Primary yolk sac tumor of the endometrium: a case report and review of the literature
2
Primary yolk sac tumor of the endometrium: a case report and review of the literature Roberto Rossi, MD; Daniela Stacchiotti, MD; Maria Grazia Bernardini, MD; Giovanna Calvieri, MD; Roberto Lo Voi, MD I n September 2004, a 30-year-old woman was admitted with abnormal vaginal bleeding that had been ongoing for 2 months. A transvaginal ultrasound showed that the uterine cavity was com- pletely occupied by an oval-shaped tu- mor, which was hyperechoic, 55 37 mm in size, highly vascularized, and showed aspects of neoangiogenesis. Re- sistive index (RI) was 0.20. Smear cytol- ogy was performed and showed that the tumor was a cervical adenocarcinoma. Hysteroscopy showed polypoid forma- tions in the cervical canal and uterine cavity. A biopsy revealed that the tumor was of germ cell origin. Abdominal and pelvic computerized scanning showed a uterine mass mimicking a myoma. No enlarged lymph nodes were present. Al- pha-fetoprotein (AFP) levels were 1.762 ng/mL (reference value: 0-20 ng/mL). A test for the beta-subunit of human cho- rionic gonadotropin (B-hcG) was nega- tive and Ca-125 was borderline (36 U/mL). After consulting the limited ex- isting literature, 1-3 the case was discussed with the pathologist and oncologist. The patient was informed of the recom- mended treatment, and she gave her consent. A simple total hysterectomy was performed. Bilateral adnexa were preserved. Pelvic paraaortic lymph nodes were not dissected. 2,3 The re- moved uterus measured 11 5.5 5.6 cm and weighed 170 g. Sectioning of the uterus revealed a tumor with rounded margins. The tumor was yellowish-white with a central hemorrhagic area, ex- tended from the region around the isth- mus to the uterine body. The tumor was infiltrating the entire wall of the myome- trium and had infiltrated the cervical stroma, reaching 1.5 mm from the outer surface. The tumor had the typical mi- croscopic features of an endodermal si- nus tumor in that it had reticular and solid growth patterns, and 47 Schiller- Duval bodies were present. The neoplas- tic cells and hyaline globules stained pos- itively for AFP. The morphologic and immunohistochemical pattern was con- sistent with a primary yolk sac tumor (YST) of the endometrium (Figure). Five days after the total hysterectomy, the patient was discharged and the levels of AFP were 759.5 ng/mL. Postoperative adjuvant therapy for the YST included 3 cycles of the bleomycin, etoposide, and cisplatin (BEP) regimen. Before the third cycle of chemotherapy, AFP levels were normal. The patient is still alive and has remained free of disease for more than 6 years after the completion of the therapy. Comment Of all the genital tumors, YSTs are rela- tively uncommon and they are mostly discovered in infants and adolescents (median age, 19 years). 4 Although they typically arise from the gonads, YSTs have already been reported in many ex- tragonadal sites. Ten to 15% of the cases may arise in a variety of midline extrago- nadal sites that mostly display an axial distribution pattern, such as the medias- tinum, the pineal region, and sacrococ- cygeal region and the female reproduc- tive tract. 