
Primary Systemic Therapy for Inflammatory Breast Cancer
23
Primary Systemic Therapy: Beginning the Journey Beth Overmoyer MD, FACP Director, Inflammatory Breast Cancer Program 1 st Annual IBC Patient Forum Dana Farber Cancer Institute May 13, 2017
-
Upload
dana-farber-cancer-institute -
Category
Healthcare
-
view
233 -
download
0
Transcript of Primary Systemic Therapy for Inflammatory Breast Cancer

Primary Systemic Therapy: Beginning the Journey
Beth Overmoyer MD, FACP
Director, Inflammatory Breast Cancer Program
1st Annual IBC Patient Forum
Dana Farber Cancer Institute
May 13, 2017

Historical Perspective of IBC
• The historical identification of IBC is important as a reminder of the acceptance of classic clinical criteria that differentiates the disease from other forms of locally advanced breast cancer
• 1814 – Sir Charles Bell described a grave prognosis associated with breast cancer when the following characteristics are present:• “when a purple color is on the skin over the tumor accompanied
by shooting pains it is a very unpropitious beginning”
• Lee and Tannenbaum (1924) – “inflammatory breast cancer”
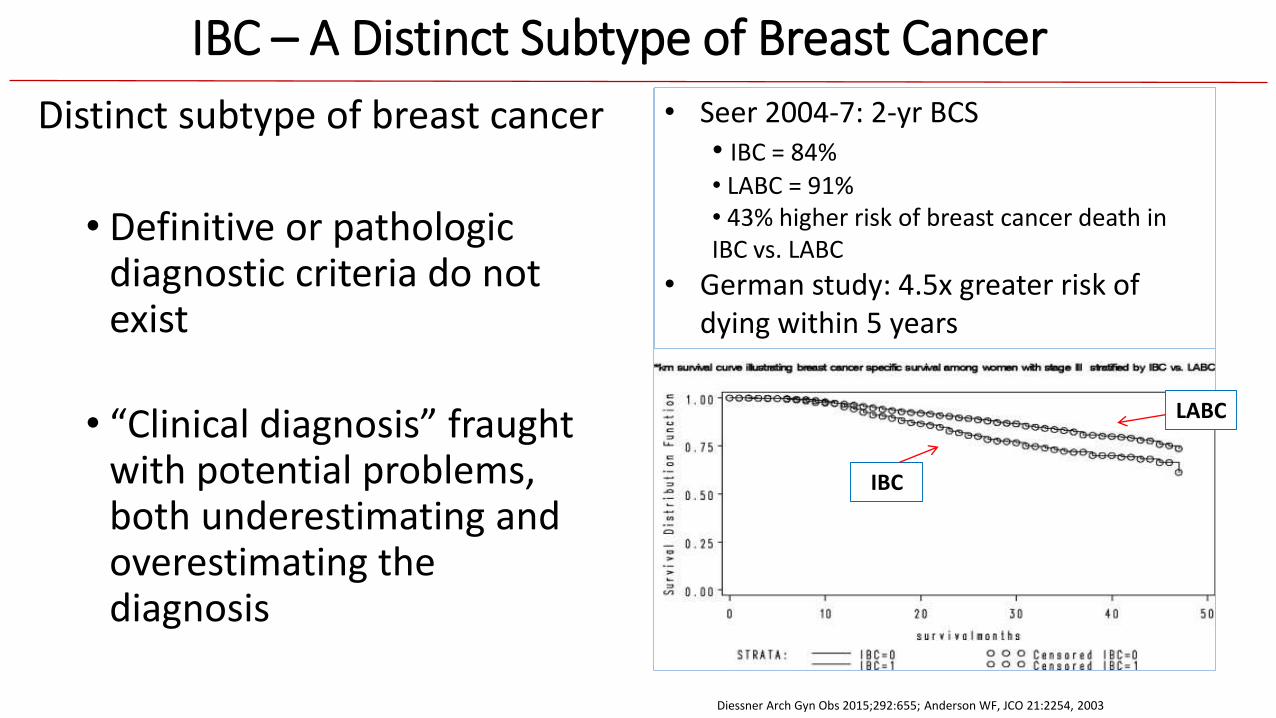
IBC – A Distinct Subtype of Breast Cancer
Distinct subtype of breast cancer
• Definitive or pathologic diagnostic criteria do not exist
• “Clinical diagnosis” fraught with potential problems, both underestimating and overestimating the diagnosis
• Seer 2004-7: 2-yr BCS • IBC = 84%
• LABC = 91%• 43% higher risk of breast cancer death in IBC vs. LABC
• German study: 4.5x greater risk of dying within 5 years
Diessner Arch Gyn Obs 2015;292:655; Anderson WF, JCO 21:2254, 2003
IBC
LABC
• 1-5% incidence in US
• Difficulty in tracking the disease due to variation in diagnostic criteria over time
• Underestimate incidence
Clinical definition with confirmed breast cancer: Rapid onset – 3 – 6 mo
• Erythema > 1/3 breast
• Edema (peau d’orange)
• Often warm breast, pain
• Breast enlargement – often without a mass
• Highly metastatic:
35% metastasis at presentation
Clinical Presentation - IBC

