HIV Screening: A Guide for Primary Care Providers Updated November 2013 1.

- Created March 2011 - Revised August 2015
Primary Care Guidelines
for the Management of HIV/AIDS
in British Columbia
On behalf of the Primary Care Guidelines Panel
BC Centre for Excellence in HIV/AIDS
August 2015

2
TABLE OF CONTENTS
Acknowledgements ..................................................................................................................................... 4
Introduction ................................................................................................................................................. 6
Objectives..................................................................................................................................................... 6
Methods ........................................................................................................................................................ 6 Table 1. Strength of Recommendation Taxonomy .............................................................................. 7 Glossary of Abbreviations ................................................................................................................. 8
Summary of Primary Care Recommendations for the Management of HIV/AIDS ........................... 10
I. Background ........................................................................................................................................ 19 Table 2. Methods of HIV Transmission ............................................................................................ 19 Figure 1. Natural History of HIV/AIDS ............................................................................................ 20 Figure 2. Sequence of appearance of laboratory markers for HIV-1 infection ................................. 22 Figure 3. Current algorithm for EIA or ELISA screening in British Columbia ................................ 23
II. Medical History and Physical Examination of HIV-Positive Individuals ................................... 26
III. HIV Disease Specific Testing ......................................................................................................... 28 Table 3. HIV Disease Specific Tests ................................................................................................. 31
IV. Screening And Immunization For Selected Co-Morbid Infections ............................................. 33 Table 4. Recommended Vaccines for HIV-positive Adults .............................................................. 44 Table 5. Vaccines provided free of charge to HIV-positive adults in British Columbia ................... 49
V. Schedule of Care for HIV-positive Individuals .............................................................................. 56 Table 6. Laboratory Monitoring ........................................................................................................ 57
VI. Special Consideration for Women and Transgender† Individuals with HIV ............................. 60
Table 7. Hormonal Contraceptives and ARV Interactions ................................................................ 65
VII. Common Non-Infectious Co-Morbidities ..................................................................................... 71 Table 8. Recommendations for cancer screening in HIV-positive individuals ................................. 82
VIII. Optimizing Adherence to Antiretroviral Therapy ..................................................................... 87
IX. Special Consideration for HIV-positive Individuals with Addictions ......................................... 89
X. Special Consideration for Individuals with Advanced HIV – Opportunistic Infection &
Prophylaxis ................................................................................................................................................ 92 Table 9: Prophylaxis to prevent first episode of opportunistic disease, and criteria for when to
discontinue or restart primary prophylaxis for adults and adolescents with HIV infection ............... 93
XI. Psycho-Social Implications of HIV Infection ................................................................................ 95 Table 10: Other Guidelines related to the care of HIV-positive individuals ................................... 100
Contact List ............................................................................................................................................. 105
Appendices ............................................................................................................................................... 106

3
EXPERT COMMITTEE MEMBERS
Rolando Barrios, MD, MCFP, FRCPC (Co-Chair)
Assistant Director, BC Centre for Excellence in HIV/AIDS;
Clinical Assistant Professor, School of Population and Public Health, University of
British Columbia;
Associate Member, Division of AIDS, Department of Medicine, University of British Columbia.
Silvia Guillemi, MD, MCFP (Co-Chair)
Clinical Associate Professor, Department of Family Practice,
Faculty of Medicine, University of British Columbia;
Director of Clinical Education, BC Centre for Excellence in HIV/AIDS;
Assistant Medical Director, Immunodeficiency Clinic, St. Paul's Hospital;
Linda Akagi, BSc Pharm, ACPR
Pharmacist, Pharmacy Department, St. Paul’s Hospital.
Marianne Harris, MD, CCFP
Clinical Assistant Professor, Department of Family Practice,
Faculty of Medicine, University of British Columbia;
AIDS Research Program, St. Paul's Hospital.
Martin Payne, NP (F), MScN, LLM
Nurse Practitioner, Dr. Peter AIDS Foundation.
Peter Phillips, MD, FRCPC
Clinical Professor, Division of Infectious Diseases, University of British Columbia; Department Head, Division of Infectious Diseases;
St. Paul’s Hospital & University of British Columbia.
Neora Pick, MD, FRCPC
Medical Director, Oak Tree Clinic, B.C. Women and Children’s Hospital;
Associate Professor, Division of Infectious Diseases;
Department of Medicine, University of British Columbia & Oak Tree Clinic.
Jonathan Postnikoff
Treatment Outreach Coordinator, Positive Living Society of British Columbia.
Aida Sadr, MD CCFP
Physician, Vancouver Native Health Clinic;
Clinical Associate Professor, Urban Health Infections Unit, St. Paul’s Hospital.
Research Assistants Stephanie Donovan, MPP
Research Assistant, BC Centre for
Excellence in HIV/AIDS
Helen Kang, MSc, PhD
Clinical Educator, BC Centre for Excellence
in HIV/AIDS

4
ACKNOWLEDGEMENTS
We would like to acknowledge the following external medical experts who were consulted
during the revising of the Guidelines:
Matthew Bennett, MD, FRCPC (Cardiologist, Vancouver Coastal Health Research
Institute)
Greg Bondy, MD, FRCPC (Physician, Immunodeficiency Clinic/Health Heart Program,
St. Paul’s Hospital)
Mark Hull, MD, MHSc, FRCPC (Researcher, HIV/AIDS Research Program, St. Paul’s
Hospital)
Mel Krajden, MD, FRCPC (Associate Medical Director, Laboratory Services, BC Centre
for Disease Control)
Janice Leung, MD, FRCPC (Respirologist, Centre for Heart Lung Innovation, Division of
Respirology, St. Paul’s Hospital)
Deborah Money, MD, FRCSC (Executive Director, Women’s Health Research Institute;
Vice President of Research, BC Women’s Hospital and Hospital Centre, Provincial
Health Services Authority)
Natasha Press, MD, FRCPC (Clinical Associate Professor, Division of Infectious
Disease, University of British Columbia, Vancouver, BC)
We would also like to acknowledge the External Review Panel of community physicians,
pharmacist, nurse, and nurse practitioners from across B.C.
Christopher Collins, MB BS (MD) (Family Physician, The Medical Arts Centre,
Nanaimo, B.C.)
Jennifer Hawkes, BSPharm, ACPR, AAHIVP (Clinical Pharmacy Specialist, Northern
Health Pharmacy Department, University Hospital of Northern B.C. & Blood Borne
Pathogens Services, Northern Health, Prince George, B.C.)
Eliza Henshaw, NP (Nurse Practitioner, Raven Song Community Health Centre,
Vancouver, B.C.)
Liz Kirkpatrick, RN (Registered Nurse, Immunodeficiency Clinic, St. Paul’s Hospital,
Vancouver, B.C.)
Laura Knebel, MD (Family Physician, Downtown Community Health Centre,
Vancouver, B.C.)
Dharma McBride, MD (Family Physician, Kootenay Medical Centre, Nelson, B.C.)
Tanya Petryk, NP(F) (Nurse Practitioner, Sunshine Wellness Centre, Campbell River,
B.C.)
Andrea Szewchuk, MD (Family Physician, Catherine White Holman Wellness Centre,
Vancouver, B.C.)
Marria Townsend, MD, CCFP (Family Physician, Catherine White Holman Wellness
Centre and Three Bridges Community Health Centre; Medical Coordinator, Trans
Specialty Care, Vancouver Coastal Health, Vancouver, B.C.)

5
Monika Naus, MD, MHSc, FRCPC, FACPM (Medical Director, Immunization Programs
& Vaccine Preventable Diseases Service, BC Centre for Disease Control; Associate
Professor, School of Population and Public Health, University of British Columbia)
James Johnston, MD, FRCPC (Respirologist and Evaluation Lead, TB Service, BC
Centre for Disease Control; Clinical Assistant Professor, Department of Medicine,
University of British Columbia)

6
INTRODUCTION
There has been a significant decrease in the morbidity and mortality of HIV-positive individuals
in the province of British Columbia since the introduction of potent antiretroviral treatment in
1996. According to the Public Health Agency of Canada’s most recent estimates using data from
2011, there are approximately 11,700 (ranging from 9,400-14,000) HIV-positive individuals
living in British Columbia.1 Among them, approximately only 6,750 were receiving
antiretroviral treatment in 2015.2
In response to the need to expand HIV treatment and requests from the larger community of
primary care providers for HIV-specific guidelines, the British Columbia Centre for Excellence
in HIV/AIDS (BC-CfE) has developed these guidelines to support care and treatment programs
for people living with HIV.
OBJECTIVES
1. To provide consensus guidelines for the management of HIV-positive individuals in the
primary care setting.
2. To provide flow-care sheets based on the guidelines that can be used as an electronic or
paper-based template.
METHODS
Committee Composition
An expert committee composed of primary care and infectious disease physicians, a nurse
practitioner, a pharmacist, and a person living with HIV prepared these guidelines.
Process Overview
In 2014/15, the committee collectively undertook a review of the 2011 guidelines. Where
applicable, committee members added new evidence up to December 2014 and revised or added
new recommendations. Changes to the guidelines are highlighted in yellow throughout the
document and summarized in the “Summary of Changes in the 2015 Update.”
Consensus Development on the Basis of Evidence
The committee met a total of seven times. Committee members developed sections, in
consultation with external medical experts where appropriate, and presented their work at
committee meetings, where all recommendations were discussed until consensus was reached.
The final report manuscript was reviewed by all committee members as well as by external
review panel of primary care providers to ensure applicability prior to dissemination.

7
Table 1. Strength of Recommendation Taxonomy (SORT) [adapted from Ebell 2004]3
Assessment Type of Evidence
Strength of Recommendation
Grade A Consistent, good quality patient-oriented evidence
Grade B Inconsistent or limited quality patient-oriented evidence
Grade C Consensus, disease-oriented evidence, usual practice, expert opinion, or case
series for studies of diagnosis, treatment, prevention, or screening
Quality of evidence
Level I Evidence from at least 1 properly designed randomized, controlled trial
Level II Evidence from at least 1 well designed clinical trial, without randomization;
from cohort or case-controlled analytic studies (preferably from >1 centre);
from multiple time series; or from dramatic results of uncontrolled experiments
Level III Evidence from opinions of respected authorities, based on clinical experience,
descriptive studies, or reports of expert committees
Conflicts of Interest
Panel members were asked to report any conflicts of interest. Aida Sadr, Martin Payne, Jonathan
Postnikoff, and Linda Akagi have no conflicts to disclose.
Disclosures: Rolando Barrios has received speaking honoraria from Gilead Sciences, Inc.
Marianne Harris has received grants for research support, honoraria for advisory board
participation and/or speaking engagements, and/or other honoraria from AbbVie, Bristol-Myers
Squibb Canada, Gilead Canada Inc., GlaxoSmithKline, Janssen Inc., Merck Canada Inc., Vertex
Pharmaceuticals, and ViiV Healthcare. Neora Pick has participated in advisory boards for
Janssen, Abbvie, Merck, and Gilead, and received research funding from CIHR. Peter Phillips
has received honoraria or participated in advisory boards for the following companies: Pfizer
Inc., Janssen Pharmaceutical Schering-Plough, Fujisawa, Merck, and Astellas. Silvia Guillemi
has received honoraria for advisory board participation, other honoraria, and/or consultancies
including speaking engagements for Bristol-Myers Squibb, Gilead, Merck, Janssen and ViiV.
References
1. Public Health Agency of Canada. HIV/AIDS Epi Updates: National HIV Prevalence and Incidence Estimates
for 2011. Centre for Communicable Diseases and Infection Control, Public Health Agency of Canada, 2014.
Available from: http://www.phac-aspc.gc.ca/aids-sida/publication/epi/2010/pdf/EN_Chapter1_Web.pdf
2. BC Centre for Excellence in HIV/AIDS. B.C. HIV/AIDS Drug Treatment Program Monthly Report January
2015. Available from: http://www.cfenet.ubc.ca/sites/default/files/uploads/publications/centredocs/cfe-status-
report_january2015.pdf
3. Ebell MH, Siwek J, Weiss BD, et al. Strength of recommendation taxonomy (SORT): A patient-centered
approach to grading evidence in the medical literature. J Am Board Fam Pract 2004; 17: 59-67.

8
Glossary of Abbreviations
AFB Acid-Fast Bacilli
AIDS Acquired Immunodeficiency Syndrome
anti-HBs Anti-hepatitis B surface antibody
anti-HBc Anti-hepatitis B core antibody
Anti-
ART Antiretroviral Therapy
ARV Antiretroviral(s)
ASO AIDS Service Organization
BCCDC British Columbia Centre for Disease Control
BC-CfE British Columbia Centre for Excellence in HIV/AIDS
BC-
PHMRL
British Columbia Public Health Microbiology Reference Laboratory
BMD Bone Mineral Density
BMI Body Mass Index
CCR5 C-C chemokine receptor type 5
CD4 cell counts (absolute and fraction) are clinical indicators of
immunocompetence in patients with HIV infection
CDC United States Centers for Disease Control
CNS Central Nervous System
COPD Chronic Obstructive Pulmonary Disease
CSF Cerebrospinal Fluid
CT Computed Tomography
CVD Cardiovascular Disease
DF Tenofovir disoproxil fumarate
DM Diabetes Mellitus
DS Double Strength
DXA Dual Energy X-Ray Absorptiometry
ECG Electrocardiogram
eGFR Estimated Glomerular Filtration Rate
EIA Enzyme Immunoassay
FBG Fasting Blood Glucose
FIT Fecal Immuno-chemical test
GC Gonorrhoea and Chlamydia
GLP-1 Glucagon-like Peptide-1
HAART Highly Active Antiretroviral Therapy
HAV Hepatitis A Virus
HbA1C Glycated Haemoglobin
HBsAg Hepatitis B virus surface antigen
HBV Hepatitis B Virus
HIV Human Immunodeficiency Virus
HCV Hepatitis C Virus
HDL High-Density Lipoprotein
HIV RNA Quantitative HIV ribonucleic acid (RNA) measures plasma viral load.
HLA- Human Leukocyte Antigen B*5701 allele; genetic test to identify persons

9
B*5701 at a high risk for hypersensitivity reaction to the antiretroviral agent
abacavir.
HPV Human Papillomavirus
HSCRP High-Sensitivity C-Reactive Protein
HSR Hypersensitivity Reaction
IGRA Interferon Gamma Release Assay, used to screen for tuberculosis infection.
IM Intramuscularly
IgA Immunoglobulin A
IgG Immunoglobulin G
IPD Invasive Pneumococcal Disease
IR Insulin Resistance
IU International Units
IUD Interuterine Device
LDL Low-Density Lipoprotein
LTBI Latent Tuberculosis Infection
MAC Mycobaterium Avium Complex
MSM Men who have sex with men
MMR Mumps, Measles, Rubella
MMT Methadone Maintenance Therapy
MRI Magnetic Resonance Imaging
MSP Medical Services Plan
NAAT Nucleic Acid Amplification Test
NACI National Advisory Committee on Immunization
NNRTI Non-nucleoside Reverse Transcriptase Inhibitor
NRTI Nucleoside Reverse Transcriptase Inhibitor
NSAIDS Non-Steroidal Anti-Inflammatory Drugs
OI Opportunistic infection
PCR Polymerase Chain Reaction
PI Protease Inhibitor
PO per os (by mouth)
PPD Purified Protein Derivative
PWID People Who Inject Drugs
pVL HIV plasma viral load (copies/mL)
RPR Rapid Plasma Reagin
STI Sexually Transmitted Infections
SC Subcutaneously
TB Tuberculosis or Mycobacterium tuberculosis
TD Tetanus and Diphtheria
TMP-SMX Trimethoprim-Sulphamethoxazole
TRT Testosterone Replacement Therapy
TST Tuberculin Skin Test
UACR Urine Albumin to Creatnine Ratio
VZV Varicella Zoster Virus
WHO World Health Organization

