primary care strategy - hammersmithfulhamccg.nhs.uk€¦ · care home’ concept to become...
27
Hammersmith and Fulham’s primary care strategy Developing primary care as the foundation for better population health across the borough September 2017
Transcript of primary care strategy - hammersmithfulhamccg.nhs.uk€¦ · care home’ concept to become...

Hammersmith and
Fulham’s
primary care strategy Developing primary care as the foundation for
better population health across the borough
September
2017

# Chapter Page
1 Foreword – an introduction from Dr Tim Spicer and Dr David Wingfield 3
2 Our vision for an integrated health and social care system 4
3 Developing primary care at scale for the benefit of local residents – towards accountable care 9
4 Appendices
16
Purpose and content
This document describes how the CCG and GP Federation in Hammersmith and Fulham will work with each other and their partners to further develop
the standard of primary care for residents of the borough. We will do this by creating primary care networks which will work with other care services on
which our patients rely. This will provide the foundation for a more unified and co-ordinated care system for local people, which we describe as
‘accountable care’.
2

FOREWORD: Improving primary care to achieve better population health
Primary care in Hammersmith and Fulham is improving, based on what
local people have said about the need for more patient-centred care
closer to home.
What we have achieved so far:
• Access to doctor appointments seven day a week
• Access to primary care through digital technology, as local practices
trial smartphone apps.
• Access to many more services in primary care including enhanced
support for mental health, warfarin monitoring and more diabetic care
and support
• Improved investment in buildings: Parkview Centre for Health and
Wellbeing was completed in 2014 and now provides primary and
community care to more than 17,000 people.
What we need to do:
Primary care is a key force in delivering the following areas of the
Sustainability and Transformation Plan (STP):
• radically upgrading prevention and wellbeing
• eliminating unwarranted variation and improving the management of
long-term conditions
• achieving better outcomes and experiences for older people
.
3
1 2 3 4
This is what our local residents have told us they require from
primary care:
We want to harness the energy and ideas of people who deliver and
receive care in Hammersmith and Fulham to create a system that works
seamlessly for everyone in the borough.
Within the limited resources we have, we are aiming for steady but
material improvement over coming years. This will be based on
sustainable changes in how local GP Practices will work together and with
other health and care services.
The end result will be a local care system that uses the collected expertise
and compassion of all of our local care organisations to deliver the health
and wellbeing outcomes that we and our residents want.
Dr Tim Spicer
Chair, Hammersmith
and Fulham CCG
Dr David Wingfield
Chair, Hammersmith and
Fulham GP Federation
“I want to access care easily and in the way most
convenient for me, either in person or by using technology.
I want the range of people who provide my care to all work
together, communicate effectively, and have clear roles
that I understand. Together, they can provide me with
seamless care”

Our vision for care and the role of primary care in achieving it
We are ambitious for how good local primary care can be and how it can
help to build a truly integrated service for patients and rewarding careers
for staff.
Expectations for how primary care should develop are set out in London’s
Strategic Commissioning Framework (2014), the GP Forward View
(2016), and the Sustainability Transformation Plan (2016), which are
already resulting in change on the ground.
The way forward
General Practice has worked more collaboratively over the past few years
through the practice networks. In order to deliver population health
benefits and improved experiences of care we need to move to the next
stage. In the future, we want primary care to be better integrated with
social care, voluntary care and other community services (i.e. district
nursing, community independence service).
4
1 2 3 4
“I want my GP and his/her colleagues to be linked in closely to all the other people and organisations who
provide care for me and support me in other ways”
The way forward for Hammersmith and Fulham

Improvements will be based on understanding local residents’ needs
Source: NWL Local Services strategy 5
1 2 3 4