Clinical Diagnosis of IBC
• Tumor emboli in dermal lymphatics without classical signs is not considered IBC
• The presence of dermal lymphatic invasion is not necessary for the diagnosis of IBC

“Trimodality” Therapy: Importance of pCR
Primary Systemic Therapy
Mastectomy + Axillary LN Dissection
Radiation to Chest Wall and Regional LN
Adjuvant Endocrine Rx (HR+)+/or Trastuzumab (HER2+)
Nakhlis 2016
Overall survival
86%
51%
Time to tumor recurrence
79%
33%

Retrospective Studies of Preoperative Chemotherapy for IBC
No. IBC
Chemotherapy RR Median Survival
Italy 68 CAF or CEF / CMF pCR: 3% 4 yr.
U Penn 52 CMF +/- CAF pCR: 12% NR
France 120 FEC-HD pCR: 15% 5 yr.
British Columbia 308 CT v intensive CT (+ T) pCR:
28% v 33%
3.2 yr.
MD Anderson 240 FAC v FAC + T pCR:
10% v 25%
3.4 v 4.3 yr
Primary chemotherapy backbone = anthracycline and taxane

Dose-Dense versus Conventional Preoperative Chemotherapy (AGO-1) – Overall ≠ IBC
• 668 patients with locally advanced breast cancer • Overall group benefitted from intensive
chemotherapy:• Improved pCR – 18% vs 10%• Improved time to disease recurrence• Improved overall survival
Untch M JCO 2009; 27:2938
• 100 IBC • No difference with intensity of chemotherapy:
• No difference in pCR – 12% vs 10%• No difference in time to disease recurrence• No difference in overall survival
≠
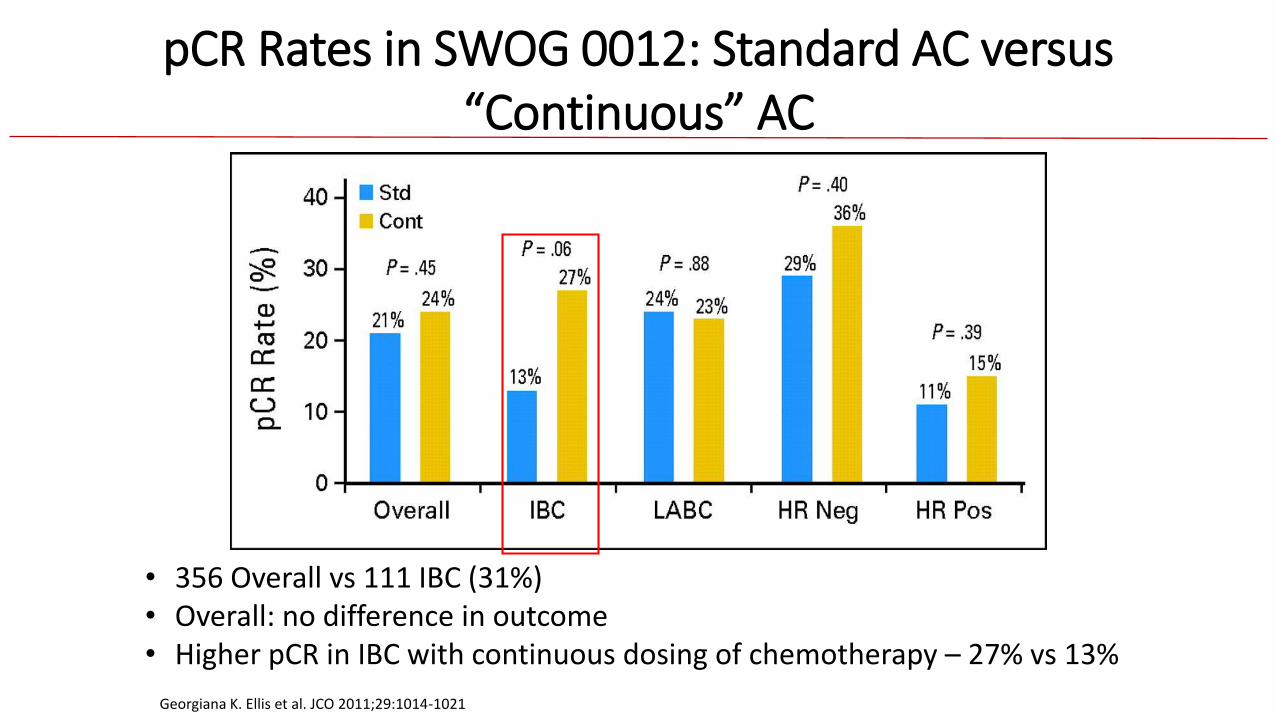