10
SUMMARY OF PRIMARY CARE RECOMMENDATIONS FOR THE MANAGEMENT
OF HIV/AIDS
Section II: Medical History and Physical Examination
1. All HIV-positive individuals should be evaluated by a primary care clinician with knowledge
and experience in the management of HIV infection. (BII) Primary care clinicians without
expertise in HIV care should consult with a physician with this expertise. (CIII)
2. Clinicians should obtain a comprehensive present and past medical history, as well as a
medication/social/family history, review of systems, and conduct a complete physical
examination upon the patient’s entry into care. (AIII)
3. Clinicians should schedule routine monitoring visits at least every 3-6 months for all HIV-
positive individuals whose clinical status is stable and on antiretroviral therapy. More frequent
visits should be scheduled for those whose clinical status is unstable or not on antiretroviral
therapy. (CIII)
4. Clinicians should assess vital signs, weight, and body mass index (BMI) at each visit, and also
note abnormalities and changes in general appearance, body habitus, physical well-being, frailty,
and mobility. (CIII)
Section III: HIV Disease Specific Testing
1. All patients entering HIV care should have documented evidence of HIV antibody testing. If
laboratory confirmation is not available, a repeat HIV antibody test should be performed. (AIII)
2. Clinicians should obtain baseline CD4 cell counts (absolute and fraction) and quantitative HIV
RNA (plasma viral load) for all patients upon entry into care. (AI)
3. All patients should be assessed for transmitted HIV drug resistance using genotypic drug
resistance testing, regardless of the estimated duration of the infection. Ideally, the drug
resistance testing should be conducted on the first available sample of HIV plasma viral load
(AIII). Note that in British Columbia, genotypic resistance testing can be performed on archived
plasma samples (all samples are archived at the BC-CfE in perpetuity).
4. If antiretroviral therapy is deferred, a repeat genotypic drug resistance testing close to the time of
initiation of therapy is recommended because of the potential for superinfection (CIII).
5. Genotypic drug resistance testing should be conducted for patients experiencing treatment failure
or incomplete viral suppression (HIV plasma viral load >250 copies/mL) while receiving
antiretroviral therapy. (AII)
HLA-B*5701
1. HLA-B*5701 testing is recommended once at baseline for all patients. (CIII) HLA-B*5701-
positive patients must not be given abacavir-containing regimens. (AII)
2. All patients taking an abacavir-containing regimen should be screened for HLA-B*5701, if not
previously screened, regardless of how well they have tolerated abacavir in the past. (CIII). If
patients stop abacavir therapy and are HLA-B*5701 positive, they should not restart abacavir-
containing therapy, as they are at a high risk of hypersensitivity reaction (HSR). (CIII)

11
Section IV: Screening and Immunization for Selected Co-morbid Infections
Part 1: Screening for Co-morbidities
Tuberculosis Screening
1. All HIV-positive individuals should be screened at baseline for Mycobacterium tuberculosis
(TB) infection. (AI) Screening involves reviewing history of TB exposure and/or treatment
history, a recent chest X-ray (within 3 months), and previous tuberculin skin test (TST) and/or
interferon gamma release assay (IGRA) results. (AIII)
2. In British Columbia, the TST using 5 tuberculin units of purified protein derivative (PPD) is the
main test for diagnosing latent TB infection (LTBI), provided there are no contraindications.
(AIII)
3. IGRAs are currently recommended as an adjunct test to TST and may be valuable in the
following two situations: a) HIV-positive individuals with CD4 cell count <200 cells/mm3 who
are TST-negative (if possible, T-spot is preferred); and b) HIV-positive individuals with a history
of contact with active TB and who are TST-negative. (BIII)
Chest X-Rays
1. All HIV-positive individuals should have a chest X-ray at baseline. (CIII)
Toxoplasmosis Screening
1. All HIV-positive individuals should be screened at baseline for Toxoplasma IgG antibodies to
determine prior exposure to Toxoplasma (T.) gondii. (BIII)
Hepatitis Screening
1. HIV-positive individuals should be screened at baseline for hepatitis A virus (HAV) using total
anti-HAV antibodies. (CIII)
2. HIV-positive individuals should be screened at baseline for hepatitis B virus (HBV) using
HBsAg, anti-HBs and anti-HBc. (AIII) Individuals testing negative for HBsAg and anti-HBs but
testing positive for anti-HBc should have HBV DNA testing to rule out occult HBV infection.
(CIII)
3. HIV-positive individuals should be screened at baseline for hepatitis C virus (HCV) using a test
for HCV antibodies. (BIII) Positive HCV antibody test results should be confirmed by measuring
HCV RNA PCR. (AII)
Screening for Syphilis and other Sexually Transmitted Infections (STIs)
1. All HIV-positive individuals should be screened for syphilis at baseline. (AIII) Syphilis
screening should be repeated annually or every 3-6 months in the presence of ongoing risk
behaviours, or in the presence of symptoms. (BII)
2. A lumbar puncture should always be performed for patients with a reactive syphilis serology
who have neurologic or ocular symptoms or signs, irrespective of past syphilis treatment history.
(AI)
3. All HIV-positive individuals should be screened for gonorrhoea and chlamydia. (AII)
4. STI assessments should be done at baseline and repeated if there is ongoing risk. (AIII)

12
Part 2: Immunizations and HIV
RECOMMENDED VACCINES
Hepatitis A
1. All HIV-positive individuals who are susceptible (anti-hepatitis A [HAV] negative) should be
vaccinated against HAV, ideally when CD4 >200 cells/mm3. (BII)
2. The HAV vaccine should be administered intramuscularly at the standard dose (AI), at 0, 1 and 6
months. (AII)
Hepatitis B
1. All HIV-positive individuals who are susceptible to hepatitis B virus (HBV) infection (HBsAg
negative and anti-HBs less than 10 IU) should be vaccinated against HBV, ideally when CD4
>200 cells/ mm3. (BII)
2. HBV vaccination should also be offered to those who have positive hepatitis B total core
antibody (anti-HBc) with negative HBsAg and anti-HBs results and undetectable HBV DNA.
(AIII)
3. In the situations described above, HBV vaccine should be administered intramuscularly (IM) to
adults 20 years of age and older at a higher dose (40 mcg). (BII)
Recombivax (10 mcg/mL): give 4.0 mL IM at 0, 1, and 6 months
Recombivax Adult Dialysis formulation (40 mcg/mL) give 1.0 mL IM at 0, 1, and 6
months
Engerix Adult (20 mcg/mL): give 2.0 mL IM at 0, 1, 2 and 6 months
4. Post-serologic testing (using anti-HBs) within 1 to 6 months of completion of the vaccine series
is recommended to monitor success of immune response to vaccine. (CIII)
Pneumococcal Disease
1. All HIV-positive individuals should be vaccinated against pneumococcal disease using standard
vaccine doses (AI), regardless of CD4 cell counts and according to the following schedules:
(i) Individuals who have not previously received any pneumococcal vaccine: One dose of
conjugate pneumococcal vaccine (Pneu-C-13) is followed at least eight weeks later by
one dose of polysaccharide pneumococcal vaccine (Pneu-P-23). (AI)
(ii) Individuals who have received a pneumococcal polysaccharide vaccine (Pneumo-P-23)
previously: The Pneu-C-13 dose should be administered at least one year after any
previous dose of Pneu-P-23. (CIII)
(iii) If re-immunization with Pneu-P-23 is needed, it should be given at least 8 weeks after
the Pneu-C-13 dose and at least 5 years after the initial Pneu-P-23 dose. (CIII)
Influenza
1. All HIV-positive individuals should be vaccinated annually against influenza using standard
doses of the inactivated vaccine, regardless of CD4 cell counts or HIV plasma viral load. (AII)
Tetanus and diphtheria
1. All HIV-positive individuals should be offered a tetanus and diphtheria (Td) toxoid booster
every 10 years, ideally when CD4 >200 cells/mm3. (AII)

13
VACCINES INDICATED UNDER SPECIAL CIRCUMSTANCES
Measles, Mumps and Rubella (New subsection added March 2015)
1. All HIV-positive individuals without evidence of immunity and with CD4 cell counts >200
cells/mm3 should be considered for measles and/or mumps and/or rubella vaccination (given as a
two dose series of MMR vaccine). (BII)
2. All HIV-positive individuals born before 1970 or who have previously received two doses of
measles- and mumps-containing vaccine, have serologic proof of immunity against measles or
rubella, or have had lab diagnosed disease, are considered to have immunity against one or more
of these diseases. If they are susceptible to one of these diseases, the only vaccine available for
use is measles, mumps and rubella vaccine. MMR vaccine is safe for use in those with prior
immunity. (BII)
3. All HIV-positive individuals born before 1957 or who have previously received one dose of
rubella-containing vaccine, have serologic proof of immunity, or have had prior lab confirmed
rubella disease, are considered to have immunity against rubella. (AII)
Varicella (New subsection added July 2015)
1. All HIV-positive individuals without evidence of immunity and with CD4 cell counts >200
cells/mm3 may be considered for varicella vaccination (given as a two dose series of varicella
vaccine). (CIII)
Herpes Zoster (New subsection added March 2015)
1. Herpes zoster vaccine is contraindicated in HIV-positive individuals with CD4 <200 cells/mm3.
(BII)
2. The use of herpes zoster vaccine for prevention of shingles in HIV-positive adults with CD4
>200 cells/mm3 is not routinely recommended. (BIII)
Human Papillomavirus (HPV) (New subsection added March 2015)
1. HPV4 vaccine is recommended for HIV-positive girls and women (AII) and HIV-positive boys
and men (BII) between 9-26 years of age, regardless of their CD4 counts, to prevent infection
caused by HPV types 6, 11, 16 and 18 and related diseases. A 3-dose series is recommended,
regardless of age. (AII)
Section V: Schedule of Care for HIV-positive Individuals
1. All HIV-positive individuals who are not on antiretroviral therapy should have CD4 cell counts
and plasma viral loads (pVL) measured every 3-4 months. (BII)
2. All individuals initiating antiretroviral therapy should have CD4 cell counts and pVL measured
on a monthly basis until pVL is <40 copies/mL, and thereafter monitoring can occur every 3-4
months. (BII)
3. In clinically stable patients with dependable antiretroviral adherence, once pVL is consistently
<40 copies/mL for two years and CD4 counts are consistently ≥350 cells/mm³, pVL monitoring
can occur at intervals of up to six months and CD4 monitoring is optional. (CIII)
4. Safety laboratory parameters (complete blood count, renal and liver function, fasting lipids, and
glucose) should be monitored approximately one month after initiation of antiretroviral therapy
(with the first pVL and CD4 count) and every 3-6 months thereafter (see Table 6 on p. 57).

14
Monitoring should be undertaken more frequently in the presence of relevant underlying co-
morbid conditions, known potential toxicities of specific antiretroviral drugs, and/or concomitant
medications. (CIII)
Section VI: Special Considerations for Women and Transgender Individuals
with HIV
Special Considerations Related to Care before, during, and after Pregnancy
1. Contraception and pregnancy plans should be discussed with all individuals of childbearing
potential upon initiation of HIV care and routinely thereafter, as pregnancy may affect the choice
and timing of antiretrovirals. (AIII) Contraceptive counselling should also be included as a
critical aspect of postpartum care. (AIII)
2. Preconception counselling in HIV-positive individuals is recommended for anyone
contemplating pregnancy, especially in the setting of HIV-serodiscordant couples. (BII)
3. Pregnancy in HIV-positive individuals is considered a high risk and complex; therefore,
consultation with or referral to an obstetrician experienced in HIV is highly recommended. (BIII)
4. All HIV-positive pregnant individuals should be treated with ART for HIV infection, regardless
of their immunologic or virologic status, to prevent infection of their fetus. (AI) Antiretroviral
therapy should be continued after delivery and reassessed by providers of adult HIV care. (AII)
5. Breastfeeding is not recommended, regardless of HIV viral load and use of ART, for HIV-
positive individuals in Canada. (AI)
6. Clinicians should avoid prescribing efavirenz, or any new under-studied drug, during the first
trimester of pregnancy, to anyone who wishes to become pregnant, and to individuals of
childbearing potential who are not using effective and consistent contraception. A pregnancy test
should be done before initiation of efavirenz in individuals of childbearing potential and
counselling should be provided on the potential risk to the fetus while the mother is receiving
efavirenz. (AIII)
7. Clinicians should not prescribe nevirapine to antiretroviral-naïve women or trans-masculine
individuals who have CD4 cell counts >250 cells/mm3, nor start nevirapine during pregnancy
(AI)
Contraception in the Context of HIV
1. Health care providers should be aware of common interactions between ART and medications
taken for contraception, which may lower contraceptive efficacy and may result in unintended
pregnancy. (AII)
2. Intrauterine devices (IUDs) can be considered as a safe and effective contraception option for
HIV-positive women and adolescents. (BII)
Screening for Cervical and Breast Cancer in HIV-positive Individuals
1. Cervical Pap smear should be done for any individual with a cervix starting at age 21 or 3 years
after first sexual contact, whichever occurs first. For those eligible HIV- positive individuals
cervical screening should be done upon initiation of care, and should be repeated 6 months later.
If results are normal in both tests, cervical Pap smear should be done annually thereafter. (AI) If
Pap smear results are abnormal, the individual should be referred for colposcopy and directed
biopsy, as recommended by the BC Cancer Agency, with further treatment as indicated by
results. (AII)

15
2. Breast cancer screening for HIV-positive people should follow provincial guidelines for the
general population. (AII) Consider screening in transgender women on long-term hormone
replacement >5 years, and in transgender men and others who may have had mastectomy for
non-cancer related reasons.
Menopause
1. Hormone replacement therapy may be considered in patients who experience severe menopausal
symptoms (i.e. vasomotor symptoms and vaginal dryness) but should generally be used only for
a limited period of time and at the lowest effective doses. (BII)
2. Hormone replacement for HIV-positive transgender individuals should be provided in
consultation with an endocrinologist or other clinician who has experience providing endocrine
care to transgender individuals.
Section VII: Common Non-infectious Comorbidities
Cardiovascular Disease
1. All HIV-positive individuals should be screened for risk of cardiovascular disease at least
annually, and modifiable cardiovascular risk factors should be addressed where possible. (AI)
2. Assess fasting lipids (total, HDL, LDL cholesterol, and triglycerides) or apolipoprotein B at
baseline and every six months once patient begins antiretroviral therapy. (AIII)
3. An ECG should be performed at baseline and monitored periodically (at intervals determined by
the degree of risk) in patients taking protease inhibitors and/or rilpivirine with other PR- or QTc-
prolonging drugs. (CIII)
Insulin Resistance (IR) and Diabetes Mellitus (DM)
1. Fasting blood glucose (FBG) and/or glycated hemoglobin (HbA1c) should be performed in all
HIV-positive individuals at baseline and at six-month intervals during antiretroviral therapy.
Abnormalities in fasting glucose and/or HbA1c should be evaluated and managed according to
the Canadian Diabetes Society guidelines (http://guidelines.diabetes.ca/). (AIII)
2. Initial management of blood glucose abnormalities in HIV-positive individuals involves lifestyle
changes (weight loss, diet, exercise). (AIII)
3. Oral anti-glycemic agents and injectable anti-glycemic agents (insulin, glucagon-like peptide-1
[GLP-1] receptor agonists) should be used as required, keeping in mind drug interactions with
some antiretrovirals. (AIII)
Bone Disease
1. Clinicians should undertake preventive measures for bone loss in all HIV-positive individuals,
including weight-bearing exercises, maintaining ideal weight, reducing smoking and alcohol
consumption, and optimizing vitamin D and calcium intake (in the form of diet and
supplements). (AIII)
2. Vitamin D supplementation should be considered for all HIV-positive individuals (e.g. 1000-
2000 IU/day). (BIII)
3. Clinicians should consider performing a baseline dual energy X-ray absorptiometry (DXA) scan
to assess bone mineral density for HIV-positive women who are post-menopausal and in all HIV
positive men aged 50 years and older, and in patients of any age with a history of fragility

