
Priming Tissue-specific Cellular Immunity in a Phase I...
9
Advanves in Brief Priming Tissue-specific Cellular Immunity in a Phase I Trial of Autologous Dendritic Cells for Prostate Cancer 1 Patrick A. Burch, Jami K. Breen, Jan C. Buckner, Dennis A. Gastineau, Judith A. Kaur, Reiner L. Laus, Douglas J. Padley, Madhusudan V. Peshwa, Henry C. Pitot, Ronald L. Richardson, Bouwien J. Smits, Pitsata Sopapan, George Strang, Frank H. Valone, and Stanimir Vuk-Pavlovic ´ 2 Divisions of Medical Oncology [P. A. B., J. C. B., J. A. K., H. C. P., R. L. R.], Transfusion Medicine [D. A. G., D. J. P.], and Stem Cell Laboratory [S. V-P.], Mayo Clinic and Mayo Foundation, Rochester, Minnesota 55905, and Dendreon Corporation, Seattle, Washington 98121 [R. L. L., M. V. P., B. J. S., P. S., G. S., F. H. V.] Abstract We attempted to induce therapeutic immunity against prostate-derived tissues in patients suffering from progres- sive hormone-refractory metastatic prostate carcinoma. Thirteen patients were treated with two infusions, 1 month apart, of autologous dendritic cells (APC8015) preexposed ex vivo to PA2024, a fusion protein consisting of human granulocyte/macrophage-colony stimulating factor (GM- CSF) and human prostatic acid phosphatase (PAP). The infusions were followed by three s.c. monthly doses of PA2024 without cells. Three groups of patients each received PA2024 at 0.3, 0.6, or 1.0 mg/injection. All Ps were two- sided. Treatment was well tolerated. After infusions of APC8015, patients experienced only mild (grade 1–2) short- lived fever and/or chills, myalgia, pain, and fatigue. One patient developed grade 3 fatigue. Four patients developed mild local reactions to s.c. PA2024. Twelve patients were evaluable for response to treatment. Circulating prostate- specific antigen levels dropped in three patients. T cells, drawn from patients after infusions of APC8015, but not before, could be stimulated in vitro by GM-CSF (P 5 0.0004) and PAP (P 5 0.0001), demonstrating broken immune tol- erance against these two normal proteins. Injections of PA2024 did not influence the reactivity of T cells against PAP and GM-CSF. However, antibodies to GM-CSF and, to a much lesser extent, to PAP reached maximum titers only after two or even three injections of PA2024, showing that directly injected PA2024 was involved in stimulation of humoral immunity. Dendritic cells exposed to antigen ex vivo can induce antigen-specific cellular immunity in pros- tate cancer patients, warranting further studies of this mode of immunotherapy. Introduction Adenocarcinoma of the prostate is the most common ma- lignancy in American men and the second most frequent cause of their death from cancer; nearly 40,000 men are projected to die from this disease in 1999 (1). For patients with advanced disease, standard care includes hormone ablation by bilateral orchiectomy or by agonists of luteinizing hormone-releasing hormone, with or without antiandrogens (2). Initially, most patients respond to this treatment, but in more than one half the disease becomes refractory to hormone therapy in ,2 years (2). The treatment of hormone-refractory disease is less than satis- factory. Treatment options include supportive care only: second- line hormonal therapy (e.g., adding or withdrawing antiandro- gens, corticosteroids, and others); chemotherapy; and/or experimental treatments (3). Nonetheless, the median survival of patients suffering from hormone-refractory disease is gener- ally ,1 year (4). Clearly, the lack of effective treatment for advanced hormone-refractory prostate cancer necessitates de- velopment of new therapies. Recent advances in immunology, particularly in isolation and characterization of dendritic cells, have raised hopes that immunotherapy might provide such an additional therapeutic modality (5). Dendritic cells are the only antigen-presenting cells that can prime naive T cells and initiate an immune response (6). Isolated dendritic cells can be exposed to tissue- or disease-associated antigens in vitro and reinfused to stimulate immunity to those antigens (5, 7, 8). Indeed, such ex vivo- processed cells have been used successfully in experimental models (9, 10) and clinical trials (5, 8, 11–14). These trials used dendritic cells exposed to disease-associated antigens (i.e., id- iotypic monoclonal protein, tumor cell lysate, and HIV-derived antigens). In this Phase I study of treatment safety, our second- ary goal was to investigate if ex vivo-processed autologous dendritic cells can prime cellular immunity against a normal tissue antigen such as PAP, 3 characteristic both of normal pros- tate (15, 16) and prostate carcinoma (15, 16). Studies in rats in vivo indicate that rat dendritic cells exposed to rat PAP induce anti-PAP cellular immunity but do not induce antibodies to PAP (17). However, when the same Received 12/11/99; revised 2/1/00; accepted 2/2/00. The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. 1 Supported by Mrs. Adelyn L. Luther, Singer Island, Florida, and the Mayo Clinic Cancer Center. 2 To whom requests for reprints should be addressed, at Mayo Clinic, Guggenheim 1311A, Rochester, MN 55905. Phone: 507-284-2814; Fax: 507-266-5146; E-mail: [email protected]. 3 The abbreviations used are: PAP, prostatic acid phosphatase; GM- CSF, granulocyte/macrophage-colony stimulating factor; PBMC, pe- ripheral blood mononuclear cell; PSA, prostate-specific antigen; HLA, human leukocyte antigen. 2175 Vol. 6, 2175–2182, June 2000 Clinical Cancer Research Research. on May 21, 2018. © 2000 American Association for Cancer clincancerres.aacrjournals.org Downloaded from
Transcript of Priming Tissue-specific Cellular Immunity in a Phase I...

Advanves in Brief
Priming Tissue-specific Cellular Immunity in a Phase I Trial ofAutologous Dendritic Cells for Prostate Cancer1
Patrick A. Burch, Jami K. Breen,Jan C. Buckner, Dennis A. Gastineau,Judith A. Kaur, Reiner L. Laus,Douglas J. Padley, Madhusudan V. Peshwa,Henry C. Pitot, Ronald L. Richardson,Bouwien J. Smits, Pitsata Sopapan,George Strang, Frank H. Valone, andStanimir Vuk-Pavlovic2
Divisions of Medical Oncology [P. A. B., J. C. B., J. A. K., H. C. P.,R. L. R.], Transfusion Medicine [D. A. G., D. J. P.], and Stem CellLaboratory [S. V-P.], Mayo Clinic and Mayo Foundation, Rochester,Minnesota 55905, and Dendreon Corporation, Seattle, Washington98121 [R. L. L., M. V. P., B. J. S., P. S., G. S., F. H. V.]