pCR Rates in SWOG 0012: Standard AC versus “Continuous” AC
Georgiana K. Ellis et al. JCO 2011;29:1014-1021
• 356 Overall vs 111 IBC (31%)• Overall: no difference in outcome• Higher pCR in IBC with continuous dosing of chemotherapy – 27% vs 13%

Finding Therapeutic Targets in IBC
•HER-2
•Angiogenesis
• JAK2-STAT3

Finding Therapeutic Targets in IBC
• Targeting HER-2
•Angiogenesis
• JAK2-STAT3

NOAH – IBC Experience
64% v 24%
74% v 44%
5-YR EFS
5-YR OS
Doxorubicin 60mg/m2 →
Paclitaxel 150mg/m2 q21d x 3
Paclitaxel 175mg/m2 q21d x 4
CMF x 3
Subset Analysis
• 61 / 228 pts with IBC, HER2+
• pCR = 48 % with trastuzumab
•13% without trastuzumab
Gianni L. Lancet Oncol 2014 15:640

Anti-HER2 Therapy
Trypheana (13/225 = 6% IBC)
FEC+HP x 3 →T+HP x 3 (N=73)
FEC x 3 → T+HP x 3 (N=75)
TCH+P x 6 (N=77)
IBC 5(7%) 4(5%) 4(5%)
tpCR 41(56%) 41(55%) 48(64%)
NeoSphere(29/417 = 7% IBC)
T+D (N=107) T+D+P (N=107) T+P (N=107) P+D (N=96)
IBC* 7 (7%) 10 (9%) 7 (7%) 5 (5%)
tpCR (all) 23 (22%) 42 (40%) 12 (11%) 17 (18%)
5y –DFS 81% 84% 80% 75%
Gianni Lancet Oncol 2012;13:25-32; Schneeweiss Ann Oncol 2013;2278-84; Gianni Lancet Oncol 2016; Gianni Lancet Oncol 2012; Boussen, JCO 2010; Untch Lancet Onc 2012.
Investigating lapatinib Regimen Number enrolled pCR
MDACC Lapatinib + paclitaxel
32 3/17 (18%)
GeparQuinto EC→D(L v H)
82/620 =13% IBC 23% v 30% (p=0.04) Odds ratio IBC = 0.72 (NS)