16
fractures or significant risk factors for osteoporosis (http://www.osteoporosis.ca/health-care-
professionals/guidelines/) (BIII).
4. DXA scan should be repeated at intervals according to local provincial guidelines. (BIII)
5. For HIV-positive transgender people who have undergone gender-affirming interventions, such
as hormone therapy or gonadectomy, clinicians should refer to appropriate resources for
guidance on osteoporosis screening. (CIII)
6. If decreased bone density is diagnosed, secondary causes such as hypogonadism, alcoholism,
glucocorticoid exposure, and vitamin D deficiency should be investigated and treated
appropriately, including referral to a specialist if necessary. (AIII)
Renal Disease
1. Due to the risk of renal disease related to HIV and antiretroviral medications, it is recommended
that blood pressure and laboratory assessment of renal function (serum creatinine and phosphate,
estimated glomerular filtration rate [eGFR], urinalysis for protein and sediment, and spot urine
for albumin to creatinine ratio [UACR]) should be performed in all HIV-positive individuals at
baseline and every 3-4 months after starting antiretrovirals, increasing to six-month intervals
when stable (depending on degree of risk). (AIII)
2. In case of renal dysfunction, clinicians should adjust doses of medications, including
antiretrovirals that are cleared by the kidney. An exception is tenofovir DF, which should be
avoided in patients with or at high risk of renal disease, and replaced with another agent in the
presence of clinically significant renal dysfunction. (AII)
Hypogonadism (New subsection added March 2015)
1. HIV-positive men presenting with symptoms of hypogonadism (decreased libido, erectile
dysfunction, reduced bone mass or low trauma fractures, hot flashes or sweats, weight loss,
reduced muscle strength or exercise capacity, sleep disturbance, fatigue, or depression) may be
assessed with a morning serum total testosterone level; an abnormal testosterone level should be
confirmed with repeat testing. An estimated bioavailable testosterone measurement may be
helpful to assess certain individuals, including obese men with borderline low total testosterone
levels. (AII)
2. Testosterone replacement is indicated only for symptomatic men with total testosterone levels
less than 10 mmol/L, and should be prescribed in consultation with a specialist. (AII)
3. Hormone replacement for HIV-positive transgender individuals should be provided in
consultation with an endocrinologist or other clinician who has experience providing endocrine
care to transgender individuals. (CIII)
Neurocognitive Impairment (New subsection added March 2015)
1. Antiretroviral therapy to suppress plasma viral load should be started early and administered
continuously, to prevent or minimize HIV-related neurocognitive impairment. (AII)
2. HIV-positive individuals presenting with cognitive complaints that affect their daily functioning
should be investigated to rule out relevant underlying conditions. (AII)
Lung Disease (New subsection added March 2015)
1. Smoking cessation should be strongly encouraged in all HIV-positive patients, because they are
at a higher risk for chronic obstructive pulmonary disease (COPD) and lung cancer than smokers
who do not have HIV. (AI)

17
2. A chest X-ray should be performed at baseline in all HIV-positive patients. Once infection has
been treated or ruled out, patients with persistently abnormal chest X-ray findings should be
investigated and referred to a respiratory specialist if necessary. (AI)
3. A diagnosis of COPD should be considered, and spirometry performed as a screening test,
among HIV-positive patients of any age presenting with persistent respiratory complaints,
especially those with additional risk factors such as smoking. COPD should be managed
according to current Canadian Thoracic Society guidelines
(http://www.respiratoryguidelines.ca/); however, concomitant use of inhaled steroids with
ritonavir or cobicistat should be avoided if possible. (AII)
Liver Disease/Cirrhosis (New subsection added March 2015)
1. Liver enzymes and liver function should be assessed in all HIV-positive individuals at baseline
and every 3-4 months after starting antiretrovirals, increasing to six-month intervals when stable.
(AIII)
2. All HIV-positive individuals with cirrhosis who are co-infected with Hepatitis B and/or C should
be screened for hepatocellular carcinoma every six months using ultrasound. (AII)
3. All HIV-positive individuals with cirrhosis should be referred for a baseline gastroscopy to
screen for esophageal varices. (AII)
Cancer (New subsection added March 2015)
1. In HIV-positive patients, screening for breast, colorectal, ovary, and prostate cancers should
follow current provincial recommendations for the general population. (BII)
2. HIV-positive patients may be at increased risk for lung cancer, HPV-related cancers
(oropharyngeal, cervical, anal), and hepatocellular cancer as compared to the general population.
Increased surveillance for these cancers is recommended. (AII)
Section VIII: Optimizing Adherence to Antiretroviral Therapy
1. All HIV-positive individuals should have timely access to routine and urgent care that is
linguistically and culturally appropriate to patient needs. (BII)
2. An interprofessional team model, with a primary provider for each patient, should be utilized to
promote trusting relationships between the patient and their health care team members. (BII)
3. Clinicians should involve patients in antiretroviral regimen selection. Clinicians should ensure
that patients understand treatment goals and are motivated to initiate and maintain adherence to
antiretroviral therapy. (BII)
4. Clinicians should educate and support patients to help maintain adherence to antiretroviral
therapy by positively reinforcing treatment success. (BII)
5. Potential behavioural, structural, and psycho-social barriers to adherence and engagement in
care, such as mental illness or substance abuse, should be identified and addressed in
collaboration with appropriate providers. These barriers may change with time and should be re-
evaluated on an ongoing basis by all health care team members. (BIII)

18
Section IX: Special Consideration for HIV-positive Individuals with
Addictions
1. All HIV-positive individuals should be asked about substance use at baseline and at least
annually thereafter. Those with a history of substance use should be re-evaluated for drug and
alcohol use at least quarterly. (CIII)
2. Clinicians should offer and support a variety of substance use treatment options for HIV-positive
substance users, including abstinence, a reduction in use, and safer use strategies. (CIII)
3. HIV-positive substance users receiving methadone or buprenorphine while on antiretroviral
therapy should be monitored for potential drug-drug interactions. (AII)
4. Substance users are at a high risk for multiple co-morbid medical and mental health conditions,
such as hepatitis B and C virus infection, tuberculosis, skin and soft tissue infections, recurrent
bacterial pneumonia, endocarditis, and depression. Primary care providers of HIV-positive
substance users should be familiar with the prevention, diagnosis, and treatment of these co-
morbidities. (BII)
Section X: Special Consideration for Individuals with Advanced HIV –
Opportunistic Infection & Prophylaxis
See Table 9 (p. 92).
Section XI: Psycho-social Implications of HIV Infection
Model of care
1. HIV care and patient education should be provided in a socially, culturally and gender
appropriate manner using a patient-centred, collaborative, and interdisciplinary chronic disease
care model which fosters trusting patient-provider relationships and improves retention in care.
(CIII)
Linkage to and retention in care
1. All HIV-positive individuals should have timely access to routine primary care and treatment.
(BII)
2. Case management for individuals with a new HIV diagnosis is recommended. (BII)
3. Intensive outreach for individuals not engaged in medical care within 6 months of a new HIV
diagnosis may be considered. (CIII)
4. Clinical and non-clinical providers are strongly encouraged to incorporate quality improvement
strategies that focus on improving delivery and quality of HIV care to HIV-positive individuals.
(CIII)
Peer and social support
1. Clinicians should perform thorough assessments of the social circumstances of HIV-positive
individuals at baseline and re-evaluate annually. (CIII)
2. All individuals living with HIV should be offered a referral to an AIDS service organization
(ASO) for counselling, social, and peer support. (CIII)
3. Peer support workers should be identified and utilized to help improve patient outcomes. (CIII)

19
I. Background
A. Introduction
The advent of potent antiretroviral therapy (ART) significantly improved the management of
HIV infection and led to substantial reductions in HIV- and AIDS-related morbidity and
mortality. ART has transformed HIV disease into a chronic, manageable condition. In addition,
new cohort data provide evidence for the effectiveness of ART treatment to prevent transmission
of HIV to sexual and needle-sharing (injection drug use) partners.1-4
In order for ART to be effective, individuals must be fully engaged in care, from the initial
assessment following diagnosis to long-term retention, and receive timely initiation of
antiretroviral therapy and, if necessary, effective psycho-social support systems.
B. Modes of HIV Transmission
The key modes of HIV transmission – sexual contact, perinatal transmission, and exposure to
infected blood through sharing of injection drug use paraphernalia or receipt of contaminated
blood products – were clarified early in the AIDS epidemic. In untreated HIV-positive
individuals, HIV is present in significant concentrations in blood, semen, pre-seminal fluids (pre-
cum), vaginal and rectal fluids, breast milk and any other body fluids contaminated with blood.
The likelihood of HIV transmission by different routes varies, as shown in Table 2 (adapted from
Garcia-Tejedor and Lewthwaite).5,6
(For further information on rates of HIV transmission, refer
to Appendix 2A of the BC-CfE Accidental Exposure Guidelines
http://www.cfenet.ubc.ca/sites/default/files/uploads/docs/Accidental_Exposure_Therapeutic_Gui
delines_Nov82010.pdf)
Table 2. Methods of HIV Transmission
Method Risk of acquisition per
100 exposures (%)*
Occupational injury 0.2
Sexual 0.2-0.5
Intravenous drug use 0.5-1.0
Mother-to-child 18-25
Parental
(blood or blood product recipient)
90
* In the absence of antiretroviral therapy in the source patient
Studies suggest that as many as 50% of HIV transmission events may occur from index patients
who are in the acute and very early stages of illness.7-11
Thus, early detection of HIV infection

20
may also be a critical component of preventing further transmission.12
Several factors contribute
to the increased risk of transmission during acute infection, including:
Very high levels of viremia during acute infection.
Likelihood that high-risk behaviours are ongoing during this period because the individual is
unaware of their HIV status.
The non-specific “influenza-” or “mononucleosis-like” symptoms of acute HIV infection
may be either absent or unrecognized as an indication of HIV infection.
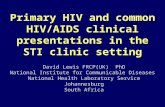
C. Natural History of HIV/AIDS
The mean time from HIV exposure to onset of acute seroconversion illness is generally 2-4
weeks, with a range of 5-29 days,13
although only an estimated 34% of HIV-positive individuals
will experience symptomatic seroconversion illness.14
After the initial drop in CD4 cell counts
and peak of viremia during seroconversion, CD4 cell counts will increase, although to levels
typically below pre-infection levels, and viral load will decrease and stabilize at a set point for
several years (Figure 1). There is considerable variability in the time of onset of further
symptoms and late-stage disease. Patients whose CD4 cell counts stabilize above 500 cells/mm3
may remain healthy for several years before CD4 cell counts begin to decline. For some patients,
CD4 cell counts will drop rapidly after infection; however, the usual scenario is one in which
CD4 cell counts decline over approximately five to eight years until symptoms begin to appear.
A small proportion of HIV-infected individuals (5-10%), called “long-term non-progressors,”
will maintain low viral load and stable CD4 cell counts for decades without specific treatment.6
Figure 1. Natural History of HIV/AIDS (Adapted from Lewthwaite, 2005)5

21
Some HIV-positive individuals may not exhibit any symptoms initially, while others may have
minor symptoms and/or persistent generalized lymphadenopathy, which usually affects cervical,
axillary and inguinal nodes, but often goes unnoticed by the patient. During this initial stage,
viral replication occurs in lymphoid tissue and thrombocytopenia may occur. HIV may also
begin to affect co-morbid conditions, such as hepatitis B and C, accelerating the progression of
liver fibrosis. As CD4 cell counts begin to decrease, HIV-positive individuals become
susceptible to a host of infections (caused by pathogens such as Mycobacterium tuberculosis,
Streptococcus pneumonia and Varicella zoster virus) and HIV-related tumours. Acquired
Immune Deficiency Syndrome (AIDS) (US CDC classification category C disease) is defined by
the development of specified opportunistic infections and cancers (see Appendix 1 on p. 106). In
addition, uncontrolled HIV replication and immune activation lead to a chronic inflammatory
state, resulting in end-organ damage and co-morbid conditions.15
D. HIV Disease Staging
Introduced in 1982, surveillance definitions for AIDS cases were initially developed to track and
monitor a disease that later was attributed to infection with the HIV virus. The definition of
AIDS has been revised over the years for increased utility for national and international
surveillance reporting systems and for public health purposes.16
There are currently two main HIV disease classification systems, developed by the US Centers
for Disease Control (CDC) and by the World Health Organization (WHO).16,17
In British
Columbia, AIDS and HIV are reportable conditions (consult the HIV testing guidelines:
http://www2.gov.bc.ca/assets/gov/health/about-bc-s-health-care-system/office-of-the-provincial-
health-officer/hiv-testing-guidelines-bc.pdf). See Appendix 1 (p. 106) for a list of AIDS-defining
illnesses.
E. Acute HIV Infection
Other terms for acute HIV infection are acute retroviral syndrome, acute HIV seroconversion,
and primary HIV infection. The following indicators should alert primary care providers to the
possibility of an acute HIV infection when certain patients present with influenza- or
mononucleosis-like symptoms: those who request HIV testing; those who have had recent sexual
or parenteral exposure to a known HIV-positive partner or a partner of unknown HIV sero-status
in the past 2-6 weeks; men who report having condomless sexual practices with men;
transgender people, in particular transgender women who have sex with men; those working in
sex trade; those who report needle use; those who present with a recent or newly diagnosed
sexually transmitted infection (STI); and those who present with aseptic meningitis. Unexplained
skin rash and mucocutaneous ulcers should also alert providers to the possibility of an acute HIV
infection. Appendix 2 on p. 107 further describes common symptoms and the frequency of their
occurrence in individuals who are symptomatic.
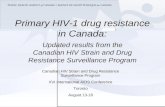
F. Diagnosis (Subsection revised March 2015)
For HIV testing, the window (or eclipse) period refers to the interval between the time when a
person is infected and when the test can first detect HIV infection. For serological tests, the

22
window or eclipse period is approximately 22 days for the third generation enzyme
immunoassay (EIA), otherwise known as enzyme-linked immunosorbent assay (ELISA), and
about 17 to 18 days for the fourth generation EIA or ELISA.18
By 6 weeks to 3 months after
infection, almost everyone who is infected will develop detectable HIV antigen or antibody. See
Figure 2 for a timeline.
Figure 2. Sequence of appearance of laboratory markers for HIV-1 infection19
At the British Columbia Provincial Public Health Reference Laboratory, as of May 27th
, 2015, all
samples submitted for HIV serology are screened by the fourth generation EIA or ELISA.20
The
sensitivity of the fourth generation EIA or ELISA is about 99.9% and the specificity is about
99.7%. Any reactivity on the screening HIV EIA or ELISA will automatically lead to a series of
additional tests to help differentiate acute HIV infection from established HIV infection or a false
positive HIV test (Figure 3 on the next page):
All EIA or ELISA positive samples are retested using a different manufacturer’s fourth
generation EIA. Samples which are concordantly positive on two manufacturers’ assays are
more likely to be true positive. The secondary EIA or ELISA is often referred to as a
supplemental test.
In the past, the Western blot, which detects an array of HIV specific proteins, has been the
gold standard for the diagnosis of established HIV infection. However, the Western blot can
be negative or indeterminate during acute infection.