AbstractWe attempted to induce therapeutic immunity against
prostate-derived tissues in patients suffering from progres-sive hormone-refractory metastatic prostate carcinoma.Thirteen patients were treated with two infusions, 1 monthapart, of autologous dendritic cells (APC8015) preexposedex vivo to PA2024, a fusion protein consisting of humangranulocyte/macrophage-colony stimulating factor (GM-CSF) and human prostatic acid phosphatase (PAP). Theinfusions were followed by three s.c. monthly doses ofPA2024 without cells. Three groups of patients each receivedPA2024 at 0.3, 0.6, or 1.0 mg/injection. AllPs were two-sided. Treatment was well tolerated. After infusions ofAPC8015, patients experienced only mild (grade 1–2) short-lived fever and/or chills, myalgia, pain, and fatigue. Onepatient developed grade 3 fatigue. Four patients developedmild local reactions to s.c. PA2024. Twelve patients wereevaluable for response to treatment. Circulating prostate-specific antigen levels dropped in three patients. T cells,drawn from patients after infusions of APC8015, but notbefore, could be stimulatedin vitro by GM-CSF (P 5 0.0004)and PAP (P 5 0.0001), demonstrating broken immune tol-erance against these two normal proteins. Injections ofPA2024 did not influence the reactivity of T cells againstPAP and GM-CSF. However, antibodies to GM-CSF and, toa much lesser extent, to PAP reached maximum titers only
after two or even three injections of PA2024, showing thatdirectly injected PA2024 was involved in stimulation ofhumoral immunity. Dendritic cells exposed to antigenexvivo can induce antigen-specific cellular immunity in pros-tate cancer patients, warranting further studies of this modeof immunotherapy.
IntroductionAdenocarcinoma of the prostate is the most common ma-
lignancy in American men and the second most frequent causeof their death from cancer; nearly 40,000 men are projected todie from this disease in 1999 (1). For patients with advanceddisease, standard care includes hormone ablation by bilateralorchiectomy or by agonists of luteinizing hormone-releasinghormone, with or without antiandrogens (2). Initially, mostpatients respond to this treatment, but in more than one half thedisease becomes refractory to hormone therapy in,2 years (2).The treatment of hormone-refractory disease is less than satis-factory. Treatment options include supportive care only: second-line hormonal therapy (e.g.,adding or withdrawing antiandro-gens, corticosteroids, and others); chemotherapy; and/orexperimental treatments (3). Nonetheless, the median survivalof patients suffering from hormone-refractory disease is gener-ally ,1 year (4). Clearly, the lack of effective treatment foradvanced hormone-refractory prostate cancer necessitates de-velopment of new therapies.
Recent advances in immunology, particularly in isolationand characterization of dendritic cells, have raised hopes thatimmunotherapy might provide such an additional therapeuticmodality (5). Dendritic cells are the only antigen-presentingcells that can prime naive T cells and initiate an immuneresponse (6). Isolated dendritic cells can be exposed to tissue- ordisease-associated antigensin vitro and reinfused to stimulateimmunity to those antigens (5, 7, 8). Indeed, suchex vivo-processed cells have been used successfully in experimentalmodels (9, 10) and clinical trials (5, 8, 11–14). These trials useddendritic cells exposed to disease-associated antigens (i.e., id-iotypic monoclonal protein, tumor cell lysate, and HIV-derivedantigens). In this Phase I study of treatment safety, our second-ary goal was to investigate ifex vivo-processed autologousdendritic cells can prime cellular immunity against a normaltissue antigen such as PAP,3 characteristic both of normal pros-tate (15, 16) and prostate carcinoma (15, 16).
Studies in ratsin vivo indicate that rat dendritic cellsexposed to rat PAP induce anti-PAP cellular immunity but donot induce antibodies to PAP (17). However, when the sameReceived 12/11/99; revised 2/1/00; accepted 2/2/00.
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisementin accordance with 18 U.S.C. Section 1734 solely toindicate this fact.1 Supported by Mrs. Adelyn L. Luther, Singer Island, Florida, and theMayo Clinic Cancer Center.2 To whom requests for reprints should be addressed, at Mayo Clinic,Guggenheim 1311A, Rochester, MN 55905. Phone: 507-284-2814; Fax:507-266-5146; E-mail: [email protected].
3 The abbreviations used are: PAP, prostatic acid phosphatase; GM-CSF, granulocyte/macrophage-colony stimulating factor; PBMC, pe-ripheral blood mononuclear cell; PSA, prostate-specific antigen; HLA,human leukocyte antigen.
2175Vol. 6, 2175–2182, June 2000 Clinical Cancer Research
Research. on May 21, 2018. © 2000 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

antigen was injected s.c., it raised a strong antibody response(17). Accordingly, in this Phase I trial we administered twodoses of dendritic cells “pulsed”ex vivowith antigen, followedby three injections of soluble antigen to men suffering fromadvanced hormone-refractory prostate cancer and monitoredtreatment safety and effects on cellular and humoral immunity.
Patients and MethodsPatients. Patients were enrolled into the trial after having
signed the informed consent form approved by the Mayo ClinicInstitutional Review Board. Men were eligible for the study ifthey suffered from histologically proven adenocarcinoma of theprostate that progressed despite the primary hormonal therapy(orchiectomy or administration of a LHRH agonist with orwithout an antiandrogen). Progression of disease was ascer-tained by the increase in the levels of circulating PSA and byradiography (bone scan and/or computed tomography). For en-rollment into the study, any antiandrogens were withdrawn, andcontinued progression of disease had to be documented. Othereligibility requirements were age.18; Eastern CooperativeOncology Group performance status 0 or 1; PSA$ 5.0 ng/ml;PAP equal to or above twice the upper limits of normal; nega-tive serological tests for HIV, human T-cell lymphotrophic virustype I, hepatitis B, and hepatitis C; adequate hematologicalparameters (WBC$2,000/mm3; absolute neutrophil count$1,000/mm3; platelets$100,000/mm3; and hemoglobin.9.0g/dl), creatinine#2.0 mg/dl; total bilirubin equal to or less thantwice the upper limit of normal; and aspartate aminotransferaseand alanine aminotransferase equal to or less than five times theupper limit of normal.
