Acoustic data logging protocols and procedures for commercial ...

OCCUPATIONAL HEALTH & WELLBEING SERVICE
PROCEDURES & PROTOCOLS FOR OCCUPATIONAL HEALTH
TUBERCULOSIS SCREENING
OHWS-SOP 01
PREPARED BY
Cepta Byrne Deputy Head of Occupational Health Service
APPROVED BY
David Maslen-Jones Head of Occupational Health & Wellbeing Service
ISSUE AND REVISION RECORD
Date Issue No. Details Review date 02/2007 01 New document 08/2010 02/2012 02 Reviewed

OCCUPATIONAL HEALTH & WELLBEING SERVICE
PROCEDURE FOR TUBERCULOSIS SCREENING
Procedure Statement Southend University Hospital NHS Foundation Trust is committed to providing a safe and healthy environment for its staff and patients. This procedure sets out the screening and vaccination process for the protection of staff against Pulmonary Tuberculosis (TB). It is recognised that TB is an infectious disease for which there is a safe and effective vaccine available. Southend University Hospital through its Occupational Health & Wellbeing Service (OH) will assess staffs susceptibility to TB and offer appropriate vaccination and screening as required. This procedure is written in line with the National Institute for Health and Clinical Excellence (NICE) Tuberculosis Clinical diagnosis and management of tuberculosis and measures for its prevention and control and the full guidelines as published by the National Collaborating Centre for Chronic Conditions, and the Department of Health (Green Book) Immunisation against Infectious Disease 2006. Ownership The Occupational Health & Wellbeing Service is responsible for the implementation, review, amendment and re-issue of this document. Frequency This procedure will be reviewed every three years in accordance with legislative requirements or if authoritative medical opinion changes. Background Tuberculosis (TB) is a disease caused by the bacteria mycobacterium tuberculosis. It is spread by droplets coughed or sneezed by someone with infectious tuberculosis. Once inhaled the bacteria reach the lungs and grows slowly over several weeks. In over 80% of people the immune system kills the bacteria and they are removed from the body. In a small number of cases a defensive barrier is built round the infection and the TB bacteria are not killed and lie dormant. This is called latent tuberculosis; the person is not ill and is not infectious. Sometimes at the time of the initial infection bacteria gets into the blood stream and can be carried to other parts of the body such as bone, lymph glands or the brain before a defensive barrier is built. One third of the world’s population, roughly two billion people have latent tuberculosis.
Primary infection can be acquired by inhaling infected microscopic droplets from a person with TB of the lungs.
Health care workers may, because of the nature of their work, be more exposed to TB and some patients may also be more susceptible to infection, in particular:
Southend University Hospital NHS Foundation Trust Plus
Those who are close contacts of an infectious case.
Those who have lived in, travel to, or receive visitors from places where TB is still very common.
Those who live in ethnic minority communities or originating from places where TB
is very common.
Those whose immune systems are weakened by HIV infection or other medical problems.
The very young and elderly, as their immune systems are less robust.
Those with chronic poor health and nutrition because of lifestyle problems such as
homelessness, drug abuse or alcoholism.
Those living in poor or crowded housing conditions including living in hostels. Once a person becomes infected they may:
Have active disease with associated symptoms.
Clear the bacterium spontaneously.
Not present symptoms at the time of infection but the disease may reactivate some years later.
Notification of TB in England and Wales was implemented in 1913. Reaching its lowest number in the mid 1980s, but in recent years there has been a steady increase. The disease is more common in areas of the world where poverty, malnutrition, poor general health and social disruption are present. The increase in the UK is thought to be due to the HIV epidemic, immigrants coming from countries with high rates of infection or inadequate health provision and the decline in recent years of control programmes such as school vaccination schedules. The last few years have also seen an increase in the number of drug resistant strains of TB which makes treating the disease more challenging and strengthens the argument for ensuring unprotected health care workers are offered screening. Clinical Features of TB The onset of TB is generally insidious with infection proceeding for some time before the person becomes sufficiently ill to seek medical advice. Clinical manifestations are variable – fatigue, weight loss, weakness, night sweats, and fever are all associated with TB. When infection occurs in the lungs, there is a characteristically chronic cough and production of sputum that may be blood stained. A diagnosis of pulmonary TB is confirmed by chest x-ray and microbiological sputum testing. Definite diagnosis is achieved by culturing the TB bacterium from samples. This not only confirms the diagnosis but shows which of the TB drugs the bacterium is sensitive to. TST (Mantoux Test) and interferon gamma test (IGT) can show if someone has been exposed to TB and may have latent infection.

Definitions BCG The Bacillus Calmette-Guerin (BCG|) vaccine was introduced for general use in 1953. It is a live vaccine, administered by intra-dermal injection into the upper arm. It has been shown to have an efficacy rate of about 80%. Incidence of active disease in vaccinated individuals is very rare but it can occur. Mantoux Test A skin test which uses a small dose of purified protein derivative of tuberculin and is injected intra-dermally into the forearm, and read 48-72 hours after the test.. Interferon-Gamma Test (IGTs) – Involves taking a blood sample, which is processed by the laboratory department. Accountability Occupational Health & Wellbeing Service is responsible for:
Ensuring the TB status of all new employees to the NHS who have contact with patient or clinical material are established and recorded, prior to starting work.
Ensuring health care workers are offered chest X-ray, TB skin testing and BCG
vaccines as required.
Being a source of advice to staff and managers on the occupational factors associated with TB.
Recruitment – Medical Staffing Ensuring that employees new to the NHS are identified to the Occupational Health & Wellbeing Service. Ensuring all new staff are sent the new Health at Work questionnaire which includes a TB proforma. Ensuring that clinical students, agency, locum staff and contract ancillary workers who have patient or clinical material contact are screened for TB status prior to commencement in post. Documentary evidence of this screening should be requested from agencies and contractors. New Employees are responsible for: Co-operating with Occupational Health procedures to screen for immunity to TB. Informing Occupational Health immediately and seek appropriate advice if they have been in contact with someone they suspect of having TB.