23
To help identify acute HIV infections, which are known to be correlated with a higher risk of
onward transmission, the EIA or ELISA signals from the screening assay and the
supplemental assay are reviewed. If weak EIA or ELISA signals or an indeterminate or
negative Western blot are identified, the sample will automatically undergo an individual
HIV RNA nucleic acid amplification test (NAAT). If HIV RNA is detected, the specimen
will be reported as being suggestive of acute HIV infection, and a follow up ethylenediamine
tetraacetic acid (EDTA) blood sample will be requested to confirm HIV infection.
If the EIA or ELISA signals are weak and the individual NAAT is negative, the specimen
will be reported as not being consistent with HIV infection, and a follow up EDTA sample
will be requested to confirm if the initial EIA or ELISA result was true or false positive.
To help identify acute pre-seroconversion infections in high-risk individuals, a limited
number of pooled HIV RNA NAATs are performed on patients attending clinics that serve
high-risk populations to improve diagnosis of acute HIV infection.21
Figure 3. Current algorithm for EIA or ELISA screening in British Columbia22
G. Management of Acute HIV Infection
Providers should offer assistance to patients in notifying sexual partners and should counsel
patients about the increased risk of HIV transmission during an acute HIV infection. HIV is a
reportable infection, and the BCCDC provides assistance in contact tracing. Baseline HIV
genotypic testing should be undertaken (to request this test, complete and fax this form:
http://www.cfenet.ubc.ca/publications/centre-documents/laboratory-requisition-form-british-
columbia).
Providers should also consult with a physician with experience in treating HIV-positive
individuals to determine whether to initiate treatment during the acute phase and to discuss
possible antiretroviral regimens.23
Treatment for individuals with acute infection is supported
under current provincial and international guidelines.
Step 1:
EIA*
Step 2:
Western
Blot
Step 3:
Individual
RNA NAAT
Non-Reactive Reactive Acute infection Inconclusive
pos
neg pos
neg indet
neg/unconfirmed pos
* Screening by 3rd generation EIA.
4th generation EIA is used as a supplemental test, if 3rd generation EIA is positive.

24
H. Treatment as Prevention (New subsection added March 2015)
Evidence of the effect of antiretroviral treatment on the prevention of HIV transmission can be
derived from several models, including mother-to-child transmission, serodiscordant couples,
and clinical trial evidence.2, 24
Hence, on the basis of these data, antiretroviral treatment, which
was already deemed cost-effective on a patient-centred basis, can generate an additional
substantial cost saving once its effect on HIV transmission is considered.24
Furthermore,
Montaner et al. have shown a strong population-level association between increasing
antiretroviral treatment coverage, decreased viral load, and decreased number of new HIV
diagnoses per year.1
References
1. Montaner JS, Lima VD, Barrios R, et al. Association of highly active antiretroviral therapy coverage, population
viral load, and yearly new HIV diagnoses in British Columbia, Canada: A population-based study. Lancet 2010;
376(9740): 532-539.
2. Cohen MS, Chen YQ, McCauley M, et al. Prevention of HIV-1 infection with early antiretroviral therapy. N Engl J
Med 2011; 365(6): 493-505.
3. Rodger A, Bruun T, Cambiano V, et al. HIV transmission risk through condomless sex if HIV+ partner on
suppressive ART: PARTNER study [Abstract 153LB]. Top Antivir Med 2014; 22(e-1): 24-25.
4. Wood E, Kerr T, Marshall BDL, et al. Longitudinal community plasma HIV-1 RNA concentrations and incidence of
HIV-1 among injecting drug users: prospective cohort study. BMJ 2009; 338: b1649.
5. Garcia-Tejedor A, Maiques V, Perales A, Lopez-Aldeguer J. Influence of highly active antiretroviral treatment
(HAART) on risk factors for vertical HIV transmission. Acta Obstet Gynecol Scand 2009; 88(8): 882-887.
6. Lewthwaite P WE. Natural history of HIV/AIDS. Medicine 2005; 37(7): 333-337.
7. Brenner BG, Roger M, Routy JP, et al. High rates of forward transmission events after acute/early HIV-1 infection.
J Infect Dis 2007; 195(7): 951-959. doi: 10.1016/j.mpmed.2009.04.015.
8. Cohen MS, Pilcher CD. Amplified HIV transmission and new approaches to HIV prevention. J Infect Dis 2005;
191(9): 1391-1393.
9. Remien RH, Higgins JA, Correale J, et al. Lack of understanding of acute HIV infection among newly-infected
persons-implications for prevention and public health: The NIMH multisite acute HIV infection study: II. AIDS
Behav 2009; 13(6): 1046-1053.
10. Wawer MJ, Gray RH, Sewankambo NK, et al. Rates of HIV-1 transmission per coital act, by stage of HIV-1
infection, in Rakai, Uganda. J Infect Dis 2005; 191(9): 1403-1409.
11. Yerly S, Vora S, Rizzardi P, et al. Acute HIV infection: Impact on the spread of HIV and transmission of drug
resistance. AIDS 2001; 15(17): 2287-2292.
12. Metsch LR, Pereyra M, Messinger S, et al. HIV transmission risk behaviors among HIV-infected persons who are
successfully linked to care. Clin Infect Dis 2008; 47(4): 577-584.
13. Apoola A, Ahmad S, Radcliffe K. Primary HIV infection. Int J STD AIDS 2002; 13(2): 71-78.
14. Tyrer F, Walker AS, Gillett J, Porter K, UK Register of HIV Seroconverters. The relationship between HIV
seroconversion illness, HIV test interval and time to AIDS in a seroconverter cohort. Epidemiol Infect 2003; 131(3):
1117-1123.
15. Deeks SG, Tracy R, Douek DC. Systemic effects of inflammation on health during chronic HIV infection. Immunity
2013; 39(4): 633-645.
16. Centers for Disease Control and Prevention. 1993 revised classification system for HIV infection and expanded
surveillance case definition for AIDS among adolescents and adults. 1992:1-19. Available from:
www.cdc.gov/mmwr/preview/mmwrhtml/00018871.htm
17. World Health Organization. WHO case definitions of HIV for surveillance and revised clinical staging and
immunological classification of HIV-related disease in adults and children. 2007. Available from:
www.who.int/hiv/pub/guidelines/HIVstaging150307.pdf
18. Taylor D, Durigon M, Davis H, et al. Probability of a false-negative HIV antibody test result during the window
period: a tool for pre- and post-test counselling. Int J STD AIDS 2015; 26(4): 215-24.

25
19. Centers for Disease Control and Prevention. Laboratory testing for the diagnosis of HIV infection: updated
recommendations. 2014. Available from: http://stacks.cdc.gov/view/cdc/23447
20. BC Centre for Disease Control. HIV Laboratory Testing: a Resource for Health Professionals. 2010. Available from:
http://www.bccdc.ca/NR/rdonlyres/2982E293-BD82-436D-B193-
F929B5CEEBEC/0/HIVTestinginBCResourceDocumentforHealthProfessionalsJune2010.pdf
21. Gilbert M, Cook D, Steinberg, et al. Targeting screening and social marketing to increase detection of acute HIV
infection in men who have sex with men in Vancouver, British Columbia. AIDS 2013; 27(16): 2649-2654.
22. Gilbert M. HIV Testing [PowerPoint slides]. Retrieved from http://www.cfenet.ubc.ca/online-course-registration
23. New York State Department of Health AIDS Institute. HIV clinical resource. UPDATE: Diagnostic, monitoring and
resistance laboratory tests for HIV. Office of the Medical Director. 2014. Available from:
http://www.hivguidelines.org/wp-content/uploads/2014/01/diagnostic-monitoring-and-resistance-laboratory-tests-
for-hiv.pdf
24. Montaner JS, Hogg R, Wood E, et al. The case for expanding access to highly active antiretroviral therapy to curb
the growth of the HIV epidemic. Lancet 2006; 368(9534): 531-536.

26
II. Medical History and Physical Examination of HIV-Positive Individuals
Evidence (adapted from New York State Department of Health AIDS Institute, 2014 & Aberg et
al., 2014)1, 2
:
Many studies have demonstrated that better outcomes are achieved in HIV-positive outpatients
cared for by a clinician with HIV expertise,3-8
which reflects the complexity of HIV infection and
its treatment. Thus, appropriate training and experience, as well as ongoing continuing medical
education, are important components for the provision of optimal care. Primary care providers
with limited HIV experience should be encouraged to link with an experienced mentor who will
provide advice and consultation support when needed, or consider accessing some of the training
programs provided by the BC-CfE. For more information, visit: http://education.cfenet.ubc.ca.
A comprehensive current and past medical history should be obtained, with an emphasis on HIV
specific issues (Appendix 3 on pp. 108-109). Important elements include HIV exposure history
(date and place of diagnosis, route of exposure), history of symptoms related to acute HIV
infection, and history of prior opportunistic infections or AIDS-related events. It is critical to
obtain a history of prior antiretroviral regimens including date of initiation, prior resistance
testing, and adverse antiretroviral drug reactions. Particular emphasis should also be placed on a
review of systems, eliciting a comprehensive listing of symptoms, including those that patients
may not deem important to mention. In the course of taking a medical history, health care
providers should also assess a patient’s understanding of HIV disease, including risk for HIV
transmission, explore potential barriers to treatment adherence, and identify the patient’s psycho-
social needs.
Recommendations:
1. All HIV-positive individuals should be evaluated by a primary care clinician with
knowledge and experience in the management of HIV infection. (BII) Primary care
clinicians without expertise in HIV care should consult with a physician with this
expertise. (CIII)
2. Clinicians should obtain a comprehensive present and past medical history, as well as
a medication/social/family history, review of systems, and conduct a complete
physical examination upon the patient’s entry into care. (AIII)
3. Clinicians should schedule routine monitoring visits at least every 3-6 months for all
HIV-positive individuals whose clinical status is stable and on antiretroviral therapy.
More frequent visits should be scheduled for those whose clinical status is unstable or
not on antiretroviral therapy. (CIII)
4. Clinicians should assess vital signs, weight, and body mass index (BMI) at each visit,
and also note abnormalities and changes in general appearance, body habitus, physical
well-being, frailty, and mobility. (CIII)

27
Providers should inquire about chronic medical conditions such as neurological conditions,
gastrointestinal disease, chronic viral hepatitis, dyslipidemia, diabetes mellitus, cardiovascular
disease (or risk), kidney disease, and psychiatric disorders that might affect the choice of
antiretroviral therapy. Other past medical conditions that may have implications for HIV-infected
patients include a history of chickenpox or shingles; tuberculosis or tuberculosis exposure,
including results of prior testing for latent Mycobacterium tuberculosis infection; sexually
transmitted infections (STIs); abnormal cervical or anal cytology; and gynecologic problems.
The status of adult immunizations as detailed in Table 4 (p. 44) should be elicited.
Patients should be asked about all medications they take, including non-prescription, herbal and
over-the-counter products, since some may interact with antiretroviral therapies. A history of
medication intolerance or allergies should be obtained, with an emphasis on prior antiretroviral
exposure.
Clinicians should perform a comprehensive physical examination at baseline and annually, with
particular attention to systems potentially affected by HIV. Please refer to Appendix 4 (p. 110-
111). Since weight fluctuations are common in HIV-positive patients, clinicians should measure
weight at each visit (see US CDC’s body mass index [BMI] calculator:
http://www.cdc.gov/healthyweight/assessing/bmi/adult_bmi/english_bmi_calculator/bmi_calcula
tor.html), as well as vital signs, with particular attention to blood pressure.
References
1. New York State Department of Health AIDS Institute. Primary care approach to the HIV-infected patient. 2014.
Available from: http://www.hivguidelines.org/wp-content/uploads/2014/11/primary-care-approach-to-the-hiv-
infected-patient.pdf
2. Aberg JA, Gallant JE, Ghanem KG, et al. Primary care guidelines for the management of persons infected with
human immunodeficiency virus: 2013 update by the HIV Medicine Association of the Infectious Diseases Society of
America. Clin Infect Dis 2014; 58(1): e1-e34 doi: 10.1093/cid/cit665.
3. Kitahata MM, Koepsell TD, Deyo RA, Maxwell CL, Dodge WT, Wagner EH. Physician’ experience with the
acquired immunodeficiency syndrome as a factor in patients’ survival. N Engl J Med 1996; 334(11): 701-706.
4. Kitahata MM, Van Rompaey SE, Shields AW. Physician experience in the care of HIV-infected persons is
associated with earlier adoption of new antiretroviral therapy. J Acquir Immune Defic Syndr 2000; 24(2): 106-114.
5. Landon BE, Wilson IB, McInnes K, et al. Physician specialization and the quality of care for human
immunodeficiency virus infection. Arch Intern Med 2005; 165(10): 1133-1139.
6. Laine C, Markson LE, McKee LJ, Hauck WW, Fanning TR, Turner BJ. The relationship of clinic experience with
advanced HIV and survival of women with AIDS. AIDS 1998; 12(4): 417-424.
7. Kitahata MM, Van Rompaey SE, Dillingham PW, et al. Primary care delivery is associated with greater physician
experience and improved survival among persons with AIDS. J Gen Intern Med 2003; 18(2): 95-103.
8. Delgado J, Heath KV, Yip B, et al. Highly active antiretroviral therapy: Physician experience and enhanced
adherence to prescription refill. Antivir Ther 2003; 8(5): 471-478.