Run In Phase – Day 1 week 1 (breast biopsy #1)
Pertuzumab IV 840 mg loading dose Trastuzumab IV 4 mg/kg loading dose
Treatment Phase – Day 8 week 2 (breast biopsy #2)
Trastuzumab IV 2mg/kg weekly and paclitaxel 80 mg/m2 IV weekly x 16 weeks.
Day 21 week 4
Continue trastuzumab and paclitaxel as above and begin pertuzumab 420 mg IV every 21 days for 5 doses
Modified radical mastectomy
(assess residual disease)
Post-operative Treatment:
Doxorubicin 60 mg/m2 IV and cyclophosphamide 600 mg/m2 IV every 3 weeks x 4 cycles*
Followed by trastuzumab 6 mg/kg and pertuzumab 420 mg every 21 days x 8 months**(loading dose given first after AC completed)
Radiation TherapyEndocrine therapy if HR+
*Optional**Metastatic disease (nodal disease only): continue on pertuzumab + trastuzumab until disease progression
Primary Objective: pCR• Accept benefit if > 8/ 27
pts have pCR
NCI-2013-01110, NCT0179619712-497; Genentech, IBC Network - sponsor
Hypothesis:Can we limit the amount of chemotherapy and maximize the HER2-directed therapy in the treatment of HER2+ IBC ?