Our journey towards an integrated system known as ‘accountable care’
6
Stage 3: forming an MCP, with the extended networks as its delivery level
• Principles of joint working are well
established through integrated
community care teams
• There is clarity about local need and
local resources and agreements are in
place which facilitate local flexibility
• The integration of services around
people is extended across health and
social care
• Links with local charities are established
to increase the services available locally
• One person, one service, one team,
one budget approach
• Improved access to community
and specialist care
• Community-facing consultants
• Greater focus on driving better
health outcomes for local residents
with payment systems linked to this
• More services delivered closer to
the patient's home
• Practices are working in larger
established networks to provide
services at scale for the local
population
• Practices work towards
reducing variation and
unnecessary admissions
/referrals through an agreed
common set of outcomes and
quality standards
• A shared workforce across
practices is established that
allows a greater range of
services to be delivered in
primary care
• Practices work
together effectively
in local groups
• Multi-disciplinary
team (MDT) working
is established as
well as the sharing
of learning and best
practice
• Low level of cross
practice shared
services
• No shared workforce
1 2 3 4

What are aims are for our residents and workforce?
Stage 3: forming an MCP, with the extended networks as its delivery level
1 2 3 4
7
“People who have low care needs can be managed by other care professionals to give GPs more time to
care for people with complex needs”

New investment in primary care will support GPs to meet local needs by improving standards
Primary care in Hammersmith and Fulham has been historically under-funded, in comparison with other areas of the country.
This is now being rectified and over the next four years, the CCG will be receiving accelerated growth monies as shown in the table below:
2016-17 2017-18 2018-19 2019-20 2020-21 2016-17 – 2020-21
£24.9m £27.2m £28.8m £30.0m £31.1m + 25%
This provides an important opportunity to address current inequalities in care provision and therefore to improve population health outcomes.
The CCG and GP Federation will work with local people and other partners to develop a suite of primary care standards that it will expect to be met for
all patients in the borough.
The core standards will focus on improving:
• improving patients’ experience of care
• radically upgrading prevention and wellbeing
• eliminating unwarranted variation and improving the management of long-term conditions
• achieving better outcomes and experiences for older people and people with mental ill-health
• reducing the number of unnecessary admissions to hospital
• ensuring high quality services are delivered in primary care, in line with the requirements of the Care Quality Commission (CQC)
.
8
1 2 3 4

Developing Primary
Care at scale for the
benefit of local
residents – towards an
accountable care
partnership
9

The networks have made significant progress: we now need to stretch our ambitions further
Recruitment problems
and other workforce
issues mean that we
have no choice but to
work at greater scale –
that is the only solution.
Relationships are key to
making the networks
function properly – so
we need to make sure
that they continue to be
based around practices
that work well together.
As a small practice, we value our
independence and autonomy – and
we want to be able to preserve this
within larger groups.
Working at scale affords benefits
in terms of freeing up GPs’ time to
do clinical work by having a larger
team with a greater distribution of
skills (including business and
management skills).
Working in larger groups
needs to be able to
preserve the continuity of
care for those patients that
need it.
This primary care strategy builds on the network system to support
practices to work more closely both with each other at scale and with a
wide range of other services.
Building on the benefits of network collaboration
There are currently five networks in the borough.
The formation of networks was an important step in enabling practices to
provide better care that meets local people’s expectations.
Networks have:
enabled General Practice to see beyond the boundaries of their own
practices
established multi-disciplinary working across practices and the sharing
of learning and best practice. This directly benefits patients in terms of
the quality of care
We are now aiming to extend this collaborative way of working to fully
develop primary care networks, which are already being tested locally
and showing positive results around the country for patients, practitioners,
and their wider systems.
The role of the CCG and GP Federation is to lead this process so that the
benefits can be delivered as quickly and uniformly as possible.
Such collaboration has already been embraced by many practices. We
recognise that there is both value and challenge in working in larger
‘primary care networks’ – a snapshot of feedback from GPs is shown
opposite. We will work with GPs to ensure that the implementation of this
strategy reflects both their ambitions and concerns.
Source:
CCG Members’ Meeting,
27 April 2017
10
The focus needs to be on clinical
outcomes - without stipulating a
single operating model,
1 2 3 4
“My practice works with other organisations to support me to maintain my physical and mental wellbeing –
and to support me when I am ill”