Treatment and Assessment. The clinical trial includedi.v. infusion of two doses of PAP antigen-loaded autologousdendritic cells [APC8015, autologous dendritic cells exposedexvivo to PA2024 (see below); Dendreon] 1 month apart andfollowed by three monthly s.c. doses of the PAP antigen(PA2024, a fusion protein consisting of human GM-CSF andPAP; Dendreon; Fig. 1). Two days before each treatment, thepatients underwent leukopheresis (1.5–2.0 blood volumes) tocollect mononuclear cells, the fraction containing dendritic cellprecursors. Patients received no chemotherapy or growth factorsbefore leukopheresis. The APC8015 dose contained all dendriticcells prepared from one leukopheresis product and was infusedi.v. over 30 min in the outpatient setting. The patients wereobserved for acute side effects for 1 h after infusion and thendischarged. The dose of APC8015 applied in this study hadalready been shown to be safe in a Phase I trial (18). We testedthree dose levels of s.c.-injected soluble antigen PA2024: 0.3,0.6, and 1.0 mg. Cohorts of three patients were entered at eachlevel as long as dose-limiting grade 3 toxicity (NIH Common
Toxicity Criteria) was not observed in more than one patient/level. Six patients were to be treated at the final dose leveldetermined either by grade 3 toxicity or by the attainment of thehighest planned dose. PA2024 was injected s.c. in the thigh (onesite for the first two dose levels and two sites for the third doselevel). Patients were observed for acute side effects and thenfollowed as outpatients. All adverse events were evaluated forthe relationship to treatment with APC8015 or PA2024, and theseverity was scored according to the NIH Common ToxicityCriteria.
Patients were monitored by history, physical examination,blood counts, serum chemistry, and measurements of PSA andPAP every 4 weeks during treatment (weeks 0–16). Tumorburden was evaluated by radiography at week 0 (baseline), week20, and then every 8 weeks until progression. Unless accompa-nied by clinical progression, generally verified by repeatedradiographic assessment, increasing levels of PSA or PAP be-fore completion of the treatment were not taken as reasons fordiscontinuation of treatment.
Preparation of Antigen-loaded Dendritic Cells(APC8015). PA2024 antigen is a recombinant protein consist-ing of human PAP fused through its COOH terminus to the NH2
terminus of GM-CSF by a Gly-Ser linker. The GM-CSF portiontargets the fusion protein to dendritic cells (19). ThePA2024gene was cloned into the pBacPak8 vector (Clontech, Palo Alto,CA) and transfected into Sf21 insect cells by the use of acommercially available kit (Clontech). Recombinant baculovi-rus was then cloned by plaque purification and propagated inSf21 cells adapted to grow in protein-free Sf900–2 medium(Life Technologies, Inc., Grand Island, NY) supplemented withhydrolyzed yeast extract (Life Technologies, Inc.). The PA2024protein was released into the culture supernatant and purified forthis trial by three sequential column chromatography steps to.90% purity.
Antigen-loaded Dendritic Cells (APC8015). PAP-loaded autologous dendritic cells were prepared at the MayoClinic Cell Processing Center. The Cell Processing Center com-prises environmental control, staffing, and process controls thatcomply with the current Good Manufacturing Practices forsomatic cell therapy. It contains a Class 10,000 clean room withClass 100 biosafety cabinets and other equipment for cell iso-lation and culture.
APC8015 was prepared by a modification of the methoddescribed by Hsuet al. (5). The leukopheresis product wascollected at the adjacent Mayo Blood Bank and transferred tothe Cell Processing Center. PBMCs were isolated by centrifug-ing over a buoyant density solution of 1.0770 g/ml, 320 mosM,and washed twice to remove platelets. The cells were thencentrifuged over the second buoyant density solution of 1.0650
Fig. 1 Treatment schedule. Patients underwentapheresis 2 days before the two infusionsof autologous antigen-loaded dendritic cells(APC8015) on weeks 0 and 4. Subsequently, therecombinant antigen consisting of the fusedGM-CSF and PAP (PA2024) was injected onweeks 8, 12, and 16. Patients were divided intogroups receiving 0.3, 0.6, or 1.0 mg of PA2024.
2176Dendritic Cells in Prostate Cancer
Research. on May 21, 2018. © 2000 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

g/ml, 320 mosM, to deplete monocytes. The high-density cellsin the pellet containing dendritic cell precursors were suspendedin AIM-V medium (Life Technologies, Inc.) at 1.03 107/mland incubated with PA2024 (10mg/ml) in the absence of ex-ogenous serum or cytokines in a humidified 5% (v/v) CO2 in airat 37°C. After 40-h of culturing, the cells were washed, sus-pended in lactated Ringer’s solution, and transported to theoutpatient Mayo Infusion Therapy Center for infusion. Qualitycontrol for each cell lot included cell number and viability,Gram’s stain, cell surface marker phenotype, and tests of steril-ity, Mycoplasma,and endotoxin. The results of tests for sterility,Mycoplasma,and endotoxin were available only after APC8015had been infused. Twenty-five lots of APC8015 were preparedfor 13 patients. APC8015 contained 18.66 9.4% (median,18.0%; range, 6.0–39.0%) dendritic cells, defined as CD54bright,65.1 6 12.0% T cells (CD31), 16.6 6 7.8% monocytes(CD141), and 5.0 6 2.4% B cells (CD191). In APC8015prepared for another prostate cancer immunotherapy study (18),we found that the CD54bright cells were also bright in CD40,CD86, HLA-A,B,C, and HLA-DR (data not shown); inAPC8015 prepared from the blood of normal healthy donors,.90% of CD54bright cells were HLA-DRbright (data not shown).
Assessment of Immune Function. To assess the im-mune response to therapy, 20–40 ml of venous blood wascollected in heparinized tubes at week 0 (baseline values beforedendritic cell infusion) and in weeks 4, 8, 12, 16, and 20.Immediately after drawing, blood was transported at ambienttemperature overnight from the Mayo Clinic to Dendreon(Mountain View, CA). There, serum was separated and frozen.Mononuclear cells containing lymphocytes were isolated bycentrifuging over a buoyant density solution of 1.0770 g/ml and320 mosM and washed twice to remove platelets. IsolatedPBMCs were resuspended in AIM-V medium (Life Technolo-gies, Inc.) containing 5.0% human AB serum (Gemini Bioprod-ucts, Calabas, CA) and used for functional testing on the day ofreceipt.