Occupational Health Procedure for Screening of Staff
1. All new employees will complete a confidential Health at Work
questionnaire which includes a TB proforma prior to starting work. This will determine any relevant past or current health issues including TB. New Staff are only required to attend Occupational Health if there is a positive response to questions that require further investigation.
2. New Staff who have previously worked in the NHS and have clinical contact with patient or specimens will be seen within two weeks of commencing employment for an induction, where a vaccination history which includes dates of BCG vaccination and dates and results of any previous TB skin testing. Where the results of testing is unclear and there is no history of having a BCG or no scar is visible, then a Mantoux skin test is required and carried out. The staff member is placed on the Mantoux screening list and informed by letter of the date of the appointment for testing. See Appendix 5b If Mantoux negative (less than 6mm) they should have an individual risk assessment for HIV infection before BCG vaccination is given. There is no upper age limit for the administration of the vaccine.
3. All new employees to the NHS who will be working with patients or clinical specimens will not commence work until they have completed a TB screen* or health check or documentary evidence is provided of such screening having taken place within the preceding 12 months. *(not Mantoux test)
4. All new employees to the NHS will be identified by either medical staffing or recruitment.
5. Health checks for employees new to the NHS who will have contact with patients or clinical materials will include:
Assessment of personal or family history of TB. Symptoms and signs highlighted by Health at Work questionnaire. Documentary evidence of TB skin testing or interferon-famma testing
and/or BCG scar. Check by an Occupational Health Adviser not relying on the applicant’s personal assessment.
Mantoux results within the last five years. 6. If new employee has no evidence of BCG vaccination then a Mantoux test
should be performed. If negative (less than 6mm) then an individual risk assessment for HIV infection is undertaken and a BCG offered, whatever their age. If they decline the BCG vaccination the risks should be explained and the oral explanation supplemented by written advice. The manager of the new employee should be informed and advised that he or she should not work where there is a risk of exposure to TB. The manager will need to consider each case individually taking into account of employment and health and safety obligations.

7. If the Mantoux test is positive then the new employee should have a
medical assessment. If suspicious symptoms or circumstances arise then they have a chest x-ray. If the x-ray is abnormal they should be referred to the TB clinic for consideration of TB treatment or for consideration of treatment of latent TB infection if the chest x-ray is normal. See Appendix 5c
8. New Employees to the NHS new entrants (members of staff arriving in or returning to the UK from a high incidence area where there are more than 40 cases per 100,000 people per year as listed by the Health Protection Agency (Appendix 5a) will require to have a chest x-ray and either Mantoux or interferon-gamma test done in the last five years or will be required to have a Mantoux test undertaken before they can start work. If the chest x-ray is normal then a Mantoux test is undertaken unless previously performed in the last five years. If they have a prior BCG scar or documentary evidence of vaccination then they can be passed to commence in the post, providing all other requirements have been met (ie blood test for Hepatitis B, Hepatitis C etc). If the Mantoux test is negative less than 6mm then follow the details as in Sub-Section 6. If the Mantoux test is positive then follow the details as in Section 7.
All staff who are in regular contact with TB patient or clinical materials or have worked in a high risk clinical setting for four weeks or longer will receive a yearly TB proforma letter They will complete this and advice will be given regarding the need for prompt reporting if symptoms occur. All staff on a ward/department will be sent a one-off TB proforma letter after a TB incident in their area. If there is no documentary evidence of prior screening, screen staff in contact with patients or clinical material who are changing post as if they were new employees. For HIV positive employees assess TB risks at the time of recruitment, be aware of areas with increased risk of exposure to TB. If HIV is diagnosed during employment then assess TB risk and modify the person’s work if needed. Author: Cepta Byrne Occupational Health Deputy Manager Issue: 2 Date: March 2012 Reference: NICE, March 2006, Clinical Guideline 33 – Tuberculosis

Figure 1. Flow chart for the protection of patients and Trust staff against tuberculosis.
Screening new NHS employees
Risk assessment
Chest X-ray normal?
Prior BCG (scar or documented)?
Suspicious symptoms or
circumstances?
Mantoux or interferon-gamma
test positive?
Working with patients or clinical
materials?
Normal?
Suspicious symptoms?
Medical assessment, chest X-ray
Mantoux/interferon-gamma test, unless performed in past 5 years
Pre-employment questionnaire
TB clinic
Medical assessment
No action
Offer BCG
Record refusals Notify
occupational health
‘Inform and advise’, consider treatment
for latent TB infection
TB clinic
Yes
Yes
Yes
Yes
Yes
No
No
No
No
No
No
Yes
Yes
No
New entranta?
Normal? Yes No
No Yes
a New entrants are people arriving in or returning to the UK from a high-incidence country (more than 40 cases per 100,000 per year, as listed by the Health Protection Agency; go to www.hpa.org.uk and search for ‘WHO country data TB’)
Chest X-ray
TB clinic
NICE Guidelines – Tuberculosis