Reinvigorating the existing GP networks with the principles of the ‘primary care home’ concept to become ‘Primary Care Networks’
The ‘primary care home’ concept preserves and
improves the features of general practice that many
patients and GPs value most:
an integrated workforce, with partnerships spanning primary care, secondary care,
social care, and the voluntary sector
provision of care to a defined, registered population of between 30,000 and 50,000
a combined focus on personalisation of care with improvements in population health
outcomes
aligned clinical and financial drivers through a unified, whole population budget with
appropriate shared risks and rewards
• a first point of contact for all new health needs
• person-centred and continuous lifetime care
• comprehensive care provided for all needs
within a local population
• co-ordination and integration of care where a
person requires special services or provision
from secondary or tertiary care
11
The ‘primary care home’ concept also sets out
principles and a series of practical ways in which the
networks in Hammersmith and Fulham can work:
• they are developed, implemented, and led by
providers
• initiatives are planned and implemented at a
deliverable scale
• staff become the drivers of positive change
• fosters collaboration across local systems
1 2 3 4
The primary care home model was launched by the National Association of Primary Care
(NAPC) and is based on improving joint working within and beyond general practice. The
model which was developed over more than a decade by clinicians around the country
provides GPs with the platform to drive the improvement of care right across the system.
The primary care home model implements change from within general practice, rather
than being overly prescriptive.
Primary care homes are designed around the needs of their local population and are
commonly characterised by the following four features:
Initially, fifteen sites across the country were chosen to test the principles of the primary
care home. There are now more than ninety. Appendix 3 provides examples of primary care
homes across the country and the benefits for patients, primary care teams and the wider
health and care system.
Hammersmith and Fulham GP Federation is a member of the NAPC’s community of
practice. Drawing learning from the ‘primary care home’ concept the GP Federation is
developing primary at scale across groups of local GP practices.

This way of working will benefit patients and primary care teams
1 2 3 4
12
WORKFORCE
INNOVATION
FINANCIAL SUSTAINABILITY
Workforce enhancement - practices can
address their workforce issues more
comprehensively than when working
alone, including recruiting for a wider
range of roles and across multiple
practices. This can improve retention by
allowing for more collaborative ways of
working such as improving clinical
processes.
More varied careers - GPs and nurses
can specialise if they wish, because there
is sufficient demand across multiple
practice lists. This allows people to
perform ‘to the top of their licence’ which
can help with recruitment and retention.
New structures for collaboration provide
more robust means of sharing learning
and best practice.
Broader multi-disciplinary teams that
brings together all expertise to deliver
better population health outcomes.
Practices can join forces to innovate
through investment in technology, as
care through digital care becomes more
effective over larger groups of people.
Patient records can be shared across
all practitioners involved in providing
care.
General Practice will be able to
influence change as they decide how to
collaborate and innovate, based on
their patients’ needs.
This may result in smoother pathways
from General Practice into a wider
primary care offer, as well as into social
care and voluntary services.
New service initiatives, based on the
needs of the networks’ registered
population.
Sharing back-office functions can
improve operational efficiency and
financially sustainability. It can also
free up GPs’ time to be spent with
patients.
Greater efficiency savings will be
realised through practices operating at
scale delivering centralised business
and clinical functions (i.e. patient
recalls)
£

