
Primary Care Panorama A 360 Degree Look at Primary Care 2015 Quality Forum Dr. Bill Cavers-...
37
Primary Care Panorama A 360 Degree Look at Primary Care 2015 Quality Forum Dr. Bill Cavers- President, Doctors of BC Dr. Brenda Hefford- ED,Practice Support and Quality, Doctors of BC Shana Ooms, Director, Primary Health Care,Ministry of Health Petra Pardy- ED Primary Care, Fraser Health
-
Upload
jarrett-spark -
Category
Documents
-
view
219 -
download
0
Transcript of Primary Care Panorama A 360 Degree Look at Primary Care 2015 Quality Forum Dr. Bill Cavers-...

Primary Care PanoramaA 360 Degree Look at Primary Care
2015 Quality Forum
Dr. Bill Cavers- President, Doctors of BCDr. Brenda Hefford- ED,Practice Support and Quality, Doctors of BCShana Ooms, Director, Primary Health Care,Ministry of HealthPetra Pardy- ED Primary Care, Fraser Health
Evidence for benefits of Primary Care:
“… helps prevent illness and death, regardless of whether the care is characterized by supply of primary care physicians, a relationship with a source of primary care, or the receipt of important features of primary care…associated with a more equitable distribution of health in populations.” - Barbara Starfield (2005)
“…available evidence confirms improved population health outcomes and equity, more appropriate utilization of services, user satisfaction and lower costs in health systems with a strong primary care orientation.” Atun R (2004) What are the advantages and disadvantages of restructuring a health care system to be more focused on primary care services? Copenhagen, WHO Regional Office for Europe

Primary Health Care Charter
“Family physicians are the cornerstone of Primary Health Care.
They are part of a broader community network and professional team…”

www.gpscbc.ca
• Ministry of Health Services + Doctors of BC• Operational rather than structural solutions • Input from Health Authorities
• Responsible for: - Care incentives (fee codes)- Practice Support Program (PSP)- Divisions of Family Practice- A GP for Me
“Finding solutions to support and sustain full service family practice in British Columbia”
General Practice Services Committee (GPSC)
www.gpscbc.ca
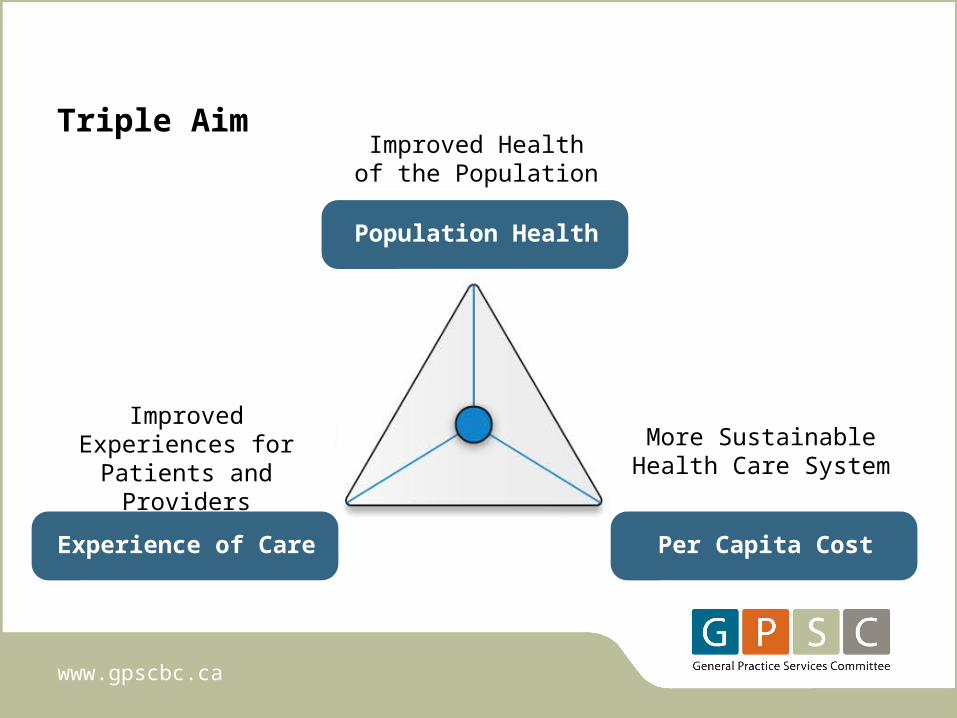
Experience of Care
Improved Experiences for Patients and
Providers
Per Capita Cost
More Sustainable Health Care System
Population Health
Improved Healthof the Population
Triple Aim