During the last twelve months, have you been a resident in any of the following areas for more than 6 months (please tick as appropriate).
South East Asia Middle East
Africa (including North Africa) South and Central America
Eastern European Countries Western Pacific
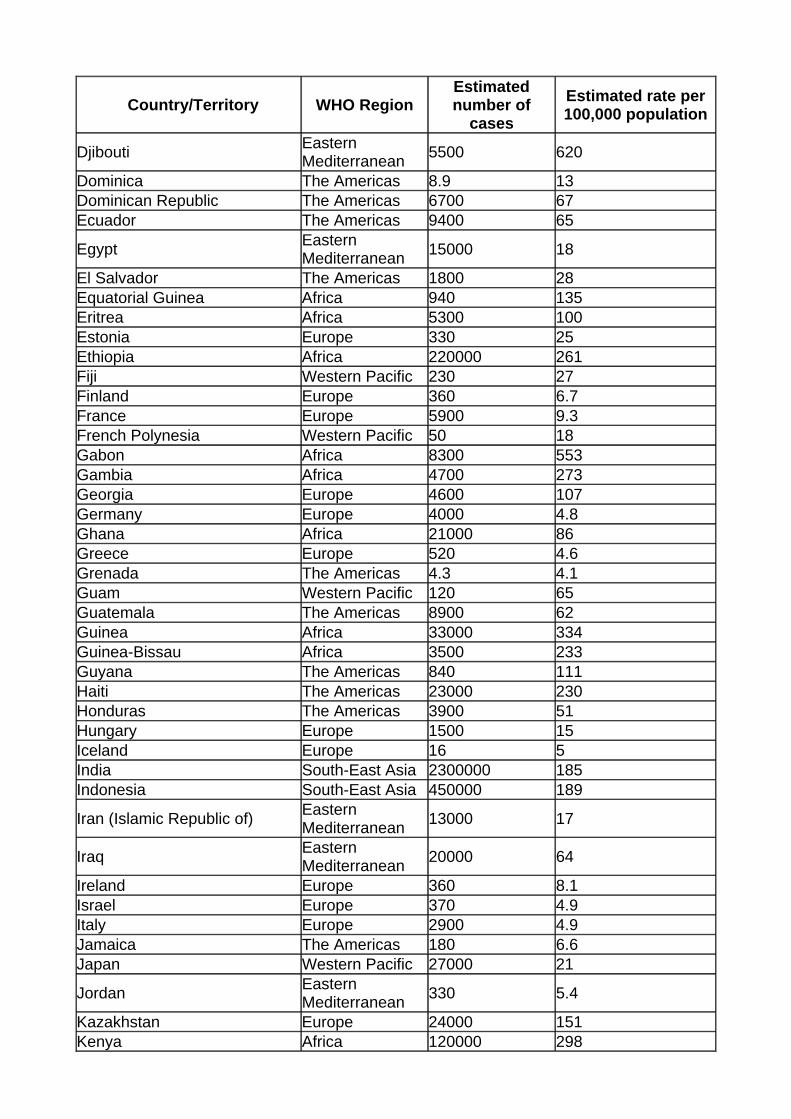
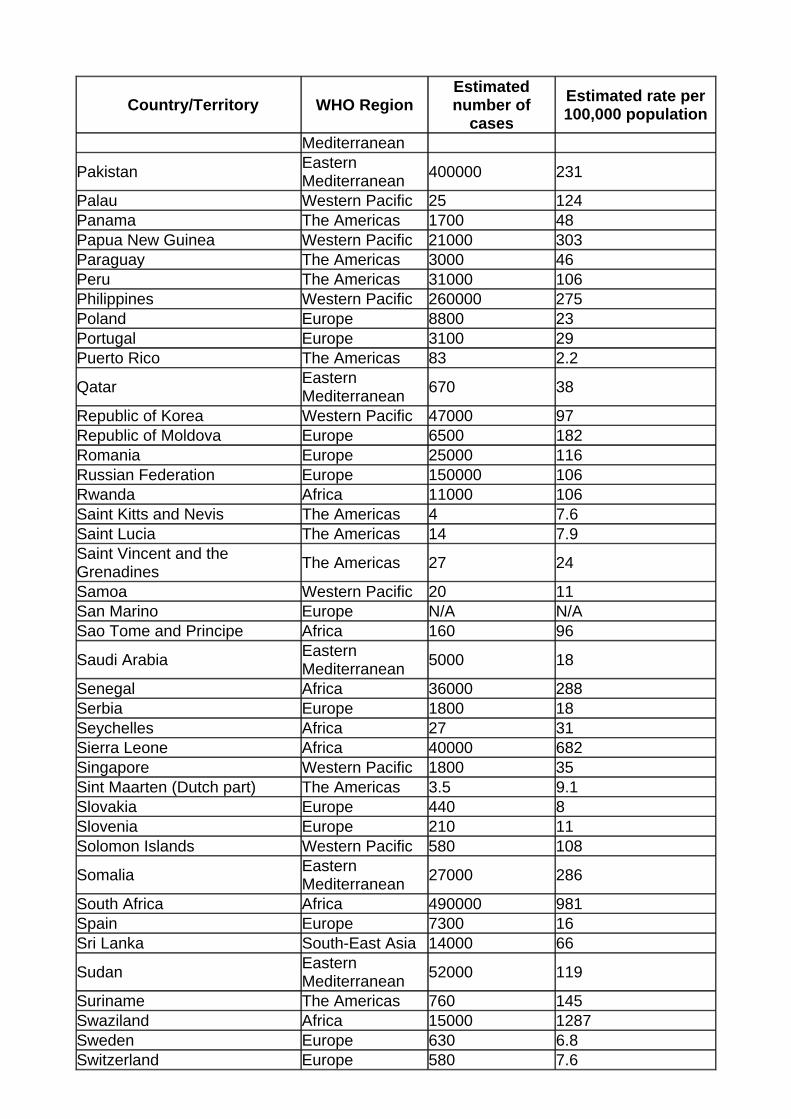
COUNTRIES CONSIDERED HIGH PREVALENCE FOR TUBERCULOSIS FOR THE PURPOSES OF SCREENING NEW IMMIGRANTS, REFUGEES AND ASYLUM SEEKERS FOR TUBERCULOSIS AND FOR SELECTIVE NEONATAL BCG IMMUNISATION POLICIES
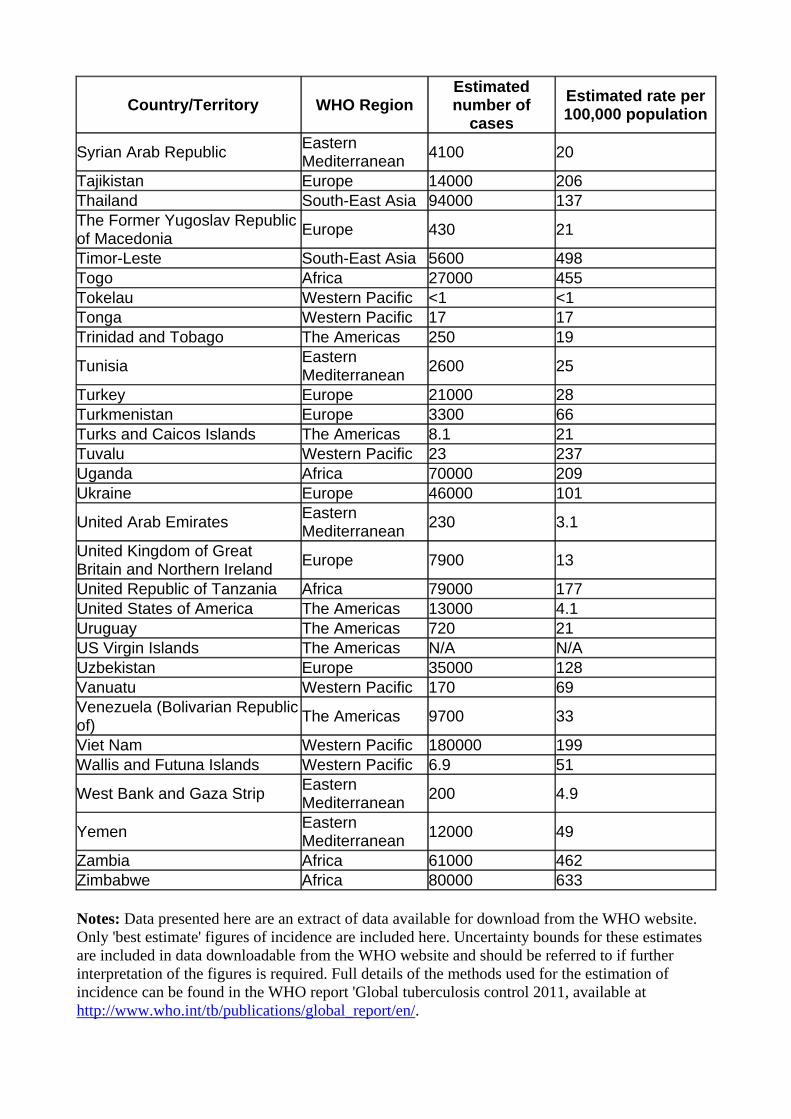
World Health Organization (WHO) estimates of tuberculosis incidence by country, 2010 (sorted by country)
World Health Organization (WHO) estimates of tuberculosis incidence by country, 2010 (sorted by country)
These WHO estimates are also available sorted by rate.
Definition of high incidence With reference to the National Institute for Health and Clinical Excellence (NICE) recommendations for BCG vaccination and screening in England and Wales, countries/territories with an estimated incidence rate of 40 per 100,000 or greater are considered to have a high incidence of tuberculosis.
Country/Territory WHO Region Estimated number of
cases
Estimated rate per 100,000 population
Afghanistan Eastern Mediterranean
59000 189
Albania Europe 450 14 Algeria Africa 32000 90 American Samoa Western Pacific 5.3 7.8 Andorra Europe 6.3 7.4 Angola Africa 58000 304 Anguilla The Americas 3.3 21 Antigua and Barbuda The Americas 4.4 4.9 Argentina The Americas 11000 27 Armenia Europe 2300 73 Aruba The Americas N/A N/A Australia Western Pacific 1400 6.3 Austria Europe 420 5 Azerbaijan Europe 10000 110 Bahamas The Americas 39 11 Bahrain Eastern 290 23
APPENDIX 5a