5 These neoplasms metastasize early and invade surrounding structures. Metastases also occur via the blood and the lymphatic system. Because of their rarity, there has been no systematic study on the surgical management of extrago- nadal YSTs with a large number of cases. In 1993, Fujita et al 6 reported 41 patients with endodermal sinus tumor of the ovary treated with conservative surgery, followed by chemotherapy with 5- and 10-year survival rates of around 80%. AFP determinations are useful in the di- agnosis to monitor the results of therapy and for detecting metastases and recur- rence after therapy. In our case, a preop- erative abdominal-pelvic computed to- mographic scan did not show pathologies of either the ovaries or involvement of ret- roperitoneal lymph nodes. The inspection of the abdomen confirmed the absence of metastatic lesions. Given the age of the pa- tient, the proven efficacy of chemotherapy in this type of malignancy, and the ability to monitor the development of cancer with the determination of AFP, we decided to perform a conservative therapy. Conclusion Extraovarian pelvic YSTs are rare, with only 9 documented previously. 7 Primary YSTs arising in the endometrium are an even more rare malignant neoplasm be- cause, to our knowledge, this is the sixth documented case and the first treated with a simple total hysterectomy without bi- lateral salpingo-oophorectomy. Because YSTs occur more often in young women, we believe that preservation of ovarian function is important when possible. We also believe that a greater number of cases are necessary to determine the most ade- quate and appropriate treatment. f From the Obstetric and Gynecologic Unit, Mazzoni Hospital, Ascoli Piceno, Italy. Received Oct. 17, 2010; revised Nov. 28, 2010; accepted Dec. 7, 2010. Reprints: Roberto Rossi, MD, Via Giuseppe di Vittorio, 52-60131 Ancona, Italy. [email protected] 0002-9378/free © 2011 Mosby, Inc. All rights reserved. doi: 10.1016/j.ajog.2010.12.014 We describe a rare case of a primary yolk sac tumor of the endometrium treated with a simple total hysterectomy without bilateral salpingo-oophorectomy and 3 cycles of the bleomycin, etoposide and cisplatin regimen. Key words: endodermal sinus tumor, germ cells tumor, yolk sac tumor Case Report www. AJOG.org APRIL 2011 American Journal of Obstetrics & Gynecology e3
-
Upload
roberto-rossi -
Category
Documents
-
view
214 -
download
2
Transcript of Primary yolk sac tumor of the endometrium: a case report and review of the literature

mssotHtcwpuepntrtUi
m
Case Report www.AJOG.org
Primary yolk sac tumor of the endometrium:a case report and review of the literature
Roberto Rossi, MD; Daniela Stacchiotti, MD; Maria Grazia Bernardini, MD; Giovanna Calvieri, MD; Roberto Lo Voi, MDwof1Aaaremoromtittp
YecdalYwfaa
In September 2004, a 30-year-oldwoman was admitted with abnormal
vaginal bleeding that had been ongoingfor 2 months. A transvaginal ultrasoundshowed that the uterine cavity was com-pletely occupied by an oval-shaped tu-mor, which was hyperechoic, 55 � 37
m in size, highly vascularized, andhowed aspects of neoangiogenesis. Re-istive index (RI) was 0.20. Smear cytol-gy was performed and showed that theumor was a cervical adenocarcinoma.ysteroscopy showed polypoid forma-
ions in the cervical canal and uterineavity. A biopsy revealed that the tumoras of germ cell origin. Abdominal andelvic computerized scanning showed aterine mass mimicking a myoma. Nonlarged lymph nodes were present. Al-ha-fetoprotein (AFP) levels were 1.762g/mL (reference value: 0-20 ng/mL). A
est for the beta-subunit of human cho-ionic gonadotropin (B-hcG) was nega-ive and Ca-125 was borderline (36/mL). After consulting the limited ex-
sting literature,1-3 the case was discussedwith the pathologist and oncologist. Thepatient was informed of the recom-mended treatment, and she gave herconsent. A simple total hysterectomywas performed. Bilateral adnexa werepreserved. Pelvic paraaortic lymphnodes were not dissected.2,3 The re-
oved uterus measured 11 � 5.5 � 5.6cm and weighed 170 g. Sectioning of theuterus revealed a tumor with roundedmargins. The tumor was yellowish-white
From the Obstetric and Gynecologic Unit,Mazzoni Hospital, Ascoli Piceno, Italy.
Received Oct. 17, 2010; revised Nov. 28,2010; accepted Dec. 7, 2010.