Next steps
1 2 3 4
13
As explained previously the following steps will be undertaken to further improve care for local residents:
• Stage 1 as described previously involves the reinvigoration of existing General Practice networks to become primary
care networks
• Stage 2 brings primary care networks together into a unified approach to provide community based care – this will be
through the platform of a Multispecialty Community Provider (MCP); and
• Stage 3 adds acute services to the MCP for a co-ordinated, outcome- based borough-wide approach to all care – this is
accountable care.
Accountable care is our end-point ambition for Hammersmith and Fulham. This means continuing furthering our work in bringing services
together into a single, co-ordinated approach to deliver:
• high-quality care that is aligned to outcomes, for the whole population;
• good patient experience of health care; and
• cost-effective care, within the given budget.
The North West London Collaboration of CCGs have developed a ‘Provider Maturity Assessment’ tool which the CCG and GP Federation
will jointly use to understand the readiness of local primary at scale organisations to take on the delivery and leadership of community-based
care as part of an MCP and an Accountable Care organisation. Appendix 5 provides more detailed information on the ‘Provider Maturity
Assessment’ tool.
The GP Federation has been working towards accountable care since January 2016, when it led the establishment of the Hammersmith and
Fulham Integrated Care Programme. This is a partnership of four organisations committed to integrated healthcare: the GP Federation,
Imperial Healthcare Trust, Chelsea and Westminster Foundation Trust, and West London Mental Health Trust. The partnership is also
working with the council on a range of issues, including the extension of partnership working into adult social care.
“I have a clear say in how my care is delivered and can access different services by using my personal
budget”

Multispecialty Community Provider:
1 2 3 4
14
“As a patient with multiple health conditions, I would like to have all my health care providers to work together”
Hammersmith and Fulham will take learning from the MCP vanguards to understand the evidence base for different approaches. In
particular, it will seek evidence about how best to extend the MCP model from health care into adult social care and public health, both
of which are commissioned by the council. This is being done in a phased way in other parts of the country.
An MCP’s core aim is to build on the primary care networks to increase the breadth of services and depth of interventions delivered in
primary care and the wider community
There are a number of options for this, which range from:
• an alliance of relevant service providers with no new contractual arrangements (a virtual MCP)
• a more formal arrangement in which all relevant budgets, including core general practice, are put within a single contract. In this
case, GPs are able to reactivate their core contracts at the end of the MCP contract period.
Whatever decision local GPs make about their own contracts, the centrality of GPs to each primary care network means that they will
be a key voice within whatever organisational form underpins the MCP. The implications and opportunities for GPs under each MCP
model are described in more detail in ‘GP participation in a multispecialty community provider’ (NHSE, 2016). There is a link to this
document in Appendix 2.
Both options will bring together providers of care delivered in the community to decide how a unified budget for the care they provide
should be invested; in order to meet the outcomes set by commissioners.

An accountable care system brings together all local providers of care,
with primary care networks at its heart
1 2 3 4
15
“More of my care needs can be delivered within primary care, without the need to visit the hospital”
Primary care networks are the building blocks to establishing an MCP and then an accountable care system in Hammersmith and
Fulham. Accountable care will bring together the MCP with the acute and mental health trusts into a single budget for all care
commissioned by the CCG (and, potentially, from the local council as well).The importance of a single approach towards shared goals is
understood by all parties. The CCG, the GP Federation, and the other Integrated Care Programme partners began developing this
single approach over the period of May to July 2017, to confirm:
• shared goals, objectives and milestones (including developmental stages) for accountable care development
• the necessary workstreams to deliver the work
• the resources needs and timelines - Appendix 7 provides a high level delivery plan for the implementation of the strategy
The approach agreed will provide the development framework for accountable care, based on the stages shown below.
Vision and model Scope and impact Contractual analysis Financial analysis Contractual approach
Review Monitoring Contract Financial
framework Specification
April 2019
NHS England has recently published contractual guidance on Accountable Care Partnerships, a link to this publication can be found in
Appendix 2. The CCG will work with NHS England to incorporate this guidance into the development of its contracting approach for
accountable care. This will be done to ensure that local integration agreements reflect the national view; in terms of the level of integration
required between primary care and other services in order to deliver integrated care.