Country/Territory WHO Region Estimated number of
cases
Estimated rate per 100,000 population
Mediterranean Bangladesh South-East Asia 330000 225 Barbados The Americas 4.6 1.7 Belarus Europe 6800 70 Belgium Europe 930 8.7 Belize The Americas 120 40 Benin Africa 8300 94 Bermuda The Americas 1.1 1.6 Bhutan South-East Asia 1100 151 Bolivia (Plurinational State of) The Americas 13000 135 Bonaire, Saint Eustatius and Saba
The Americas N/A N/A
Bosnia and Herzegovina Europe 1900 50 Botswana Africa 10000 503 Brazil The Americas 85000 43 British Virgin Islands The Americas 2.3 9.7 Brunei Darussalam Western Pacific 270 68 Bulgaria Europe 3000 40 Burkina Faso Africa 9000 55 Burundi Africa 11000 129 Cambodia Western Pacific 62000 437 Cameroon Africa 35000 177 Canada The Americas 1600 4.7 Cape Verde Africa 730 147 Cayman Islands The Americas 4.6 8.2 Central African Republic Africa 14000 319 Chad Africa 31000 276 Chile The Americas 3200 19 China Western Pacific 1000000 78 China, Hong Kong SAR Western Pacific 5700 80 China, Macao SAR Western Pacific 410 76 Colombia The Americas 16000 34 Comoros Africa 270 37 Congo Africa 15000 372 Cook Islands Western Pacific <1 3.5 Costa Rica The Americas 630 13 Côte d'Ivoire Africa 27000 139 Croatia Europe 940 21 Cuba The Americas 1000 9.3 Curaçao The Americas 5.8 4 Cyprus Europe 49 4.4 Czech Republic Europe 710 6.8 Democratic People's Republic of Korea
South-East Asia 84000 345
Democratic Republic of the Congo
Africa 220000 327
Denmark Europe 330 6
Country/Territory WHO Region Estimated number of
cases
Estimated rate per 100,000 population
Djibouti Eastern Mediterranean
5500 620
Dominica The Americas 8.9 13 Dominican Republic The Americas 6700 67 Ecuador The Americas 9400 65
Egypt Eastern Mediterranean
15000 18
El Salvador The Americas 1800 28 Equatorial Guinea Africa 940 135 Eritrea Africa 5300 100 Estonia Europe 330 25 Ethiopia Africa 220000 261 Fiji Western Pacific 230 27 Finland Europe 360 6.7 France Europe 5900 9.3 French Polynesia Western Pacific 50 18 Gabon Africa 8300 553 Gambia Africa 4700 273 Georgia Europe 4600 107 Germany Europe 4000 4.8 Ghana Africa 21000 86 Greece Europe 520 4.6 Grenada The Americas 4.3 4.1 Guam Western Pacific 120 65 Guatemala The Americas 8900 62 Guinea Africa 33000 334 Guinea-Bissau Africa 3500 233 Guyana The Americas 840 111 Haiti The Americas 23000 230 Honduras The Americas 3900 51 Hungary Europe 1500 15 Iceland Europe 16 5 India South-East Asia 2300000 185 Indonesia South-East Asia 450000 189
Iran (Islamic Republic of) Eastern Mediterranean
13000 17
Iraq Eastern Mediterranean
20000 64
Ireland Europe 360 8.1 Israel Europe 370 4.9 Italy Europe 2900 4.9 Jamaica The Americas 180 6.6 Japan Western Pacific 27000 21
Jordan Eastern Mediterranean
330 5.4
Kazakhstan Europe 24000 151 Kenya Africa 120000 298