28
III. HIV Disease Specific Testing
A. CD4 cell counts, HIV viral load, and HIV resistance testing
Evidence:
Documented HIV antibody testing is necessary for a number of reasons. Patients may have tested
non-nominally or anonymously,1,2
or outside of their local jurisdiction (i.e. in a different
province or country), resulting in an absence of prior documentation.3
There is also the
possibility of testing errors (specimen handling or mislabelling) among individuals identified as
HIV-positive for the first time.2 Patients may also be unclear about whether an HIV test has been
performed, or they may present with misinformation regarding previous test results.4,5
The
absolute CD4 cell count is a significant clinical indicator of immunocompetence in patients with
HIV infection.3,4,6
The fraction of CD4 cells, expressed as a percentage of the total number of
lymphocytes, has also been used to predict mortality.7 These markers are used to stage HIV
disease initially and are subsequently used as predictors of disease progression and survival.8,9
CD4 cell counts are also used to determine the need for prophylaxis for opportunistic infections
(OIs) or other AIDS-defining illnesses, the risk of OIs, and when to stop prophylaxis.10
Caution
should be used when interpreting CD4 cell counts. In British Columbia, two distinct reporting
measures are in place. The more widely available measure uses absolute cells/µL (or cells/mm3)
and fraction of lymphocytes expressed as a percentage (e.g. absolute CD4 cell count: 500
Recommendations:
1. All patients entering HIV care should have documented evidence of HIV antibody
testing. If laboratory confirmation is not available, a repeat HIV antibody test should
be performed. (AIII)
2. Clinicians should obtain baseline CD4 cell counts (absolute and fraction) and
quantitative HIV RNA (plasma viral load) for all patients upon entry into care. (AI)
3. All patients should be assessed for transmitted HIV drug resistance using genotypic
drug resistance testing, regardless of the estimated duration of the infection. Ideally,
the drug resistance testing should be conducted on the first available sample of HIV
plasma viral load (AIII). Note that in British Columbia, genotypic resistance testing
can be performed on archived plasma samples (all samples are archived at the BC-CfE
in perpetuity).
4. If antiretroviral therapy is deferred, a repeat genotypic drug resistance testing close to
the time of initiation of therapy is recommended because of the potential for
superinfection (CIII).
5. Genotypic drug resistance testing should be conducted for patients experiencing
treatment failure or incomplete viral suppression (HIV plasma viral load >250
copies/mL) while receiving antiretroviral therapy. (AII)

29
cells/µL [or cells/mm3], and fraction: 25%). The less common measure uses numbers of cells x
109/L (e.g. absolute CD4 cell count: 0.500 cells x 10
9/L and fraction: 0.25), requiring some
calculations to convert to the more explicit method of absolute cell count.
Plasma viral load testing is another way to assess patient prognosis3
and to determine a patient’s
need for antiretroviral therapy.6
The association between a decrease in plasma viremia and
improved outcomes has been well-established11
; thus, HIV plasma viral load is an essential
indicator of therapeutic response and for identifying patients who are experiencing treatment
failure.9,12
HIV plasma viral load is also useful in predicting clinical progression.13,14
After the introduction of the Roche TaqMan test for measuring HIV plasma viral load (range
from 40-10,000,000 copies/mL) in British Columbia, a significant number of specimens with
low-level viremia have been reported. Current laboratory assays in use for quantifying HIV
plasma viral load have a good correlation across their linear range, but concordance at the lower
level of quantification is generally poor.15
Hence, it can be challenging to interpret low-level
viremia results and to assess the relevance of these results to the clinical management of HIV-
positive individuals receiving antiretroviral therapy. In this setting, a review of the patient’s
treatment adherence and close monitoring (i.e. repeat viral load testing) may be warranted.
However, plasma viral load testing should not be undertaken more frequently than once a month.
In addition, if viremia reaches levels greater than 250 copies/mL, genotypic drug resistance
testing is strongly recommended (complete and submit the BC-CfE Laboratory Requisition Form
to receive HIV genotype drug resistance testing:
(http://www.cfenet.ubc.ca/publications/centre-documents/laboratory-requisition-form-british-
columbia). Genotypic resistance testing may also be requested for patients with consistently
detectable plasma viral load between 200-250 copies/mL; these levels of viremia have been
shown in some studies to be predictive of later virologic failure.16,17
However, the success of
genotypic testing decreases at lower viral loads.17,18
For management of antiretroviral treatment
failure, clinicians should refer to the BC-CfE Therapeutic Guidelines for Antiretroviral (ARV)
Treatment of Adult HIV Infection (http://www.cfenet.ubc.ca/therapeutic-guidelines/adult).
In addition to the development of drug-resistant virus after being exposed to antiretroviral
therapy (secondary resistance), drug-resistant virus can be transmitted from one person to
another in the absence of previous exposure to antiretroviral therapy (primary resistance).
Resistant viral strains lead to suboptimal virological response to initial antiretroviral therapy.19-22
Results of drug resistance testing are useful in guiding initial antiretroviral therapy and assessing
failing therapy,23,24
and have also been shown to improve the outcomes of people taking
antiretrovirals.24
In British Columbia, genotypic drug resistance testing can be done
retrospectively from the first HIV plasma viral load test sample (or any other stored plasma viral
load sample).
B. Tropism testing
Tropism testing is not recommended at baseline as it can change over time. However, it is a test
that has relevance when considering the use of CCR5 receptor antagonist drug, maraviroc. For
more information about indications and type of tropism testing, see:
http://www.cfenet.ubc.ca/clinical-activities/lab-tests/ccr5-tropism;

30
to order the test in BC, requisition form available at:
http://www.cfenet.ubc.ca/publications/centre-documents/laboratory-requisition-form-british-
columbia.6
C. HLA-B*5701
Evidence:
HLA-B*5701 is not a specific HIV viral test. Screening for HLA-B*5701 identifies persons at a
high risk for hypersensitivity reaction (HSR) to the antiretroviral agent abacavir. Screening
should be performed prior to starting any patient on an abacavir-containing regimen (including
fixed-dose combinations, e.g Triumeq®). HSRs, including fatalities, have been documented in
individuals re-challenged with abacavir after a suspected HSR. In addition, screening for HLA-
B*5701 should be performed, if not done previously, for patients who are re-initiating abacavir
following a gap in therapy, even if they had previously tolerated the drug, because there is a
potential for HSR in this setting.25-29
Therefore, all patients taking an abacavir-containing
regimen and who have not previously undergone screening should be screened once for HLA-
B*5701, regardless of how well they have tolerated abacavir in the past. Patients in these
circumstances are at a higher risk of developing abacavir-related HSR if treatment is interrupted
and re-introduced. For more information about indications for abacavir and screening for HLA-
B*5701, see: http://www.cfenet.ubc.ca/clinical-activities/lab-tests/hla-b5701;
to order the test in BC, requisition form available at:
http://www.cfenet.ubc.ca/publications/centre-documents/laboratory-requisition-form-british-
columbia.6
Recommendations:
1. HLA-B*5701 testing is recommended once at baseline for all patients. (CIII) HLA-
B*5701-positive patients must not be given abacavir-containing regimens (AII)
2. All patients taking an abacavir-containing regimen should be screened for HLA-
B*5701, if not previously screened, regardless of how well they have tolerated
abacavir in the past. (CIII). If patients stop abacavir therapy and are HLA-B*5701
positive, they should not restart abacavir-containing therapy, as they are at a high risk
of hypersensitivity reaction (HSR). (CIII)

31
Table 3. HIV Disease Specific Tests
Test Baseline Follow-up before ART
initiation*
HIV Infection Status HIV diagnostic test
Immunologic
Assessment
CD4 absolute count
and percentage
√ Every 3-4 months
HIV Plasma Viral
Load (HIV pVL)
Quantitative RNA
testing
√ Every 3-4 months
Drug Resistance
Testing
HIV genotypic drug
resistance
√ (At the time of first HIV
pVL)
At the time of initiation of ART
Other HLA-B*5701 √ At baseline or before initiating
or restarting therapy with
abacavir, if not previously done.
Other Tropism testing When considering CCR5
antagonist
*For frequency of follow-up after antiretroviral initiation, see Section V: Schedule of Care, Table 6 (p. 57)
References
1. Aberg JA, Gallant JE, Ghanem KG, Emmanuel P, Zingman BS, Hoberg MA. Primary care guidelines for the
management of persons infected with human immunodeficiency virus: 2013 update by the HIV Medicine
Association of the Infectious Diseases Society of America. Clin Infect Dis 2014; 58(1): e1-e34 doi:
10.1093/cid/cit665.
2. BC Centre for Disease Control. HIV Laboratory Testing: a Resource for Health Professionals. 2010. Available from:
http://www.bccdc.ca/NR/rdonlyres/2982E293-BD82-436D-B193-
F929B5CEEBEC/0/HIVTestinginBCResourceDocumentforHealthProfessionalsJune2010.pdf
3. U.S. Department of Health and Human Services. Guidelines for the use of antiretroviral agents in HIV-1-infected
adults and adolescents. 2015:1-288. Available from:
http://aidsinfo.nih.gov/contentfiles/lvguidelines/adultandadolescentgl.pdf
4. U.S. Department of Health and Human Services. A guide to primary care for people with HIV/AIDS. 2004.
Available from: http://www.hab.hrsa.gov/tools/primarycareguide/index.htm
5. John Ruedy Immunodeficiency Clinic, St. Paul’s Hospital, Providence Health Care. Clinical protocols. 2009.
6. BC Centre for Excellence in HIV/AIDS. Therapeutic guidelines. Antiretroviral (ARV) treatment of adult HIV
infection. 2015 Available from: http://www.cfenet.ubc.ca/therapeutic-guidelines/adult
7. Moore DM, Hogg RS, Yip B, Craib K, Wood E, Montaner JSG. CD4 percentage is an independent predictor of
survival in patients starting antiretroviral therapy with absolute CD4 cell counts between 200 and 350 cells/μL. HIV
Infection 2006; 7(6): 383-388.
8. Mellors JW, Munoz A, Giorgi JV, et al. Plasma viral load and CD4+ lymphocytes as prognostic markers of HIV-1
infection. Ann Intern Med 1997; 126(12): 946-954.
9. Egger M, May M, et al. Prognosis of HIV-1-infected patients starting highly active antiretroviral therapy: A
collaborative analysis of prospective studies. Lancet 2002; 360(9327): 119-129.
10. BC Centre for Excellence in HIV/AIDS. Therapeutic guidelines for opportunistic infections. 2009. Available from:
http://www.cfenet.ubc.ca/therapeutic-guidelines/opportunistic-infection
11. Kaufmann GR, Perrin L, Pantaleo G, et al. CD4 T-lymphocyte recovery in individuals with advanced HIV-1
infection receiving potent antiretroviral therapy for 4 years: The Swiss HIV cohort study. Arch Intern Med 2003;
163(18): 2187-2195.
12. Hughes MD, Johnson VA, Hirsch MS, et al. Monitoring plasma HIV-1 RNA levels in addition to CD4+ lymphocyte
count improves assessment of antiretroviral therapeutic response. ACTG 241 protocol virology substudy team. Ann
Intern Med 1997; 126(12): 929-938.
13. Marschner IC, Collier AC, Coombs RW, et al. Use of changes in plasma levels of human immunodeficiency virus
type 1 RNA to assess the clinical benefit of antiretroviral therapy. J Infect Dis 1998; 177(1): 40-47.

32
14. Thiebaut R, Morlat P, Jacqmin-Gadda H, et al. Clinical progression of HIV-1 infection according to the viral
response during the first year of antiretroviral treatment. Groupe d'epidemiologie du SIDA en aquitaine (GECSA).
AIDS 2000; 14(8): 971-978.
15. Yan CS, Hanafi I, Kelleher AD, et al. Lack of correlation between three commercial platforms for the evaluation of
human immunodeficiency virus type 1 (HIV-1) viral load at the clinically critical lower limit of quantification. J
Clin Virol 2010; 49(4): 249-253.
16. Laprise C, dePokomandy A, Baril JG, Dufresne S, Trottier H. Virologic failure following persistent low-level
viremia in a cohort of HIV-positive patients: results from 12 years of observation. Clin Infect Dis 2013; 57(10):
1489-1496.
17. Vandenhende MA, Ingle S, May M, et al. Impact of low-level viremia on clinical and virological outcomes in
treated HIV infected patients [Abstract 1014]. Top Antivir Med 2014; 22 (e-1): 535-536.
18. Gonzalez-Serna A, Min JE, Woods C, et al. Performance of HIV-1 drug resistance testing at low-level viremia and
its ability to predict future virologic outcomes and viral evolution in treatment-naïve individuals. Clin Infect Dis
2014; 58(8): 1165-73.
19. Pozniak AL, Gallant JE, DeJesus E, et al. Tenofovir disoproxil fumarate, emtricitabine, and efavirenz versus fixed-
dose zidovudine/lamivudine and efavirenz in antiretroviral-naive patients: Virologic, immunologic, and
morphologic changes--a 96-week analysis. J Acquir Immune Defic Syndr 2006; 43(5): 535-540.
20. Borroto-Esoda K, Waters JM, Bae AS, et al. Baseline genotype as a predictor of virological failure to emtricitabine
or stavudine in combination with didanosine and efavirenz. AIDS Res Hum Retroviruses 2007; 23(8): 988-995.
21. Kuritzkes DR, Lalama CM, Ribaudo HJ, et al. Preexisting resistance to nonnucleoside reverse-transcriptase
inhibitors predicts virologic failure of an efavirenz-based regimen in treatment-naive HIV-1-infected subjects. J
Infect Dis 2008; 197(6): 867-870.
22. Little SJ, Holte S, Routy JP, et al. Antiretroviral-drug resistance among patients recently infected with HIV. N Engl
J Med 2002; 347(6): 385-394.
23. New York State Department of Health AIDS Institute. HIV clinical resource. UPDATE: Diagnostic, monitoring and
resistance laboratory tests for HIV. Office of the Medical Director. 2014. Available from:
http://www.hivguidelines.org/wp-content/uploads/2014/01/diagnostic-monitoring-and-resistance-laboratory-tests-
for-hiv.pdf
24. Hirsch MS, Gunthard HF, Schapiro JM, et al. Antiretroviral drug resistance testing in adult HIV-1 infection: 2008
recommendations of an international AIDS society-USA panel. Top HIV Med 2008; 16(3): 266-285.
25. Frissen JPH, de Vries J, Weigel HM, Brinkman K. Severe anaphylactic shock after rechallenge with abacavir
without preceding hypersensitivity. AIDS 2001; 15(2): 289.
26. Hetherington S, McGuirk S, Powell G, et al. Hypersensitivity reactions during therapy with the nucleoside reverse
transcriptase inhibitor abacavir. Clin Ther 2001; 23(10): 1603-1614.
27. Gervasoni C, Vigano O, Grinelli E, Ortu M, Galli M, Rusconi S. Abacavir hypersensitivity reaction after switching
from the twice-daily to the once-daily formulation. AIDS Patient Care STDS 2007; 21(1): 1-3.
28. El-Sahly HM. Development of abacavir hypersensitivity reaction after rechallenge in a previously asymptomatic
patient. AIDS 2004; 18(2): 359-360.
29. Loeliger AE, Steel H, McGuirk S, Powell WS, Hetherington SV. The abacavir hypersensitivity reaction and
interruptions in therapy. AIDS 2001; 15(10): 1325-1326.