APPENDICES
16
o Appendix 1 - Glossary – acronym
and abbreviations
o Appendix 2 - Links to documents
referenced in this strategy
o Appendix 3 - Key benefits and results
from the primary care home test sites
o Appendix 4 - Examples of the
difference that the strategy will make
to patients’ experience of care
o Appendix 5 - Introduction to North
West London Collaboration of CCGs’
Maturity assessment tool
o Appendix 6 - Developing the optimum
network configuration for primary at
scale
o Appendix 7 - High level delivery plan
for the implementation of the strategy
o Appendix 8 - Local Engagement
undertaken for the development of the
strategy
o Appendix 9 - List of Hammersmith
and Fulham GP Practices

Appendix 1 – acronyms and abbreviations glossary Appendix 2 – links to documents referenced in this strategy
1
2 Five Year Forward View (2014) www.england.nhs.uk/wp-content/uploads/2014/10/5yfv-web.pdf
Transforming Primary Care in London: A Strategic
Commissioning Framework (2015)
www.england.nhs.uk/london/wp-content/uploads/sites/8/2015/03/lndn-prim-care-doc.pdf
NHS England’s publications on Accountable Care Models https://www.england.nhs.uk/publication/?filter-category=new-care-models
The GP Forward View (2016) www.england.nhs.uk/wp-content/uploads/2016/04/gpfv.pdf
NWL Sustainability and Transformation Plan (2016) www.healthiernorthwestlondon.nhs.uk/sites/nhsnwlondon/files/documents/nwl_stp_octob
er_submission_v01pub.pdf
GP participation in a multispecialty community provider (2016) www.england.nhs.uk/wp-content/uploads/2016/12/gp-participation-mcp-contract-5.pdf
Next Steps on the Five Year Forward View (2017) www.england.nhs.uk/wp-content/uploads/2017/03/NEXT-STEPS-ON-THE-NHS-FIVE-
YEAR-FORWARD-VIEW.pdf
‘Does the Primary Care Home make a difference? Understanding
its impact’ (2017)
www.napc.co.uk/control/uploads/files/1490953667~NAPC_Does_the_primary_care_hom
e_make_a_difference_March_2017.pdf
17
CCG Clinical Commissioning Group
GP General Practice / General Practitioner
MCP Multispecialty Community Provider
MDT Multi-Disciplinary Team
NAPC National Association of Primary Care
NHS National Health Service
PCH Primary Care Home
STP Sustainability and Transformation Plan
1 2 3 4

Appendix 3: Key benefits and results from the primary care home test sites
Evaluating the impact of the first primary care homes
The National Association of Primary Care (NAPC) has recently evaluated
the early impact of three of the primary care home test sites.
In line with the approach of fostering provider-led innovation designed to
meet the specific local needs, the sites have introduced a range of
initiatives.
The sites analysed are shown opposite.
The evaluation covered three perspectives relevant to
Hammersmith and Fulham:
1. the patient perspective – new services and better experience
3. the system perspective – impact on demand for other services
2. the practitioner perspective – satisfaction, recruitment, retention
The Beacon Medical Group
in Plymouth –
four practices covering
32,500 people
Thanet Health
Community Interest Company –
eighteen practices
covering 47,550 people
Larwood and Bawtry
practices in
South Yorkshire –
two practices covering
30,450 people
18
1 2 3 4

Appendix 3: The first primary care homes - exciting results for patients, GPs and other practitioners
The three primary care homes on the previous page have introduced a
range of new services to meet the needs of their combined practice
populations. Examples include:
• enhanced care home services, including ward rounds, medication
changes, and review of discharge summaries
• a new acute response team to safely manage unwell people outside
of hospital
• the reconfiguration of ‘virtual wards’ to involve community health and
the voluntary sector
• new roles for pharmacists within and beyond practices
• a collaborative flu campaign
• additional GP input into the redesign of care pathways, including for
dermatology and musculoskeletal conditions
Other initiatives in the pipeline include:
• hosting Citizens’ Advice clinics in practices, run by local volunteers
• providing social care clinics to reduce assessment waiting times;
reviewing clinical and non-clinical processes to identify opportunities
for improving productivity
Initiatives have been funded in a variety of ways – from existing CCG
budgets, by practices, and a combination of the two. In some cases, no
additional funding was required.
The patient perspective – new services and better experience The initial combined impact of these initiatives for the patient experience
looks promising, in terms of:
• shorter GP waiting times
• lower A&E attendances
• lower A&E admissions
• more appropriate medication regimes
• slower growth in referrals, demonstrating that more of people’s total
care needs are being accommodated within primary care
The information on this page is taken from ‘Does the Primary Care Home make a
difference? Understanding its impact’ (NAPC, 2017)
19
1 2 3 4

