Principles pertaining to newer instrumentation techniques for management of cervical spine trauma
13
PRINCIPLES PERTAINING TO NEWER INSTRUMENTATION TECHNIQUES FOR MANAGEMENT OF CERVICAL SPINE TRAUMA DANIEL GREEN, MD, R. DAVID BAUER, MD, and STEVEN R. GARFIN, MD The use of internal fixation in the cervical spine has increased as implant materials and implant designs have improved. In many situations, fusion with standard wiring techniques and/or the use of immobilization in a halo vest will be adequate for stabilization of cervical trauma. Decreased postoperative immobilization and increased postoperative range of motion may be possible using newer instrumentation techniques. The following article will discuss recent advances in implant design as well as indications for use and techniques of implantation. KEY WORDS: fractures, cervical spine trauma, cervical trauma, instrumentation The major question when dealing with new technology is this: Why do we need to improve on standard tech- niques? In his presidential address to the Cervical Spine Research Society in 1988/ A. A. White, III, MD, PhD, stated, We can do anything we want with some combination of the halo, bone grafts and wires. While the clinical science of cer- vical spine implants is in its infancy ... the use of the halo device and wire fixation of the cervical spine is not. The reasons that he gave for improving cervical instru- mentation were to avoid the use of the halo and to avoid the use of sublaminar wires. We can also add to this list the desire to immobilize the patient with as little external support as possible. The history of cervical instrumentation is quite long. In 1891 Hadra described posterior wiring of the cervical spine for injury. In 1914 Lane was the first to apply plates to the spine to treat fractures. The modern era of cervical instrumentation began in 1970 when Roy-Camille and SaiIlant published their technique of posterior cervi- cal fusion using plates fixed with screws to the articular masses. Since that time, variations of these techniques have been proposed. One should remember when using cervical instrumen- tation that the primary goal is to obtain a fusion. The use of hardware in cervical spine fusion provides imme- diate/ temporary stability while allowing bony fusion to occur. In many traumatic injuries there is sufficient bony disruption that the fusion will heal itself." How- From the Department of Orthopaedic Surgery, University of Cali- fornia San Diego, Medical Center, and the Department of Orthopae- dic Surgery, West Virginia University School of Medicine, Morgan- town. Address reprint requests to Steven R. Garfin, MD, Department of Orthopaedic Surgery, UCSD Medical Center, University of California San Diego, 225 Dickenson St, No. 8894, San Diego, CA 92103. © 1993 by W. B. Saunders Company 1060-1872193/0103-0006$05.00 ever, this is not assured, and it is not usually prudent at the time of surgery to assume that the body will sponta- neously fuse. POSTERIOR CERVICAL INSTRUMENTATION Cervical Screws and Plates Indications for posterior cervical plating have been in- creasing over the years. Cervical plates have an advan- tage over posterior wiring techniques in that they do not depend on intact facets or laminae for bony stabllity.i Additionally, traditional spinous process wiring tech- niques do not control rotational instability, which occurs with a unilateral dislocation or fractured facets. Posterior cervical plates are also especially useful when the laminae or spinous processes are missing or incompetent and when the anterior column is incapable of load bearing. Wire techniques cannot maintain axial height in burst fractures and cannot control the spine when the spinous processes and the laminae are fractured. There is con- siderable controversy over whether the cervical plate adds enough strength in the more stable injuries with bony integrity to justify the added surgery and risk. Anderson et ae recommend posterior plating in most cases, claiming that immediate stability and increased fix- ation strength give it advantages over wire methods. When performing posterior cervical plating, the stan- dard posterior cervical approach is made. The patient is carefully turned to the prone position with traction. In the incompletely injured or neurologically normal pa- tient/ it is helpful to intubate and turn the patient while he or she is awake, using the patient as a neurological monitor while turning him or her prone. Some authors" have recommended the use of local anesthetic during posterior cervical fusions so that the patient serves as the neurological monitor throughout the procedure. 208 Operative Techniques in Sports Medicine, Vol 1, No 3 (July), 1993: pp 208-220
-
Upload
daniel-green -
Category
Documents
-
view
214 -
download
0
Transcript of Principles pertaining to newer instrumentation techniques for management of cervical spine trauma

PRINCIPLES PERTAINING TO NEWERINSTRUMENTATION TECHNIQUES FORMANAGEMENT OF CERVICAL SPINE TRAUMA
DANIEL GREEN, MD, R. DAVID BAUER, MD, andSTEVEN R. GARFIN, MD
The use of internal fixation in the cervical spine has increased as implant materials and implant designs haveimproved. In many situations, fusion with standard wiring techniques and/or the use of immobilization in ahalo vest will be adequate for stabilization of cervical trauma. Decreased postoperative immobilization andincreased postoperative range of motion may be possible using newer instrumentation techniques. Thefollowing article will discuss recent advances in implant design as well as indications for use and techniques ofimplantation.KEY WORDS: fractures, cervical spine trauma, cervical trauma, instrumentation
The major question when dealing with new technologyis this: Why do we need to improve on standard techniques? In his presidential address to the Cervical SpineResearch Society in 1988/ A. A. White, III, MD, PhD,stated,
We can do anything we want with some combination of thehalo, bone grafts and wires. While the clinical science of cervical spine implants is in its infancy ... the use of the halodevice and wire fixation of the cervical spine is not.
The reasons that he gave for improving cervical instrumentation were to avoid the use of the halo and to avoidthe use of sublaminar wires. We can also add to this listthe desire to immobilize the patient with as little externalsupport as possible.
The history of cervical instrumentation is quite long.In 1891 Hadra described posterior wiring of the cervicalspine for injury. In 1914 Lane was the first to applyplates to the spine to treat fractures. The modern era ofcervical instrumentation began in 1970when Roy-Camilleand SaiIlant published their technique of posterior cervical fusion using plates fixed with screws to the articularmasses. Since that time, variations of these techniqueshave been proposed.