Finding Therapeutic Targets in IBC
• Targeting HER-2
•Angiogenesis
• JAK2-STAT3

Angiogenesis and Lymphangiogenesis in IBC• IBC makes its own blood supply and
lymphatic supply throughout the breast
• Increased expression of angiogenesis related genes
• Increased expression of lymphangiogenesis related genes
• Is this “encircling lymphovasculogenesis” or lymphovascular invasion ?
Colpaert CG, Br J Ca 2003;88:718; Van der Auwera Clin Can Res 2005;11:7637
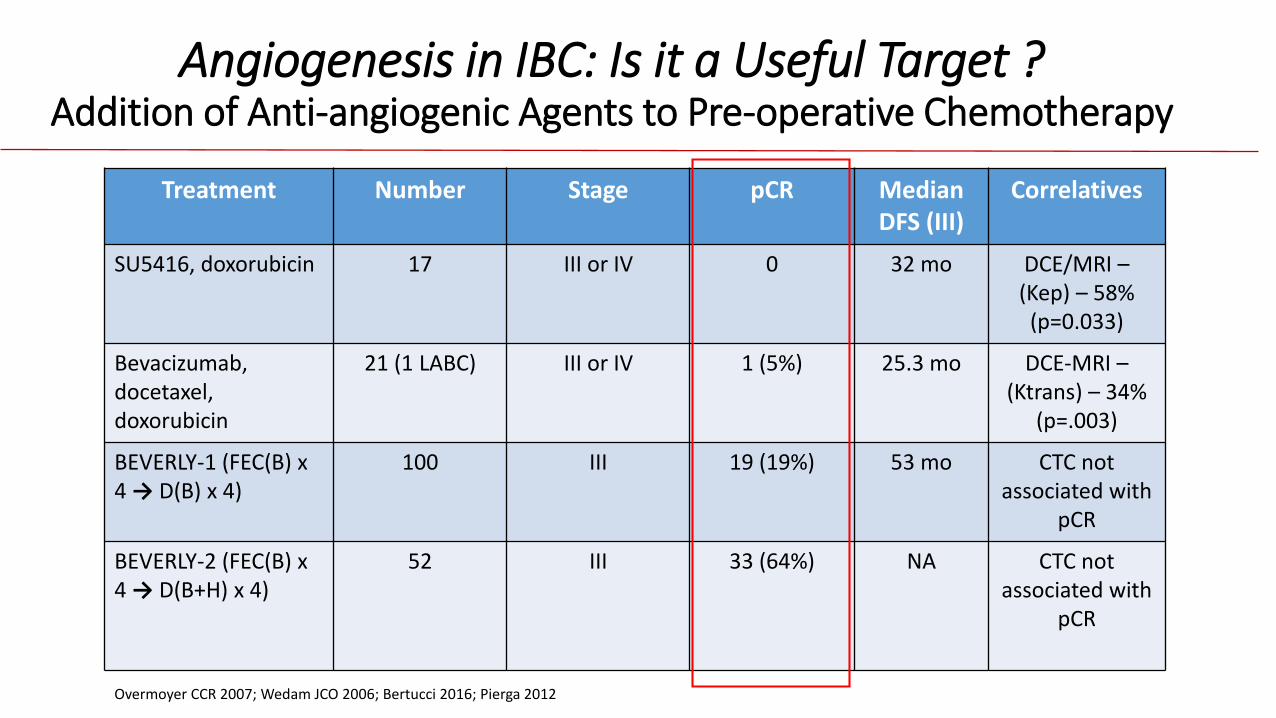
Angiogenesis in IBC: Is it a Useful Target ? Addition of Anti-angiogenic Agents to Pre-operative Chemotherapy
Treatment Number Stage pCR Median DFS (III)
Correlatives
SU5416, doxorubicin 17 III or IV 0 32 mo DCE/MRI –(Kep) – 58%
(p=0.033)
Bevacizumab,docetaxel, doxorubicin
21 (1 LABC) III or IV 1 (5%) 25.3 mo DCE-MRI –(Ktrans) – 34%
(p=.003)
BEVERLY-1 (FEC(B) x 4 → D(B) x 4)