Country/Territory WHO Region Estimated number of
cases
Estimated rate per 100,000 population
Kiribati Western Pacific 370 370
Kuwait Eastern Mediterranean
1100 41
Kyrgyzstan Europe 8500 159 Lao People's Democratic Republic
Western Pacific 5600 90
Latvia Europe 890 39
Lebanon Eastern Mediterranean
720 17
Lesotho Africa 14000 633 Liberia Africa 12000 293
Libyan Arab Jamahiriya Eastern Mediterranean
2500 40
Lithuania Europe 2300 69 Luxembourg Europe 45 8.8 Madagascar Africa 55000 266 Malawi Africa 33000 219 Malaysia Western Pacific 23000 82 Maldives South-East Asia 110 36 Mali Africa 10000 68 Malta Europe 50 12 Marshall Islands Western Pacific 270 502 Mauritania Africa 12000 337 Mauritius Africa 280 22 Mexico The Americas 18000 16 Micronesia (Federated States of)
Western Pacific 230 206
Monaco Europe N/A N/A Mongolia Western Pacific 6200 224 Montenegro Europe 120 19 Montserrat The Americas <1 9.9
Morocco Eastern Mediterranean
29000 91
Mozambique Africa 130000 544 Myanmar South-East Asia 180000 384 Namibia Africa 14000 603 Nauru Western Pacific 4.1 40 Nepal South-East Asia 49000 163 Netherlands Europe 1200 7.3 New Caledonia Western Pacific 57 23 New Zealand Western Pacific 330 7.6 Nicaragua The Americas 2400 42 Niger Africa 29000 185 Nigeria Africa 210000 133 Niue Western Pacific <1 6.5 Northern Mariana Islands Western Pacific 44 72 Norway Europe 300 6 Oman Eastern 360 13
Country/Territory WHO Region Estimated number of
cases
Estimated rate per 100,000 population
Mediterranean
Pakistan Eastern Mediterranean
400000 231
Palau Western Pacific 25 124 Panama The Americas 1700 48 Papua New Guinea Western Pacific 21000 303 Paraguay The Americas 3000 46 Peru The Americas 31000 106 Philippines Western Pacific 260000 275 Poland Europe 8800 23 Portugal Europe 3100 29 Puerto Rico The Americas 83 2.2
Qatar Eastern Mediterranean
670 38
Republic of Korea Western Pacific 47000 97 Republic of Moldova Europe 6500 182 Romania Europe 25000 116 Russian Federation Europe 150000 106 Rwanda Africa 11000 106 Saint Kitts and Nevis The Americas 4 7.6 Saint Lucia The Americas 14 7.9 Saint Vincent and the Grenadines
The Americas 27 24
Samoa Western Pacific 20 11 San Marino Europe N/A N/A Sao Tome and Principe Africa 160 96
Saudi Arabia Eastern Mediterranean
5000 18
Senegal Africa 36000 288 Serbia Europe 1800 18 Seychelles Africa 27 31 Sierra Leone Africa 40000 682 Singapore Western Pacific 1800 35 Sint Maarten (Dutch part) The Americas 3.5 9.1 Slovakia Europe 440 8 Slovenia Europe 210 11 Solomon Islands Western Pacific 580 108
Somalia Eastern Mediterranean
27000 286
South Africa Africa 490000 981 Spain Europe 7300 16 Sri Lanka South-East Asia 14000 66
Sudan Eastern Mediterranean
52000 119
Suriname The Americas 760 145 Swaziland Africa 15000 1287 Sweden Europe 630 6.8 Switzerland Europe 580 7.6
Country/Territory WHO Region Estimated number of
cases
Estimated rate per 100,000 population
Syrian Arab Republic Eastern Mediterranean
4100 20
Tajikistan Europe 14000 206 Thailand South-East Asia 94000 137 The Former Yugoslav Republic of Macedonia
Europe 430 21
Timor-Leste South-East Asia 5600 498 Togo Africa 27000 455 Tokelau Western Pacific <1 <1 Tonga Western Pacific 17 17 Trinidad and Tobago The Americas 250 19
Tunisia Eastern Mediterranean
2600 25
Turkey Europe 21000 28 Turkmenistan Europe 3300 66 Turks and Caicos Islands The Americas 8.1 21 Tuvalu Western Pacific 23 237 Uganda Africa 70000 209 Ukraine Europe 46000 101
United Arab Emirates Eastern Mediterranean
230 3.1
United Kingdom of Great Britain and Northern Ireland
Europe 7900 13
United Republic of Tanzania Africa 79000 177 United States of America The Americas 13000 4.1 Uruguay The Americas 720 21 US Virgin Islands The Americas N/A N/A Uzbekistan Europe 35000 128 Vanuatu Western Pacific 170 69 Venezuela (Bolivarian Republic of)
The Americas 9700 33
Viet Nam Western Pacific 180000 199 Wallis and Futuna Islands Western Pacific 6.9 51
West Bank and Gaza Strip Eastern Mediterranean
200 4.9
Yemen Eastern Mediterranean
12000 49
Zambia Africa 61000 462 Zimbabwe Africa 80000 633
Notes: Data presented here are an extract of data available for download from the WHO website. Only 'best estimate' figures of incidence are included here. Uncertainty bounds for these estimates are included in data downloadable from the WHO website and should be referred to if further interpretation of the figures is required. Full details of the methods used for the estimation of incidence can be found in the WHO report 'Global tuberculosis control 2011, available at http://www.who.int/tb/publications/global_report/en/.

Source: WHO TB burden estimates, available at: http://www.who.int/tb/country/data/download/en/index.html, and Global tuberculosis control 2011, available at http://www.who.int/tb/publications/global_report/en/ . Accessed 29/11/2011.
Prepared by: TB Section, Health Protection Services - Colindale
Last reviewed: 9 March 2012
© Health Protection Agency 2012
Occupational Health & Wellbeing Service
Thamesgate House 33 Victoria Avenue
CONFIDENTIAL Southend-on-Sea Essex SS2 6BU
Tel: 01702 222900
Date: ________________ Fax: 01702 222919 ____________________________
____________________________
____________________________
Dear _______________________ RE: MANTOUX TESTING FOR ASSESSING T.B. IMMUNITY An appointment has been arranged for you to attend the Occupational Health Service for Mantoux testing. Prior to attending all staff must read the information on Staffnet, Occupational Health Service, TB, which fully explains the Mantoux screening and the possible complications associated with it. On attendance for screening, you will need to sign a document indicating that you have read through this information and are happy to proceed with the test. If you do not have access to Staffnet then you will need to attend for your appointment 10 minutes prior to your screen time in order to read the information pack. Your date and time of attendance at the Occupational Health Service for screening is _____________________________________________________ at _______________ Then to return on: _____________________________________________________ at ________________ Depending on the result of you test, you may need to see the Occupational Health Physician and have a BCG inoculation against TB If you have any queries about this, please do not hesitate to contact the Occupational Health Service. Yours sincerely, Occupational Health & Wellbeing Service Thamesgate House O.H.S.02E/2007/2008/2009/2012
APPENDIX 5b
Southend University Hospital NHS Foundation Trust Plus
OCCUPATIONAL HEALTH & WELLBEING SERVICE
Thamesgate House 33 Victoria Avenue
CONFIDENTIAL Southend-on-Sea Essex SS2 6BU
Tel: 01702 222900
Date: ____________________ Fax: 01702 222919 Dr Ansari / Dr Day CHEST CLINIC Southend University Hospital NHS Foundation Trust Dear Dr Ansari / Dr Day Re : Positive Mantoux Test Greater Than 15 millimetres The following member of staff had a Mantoux Test read here in the Occupational Health and the result is greater than 15 millimetres. I am therefore referring the member of staff to you for a further follow up. From our records:-
1. This person has had a previous BCG YES/NO
2. This person last had a chest x-ray on -
3. This person is complaining of symptoms compatible with possible Tuberculosis YES/NO
Thank you very much for your anticipated co-operation. With best wishes. Yours sincerely Dr Grahame Sofoluwe MB BS MRCS LRCP DCH DRCOG MRCGP AFOM Msc CUEW Occupational Health Physician Southend Hospital Chairman: Alan Tobias MBE Chief Executive: Jacqueline Totterdell www.southend.nhs.uk
APPENDIX 5c Southend University Hospital NHS Foundation Trust Plus

