Principles of Mechanical Ventilation in ICU Raafat Abdel Azim.
Upload
rashmit-shresthaCategory
view
197download
3
Principles of Mechanical Ventilation
Presenter : Dr. Rashmit Shrestha (1st yr Resident)Moderator : Dr. Ramesh GhimireDepartment of Anaesthesiology, NMCTH,
Birgunj, Nepal16th Aug,2016.

Introduction:Mechanical ventilation is a useful modality for patients who are unable to sustain the level of ventilation necessary to maintain the gas exchange functions (oxygenation and carbon dioxide elimination).
Indications for mechanical ventilation vary greatly among patients.

Mechanical ventilation may be indicated in conditions due to :-
◦Physiologic changes (e.g., deterioration of lung parenchyma), disease states (e.g., respiratory distress syndrome)
◦ Medical/surgical procedures (e.g., postanesthesia recovery)
◦and many other causes (e.g., head trauma, drug overdose) leading to ventilatory failure or oxygenation failure.

Airway ResistanceAirflow obstruction in the
airways. In mechanical ventilation, the
degree of airway resistance is primarily affected by the Length, sizepatency of the airway, endotracheal tubeventilator circuit.

Factors Affecting Airway Resistance Airway resistance causes obstruction of airflow in the airways. It is increased when the patency or diameter of the airways is
reduced. Obstruction of airflow may be caused by:
(1) changes inside the airway (e.g., retained secretions) (2) changes in the wall of the airway (e.g., neoplasm of the bronchial muscle structure) (3) changes outside the airway (e.g., tumors surrounding and compressing the airway)
When one of these conditions occurs, the radius of the airway decreases and airway resistance increases.
Radius Air Resistance

Hagen–Poiseuille Equation
Simplified form of Poiseuille's Law:
∆P = V r4

Poiseuille’s LawBased on this law, 1) the work of breathing increases by the factor of
16 fold when the radius ( r ) of the airway is reduced by half its original size.
2) Airway resistance α length
3) Airway resistance α 1 diameter of airway or ET tube

Airway Resistance and the Work of Breathing (∆P)
Airway resistance = Pressure Change Flow Raw = ∆P VWhere, Raw = airway resistance ∆P = pressure change ( Peak Inspiratory Pressure – Plateau pressure)V = Flow
↑airway resistance = ↑work of breathing

HypoventilationInadequacy of ventilation to remove CO2. The
arterial PCO2 is elevated in this condition.
COPD high compliance deeper slower
RLD low compliance shallower faster


Effect on Ventillation and Oxygenation
Abnormally ↑airway resistance → fatigue →ventilatory and oxygenation failure
Ventilatory Failure : Failure of the respiratory system to remove CO2 from the body.
Oxygenation Failure: Failure of the heart and lungs to provide adequate oxygen for metabolic needs.

Airflow Resistance

Lung Compliance The degree of lung expansion per unit pressure
change.
C = ∆V / ∆Pwhere,C = compliance,∆V = volume change (lung expansion)∆P = pressure change (work of breathing)

Lung Compliance
Plateau Pressure: The pressure needed to maintain lung inflation in the absence of airflow.
Peak Inspiratory Pressure: The pressure used to deliver the tidal volume by overcoming nonelastic (airways) and elastic (lung parenchyma)resistance.



Compliance MeasurementLow and high compliance impairs the patient’s ability to
maintain efficient gas exchange. These abnormalities lead to mechanical ventilation.
↓ Lung compliance = ↑ work of breathing ↑↑↑ compliance situations, exhalation is often
incomplete d/t ↓ elastic recoil of the lungs

low complianceE.g : ARDSlow comliance is a/w refractory
hypoxemia.Refractory hypoxemia: A persistent
low level of oxygen in blood that is not responsive to medium to high concentration of inspired oxygen. (intrapulmonary shunting ).
Leads to ↓ :- FRC , lung volume, minute ventilation
This condition is compensated by ↑ frequency.