Antigen-dependent T-cell proliferation was tested againstPA2024, human seminal fluid PAP (Biodesign International,Kennebunk, ME), and GM-CSF (Leukine; Immunex, Seattle,WA). One hundred thousand PBMCs were plated per well ofround-bottomed, 96-well microtiter plates. Antigens were dis-solved in AIM-V medium containing 5.0% human AB serumand added to triplicate wells at the final concentration of 0.4,2.0, 10, or 50 mg/ml in the total volume of 200ml. Control wellscontained no antigen. The cells were incubated at 37°C in 5%CO2 for 5 days. Tritiated thymidine (Amersham, Piscataway,NJ), 1.0mCi/well, was added for the last 16 h of incubation,after which the cells were harvested with a Tomtec harvester(Wallac, Gaithersburg, MD). The radioactivity of incorporatedthymidine was measured as cpm in a Wallac-LKB Betaplatecounter (Wallac). T-cell proliferation response was consideredsignificant when the mean radioactivity of the wells containingantigen was at least twice above the mean radioactivity of thecontrol wells.
Proliferation is expressed as proliferation index calculatedfrom the formula.
logPI5 average(logcpmexp) 2 average(logcpmcontrol)
where PI is proliferation index, cpmexp denotes cpm of radio-activity incorporated by the cells in the presence of antigen, andcpmcontrol is the radioactivity incorporated by the analogouslytreated cells devoid of antigen. The logarithmic transformationobviates the effects of the nonnormal distribution of cpm deter-minations representing the radioactivity incorporated by cells.4
Antibodies specific for PA2024, GM-CSF, and PAP in theserum were quantified by an ELISA that was comprised ofimmobilized antigens and goat antibodies specific for humanIgG and IgM (Jackson ImmunoResearch, Westgrove, PA) con-jugated to horseradish peroxidase. Multiwell plates (DynexTechnologies, Chantilly, VA) were coated with antigens dis-solved at 1–2mg/ml in Dulbecco’s PBS (D-PBS) by overnightincubation at 4°C, washed with D-PBS (pH 7.4), containing0.05% Tween 20 (Sigma Chemical Co., St. Louis, MO), blockedwith 5% powdered milk dissolved in Tris-buffered saline, andwashed in D-PBS. Serial dilutions of the test serum were dis-pensed onto the plate, which included a negative control (poolednormal human serum) and a positive control serum. The plateswere incubated for 1 h and washed. Then human immunoglob-ulin bound to the plate was detected by horseradish peroxidase-conjugated goat antihuman IgG/IgM. Color was developed fromo-phenylenediamine dihydrochloride and read on a plate readerat 492 nm. The coefficient of variability of controls for thesemeasurements was routinely,20%. The absorbance measuredfor each tested serum was compared with the curve for anegative control serum obtained from a subject who did notsuffer from prostate cancer. The measured values two timesabove the background were statistically significant. The titer ofthe tested antibody was determined as the highest dilution thatresulted in absorbance two times above the background.
Statistics. Changes in antigen-specific cellular immunitywere analyzed by comparing proliferation of T cells drawn atsuccessive times before and during treatment at 4-week inter-vals. By the use of the PROC MIXED program package (SASInstitute, Cary, NC), the relationship was examined by compar-ing radioactivity (cpm) incorporated by cells from each of ninepatients stimulated by four concentrations of each antigen. Eachtime/antigen combination was compared separately, yielding therespectiveP. The significance of differences between meanvalues was assessed by the two-tailed Student’st test for un-equal variances (see Table 2). The difference between medianlevels of antibodies to PAP was determined by the two-tailedMann-Whitney test. The significance level for all comparisonswas set atP , 0.05.
ResultsPatients. Thirteen patients were enrolled between De-
cember 15, 1997, and July 7, 1998. They were all eligible andprovided written informed consent before enrollment. The pa-tients were evaluated if they received at least one dose ofPA2024. One patient (no. 7) was not evaluated because thedisease progressed after one dose of APC8015. Demographic
4 G. Strang, W. G. Haag, B. Smits, J. Breen, P. Sopapan, and W. C. A.van Schooten. Quantitation of cellular immune response after immuno-therapy for prostate cancer, manuscript in preparation.
2177Clinical Cancer Research
Research. on May 21, 2018. © 2000 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

data are shown in Table 1. Seven patients had primarily osseousmetastases, and five patients had soft tissue/nodal disease. Atthe time of entry into the study, no patient suffered from anyapparent visceral metastases. All patients failed prior hormonetherapy and were ambulatory. Most tumor-related symptomswere mild.
Treatment Received. Table 2 shows the number of den-dritic cells and the dose of PA2024 administered to each patientgroup. All patients received two doses of APC8015 exceptpatient 7. The patients received the full course of PA2024 ateach dose level except patients 5 and 8, who received only oneinjection, and patients 9 and 12, who received two injections.The achieved numbers of dendritic cells in the first and seconddoses of APC8015 were similar, demonstrating that cell proc-essing was consistent. Variation in the total number of nucleatedcells was slightly larger and ranged among patients between1.1 3 109 and 5.43 109.
Adverse Events. Generally, the treatment was well tol-erated. Five patients developed mild fever (grade 1–2) and/orchills within 1 h after infusion of APC8015; these symptomslasted less than 24 h. Five patients developed mild (grade 1–2)myalgia or pain, usually 1–2 days after treatment withAPC8015; these symptoms were fully resolved within 1 week.Six patients reported transient grade 1–2 fatigue, and one expe-rienced prolonged grade 3 fatigue that was temporally related totreatment. Four patients developed mild (grade 1) local reactionsafter injection of PA2024: patient 2 upon injections on weeks 12and 16, patient 3 on week 8, patient 4 on weeks 12 and 16, andpatient 10 on week 12. There were no adverse events related toleukopheresis, and all procedures were performed using periph-eral venous access.
Response to Treatment. Twelve patients could be eval-uated for the response to treatment. In patients 5, 10, and 11,PSA levels were reduced by more than one-half in the course of
treatment (Fig. 2; note the logarithmic scale on the ordinate),although in patient 5, PSA declined despite the rapid progres-sion of disease. Three patients (4, 10, and 11) experiencedsignificant drops in circulating PAP levels (Fig. 2). No responsewas detected by radiography. The median time to disease pro-gression was 135 days after registration (range, 30–274 days).
