
Orthopaedic Research Unit Dept. of Orthopaedic Surgery and Traumatology
Upload
jessica-nelsonCategory
view
228download
6
Principles of Fracture Healing
Faik Altıntas M.D.
Orthopaedic and Traumatology
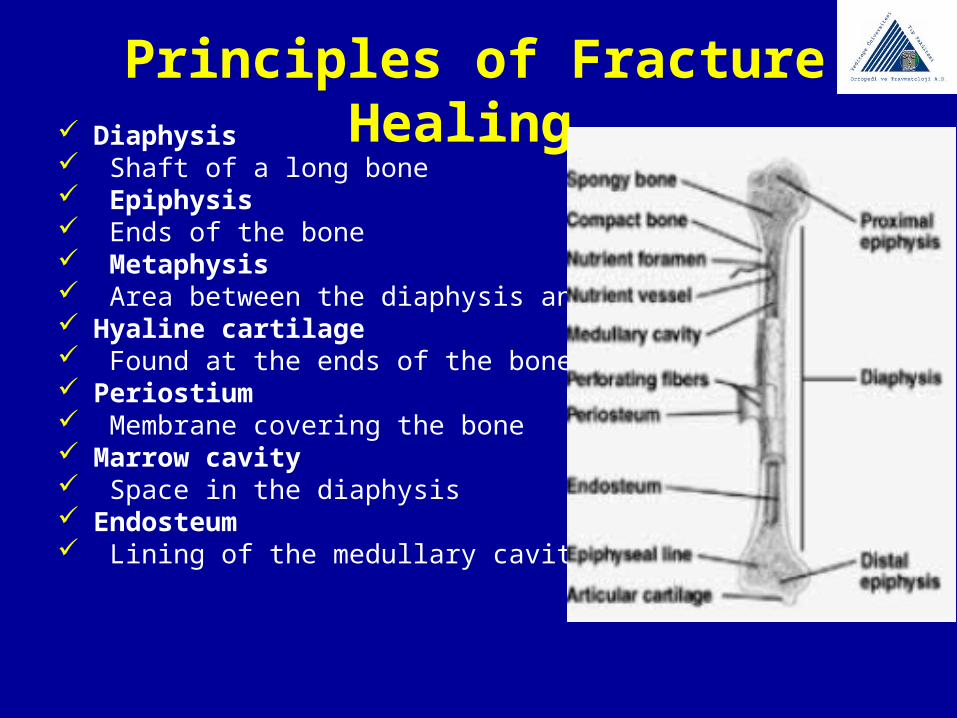
Principles of Fracture Healing Diaphysis Shaft of a long bone Epiphysis Ends of the bone Metaphysis Area between the diaphysis and epiphyses Hyaline cartilage Found at the ends of the bone Periostium Membrane covering the bone Marrow cavity Space in the diaphysis Endosteum Lining of the medullary cavity
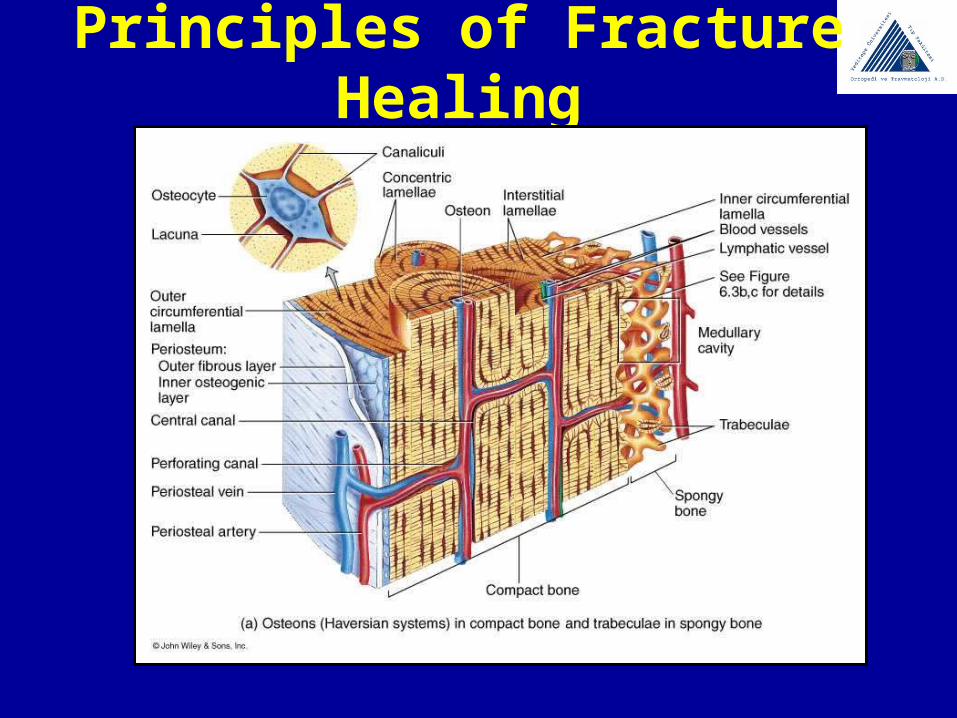
Principles of Fracture Healing
Principles of Fracture Healing
Bone ConsistsOrganic component (%40)
CollagenProteoglicansMatrix proteins