PROTOCOL FOR MANTOUX TEST The Mantoux Test has now superseded the Heaf Test for screening for people who are not immune to Tuberculosis and require BCG immunisation. The current supply of Tuberculin PPD is unlicensed but is recommended by the Department of Health for Mantoux Testing. The Department of Health Licences its use under the Patients Specific Direction which means that there must be written instructions by an independent prescriber for it to be used. The protocol for Mantoux Testing will then consist of the following:-
1. Staff would have filled in the TB Proforma.
2. If this indicates that they do not have BCG immunisation and are at risk of Tuberculosis then they should proceed on to Mantoux Testing.
3. Prior to Mantoux Testing, all staff members will be given a copy of the letter by Dr
Jane Leese, dated 19th July 2005, which fully explains the Mantoux Testing and the possible complications associated with it.
4. The staff member will have to sign a document indicating that they have been given
and read through the letter from Dr Jane Leese, including Appendices 1 and 2 and are happy to proceed with the Mantoux Testing.
5. The nurse who will carry out the Mantoux Testing will have to have a signed
Patients Specific Direction for administration of Tuberculin PPD as contained in Appendix 5X. The name should be filled in prior to any Mantoux Testing.
6. If there is any new entrant to the Mantoux Testing clinic (not already on the Patient
Specific Directive) then there must be either verbal confirmation or written confirmation from the Occupational Health Physician that they can be tested for Mantoux.
7. Appendix 3 of the Department of Health Guidelines will therefore be used at all
Mantoux Testing clinics.
8. The results will be read 48 to 72 hours after Testing and if the size of the lesion is 0mm to 5mm then the member of staff would be eligible to having the BCG vaccination except if new entrant screen with a definite BCG scar who is immune.
9. If the result is between 6mm and 14mm then the member of staff will be deemed to
be immune to TB and should not be given the BCG vaccination.
10. If the lesion is greater than 15mm then the member of staff will need to be referred to Dr Ansari/Dr Day in the Chest Clinic for further investigation.
APPENDIX 5d
Southend University Hospital NHS Foundation Trust Plus
OCCUPATIONAL HEALTH & WELLBEING SERVICE
Thamesgate House 33 Victoria Avenue
CONFIDENTIAL Southend-on-Sea Essex SS2 6BU
Tel: 01702 222900 Fax : 01702 222919
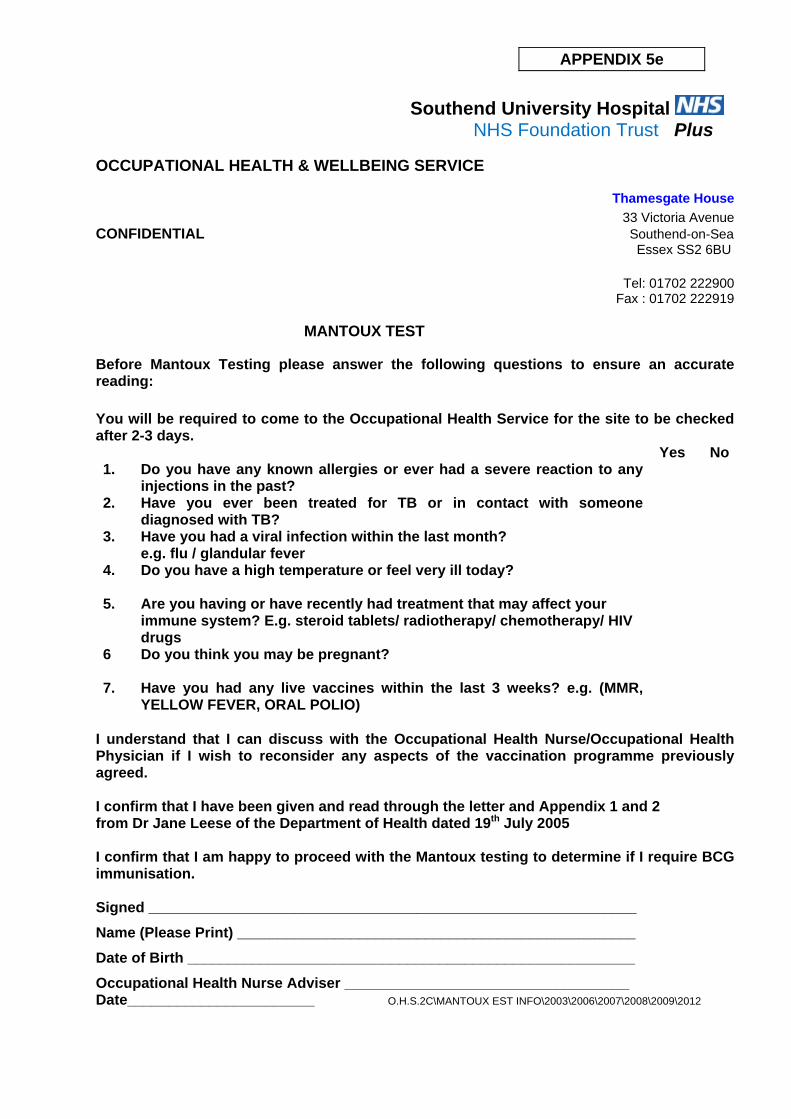
MANTOUX TEST
Before Mantoux Testing please answer the following questions to ensure an accurate reading:
You will be required to come to the Occupational Health Service for the site to be checked after 2-3 days. Yes No 1. Do you have any known allergies or ever had a severe reaction to any
injections in the past?
2. Have you ever been treated for TB or in contact with someone diagnosed with TB?
3. Have you had a viral infection within the last month? e.g. flu / glandular fever
4. Do you have a high temperature or feel very ill today?
5. Are you having or have recently had treatment that may affect your immune system? E.g. steroid tablets/ radiotherapy/ chemotherapy/ HIV drugs
6 Do you think you may be pregnant?
7. Have you had any live vaccines within the last 3 weeks? e.g. (MMR, YELLOW FEVER, ORAL POLIO)
I understand that I can discuss with the Occupational Health Nurse/Occupational Health Physician if I wish to reconsider any aspects of the vaccination programme previously agreed.
I confirm that I have been given and read through the letter and Appendix 1 and 2 from Dr Jane Leese of the Department of Health dated 19th July 2005 I confirm that I am happy to proceed with the Mantoux testing to determine if I require BCG immunisation. Signed ____________________________________________________________
Name (Please Print) _________________________________________________
Date of Birth _______________________________________________________
Occupational Health Nurse Adviser ___________________________________ Date_______________________ O.H.S.2C\MANTOUX EST INFO\2003\2006\2007\2008\2009\2012
APPENDIX 5e