One should remember when using cervical instrumentation that the primary goal is to obtain a fusion. Theuse of hardware in cervical spine fusion provides immediate/ temporary stability while allowing bony fusion tooccur. In many traumatic injuries there is sufficientbony disruption that the fusion will heal itself." How-
From the Department of Orthopaedic Surgery, University of California San Diego, Medical Center, and the Department of Orthopaedic Surgery, West Virginia University School of Medicine, Morgantown.
Address reprint requests to Steven R. Garfin, MD, Department ofOrthopaedic Surgery, UCSD Medical Center, University of CaliforniaSan Diego, 225 Dickenson St, No. 8894, San Diego, CA 92103.
© 1993 by W. B. Saunders Company1060-1872193/0103-0006$05.00
ever, this is not assured, and it is not usually prudent atthe time of surgery to assume that the body will spontaneously fuse.
POSTERIOR CERVICALINSTRUMENTATION
Cervical Screws and Plates
Indications for posterior cervical plating have been increasing over the years. Cervical plates have an advantage over posterior wiring techniques in that they do notdepend on intact facets or laminae for bony stabllity.iAdditionally, traditional spinous process wiring techniques do not control rotational instability, which occurswith a unilateral dislocation or fractured facets. Posteriorcervical plates are also especially useful when the laminaeor spinous processes are missing or incompetent andwhen the anterior column is incapable of load bearing.Wire techniques cannot maintain axial height in burstfractures and cannot control the spine when the spinousprocesses and the laminae are fractured. There is considerable controversy over whether the cervical plateadds enough strength in the more stable injuries withbony integrity to justify the added surgery and risk.Anderson et ae recommend posterior plating in mostcases, claiming that immediate stability and increased fixation strength give it advantages over wire methods.
When performing posterior cervical plating, the standard posterior cervical approach is made. The patient iscarefully turned to the prone position with traction.In the incompletely injured or neurologically normal patient/ it is helpful to intubate and turn the patient whilehe or she is awake, using the patient as a neurologicalmonitor while turning him or her prone. Some authors"have recommended the use of local anesthetic duringposterior cervical fusions so that the patient serves as theneurological monitor throughout the procedure.
208 Operative Techniques in Sports Medicine, Vol 1, No 3 (July), 1993: pp 208-220

Once the patient is in the prone position, his or hershoulders are taped down, and axial traction is providedon the arms so that the cervico-thoracic junction can bevisualized. The patient is placed in a reverse Trendelenburg position to decrease bleeding in the wound. It isimportant to position the patient to prevent any motion.Cervical traction is maintained on the patient until theinstrumentation is in place.
A midline posterior incision is made, dissecting subperiosteally to expose the spinous processes, laminae, andfacets of the involved area. Exposure should be limitedto the area undergoing fusion to prevent late instabilityand extension of the fusion to unintended levels.f Theinterspinous ligaments should be left intact, if possible.If it is necessary to approach the upper cervical spine, themuscular attachments to C2 should be left intact or repaired to prevent late kyphosis.
Once the surgeon has achieved adequate exposure ofthe cervical spine and has obtained an intraoperative radiograph to document the level, a choice must be made asto which screw technique to use. It is our preference touse the Roy-Camille technique.
In this technique the starting point for screw entry is atthe apex of the convexity of the lateral mass. The convexity is bounded medially by the laminar groove. Thecephalad and caudal limits of the articular mass are defined by the articular cartilage of the superior articularprocess and the tip of the inferior articular process, respectively. The screw should be oriented perpendicularto the posterior cortex of the vertebral body and directed10° laterally in the parasagittal direction. The screwroute is posteromedial to anterolateral, avoiding the vertebral artery. The vertebral artery is directly anterior tothe "valley," which is the junction between the laminaeand the facet. Bicortical screw purchase can be obtainedby penetrating the dorsal and ventral cortices of the lateral mass.
The other major technique for screw insertion that isfrequently used is Magerl's. In this technique the screwstarts 2 to 3 mm medial and superior to the apex of theconvexity. In the sagittal plane the screw is orientedparallel to the surface of the superior articular process.The screw is directed 25° laterally in the parasagittal direction. Screw purchase is bicortical, with the tip engaging the superior and lateral portion of the ventral cortexof the superior articular process.
In a comparison of the two techniques" by Heller et al,the Roy-Camille technique was believed to be slightlysafer. ,There was less risk of actual (.8% v 7.3%) andpotential (10.8% v 26.8%) nerve root injury. There wasless error in orientation of the screw as well (6°·v 13°).There was also less error in the final resting place of thescrew. The Magerl technique did have the advantage ofless risk of facet joint violation (2.4% v 22.5%); however,it was more difficult to aim correctly in the sagittal plane.The normal prominence of the cervicothoracic junctionmakes it difficult to achieve ideal screw orientation in thelower segments of the cervical spine.
It should be noted that neither technique threatenedeither the spinal cord or the vertebral arteries. Clinically, however, reported radiculopathies induced byscrews, independent of the techniques, are quite rare.
INSTRUMENTATION TECHNIQUES
There also has been no mention in the literature of facetjoint "injuries." This remains a theoretical problem, except with the most caudal screw. In this instance it maybe wise to aim slightly more cephalad to avoid the mostinferior joint. Screws have been known to loosen if theyare placed into the facet joints.i'
In a biomechanical study Montesano et af found thatthe Magerl technique was stiffer, with a higher load tofailure, than the Roy-Camille technique, probably due tothe ability to place a longer screw with the Magerl technique. The Magerl technique failed by plate bending,whereas the Roy-Camille technique failed by caudalscrew pull-out. However, this has not been a clinicalproblem. Gill et al" noted that it is important to obtainbicortical screw purchase, if possible. In their biomechanical study using one-third tubular plates, bicorticalscrew purchase was far stiffer than that achieved withunicortical screws.