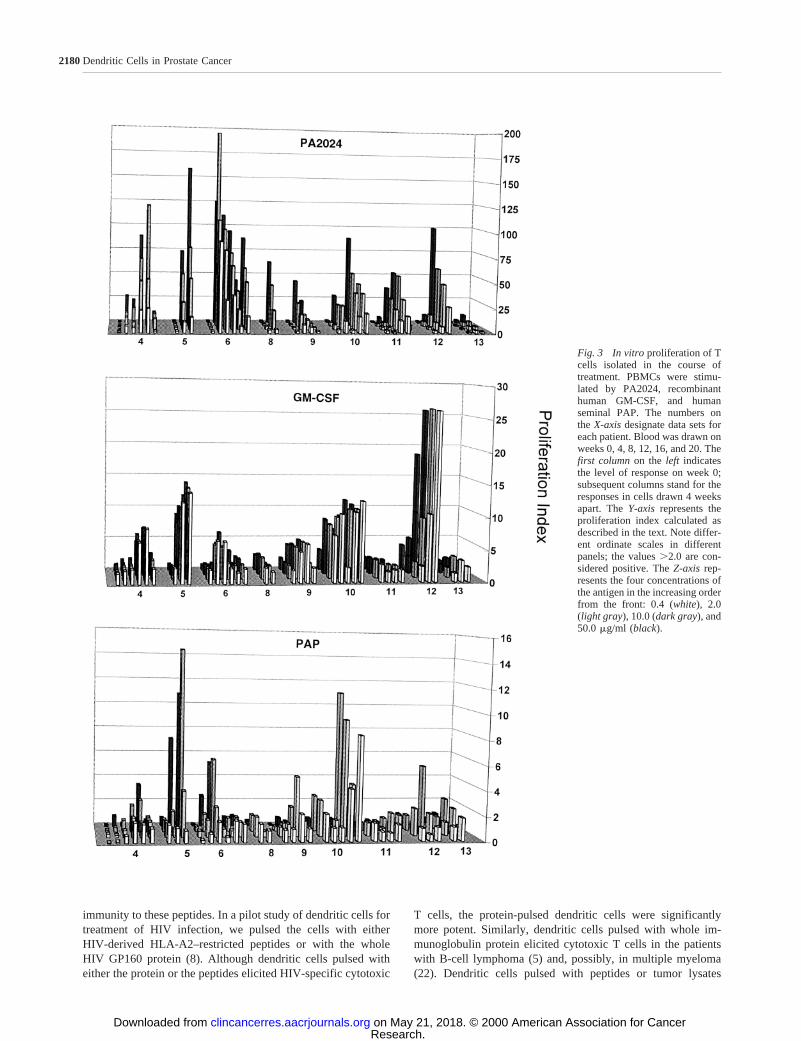
Antigen-specific T Cells. Development of T cells inresponse to APC8015 (i.e.,PA2024-laden dendritic cells) and tosoluble PA2024 was evaluated in nine patients. Data in Fig. 3show the T-cell response measured from week 0 every 4 weeksuntil week 20, or until the withdrawal from trial because ofdisease progression. The cells from patients 1–3 could not beevaluated because they proliferated strongly in the absence ofantigens; the reason for this phenomenon is unclear. Four weeksafter the first treatment with APC8015, T cells from all evalu-ated patients proliferatedin vitro in response to PA2024 (P50.0001). The change in the proliferation index differed amongpatients and ranged from 3 to 120. The response to PA2024persisted for the duration of treatment or duration of monitoring(Fig. 3, top).
To determine more precisely the specificity of T cellsproliferating in vitro in response to PA2024, we stimulated thecells with Leukine (recombinant GM-CSF; Fig. 3,middle) andPAP isolated from human seminal fluid (Fig. 3,bottom). BothGM-CSF and PAP induced T-cell proliferation (P 5 0.0004 and0.0001, respectively), in some patients more than 10 timesabove the baseline. Thus, infusion of APC8015 clearly inducedT cells specific for GM-CSF and for PAP, the components of thefusion protein PA2024.
On week 8, we administered the first of three s.c. injectionsof the soluble antigen and evaluated the effects on T-cell pro-liferation monthly. Within the limits of resolution of the assay,soluble antigen contributed little to the antigen-specific T-cellresponse induced by APC8015 (compare T-cell proliferationbefore week 12 with the proliferation on or after week 12;Fig. 3).
Antibody Response to Dendritic Cells and Soluble An-tigen. Eleven patients were evaluable for antibody responsesto PA2024 (Table 3). After treatment, all patients developedantibodies to PA2024. Nine patients responded after adminis-tration of antigen-loaded dendritic cells alone (before adminis-tration of PA2024) and two patients after administration ofPA2024 (week 12). We evaluated also the antibodies to GM-CSF and PAP. We found that three patients contained low titersof preexisting antibodies to GM-CSF (Table 3).
Table 1 Characteristics of patients enrolled in the triala
Age (median, range) 67.5 (59–84)ECOGb performance status 0 (0–1)Baseline PSA (median, range) 323 (19.8–920.9)Baseline PAP (median, range) 22.4 (9.1–831)Disease duration (mo) 72 (20–134)Primary therapy
Prostatectomy 3Radiation therapy 3Other 6
No. of hormone manipulationsOne 3Two 3Three 5Four 1
Anemia 4Elevated alkaline phosphatase 6Pain level
None 2Mild 9Moderate 0Severe 1
a The table does not contain data for patient 7, who was not fullyevaluable.
b ECOG, Eastern Cooperative Oncology Group.Values are number of patients.
Table 2 Dose of dendritic cells (APC8015) and soluble antigen(PA2024) delivered to patients
Patient
Dendritic cells (CD541; 106/m2)a
PA2024(mg/dose)Infusion no. 1 Infusion no. 2
1–3 2486 86 3066 237 0.34–6 2306 140 1476 49 0.67–13b 3256 155 2176 128 1.0
a No difference among groups was statistically significant.b Patient 7 received one dose of dendritic cells and no PA2024
because of early disease progression. Patients 5 and 8 received only onedose of PA2024, and patients 9 and 12 received only two doses.
2178Dendritic Cells in Prostate Cancer
Research. on May 21, 2018. © 2000 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

Antibodies to GM-CSF became measurable in mostpatients, in some with high titers, mostly at weeks 16 and 20. Indistinction to GM-CSF, antibodies to PAP were low in titer andoccurred in only five patients. Thus, APC8015 and PA2024raised antibodies mostly to PA2024 and GM-CSF.