Reprints: Roberto Rossi, MD, Via Giuseppe diVittorio, 52-60131 Ancona, [email protected]
0002-9378/free© 2011 Mosby, Inc. All rights reserved.
doi: 10.1016/j.ajog.2010.12.014with a central hemorrhagic area, ex-tended from the region around the isth-mus to the uterine body. The tumor wasinfiltrating the entire wall of the myome-trium and had infiltrated the cervicalstroma, reaching 1.5 mm from the outersurface. The tumor had the typical mi-croscopic features of an endodermal si-nus tumor in that it had reticular andsolid growth patterns, and 47 Schiller-Duval bodies were present. The neoplas-tic cells and hyaline globules stained pos-itively for AFP. The morphologic andimmunohistochemical pattern was con-sistent with a primary yolk sac tumor(YST) of the endometrium (Figure).
Five days after the total hysterectomy,the patient was discharged and the levelsof AFP were 759.5 ng/mL. Postoperativeadjuvant therapy for the YST included 3cycles of the bleomycin, etoposide, andcisplatin (BEP) regimen. Before the thirdcycle of chemotherapy, AFP levels werenormal. The patient is still alive and hasremained free of disease for more than 6years after the completion of the therapy.
CommentOf all the genital tumors, YSTs are rela-tively uncommon and they are mostlydiscovered in infants and adolescents(median age, 19 years).4 Although theytypically arise from the gonads, YSTshave already been reported in many ex-tragonadal sites. Ten to 15% of the casesmay arise in a variety of midline extrago-nadal sites that mostly display an axialdistribution pattern, such as the medias-tinum, the pineal region, and sacrococ-cygeal region and the female reproduc-tive tract.5 These neoplasms metastasize
We describe a rare case of a primary yolksimple total hysterectomy without bilaterableomycin, etoposide and cisplatin regimen
Key words: endodermal sinus tumor, germ
early and invade surrounding structures. q
APRIL 2011 Am
Metastases also occur via the blood andthe lymphatic system. Because of theirrarity, there has been no systematic studyon the surgical management of extrago-nadal YSTs with a large number of cases.In 1993, Fujita et al6 reported 41 patients
ith endodermal sinus tumor of thevary treated with conservative surgery,ollowed by chemotherapy with 5- and0-year survival rates of around 80%.FP determinations are useful in the di-gnosis to monitor the results of therapynd for detecting metastases and recur-ence after therapy. In our case, a preop-rative abdominal-pelvic computed to-ographic scan did not show pathologies
f either the ovaries or involvement of ret-operitoneal lymph nodes. The inspectionf the abdomen confirmed the absence ofetastatic lesions. Given the age of the pa-
ient, the proven efficacy of chemotherapyn this type of malignancy, and the abilityo monitor the development of cancer withhe determination of AFP, we decided toerform a conservative therapy.
ConclusionExtraovarian pelvic YSTs are rare, withonly 9 documented previously.7 Primary
STs arising in the endometrium are anven more rare malignant neoplasm be-ause, to our knowledge, this is the sixthocumented case and the first treated withsimple total hysterectomy without bi-
ateral salpingo-oophorectomy. BecauseSTs occur more often in young women,e believe that preservation of ovarian
unction is important when possible. Welso believe that a greater number of casesre necessary to determine the most ade-
tumor of the endometrium treated with alpingo-oophorectomy and 3 cycles of the
lls tumor, yolk sac tumor
sacl sa.