33
IV. Screening And Immunization For Selected Co-Morbid Infections
PART 1: SCREENING FOR CO-MORBID INFECTIONS
A. Tuberculosis Screening
Evidence:
Among HIV-positive individuals, the annual risk of reactivating latent TB may be as high as 10
per 100 person-years, making HIV the most powerful known factor in promoting reactivation of
TB.1 Although it is considered an AIDS-defining illness, TB can occur at any stage in the course
of HIV infection as determined by the CD4 cell count.2 The risk of acquiring TB increases with
advancing immunosuppression, and decreases in individuals receiving effective antiretroviral
therapy.3,4
Thus, the identification of latent TB infection (LTBI) and the implementation of
measures to prevent the development of active disease are of high priority in the care of HIV-
positive individuals.
The tuberculin skin test (TST), consisting of the intradermal injection of a small amount of
purified protein derived from M. tuberculosis bacteria, is the standard screening test for TB. In a
person who has cell-mediated immunity to these tuberculin antigens, a cell-mediated, delayed
hypersensitivity reaction will occur within 48-72 hours. The reaction will cause localized
swelling and will manifest as induration of the skin at the injection site. Induration of ≥5 mm is
considered significant for an HIV-positive individual.1 TST remains the standard method of
diagnosing LTBI1 in Canada, although it is recognized that TST has certain limitations. The
Recommendations:
1. All HIV-positive individuals should be screened at baseline for Mycobacterium
tuberculosis (TB) infection. (AI) Screening involves reviewing history of TB exposure
and/or treatment history, a recent chest X-ray (within three months), and previous
tuberculin skin test (TST) and/or interferon gamma release assay (IGRA) results.
(AIII)
2. In British Columbia, the TST using 5 tuberculin units of purified protein derivative
(PPD) is the main test for diagnosing latent TB infection (LTBI), provided there are no
contraindications. (AIII)
3. IGRAs are currently recommended as an adjunct test to TST and may be valuable in
the following two situations: a) HIV-positive individuals with CD4 cell count <200
cells/mm3 who are TST-negative (if possible, T-spot is preferred); and b) HIV-
positive individuals with a history of contact with active TB and who are TST-
negative. (BIII)

34
sensitivity of the TST decreases in parallel with an individual’s CD4 cell count. The TST has
particularly low sensitivity in people with CD4 <200 cells/mm3.
False positive TST results are also not uncommon in those who have received Bacille Calmette-
Guerin (BCG) vaccination.5
Interferon gamma release assay (IGRA) is an immunologic in vitro test that was developed more
than a decade ago to diagnose TB infection, among other conditions. Currently, there are two
IGRA tests available in BC – QuantiFERON®-Gold-in-Tube (QFT) and T-SPOT®.TB (T-spot)
assays. Overall superiority of either IGRA test has yet to be clearly demonstrated,6 despite some
studies suggesting IGRA may be less affected by low CD4 count (especially T-spot) or prior
BCG vaccination.7-9
Therefore, IGRA is currently recommended as an adjunct test to TST and
may be valuable in the following two situations:9,10
a) HIV-positive individuals with CD4 count
<200 cells/mm3 who are TST-negative (if possible, T-spot is preferred); and b) HIV-positive
individuals with a history of contact with active TB and who are TST-negative.
A TST should be performed unless there is documentation of one of the following: (a) history of
a previous positive TST; (b) history of a positive IGRA; (c) documented prior or current active
TB; or (d) a previous severe reaction to TST. Individuals with advanced HIV disease who
initially had negative TST results (and negative IGRA, if done) are also recommended for repeat
TST testing if their CD4 cell counts increase to >200 cells/mm3, indicating immunocompetence
sufficient to mount a response to the test. TST is contraindicated in patients with a history of
severe blistering TST reactions in the past; those with extensive burns or eczema present over
TST testing sites; those with documented active TB or a well-documented history of adequate
treatment for TB infection or disease in the past; and those who have received measles
immunization within the past 4 weeks, as this has been shown to increase the likelihood of false-
negative TST results.1
A review of previous chest X-rays, TST results (and IGRA, if done), and history of TB disease
or exposure is part of TB screening for HIV-positive individuals.11
However, HIV-positive
individuals appear to be more likely to have active TB in the absence of typical clinical or
radiologic features, such as cough or chest X-ray abnormalities.12
A systematic review including
eleven clinical trials concluded that treatment of latent TB infection (LTBI) significantly reduces
the risk of active TB in HIV-positive individuals with a positive TST.13
TB screening (including
TST, exposure history, symptom screening, and chest X-ray) should be repeated annually for
individuals with negative baseline TST results who are at ongoing risk for exposure. Testing may
be repeated more frequently if there is evidence of new exposure to TB.
Positive TST results should be followed by treatment for LTBI once active TB disease is ruled
out. All TST- or IGRA-positive individuals should have sputum acid-fast bacilli (AFB)
microscopy and culture for M. tuberculosis performed, regardless of symptoms and chest X-ray
results.

35
B. Chest X-Rays
Evidence:
Chest X-rays are used in conjunction with sputum acid-fast bacilli (AFB) and culture to rule out
active tuberculosis, particularly among those who test positive during TB screening.
Certain populations, such as the homeless, individuals abusing alcohol and drugs, and chronic
smokers, are at an increased risk of having radiographic abnormalities.14
Because of the
potentially high prevalence of these risk factors in the HIV-positive population in British
Columbia, it is important to perform a chest X-ray at baseline in all HIV-positive individuals, not
only to rule out abnormalities but also to use as a comparison for future evaluation of respiratory
complaints.
C. Toxoplasmosis Screening
Evidence:
Seroprevalence of T. gondii in North American adults is approximately 10-20%. The serologic
test for Toxoplasma cannot be used to diagnose or exclude toxoplasmosis in HIV-positive
individuals.11
Toxoplasma encephalitis is the most frequent clinical manifestation of central
nervous system (CNS) disease in HIV-positive individuals.15
While positive serology identifies
individuals at a greater risk, up to 16% of those presenting with CNS toxoplasmosis will have
negative serology.15
Among HIV-positive/T. gondii-infected (i.e. Toxoplasma IgG antibody
positive) adults not receiving prophylaxis and with CD4 cell counts of <100 cells/mm3, the
probability of developing clinical toxoplasmosis is approximately 38%.11
D. Hepatitis Screening
Recommendations:
1. HIV-positive individuals should be screened at baseline for hepatitis A virus (HAV)
using total anti-HAV antibodies. (CIII)
Recommendation:
1. All HIV-positive individuals should have a chest X-ray at baseline. (CIII)
Recommendation:
1. All HIV-positive individuals should be screened at baseline for Toxoplasma IgG
antibodies to determine prior exposure to Toxoplasma (T.) gondii. (BIII)

36
2. HIV-positive individuals should be screened at baseline for hepatitis B virus (HBV)
using HBsAg, anti-HBs and anti-HBc. (AIII) Individuals testing negative for HBsAg
and anti-HBs but testing positive for anti-HBc should have HBV DNA testing to rule
out occult HBV infection. (CIII)
3. HIV-positive individuals should be screened at baseline for hepatitis C virus (HCV)
using a test for HCV antibodies. (BIII) Positive HCV antibody test results should be
confirmed by measuring HCV RNA PCR. (AII)
Evidence:
Hepatitis A virus (HAV) is most frequently transmitted by the fecal-oral route, through direct
contact with infected people, or indirectly by ingesting contaminated water or food. Rarely, HAV
is transmitted through exposure to HAV-contaminated blood or blood products. Transmission
through sexual activities that involve direct or indirect oral-anal contact can also occur.16
In
Canada, the number of cases of HAV has steadily declined since 2003.17
The main risk factors
for HAV infection include: sexual behaviours involving anal contact, particularly among men
who have sex with men (MSM); travel or residence in endemic countries; and illicit drug use.17-19
Pre-immunization serologic testing is only cost-effective in populations that have a
seroprevalence of >30%.14
Older people, people coming from endemic areas, and people with a
history of jaundice or hepatitis should be considered for assessment of immunity before
immunization is undertaken.17
Because these risk factors and populations are highly prevalent
among HIV-positive individuals, all HIV-positive individuals without previous evidence of
vaccination or diagnosis of HAV should be vaccinated.
HIV and hepatitis B virus (HBV) share routes of transmission, including percutaneous
(principally among people who inject drugs [PWID]), sexual (anal, vaginal, and oral) and
vertical transmission.16
The reported prevalence of HIV-HBV co-infection is between 6-10%,
with higher rates observed in PWID, in MSM, and in individuals from endemic areas.20
HIV-
HBV co-infection is associated with an eight-fold increase in risk of mortality compared to HBV
mono-infection.21
Therefore, traditional HBV markers, such as HBsAg (surface antigen), anti-
HBs (surface antibodies), and anti-HBc (core antibodies), will assist in distinguishing individuals
who are chronically infected from those who have developed a natural or acquired immune
response or those susceptible to HBV infection (thus, in need of receiving immunization).
Management of chronic HBV infection should follow standard international guidelines (see
Table 10 on p. 100).
In Canada, the prevalence of HIV-hepatitis C (HCV) co-infection ranges from 20% to almost
90% in certain subgroups.22
HCV is highly prevalent among PWID; a review of international
studies suggests that between 50-95% of PWID are infected with HCV.23
Canadian studies report
HCV rates as high as 82% among PWID.24,25
If left untreated, HCV infection becomes chronic in
50-85% of co-infected individuals, potentially leading to death.23
A meta-analysis of seventeen
studies concluded that the rate of progression to hepatic fibrosis among individuals co-infected
with HIV-HCV appears constant across all stages of fibrosis, and that chronic HCV outcomes

37
are worse among co-infected individuals. Over the period studied, antiretroviral therapy did not
appear to fully reverse the adverse effect of HIV infection on HCV disease prognosis.26
The
probability of survival is also reduced among HIV-HCV co-infected individuals compared to
those who are HIV mono-infected.27
Anti-HCV antibody is the standard screening test; however,
approximately 6% of HIV-HCV co-infected patients do not develop HCV antibodies.14
HCV
RNA testing should be considered if the index of suspicion for HCV infection is high, for
instance in individuals presenting with ongoing risk factors (e.g. sharing needles) or those with
unexplained abnormally elevated liver enzymes. Patients with confirmed HIV-HCV co-infection
should be managed according to current guidelines.28
E. Screening for Syphilis and other Sexually Transmitted Infections (STIs)
Evidence:
In North America, sexual transmission is the predominant route for acquiring HIV. This has
prompted the recommendation to screen all HIV-positive individuals for asymptomatic STIs. A
cohort study reported a baseline STI prevalence of 14% among HIV-positive individuals (n=212,
95% confidence interval [CI] 9%-19%) and the incidence of new infections was 20.8 cases per
100 person-years (95% CI 14.8-28.4).29
The prevalence of STIs in British Columbia is increasing. The provincial prevalence of
infectious syphilis, as elsewhere in North America, has increased over the past fifteen years.
With the exception of a short period of decline in 2009-2010, infectious syphilis rates have
increased to 8.1 per 100,000 population as of 2012.30
Similarly, the overall provincial trend for
genital gonorrhoea has increased steadily since 1998, with a slight decrease in 2012 to 28.1 per
100,000 population (1,291 cases). In 2012, the rate of genital chlamydia was 267.9 per 100,000
population (12,364 cases), continuing an overall increase since 1998. MSM continue to be the
most affected, representing 84% of new syphilis cases in the same period. Among MSM whose
HIV status was known, over 65% were syphilis and HIV co-infected.29
Recommendations:
1. All HIV-positive individuals should be screened for syphilis at baseline. (AIII)
Syphilis screening should be repeated annually or every 3-6 months in the presence of
ongoing risk behaviours, or in the presence of symptoms. (BII)
2. A lumbar puncture should always be performed for patients with a reactive syphilis
serology who have neurologic or ocular symptoms or signs, irrespective of past
syphilis treatment history. (AI)
3. All HIV-positive individuals should be screened for gonorrhoea and chlamydia. (AII)
4. STI assessments should be done at baseline and repeated if there is ongoing risk.
(AIII)

38
Traditionally, syphilis screening has been done with a non-treponemal test (e.g. rapid plasma
reagin [RPR]) followed by a treponemal test (e.g. fluorescent treponemal antibody absorption).
In July 2014, the BC Public Health Microbiology Reference Laboratory (BC-PHMRL) switched
the preliminary screening test for syphilis from the rapid plasma reagin (RPR) antibody test to an
Enzyme Immunoassay (EIA), a Treponema pallidum-specific antibody test. Because Treponema
pallidum antibodies persist for the life of an individual, the EIA test will detect a greater number
of old syphilis cases. Confirmatory tests do not need to be ordered by clinicians as they are
automatically done by the BC-PHMRL.31
For gonorrhoea and chlamydia (GC), Nucleic Acid Amplification Test (NAAT) should be
conducted in all HIV-positive patients using first-catch urine specimen for urethral samples. In
women and transgender individuals who have a cervix, a cervical swab also should be taken.
Although not validated, vaginal swabs can be used for screening in transgender women who are
post-operative (i.e. after gender reassignment surgery). MSM who are symptomatic should be
screened for GC using pharyngeal (throat) and anal swabs using a standard culture and
sensitivity transport media. Pharyngeal and anal swabs should be considered for other patients
who are at risk (e.g. individuals engaging in anal or oral sex practices, regardless of sexual
orientation). In cases of possible sexual assault, pharyngeal, anal, and/or vaginal swabs should be
taken.32
In patients who wish to avoid pelvic and/or anal examinations, the clinician should rely
on the NAAT of a urine specimen.
STI screening for HIV-positive individuals has generally been recommended to be performed at
baseline and repeated at least annually.14,33
However, limiting screening to annually likely leaves
patients infectious for long periods and there are reports that as many as 24% of asymptomatic
STIs would have been missed by risk-based screening. Increasing screening frequency has
minimal effect on the cost of identifying asymptomatic STIs.29
Prevalent and incident asymptomatic STIs are common among HIV-positive MSM, and thus
increasing the frequency of screening to every 3-6 months is warranted for those with ongoing
risk factors such as unprotected intercourse, multiple partners, anonymous sex, illicit drug use in
association with sex, recreational drug use, methamphetamine use, attendance at sex-on-premises
venues, and seeking sexual partners through the Internet.34
F. Papanicolaou (Pap) Smear Screening
Regarding screening for cervical cancer, please see Section VI: Special Considerations for
Women and Transgender Individuals in HIV (pp. 64-65).
Anal cytological screening (anal Pap smear) in HIV-positive individuals is not considered
standard of care at this time but is being performed in some health care centres in Canada. A few
US guidelines have recommended routine anal Pap tests for some populations.14,35,36
The
rationale behind screening for anal cancer is based on the similarities between anal dysplasia and
cervical dysplasia, and the success of the cervical Pap screening program.37,38
However, there are
currently no randomized clinical trials to corroborate the benefits of anal Pap smear in decreasing
incidence of anal cancer and related mortality. Additional studies of screening and treatment
protocols, diagnostic approaches, natural history of the condition, and cost-effectiveness analysis
are in progress and will inform the decision whether to include anal Pap smears as a standard of
care in the future.34

39
PART 2: IMMUNIZATIONS AND HIV
Prevention of inter-current illness is a crucial aspect of HIV care.14,35
The use of vaccines
provides an opportunity to prevent infectious diseases in HIV-positive individuals, who are more
susceptible to these diseases.17
Immunosuppression can reduce the effectiveness of vaccines and
increase the risks associated with live vaccines.17,19,39
CD4 cell counts are an important measure
that can be used to help optimize the timing of immunizations and predict patient response to
vaccines.
General principles that primary care physicians can follow for HIV-positive individuals are
shown below (adapted from the Canadian Immunization Guide)17
:
Tailor immunizations to the needs of each patient.
Immunize at the time when maximum immune response can be anticipated (i.e. early in the
course of HIV disease or following CD4 recovery with antiretroviral therapy).
It is safer, and likely more effective, to immunize when CD4 cell counts are >200 cells/mm3.
The magnitude and duration of vaccine-induced immunity are often reduced in
immunocompromised individuals.
Use caution in the use of live vaccines based on CD4 cell counts and recommendations for
use.
There is no contraindication to the use of inactivated or component vaccines at any CD4 level.
RECOMMENDED VACCINES
A. Hepatitis A
Evidence:
Serologic response rates of all HAV vaccines are between 95-100% amongst HIV negative
individuals.17
Seroconversion rates are lower among HIV-positive individuals for many vaccines
and HAV seroconversion is no exception, with rates ranging from 48-64% (depending on the
timing of measurement of serological response).40,41
A meta-analysis reported an overall
response rate of 64% for HIV-positive individuals.42
A three dose regimen (0, 1, 6 months) has
been shown to have better results than a two dose regimen (0, 6 months) among HIV-positive
individuals, with reported seroconversion rates in one study of 78% and 61%, respectively.43
The
standard HAV vaccination doses are 1.0 mL intramuscularly (IM).39
Recommendations:
1. All HIV-positive individuals who are susceptible (anti-hepatitis A [HAV] negative)
should be vaccinated against HAV, ideally when CD4 >200 cells/mm3. (BII)
2. The HAV vaccine should be administered intramuscularly at the standard dose (AI), at
0, 1 and 6 months. (AII)