The anatomy of the cervicothoracic junction is somewhat different than the remainder of the cervical spine.C7 is a transitional vertebra. Both pedicular and lateralmass techniques are difficult." The lateral mass isthinned at this level, and the inferior facet is in danger ofbeing violated. If the lateral mass technique is to beused, a more cephalad and lateral entry point for betterbony purchase should be used. Pedicle screws may beconsidered at the C7 and T1 level. The spinal cord isespecially at risk if drilling occurs too far in the medialdirection.
One difficulty with posterior cervical instrumentationis that there exists considerable variability of interfacetdistances among individuals. 9 Ideally, plates usedshould accommodate different patients. Currently,there are several posterior cervical plates available, whichdiffer in the distance separating the various screw holesin the plate (Fig 1). Advances in plate design may include the use of oblong holes to allow for interfacet variability or even to abandon the plate in favor of a moreuniversal screw and rod system as designed by Wiltseand Abitbol (Fig 2).
Plating of the cervical spine enhances the fixation ofmultiple levels. This more rigid fixation is of greaterbenefit in patients with multilevel diseases caused by injury or neoplasm. Rigid fixation also allows for earlyimmobilization of the patient with minimal postoperativeexternal support, which may be particularly significant inpatients with multiple trauma.
Halifax ClampAlternative posterior instrumentation is available. TheHalifax clamp (Levtech, Jacksonville, FL) was describedin 1984 by Holness et al. I O The clamp hooks onto thelaminae and can be used in patients with cervical subluxations and dislocations where there is posterior ligamentous instability but minimal or no vertebral body involvement. The pedicle and the lamina of the instrumentedvertebrae should be intact to obtain sufficient purchase.Sublaminar fixation with the hooks is achieved across theinvolved level.
Although Holness et allO recommended that if laminaror facet fractures were found, then a single clamp could
209

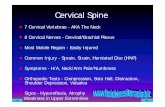
Fig 1. (A) AP and (B) lateral radiographs demonstrating lateral mass plates. Note the upward and outward direction of thescrews placed in the lateral masses.
Fig 2. (A) AP and (B) lateral radiographs demonstrating a screw and rod system for the cervical spine. The lateral mass screwscan be placed as the anatomy requires, and the rod is then contoured to fit to the screws.
210 GREEN, BAUER, AND GARFIN

be applied to the opposite and nonfractured side, recentauthors have advocated the use of bilateral Halifaxclamps. Bilateral clamps provide increased stability.Biomechanical studies have shown that Halifax clampshave some weakness in extension and rotation and maytherefore be less useful than cervical plates.u·12 TheHalifax clamp is now produced in titapiurn to diminishmagnetic resonance imaging (MRI) artifacts.P
The clamps are placed using a standard posterior cervical exposure. The superior border of the superior laminae and the inferior border of the inferior laminae arefreed to the ligamentum flavum attachments medially.Small rongeurs are used to prepare the clamp sites.The laminae, spinous processes, and posterior surface ofthe facets in the region of the fusion are denuded of periosteum. High-speed drills and rongeurs are used toroughen the bone until it is bleeding freely. Once theclamp is applied over the superior and inferior laminae, itis tightened until no motion is possible between the involved vertebrae and adequate alignment is achieved'?(Fig 3).
Hook PlateMager! has devised a plate and screw system for the cervical spine in which the inferior portion of the plate is ahook that goes under the lamina, the so-called hook-plate(Synthes, Paoli, PA).15 The Arbeitsgemeindschaft furOsteosyntesisfragen group recommends that hook platesbe used for posterior stabilization and fusion over one ortwo cervical motion segments. The hook-plate dependson the integrity of the intervertebral joint. An interspinous H graft is concomitantly used to create stability.A compression force is provided by the plate when thescrews are tightened.
The hook-plates should be contoured to match the posterior aspect of the laminae as well as the articular mass.A corticocancellous H graft is inserted between thespinous processes, with the vertebra in the neutral position. The contoured hook plates are placed into prepared notches (cutting into the laminae medial to thejoints). At this time the cortical screws are inserted into
Fig 3. Halifax clamp Instrumentation. (Top to bottom)Ratchet screw driver, various length Screws and clamps,screw driver.
INSTRUMENTATION TECHNIQUES
the superior articular masses in the technique describedby Mager!.
Transarticular C1-C2 FixationIn the rare event that an odontoid fracture is suffered ina sporting event, there are several therapeutic alternatives available to the surgeon. The standard nonoperative treatment has been the use of a halo. When surgeryis considered, alternatives include the use of anterior fixation using a lag screw across the fracture; posterior ClC2 wiring and fusion; and posterior transarticular screwfixation from C2 to Cl. Some indications for the use ofthe transarticular screw technique include type II odontoid fractures with comminution of the atlantoaxial joints;a fracture of the odontoid with an unstable Jefferson fracture; an unstable type 3 fracture when a halo is unsuitable(elderly patients or those involved with multitrauma); oran atypical type 2 fracture such as those that are comminuted or oblique in the frontal plane and thus unsuitablefor anterior fixation or transverse ligament disruption.The posterior technique should be considered in fracturesof the odontoid in patients with narrow spinal canals.The advantage of the posterior transarticular technique isthat it can be used even in the absence of the posteriorarch.
The technique is technically demanding. The screw isdriven from the tip of the laminae/facet of C2 and acrossthe CI-C2 articulation into the lateral mass of Cl. 16
The patient is in the prone position, and the reduction ofCI-C2 is controlled using an image intensifier in the lateral position. The neck, as well the as head on neck, areflexed as much as possible to facilitate insertion of thescrews. The image intensifier is used to assure that noredislocation occurs during positioning. A standardmidline incision is made from the occiput to the tip of thespinous processes of C7. Subperiosteal exposure of thearch of CI, spinous processes, lamina, inferior articularprocesses of C2, and lamina and articular masses of C3 isperformed. Persistent anterior dislocation of CIon C2may be reduced by pushing on the spinous processes ofC2 and/or by pulling gently on the posterior arch of Cl.This can be accomplished either with a Kocher clamp orwith a sublaminar wire.
