surveillance will require new funding. As evi-dence of the NIOSH commitment to these efforts, therewill bean announcement soon of another round of NIOSH-State cooperative agreements, totaling about $1,000,000 infiscal year 87. It is reasonable for the States to assume thatmany of the factors that we have discussed at this Work-shop will find their way into these guidelines. Specifically,reference will be made to the concept of occupationalinjury and disease smveillance centerq the continuation ofState efforq the existence of State capabilities (in somecases working cooperatively with NIOSH staff to follow upon the leads developed from surveillance efforts); the com-mitment of NIOSH to staff consultation in addition todollars; and, in some cases, the assignment of a NIOSHEpidemic Intelligence Service officer to a State. Anotherproposal was to build on the cooperative agreements a “lineof credit” to States consisting of a specified number ofHealth Hazard Evaluations or similar forms of technicalassistance.
Because more active provider reporting of occupa-tional disorders through the Sentinel Event NotificationSystem for Occupational Risks (SENSOR) was discussedbriefly by Dr. Millar in his opening remarks, I would like totake this opportunity to describe it in greater detail.
Although many States require health providers to re-port occupational illness and injury, none maintains acomprehensive system to deteet and respond to such re-ports. Because little action is taken in response to casereports, physicians and other providers have little interest incontinuing to contribute to a reporting system that justcollects data. The SENSOR project proposes a comprehen-sive system that would utilize a network of sentinelprovidersto recognize and report selectedoccupationaldisordm to aswveillance center. The center would be responsible foranalyzing a case report and directing three types of re-sponset management of the reported case, screening forpossible disease in coworkers of the case, and evaluation ofworksite factors potentially responsible for the case. AI-though primarily useful as a surveillance system designedfor case identification, data from a SENSOR projeet couldbe used to monitor trends in the occurrence of selectedoccupational disorders within a State.
As discussed by Langmuir (1976) and by Foege andcolleagues (1976), the purpose of surveillance is not only tocollect and analyze data but also to direct active preventionprograms designed to control and, in some cases, eliminatethe occurrence of preventable disorders. In the past, anumber of States have enacted speeific regulations
47

requiring physicians and other health-care providers toreport selected occupational diseases (table 5). Unfortu-nately, in most instances, these provider reporting pro-grams were not linked to specific intervention efforts.
Table 5. Surveillance ●ctlvittes for oecupmiorml diseaee reportedby health departntents in 50 Sfatas, New York City, ●ndWashington, D.C.: 1985
Number ofdeprlrrrt?rrfsSurwwncehporllrrg
Item adhlty
Healttr-caraprcrviders. . . . . . . . . . . . . . . . . . . . . . .Mandato~reporfing . . . . . . . . . . . . . . . . . . . . . . .Volunlaryraporting. . . . . . . . . . . . . . . . . . . . . . . .PenalUaefornotreporting. . . . . . . . . . . . . . . . . . . .Sixeanlinel health evente . . . . . . . . . . . . . . . . . . . .Repotting. . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Dataanalyzad . . . . . . . . . . . . . . . . . . . . . . . . . . .Followupconducfad . . . . . . . . . . . . . . . . . . . . . . .Worker adueatbn linkerlto reporting. . . . . . . . . . . . .
31274
161978
187
SOIJW2 kwcQn d d., lee7.
Other shortcomings of provider reporting systems htwelimited their usefulness. These include the uncertaintyamong providers of the nature of a specific occupationaldisorder, that is, lack of case reporting criteria. In the caseof communicable disease reporting, developmentof report-ing criteria have greatly facilitated the epidemiologic inves-tigation of selected conditions (Thacker et al., 1983).Another limitation of existing occupational disease report-ing systems, which is similar to that observed in communi-cable disease reporting (CDC, 1987), is the lack of adefined network of sentinel providers who have responsibil-ity to report selected conditions to an appropriate Stateagency. Finally, in most States, the resources needed tor=eive, anal~e, and direct a response to a provider reportare minimal or lacking.
To address these-limitations, a uniform provider re-porting system will be developed for use by States toperform active surveillance of selected occupational condi-tions. The SENSOR system will build on previous experi-ence of State health and labor departments. To someextent, prior support from NIOSH has contributed to thedevelopment of this capacity.
The SENSOR system will consist of two organizationalcomponents (figure 3). First, a network of sentinel provid-ers, individual practitioners of clinic groups, will be devel-oped. The function of the sentinel provider network will beto recognize and report cases of selected occupationaldisorders. The second component, a surveillance center,will receive the report from the provider, analyze the data,and direct action toward the individual cases, coworkers ofthe case, and to the workplace. In addition to fulfilling acentral role in the coordination of response to providerreports of occupational disorders, the center would providetechnical consultation in a wider variety of occupationalhealth issues (for example, surveillance using vital records,hospital discharge records, or workers’ compensation filesto monitor trends of occupational disorders). Because State
Recognition
n
SentinelProvider
Reporting
I
*
nSurveillance
AnalysisCenter
Action
/1143
BmlxI
Figure 3. Sentinel event notification system for occupational risks(SENSOR): 1987
health departments and labor departments have variable,shared responsibilities in occupational safety and health,the creation of a surveillance center will serve to unitecomplementary programs that currently exist in relativeisolation.
To facilitate the recognition of selected occupationalconditions by the sentinel provider network, NIOSH willdevelop and maintain a list of conditions that lend them-selves to provider reporting. To the greatest extent feasible,such conditions should be attributable to work in a highpercentage of cases, reasonably frequent, easily diagnosableby practitioners having no access to sophisticated diagnostictests, of reasonably short latency, and potentially reversiblefollowing case identification.
In addition to developing a list of conditions, NIOSHwill develop a set of reporting criteria that can be used bypractitioners to facilitate recognition. Such criteria are to beused for the purposes of improving provider recognition ofselected occupational conditions and enhancing uniformreporting between different regions of the country. Analy-ses of these case reports will provide useful informationregarding the characteristics of selected occupational con-ditions, their sequelae, and other important and clinicalepidemiologic features.
Reporting by providers to State health departments hasrelied on a passive system in which the provider is encour-aged to mail in reports of cases using forms developed bythe requesting agency. In view of the recent advances incomputer technolog and telecommunication techniques,other alternatives exist for transferring information fromproviders to a central surveillance center. To facilitate amore active transmission of data from providers to a centralsurveillance center, NIOSH will support the developmentof computer technology that would allow for the transmis-sion of data on suspected cases from providers to the centerfor analysis and possible response.
48