Appendix 3: The first primary care homes - exciting results
As part of the evaluation, GPs and their colleagues in the primary care
homes were surveyed about the difference that the new ways of working
have made to their professional lives.
Some of the main results were:
Beacon Medical Group:
• 87% of staff enjoy their job, compared to 61% in 2015
• 90% of staff speak positively of the practice when speaking to patients
or external colleagues, compared to 69% in 2015
Thanet Health Community Interest Company:
• vacancies for community nurses have fallen from 24 to 0 over the
PCH pilot
Larwood and Bawtry:
• 87% of staff feel that the primary care home way of working has
improved their job satisfaction
• 78% of staff over the three sites feel that the PCH model has
decreased or not added to their workload
Overall, the pilot sites reported that the PCH way of working had
activated staff – GPs and others – to become the drivers of positive
change.
The system perspective – impact on demand for other services.
The PCH initiatives have not yet been underway for long enough to
establish a definitive causal link between new ways of working and a
range of system metrics. However, the early results suggest some
exciting results are already being achieved. Across the three primary
care homes, these include:
• reduced A&E attendances and admissions
• reduced lengths of stay in hospital following care home admissions
• a slow-down in the growth rate of GP referrals
• waiting times for GP appointments
• prescribing savings
The report also quantifies the savings realised. In Thanet these were:
• c.£295,000 annual savings from a reduction of 14 A&E admissions a
week following the roll out of the Acute Response Team
• £27,000 expected annual savings from reduced A&E attendances by
cross-practice working to provide extended primary care access on
bank holidays, supported by the shared patient care record
• £165 per care home medication review from a pilot – extended
across the local care home population, this would equate to a
system saving of £216,000
These impacts on the patient experience, practitioner experience, and
system metrics are key means of delivering the triple aim ambitions set
out in the test sites’ local STPs – and the same is true locally.
The practitioner perspective - satisfaction, recruitment, retention The system perspective – impact on demand for other services
The information on this page is taken from ‘Does the Primary Care Home make a difference?
Understanding its impact’ (NAPC, 2017) 20
1 2 3 4

ROD SMITH: Age 53. Diagnosed with Schizophrenia aged 24. Lives with sister, but often sleeps rough especially when
drinking. Prescribed small dose of regular tranquiliser.
Currently: Anticipated benefits of Accountable Care:
• Has been discharged from follow up by psychiatrist
• Under care of Community Psychiatric Nurse (CPN) but frequently fails to
attend
• Rod feels he is a nuisance to his sister who works from home. He tries to get
out from under her feet and spends a lot of time wandering the area, smoking,
and sometimes sleeps rough for days or weeks at a time
• Rod sometimes forgets to take his medication. Over the years there have
been a couple of crises that have required urgent visits by a psychiatrist
• Rod doesn't like his current medication. His GP would like specialist advice on
an alternative but Rod is reluctant to visit the psychiatrist
• Rod seems to develop chronic bronchitis rather suddenly. The GP
recommends an urgent hospital investigation but knows that Rod is unlikely to
attend for all the necessary appointments
• CPN is available to see patients locally in one of the GP practices that forms
part of a small, local health and social care network, and can visit patients at
home when necessary
• The Primary Care Collaboration includes various local community
organisations. The CPN has referred Rod to a health and social care
coordinator. After a discussion Rod has joined a local allotment group and
finds he enjoys gardening. He has also joined an art group and smokes and
drinks much less
• The Primary Care Collaboration employs pharmacists who routinely monitor
repeat prescribing systems including Rod’s usage of medication. They can use
the shared computer system to leave messages for GP colleagues, the CPN
and to ensure that someone contacts Rod to check on his wellbeing
• The GP and consultant can both access Rod’s medical record and hold a
‘virtual clinic’ where they discuss the case by video link while both viewing the
record at the same time. They agree on a plan of action including a trial of a
modern medicine with fewer side-effects
• There is a multidisciplinary diagnostic service in the local hospital where the
staff includes GPs from Rod’s local GP network. A care navigator keeps him
informed as the day progresses with various investigations
• The chest specialist and GP compare notes and exclude a diagnosis of cancer.
They make a record in Rod’s clinical notes and agree with Rod that he will
attend for follow up with his GP rather than the hospital
Appendix 4: PATIENT EXAMPLE 1
Highlighting the benefits of accountable care for patients with mental heath needs
21
1 2 3 4