İnorganic component (%60)Calsiyum hidroksiapatite [Ca10(PO4)6(OH)2]
Osteocalsiyun Phosfate
Principles of Fracture Healing
Types of Fracture Healing1. Primary Healing
2. Secondary Healing
3. Distraction Osteogenesis
Principles of Fracture Healing
Primary fracture healing Involves direct attempt by the cortex to
reestablish itself Occurs only with anatomic reduction & rigid
fixation Gaps in reduction heal by vessel ingrowth-
mesenchymal cells- osteoblasts-osteoclast cutting cones
Direct contact areas heal by cutting cones allowing passage of vessels
Principles of Fracture Healing
Secondary fracture healing Response of periosteum/ external soft tissues Recapitulation of embryonic intramembranous
ossification and endochondral bone formation Intramembraneous= peripheral to fracture Endochondral= adjacent to fracture Motion enhances periosteal response External soft tissue forms bridging calus
(endochondral)
Principles of Fracture Healing
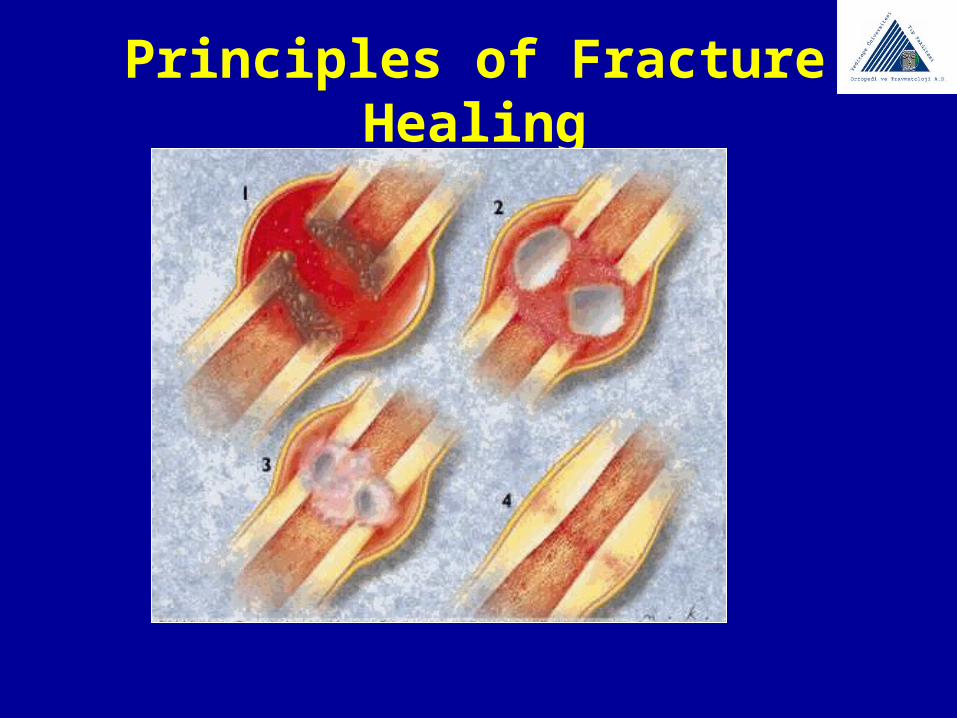
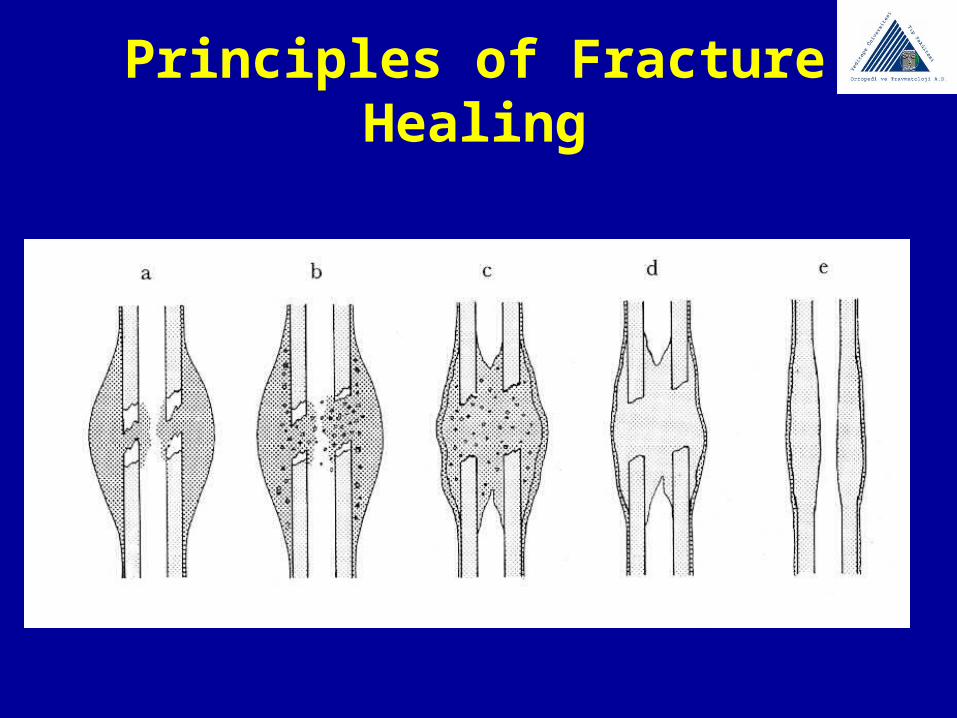
Stages of Healing Hematoma Formation 1-2 Days Inflammation 2-7 Days Soft Callus Formation 1-3 Weeks Hard Callus Formation 3-6 Weeks Remodelling Phase >8. Weeks
Principles of Fracture Healing
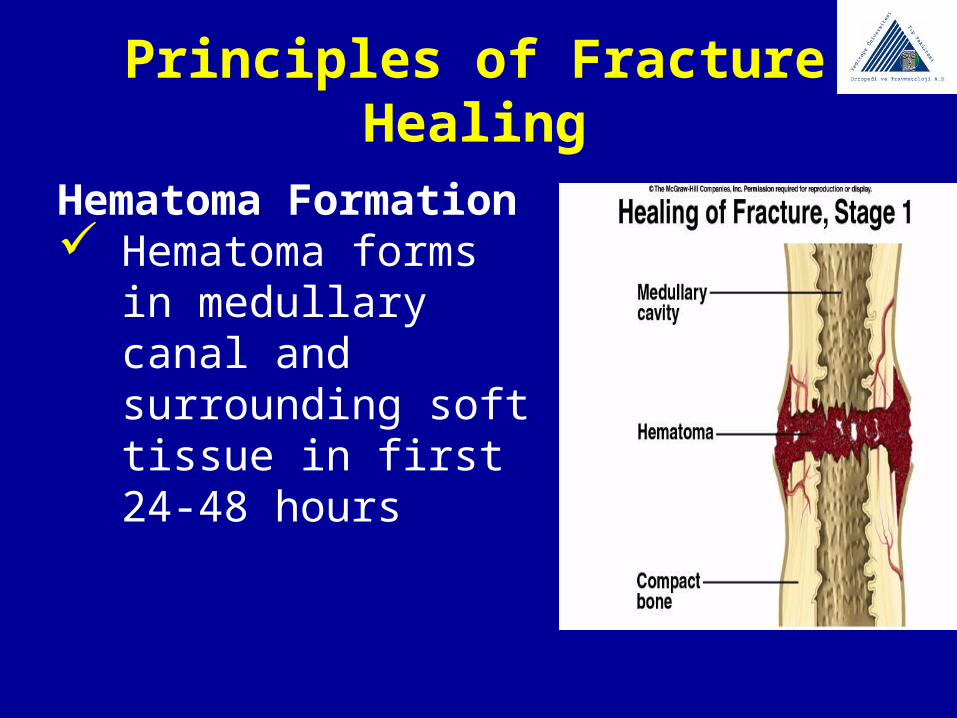
Hematoma Formation Hematoma forms in
medullary canal and surrounding soft tissue in first 24-48 hours
Principles of Fracture HealingInflammation Hematoma in fracture site brings hematopoietic cells