A small dissector is used to expose the cranial surfaceof the lamina and isthmus of C2, with careful dissectionup to the posterior capsule of the atlantoaxial joint.Medial to the isthmus, the dura over the spinal cordshould be seen. The laterally situated vertebral arterymay be visualized at C2. Using lateral image intensifiercontrol, a long 2.S-mm drill is inserted in a sagittal direction. The entry point of the drill is at the lower edge ofthe inferior articular processes of C2. The drill goesthrough the isthmus, near its posterior and medial surface. It then enters the lateral mass of the atlas, close tothe posterior-inferior edge. Anteriorly, the drill perforates the cortex of the lateral mass of Cl. The drill tipshould approach the anterior arch of CIon the lateralimage. It should stop at the anterior arch. The screwlength is measured, and the direction of the screw canalis again checked using the image intensifier. The screwsare inserted after tapping with a 3.S-mm tap. Proper
211

direction of the drill in the cranial direction may be difficult because of the neck muscles and upper torso. Drilling in a horizontal direction must be avoided; at the levelof C2 the vertebral artery runs upward anterior to theCI-C2 joint and could be damaged. In addition, thescrew could exit C2 anteriorly and miss the atlas. Afterbilateral screw fixation, a posterior CI-C2 fusion is performed (Fig 4).
In a clinical study Grob et al17 evaluated transarticularscrew fixation of the atlantoaxial joint. Forty-one oftheir patients were either acutely injured or had posttraumatic instability. Fusion was achieved in almost all patients. Screw misplacement is common, however, andcan lead to screw breakage or to pseudarthrosis. Neither, the vertebral artery nor the spinal cord were injuredin any of their patients.
A
212
Montesano? studied the C1-C2 posterior screw technique as an alternative to standard posterior wiring.Magerl's technique is significantly stiffer than the Galliemethod. Anterior-posterior (AP) translation is blockedwith screw fixation . However, this technique requiressignificantly more dissection and does have a narrow"safe" window in which to place the screws when compared to posterior, sublaminar wiring.
Occipitocervical PlatingOccipitocervical fusions are rarely necessary and sometimes difficult to achieve. First reported by Foester in1927 as a means of stabilizing a dens fracture, the technique has been modified several times. Many of thesemodifications use the halo to stabilize the patient in this
B
FG
Fig 4. (A) AP and (B) lateral radiographs of C1-C2 fusionusing facet screws and wiring. Note on the AP film that thescrews cross the C1-C2 facets. (C) CT scan demonstratingfixation of screws into the lateral masses of C1.
GREEN, BAUER. AND GARFIN

extremely unstable situation. However, plate and screwtechniques can be applied to this area and obviate theneed for a halo. Plates directly connect the skull to thecervical spine. Fusion can be restricted in the involvedsegments, there is no manipulation of the spinal canal,and a better, more rigid reduction can be achieved thanwhen using wires.
The posterior skull is suitable for screw fixation. Inthe sagittal plane the occiput has a thick section of boneextending posteriorly from the foramen magnum to theregion of the occipital protuberance. In this region thebone is thickened and can reach a depth of 7 mm. Thisis the region best used to prepare a graft bed and to fix the~raft to ~he occiput. However, the junction of the supenor sagittal and transverse sinuses occurs above thispoint, and one should not go above the occipital protuberance. Grob et aIlS reported on posterior occipitocervical fusions using plates and screws. They recommended using the bone in the middle of the skull, because it is thicker than off the midline, employingY-reconstruction plates molded into shape. We haveused two plates, laterally placed, so that they are in directline with the lateral masses. Both techniques are equallysuccessful. C2 fixation is achieved using pedicularscrews. Occipital screws are bicortical and usually measure 9 to 12 mm. Standard 3.5-mm reconstruction platescan be used, as can specially designed Roy-Camilleplates, Additional instrumentation options are also being developed.
As posterior cervical instrumentation becomes morecommon, new techniques will be described. It is important to keep our eye on the goal of firm arthrodesis of theinvolved region with minimal complications.
ANTERIORCERVICAL INSTRUMENTATION
The use of anterior instrumentation in the cervical spinehas become increasingly popular as part of the treatmentfor traumatic as well as degenerative cervical lesions.At present there are two types of anterior instrumentation commonly used: screw fixation for odontoid fractures and cervical plating for immediate postoperativestability after strut grafting or anterior fusions. The indications for the use of anterior instrumentation in thecervical spine are rapidly expanding. Direct anteriorscrew, fixation of odontoid fractures is being performedmore frequently as clinical studies demonstrate high healing and low complication rates. Plates made specificallyfor the cervical spine, with new designs allowing for unicortical screw fixation in the vertebral body, have madeplate application potentially safer, quicker, and easierthan using bicortical screw fixation. The use of titaniumin cervical implants allows for high quality postoperativeimaging with computed tomography (CT) and MRI.As newer designs emerge and biomechanical and clinicalstudies better define indications, anterior cervical instrumentation may be used increasingly to stabilize fractures,increase fusion, and decrease the need for rigid postoperative bracing.
INSTRUMENTATION TECHNIQUES
Odontoid Screw FixationOdontoid fractures most frequently occur at the junctionof the body of C2 and the base of the dens. Andersonand 0'Alonzo'? classified this as a type II odontoid fracture. In their series of odontoid fractures, 65% weretype II injuries. Even with immobilization in a halo vestthere is a significant incidence of nonunion with theseinjuries. In a multicenter study for the Cervical SpineResear~h Society, Clark and White20 critically evaluatedodontoid fractures and nonunion. In their series of 96type II odontoid fractures, 21 injuries that were left untreated or that were treated with an orthosis went on tononunion. Those that were treated with halo-vest im~ob!l~zation had only a 68% fusion rate. Statisticallysignificant factors associated with nonunion includedfracture displacement greater than 5 mm and angulationgreater than 10°.20 Although in this study an associationb.et",:,~en advanced age and nonunion was not statisticallysignificant, other studies have shown that the nonunionrat~ incre~seswith age over 50 years as well as with postenorly displaced odontoid fractures.P. Opera.tive. treatment :hDuld be considered for those pa
tients with Increased nsk factors for nonunion. Poste-
Fig 5. Cannulated screw instrumentation (Synthes). (Left toright) Cannulated drills, cannulated tap, guide wire and fullythreaded 3.5-mm diameter screw, guide wire and partiallythreaded 3.5-mm diameter screw, reverse measure.