www.gpscbc.ca
• Chronic Disease Management (CDM)
• Conferencing fees
• Complex Care Initiative
• Maternity Network Initiative
• Mental Health Initiative
Family Practice Incentive Program
7
Evidence from BC
“…the more higher-care-needs patients were attached to a primary care practice, the lower the costs were for the overall health care system (for the total of medical services, hospital services, and drugs).
The majority of the cost reductions stemmed from decreases in the costs of hospital services.”
- Marcus HollanderHealthcare Quarterly, Vol 12 no 4, 2009
Learning modules: Advanced Access/Office Efficiency, Group Medical Visits, Practice Self-Assessment
Adult Mental Health
Child and Youth Mental Health
Chronic Disease Management
End of Life
Advanced Care Planning
Shared Care - COPD/Heart Failure
Practice Coaching
Practice Support Program

• Formed in 2006 (PMA)
• Mandate to provide funding and project support to family
physicians and specialist physicians to improve the flow of patient
care from primary to specialist services.
• Works closely with the other collaborative committees; the GPSC
and SSC
• has helped more than 2,500 family physicians and 240 specialist
physicians to work together on over 240 projects across BC.
www.sharedcarebc.ca
Shared Care Committee

Partners in Care (PIC)
Transitions in Care (TIC)
Polypharmacy
Rapid Access to Psychiatry
Teledermatology
Youth Transitions
Child and Youth Mental Health Collaborative (CYMHC)
www.sharedcarebc.ca
Shared Care Committee

• Improve patient care
• Increase family physicians’ influence on
health care delivery and policy
• Provide professional satisfaction for
physicians
www.divisionsbc.ca
Doctors of BC
MoHMinistry of Health
PMAPhysician Master
Agreement
GPSCGeneral Practice
Services Committee
DoFPDivisions of Family
Practice
Divisions of Family Practice was founded to:

Local Divisions of Family Practice are community-based groups of family physicians working together to achieve common health care goals.