100 III 19 (19%) 53 mo CTC not associated with
pCR
BEVERLY-2 (FEC(B) x 4 → D(B+H) x 4)
52 III 33 (64%) NA CTC not associated with
pCR
Overmoyer CCR 2007; Wedam JCO 2006; Bertucci 2016; Pierga 2012
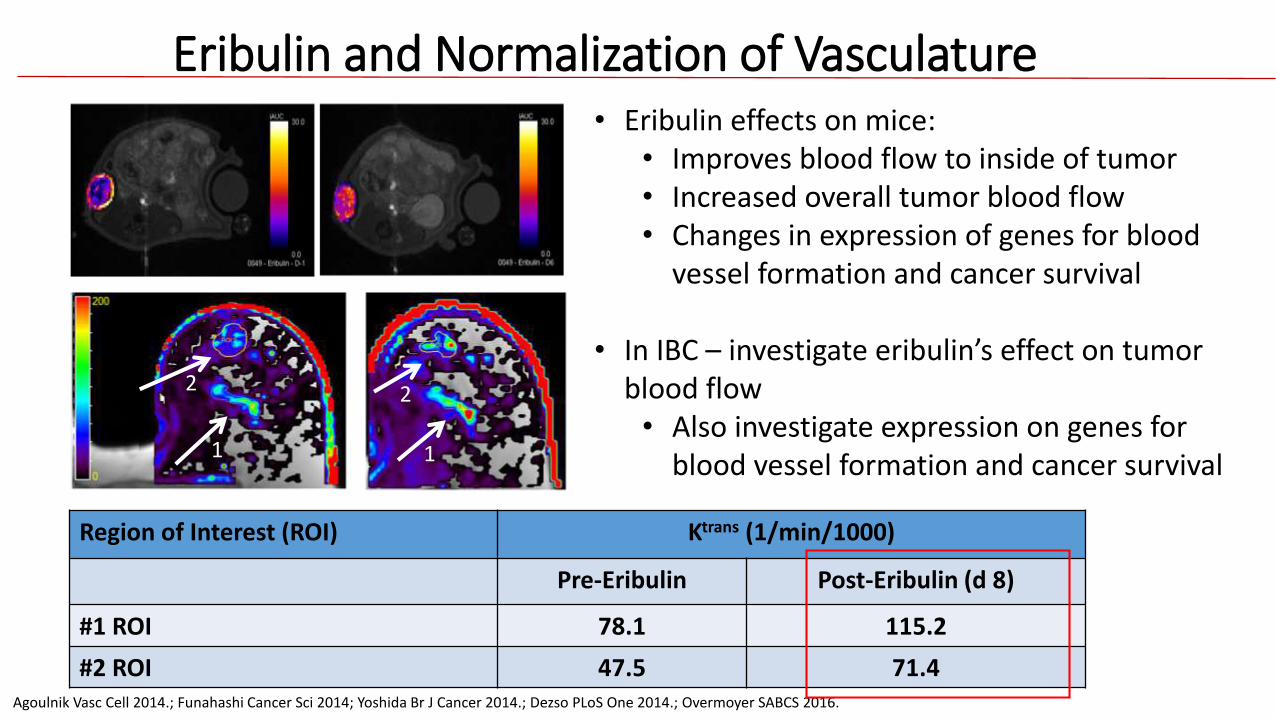
Eribulin and Normalization of Vasculature
Region of Interest (ROI) Ktrans (1/min/1000)
Pre-Eribulin Post-Eribulin (d 8)
#1 ROI 78.1 115.2
#2 ROI 47.5 71.4
• Eribulin effects on mice:• Improves blood flow to inside of tumor • Increased overall tumor blood flow • Changes in expression of genes for blood
vessel formation and cancer survival
• In IBC – investigate eribulin’s effect on tumor blood flow• Also investigate expression on genes for
blood vessel formation and cancer survival
2
1
Agoulnik Vasc Cell 2014.; Funahashi Cancer Sci 2014; Yoshida Br J Cancer 2014.; Dezso PLoS One 2014.; Overmoyer SABCS 2016.
2
1

