Anticholinergics PS postganglionic Ganglionic & Neuromuscular blocking agents.
Upload
antonio-basileCategory
view
212download
0
Eur Radiol (2006) 16: 422–427DOI 10.1007/s00330-005-2680-6 GASTROINTESTINAL
Antonio BasileJoachim KettenbackElena MundoAngelo NatoliSimona CaloggeroMarina MinciulloAntonella Garito
Received: 19 April 2004Revised: 28 August 2004Accepted: 13 January 2005Published online: 22 February 2005# Springer-Verlag 2005
Primitive mesenteric gastrointestinal stromaltumor with autonomic nerve/ganglionicdifferentiation presenting as a huge masswith small synchronous nodules
Abstract We present a case of aprimary mesenteric ectopic gastroin-testinal stromal tumor. The pathologic
characteristics of this neoplasm, au-tonomic nerve/ganglionic differentia-tion and presentation as a huge masswith small synchronous nodules, havenot been previously described in theliterature.
Keywords Gastrointestinal stromaltumor . Mesentery neoplasms .
Computed tomography
Introduction
The term gastrointestinal stromal tumor (GIST) was firstused in 1983 by Mazur and Clark [1]; however, thediscovery in 1998 by Hirota et al. [2] that GISTs can containmutations in the c-kit gene marked the beginning of a newunderstanding and reclassification of sarcomas of the gas-trointestinal tract. GIST defines a heterogeneous subgroupof gastrointestinal mesenchymal neoplasms, histologicallyand genetically different from soft-tissue sarcoma, includ-ing tumors of smooth-muscle origin (most commonlyleiomyosarcoma, and also leiomyoma or leiomyoblastoma)and of neural-crest origin (e.g., schwannoma, or nerve-sheath tumor). However, GISTs do not originate fromsmooth muscle, but rather arise either from stem cells thatdifferentiate towards interstitial cells of Cajal or directlyfrom interstitial cells of Cajal. The interstitial cells of Cajalstimulate the movement (contractions) of the gastrointes-tinal tract. About 40–70% of GISTs arise from the stomach,the small intestine, and from the colon and rectum [3, 4].Rarely GISTs can also be found in the esophagus, omentum,
mesentery, or retroperitoneum [4] and in these cases theyare called extragastrointestinal stromal tumors (EGISTs)[5]. GISTs often spread from the primary site to distant lo-cations such as liver or peritoneum. Metastases to the lymphnodes and lungs are rare, but do occur [3, 4]. Computedtomography (CT) examination represents the gold standardin the diagnosis of EGISTs of omentum or mesentery [6]; inCT images they have the same characteristics as GISTs[7]: a well-circumscribed large mass, with a median size of16.5 cm [8], containing areas of low attenuation corre-sponding to hemorrhage or necrosis [6]. In this case studywe present a case of a mesenteric EGIST presenting as ahuge mesenteric mass with multiple mesenteric and omen-tal nodules with the same pathologic characteristics.
Case report
A 52-year-old male, was admitted presenting abdominalpain, and with a palpable abdominal mass. He reported theonset of symptomatology 15 days before the admission. An
A. Basile . E. MundoDepartment of Radiology,Ospedale Ferrarotto,Catania, Italy
A. Basile . A. Natoli . S. Caloggero .M. Minciullo . A. GaritoDepartment of Radiology,Ospedale Barone I. Romeo,Patti, Messina, Italy
J. KettenbackDepartment of Angiography andInterventional Radiology,University Clinic,Vienna, Austria
A. Basile (*)Via Papa Giovanni XXIII, 166,98051 Barcellona P.G., Messina, Italye-mail: [email protected].: +39-9-9762324

ultrasound examination disclosed a large mass (transversediameter of about 16 cm) that had soft-tissue echogenitywith internal hypoechogenic areas (Fig. 1). Laboratoryfindings of tumor markers were normal. Subsequently, thepatient underwent contrast-enhanced CT (Secura; Philips,pitch 1.5; collimation 5 mm, reconstruction index 3 mm) ofabdomen and pelvis. Image acquisition was started 60 and180 s following injection of 120 ml nonionic iodinatedcontrast material (320 mg/ml) in the left antecubital fossa
(flow rate, 3 ml/s). From CT, a smooth-shaped heteroge-neous pelvic mass with maximum dimension of 18 cm wasseen (Fig. 2); no lesions were discovered in the liver. De-termining the site of origin was difficult since the massdisplaced pelvic structures and compressed both ureters.Small nodular mesenteric lesions ranging from 0.5 to2.5 cm in diameter were also seen close to the main mass,and were thought to be lymph node metastasis (Figs. 3, 4).Surgeons asked us to perform a selective transfemoralarteriography of both the superior and the inferior mesen-teric arteries (SMA and IMA), with the aim of targeting therelationship between the mass and the vessels, and to checkfor the possibility to preoperatively embolize the vascularsupply of the tumor, reducing the potential risk of intraop-erative bleeding. Although the neoplasm was fed massivelyby both arteries, targeting of vessels feeding exclusively thetumor was difficult (Fig. 5). Thus, owing to the high risk ofintestinal infarction, we decided not to perform a trans-catheter embolization.