213

A B
Fig 6. (A) Admission lateral radiograph of a type" odontoid fracture. Note the anterior displacement of the odontoid. (B)Lateral radiograph after attempted treatment with a halo vest. Note the posterior displacement of the odontoid. (C) Roomprepared for odontoid screw placement. Note the two C-arms at the head of the bed, the long endotracheal tube extending tothe anesthesiologist at the foot of the bed, and the bite block In the patient's mouth. (D) Postoperative AP radiograph afterscrew fixation of the odontoid. (Continued on next page.)

E
Fig 6. (Cont'd). (E) Postoperative lateral radiograph after screw fixation of the odontoid. (F) CT scan demonstrating accurateplacement of the two fixation screws.
rior C1-C2 fusions using wiring techniques have been thestandard treatment when operative stabilization has beendesired, Fusion rates as high as 96% have been reportedusing these posterior techniques.i'' Although the success rate of atlantoaxial wiring is quite high, there aredisadvantages of this method of treatment. With C1-C2wiring approximately 50% of cervical rotation is lost. 22
In type II odontoid fractures there is a 16% incidence of aconcomitant C1 ring fracture.P With this combinationof injuries, primary posterior C1-C2 wiring is not possible. One must either treat the fracture in a halo until theC1 ring unites, followed by a C1-C2 wiring if the odontoid goes on to a nonunion, or perform a fusion usingC1-C2 transarticular screw fixation, or perform an occiput-C2 fusion. Because of these disadvantages of posterior fusions, direct repair of the fractured dens using lagscrew fixation has been increasing in popularity.
Screw fixation of the odontoid was first performed byNakanishi in Japan and Mager! in Europe in the late19705. Since these early series, techniques have advanced, and complication rates have decreased. Generally, when primary operative therapy is indicated, eg, ina patient with a displaced or angulated type II odontoidfracture, direct fixation can be considered. Also, patients unable to tolerate a halo, such as some polytraumapatients or elderly patients, may be able to avoid halobracing with surgical fusion, C1-2 fusion, or direct odontoid repair. Young patients and athletes may not bewilling to accept the 50% loss of rotation that occurs witha C1-C2 fusion.
Early studies of odontoid screw fixation reported a relatively high complication rate and low fusion rate whencompared with C1-C2 fusions. Using newer techniques,fusion rates are reported as high as 88% to 100% withcomplication rates comEarable with those seen with C1C2 posterior fusions.f -26 The use of two cannulated
INSTRUMENTATION TECHNIQUES
screws has been partially responsible for these improvedresults. However, although two screws may increaserotatory stability at the fracture, not all patients will havea dens large enough to accept two 3.5-mm screws. In ananatomic study looking at the morphology of the dens,Heller et at27 demonstrated that the internal diameter ofthe dens averages 6.2 mm (ranging from 2.8 to 8.7 mm) inthe anterior to posterior diameter. The transverse diameter averaged 4.5 mm, with an even greater range. Thiseloquent study clearly demonstrated that not all patientshave a dens large enough to accept two screws. Therefore, CT is very important in preoperative assessment todetermine if the dens is of adequate size for two screws.Patient size is not helpful to use when estimating odontoid size, because it has been shown that body height andweight are not well correlated with dens size.28
TechniqueWhen the decision is made to perform screw fixation ofthe odontoid, it is important to make all necessary arrangements before the patient arrives in the operatingroom. Equipment required includes a small-fragmentcannulated screw set. We use 3.5-mm cannulated cancellous screws that fit over 1.2-mm guide wires (Synthes);(Fig 5). Two fluoroscopic C-arm image intensifiers arerequired. An experienced fluoroscopy technician in theoperating room is important for the procedure is to runsmoothly. A radiolucent bite block is used to obtain an"open mouth odontoid" view in the AP plane. The procedure is simplified if the room is arranged so that theimage intensifiers are at the head of the patient and theanesthesiologist is at the foot. The anesthesiologistshould be told of this preoperatively so that he or she willset up the anesthetic machines at the foot of the bed andhave a long endotracheal extension tube available to run
215

from the endotracheal tube at the head of the bed to therespirator at the foot. The patient's head must be heldrigidly during the procedure.
An awake intubation is performed, and the patient isthen positioned. The image intensifiers must be set upbefore beginning the procedure to be absolutely certainthat the odontoid is adequately visualized and reduced inthe AP and lateral planes. Both of the C-arms are left inposition so that they do not have to be manipulated during the procedure.
The angle that the guide wire must take is acute withrespect to the neck and chest. If the patient has a shortneck or large barrel-shaped chest, there may not be roomto drop the drill (hand) to appropriately align the wireand drill it into the dens. This can be roughly assessedpreoperatively by laying a guide wire lateral to the neckand obtaining a lateral image with the wire following thedesired path. It may be necessary to extend the neck toallow more space (be cautious of displacing the odontoid), or it may be necessary to have an assistant press onthe chest when the wire is being drilled into position.
A standard anterolateral, Smith-Robinson approach tothe cervical spine, centered at the CS-6 disc space, is performed using the interval between the carotid sheathstructures laterally and the esophagus and trachea medially. When the cervical spine is reached, blunt fingerand sponge-stick or peanut-gauze dissection is carriedsuperiorly until the C2-3 disc space is palpated and visualized, The initial approach is made at the CS-6 level,because it is necessary to start low to obtain the necessaryangle to place the wires from the anterior-inferior cornerof C2 into the tip of the dens.