40
B. Hepatitis B
Evidence:
The overall seroconversion rate (defined as HBsAb >10 mIU/mL) to standard HBV vaccine
dosing (10 mcg of Recombivax HB® or 20 mcg of Engerix®-B IM [deltoid]) following a 0, 1
and 6 month dosing regimen appears to be on the order of 26-65%.17,44-46
The etiology of poor
seroconversion rates in individuals who are HIV-positive is multi-factorial and not completely
elucidated. Contributing factors may include age, sex, race, CD4 cell count (both nadir and at
time of vaccination), HIV viral load, treatment with antiretrovirals, smoking and alcohol abuse.
The benefit of using higher doses of HBV vaccine in immunocompromised individuals is now
well-established, both in HIV and in other immunodeficiency states.44,47,48
In particular, higher
HBV seroconversion rates are reported in HIV-positive individuals on antiretroviral therapy with
low HIV plasma viral load and high CD4 cell counts. The low seroconversion rate is an
indication to conduct post-vaccination testing (HBsAg and anti-HBs) on one occasion, between
one month and 6 months after the completion of the initial vaccination series. 49
Patients with isolated antibody to hepatitis B core antigen (HBsAg and anti-HBsAg antibody
negative and no detectable HBV DNA) also benefit from HBV vaccination.50
Vaccine non-responders following the first series should receive a complete second series of 3
doses. If they fail to respond to a second series, they should be recorded as susceptible and
receive Hepatitis B immune globulin (HBIg) following an exposure.51
Recommendations:
1. All HIV-positive individuals who are susceptible to hepatitis B virus (HBV) infection
(HBsAg negative and anti-HBs less than 10 IU) should be vaccinated against HBV,
ideally when CD4 >200 cells/ mm3. (BII)
2. HBV vaccination should also be offered to those who have positive hepatitis B total
core antibody (anti-HBc) with negative HBsAg and anti-HBs results and undetectable
HBV DNA. (AIII)
3. In the situations described above, HBV vaccine should be administered
intramuscularly (IM) to adults 20 years of age and older at a higher dose (40 mcg).
(BII)
Recombivax (10 mcg/mL): give 4.0 mL IM at 0, 1, and 6 months
Recombivax Adult Dialysis formulation (40 mcg/mL) give 1.0 mL IM at 0, 1, and 6
months
Engerix Adult (20 mcg/mL): give 2.0 mL IM at 0, 1, 2 and 6 months
4. Post-serologic testing (using anti-HBs) within 1 to 6 months of completion of the
vaccine series is recommended to monitor success of immune response to vaccine.
(CIII)

41
C. Pneumococcal Disease
Evidence:
HIV-positive individuals are at a higher risk of developing invasive pneumococcal disease than
HIV-negative individuals.52-56
Streptococcus pneumoniae is the most common agent causing
pneumonia in HIV-positive individuals, followed by gram negative bacteria, including
Haemophilus influenzae, Pseudomonas aeruginosa and Legionella pneumophila.57,58
Low CD4
cell count is a predictor of the occurrence of bacterial infections, but these can occur at any CD4
level. Other risk factors influencing the development of bacterial pneumonia include cigarette
smoking, low socioeconomic status, alcohol abuse, injection drug use, co-morbidities including
asthma and underlying lung disease (e.g. COPD), malnutrition, uncontrolled viral replication,
and lack of antiretroviral treatment.59-61
Two forms of pneumococcal vaccine are currently available in BC: conjugated vaccine (Pneu-C-
13) and polysaccharide vaccine (Pneu-P-23). The efficacy of any form of the pneumococcal
vaccine is unclear for HIV-positive individuals with CD4 cell counts <200 cells/mm3. A study of
individuals on antiretroviral therapy showed a failure to induce serotype specific antibodies when
administering Pneu-P-23 to patients with CD4 cell counts <100 cells/mm3.62
However, another
study demonstrated that, although Pneu-P-23 failed to prevent the occurrence of invasive
pneumococcal disease (IPD), it decreased the severity and mortality of illness related to IPD.63
Research on the efficacy of the pneumococcal conjugate 7-valent vaccine (Pneu-C-7) in HIV-
positive individuals has demonstrated improved health outcomes,64,65
yet also showed the
emergence of non-vaccine type pneumococci, which may highlight the need for greater breadth
of Streptococcus pneumoniae serotype coverage in regard to conjugated vaccines.66, 67
Research
is ongoing to develop an optimal vaccine regime against IPD in the HIV-positive population.
Recommendations:
1. All HIV-positive individuals should be vaccinated against pneumococcal disease using
standard vaccine doses (AI), regardless of CD4 cell counts and according to the
following schedules:
(i) Individuals who have not previously received any pneumococcal vaccine:
One dose of conjugate pneumococcal vaccine (Pneu-C-13) is followed at least
eight weeks later by one dose of polysaccharide pneumococcal vaccine
(Pneu-P-23). (AI)
(ii) Individuals who have received a pneumococcal polysaccharide vaccine
(Pneumo-P-23) previously: The Pneu-C-13 dose should be administered at
least one year after any previous dose of Pneu-P-23. (CIII)
(iii) If re-immunization with Pneu-P-23 is needed, it should be given at least 8
weeks after the Pneu-C-13 dose and at least five years after the initial Pneu-P-
23 dose. (CIII)

42
While one study comparing Pneu-C-7 to Pneu-P-23 found that the conjugated vaccine elicited
better serologic response,68
other studies have looked into possible synergistic effect of a dual
vaccination regimen that incorporates both the conjugate and the polysaccharide vaccines.69-71
Although there are no data on the efficacy and effectiveness of Pneu-C-13 in the HIV-positive
population, it is logical to extrapolate such data from previous research on the use of Pneu-7 in
this population, since the components of the two vaccines are so similar (Pneu-C-13 is equivalent
to Pneu-C-7 plus six other serotypes). Based on this extrapolation, a recent cost-effectiveness
vaccine study supports adding Pneu-C-13 to the existing Pneu-P-23 regimen in HIV-positive
individuals.72
The National Advisory Committee on Immunization (NACI) concluded that there
is good evidence to recommend the use of Pneu-C-13 for HIV-positive patients, given the
efficacy and immunogenicity of Pneu-C-7.73
Nevertheless, further research will need to be done
on Pneu-C-13 alone or in combination with Pneu-P-23 in the HIV-positive population to validate
this assumption.71
The Pneu-C-13 vaccination dose is 0.5 mL (IM) and the Pneu-P-23
vaccination dose is 0.5 mL (subcutaneously [SC] or IM), although SC administration is
associated with more discomfort at the injection site.39
D. Influenza
Evidence:
Caused by influenza A and B viruses, influenza occurs in Canada every year, generally during
late fall and the winter months. Influenza A viruses are the most common cause of annual
influenza epidemics.17
The annual incidence of influenza varies widely, depending on the
virulence of circulating strains and the susceptibility of the population, which is affected by
antigenic changes in the virus, vaccine match, and vaccine coverage.17
HIV-positive individuals
form part of the group at the greatest risk of serious infections, complications, hospitalizations,
and/or death from influenza.17,74
In the HIV-positive population, influenza vaccine reduces the
incidence of respiratory illnesses from 49% to 29% and of laboratory-confirmed influenza from
21% to 0%.75
As is the case with other vaccines, influenza vaccine efficacy is impaired in HIV-positive
individuals. One study estimated that vaccine efficacy decreased from 65% in patients with CD4
cell counts >100 cells/mm3 to 11% in those with lower CD4 cell counts.
76 The same study also
showed that efficacy was 52% in patients with plasma HIV RNA levels below 30,000 copies/mL
and 40% in those with higher viral loads.75
However, the benefits of the influenza vaccine in
preventing severe illness and hospital/intensive care unit admissions prompted the US Centers
for Disease Control (CDC) to recommend the use of the vaccine in HIV-positive individuals,
regardless of CD4 cell counts or HIV plasma viral load.77
A single annual intramuscular dose of
0.5 mL is currently recommended.17,39
There is no indication for pre- or post-immunization
Recommendation:
1. All HIV-positive individuals should be vaccinated annually against influenza using
standard doses of the inactivated vaccine, regardless of CD4 cell counts or HIV
plasma viral load. (AII)

43
serology testing.17
Inactivated influenza vaccine is recommended and live attenuated intranasal
vaccine should not be used in this population.14,19,39,78
Influenza vaccines publicly funded in British Columbia vary year to year. For details of which
vaccines are being used in any given season, refer to the BC Communicable Disease Control’s
Immunization Manual (http://www.bccdc.ca/dis-cond/comm-manual/CDManualChap2.htm).79
E. Tetanus and diphtheria
Evidence:
The recommendation above assumes that the diphtheria vaccination is being offered to an adult
who has completed a primary series of childhood vaccinations. Routine immunization against
diphtheria in infancy and childhood is a common practice throughout the world and has
contributed to a significant decline in morbidity and mortality from this disease.80
Serosurveys of
healthy adult populations in Canada indicate that approximately 20% of those surveyed (higher
in some age groups) do not have protective levels of antibody to diphtheria. Thus, the potential
for re-emergence of this disease exists.81
The immunity conferred by diphtheria vaccine is antitoxic, not antibacterial. Vaccination thus
protects against the systemic effects of diphtheria toxin but not directly against local infection.81
After the primary vaccination series in immunocompetent individuals, over 99% develop
antibody levels that are considered protective against disease.80
The antitoxin is believed to
persist at protective levels for ten years or more. Titres decline slowly with time but are boosted
by additional vaccine doses.80
Tetanus is rare in Canada. However, serosurveys suggest that a substantial proportion of
Canadians have non-protective tetanus antitoxin levels. Factors associated with lack of immunity
to tetanus include increasing age, birth outside Canada, and absence of immunization records.81
The antibody response to tetanus boosters given to adults with HIV or other humoral immune
deficiencies is suboptimal.80
Recommendation:
1. All HIV-positive individuals should be offered a tetanus and diphtheria (Td) toxoid
booster every 10 years, ideally when CD4 >200 cells/mm3. (AII)

44
Table 4. Recommended Vaccines* for HIV-positive Adults (Table revised March 2015)
Vaccine Recommendation
Hepatitis A Vaccine (Inactivated virus
vaccine)
Formulations: Vaqta®, Havrix®, Avaxim®
Schedule: 0, 1, 6 months (different from standard schedule of 0,
and 6-12 months) for susceptible individuals.
Dosage: Standard adult dose (formulation dependent)
Route of administration: Intramuscular (IM)
Hepatitis B Vaccine (Monovalent
recombinant DNA vaccine)
Formulations: Recombivax HB® (10 mcg/1.0 mL) or
Engerix®-B (20 mcg/1.0mL)
Schedule: 0, 1, 6 months for susceptible individuals.
Dosage: 2 mL (20 mcg of Recombivax HB® or 40 mcg of
Engerix®-B)
Route of administration: IM
Pneumococcal Vaccine
Pneu-P-23 (23-valent pneumococcal
polysaccharide vaccine), and
Pneu-C-13 (13-valent conjugate
pneumococcal vaccine)
Formulations: Pneu-P-23 - Pneumovax® 23.
Pneu-C-13 - Prevnar13®
Schedule:
A) No prior Pneu-P-23: One dose of Pneu-C-13 followed eight
weeks later by Pneu-P-23. Then, a single Pneu-P-23 booster
five years later;
B) Previous Pneu-P-23: One dose of Pneu-C-13 at least one
year after any prior Pneu-P-23. A single Pneu-P-23 booster at
least five years after the initial Pneu-P-23 dose, and at least
eight weeks after Pneu-C-13.
Dosage: 0.5 mL.
Route of administration: polysaccharide vaccine may be given
subcutaneous (SC) or IM; conjugate vaccine must be given IM
Influenza Vaccine (Inactivated virus
vaccine)
Formulations: change annually; see BC Immunization Manual
(http://www.bccdc.ca/dis-cond/comm-
manual/CDManualChap2.htm)
Schedule: Single yearly injection
Dosage: 0.5 mL
Route of administration: IM
Td (Tetanus, diphtheria) - adsorbed Formulations: Td®
Schedule: Routine boosters every 10 years
Dosage: 0.5 mL
Route of administration: IM
* All publicly funded in B.C.

45
VACCINES INDICATED UNDER SPECIAL CIRCUMSTANCES (New subsection added
March 2015)
A. Measles, Mumps and Rubella (New subsection added March 2015)
Evidence:
In general, live-virus vaccines should not be used among HIV-positive individuals. In severely
immunocompromised populations, measles can present critically and in a prolonged fashion,
with a high risk for severe complications.82-85
Measles, Mumps, Rubella (MMR) vaccination in
HIV-positive individuals with CD4 cell counts >200 cells/mm3 appears to be safe with no
serious adverse events reported.86-88
Thus, all HIV-positive individuals without severe
immunosuppression (i.e. with CD4 cell count >200 cells/mm3) and no evidence of immunity to
measles, mumps or rubella should be considered for the MMR vaccine.14,89
Evidence of
immunity includes being born before 1970 or having previously received two doses of measles-
or mumps-containing vaccine. All HIV-positive individuals born before 1957 or who have
previously received one dose of rubella-containing vaccine, have serologic proof of immunity, or
have had prior lab confirmed rubella disease, are considered to have immunity against rubella.
Thus, serological testing may be indicated to confirm the diagnosis of measles, mumps or rubella
or to determine immune status. Serologic testing is not recommended before or after receiving
measles-, mumps- or rubella-containing vaccine. If serology is inadvertently done subsequent to
appropriate MMR immunization and does not demonstrate immunity, re-immunization is not
necessary.90
Recommendation:
1. All HIV-positive individuals without evidence of immunity and with CD4 cell counts
>200 cells/mm3 should be considered for measles and/or mumps and/or rubella
vaccination (given as a two dose series of MMR vaccine) (BII).
2. All HIV-positive individuals born before 1970 or who have previously received two
doses of measles- and mumps-containing vaccine, have serologic proof of immunity
against measles or rubella, or have had lab diagnosed disease, are considered to have
immunity against one or more of these diseases. If they are susceptible to one of these
diseases, the only vaccine available for use is measles, mumps and rubella vaccine.
MMR vaccine is safe for use in those with prior immunity (BII).
3. All HIV-positive individuals born before 1957 or who have previously received one
dose of rubella-containing vaccine, have serologic proof of immunity, or have had
prior lab confirmed rubella disease, are considered to have immunity against rubella
(AII).