On surgical exploration, a mass (18×14×12 cm) arisingfrom the jejunal mesentery was disclosed; laparotomy alsoshowed four small nodules in the mesentery and omentumranging in size from 0.5 to 3 cm. Despite major bleedingduring surgery, the tumor was resected from the adheredsigmoid and other small bowel segments that did not pres-
Fig. 1 Ultrasound examination shows a heterogeneous mass in theright iliac fussa.
Fig. 2 Unenhanced (a) and enhanced after 60-in. (b) and 180-in. (c) computed tomography (CT) examination revealed a heterogeneoushuge pelvic mass, with areas of hypodensity probably due to necrosis.
Fig. 3 Small omental nodule of about 1 cm (arrow) with low attenuation in all the phases of CT examination: a precontrast, b venous phase,c equilibrium phase
423
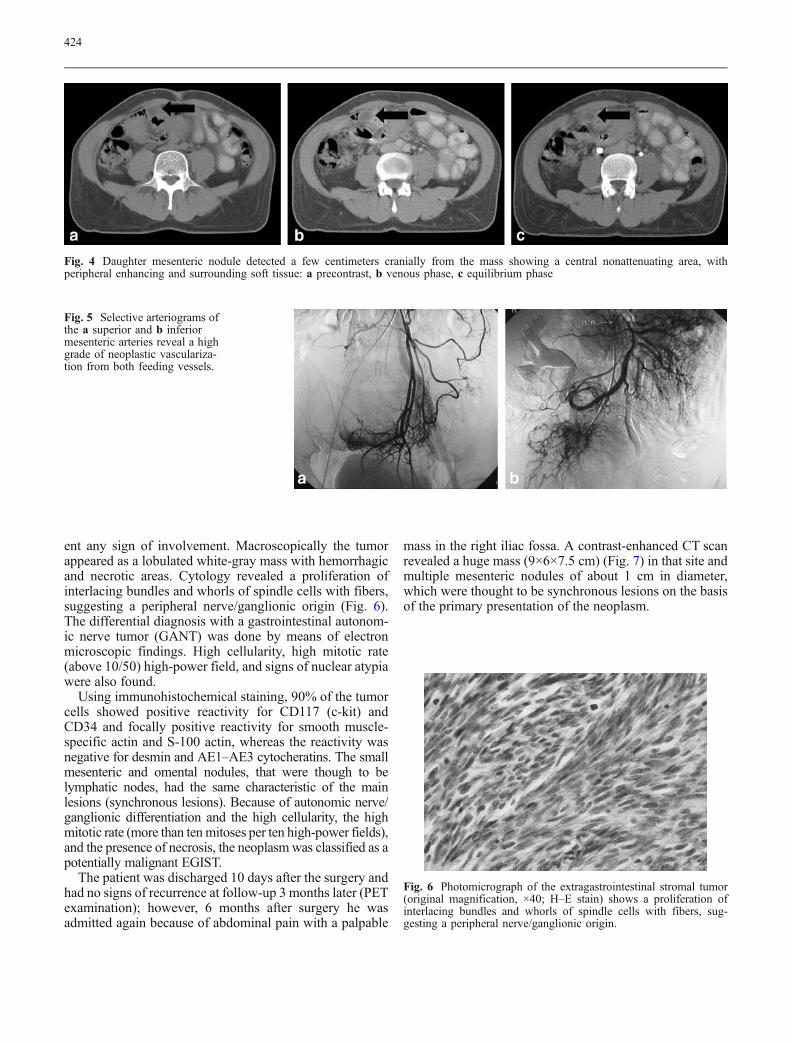
ent any sign of involvement. Macroscopically the tumorappeared as a lobulated white-gray mass with hemorrhagicand necrotic areas. Cytology revealed a proliferation ofinterlacing bundles and whorls of spindle cells with fibers,suggesting a peripheral nerve/ganglionic origin (Fig. 6).The differential diagnosis with a gastrointestinal autonom-ic nerve tumor (GANT) was done by means of electronmicroscopic findings. High cellularity, high mitotic rate(above 10/50) high-power field, and signs of nuclear atypiawere also found.