Utilizing staff epidemiologists, statisticians, and otheroccupational health professionals, the surveillance centerwill analyze cases reported from the provider network anddetermine whether additional actions are appropriate. Inmany States, opportunities exist for disseminating the re-sults of such analyses through publications directed atpublic health professionals, physicians, and other profes-sionals. The results of such analyses may also be appropri-ate for inclusion in the Centers for Disease Control’sMorbidity and Mortality WeekZy Repoti.
Three types of action could result from the receipt of a
definite case report. First, individual case managementrecommendations will be developed by NIOSH for theconditions to be placed under active surveillance. Suchguidelines will be made available to practitioners reportingthese cases as a form of consultative assistance. The secondtype of action will be directed at coworkers of the case.Because coworkers with similar workplace exposures maybe at risk for the development of occupational illness orinjury similar to that experienced by the case, medicalevaluation of such workers to detect early, potentiallyreversible health disorders is appropriate. Finally, actiondirected at specific workplace causes will be coordinated bythe surveillance. center in response to the report of anindividual case. In view of the variable capacity of Stateprograms tb control occupational safe~ and health hazards,local resources will be examined to determine the mostappropriate mechanism for directing such worksite action.
Provider reporting systems have been in effect in anumber of States for many years, but because of variousshortcomings, have not developed active surveillance ofoccupational illness and injury. To achieve a more uniform,active approach to provider reporting, SENSOR will becreated as a cooperative State-Federal effort designed todevelop local capability for the recognition, reporting, andprevention of selected occupational disorders. To demon-strate the feasibility of this approach, NIOSH will fund asti’all number of SENSOR projects in fiscal year 87. Ulti-mately, joint State-Federal support will be essential tomaintaining SENSOR activity within a State.
SENSOR should not be viewed as the sole approach tothe surveillance of occupational illness and injury. Otherapproaches to the identification of cases of occupationalillness or injury and to monitoring trends of occurrence ofthese disorders have been developed by NIOSH and someStates and will continue to function (Frazier, 1985;Halperin and Frazier, 1985). These programs will addressother of the six objectives enunciated by NIOSH for im-proving surveillance in the future
● Improve hazard surveillance.● Develop uniform approaches for using existing health
data sources.. Disseminate information and share methodology.. Perform surveillance for Leading Work-Related Dis-
ease and Injuries.
In closing, in my view we are presented with an unusualopportunity for improving surveillance data for occupa-tional illness and injury. This can only be accomplished by acollaborative effort involving NIOSH and other Federaland State agencies committed to improving the collection ofaccurate data and, more importantly, a direct interventionprogram designed to improve the health of the U.S. work-force. I am convinced that through the activities, such asthis Workshop, which have been organized over the pastseveral months, we will achieve a dramatic improvement inthe surveillance of occupational illness and injury for thiscountry.
References
Centers for Disease Control. 1987. Comprehensive SurveillancePlan. Washingtorr U.S. Department of Health and Human Servic-es, Public Health Service, Centers for Disease Gmtrol.
Foege, W. H., R. Hogan, and L. H. Newton. 1976. Surveillanceprojects for selected diseases. ht. 1 Epidemiol. 5(1):29-37.
Frazier, T. M. 1985. Occupational health reporting systems–U.S.A.A 1 Industr. Med. 8441-446.
Halpenn, W. E., and T. M. Frazier. 1985. Smveillance for theeffects of workplace exposure. Annu, Rev. Public Healtiz 6419-432.
Langmuir, A. D. 1976. William Fam Founder of modem conceptsof surveillance. ht. J. Epidemiol 5(1):13-18.
Muldoon, J. T., L. A. Wintermeyer, J. A. Eure, et al. 1987. Stateactivities for swveillance of occupational disease and injury.Surveillance Summaries. Washin~om U.S. Department of Healthand Human Services, Public Health Service, Centers for DiseaseControl.
Public Health Semite. 1986. The 1990 Heaith Objectives for theNation: A Midcourse Review. Washington: U.S. GovernmentPrinting Office.
Rutstein, D. D., R. J. Mulhm, T. M. Frazier, et al. 1983. Sentinelhealth events (occupational): A basis for physician recognitionand public health surveillance. An 1 Public Health 76(9):1054-1062.
Thacker, S.B., R. Choi, and P.S. Brachman. 1983. The surveillanceof infectious disease. JAiM4 249(9):1181-1185.
. Develop a model occupational disease reporting systemfor health care providers (SENSOR),
. Incorporate occupational health issues into nationaland regional surveys.
49