To determine the effects of soluble PA2024 on circulatingantibody levels, we compared the titers of antibodies to PAP inthis study with the titers obtained in a similar study of prostatecancer that used APC8015 only (18). In this study, 2 of 12evaluated patients developed titers.40 (Table 3). In the otherstudy, 15 of 31 patients developed titers.40. This difference isstatistically significant (P5 0.01, Mann-Whitney test).
DiscussionIn a previous study, it was determined that APC8015 is safe
at any dose that could be manufactured (18). Such dendritic cellpreparations induced PAP-specific T cells, independent of theroute of administration (i.v., intradermal, or intralymphatic; Ref.20). This Phase I trial was designed to evaluate the safety andthe maximum tolerable dose of PA2024 administered s.c. aftertwo i.v. infusions of APC8015. The impetus for the study camefrom an analogous study in rats that showed that soluble antigenboost after infusions of antigen-loaded dendritic cells raisedantibodies against the antigen (17). We speculated that a similareffect in men might be beneficial in the control of metastaticprostate disease. Immunological end points, evaluated in mostpatients, allowed us to assess the effects of treatment on immu-nity against PAP, a prostate tissue-specific antigen, and on theserum levels of PSA and PAP as surrogate markers of treatmentefficacy.
Antigen-specific T cells and antibodies raised by APC8015and PA2024 have provided important insights into the efficacyof antigen-loaded dendritic cells and the elicited immune re-sponse. Antigen-loaded dendritic cells were highly efficaciousin eliciting antigen-specific T cells; in most patients, antigen-specific T cells were present within 4 weeks of the first infusion
of APC8015. The immune response to the fusion proteinPA2024 could be clearly dissected into immunity against theconstituent PAP and GM-CSF. This is a direct demonstrationthat the treatment broke tolerance to a normal tissue-associatedantigen (PAP) and a normal cytokine (GM-CSF).
Overall, the treatment was tolerated well. Infusions ofAPC8015 resulted in mild symptoms observed previously insimilar studies (18). s.c. injections of PA2024 were generallyharmless, with six patients experiencing mild (grade 1–2) sys-temic toxicity and four patients having a local grade 1 reactionat the site of s.c. injection. Interestingly, at the time of thesereactions, two patients (4 and 10) demonstrated high levels ofT-cell reactions to PA2024 and its componentsin vitro. Thisindicates the possibility that the s.c. administration of PA2024induced a delayed-type hypersensitivity-like reaction.
PA2024, the fusion protein used for “pulsing” dendriticcells, contains full-length PAP and GM-CSF. The fusion mol-ecule is endowed with the enzyme function of acid phosphataseand can stimulate growth in GM-CSF–dependent cell lines.Exposure to PA2024 allows dendritic cells to process, edit, andpresent antigen in the context of HLA class I and class IIrestriction characteristic for each individual. Consequently, wedid not select patients on the basis of their HLA makeup; thisdecision is supported by an analysis of the ability of differentHLA class I molecules to present PAP-derived peptides, whichshowed that most can present one or more peptides derived fromPAP.5 Such peptides can elicit cytotoxic T cells that can effec-tively lyse PAP-secreting prostate tumor cellsin vitro (21).
Murphy and colleagues treated prostate cancer patientswith autologous dendritic cells pulsed with HLA-A0201-specific peptides derived from prostate-specific membrane an-tigen (11). In contrast to our experience, no patient developed
5 S. Vuk-Pavlovic, unpublished data.
Fig. 2 Levels of PSA and PAP in patient bloodbefore treatment (baseline) and at the nadir duringtreatment. The numbers designate individual pa-tients. Thefull lines indicate patients who experi-enced the largest change in the levels of PSA andPAP, respectively.
2179Clinical Cancer Research
Research. on May 21, 2018. © 2000 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
immunity to these peptides. In a pilot study of dendritic cells fortreatment of HIV infection, we pulsed the cells with eitherHIV-derived HLA-A2–restricted peptides or with the wholeHIV GP160 protein (8). Although dendritic cells pulsed witheither the protein or the peptides elicited HIV-specific cytotoxic
T cells, the protein-pulsed dendritic cells were significantlymore potent. Similarly, dendritic cells pulsed with whole im-munoglobulin protein elicited cytotoxic T cells in the patientswith B-cell lymphoma (5) and, possibly, in multiple myeloma(22). Dendritic cells pulsed with peptides or tumor lysates
Fig. 3 In vitro proliferation of Tcells isolated in the course oftreatment. PBMCs were stimu-lated by PA2024, recombinanthuman GM-CSF, and humanseminal PAP. The numbers onthe X-axisdesignate data sets foreach patient. Blood was drawn onweeks 0, 4, 8, 12, 16, and 20. Thefirst columnon the left indicatesthe level of response on week 0;subsequent columns stand for theresponses in cells drawn 4 weeksapart. TheY-axis represents theproliferation index calculated asdescribed in the text. Note differ-ent ordinate scales in differentpanels; the values.2.0 are con-sidered positive. TheZ-axis rep-resents the four concentrations ofthe antigen in the increasing orderfrom the front: 0.4 (white), 2.0(light gray), 10.0 (dark gray), and50.0mg/ml (black).
2180Dendritic Cells in Prostate Cancer
Research. on May 21, 2018. © 2000 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

resulted in T-cell immune responses in the patients sufferingfrom melanoma (7). These studies did not compare immunoge-nicity of dendritic cells pulsed with peptides with immunoge-nicity of the cells pulsed with whole proteins, but it is highlyprobable that tumor-cell lysates contained both HLA class I- andclass II-restricted peptides.
Development of an effective immune response requirescomplex interactions between CD4-positive class II-restricted Tcells and C8-positive class I-restricted T cells. Possibly, protein-pulsed dendritic cells can stimulate both CD4- and CD8-positiveT cells, whereas peptide-pulsed dendritic cells are designed tostimulate CD8-positive T cells only. The limited clinical datawith antigen-pulsed dendritic cells suggest that breaking toler-ance to hitherto unrecognized antigens such as PAP and pros-tate-specific membrane antigen requires stimulation of bothCD4- and CD8-positive T cells (23). Under some circum-stances, targeting CD8-positive T cells alone with class I-restricted peptides may suffice for stimulation of immunity, butthe concurrent targeting of CD4-positive T cells may augmentthe response.
