Principles of Therapeutic Exercise Exercise Prescription Week 4 Jane Simmonds.
30
Principles of Principles of Therapeutic Exercise Therapeutic Exercise Exercise Exercise Prescription Prescription Week 4 Week 4 Jane Simmonds Jane Simmonds
-
Upload
shona-shaw -
Category
Documents
-
view
236 -
download
3
Transcript of Principles of Therapeutic Exercise Exercise Prescription Week 4 Jane Simmonds.
Principles of Principles of Therapeutic ExerciseTherapeutic Exercise
Exercise PrescriptionExercise PrescriptionWeek 4Week 4
Jane SimmondsJane Simmonds
FormatFormat
• Exercise in the context of the physiotherapy profession and practice
• Review the principles of training • Review the different types of exercise• Explore the concept of exercise prescription
for the prevention and management of diseases and disorders
• Review muscle physiology
Learning OutcomesLearning Outcomes
• By the end of the session and independent study you should;– Understand the cope of exercise used in
physiotherapy practice – Understand the principles of training– Understand the concept of training variables
Core Skills - Core Skills - PhysiotherapyPhysiotherapy
• Movement analysis• Manual therapy• Electrotherapy• Exercise therapy – exercise prescription (ACPET)
Exercise for the prevention Exercise for the prevention of diseaseof disease
• Relationship between a sedentary lifestyle and chronic degenerative disorders
• More than 20 disorders related to inactivity
• 50 years of research– Seminal research bus
conductors– Parffenbarger’s research
• Physiotherapists have a role to play in health promotion Morris & Crawford 1958
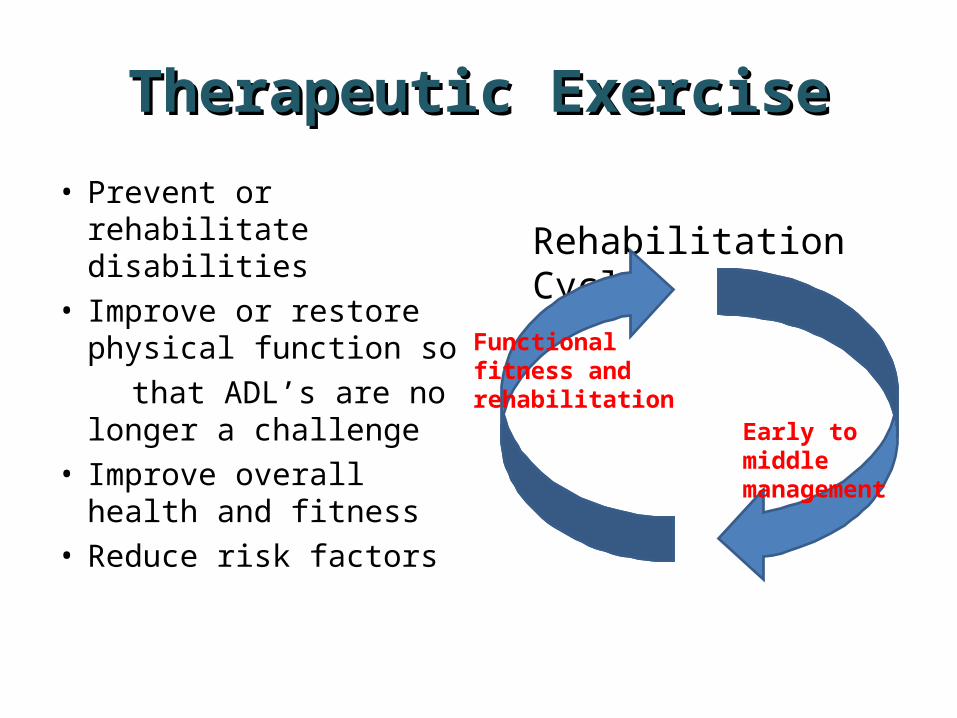
Therapeutic ExerciseTherapeutic Exercise
• Prevent or rehabilitate disabilities
• Improve or restore physical function so
that ADL’s are no longer a challenge
• Improve overall health and fitness
• Reduce risk factors
Rehabilitation Cycle
Early to middle management
Functional fitness and rehabilitation

Which patients groups Which patients groups benefit from therapeutic benefit from therapeutic
exercise?exercise?• Cardiac patients• Orthopaedic patients• Amputees• General surgical• Neurological• Elderly• Learning disabilities• Psychiatric• Palliative care