secreting growth factor Growth factors
Insulin-like growth factor (IGF-1) Transforming growth factor (TGF) Vascular endothelial growth factor (VEGF) Fibroblast growth factor (FGF)
Fibroblasts, osteoprogenitor cells produce granulation tissue around fracture ends
Osteoblasts proliferate By 1st-2nd week, abundant cartilage over fracture site
ready for calcification (occurs identical to growth plate)
Principles of Fracture Healing
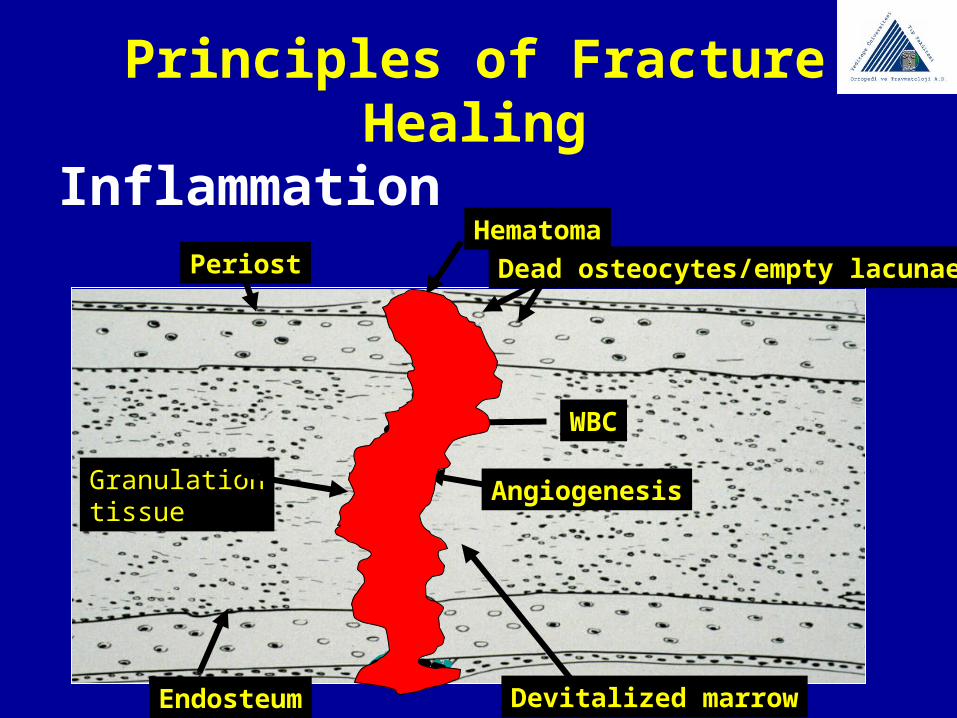
InflammationPeriost
Devitalized marrowEndosteum
Hematoma
Dead osteocytes/empty lacunae
WBC
AngiogenesisGranulationtissue
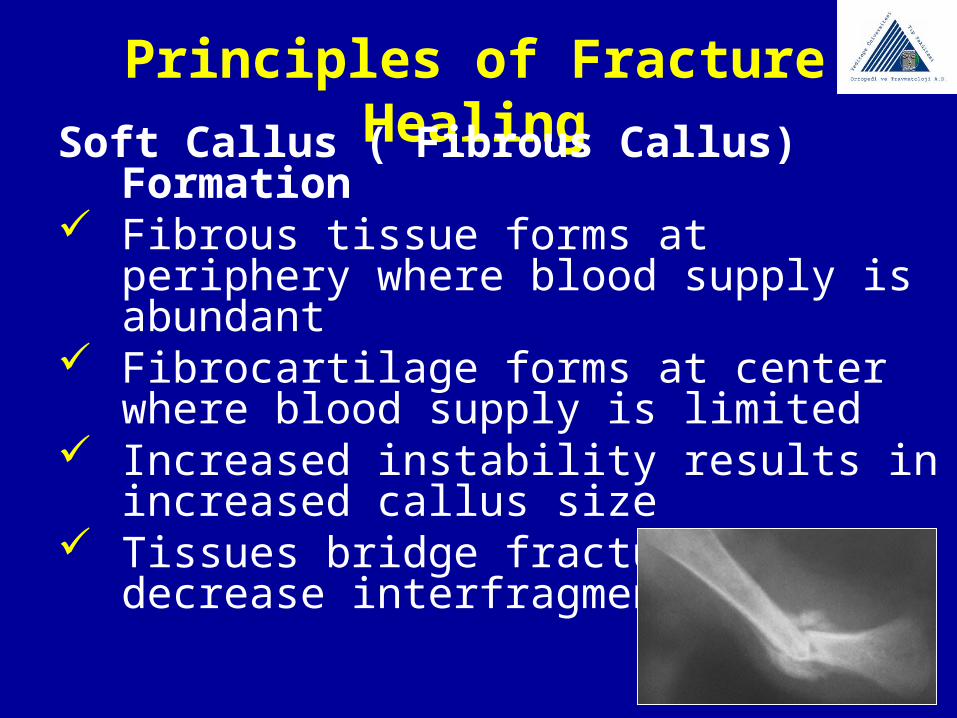
Principles of Fracture HealingSoft Callus ( Fibrous Callus) Formation Fibrous tissue forms at periphery where blood