Postscript Nationai Center forHealth Statistics
by Manning Feinleib, M.D., Dr. P.H., Director,National Center for Health Statistics
As evidenced by these Proceedin~ this Workshop wasquite sueeessful, bringing together experts from Federaland State ageneie$ Congresq academia, indushy, and laborto evaluate a wide range of options for studying occupa-tional effects on mortality. I would like to thank membersof the National Center for Health Statistics’ (NCHS) staff,in particular, Drs. Patricia Buffler, Bruce Cohen, and HarryRosenberg for organizing the Workshop. Further, with thehelp of other participants, a great deal of effort was devotedto carefully drafting and documenting the options pre-sented to the Workshop. Finally, the format for the pro-gram that allowed a long working group time wassuccessful in generating vigorous discussion that could onlybe briefly recounted in the working group reports.
NCHS will take all of the reeommendations underadvisement. There appears to be consensus that the goalshould be the eventual nationwide coding of industry andoccupation on the death eertiikates. The achievement ofthis goal will not be simple. As was noted before, not allStates code this information. Therefore, an educationalinitiative is needed to make the States aware of the value ofindushy and occupation information on the death certifi-cate. Such an initiative would be best accomplished by theinstitutions that are devoted to the study of the working
population and occupational health, including not only theDepartment of Labor, the National Institute for Occupa-tional Safety and Health, the National Institute of Environ-mental Health Sciences, the Environmental Prot-”onAgency, and the Agency for Toxic Substances and DiseaseRegistry, but also labor and industrial groups.
The value of occupation and industry coding wouldbecome clearer if there were more studies available thatdemonstrate their use. There are a few, by now elassi@studies that demonstrate the utility of some kinds of data.But new analyses and new ways of combining data fromdifferent sources are needed to expand the usefulness ofthe data that already are available. This work can beaccomplished by the academic community working with thevarious State and Federal agencies.
The Memorandum of Understanding that was signedat this Workshop encourages collaboration in the analysesof data and in planning and implementation of programs topromote and expedite collection of information essentialfor improving occupationally related health. Within NCHS,our occupational program will emphasize the analysqs ofmultiple sets of data already available and a coordinatedapproach to the collection of data in the future. In addition,NCHS will continue to stren@hen its capabilities to provideusers with data relevant to subnational problems throughprograms such as benchmark communities or model-basedestimation for small area data analyses. Finally, on theadvice of this Workshop, we will evaluate ways to obtainfunding to continue and improve the collection of theindustry and occupation coding from death certificates.
50

Appendixes
I. Memorandum of understanding . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52
IL Workshop participant questionnaire . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53
III. Workshop participants . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59
51