Using the 1.2-mm guide wire with an overriding softtissue protector, the wire is drilled beginning at the inferior end plate of C2 at its most anterior edge. Flatteningthis edge with a small burr is helpful to keep the wiresfrom slipping off the edge. If two screws are to be used,it will be necessary to start slightly lateral to the midlineand aim slightly medial. If only one screw is used, thestarting point is in the midline. The anterior-toposterior angle is shallow so that the guide wire exits thetip of the dens in the midline or slightly posterior to themidline when seen in the lateral plane. The wire shouldengage the outer cortex of the cephalic tip of the dens.If two screws are used, both guide wires should be placedbefore the insertion of either screw. In the latter case,only one wire is required to penetrate the outer cortex ofthe dens, because only one screw (the screw insertedfirst) is needed to compress the fracture. The otherscrew is to increase fixation and rotatory control; therefore, the threads do not necessarily have to all be acrossthe fracture line.
After the guide wires are in place they are measured,and screw length is determined. A cannulated drill isplaced over the wires, and the screw path is drilled.This must be done under fluoroscopic imaging, becausethe guide wires may bind in the cannulated drill and bepushed forward into the foramen magnum as the drillingproceeds, resulting in potentially catastrophic injury.Often, the guide wires are pulled out as the cannulateddrill is removed. They should be reinserted under fluoroscopic guidance. After tapping, the screws are then
216
inserted over the wires. As in the other cannulatedsteps, great care must be used to visualize the insertion ofthe screws with fluoroscopy to be sure that the wires donot bind and migrate proximally. As stated above, atleast one screw (the first screw placed) should have all ofits threads across the fracture site so that the fracture canbe compressed. The tip of the screw should be placedinto the outer cortex of the dens to increase its purchase(Fig 6).
After screw insertion, the guide wires are removed,and the wound is irrigated and then closed over a drain.Postoperatively, the patient should be placed in a rigidorthosis (not necessarily a halo), which should worn forapproximately 8 to 12 weeks.
Anterior PlatingAnterior plating of the cervical spine is becoming morecommon as indications are increasing. Anterior platingadds immediate stability across injured motion segmentswhile fusion takes place. We find plating useful whenwe perform an anterior corpectomy with strut grafting.The plate adds immediate stability and often allows thepatient to be put in a hard collar or cervicothoracic orthosis rather than a halo vest. The plate decreases the likelihood of anterior displacement of the bone graft and, if ascrew is placed in the graft, of posterior displacement.
There are varying opinions as to whether anterior plating should be performed in the case of posterior injury orin combined anterior and posterior injury. Clinically,there are reports of anterior plating without additionalposterior fusion and instrumentation or postoperativehalo brace treatment for isolated posterior injuries such asfacet fractures and dislocations. The results in these series support the possible use of anterior stabilization forposterior instability.29,30 Also, in combined anterior andposterior instability, clinical studies have demonstratedthat treatment with anterior plating alone, without combined posterior surgery or postoperative halo vest immobilization, has a high success rate. 29,30 However, biomechanical studies have not supported this in injury models. In a posterior flexion-distraction injury model,posterior wiring demonstrated significantly greater stiffness and strength compared with anterior plating.Montesano et af recommend that in flexion type injuries,anterior instrumentation should be supplemented withposterior instrumentation or rigid external immobilization. Ulrich et al31 evaluated flexural and torsional stability in injuries involving anterior and posterior structures. They demonstrated that, in isolated posterior instability, posterior instrumentation alone or combinedwith anterior plating restored rotational stability equal orgreater to that of the intact specimen. Similarly, in complete anterior and posterior discoligamentous instability,anterior fixation with plating was not adequate fixationby itself, and additional posterior instrumentation orpostoperative halo vest bracing was necessary.
We presently treat posterior instability, such as facetfracture/dislocations, with posterior plating or wiring unless a discectomy is required. In the case of significantcombined anterior and posterior injuries, such as a burstfracture with combined posterior instability, we perform
GREEN, BAUER, AND GARFIN

an anterior corpectomy, strut grafting, and plating.Additional posterior fusion and instrumentation are performed if there is a posterior injury that would lead toposterior instability. Halo bracing may be consideredinstead of the additional posterior fusion in this situation.
Presently, there are two instrumentation systems thatwe commonly use . The Caspar (Aesculap, Tuttlingen,Germany) system consists of a plate and screws. Therecommended technique includes bicortical fixation, necessitating drilling the posterior cortex of the vertebralbody. The Cervical Spine Locking Plate (CSLP;Synthes)is a modification of the Orozco (Synthes) Cervical Plate,which, like the Caspar plate, required bicortical screwpurchase. However, the CSLP uses unicortical bone anchoring screws whose heads are recessed into the plate.A smaller locking screw then screws into the head of thebone screw. As this smaller screw is tightened, the bonescrew's head expands, locking the bone screw into theplate. By locking the screws into the plate, there is increased stability at the plate-screw interface. An individual screw cannot back out of the plate; rather, theplate would have to pull out. The rostral screws areangled 12° cephalad and 10° convergent; the caudalscrews also converge 10°, decreasing the incidence of theplate backing out. The bone screws are a solid 4 mm indiameter and 14 mm in length. Although 14-mm screwsshould not penetrate the posterior cortex, we have seenone adult patient in whom the 14-mm length resulted inbicortical purchase.
Although the CSLP has the significant advantage ofrequiring only unicortical purchase, we have found theCaspar system to be useful. Therefore, we believe thatskill in bicortical screw placement is valuable. We presently use the Caspar system when the bone is soft andunicortical purchase is not secure and when revision surgery is required in a patient with a CSLP in place.