Using immunohistochemical staining, 90% of the tumorcells showed positive reactivity for CD117 (c-kit) andCD34 and focally positive reactivity for smooth muscle-specific actin and S-100 actin, whereas the reactivity wasnegative for desmin and AE1–AE3 cytocheratins. The smallmesenteric and omental nodules, that were though to belymphatic nodes, had the same characteristic of the mainlesions (synchronous lesions). Because of autonomic nerve/ganglionic differentiation and the high cellularity, the highmitotic rate (more than tenmitoses per ten high-power fields),and the presence of necrosis, the neoplasmwas classified as apotentially malignant EGIST.
The patient was discharged 10 days after the surgery andhad no signs of recurrence at follow-up 3 months later (PETexamination); however, 6 months after surgery he wasadmitted again because of abdominal pain with a palpable
mass in the right iliac fossa. A contrast-enhanced CT scanrevealed a huge mass (9×6×7.5 cm) (Fig. 7) in that site andmultiple mesenteric nodules of about 1 cm in diameter,which were thought to be synchronous lesions on the basisof the primary presentation of the neoplasm.
Fig. 4 Daughter mesenteric nodule detected a few centimeters cranially from the mass showing a central nonattenuating area, withperipheral enhancing and surrounding soft tissue: a precontrast, b venous phase, c equilibrium phase
Fig. 5 Selective arteriograms ofthe a superior and b inferiormesenteric arteries reveal a highgrade of neoplastic vasculariza-tion from both feeding vessels.
Fig. 6 Photomicrograph of the extragastrointestinal stromal tumor(original magnification, ×40; H–E stain) shows a proliferation ofinterlacing bundles and whorls of spindle cells with fibers, sug-gesting a peripheral nerve/ganglionic origin.
424

The patient underwent a second laparotomy, whichrevealed the same macroscopic and microscopic character-istics of the primitive mass. After this intervention the pa-tient was treated with imatinib mesylate (Gleevec/Glivec,Novartis Pharma, Basel, Switzerland) and after an 11-month follow-up is doing well.
Discussion
GISTs often grow quite large before they are discovered andprimary tumors often produce few symptoms. Thus, GISTsare often discovered during emergency surgery for unex-pected perforation of the gastrointestinal tract and conse-quent bleeding. Metastatic tumors however can be quitenumerous and factors for a high risk of recurrence includerupture of the tumor either prior to or during surgery orfailure to obtain clear margins during surgery. GISTs are themost common mesenchymal tumors of the gastrointestinaltract. On the basis of the most accepted classification re-ported by Suster in 1996 [9], GISTs may have complete orincomplete myoid, neural, autonomic nerve/ganglionic, ormixed myoid/neural differentiation, or may show nodifferentiation [9, 10].
The expression of CD117 (c-kit gene product; in 94% ofcases) and less specifically of CD34 constitutes the basis ofthis differentiation [11]. The gene CD117 is also expressedby interstitial cells of Cajal, and on the basis of this severalauthors proposed the origin of GISTs from these cells [12,13]. Investigators have also characterized the mutationsseen in the c-kit protooncogene and found an associationbetween the presence of c-kit mutation and prognosis inhuman GISTs [2, 14]. Others authors, despite historicallythe most reproducible predictor of malignancy being themitotic rate, consider the tumor dimension directly relatedto the malignancy, and classify as benign tumors smallerthan 6 cm and as malign tumors larger than 6 cm [15];however, metastases from tumors smaller than 5 cm havebeen reported [16, 17].
Currently it is most prudent to classify GISTs on the basisof risk assessment, rather than to try to classify them asbenign or malignant, since almost all GISTs should be con-sidered as having some malignant potential. Thus, althoughmany factors have been suggested to contribute to malig-
nant potential, the two most commonly quoted factors aresize and mitotic activity as stated by the GastrointestinalStromal Tumor Workshop [18].