supply is abundant Fibrocartilage forms at center where blood
supply is limited Increased instability results in increased callus
size Tissues bridge fracture and decrease
interfragmentary strain
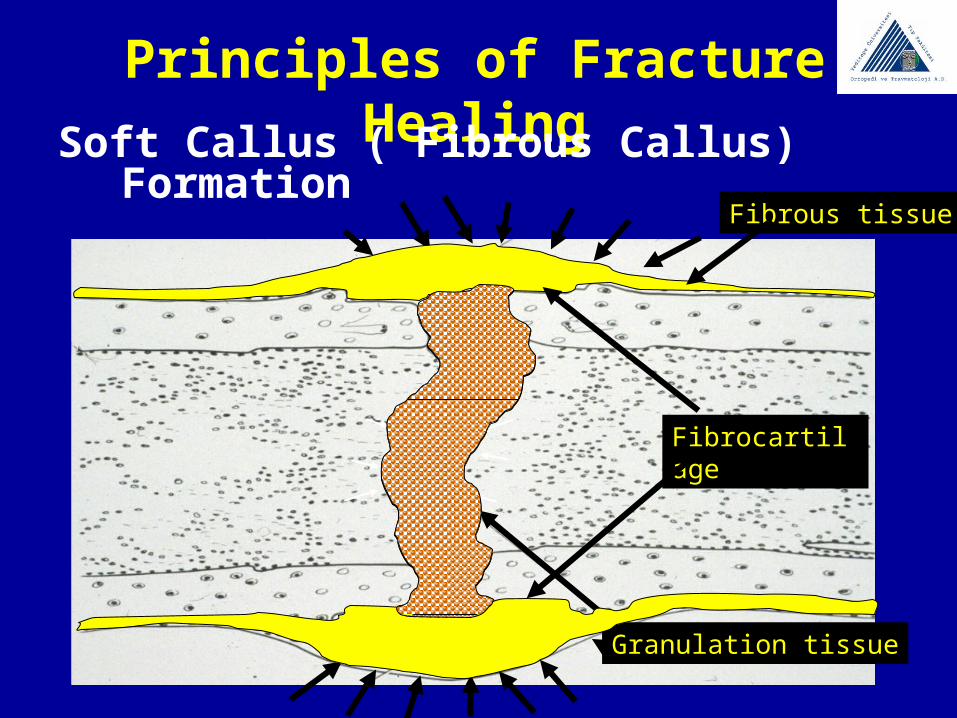
Principles of Fracture HealingSoft Callus ( Fibrous Callus) Formation
Granulation tissue
Fibrous tissue
Fibrocartilage
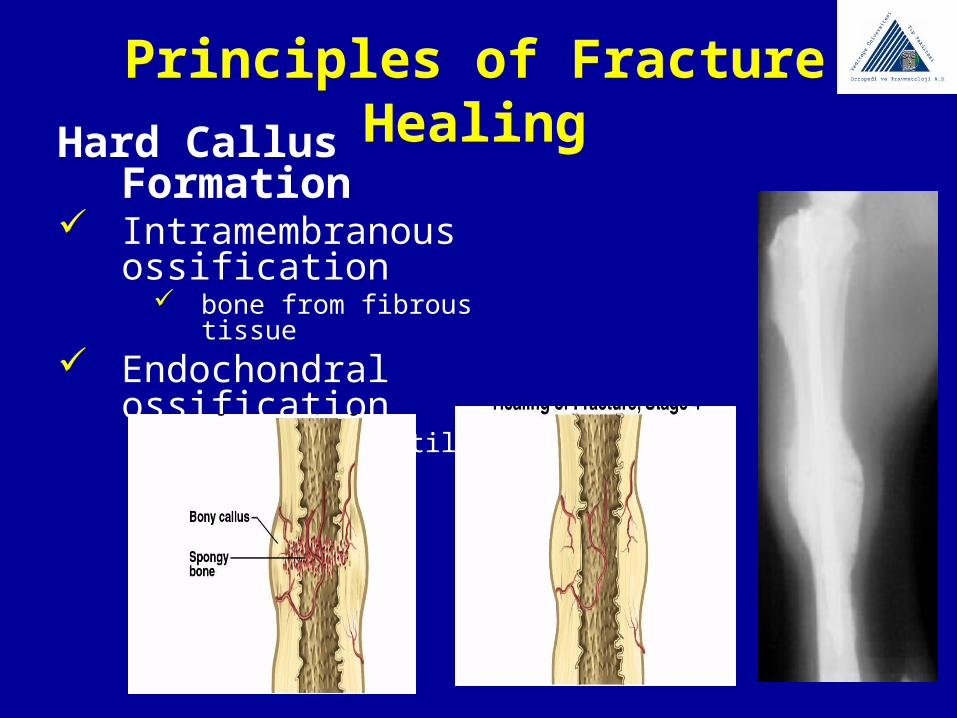
Principles of Fracture HealingHard Callus Formation Intramembranous
ossification bone from fibrous tissue
Endochondral ossification bone from cartilage
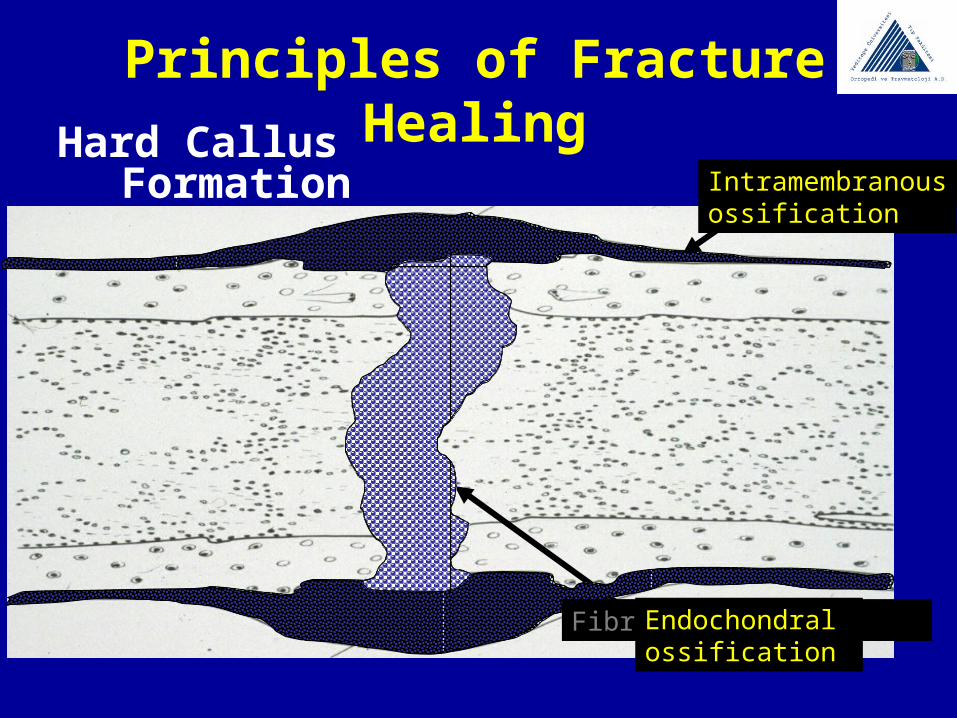
Principles of Fracture HealingHard Callus Formation
Fibrous tissueIntramembranousossification
Fibrocartilage Endochondralossification