DANUTA KOWALSKI: Age 79. Widow. Lives alone. Suffers from diabetes, chronic kidney disease, high blood pressure and mild heart
failure. She has been admitted to hospital recently following some falls. She tries to help her struggling daughter with cash, leaving
her with little money of her own to feed herself properly.
Currently: Anticipated benefits of Accountable Care:
• A heart failure nurse visits Danuta at home, but sometimes Danuta needs to attend the
hospital for tests. She tries to combine visits to her GP for diabetes or blood pressure
review with days when her daughter is available. She can also usually co-ordinate her
hospital visits to the kidney specialist every three months to suit her daughter. She
sometimes misses her appointments
• Danuta frequently needs hospital admissions, for heart failure or worsening of her
kidney condition
• Currently, communication between health care professionals and social care is typically
in the form of letters
• There are frequent mix-ups over medication, when for example one of the specialists
recommends a change, but the letter arrives late at the GP surgery
• Danuta’s daughter is re-housed to another borough following the birth of her child, and
Danuta becomes increasingly isolated. A neighbour suggests she discuss the issue with
social services. She is offered a weekly visit to a day care centre but feels that would
not suit her
• Danuta’s daughter is increasingly pre-occupied and it becomes more difficult for Danuta
to access help or get equipment.
• Danuta sees a GP she has not seen before who is a little concerned to hear about
Danuta's financial support for the daughter. The GP is reluctant to trigger formal
safeguarding proceedings and takes no action.
• Local GPs and social services are combined in an integrated care service. The team is
based in one of the GP practices. The combined team ensures that the same, suitably
trained nurse can provide home visiting for all the various specialist needs in a single,
regular visit. The nurse can discuss Danuta’s case regularly with each of the specialists in
virtual clinics where both have access to the same, shared record system. Hospital visits
become less frequent
• An integrated team as well as shared records allows for better planning and anticipation of
crises, especially by making use of pharmacists who keep track of medication usage.
When crises do occur, they can usually be managed by a community support team that
visits Danuta several times daily including the use of mobile diagnostic equipment
• With health and social care combined in a single, local organisation, communication is
much easier using a shared record and regular meetings
• All the specialists involved have access to the GP record, and changes to medication are
more immediate. Also each integrated local care network will include pharmacists who
can regularly review prescribing and raise issues with the doctors or nurses involved.
• Integrated health and social care makes it easier for the nurse and social care to share
information. With more emphasis on prevention and with better communication, this
situation is anticipated much earlier, and a local housing solution is found which allows
Danuta’s daughter to continue providing some support
• Whenever help is required, it is accessed by a single phone call to the same number each
time. Danuta knows her care navigator very well, and since payments for equipment come
directly from a single, unified budget, personalised help and equipment can be accessed
much quicker
• The care navigator is able to connect Danuta to a local visiting service. One of their
volunteers is Polish and subsequently visits Danuta regularly to chat in her native
language
• The GP is very familiar with their social care colleagues who now work in the same team.
They are able to have an informal discussion and the nurse who visits feels able to raise
the issue with Danuta and her daughter and finds a solution that everyone is happy with
Appendix 4: PATIENT EXAMPLE 2:
Highlighting the benefits of accountable care for patients with multiple long term conditions
22
1 2 3 4

Appendix 5 – Introduction to North West London Maturity Assessment Tool
23
1 2 3 4
North West London Collaboration of CCGs are introducing a provider maturity assessment to evaluate
the willingness and capability of at scale primary care providers to deliver future population and
outcomes based contracts.