Appendix LMemorandum ofUnderstanding
Among the Bureau of Labor Statistics, theNational Center for Health Statistics, and theNational Inat”Wte for Occupational Safety andHealth
L Purpose
In response to the need to improve occupational health andsafety information, the Bureau of Labor Statistics (BLS),the National Center for Health Statistics (NCHS), and theNational Institute for Occupational Safety and Health(NIOSH) enter into this Memorandum of Understandingfor the primary purpose of developing collaborative plansfor improving occupational illness and injury reportingsystems and surveys.
Il.
1.
2.
3.
4.
5.
6.
Provisions and goals
Exchange data and information relevant to respectiveagency programs, capabilities, and needs.As necessary, collaborate on the development of issuepapers psition papera proposals, and projects ofmutual ctmcem and interest.Identi& program areas where tripartite assistance orsupport is needed and identify
● kinds of assistance or support needed● when needed● resources involved.
For projects or propos~s submitted for official approval of joint agen~ heads, develop funding andresource requirements and timetables for implementa-tion.Jointly pursue the cooperation of other agencies in theimplementation of projects or proposals where involve-ment of other Federal and State agencies is required.Develop options that promote the recognition andreporting of occupational illnesses and injuries.
7.
8.
Develop options that promote and expedite obtaininginformation essential for improving health and safetyreporting systems, sumey~ and data.Collaborate in phmnin~ sponsorin~ and conductingseminars, conferences, or similar forums of discussionto exchange information, resolve problems, reptprogress, and so forth.
Ill. Performance requirements
A.
B.
c.
Designation of representative(s)
Each agenq will designate a person or persons tocoordinate and carry out the provisions outlined in thisMemorandum of Understanding. The agency represen-tatives are as follows Ronald W. Wilson (NCHS);Edward L. Baker, M.D. (NIOSH); and William M.Eisenberg (BLS).
Meetings
To accomplish the purpose and goals defined in thisMemorandum of Understanding the joint agency rep-resentatives will meet regularly (at least semiannually).In the planning development, and execution of projectsproposed under this tripartite agreement, meetings onsuch projects involving agencies not party to this agree-ment will be jointly attended.
Notification
The joint agenq representatives will make oral orwritten reports as requested by joint agenq officials.All written communications pertaining to joint projectwork will be mutually exchanged and copies of suchcommunications will be sent to agency heads or theirrepresentatives, as appropriate.
52

Amendix Il.Workshop participantquestionnaire
OCCUPATIONALMORTALITYDATAMORKSHOP:
Option Preference Questionnaire
The purpose of this questionnaire is to determirieyour personal preference foroption? that NCHS might implement to produce occupational mortality statisticsa$ part of its ongoing. program (or’ encourage other agencies in their datacollection efforts). Please circle how strongly you agree or disagree with eachoption for this purpose.
Please CircleStrongly StronglyDisagree A!lE9
Industry/Occupation Coding on Death Certificates
Option 1: Use existing system
Option 2: Use annual 1/0 coding for all States
Option 3: Use pericensal approach
Option 4: Use annual, for subset of causes and/orsubset of States (please specify)
Cmmnents:
Use ofNCHS Surveys for Followup
Option 5: Use mortality followback surveys
12 345
12345
12345
12345
12345
Caunents:
53

Option 6a: Followup MANESsurveys using NDI
Cmnents:
-.Option 6b: FOI’1OWUPNHISsu’rveys using NDI
Cmuents:
Option 7: Followup other NCHS Surveys using NDI(PI ease specify)
Please CircleStrongly Stron91yDisa&e@ &9B- -
12 345
12 345
12 345
Comments:
54

Please CircleStrongly StronglyDisagree A9Jx!2
Other Data SourcesOption 8a: Use National Longitudinal Mortality Study 12345
Cmunents:
Option 8b: Use Continuous Work History Sample
Cmnents:
Option 8c: Use IRS Record Followup with NDI orother data systems (please specify)
12345
12345
Cements:

Please CircleStrortgly StronglyDisagree &
Option 9iJ: Use BLS Annual Survey of Illness and 12 345Injury for occupational mortality surveillance
Conments:
Option 9b: Use Supplementary Data System (BLS) and/orother workers’ compensation data systems
Comments:
Option 10: Use Compressed Mortality File
Corments:
Option 11: Other options (please specify)
Cournents:
12 345
12345
12345