ce
uate and appropriate treatment. f
erican Journal of Obstetrics & Gynecology e3
Case Report www.AJOG.org
e4 American Journal of Obstetrics & Gynecology APRIL 2011
REFERENCES1. Ohta M, Sakakibara K, Mizuno K, et al. Suc-cessful treatment of primary endodermal sinustumor of the endometrium. Gynecol Oncol1988;31:357-64.2. Joseph MG, Fellows FG, Hearn SA. Primaryendodermal sinus tumor of the endometrium: aclinicopathologic, immunocytochemical, andstructural study. Cancer 1990;65:297-302.3. Dede M, Pabuccu R, Yagci G, Yenen MC,Gotktolga U, Gunhan O. Extragonadal yolk sactumor in pelvic localization: a case report andliterature review. Gynecol Oncol 2004; 92:989-91.4. Razzi S, Luisi S, Gabbanini M, Lazzeri L,Mazzini M, Petraglia F. Yolk sac tumor in ayoung girl: a case report. Gynecol Endocrinol2005;20:334-5.5. Zhang B, Gao S, Chen Y, Wu Y. Primary yolksac tumor arising in the pancreas with hepaticmetastasis: a case report. Korean J Radiol2010;11:472-5.6. Fujita M, Inoue M, Tanizawa O, Minagawa J,Yamada T, Tani T. Retrospective review of 41patients with endodermal sinus tumor of theovary. Int J Gynecol Cancer 1993;3:329-35.7. Pasternack T, Shaco-Levy R,Wiznitzer A,Piura B. Extraovarian pelvic yolk sac tumor casereport and review of published work. J ObstetGynaecol Res 2008;34:739-44.
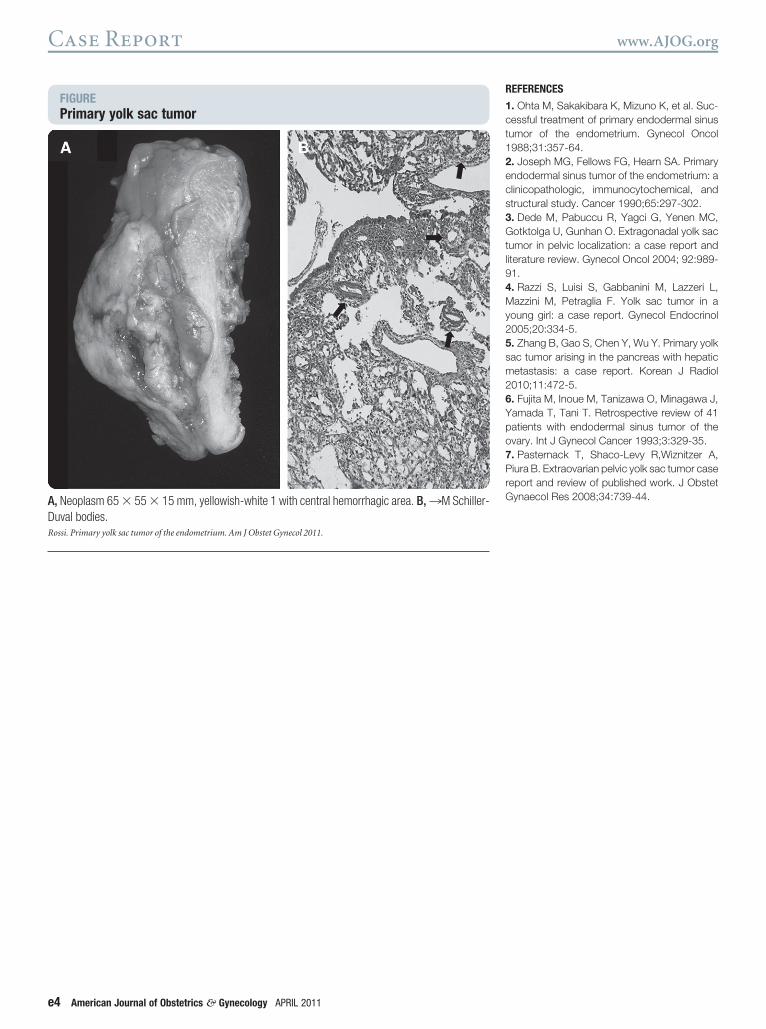
FIGUREPrimary yolk sac tumor
A, Neoplasm 65 � 55 � 15 mm, yellowish-white 1 with central hemorrhagic area. B, ¡M Schiller-Duval bodies.Rossi. Primary yolk sac tumor of the endometrium. Am J Obstet Gynecol 2011.