High compliance ↑C = ↑∆V / ∆PExhalation is often incomplete d/t lack of elastic recoil of lungs e.g. Emphysema d/t chr. Air trapping, destruction of lung tissues, enlargement of
terminal and respiratory bronchioles.
↑ FRC and TLCPt. develop airflow obstruction, incomplete exhalation, air
trapping and poor gas exchange.

Static Compliance Static compliance (SC) reflects the elastic
properties (elastic resistance) of the lung and chest wall.
SC = volume pressure (i.e. plateau pressure)It is measured when the flow is momentarily
stopped.
NO Airflow → NO Airway Resistance

Dynamic ComplianceDynamic compliance (DC) reflects the airway
resistance (nonelastic resistance) and the elastic properties of the lung and chest wall (elastic resistance).
DC = volume pressure (i.e. peak inspiratory pressure)
Its measured when airflow is present.
Therfore , airway resistance becomes a factor in the measurement of dynamic compliance.




Lung Compliance The degree of lung expansion per unit pressure
change.
C = ∆V / ∆Pwhere,C = compliance,∆V = volume change (lung expansion)∆P = pressure change (work of breathing)

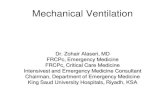
Pressure – Volume Loop
Its essentially a “compliance loop,” and it provides useful information on the characteristic of a patient’s compliance.



DEADSPACE VENTILATIONVentilation in excess of perfusion,wasted ventilation3 types of Deadspace ventilation.A. Anatomic deadspace: The volume occupying the conducting
airways that does not take part in gas exchange (estimated to be 1 mL/lb ideal body weight.
B. Alveolar deadspace: The normal lung volume that has become unable to take part in gas exchange because of reduction or lack of pulmonary perfusion (e.g.pulmonary embolism).
C. physiologic deadspace: Sum of anatomic and alveolar deadspace Under normal conditions, it is about the same as anatomic deadspace.

Ventilatory Failure Inability of the pulmonary system to
maintain proper removal of carbon dioxide.
Hypercapnia (increase in PaCO2) is the key feature of ventilatory failure.

Five mechanisms leading to the development of Ventilatory Failure.

V/Q mismatch: An abnormal distribution of ventilation and pulmonary blood flow. High V/Q is related to deadspace ventilation, whereas low V/Q is associated with intrapulmonary shunting.
Intrapulmonary shunting: Pulmonary blood flow in excess of ventilation; wasted perfusion (e.g.,atelectasis).
Diffusion defect: Pathologic condition leading to impaired gas exchange through the alveolar-capillary membrane (e.g.,interstitial or pulmonary edema).

OXYGENATION FAILUREOxygenation failure is defined as severe hypoxemia
that does not respond to moderate to high levels of supplemental oxygen.
Causes: hypoventilation, ventilation/perfusion mismatch, or intrapulmonary shunting.
Regardless of the etiology of oxygenation failure, mechanical ventilation may be needed to minimize the work of breathing and provide oxygenation support.

Hypoxemia and HypoxiaHypoxemia is present when the oxygen level (e.g.,
PO2, SaO2) is decreased in arterial blood.
Hypoxia is reduced oxygen in the body organs and tissues.

Oxygenation failure
It may develop when severe hypoxemia (PaO2 , 40 mm Hg) does not respond to a moderate to high level (50% to 100%) of supplemental oxygen.
The important clinical signs of oxygenation failure and hypoxia include hypoxemia,dyspnea, tachypnea, tachycardia, and cyanosis.

CLINICAL CONDITIONS LEADING TOMECHANCIAL VENTILATION
Mechanical ventilation is often used to support ventilatory or oxygenation failure.
Failure to ventilate or oxygenate adequately may be caused by pulmonary or nonpulmonary conditions.
They are separated into three distinct groups: (1) depressed respiratory drive (e.g.,drug overdose)(2) excessive ventilatory workload (e.g., airflow
obstruction),(3) failure of ventilatory pump (e.g., chest trauma)

Depressed or insufficient respiratory drive may lead to ventilatory and oxygenation failure.
Excessive ventilatory workload may lead to muscle fatigue and ventilatory/oxygenation failure.
Failure of the ventilatory pump may lead to an increased work of breathing and to eventual ventilatory and oxygenation failure





THANK YOU