• Respiratory• Paediatric• Rheumatology• Musculo-skeletal• Occupational• Spinal injuries• Obstetrics• Gynacological• Burns and plastics
Aims of Therapeutic Aims of Therapeutic ExerciseExercise
• Enable ambulation• Release contracted soft tissues• Mobilise joints• Improve circulation• Improve respiratory capacity• Decrease stiffness
Aims of Therapeutic Aims of Therapeutic ExerciseExercise
• Improve muscle strength
• Improve endurance• Improve co-ordination• Promote confidence
and wellbeing • Improve balance• Promote relaxation
Overarching GoalOverarching Goal
• To try whenever possible to restore full function and achieve an optimal level of physical fitness.
• Achieve this by setting shared realistic goals and identifying how fit the client needs to be.
• Motivation• Adherence, compliance
and concordance
Designing Exercise Designing Exercise ProgrammesProgrammes
• When designing an exercise programme consider;
• Pathology• Person (age, personality
– psychology)• Needs - aspirations• Environment• Physiological processes• Principles of training
Types of ExercisesTypes of Exercises
• Stretching• Range of movement
exercises• Strengthening exercises• Endurance exercises• Proprioceptive or
balance training• Cardio-vasacular
training
Principles of TrainingPrinciples of Training
• Readiness• Overload • Specificity• Motivation• Learning• Reversibility• Diminishing returns
Prescription VariablesPrescription Variables
• 5 key components• Frequency• Duration• Intensity• Type of exercise• Progression
StretchingStretching• Passive or active• Stretching to retain range
e.g. joint pathology• Stretching to increase
normal range e.g. sport and dance
• Stretching to lengthen contracted, fibrosed, shortened tissue e.g. congenital conditions, post-surgery/immobilisation/injury
• How long should we stretch for?
Mobility ExercisesMobility Exercises
• Active assisted Usually used as interim
measure moving from passive to active, also when joint pain limits free active movement
• Free active• Knowledge of aging and
pathologies required to prevent undesirable movements e.g. trunk flexion exercises in osteoporosis
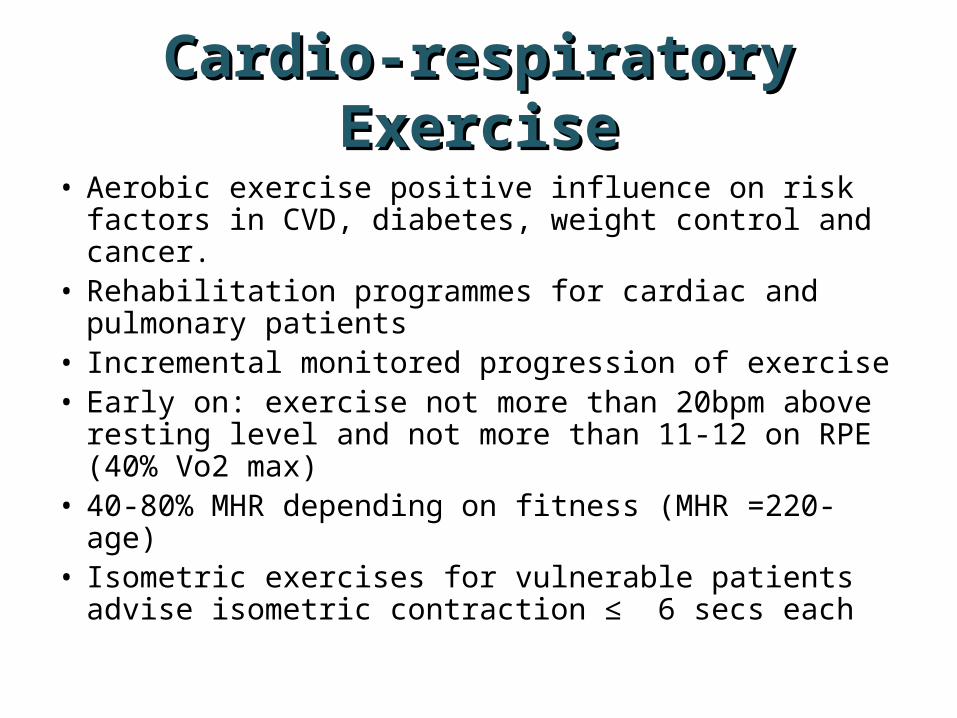
Cardio-respiratory Cardio-respiratory ExerciseExercise
• Aerobic exercise positive influence on risk factors in CVD, diabetes, weight control and cancer.