Pre-treatment breast biopsy #1
Eribulin x 1 (cycle 1 day 1)
Breast biopsy #2: 1 wk after eribulin (cycle 1 day 8)
Eribulin q 3 wks x 3 cycles
dd AC q 2 wks x 4 cycles
Mastectomy (harvest residual tumor)
Radiation therapy + endocrine therapy
Imaging subset study
Pre-treatment breast DCE-MRI
1 wk after eribulin (c1,d8) breast DCE-
MRI
Eribulin 1.4mg/m2 IV
d1,d8 q21d x 4 cycles
Doxorubicin 60 mg/m2 +
cyclophosphamide 600 mg/m2 IV q2w x
4 cycles
Overview
• Primary Objective: pCR rate• Two-stage design:
• Reject if pCR is < 15%• Accept if pCR > 30%• > 2/16 pCR – go forward
• Accept benefit if > 5/ 25 pts have pCR
NCI-2016-00329, NCT0262397215-292; Eisai-sponsor

Finding Therapeutic Targets in IBC
• Targeting HER-2
•Angiogenesis
• JAK2-STAT3

Slides curtesy of Kornelia Polyak MD, PhD
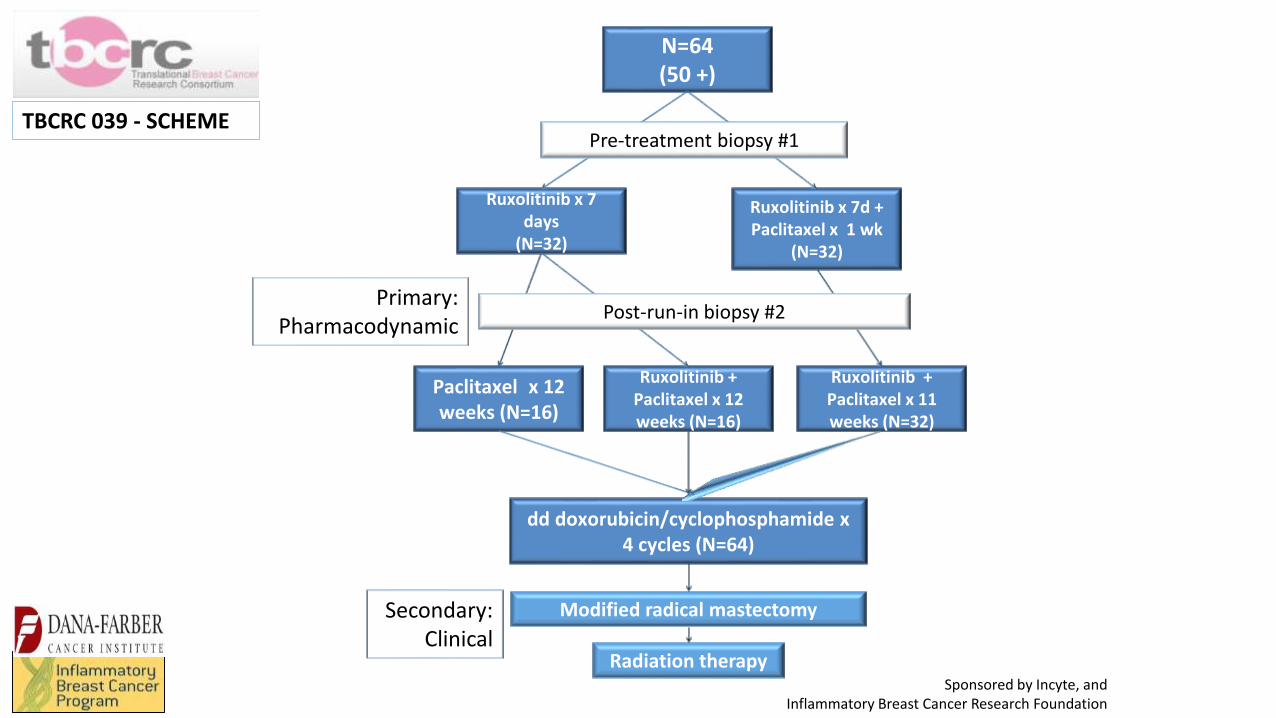
N=64(50 +)
Ruxolitinib x 7 days
(N=32)
Ruxolitinib x 7d + Paclitaxel x 1 wk
(N=32)
Paclitaxel x 12 weeks (N=16)
Ruxolitinib + Paclitaxel x 12 weeks (N=16)
Ruxolitinib + Paclitaxel x 11 weeks (N=32)
dd doxorubicin/cyclophosphamide x 4 cycles (N=64)
Modified radical mastectomy
Radiation therapy
Pre-treatment biopsy #1
Post-run-in biopsy #2Primary:
Pharmacodynamic
Secondary:Clinical
TBCRC 039 - SCHEME
Sponsored by Incyte, and Inflammatory Breast Cancer Research Foundation

Primary Systemic Therapy for IBC: Beginning the Journey
• IBC is inoperable at the time of diagnosis, therefore initial therapy with “systemic treatment” is indicated.
• IBC is relatively chemo-resistant, therefore identifying therapeutic targets is critical.
• We must focus our efforts on designing clinical trials specifically for IBC
• Inclusion of IBC patients into LABC trials will dilute the interpretation of outcome
• Incorporate translational components
• Identify biologic markers that confirm the diagnosis, not just rely on “clinical features” that are not consistent.


