Although APC8015 raised T cells specific for GM-CSFand PAP with similar efficacy, the combined treatment(APC8015 and PA2024) had a different effect on raising anti-bodies against GM-CSF and PAP: (a) after 16–20 weeks, anti-bodies against GM-CSF were observed in most patients. Inter-estingly, antibodies against PAP were detected in only 5 (of 11)patients, invariably at low titers; (b) the titer of antibodies toGM-CSF was inversely proportional to the administered dose ofPA2024; and (c) it is noteworthy that some patients harboredspontaneous antibodies to GM-CSF; however, this condition didnot predict a high-antibody response to GM-CSF after treat-ment. In contrast to these results, we observed a higher rate ofantibody responses to PAP and higher titers of anti-PAP anti-bodies in a study of APC8015 alone given on a schedule similarto the one used in the current trial (weeks 0, 4, and 8; Ref. 18).Comparison of the two trials of APC8015 suggests that admin-istration of soluble antigen PA2024 in the dose and schedule
used in this trial actually suppressed antibody generation. Theadministration of soluble antigen without adjuvant can sup-presses B-cell immune responses (24). However, GM-CSF is animmune adjuvant; our data and those of others demonstrate thatfusion proteins containing GM-CSF elicit potent antibody re-sponses in the absence of exogenous adjuvant.
Development of anti-GM-CSF antibodies after parenteraladministration has been well documented (25, 26), but theseantibodies appear to have no apparent clinical consequences. Itis unlikely that antibodies to GM-CSF would affect the potencyof APC8015 because dendritic cells display peptide fragmentsof GM-CSF and antibodies cannot recognize such peptides.Antibodies to GM-CSF could, however, limit the adjuvant effectof GM-CSF administered either as a fusion protein such asPA2024 or as a soluble protein boost.
In the reduction of the levels of circulating PSA and PAP,we found preliminary evidence of activity of this immunother-apy protocol. In one patient (5), however, PSA dropped to lessthan one-half of the pretreatment value at the time when thedisease actively progressed; his PAP remained unchanged. Thisobservation is in line with the concerns about the use of PSA asthe sole end point for measuring the response of prostate cancerto novel treatments (27).
We did not observe any objective radiographic response totreatment. The time to disease progression after diagnosis was inthe range of values reported for cytotoxic treatments for hor-mone-refractory prostate cancer, where progression was deter-mined by means other than changes in PSA (28, 29). However,the treatment was well tolerated and elicited few side effectscompared with chemotherapy. It raised PAP-specific immunityeffectively. In addition, we observed sporadic treatment-induceddecreases of circulating PSA and PAP. Consequently, we haveinitiated a Phase II trial with the highest dose of PA2024; thegoal of the trial is to define better the response, time to progres-sion, and survival in a cohort of men with hormone-refractoryprostate cancer treated with APC8015 followed by PA2024.
AcknowledgmentsWe thank Dr. Franklyn G. Prendergast for continuing interest and
support.
References1. Landis, S., Murray, T., Bolden, S., and Wingo, P. Cancer Statistics1999. CA Cancer J. Clin.,49: 8–31, 1999.2. Dowling, A. J., and Tannock, I. F. Systemic treatment for prostatecancer. Cancer Treat. Rev.,24: 283–301, 1998.3. Oh, W. K., and Kantoff, P. W. Management of hormone refractoryprostate cancer: current standards and future prospects. J. Urol.,160:1230–1231, 1998.4. Newling, D. W., Dennis, L., and Vermeylen, K. Orchiectomyversusgoserelin and flutamide in the treatment of newly diagnosed metastaticprostate cancer. Analysis of the criteria for evaluation used in theEuropean Organization for Research and Treatment of Cancer. Genito-urinary Group Study, 30853. Cancer (Phila.),72: 3793–3798, 1993.5. Hsu, F. J., Benike, C., Fagnoni, F., Liles, T. M., Czerwinski, D.,Taidi, B., Engleman, E. G., and Levy, R. Vaccination of patients withB-cell lymphoma using autologous antigen-pulsed dendritic cells. Nat.Med., 2: 52–58, 1996.6. Banchereau, J., and Steinman, R. M. Dendritic cells and the controlof immunity. Nature (Lond.),392: 245–252, 1998.
Table 3 Antibodies to GM-CSF and PAP in sera of patients treatedwith APC8015 and PA2024
Patienta
Maximum antibody titerto GM-CSF (time to
maximum response, weeks)b
Maximum antibody titerto PAP (time to
maximum response, weeks)b
1 10,000c (16) 02 20,000c (16) 320 (8)3 40,000 (16) 04 20,000 (20) 05 320 (8) 06 640 (20) 10 (4)9 80c,d 10 (16)
10 640 (16) 011 1280 (16) 160 (20)12 80 (16) 20 (12)13 1280 (16) 0
a Patients 7 and 8 suffered from rapidly progressive disease, andserum was not available for testing.
b Time to development of titer$10; for patients with preexistingantibodies, time to a 2-fold or larger increase in titer.
c Patient with preexisting antibodies to GM-CSF at titers.20.d Preexisting titer was unaffected by treatment.