• Rehabilitation programmes for cardiac and pulmonary patients
• Incremental monitored progression of exercise• Early on: exercise not more than 20bpm above resting
level and not more than 11-12 on RPE (40% Vo2 max)• 40-80% MHR depending on fitness (MHR =220-age)• Isometric exercises for vulnerable patients advise
isometric contraction ≤ 6 secs each
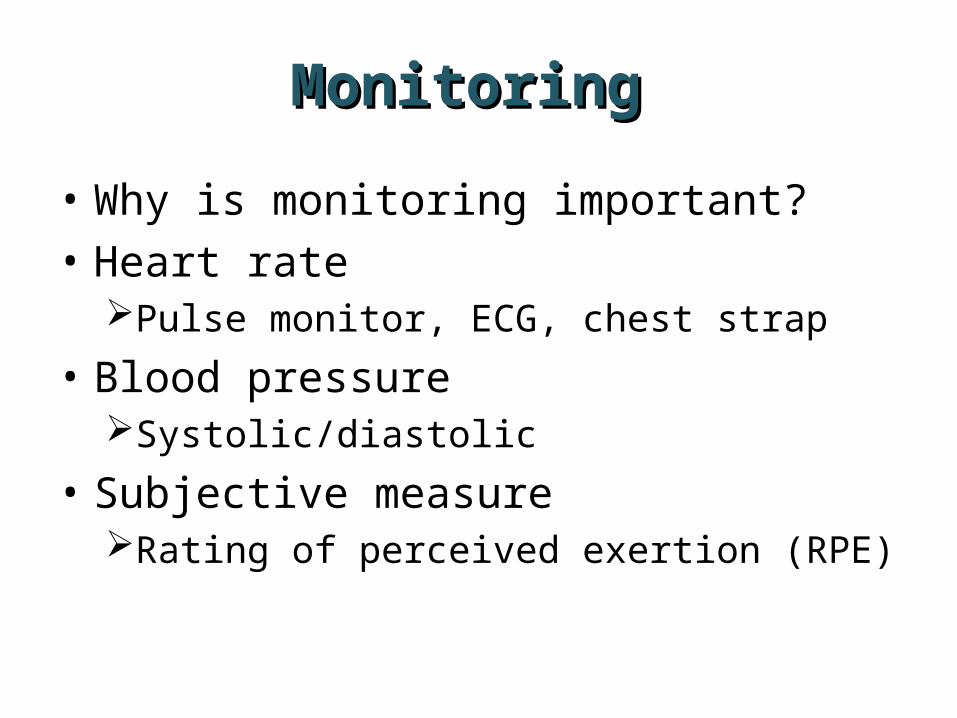
Monitoring Monitoring
• Why is monitoring important?• Heart rate
Pulse monitor, ECG, chest strap
• Blood pressureSystolic/diastolic