Patients with tumors with a spindle cell histology (n=32)had longer recurrence-free survival times than patients withepithelioid cell tumors (n=3), and patients with a mixedspindle/epithelioid (n=13) cell type had the lowest recur-rence-free survival times. Tumors with parameters fallingbetween low risk and high risk were classified as interme-diate-risk tumors (according to grade).
GISTs could be totally asymptomatic or lead to symp-toms related to the size and anatomic location. In addition,size may vary somewhat between prefixation and postfixa-tion and between observers. The most common symptomsof GISTs are vague abdominal discomfort or pain, thepresence of a palpable abdominal mass, a feeling of ab-dominal fullness, and secondary symptoms resulting fromtumor bleeding and associated anemia [4, 11]. Othersreported weight loss, abdominal distension, and intestinalobstruction [9]. About 40–70% of GISTs arise from thestomach, 20–40% arise from the small intestine, and 5–15%from the colon and rectum. GISTs can also be found in theesophagus (fewer than 5%), omentum (fewer than 5%), themesentery, or the retroperitoneum [3, 4, 20]. Rare locationsof GISTs at the omentum or mesentery were also calledEGISTs [5, 8, 19, 20]. So far, only a few cases of primarydistinct mesenteric location of tumors showing histologicfeatures similar to GISTs have been reported in the liter-ature [8, 19, 20], apart from other studies that do not make asure selection between mesenteric and omental neaoplasms[6]. Ten of the mesenteric tumors are reported in a study ofMiettinen et al. [8]; one is collected in a large series of studiesof Levy et al. [19]; one is in a recent single case report ofGorospe et al. [20]; and one is in a recent series of Kim et al.[6]. In all these cases, the median size of the primary mes-enteric tumors was more than 10 cm; this is probably due tothe fact that small EGISTs are rarely encountered becausethey seldom produce symptoms leading to detection.
In a recent study a group of 48 patients with mesentericand omental gastrointestinal tumors (EGIST) was analyzedwithout differentiation of the two origins [6]. In this study,the parameters affecting the prognosis of EGISTs in com-parison with normal GISTs were evaluated. Parameterssuch as cellularity, mitotic activity, and necrosis were sig-
Fig. 7 Follow up after 6 monthswith a unenhanced and b en-hanced CT examination dis-covers a recurrent mass in theright iliac fossa with the samecharacteristics as the primitivemass.
425

nificantly associated with an adverse outcome in a uni-variate analysis, whereas nuclear atypia, growth pattern,and size were not. Grouping patients in terms of the numberof potential risk factors (zero or one of cellularity, mitoticactivity, or necrosis versus two or three of these factors) washighly discriminatory as a diagnostic indicator of the likelyincidence of an adverse event [6].
Macroscopically, GISTs appear as a complex mass withgrossly hemorrhagic, necrotic, or cystic cavities. CT andmagnetic resonance are the imaging methods of choice fordetection of mesenteric neoplasms [7, 19, 21, 22]. In CTimages, mesenteric GISTs appear as soft-tissue masses witha variable amount of hypodense area owing to haemor-rhage, necrosis, or cystic zones; post-contrast homogeneousenhancement at the solid component of viable tumors iscommonly seen [3, 19]. In MRI, the degree of necrosis andhaemorrhage affects substantially the signal intensity pat-tern. Commonly, the solid portion of the mesenteric GISTshas a typically low signal intensity on T1-weighted images,with good enhancement after administration of gadolinium;depending on the age of the bleeding hemorrhagic areas, avariable from high to low signal intensity in both T1- andT2-weighted images could be seen in the haemorrhagicareas [23]. However, the imaging features of mesentericGISTs are unspecific and do not differ from other sarcomassuch as leiomyosarcoma, malignant fibrous histiocytoma,fibrosarcoma, and liposarcoma arising in this location [19].
Other possible differential diagnoses at the same site aredesmoid tumors, which commonly present homogeneousattenuation on CT images, and cystic masses such as entericcysts and lymphangioma [24].