A new way of working together
GP
Doctors of BC
Health Authorities
GP
GP
GP
GP
GP
MoH
Divisions
HealthAuthority
Doctors of BC
Municipalities Community Groups Non-profit Societies
Results
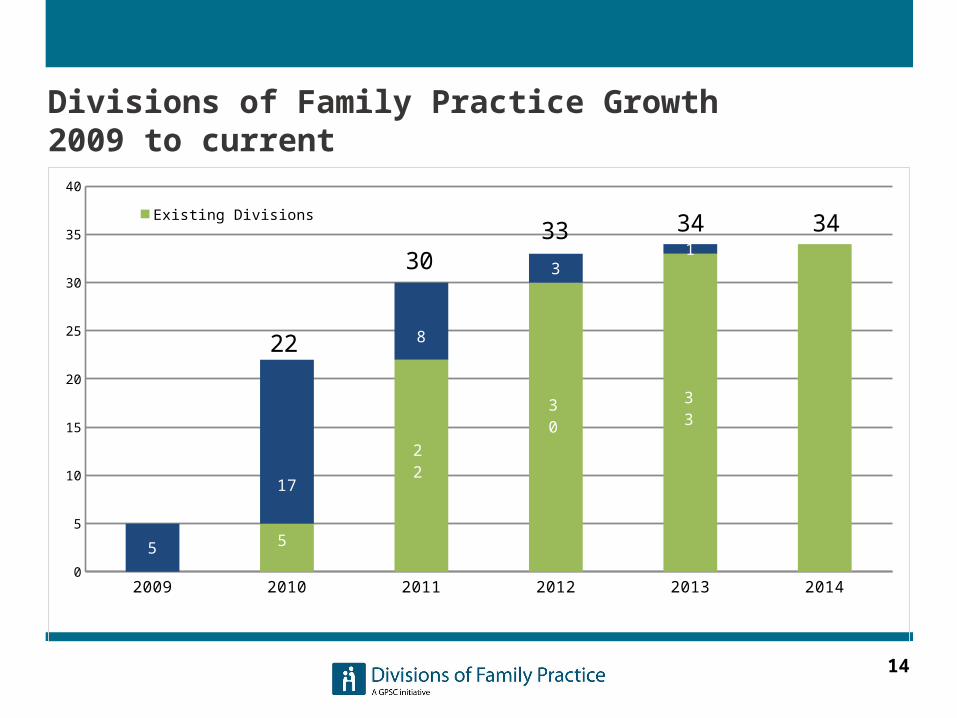
Divisions of Family Practice Growth 2009 to current
14
2009 2010 2011 2012 2013 20140
5
10
15
20
25
30
35
40
5
17
8
31
Existing Divisions New Divisions
22
3033 34 34
5
22
30 33

Promoting Clinical Integration Through Collaborative Services Committees
Chilliwack Primary Care Seniors Clinic
Home Health Integration in White Rock-South Surrey
Residential Care Program in South Okanagan Similkameen

16
Attachment Initiative: Three prototype communities
17
A province-wide initiative funded jointly by Doctors of BC and the Government of BC to strengthen the primary care system

18
Goals of A GP for Me
• Enable patients who want a family physician to find one
• Strengthen and support the family doctor - patient continuous relationship, including better support for vulnerable patients
• Increase capacity of the primary health care system
19
Multi-pronged approach
1. Physician practice level incentive fees
2. Community patient attachment strategies through Divisions of Family Practice
3. Integration, alignment, and leveraging of existing health authority, ministry, joint clinical committees, and partner initiatives, programs and policies
4. Patient and public engagement and education

Practice Level - attachment incentives
Four new family physician fees.The fees are for:
• Attaching unattached patients with complex health needs;
• Managing the care of frail patients;
• Providing patient care over the telephone for all patients;
• Conducting conferences with other health care providers for all patients.
20

Practice level results to date*
3,101 family physicians have ‘signed-up’ to participate in A GP for Me locally via their Division of Family Practice.
• 75% of full service family physicians.
More than 415,000 patients have received attachment related services
$31.0 million has been paid for these services
*Based on services from April 1, 2013 to December 31, 2014, paid to December 31, 2014

22
Community supports:Local divisions of family practice
$40 million over three years to:
• Engage and assess: community and patient needs, local family doctor needs, strengths and gaps in local primary care resources
• Develop and implement community plans for improving local primary care capacity, including finding doctors for patients who want one

23
Principles and Funding Parameters
1. Contribution to A GP for me Goals
2. Patient Centred
3. Accountable
4. Quality Improvement Oriented
5. Locally based and community developed
6. Collaborative
24
Principles and Funding Parameters
7. Aligned with regional and provincial
strategies and initiatives
8. Contribute to integration
9. Comprehensive (promoting generalism and
full scope of practice)
10. Sustainable• www.divisionsbc.ca; http://agpforme.ca/;
www.gpscbc.ca/attachment-initiative