Caspar plating. In preparation for plating, the surgeon must be certain that all instruments are availablebefore making the incision. An approximation of plateand screw length can be made preoperatively by measuring the plain radiographs. The Caspar system includesa vertebral body distractor, which screws into the vertebral bodies above and below the decompression site.This instrument is useful in opening the disc space orcorpectomy site during decompression and graft insertion (Fig 7). Fluoroscopy is helpful for screw placement,particularly during posterior cortex drilling and in aligning the screws parallel to the end plates. A standardanterolateral approach to the cervical spine is made usingthe interval between the sternocleidomastoid muscle andcarotid sheath laterally and the trachea and esophagusmedially. A transverse incision using Langer's lines ismade if a single-level discectomy or corpectomy is to beperformed. A longitudinal oblique incision, parallel tothe anterior border of the sternocleidomastoid muscle, ishelpful if more than a two levels are resected or if thepatient has an unusually short, thick neck.
The Caspar vertebral body distractor requires the placement of a distractor screw into the body above and belowthe decompression site. These screws are unicorticaland should be inserted as close to parallel as possible .
CRITERIA FOR RETURN TO COLLISION ACTIVITIES
Fig 7. Caspar cervical Instruments (Aesculap). (Left to right)Drill and adjustable-depth drill guide; Caspar dlstractor withdistraction screws.
After the decompression has been completed, thedepth of the vertebral body should be measured with adepth gauge. This should be performed for the vertebral body on each side of the decompression. The graftis then keyed in with the cervical spine distracted. Thedistraction is released, and the plate is applied. Afterchoosing a plate of the proper length, it should be bentinto the desired lordosis. The Caspar drill guide has adepth stop to prevent overdrilling. This should initiallybe set to 1 to 2 mm less than the measured vertebral bodydepth. The drill guide must seat fully into the plate forproper drilling depth and screw positioning. Under fluoroscopic guidance the screw holes are then drilled .Until experience is gained, it may be safer to shorten thedrill guide 1 to 2 mm at a time to allow controlled penetration of the posterior cortex. Using fluoroscopic imaging, the holes are measured with a depth gauge andtapped, and the are screws inserted. It is extremely important in this system that the posterior cortex be engaged to prevent screw loosening. Shorter, unicorticalscrews can be placed in the strut graft to decrease motionat the graft-vertebral body interface and to stabilize thegraft from possible posterior displacement (Fig 8).
Even using a controlled drilling technique with fluoroscopic imaging, it is possible to overdrill or underdrill theposterior cortex. Overdrilling increases the risk of neurological injury and underdrilling the risk of screw loosening. Segal and Cahill32 demonstrated that because ofthe difficulty of imaging and the concave posterior cortex,
217

Fig 8. (A) AP and (B) lateral radiographs demonstrating the Caspar cervical plate. Note the bicortical screw fixation.
particularly at C7 and TI, it is extremely difficult to knowthe exact relationship of the screw to the posterior wall ofthe vertebral body. Great caution must be used at theselevels, and consideration must be given to using instrumentation that requires unicortical screw fixation.
CSLP. Application of the CSLP is similar to that of theCaspar system except that fluoroscopy is not necessarybecause the screws are all one length, and the posteriorcortex is not penetrated. After the decompression or
Fig 9. The CSLP. (Left to right) Plate holder, plate, anchoringscrews with smaller locking screws (fenestrated screws notpresently available), tap and guide with depth stop, drill andguide with 14·mm depth stop.
218
discectomy is complete, a plate of the appropriate lengthis chosen. Bone near the end plates has the best purchase; however, it must be remembered that the rostralscrews angle 12° cephalad, and care must be taken toensure that the screws will not enter the disc space.Attention also should be paid to center the plate as muchas possible, because it is easy to mistakenly apply theplate lateral to midline in the direction of the approach.
The CSLP comes with a plate holder, which can beused to hold the plate in position while the first screwhole is drilled. The drill guide must be used, because ithas a drill stop that limits the drill from penetrating beyond 14mm when used with the drill that comes with theCSLP set. It also seats into the screw holes in the plateand directs the drill in the proper manner so that thescrews will be angled correctly (the rostral screws shouldbe 12° cephalad and 10° medial, and the caudad screwsshould be 10° medial; Fig 9).
After the hole is drilled, tapping is recommended. The soft-tissue protector should be used with thetap that comes with the CSLP set, because it also has astop that limits tapping to 14 mm. The bone-anchoringscrews are then inserted but not fully tightened. Thefirst two screws inserted should be the most proximal andmost distal screw on opposite sides of the plate. Thiswill ensure that the plate will be aligned adequately alongits length.
After all screws have been placed through the plate,tightening of the screws should be completed. Thescrews must sit recessed in the plate before insertionof the locking screws. If the anchoring screws are notfully seated into the plate, the locking screws will notexpand properly, and screw-plate fixation will not be secured.
The 1.8-mm locking screws are inserted. These locking screws seat within the head of the anchoring screws.As the locking screws are tightened, they cause the headof the anchoring bone screw to expand, pressing againstthe plate and locking the screw to the plate (Fig 10).
Postoperative immobilization is tailored to the injury.Generally, if carpectomy and plating is performed, halo
GREEN, BAUER, AND GARFIN

Fig 10. (A) Lateral radiograph (in traction) of a C6 burst fracture. The patient had an incomplete central cord syndrome.Postoperative (B) AP and (C) lateral films. The patient underwent C6 corpectomy, autologous iliac crest strut grafting,and stabilization with the CSLP.

vest bracing is unnecessary. If there is a significant posterior injury that is not stabilized surgically, halo vest orcervicothoracic bracing may be necessary. In most othercases we use a rigid cervical orthosis for 8 to 12 weeks.
Complications of anterior cervical spine surgery canlead to significant morbidity and mortality. The carotidsheath structures, the trachea and esophagus, and therecurrent laryngeal and superior laryngeal nerves are inclose proximity to the operative site. These structuresare all at danger during exposure and insertion of hardware.