On the basis of such unspecific characteristics, thediagnosis of EGISTs is commonly done on a surgical spec-imen owing to the fact that because of their size the tumorsalmost always deserve surgical removal; there are no data inthe literature on the use of preoperative biopsy. In a recentreview article [6], in a series of eight patients only onepatient had only open biopsy, and seven underwent surgicalremoval. The authors also assumed that an important andperhaps unique CTsign militating against the diagnosis of a
mesenteric or an omental EGIST is the presence of cavi-tation and the gas content; this is because EGISTs are not incontact with the gastrointestinal lumen, and then they can-not discharge the necrotic content into the bowel [6].
In our case, as part of standard diagnostic tools, weperformed an arteriography that was requested by the sur-gical team. The aim was either to delineate the vascularityof the tumor or to check for the possibility to perform apreoperative embolization, thus reducing the risk of intra-operative bleeding. Furthermore, achieving a devascular-ization of the tumor, we could prevent the risk of recurrenceor metastasis related to rupture of a GIST either prior to orduring surgery or failure to obtain clear margins duringsurgery, as previously mentioned. However the mass wassupplied by a large number of vessels arising either fromSMA or IMA, and we thought it was too risky to carry outa target and safe embolization. The vascularization ofEGISTs is commonly high, even if the enhancement patternafter contrast medium administration is variable [6]. Thereare no literature data confirming a high risk of intraoperativebleeding for EGISTs; however, there is no study comparingthe rate of intraoperative blood loss between embolized andnot embolized EGISTs.
In our case, the neoplasm was diagnosed as an EGISTbecause of the immunohistochemical analysis revealingpositive reactivity for CD117 (c-kit) and CD34; the exam-ination also demonstrated focally positive reactivity forsmooth muscle-specific actin and S-100 actin, whereas thereactivity was negative for desmin and AE1–AE3 cito-cheratins. Electron microscopy excluded the diagnosis of aGANT, which is considered a distinct subcategory of a GIST[25]. After the second intervention, the patient was treatedwith imatinib mesylate, a new oral targeted chemotherapyagent which has been successfully proven in the manage-ment of GISTs [26, 27].
To our knowledge, this is the first case of a mesentericEGIST with autonomic nerve/ganglionic differentiation,presenting as a huge mass with multiple synchronous nod-ules; GISTs commonly present spreading to the mesentery,however this has not been yet reported in a primary EGIST.
References
1. Mazur MT, Clark HB (1983) Gastricstromal tumors. Reappraisal of histo-genesis. Am J Surg Pathol 7(6):507–519
2. Hirota S, Isozaki K, Moriyama Y,Hashimoto K, Nishida T, Ishiguro S,Kawano K, Hanada M, Kurata A,Takeda M, Muhammad TG, MatsuzawaY, Kanakura Y, Shinomara Y, KitamuraY (1998) Gain-of-function mutations ofc-kit in human gastrointestinal stromaltumors. Science 279:577–580
3. Sharp RM, Ansel HJ, Keel SB (2001)Best cases from the AFIP: gastrointes-tinal stromal tumor. Radiographics21:1557–1560
4. Miettinen M, Lasota J (2001) Gastroin-testinal stromal tumors: definition, clini-cal, histological, immuno-histochemical,and molecular genetic features and dif-ferential diagnosis. Virchows Arch438:1–12
426

5. Reith JD, Goldblum JR, Lyles RH,Weiss SW (2000) Extragastrointestinal(soft tissue) stromal tumors: an analysisof 48 cases with emphasis on histologicpredictors of outcome. Mod Path 13(5):577–585
6. Kim HC, Lee JM, Kim SH, Kim KW,LeeW, KimYJ, Han JK, Choj BI (2004)Primary gastrointestinal stromal tumorsin the omentum and mesentery: CTfindings and pathologic correlations.Am J Roentgenol 182:1463–1467