25
Key Community Strategies
• Physician retention and recruitment
• Practice Efficiency and Clinical Improvement Supports
• Inter-professional team based care
• Public Education and Health Promotion
• Attachment mechanism
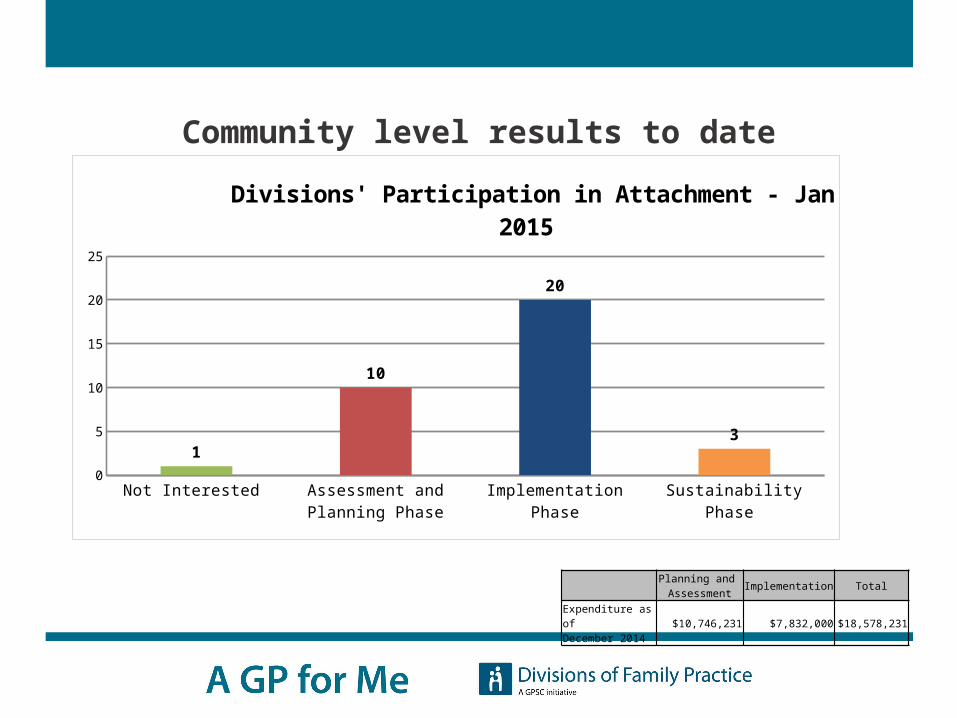
Community level results to date
Not Interested Assessment and Planning Phase
Implementation Phase Sustainability Phase 0
5
10
15
20
25
1
10
20
3
Divisions' Participation in Attachment - Jan 2015
Planning and Assessment Implementation Total
Expenditure as ofDecember 2014 $10,746,231 $7,832,000 $18,578,231