2181Clinical Cancer Research
Research. on May 21, 2018. © 2000 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

7. Nestle, F. O., Alijagic, S., Gilliet, M., Sun, Y., Grabbe, S., Dummer,R., Burg, G., and Schadendorf, D. Vaccination of melanoma patientswith peptide- or tumor lysate-pulsed dendritic cells. Nat. Med.,4:328–332, 1998.8. Kundu, S. K., Engleman, E., Benike, C., Shapero, M. H., Dupuis, M.,van Schooten, W. C., Eibl, M., and Merigan, T. C. A pilot clinical trialof HIV antigen-pulsed allogeneic and autologous dendritic cell therapyin HIV-infected patients. AIDS Res. Hum. Retrovir.,14: 551–560,1998.9. Gong, J., Chen, D., Kashiwaba, M., and Kufe, D. Induction ofantitumor activity by immunization with fusions of dendritic and carci-noma cells. Nat. Med.,3: 558–561, 1997.10. Zitvogel, L., Regnault, A., Lozier, A., Wolfers, J., Flament, C.,Tenza, D., Ricciardi-Castagnoli, P., Raposo, G., and Amigorena, S.Eradication of established murine tumors using a novel cell-free vac-cine: dendritic cell-derived exosomes. Nat. Med.,4: 594–600, 1998.11. Murphy, G., Tjoa, B., Ragde, H., Kenny, G., and Boynton, A. PhaseI clinical trial: T-cell therapy for prostate cancer using autologousdendritic cells pulsed with HLA-A0201-specific peptides from prostate-specific membrane antigen. Prostate,29: 371–380, 1996.12. Segel, L. A., Jaeger, E., Elias, D., and Cohen, I. R. A quantitativemodel of autoimmune disease and T-cell vaccination: does more meanless? Immunol. Today,16: 80–84, 1995.13. Lotze, M. T., Shurin, M., Davis, I., Amoscato, A., and Storkus,W. J. Dendritic cell based therapy of cancer. Adv. Exp. Med. Biol.,417:551–569, 1997.14. Bendandi, M., Gocke, C. D., Kobrin, C. B., Benko, F. A., Sternas,L. A., Pennington, R., Watson, T. M., Reynolds, C. W., Gause, B. L.,Duffey, P. L., Jaffe, E. S., Creekmore, S. P., Longo, D. L., and Kwak,L. W. Complete molecular remissions induced by patient-specific vac-cination plus granulocyte-monocyte colony-stimulating factor againstlymphoma. Nat. Med.,5: 1171–1177, 1999.15. Solin, T., Kontturi, M., Pohlmann, R., and Vihko, P. Gene expres-sion and prostate specificity of human prostatic acid phosphatase (PAP):evaluation by RNA blot analysis. Biochim. Biophys. Acta,1048:72–77,1990.16. Lam, K., Li, C., Yam, L., Sun, T., Lee, G., and Ziesmer, S.Improved immunohistochemical detection of prostatic acid phosphataseby a monoclonal antibody. Prostate,15: 13–21, 1989.17. Valone, F. H., Yang, D. M., Ruegg, C. L., Shapiro, M. H., Slagle,P. H., and Laus, R. Dendritic cell immunotherapy of prostate cancer:preclinical models of autoimmune prostatitis and early clinical experi-ence. Exp. Haematol. Today, in press, 2000.18. Valone, F. H., Small, E. J., Peshwa, M., Strang, G., Laus, R.,Ruegg, C., and van Schooten, W. Immunotherapy of hormone refractory
hormone cancer (HRPC) with prostate acid phosphatase (PAP)-loadeddendritic cells (APC8015). Proc. Am. Soc. Clin. Oncol. Annu. Meet.,18: 312a, 1999.19. Tao, M. H., and Levy, R. Idiotype/granulocyte-macrophage colony-stimulating factor fusion protein as a vaccine for B-cell lymphoma.Nature (Lond.),362: 755–758, 1993.20. Fong, L., Ruegg, C. L., Brockstedt, D., Engleman, E. G., and Laus,R. Induction of tissue-specific autoimmune prostatitis with prostaticacid phosphatase immunization: implications for immunotherapy ofprostate cancer. J. Immunol.,159: 3113–3117, 1997.21. Peshwa, M. E., Shi, J. D., Ruegg, C. L., Laus, R., and van Shooten,W. C. A. Induction of prostate tumor-specific CD81cytotoxic T-lymphocytesin vitro using antigen presenting cells pulsed with prostaticacid phosphatase peptide. Prostate,36: 129–138, 1998.22. Lacy, M., Wettstein, P., Greipp, P. R., Fonseca, R., Dispenzieri, A.,Rajkumar, S. V., Gastineau, D. A., Lust, J., Witzig, T., Valone, F., Kyle,R. A., and Gertz, M. A. Dendritic cell-based idiotype vaccination forpost transplant multiple myeloma. Book of Abstracts, VII InternationalMultiple Myeloma Workshop, p. 109. Stockholm: 1999.23. Ridge, J. P., Di Rosa, F., and Matzinger, P. Superactivation ofdendritic cells: a T helper’s way of helping killers. Nature (Lond.),393:474–478, 1998.24. Taussig, M. J. Induction of hapten-specific B cell tolerance by lowdoses of hapten-carrier conjugate. Nature (Lond.),245: 34–36, 1973.25. Gribben, J., Devereux, S., Thomas, N., Keim, M., Jones, H., Gol-stone, A., and Linch, D. Development of antibodies to unprotectedglycosylation sites on recombinant human GM-CSF. Lancet,335: 434–437, 1990.26. Chen, T. T., and Levy, R. Induction of auto-antibody responses toGM-CSF by hyperimmunization with an Id-GM-CSF fusion protein.J. Immunol.,154: 3105–3117, 1995.27. Thalmann, G. N., Sikes, R. A., Chang, S. M., Johnston, D. A., vonEschenbach, A. C., and Chung, L. W. K. Suramin-induced decrease inprostate-specific antigen expression with no effect on tumor growth inthe LNCaP model of human prostate cancer. J. Natl. Cancer Inst.,88:794–801, 1996.28. Murphy, G. P., Priore, R. L., and Scardino, P. T. Hormone-refrac-tory metastatic prostatic cancer treated with methotrexate, cyclophos-phamide plus Adriamycin, cis-platinum plus 5-fluorouracil plus cyclo-phosphamide. National Prostatic Cancer Project Randomized Trial.Urology, 32: 33–40, 1998.29. Wozniak, A. J., Blumenstein, A. B., Crawford, E. D., Moileau, M.,Rivkin, S. E., and Fletcher, W. S. Cyclophosphamide, methotrexate, and5-fluorouracil in the treatment of metastatic prostate cancer. A South-west Oncology Group Study. Cancer (Phila.),71: 3975–3978, 1993.
2182Dendritic Cells in Prostate Cancer
Research. on May 21, 2018. © 2000 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

2000;6:2175-2182. Clin Cancer Res Patrick A. Burch, Jami K. Breen, Jan C. Buckner, et al. Autologous Dendritic Cells for Prostate CancerPriming Tissue-specific Cellular Immunity in a Phase I Trial of
Updated version
http://clincancerres.aacrjournals.org/content/6/6/2175
Access the most recent version of this article at:
Cited articles
http://clincancerres.aacrjournals.org/content/6/6/2175.full#ref-list-1
This article cites 24 articles, 2 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/6/6/2175.full#related-urls
This article has been cited by 19 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/6/6/2175To request permission to re-use all or part of this article, use this link
Research. on May 21, 2018. © 2000 American Association for Cancerclincancerres.aacrjournals.org Downloaded from


