Anteriorly placed hardware can erode through theesophagus, resulting in significant complications. In aseries of 22 reported cases of esophageal perforation frommembers of the Cervical Spine Research Society, the useof anterior instrumentation in fracture patients was mostclosely correlated with this complication. Of those perforations recognized after surgery, 40% were related tohardware.P
Although the use of anterior cervical instrumentation isincreasing, one must remember that these procedures aredemanding and should be performed only by those thoroughly familiar with anterior cervical spine surgery andthose with training in instrumentation implantation techniques.
REFERENCES1. Allen BL, Ferguson RL, Lehman TR, et al: A mechanistic classifica
tion of closed, indirect fractures and dislocations of the lower cervical spine. Spine 7:1-27, 1983
2. Coe JC, Warden KE:Biomechanical evaluation of cervical spine stabilization methods in a human cadaveric model. Spine 14:1122-1131,1989
3. Anderson PA, Henley MB, Grady MS, et al: Posterior cervical arthrodesis with AO reconstruction plates and bone graft. Spine 16:72-79, 1991
4. Capen DA, Zigler J, Garland DE: Surgical stabilization in cervicalspine trauma. Con temp Orthop 14:25-32, 1987
5. Ebraheim NA, An H5, Jackson, WT, et al: Internal fixation of theunstable cervical spine using posterior Roy-Camille plates: Preliminary report. J Orthop Traumatol 3:23-28, 1989
6. Heller JG, Carlson GD, Abitbol 11, et al: Anatomic comparison of theRoy-Camille and Magerl techniques for screw placement in thelower cervical spine. Spine 16:5552-5557, 1991
7. Montesano PX, [uach EC, Anderson PA, et al: Biomechanics ofcervical spine fixation. Spine 16:510-516, 1991
8. Gill K, Paschal 5, Corin J, et al: Posterior plating of the cervicalspine: A biomechanical comparison of different posterior fusiontechniques. Spine 13:813-816, 1988
220
9. An H5, Gordin R, Renner K: Anatomic considerations for platescrew fixation of the cervical spine. Spine 16:5548-5551, 1991
10. Holness RO, Heustis WS, Howes WJ, et al: Posterior stabilizationwith an interlaminar clamp in cervical injuries: Technical notes andreview of long term experience with the method. Neurosurgery14:318-322, 1984
11. White AA, Panjabi M: Clinical Biomechanics of the Spine. Philadelphia, PA, Lippincott, 1991
12. Cybulskigr AB, Stone JL, Crowell RM: Use of Halifax interiaminarclamps for posterior CI-2 arthrodesis. Neurosurgery 22:429-431,1988
13. Aldrich EF, Crow WN, Weber PB, et al: Use of MR imaging compatible Halifax interlaminar clamps for posterior spinal fusion. JNeurosurg 74:185-189, 1991
14. Tucker HH: Method of fixation of subluxed or dislocated cervicalspine below CI-C2. Can J Neurol Sci 00:381-382, 1975
15. [eanneret B, Magerl F, Haletrward E, et al: Posterior stabilization ofthe cervical spine with hook plates. Spine 16:556-563, 1991
16. Mueller ME, Allgower M, Schneider R, et al: Manual of InternalFixation: Techniques Recommended by the AO-ASIF Group (ed 3).Berlin, Germany, Springer-Verlag, 1991, pp 634-635
17. Grob D, Jeanneret B, Aebi M, et al: Atlanto-axial fusion withtransarticular screw fixation. J Bone Joint Surg [BI 73:972-976, 1991
18. Grob D, Dvorak J, Panjabi M, et al: Posterior occipitocervical fusion:A preliminary report of a new technique. Spine 16:517-524, 1991
19. Anderson LD, D'Alonzo RT: Fractures of the odontoid process ofthe axis. J Bone Joint Surg [AI 56:1663-1674, 1974
20. Clark CR, White AA: Fractures of the dens. J Bone Joint Surg [AI67:1340-1348, 1985
21. Schatzker J, Rorabeck CH, Waddell JP: Non-union of the odontoidprocess. CIin Orthop 108:127-137, 1975
22. Penning L, Wilmink JT: Rotation of the cervical spine: A CT studyin normal subjects. Spine 12:732-738, 1987
23. Montesano PX, Anderson PA, Schlehr F, et al: Odontoid fracturestreated by anterior odontoid screw fixation. Spine 16:533-537, 1991
24. Aebi M, Etter C, Coscia M: Fractures of the odontoid process: Treatment with anterior screw fixation. Spine 14:1065-1070, 1989
25. Apfelbaum RI: Odontoid screw fixation. Presented at the CervicalSpine Research Society, December, 1992
26. Etter C, Coscia M, [abery H, et al: Direct anterior fixation of densfractures with a cannulated screw system. Spine 16:525-532, 1991
27. Heller JG, Alson MD, Schaffler MB, et al: Quantitative internal densmorphology. Spine 17:861-866, 1992
28. Schaffler MB, Aslon MD, Heller JG, et al: Morphology of the dens.Spine 17:738-743, 1992
29. Aebi M, Zuber K, Marchesi D: Treatment of cervical spine injurieswith anterior plating. Spine 16:538-545, 1991
30. Ripa DR, Kowall MG, Meyer PR, et al: Series of 92 traumatic cervicalspine injuries stabilized with anterior ASlF plate fusion techniques.Spine 16:546-555, 1991
31. Ulrich C, Woersdoerfer 0, Kalff R, et al: Biomechanics of fixationsystems to the cervical spine. Spine 16:54-59, 1991
32. Segal J, Cahill D: Placement of anterior cervical instrumentationwithout intraoperative radiography. J Spinal Disord 5:162-169, 1992
33. Newhouse KE, Lindsey RW, Clark CR, et al: Esophageal perforationfollowing anterior cervical surgery. Spine 14:1051-1053, 1989
GREEN, BAUER, AND GARFIN