11. The purpose of this section is to identify your preference for differentoptions or groups of options under varying resource constraints. Pleaseuse the option numbers designated below, our discussions in the workinggroups, and reasonable cost estimates to design a program given the fundingconstraints:
Option 1Option 2Option 3Option 4Option 5Option 6aOption 6bOption 7Option 8aOption 8bOption 8COption !?aOption 10Option 11
Existing 1/0 Coding on Death CertificatesAnnual 1/0 Coding for all StatesPericensal approachSubset of causes and/or subset of StatesMortality folJowback surveysFollowback of NHANES using NDIFollowback ofNHIS using NDIFollowback of other NCHS surveys using NDINational Longitudinal Mortality SurveyContinuous work History Sample followup using NDIIRS record followup or other data system (please specify) using NDIAnnual Survey of Occupational Illness and Injury (BLS)Compressed Mortality FileOther options (please specify)
1. What option or group of options should be implemented if less than $400,000per year for funding is available?
2. What option or group of options should be implemented if between $400,000-$800,000 is available?
57

3. What option or group of options should be implemented if between $800,000-$1,200,000 is available?
4. What options should be implemented if there are no financial constraints?
III. This is an opportunity for you to provide any additional comnents on theworkshop.
A. Are there additional options that you feel NCHSshould explore?
f). Additional comments.
58

Appendix111.Workshop participants
Dr. Henry AndersonWisconsin Divisionof HealthP.O. Box 309Madison, Wisconsin 53705
Faye AzizSocial Security Administration1875 Connecticut Avenue, NWRoom 320-DWashington, DC 20009
Dr. Edward BakerAssistant Director, National Institute ofOccupational Safety and Health
Room 3007 Building 1Centers for Disease Control1600 Clifton Road, NEAtlanta, Georgia 30333
Dr. Gilbert BeebeNational Cancer InstituteRoom 8C41 Landow Building7910 Woodmont AvenueBethesda, Maryland 20892
Robert BilgradNatiomd Center for Health Statistics3700 East-West HighwayHyattsville,Maryland 20782
Dr.’Aaron BlairOccupational Studies SectionNational Cancer InstituteRoom 4C16 Landow Building7910 Woodmont AvenueBethesda, Maryland 20892
Fred BlosserOccupational Safety andHealth Reporter
The Bureau of National Affairs, Inc.1231 25th Street, NWWashington, DC 20037
Dr. Greg BondDow Chemical Company1803 BuildingMidland, Michigan 48674
Dr, Demis BregmanSurveillanceBranchNational Institute for OccupationalSafety and Health
4676 Columbia ParkwayR-18Cincinnati, Ohio 45226
John E. BrockertDirector, Bureau of Health StatisticsUtah Department of HealthP.O. BOX 16700Salt Lake City, Utah 84116-0700
David BrownSurveillanceBranchNational Institute for OccupationalSafety and Health
4676 Columbia ParkwayR-18Cincinnati, Ohio 45226
Warren BucklerDirector, Division of StatisticalOperations and Services
Officeof Research and StatisticsSocial Security AdministrationRoom 2B2 Operations Building “6401 Security BoulevardBaltimore, Maryland 21235
Dr. Patricia BufflerProfessor, Epidemiology Research UnitUniversity of Texas School of Public HealthP.O. BOX 20186Houston, Texas 77225
carol BurnettSurveillanceBranchNational Institute for OccupationalSafety and Health
4676 Columbia ParkwayR-18Cincinnati, Ohio 45226
Dr. Harvey CheckowayRes. Assoc. Professor of EpidemiologyDepartment of EpidemiologyUniversityof North CarolinaChapel Hill, North Carolina 27514
Dr. Bruce CohenNational Center for Health Statistics3700 East-West HighwayHyattsville,Maryland 20782
Dr. John A. CooperChief, IMmmural Programs BranchNational Cancer InstituteLandow Building7910 Woodmont AvenueBethesda, Maryland 20892
59