PATIENT SPECIFIC DIRECTION FOR ADMINISTRATION OF TUBERULIN PPD (SSI) FOR MANTOUX TESTING
The below named patient is eligible for routine Mantoux testing by intradermal injection of Tuberculin PPD (SSI) 2 TU per 0.1ml (20 units in 1ml) and Tuberculin PPD (SSI) 10 TU/0.1 ml. The higher concentration 10 TU/0.1 ml may be used for a second test if the first test (2 TU per 0.1ml) is negative (less than approx. 6 mm in diameter) and a retest is considered appropriate.
Patient’s Name: Signature of prescriber:
Name:
Date:
O.H.S.2C\MANTOUX TEST INFO\2003\2006\2007\2008\2009\2012 – (back) Chairman: Alan Tobias MBE Chief Executive: Jacqueline Totterdell www.southend.nhs.uk

Occupational Health & Wellbeing Service Suite 40, Thamesgate House
33 Victoria Avenue Southend on Sea Essex SS2 6BU
01702 222900
STAND LETTERS\O.H.S.02F (MANTOUX LEAFLET)\10\2006 \04\2007\2008\2009
Occupational Health & Wellbeing Service
Mantoux Test
Advice Leaflet
APPENDIX 5f
Southend University Hospital NHS Foundation Trust Plus
MANTOUX TEST ADVICE
You have had a skin test (Mantoux) done today. The test involves injecting a small amount of vaccine under the skin which causes a bleb (blister) to appear. It is essential you are available in 2-3 days time for the Nurse to examine the results. An appointment has already been sent to you. If you fail to attend, the test will need to be repeated. The reaction that develops will determine if you need a BCG vaccine. A reaction may occur around the test site only. It is very unlikely you will feel unwell following this test. The test area may react in one of the following ways:
1. The bleb may disappear within the hour 2. A hard spot/swelling may occur 3. An ulcer or blistered area
Do not apply ointment or creams on the area or cover with sticky plasters or bandages even if a reaction occurs.
Wear normal clothing but leave area open to air whenever possible. Normal washing with soap/shower gel is permitted. The area may irritate or itch. If the area does itch, do not scratch, placing a cold compress on the site for a short time will give relief (e.g. ice wrapped in cloth) The reaction may take a number of weeks to disappear and may leave a scar. (No treatment is necessary). Please phone the Occupational Health & Wellbeing Service on:
01702 222 900 if a problem arises with your appointment.
RESULTS OF MANTOUX
Negative
Positive
Strongly Positive
0-5mm
6-14mm
15+mm
Heaf grade 0-1
Heaf grade 2
Heaf grade 3-4
APPENDIX 5g

Occupational Health & Wellbeing Service Protocol for Management of Suspected Case of Tuberculosis in Staff Member If a member of staff contacts the department, with a possible case of Tuberculosis then the Occupational Health Department would need to determine the following.
a. Determine if any clinician has made a possible diagnosis of Tuberculosis?
b. Determine what, if any, steps or follow-up have been arranged by the clinician making the diagnosis?
c. Determine if the Heart and Chest Clinic and Infection Control have been informed
about the case?
d. Determine if the member of staff stopped working? 1. If a staff member has already seen a clinician, who has made a diagnosis of Tuberculosis,
and appropriate clinical follow-up has been arranged, then the Occupational Health Department would be responsible for supporting the member of staff, facilitating and determining fitness to return to work.
2. If no clear diagnosis has been made about Tuberculosis, then the role of the Occupational
Health Department would be to refer the member of staff to the Heart and Chest Clinic and inform the Infection Control Team.
3. If the Heart and Chest Clinic is closed then Infection Control Team should be informed and
referral made to the on-call medical team. The Infection Control Team would be responsible for contacting the Heart and Chest Clinic. The Occupational Health Department would as a back-up also contact the Heart and Chest Clinic.
4. The Occupational Health Department cannot play the role of the Prime Care Provider as its
role is primarily to facilitate appropriate referral if not already done. This would involve contacting the Heart and Chest Clinic and also the Infection Control Team.
5. The current agreed practice ensures that the Occupational Health Department is notified
by both the Infection Control Team and the Heart and Chest Clinic if any member of staff is diagnosed with Tuberculosis.
Protocol for Management of Suspected Case of Tuberculosis in Staff Member GS 02 February 2005
APPENDIX 5h
Occupational Health & wellbeing Service
Guidelines on Health Clearance for New Health Care Workers to the UK
(Mantoux/T.B.) As per the NICE Guidelines in line with the Department of Health Guidance on Health Clearance for New Health Care Workers to the UK: New entrants arriving from countries where the annual incidence of TB is greater than
40 in 100,000 and who have not been screened on entry, in the district, or by a previous employer in the United Kingdom within the last 12 months should be referred for chest radiography.
New entrants will require a Mantoux skin test irrespective of previous BCG vaccination.
Process Undertake a pre –clearance assessment questionnaire and check TB proforma, if no
risk identified then undertake Mantoux test and send for chest x-ray . X-ray form should be pre-signed by Dr Sofoluwe with TB Screening/Pre clearance
stamp insitu. Please request fax (include number on form, 01702 222919) results to be sent to the Occupational Health Service.
A Mantoux test result of 6mm or more in an employee with no previous BCG
vaccination, or larger than 15mm in an employee with previous BCG vaccination is a positive result.
A positive test should, result in a referral for medical assessment to exclude active
disease and possible presence for latent infection. \c\guidelines\Health Clearance for New HCW to the UK (Mantoux/T.B.) February 2010
APPENDIX 5i
Southend University Hospital NHS Foundation Trust Plus