Principles of Fracture Healing
Remodelling Phase Begins in middle of repair phase, continues until fx
clinically healed Osteoclastic tunneling (cutting cones) in concert
with osteoblast deposition Can continue up to 7 years Remodeling based on stresses (Wolff’s law)
Bone formed in response to mechanical load
Principles of Fracture Healing
Principles of Fracture Healing

Principles of Fracture Healing
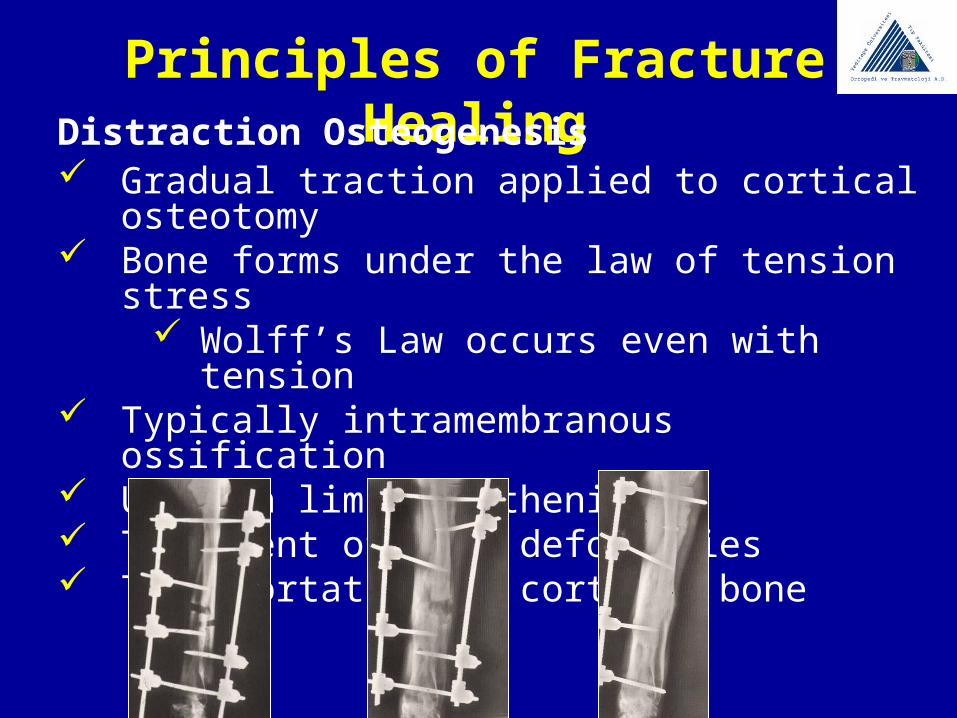
Principles of Fracture HealingDistraction Osteogenesis Gradual traction applied to cortical osteotomy Bone forms under the law of tension stress
Wolff’s Law occurs even with tension Typically intramembranous ossification Used in limb lengthening Treatment of limb deformities Transportation of cortical bone
Principles of Fracture Healing
Conditions that interfere with fracture healingHigh energy traumas brings soft tissue problems that lead
non uniounPoor blood supply to the fractured area; could lead to
avascular or aseptic necrosis Poor immobilization of fracture site may cause
misalignment, nonunion or deformity Infection – more common with open fractures Cortisone= negative effect, decreased callus formation






![[Forensics] traumatology 2.ppt](https://static.fdocuments.in/doc/165x107/55ce4f98bb61eb46528b47b2/forensics-traumatology-2ppt.jpg)
![[Forensics] traumatology 1](https://static.fdocuments.in/doc/165x107/55c475bdbb61ebbc228b45ab/forensics-traumatology-1.jpg)