• Subjective measure Rating of perceived exertion (RPE)
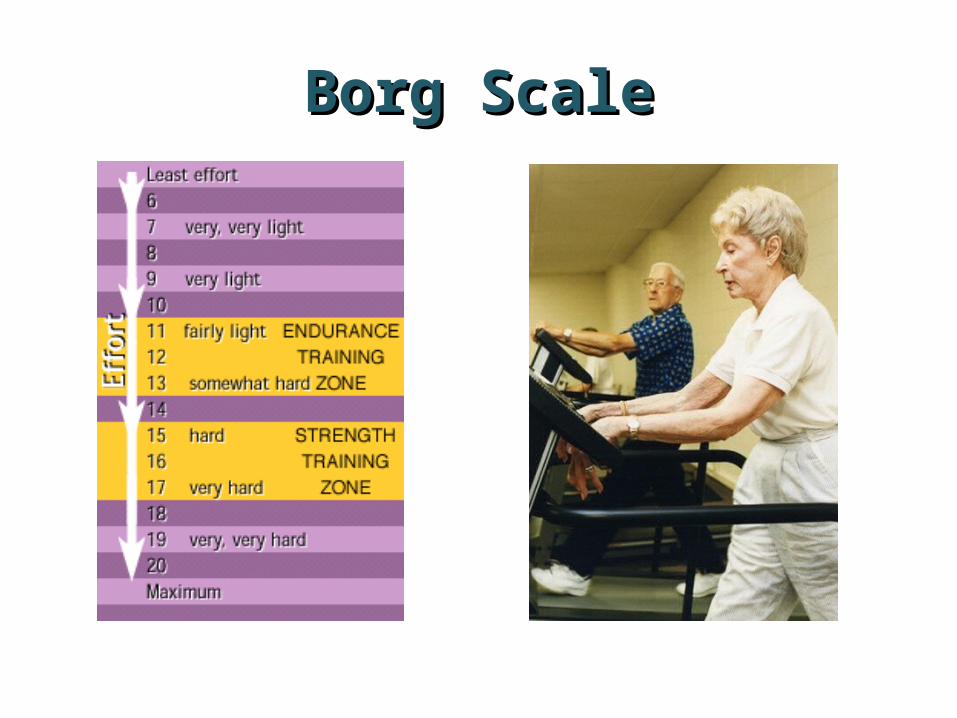
Borg ScaleBorg Scale
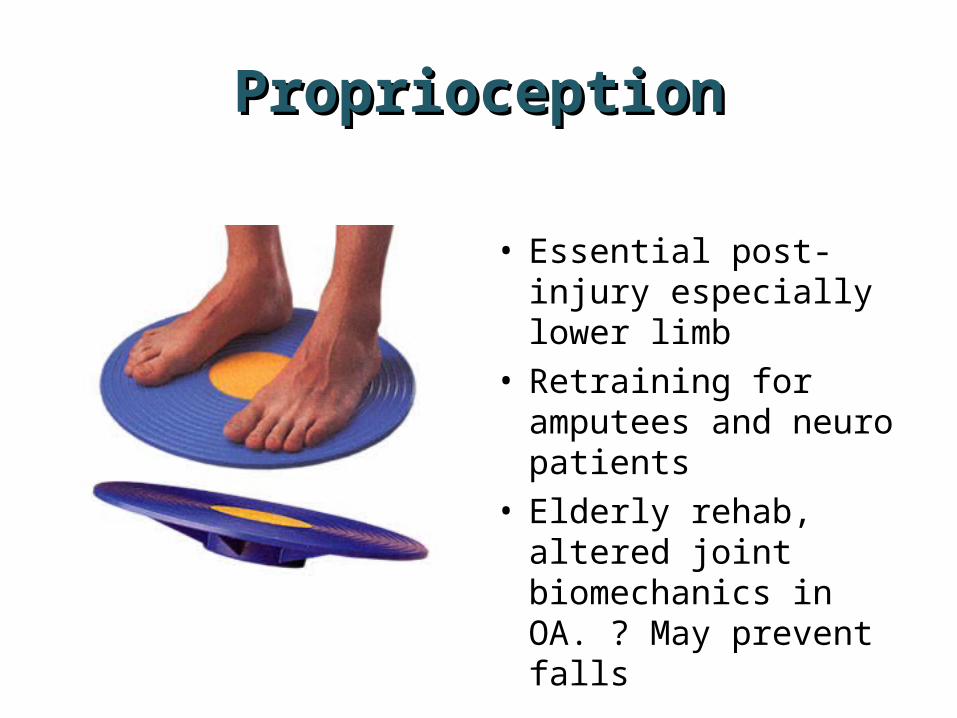
ProprioceptionProprioception
• Essential post-injury especially lower limb
• Retraining for amputees and neuro patients
• Elderly rehab, altered joint biomechanics in OA. ? May prevent falls
Muscle Contractions and Muscle Contractions and Resistance ExercisesResistance Exercises
• Consider why we might choose these different types of exercises?