Dr. Deborah DawsonDivision of Health Intemiew StatisticsNational Center for Health Statistics3700 East-West HighwayHyattsville, Maryland 20782
Karen M. DeasyOffice of the Dircetor, NIOSHRoom 714B HHH Building200 Indepcndenee Avenue, SWWashington, DC 20201
Dr. Eliibeth DelzellAssistant Professor of EpidemiologyUniversity of Alabama at Birmingham209 Tidwell HallBirmingham, Alabama 35294
Dr. Ernest M. Dixon6305 Evermay DriveMclean, Virginia 22101
Gwendolyn DoebbertHealth Data and Statistics BranchDepartment of Health Serviees7144 P StreetSacramento, California 95814
Joseph DuBoisMathematical StatisticianU.S. Department of LaborOSHA - Room N3626200 Constitution Avenue, NWWashington, DC 20210
William EisenbergAssociate Commissioner for
Occupational Safety and Health StatisticsBureau of Labor StatisticsRoom 4014 Patrick Henry Building601 D Street, NWWashington, DC 20212
Dr. William FaymweatherManager, Epidemiology SectionE.I. DuPont deNemours and CompanyN 11510Wilmington, Delaware 19898
Dr. Jacob FeldmanDirector, Office of Analysis and
EpidemiologyNational Center for Health Statistics3700 East-West HighwayHyattsville, Maryland 20782
Dr. Ralph FrankowskiProfessor of BiometryUniversity of TexasHealth Sciences Center at HoustonSchool of Public HealthP.O. BOX 20186Houston, Texas 77225-0186
Dr. Todd FrazierSurveillance BranchNational Institute for Occupational
Safety and Health4676 Columbia ParkwayR-18Cincinnati, Ohio 45226
Frank FrodymaActing Director of PolicyU.S. Department of LaborOccupational Safety and HealthAdministration
Room N3626200 Constitution Avenue, NWWashington, DC 20210
Dr. John FroinesAssociate ProfessorDivision of Occupational Health
and Environmental ScieneesSchool of Public HealthUniversity of California at Los AngelesLos Angeles, California 90024
Eric FmminHealth and Safety DepartmentAmeriean Confederation of TextileWorkers’ Unions
15 Union SquareNew Yorlq New York 10003
George GayNational Center for Health Statistics3700 East-West HighwayHyattsville, Maryland 20782
“Lillian GuralnickNorth 63510 N Street, SWWashington, DC 20004
Hawey HilaskiBureau of Labor StatisticsRoom 4014 Patrick Henry Building601 D Street, NWWashington, DC 20212
Dr. Patricia HoncharBureau of EpidemiologyTexas State Department of Health1100 W. 49th StreetAustin, Texas 78756
Allan HoskinManager, Statistics DepartmentNational Safety Council444 N. Michigan AvenueChicago, Illinois 60611
Edward HunterPlanning and Evaluation OfficerOffice of Program Evaluation and PlanningNational Center for Health Statistics3700 East-West HighwayHyattsville, Maryland 20782
60

Robert IsraelDeputy DirectorNational Center for Health Statistics3700 East-West HighwayHyattsville,Maryland 20782
Deborah KeimigCommittee on National StatisticsNational Academy of Sciences2101 Constitution Avenue, NWWashington, DC 20418
Dr. Carl A. KellerNational Institute of EnvironmentalHealth Sciences
Room 2B55, Building 31Bethesda, Maryland 20892
Barbara KerrOfficeof the Center DirectorNational Center for Health Statistics3700 East-West HighwayHyattsville,Maryland 20782
Karl KroncbuschU.S. CongressOfficeof TechnologyAssessmentWashington, DC 20510
Dr. Philip LandriganProfessor of Community Medicine andDirector, Division of Environmental andOccupational Medicine
Mt. Sinai School of MedicineNew Yorl$ New York 10029
Dr. David LilienfeldAssistant Professor of CommunityMedicine
Divisionof Environmental andOccupational Medicine
Mt. Sinai School of MedicineNew York New York 10029
Dr. Jay ImbinNational Cancer InstituteLandow Building7910 Woodmont AvenueBethesda, Maryland 20892
Dr. Thomas MasonNational Cancer InstituteRoom 3A06 Landow Building7910 Woodmont AvenueBethesda, Maryland 20892
Jeffrey MaurerNational Center for Health Statistics3700 East-West HighwayHyattsville,Maryland 20782
Dr. James M. MeliusDirector, Division of SurveillanceHazardEvaluations and Field Studies,
NIOSH4676 Columbia Parkway - R-18Cincinnati, Ohio 45226
Dr. Samuel MilhamDepartment of Health and Human Services -ET 13State of Washington GovernmentOlympia,Washington 98504
Dr. J. Donald MillarDirector, NIOSHRoom 3007 Building 1Centers for Disease ControlMOOClifton Road, NEAtlanta, Georgia 30333
Dr. Michael Mo]]National Institute for Occupational Safetyand Health
Morgantown, West Virginia
Dr. Robert J. MullanDivision of Surveillance,HazardEvaluations and Field Studies
National Institute for OccupationalSafety and Health
4676 Columbia ParkwayCincinnati, OH 45226
Melvin L. MyersDirector, Officeof Program Planningand Evaluation,
NIOSHRoom 3040 Building 1Centers for Disease Control1600 Clifton Road, NEAtlanta, Georgia 30333
Raymond D. Nashold, Ph.D.Director, Center for Health Statisticsand State Registrar
Divisionof HealthP.o. Box 309Madison, Wisconsin53701
Dr. Janet NorwoodCommissionerBureau of Labor Statistics441 G Street, NWWashington, DC 20212
John PattersonDirector, Division of Vital StatisticsNational Center for Health Statistics3700 East-West HighwayHyattsville,Maryland 20782
Dr. Dennis PerrottaDirector, Epidemiology DivisionBureau of Epidemiolo~Texas State Department of Health1100 W. 49th StreetAustin, Texas 78756
William G. Phillips417 6th Streetj SEWashington, DC 20003
61