Appendix 6: Our delivery plans set out a demanding programme of work
24
2017/18 2018/19 2019/20 2020/21
GPFV implementation
Borough-wide primary care homes:
formation, mobilisation, innovation
Borough-wide primary care homes:
scaling and maturity
MCP
Accountable care Development and extension of
accountable care
Accountable care: launch planning
Network plan implementation
Primary care
standards:
development
Primary care standards: implementation
Implementation is under way
Plans included within the primary care strategy
Plans to be developed
Implementation state
Key
Accountable care: development and extension planning
SCF implementation
GPFV implementation
1 2 3 4

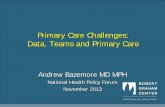
Appendix 7: Developing the optimum network configuration for primary at scale
The CCG and GP Federation are working with
practices to develop the current network system
into the best configuration for working at scale.
This will be completed by October 2017 and will
be based on a series of considerations, including
existing collaborative relationships, common
challenges, and an appropriate mix of practice
readiness to lead the transformation process.
The map on the right shows the current Network
configuration. The practice names for each
number can be found in Appendix 9.
25
1 2 3 4

Appendix 8 – Local engagement for strategy development
26
1 2 3 4
Stakeholders / Forum Dates
Hammersmith and Fulham GP Members Meeting 27th April 2017
Hammersmith and Fulham GP Members Meeting 7th June 2017
Patient Reference Group (which included representation from Healthwatch, the London Borough
of Hammersmith and Fulham (LBHF) as well as Community and Voluntary sector organisations)
15th June 2017
Practice Managers Forum 5th July 2017
Primary Care Strategy Patient Focus Group 10th July 2017
Hammersmith and Fulham GP Members Meeting 20th July 2017
Primary Care Strategy Patient Focus Group 27th July 2017
Hammersmith and Fulham CCG and GP Federation have undertaken clinical and public consultation into the
development of the primary care strategy. A series of engagement events were undertaken (including two patient
focus groups) in which discussions were held with GP members, local residents and other stakeholders to gain an
understanding of the improvements they want to see in General Practice and the wider health and care system in
future. The table below provides a list of local engagement events that were carried out.
The outputs from local engagement were useful and have informed the final iteration of the strategy. For example,
a request to see greater emphasis on mental health needs alongside physical health needs has been incorporated
into the strategy.

21 Dr Kukar, Parkview
22 Salisbury Surgery
23 Park Medical Centre
24 The Bush Doctors
25 Brooks Green Surgery
26 Dr Uppal and Partners, Parkview
27 North End Medical Centre
28 Ashchurch Surgery
29 Brook Green Medical Centre
30 Hammersmith & Fulham Centres for Health (two sites)
1 Canberra Old Oak Surgery
2 Ashville Surgery
3 Shepherd’s Bush Medical Practice
4 82 Lillie Road Surgery
5 Parkview Practice, Dr Canisius & Dr Hasan
6 South Fulham Health Clinic
7 Westway Surgery
8 Cassidy Road Medical Centre
9 Sterndale Surgery
10 Lillyville Surgery
11 Hammersmith Surgery
12 Fulham Cross Medical Centre
13 Dr Jefferies, 139 Lillie Road
14 Dr Jefferies, 292 Munster Road
15 Richford Gate Medical Centre
16 The Medical Centre (Dr Kukar)
17 Sands End Clinic
18 Palace Surgery
19 Fulham Medical Centre
20 The New Surgery
Appendix 9 – practice list
3
27
1 2 3 4