Occupational Health & Wellbeing Service
Aftercare Following BCG In 2 to 6 week, the site of the injection will become red and develop a small pustule (spot), which will ooze slightly, subsiding over several months leaving a small scar. To heal quickly, the lesion should be kept clean, dry and open to the air, using a temporary dressing only if necessary. You may swim, covering the lesion only if it is oozing, with a waterproof plaster. Make sure you remove the plaster afterwards. Avoid getting the area knocked and do not scratch or remove any scabs that form. You should have no further live vaccines/immunisations (except oral polio vaccine) for 4 weeks following BCG and NO injections in your left arm for 3 months. If you have any questions afterwards, please telephone 01702 222900. THANKYOU
APPENDIX 5 j
Southend University Hospital NHS Foundation Trust Plus
OCCUPATIONAL HEALTH & WELLBEING SERVICE
Thamesgate House 33 Victoria Avenue
CONFIDENTIAL Southend-on-Sea Essex SS2 6BU
Tel: 01702 2229
BCG VACCINATION Fax: 01702 222919
Before BCG Vaccination, please answer the following questions to ensure you are fit for the vaccine:
You will be required to come to the Occupational Health Service for the site to be checked 6 weeks after. Yes No 1. Do you have any known allergies or ever had a severe reaction to
any injections in the past?
2. Have you ever been treated for TB or in contact with someone diagnosed with TB?
3. Have you had a viral infection within the last month? e.g. flu / glandular fever
4. Do you have a high temperature or feel very ill today?
5. Are you having or have recently had treatment that may affect your immune system? E.g. steroid tablets/ radiotherapy/ chemotherapy/ HIV drugs
6. If in doubt please read the attached leaflet about HIV to decide if you need an HIV test prior to inoculation.
7 Do you think you may be pregnant?
8. You must not get pregnant for 3 months after vaccination
9. Have you had any live vaccines within the last 3 weeks? e.g. (MMR, YELLOW FEVER, ORAL POLIO)
I understand that I can discuss with the Occupational Health Nurse/Occupational Health Physician if I wish to reconsider any aspects of the vaccination programme previously agreed. I confirm that I am happy to proceed with the BCG Vaccination. Signed ____________________________________________________________________
Name (Please Print) _________________________________________________________
Date of Birth _______________________________________________________________
Occupational Health Nurse Adviser ___________________________________________
Date ____________________________ OHS.2B/BCG VACCINATION/2006/2007/2008/2009/2012
APPENDIX 5k
APPENDIX 5l

Southend University Hospital NHS Foundation Trust Plus
OCCUPATIONAL HEALTH & WELLBEING SERVICE
Thamesgate House 33 Victoria Avenue
CONFIDENTIAL Southend-on-Sea Essex SS2 6BU
Tel: 01702 222900
Fax: 01702 222919 B.C.G. INOCULATION
I confirm that I accept this inoculation and understand the following conditions:-
1. I must have the inoculation within nine days of the first day of my last period or if I am certain that I cannot be pregnant.
2. I must avoid pregnancy for the next three months.
3. I will not have any other immunisation in the arm I had my
BCG for 3 months.
A local reaction may develop at the immunisation site within two to six weeks. There may be a discharge, this is quite normal. A dry dressing should be used to protect clothing. DO NOT apply ointments or strapping direct to the skin. A waterproof dressing may be applied if you go swimming. (Dressings should be burnt after removal). If the discharge is excessive, or you are at all worried, please contact Occupational Health for advice.
NAME ___________________________________________________
SIGNED _________________________________________________
DATE ___________________________________________________ O.H.S.2A/BCG Vaccination info/2005/2006/2007/2008/2009/2011 Chairman: Alan Tobias mbe Chief Executive: Jacqueline Totterdell www.southend.nhs.uk

BCG CLINIC ________________________
1.00 pm
1.10 pm
1.10 pm
1.20 pm
1.30 pm
1.30 pm
1.40 pm
1.45 pm
1.45 pm
APPENDIX 5m

OCCUPATIONAL HEALTH & WELLBEING SERVICE Thamesgate House 33 Victoria Avenue Essex-on-Sea Essex
SS2 6BU
Tel: 01702 222900 CONFIDENTIAL Fax: 01702 222919
Date: _______________________ Jennie Keane TB Nurse Specialist HEART & CHEST CLINIC Essex University Hospital NHS Foundation Trust Dear Jennie, Re : ___________________________________________ DOB: ______________ Address: __________________________________________________________ Positive Mantoux Test Greater Than 15 millimetres The following member of staff had a Mantoux Test read here in the Occupational Health Service and the result is greater than 15 millimetres. I am therefore referring the member of staff to you for a further follow up. From our records:-
4. This person has had a previous BCG YES/NO
5. This person last had a chest x-ray on - _____________________________
6. This person is complaining of symptoms compatible with possible Tuberculosis YES/NO
Thank you very much for your anticipated co-operation. With best wishes. Yours sincerely Dr Grahame Sofoluwe MB BS MRCS LRCP DCH DRCOG MRCGP AFOM Msc CUEW Occupational Health Physician Essex Hospital O.H.S.58 Positive Mantoux Test ref to Essex Hospital/2009/2011
APPENDIX 5n Southend University Hospital NHS Foundation Trust Plus

OCCUPATIONAL HEALTH & Thamesgate House
WELLBEING SERVICE 33 Victoria Avenue
CONFIDENTIAL Essex-on-Sea Essex SS2 6BU
Tel: 01702 222900
Date: ________________ Fax: 01702 222919 Dear An appointment has been made for you to visit the Occupational Health Service at Thamesgate House, 33-41 Victoria Avenue, Essex on Sea, Essex SS2 6BU for:
Hepatitis B Immunisation Chickenpox Blood Test for Antibody levels
Immunisation Check Induction Rubella/MMR Immunisation Polio/Tetanus/Diphtheria Other _____________________________ FEMALE STAFF please note, you must have MMR and BCG vaccinations within nine
days of the first day of your last period and must avoid pregnancy for the next three months.
On: __________________________________________________________________ At: __________________________________________________________________ Please telephone the Occupational Health Service at Thamesgate House if this appointment is inconvenient, 01702 222900. NB If your appointment is for an immunisation check, it would be very helpful if you could bring
the following information:
Date of last Tetanus Vaccine Date of last Polio Vaccine Dates of Hepatitis B immunisations A photocopy of the Hepatitis B, Rubella and Chickenpox immunity blood test undertaken at the end of the course
If you do not have this information, it may be helpful to contact your General Practitioner/ previous Occupational Health Department before the appointment who may be able to help you.
IMPORTANT: If you are unwell or taking any medication at this time, please telephone this Department for advice before attending.
PLEASE BRING PHOTOGRAPHIC PROOF OF IDENTITY WITH YOU WHEN YOU ATTEND FOR YOUR APPOINTMENT Standlt\appt\sh\2007\2008\2009 Chairman: Alan Tobias mbe Chief Executive: Jacqueline Totterdell www.southend.nhs.uk
APPENDIX 5o Southend University Hospital NHS Foundation Trust Plus