Dr. Gail PoeOffice of Associate Director of Vital andHealth Statistics Systems
National Center for Health Statistics3700 East-West HighwayHyattsville, Maryland 20782
Dr. Earl PollackNational Academy of Sciences2101 Constitution Avenue, NWWashington, DC 20418
Dr. Patricia PotrzebowskiDirector, Division of Health Statistics
and ResearchP.O. Box 90Harrisburg Pennsylvania 17108
John PriebeLabor Force Statistics BranchPopulation DivisionU.S. Bureau of the CensusWashington, DC 20237
Dr. Harry M. RosenbergChief, Mortality Statistics BranchNational Center for Health Statistics3700 East-West HighwayHyattsville, Maryland 20782
Charles J. RothwellFormer DirectorState Center for Health StatisticsPost officeBox 2091Raleigh, North Carolina 27602
Dr. Linda RudolphChief, Occupational Health Sumeillance
and Evaluation ProgramCalifornia Department of Health Services2151 Berkeley WayBerkeley, California 54704
Peter SailerStatistics of Income Division, DRSTInternal Revenue ServiceWashington, DC 20224
Dr. David SavitzAssistant Professor of EpidemiologySchool of Public HealthUniversity of North CarolinaChapel Hill, North Carolina 27514
Fritz ScheurenStatistics of Income Division, DRSTInternal Revenue SemiteWashington, DC 20224
Dr. Joseph SchwerhaDirector, Industrial MedicineU.S. SteelRoom 25816(XIGrant Street ‘Pittsburgh, Pennsylvania 15230
Thomas SCOURLabor For=” statistics BranchPopulation DivisionBureau of the CensusWashington, DC 20237
Dr. John SestitoSurveillance BranchNational Institute for
Occupational Safety and Health4676 Columbia ParkwayR-18Cincinnati, Ohio 45226
Dr. Michael SilversteinAssistant Director of Health and SafetyUAW Health and Safety Department8000 E. JeffersonDetroit, Michigan 48213
Dr. Robert SpirtasEnvironmental Epidemiology BranchOccupational Studies SectionRoom 4C16 Landow BuildingBethesda, Maryland 20205
Elsie StantonNationaJ Center for Health Statistics3700 East-West HighwayHyattsville, Maryland 20782
Dr. Alice StarkBureau of Environmental Epidemiology
and Occupational HealthNew York State Department of HealthRoom 742 ESP Tower BuildingAlbany, New York 12237
George StellutoBureau of Labor Statistics441 G Street, NWWashington, DC 20212
Dr. William StewartAssistant Professor of EpidemiologyOccupational Epidemiology ProgramJohns Hopkins School of HygieneRoom 6033615 N. Wolfe StreetBaltimore, Maryland 21205
Sabrina SturbaNational Center for Health Statistics3700 East-West HighwayHyattsville, Maryland 20782
George VanAmburgState Registrar3500 N. Logan StreetP.O. Box 30035Lansing Michigan 48909
62

Dr. Diane WagenerBoard on Environmental Studiesand Toxicology
National Academy of Sciences2101 Constitution Avenue, NWWashington, DC 20418
Dr. Bailus WalkerCommissionerMassachusetts Department of
Public Health150 TremontBoston, Massachusetts 02111
Lacola WashingtonNational Center for Health Statistics3700 East-West HighwayHyattsville, Maryland 20782
Dr. James WeeksDeputy Administrator for Occupational HealthUnited Mine Workers of America900 15th Street, NWWashington, DC 20005
Ronald W. WilsonDirector, Division of Epidemiology andHealth Promotion
National Center for Health Statistics3700 East-West HighwayHyattsville, Maryland 20782
Janice WindauBureau of Labor StatisticsRoom 4014 Patrick Henry Building601 D Street, NWWashington, DC 20212
Diana ZuckermanHouse Government Operations CommitteeSubcommittee on Intergovernmental Relations
and Human ResourcesB372 Raybum House Office BuildingWashington, DC 20515
63
wLS. Oovemunt Printing OffLee 1988$ 201-855/80006