• Are there any risks?• Isometric• Concentric• Eccentric• Isokinetic• Closed and open chain
exercises
Strength, Power and Strength, Power and EnduranceEndurance
• What is the difference?• Load (resistance)• Repetitions• Sets• Frequency• Consider muscle fibre
type

Muscle Fibre TypesMuscle Fibre Types
• Skeletal muscle fibers are classified into two major categories; slow-twitch (Type 1) and fast-twitch fibers (Type II).
• The difference between the two fibers can be distinguished by; – metabolism– contractile velocity– neuromuscular differences– glycogen stores – capillary density of the muscle – and the actual response to hypertrophy
Fibre TypeFibre Type• Slow twitch – type 1
– Rich in haemaglobin– Mitochondria– Rich in blood vessels– Red– Common postural muscles.
• Slow twitch – type II• Type II a - fast oxidative -
fatigue resistant – fast oxidative fibres
• Type II (b)x - fast glycolytic fibres - split ATP at a fast rate and have a fast contraction velocity.
Progressing ExerciseProgressing Exercise
• Overload principle• Motivation principle• Strength?• Endurance?• Power?• Complexity of task• Functional
Exercise PrescriptionExercise Prescription
• Exercise prescription is based on physiological principles and laws of training and modified by clinical findings.– Pain– Underlying medical conditions – diabetes,
cardiovascular disease, diabetes, psychological factors etc.
– Safety
Exercise prescription requires Exercise prescription requires a detailed knowledge of;a detailed knowledge of;
• Motor learning• Anatomy• Biomechanics/pathomechanics• Kinesiology• Pathology• Exercise physiology
Exercise PsychologyExercise Psychology
• Adherence, compliance and concordance• Goals• Patient factors: age, sex, socio-economics,
fear, self-efficacy, support• Programme factors: personnel, education,
attention, group dynamics, logistics
SummarySummary• Exercise prescription is a core skill
for physiotherapists• Underpinned by physiological and
patho-physiological processes• Requires a good understanding of
exercise physiology and the principles of training
• Motivational psychology - stages of change
• ImaginationImagination
ReferencesReferences
• Hanandez Kravitz (2006) http://www.unm.edu/~lkravitz/Article%20folder/hypertrophy.html
• Robergs, R. A. and S. O. Roberts(1997) Exercise Physiology: Exercise, Performance, and Clinical Applications. Boston, WCB McGraw-Hill
• National Institute on Aging (2005) www.niapublications.org/exercisebook/chapter4.htm .
• Skinner JS (2005) Exercise Testing and Exercise Prescription for Special Cases. Philadelphia, Lippincott, Williams &
Wilkins• Woolf-May K (2006) Exercise Prescription – physiological
foundations. Churchill Livingstone