7. Ghanem N, Altehoefer C, FurtwänglerA, Winterer J, Schäfer O, Springer O,Kotter E, Langer M (2003) Computedtomography in gastrointestinal stromaltumors. Eur Radiol 13:1669–1678
8. Miettinen M, Monihan JM, Sarlomo-Rikala M, Kovatich AJ, Carr Emory TS,Sobin LH (1999) Gastrointestinal stro-mal tumors/smooth muscle tumors(GISTs) primary in the omentum andmesentery: clinicopathologic and im-muno-histochemical study of 26 cases.Am J Surg Pathol 23:1109–1118
9. Suster S (1996) Gastrointestinal stromaltumors. Sem Diagn Pathol 13:297–313
10. Morgan BK, Compton C, Talbert M,Gallagher WJ, Wood WJC (1990) Be-nign smooth muscle tumors of the gas-trointestinal tract. Ann Surg 211:63–66
11. Pidhorecky I, Cheney RT, KraybillWG, Gibbs JF (2000) Gastrointestinalstromal tumors: current diagnosis, bio-logic behavior, and management. AnnSurg Oncol 7:705–712
12. Kindblom LG, Remotti HE, AldenbergF, Meis-Kindblom JM (1998) Gastro-intestinal pacemaker cell tumor (GI-PACT). Gastrointestinal stromal tumorsshow phenotypic characteristics of theinterstitial cell of Cajal. Am J Pathol152:1259–1269
13. Sincar K, Hewlett BR, Riddel RH(1998) Most gastrointestinal stromaltumors arise from interstitial cells ofCajal. Mod Pathol 11:71A
14. Moskaluk CA, Tian Q, Marshall CR,Rumpel CA, Franquemont DW,Frierson HF (1999) Mutations of c-kitJM domain are found in a minority ofhuman gastrointestinal stromal tumors.Oncogene 18:1897–1902
15. Appelman HD, Helwig EB (1977)Sarcomas of the stomach. Am J ClinPathol 67:2–10
16. Evans HL (1985) Smooth muscle tu-mors of the gastrointestinal tract: astudy of 56 cases for a minimum of 10years. Cancer 56:2242–2250
17. Ballarini C, Intra M, Ceretti AP,Prestipino F, Bianchi FM, Sparacio F,Berti E, Perrone S, Silva F (1998)Gastrointestinal stromal tumors: a “be-nign” tumor with hepatic metastasisafter 11 years. Tumori 84:78–81
18. Berman JJ, O’Leary TJ (2001) Gastro-intestinal stromal tumor workshop.Human Pathol 32:578–582
19. Levy AD, Remotti HE, ThompsonWM, Sobin LH, Miettinen M (2003)Gastrointestinal stromal tumors: radio-logic features with pathologic correla-tion. Radiographics 23:283–304
20. Gorospe L, Simon MJ, Lima F, EstebanI, Madrid C, Hitos E (2002) Primarymesenteric tumor with phenotypicalfeatures of gastrointestinal stromal tu-mors. Eur Radiol 12:S82–S85
21. Healy JC, Reznek RH (1998) Theperitoneum, mesenteries and omenta:normal anatomy and pathologic pro-cesses. Eur Radiol 8(6):886–900
22. Coakley FV, Hricak H (1999) Imagingof peritoneal and mesenteric disease:key concepts for the clinical radiologist.Clin Radiol 54:563–574
23. Hasegawa S, Semelka RC, Noone TC,Woosley JT, Marcos HB, Kenney PJ,Siegelman ES (1998) Gastric stromalsarcomas: correlation of MR imagingand histopathologic findings in ninepatients. Radiology 208:591–595
24. Stoupis C, Ros PR, Abbitt PL, BurtonSS, Gauger J (1994) Bubbles in thebelly: imaging of cystic mesenteric andomental masses. Radiographics14:729–737
25. Herrera GA, Pinto de Moraes HP,Grizzle WE, Han SG (1984) Malignantsmall bowel neoplasm of enteric plexusderivation (plexosarcoma): light andelectron microscopy study confirmingthe origin of the neoplasm. Dig Dis Sci29:275–284
26. Demetri GD, von Mehren M, BlankeCD, Van den Abbeele AD, EisenbergB, Roberts PJ, Heinrich MC, TuvesonDA, Singer S, Janicek M, Fletcher JA,Silverman SG, Silberman SL,Capdeville R, Kiese B, Peng B,Dimitrijevic S, Druker BJ, Corless C,Fletcher CDM, Joensuu H (2002)Efficacy and safety of imatinibmesylate in advanced gastrointestinalstromal tumors. N Engl J Med347:472–480
27. van Oosterom AT, Judson I, Verweij J,Stroobants S, Donato di Paola E,Dimitrijevic S, Martens M, Webb A,Sciot R, Van Glabbeke M, Silberman S,Nielsen OS (2001) Safety and efficacyof imatinib (STI571) in metastatic gas-trointestinal stromal tumours: a phase Istudy. Lancet 358:1421–1423
427