Vital and Health Statisticsseries descriptions
SERIES 1.
SERIES 2.
SERIES 3.
SERIES 4.
SERIES 5.
SERIES 10.
SERIES 11,
SERIES 12.
SERIES 13.
Programa and Collation Procaduras—Reports describingthe general programs of the National Center for HealthStatistics and its offices and divisions and the date col-
lection methods used. They also include definitions andother material necesssry for understanding the data.
Data Evaluation and Mathoda Reaaarch—Studies of newstatistical methodology including experimental tests of
new survey methods, studies of vital statistics collectionmethods, new analytical techniques, objective evaluationsof reliability of collected data, and contributions tostatistical theory. Studies also include comparison of
U.S. methodology with those of other countries.
Analytical and Epidemiological Studies— Repotis pre-senting analytical or interpretive studies based on vital
and heelth statistics, carrying the analysis further thanthe expository types of reports in the other series.
Documants and Committaa Reports-Final repons ofmajor committees concerned with vital and health sta-
tistics and documents such as recommended model vitalregwtration laws and revised birth and death certificates.
Comparative Intamational Vial and Haalth StatisticsReports-Analytical and descriptive reporw comparingU.S. vital and health statistics with those of other countries.
Data From tha National Health Interview Survay-Statis-tics on illness, accidental injuries, disability, use of hos-pital, medical, dental, and other services, and other
haalth-ralated topics, all based on data collected in thecontinuing national household interview survey.
Data From tha National Health Examination Survay andtha National Health and Nutrition Examination Survey—Data from direct examination, testing, and measurementOf national sampie.s of th,e civilian noninstitutionaliz~d
population provide the basis for (1) estimates of themedically defined prevalence of specific diseases in the
United States and the distributions of the populationwith respect to physical, physiological, and psycho-logical characteristics and (2) analysis of relationships
among the various measurements without reference toan explicit finite universe of persona.
Data From tha Inatitutionaliied Population Survays-Dis-continued in 1975. Reports from these surveys are in-
cluded in Series 13.
Data on Haalth Ro~ourcas Utilization—Statistics on theutilization of health manpower and facilities providing
long-term care, ambulato~ care, hospital care, and familyplanning servicas.
SERIES 14.
SERIES 15.
SERIES 20.
SERIES 21.
SERIES 22.
SERIES 23.
Data on Health Rasourcea: Manpower and Facilitiaa—Statistics on the numbers, geographic distribution, andcharacteristics of health resources including physicians,
dentists, nurses, other health occupations, hospitals,nursing homes, and outpatient facilities.
Data From Special Surveys-Statistics on health andhealth-related topics collected in special surveys that
are not a part of the continuing data systems of theNational Center for Health Statistics.
Data on Mortality-Various statistics on mortality otherthan as included in regular annual or monthly reports.
Special analyses by cause of death, age, and other demo-graphic variables; geographic and time saries analyses;and statistics on characteristics of deaths not availablefrom the vital records based on sample surveys of those
records.
Data on Natahty, Marriage, and Divorce-Various sta-tistics on natality, marriage, and divorce other than asincluded in regular annual or monthly reports. Special
analyses by demographic variables; geographic and time
series analyses; studies of fertility; and statistics oncharacteristics of births not available from the vital
records based on sample surveys of those records.
Data From the National Mofiality and NatalitySurveya—Disoontmuedin 1975. Reports from these sample surveysbased on vital records are included in Series 20 and 21,respectively.
Data From tha National Survey of Family Growtft-Statistics on fertility, family formation and dissolution,family planning, and related maternal and infant healthtopics derived from a periodic survey of “a nationwide
probability sample of women 15-44 years of age.
For answers to questions about this report or for a list of titles ofreports published in these series, contact:
Scientific and Technical Information Branch
National Center for Health Statistics
Centers for Disease ControlPublic Health ServiceHyattsville, Md. 20782
301-436-8500

U.S. DEPARTMENT OF HEALTH ANDHUMAN SERVICES
Public Health SemlceCenters for Dmease ControlNational Center for Health Stawxlcs3700 East-West HighwayHyattsville, Maryland 20782
OFFICIAL 8USINESSPENALTY FOR PRIVATE USE, S300
THIRD CLASS MAILBULK RATE
POSTAGE & FEES PAIDPHSINCHS
PERMIT No. G-281
DHHS Publication No. (PHS) 88-1463, Series 4. No. 26