27
Integrate and Navigate Primary and Community Care - Supporting Frail
Seniors 1. Creation of meaningful
connections between clients’ GPs and case managers.
2. The expansion of the care management team to include a Surveillance Nurse (SN) and a client services assistant (CSA) .
3. Incorporation of the CARE Management approach into daily practice by Case Managers and the SN
28
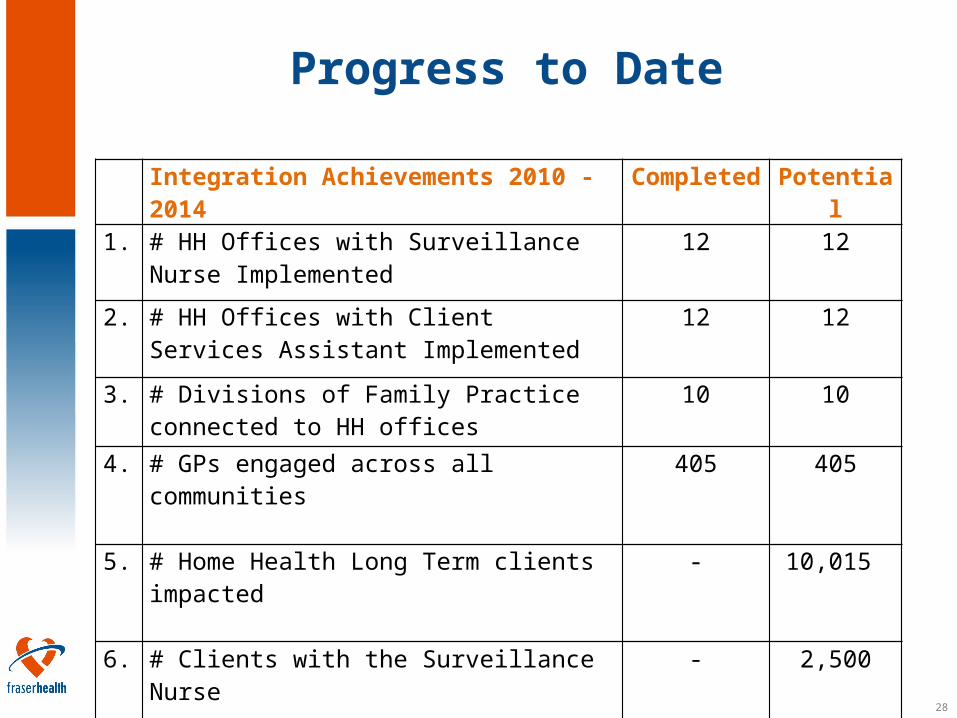
Progress to Date
Integration Achievements 2010 - 2014
Completed
Potential
1. # HH Offices with Surveillance Nurse Implemented
12 12
2. # HH Offices with Client Services Assistant Implemented
12 12
3. # Divisions of Family Practice connected to HH offices
10 10
4. # GPs engaged across all communities
405 405
5. # Home Health Long Term clients impacted
- 10,015
6. # Clients with the Surveillance Nurse
- 2,500

29
Impact of the Surveillance Nurse
on Client Outcomes Clients with the Surveillance Nurse (SN)
are 3.2 times more likely to survive in the community than clients not with the SN.
Clients who are with the SN and who are contacted more frequently by the SN, survive for longer in the community.
A CARE Management approach appears to delay death or transition to AL /RC.

30
Survival In the Community(SN vs non-SN clients, N=590)

31
Survival In the Community(Total N= 954)
Clients who were seen less frequently by SN ( who had 1 or 2 RVs n=408)
Clients who were seen morefrequently by SN ( who had 3 or more RVs n=546)
Days between initial call from SN to any adverse event (AL, RC or
Death)
32
Added Value & Impact
1. Case Manager – GP Connections:
“This is the missing link..” Surrey Case Manager
“I met (Case Manager) last week. It was one of the most productive 20 minutes I’ve spent in medicine. She had a list of my patients on her books. We decided on the best way to contact each other quickly…(This initiative) is a wonderful positive example of the new relationship between MOH, BCMA & HA’s. When something is so right for your patients, it’s obvious” Dr. Ralph Jones (Chilliwack Family Physician / President, SGP)
“Very efficient use of my time, a no-brainer.” Dr. Robert Hepburn, Surrey Family Physician

33
Success Factors
Relationships• Doctor/ patient
• Members of the health care team
• GPs and specialists, multi-disciplinary providers, system planners, administrators, community
• Patients and families, as partners
Orca Pod Pacific Coast, British Columbia

34
Success factors
Shared Perspectives
• Shared vision
• Common ground
• Flexibility, adaptable
• Bottom-up
• Stimulating for all
It is not the answer that enlightens, but the question.Eugene Ionesco Decouvertes British Columbia
Coastal Rain Forest
“”

35
Success Factors
Annual Polar Bear Swim, Pacific Coast, British ColumbiaPhoto: Mark Klotz, Vancouver, BC
Courage
• Unfamiliar territory
• Letting go of old ways
• Okay to fail and learn
• Trust in the process
• Open to new possibilities

If you want to travel fast, travel alone.
If you want to travel far, travel together.
“
”
West Coast Trail,Vancouver Island, British
Columbia

37
Section Title goes hereSection 3
An initiative of the GPSC, funded by Doctors of BC and the Government of BC
Thank you!


