46
B. Varicella (New subsection added July 2015)
Evidence:
At the time of publication of these guidelines, there were no published data on varicella
vaccination among susceptible HIV-positive individuals. However, based on expert opinion,
varicella vaccine may be safe to offer to susceptible individuals with CD4 counts >200
cells/mm3. Live attenuated varicella vaccine remains contraindicated in HIV-infected individuals
with CD4 counts <200 cells/mm3.
A varicella susceptible person is defined as someone who does not have a history of varicella or
herpes zoster after 12 months of age and not having a history of age-appropriate varicella
immunization. A self-reported history of varicella is adequate for those born before 2004; for
those born in 2004 and later, history of a diagnosis by a health care provider is required for
reliability. Children who have a history of either physician-diagnosed herpes zoster or lab-
confirmed varicella after their first dose of vaccine do not require a second dose. If disease
history is uncertain, provide a second dose.91
C. Herpes Zoster (New subsection added March 2015)
Evidence:
Herpes zoster, commonly known as shingles, is a cutaneous manifestation of the reactivation of
the varicella zoster virus (VZV), which causes chickenpox. The use of Zostavax II ® (a live
attenuated herpes zoster vaccine) in healthy HIV-negative adults aged 60 and older for
prevention of shingles is currently recommended by National Advisory Committee on
Immunization (NACI) in Canada.92
A study in immunocompetent older adults demonstrated that
vaccination with high potency live attenuated VZV vaccine reduces the frequency of herpes
zoster by half and its morbidity by two-thirds.93
Unfortunately, the same level of confidence in
Recommendation:
1. All HIV-positive individuals without evidence of immunity and with CD4 cell counts
>200 cells/mm3 may be considered for varicella vaccination (given as a 2-dose series
of varicella vaccine) (CIII).
Recommendation:
1. Herpes zoster vaccine is contraindicated in HIV-positive individuals with CD4 <200
cells/mm3. (BII)
2. The use of herpes zoster vaccine for prevention of shingles in HIV-positive adults with
CD4 >200 cells/mm3 is not routinely recommended. (BIII)

47
the safety, efficacy, and effectiveness in the ability of this vaccine to prevent shingles could not
be replicated directly in HIV-positive persons without rigorous research. It is also recognized
that shingles is common in HIV-positive individuals, in whom impaired cell-mediated immunity
may lead to increased incidence, severity, and complications of shingles.94-98
However, while
there are currently limited data to show the safety of vaccinating HIV-positive adults with CD4
>200 cells/mm3 against herpes zoster, some small cohorts have shown that two doses of VZV
vaccine were safe in HIV-infected subjects with CD4 ≥400 cells/mm3, but were only modestly
immunogenic.99,100
Thus, the vaccine’s efficacy in shingles prevention is yet to be clearly
demonstrated in HIV-positive persons. An evidence-based recommendation for the VZV vaccine
in all immunocompetent HIV-positive adults (i.e. with CD4 >200 cells/mm3) cannot be made at
this time. Since the VZV vaccine is a live vaccine, it is contraindicated in HIV-positive
individuals with CD4 <200 cells/mm3.
As in the general population, one’s risk of developing shingles increases with increasing age. It
will be prudent to revisit this topic as more research becomes available, since the life expectancy
of HIV-positive individuals is continuously improving in the era of antiretroviral therapy, with
many patients expected to live well into old age.
D. Human Papillomavirus (HPV) (New subsection added March 2015)
Evidence:
Human Papillomavirus (HPV) is a sexually transmitted pathogen that causes ano-genital disease
in males and females. The link between HPV and cervical cancer is well established: HPV DNA
is detected in 96.6% of cervical cancer tissue and the vast majority of cervical cancers can be
attributed to HPV infection.101
Based on both epidemiologic and phylogenetic data, the high-risk
HPV types for cervical cancer, in order of frequency, are: 16, 18, 33, 45, 31, 58, 52, and 35, and
probably high risk are: 51, 56, 39, and 59.102
Overall, 70% of cervical cancer cases are caused by
the two most common HPV types – 16 and 18 (high risk) – and 90% of genital warts are caused
by HPV 6 and 11 (low risk).103
The same HPV genotypes that cause cancer of the cervix also
cause most cases of anal cancer,104
a significant proportion of vulvar and vaginal cancer, and
penile cancer.
HIV-mediated immune suppression appears to facilitate HPV persistence and its oncogenic
potential. In part, this appears to be due to direct enhancement of HPV integration in the
presence of HIV.105
Recommendation:
1. HPV4 vaccine is recommended for HIV-positive girls and women (AII) and HIV-
positive boys and men (BII) between 9-26 years of age, regardless of their CD4
counts, to prevent infection caused by HPV types 6, 11, 16 and 18 and related
diseases. A 3-dose series is recommended, regardless of age. (AII)

48
In an international study, 77% of HIV-positive women had HPV detected at least once (incident
infection). HPV 16 was the most frequent genotype, with mixed infection seen in 26%.106
Persistent infection was seen in 41.5% of women. Canadian Women’s HIV study group found
high-risk HPV genotypes, as detected by genital tract sampling in HIV-infected women, with
62.1% of women being HPV-positive at least once for one or more of the twenty-seven HPV
types tested. An improved response to treatment for cervical dysplasia was observed for women
on highly active antiretroviral therapy (HAART).107
HIV-positive men who have sex with men (MSM) are at an increased risk for anal cancer, of
which 80% is caused by vaccine-preventable HPV. External genital warts can also be
challenging to treat in HIV-positive MSM, and are mostly due to vaccine-preventable HPV. The
quadrivalent human papillomavirus (HPV4) vaccine decreases risk of developing anal cancer
precursors (75%) and external genital warts (90%).108
Canada’s National Advisory Committee of
Immunization (NACI) recommends HPV4 vaccine for boys and men between 9-26 years of
age.109
Although the randomized controlled trial demonstrating these clinical outcomes excluded
HIV-positive men, HPV4 vaccine has been shown to be safe and immunogenic in HIV-positive
men.110
However, clinical efficacy data in HIV-positive individuals are lacking.
The prevalence of anal HPV is high among HIV-positive women.111
The clinical significance of
these findings is unclear, since anal cancer remains extremely rare in this population and the
clinical utility of anal Pap screening in HIV-positive women has not yet been determined at this
time.
Safety and efficacy data of the HPV vaccine in the context of HIV infection are sparse. There are
a few studies evaluating the immunogenicity of the HPV vaccine in HIV-positive men and
women.112,113
HPV4 vaccine appears safe, and immunogenic in the short term among young
women with HIV, including those with CD4 <200 cells/mm3.114,115
The long-term protection
level of these vaccines in HIV-positive women needs to be further studied, as there is some
preliminary evidence that HPV antibody levels in HIV-positive girls and women will decline
more rapidly compared to those in HIV-negative women.116
It may not be cost-effective to give HPV4 vaccine to boys if uptake in girls is high and provides
herd immunity.117
However, MSM may not benefit from herd immunity provided by vaccinated
girls and women. A recent British model suggested that at the current price of the HPV4 vaccine,
it would be cost effective to vaccinate HIV-positive MSM 16-40 years old (although certain
operational and delivery issues would need to be addressed).118
The CDC also reports cost-
effectiveness for vaccination of MSM through 26 years, referencing an analysis showing
<$50,000 per quality-adjusted life year.119
The quadrivalent HPV vaccine, Gardasil®, consisting of the L1 capsid protein of each of four
HPV strains (types 6, 11, 16 and 18), and the bivalent HPV vaccine, Cervarix™, consisting of
L1 capsid proteins of two HPV genotypes (HPV type 16 and HPV type 18), are available in
Canada. The 9-valent HPV vaccine (HPV9), which will cover additional strains (types 6, 11, 16,
18, 31, 33, 45, 52, 58), is expected to become available in the next couple of years.
HPV testing as an adjunct to Pap testing is not currently available in BC outside of research
settings.

49
Table 5. Vaccines provided free of charge to HIV-positive adults in British Columbia (New table
added August 2015)*
Vaccine Publicly Funded
Hepatitis A Vaccine (Inactivated virus
vaccine)
Yes
Hepatitis B Vaccine (Monovalent
recombinant DNA vaccine)
Yes
Pneumococcal Vaccine
PNEU-P-23 (23-valent pneumococcal
polysaccharide vaccine), and
PNEU-C-13 (13-valent conjugate
pneumococcal vaccine)
Yes
Influenza Vaccine (Inactivated virus
vaccine)
Yes
Td (Tetanus, diphtheria) - adsorbed Yes
Measles, Mumps, Rubella (MMR)
Vaccine
Yes
Varicella Vaccine Yes
Herpes Zoster Vaccine No
HPV Vaccine Yes, but limited. [HPV4 vaccine (Gardasil®) is free to females
aged 9-14 as part of routine immunization in grade 6, girls and
young women born in 1994 or later, and at-risk boys and young
men between 9 to 26 years of age. HPV2 vaccine (Cervarix®) is
ONLY free to young women who are 26 years old and younger
and born before 1994 through a one-time and time limited
program.]
*Note: Based on HealthLink BC’s Immunization Schedule for BC Adults, Seniors and Individuals at
High Risk120
CONTRAINDICATED VACCINES (New subsection added March 2015)
For HIV-positive individuals, live vaccines are either contraindicated or should be used with
caution in circumstances where the benefits of a live vaccination are likely to outweigh the risks.
Primary care providers may wish to consult with a physician with expertise in HIV or
immunization about offering such vaccines to their HIV-positive patients.
References
1. Public Health Agency of Canada and The Lung Association. Canadian tuberculosis standards. 7th edition. 2014.
Available from: http://www.respiratoryguidelines.ca/sites/all/files/Canadian_TB_Standards_7th_Edition_ENG.pdf
2. Sonnenberg P, Glynn JR, Fielding K, Murray J, Godfrey-Faussett P, Shearer S. How soon after infection with HIV
does the risk of tuberculosis start to increase? A retrospective cohort study in South African gold miners. J Infect
Dis 2005; 191(2): 150-158.

50
3. Kirk O, Gatell JM, Mocroft A, et al. Infections with mycobacterium tuberculosis and mycobacterium avium among
HIV-infected patients after the introduction of highly active antiretroviral therapy. EuroSIDA study group JD. Am J
Respir Crit Care Med 2000; 162(3 Pt 1): 865-872.
4. Badri M, Wilson D, Wood R. Effect of highly active antiretroviral therapy on incidence of tuberculosis in South
Africa: A cohort study. Lancet 2002; 359(9323): 2059-2064.
5. Huebner RE, Schein MF, Bass JB Jr. The tuberculin skin test. Clin Infect Dis 1993; 17(6): 968-975.
6. Sester M, van Leth F, Bruchfeld J, et al. Risk Assessment of Tuberculosis in Immunocompromised Patients - A
TBNET Study. Am J Respir Crit Care Med 2014; 190(10): 1168-1176.
7. Pai M, Zwerling A, Menzies D. Systematic review: T-cell-based assays for the diagnosis of latent tuberculosis
infection: an update. Ann Intern Med 2008; 149(3): 177-184.
8. Rangaka MX, Wilkinson KA, Seldon R, et al. Effect of HIV-1 infection on T-Cell-based and skin test detection of
tuberculosis infection. Am J Respir Crit Care Med 2007; 175(5): 514-520.
9. Elzi L, Steffen I, Furrer H, et al. Improved sensitivity of an interferon-gamma release assay (T-SPOT.TB™) in
combination with tuberculin skin test for the diagnosis of latent tuberculosis in the presence of HIV co-Infection.
BMC Infect Dis 2011; 11: 319.
10. BC Centre for Disease Control. TB Manual: Interferon Gamma Release Assay Testing Guideline for Diagnosis of
Latent Tuberculosis Infection by Physicians. 2014. Available from: http://www.bccdc.ca/NR/rdonlyres/F34F0725-
9087-457D-8059-F30BE18946C4/0/TB_manual_IGRA_guidelines.pdf
11. BC Centre for Excellence in HIV/AIDS. Therapeutic Guidelines for Opportunistic Infections. 2009. Available from:
http://www.cfenet.ubc.ca/therapeutic-guidelines/opportunistic-infection
12. Mtei L, Matee M, Herfort O, et al. High rates of clinical and subclinical tuberculosis among HIV-infected
ambulatory subjects in Tanzania. Clin Infect Dis 2005; 40(10): 1500-1507.
13. Woldehanna S, Volmink J. Treatment of latent tuberculosis infection in HIV infected persons. Cochrane Database
Syst Rev 2004; (1): CD000171.
14. Aberg JA, Gallant JE, Ghanem KG, Emmanuel P, Zingman BS, Hoberg MA. Primary care guidelines for the
management of persons infected with human immunodeficiency virus: 2013 update by the HIV Medicine
Association of the Infectious Diseases Society of America. Clin Infect Dis 2014; 58(1): e1-e34, doi:
10.1093/cid/cit655.
15. Porter SB, Sande MA. Toxoplasmosis of the central nervous system in the acquired immunodeficiency syndrome. N
Engl J Med 1992; 327(23): 1643-1648.
16. Public Health Agency of Canada. Canadian guidelines on sexually transmitted infections. 2014. Available from:
http://www.phac-aspc.gc.ca/std-mts/sti-its/cgsti-ldcits/index-eng.php
17. Public Health Agency of Canada. Canadian immunization guide. 2014. Available from: http://www.phac-
aspc.gc.ca/publicat/cig-gci/index-eng.php
18. Sun HY, Kung HC, Ho YC, et al. Seroprevalence of hepatitis A virus infection in persons with HIV infection in
Taiwan: Implications for hepatitis A vaccination. Int J Infect Dis 2009; 13(5): e199-205, doi:
10.1016/j.ijid.2008.12.009.
19. Centers for Disease Control and Prevention. Recommended adult immunization schedule - United States, 2009.
MMWR. 2008; 57.
20. Nunez M, Soriano V. Management of patients co-infected with hepatitis B virus and HIV. Lancet Infect Dis 2005;
5(6): 374-382.
21. Thio CL, Seaberg EC, Skolasky R. Jr, et al. HIV-1, hepatitis B virus, and risk of liver-related mortality in the
multicenter cohort study (MACS). Lancet 2002; 360(9349): 1921-1926.
22. Buxton JA, Yu A, Kim PH, et al. HCV co-infection in HIV-positive population in British Columbia, Canada. BMC
Public Health. 2010; 10: 225.
23. Hagan H. Hepatitis C virus transmission dynamics in injection drug users. Subst Use Misuse 1998; 33(5): 1197-
1212.
24. Lamothe F, Vincelette J, Bruneau J, et al. Prevalence, seroconversion rates and risk factors for hepatitis B core,
hepatitis C and HIV antibodies among intravenous drug users (IDU) of the Saint-Luc cohort (abstract 221) 6th
annual Canadian conference on HIV/AIDS research. Can J Infectious Diseases 1997; 8: 28A.
25. Patrick DM, Tyndall MW, Cornelisse PGA, et al. Incidence of hepatitis C virus infection among injection drug users
during an outbreak of HIV infection. CMAJ 2001; 165(7): 889-895.
26. Thein HH, Yi Q, Dore GJ, Krahn MD. Natural history of hepatitis C virus infection in HIV-infected individuals and
the impact of HIV in the era of highly active antiretroviral therapy: A meta-analysis. AIDS 2008; 22(15): 1979-1991.

51
27. Moore DM, Hogg RS, Braitstein P, Wood E, Yip B, Montaner JS. Risks of non-accidental mortality by baseline
CD4+ T-cell strata in hepatitis-C-positive and -negative individuals initiating highly active antiretroviral therapy.
Antivir Ther 2006; 11(1): 125-129.
28. Soriano V, Puoti M, Sulkowski M, et al. Care of patients coinfected with HIV and hepatitis C virus: 2007 updated
recommendations from the HCV-HIV international panel. AIDS 2007; 21(9): 1073-1089.
29. Rieg G, Lewis RJ, Miller LG, Witt MD, Guerrero M, Daar ES. Asymptomatic sexually transmitted infections in
HIV-infected men who have sex with men: Prevalence, incidence, predictors, and screening strategies. AIDS Patient
Care STDS 2008; 22(12): 947-954.
30. BC Centre for Disease Control. STI Annual Report. 2012. Available from:
http://www.bccdc.ca/NR/rdonlyres/408F1F9F-25AE-41B9-98E3-
9598E72E3015/0/STI_Annual_Report_2012FINAL.pdf
31. BC Centre for Disease Control. British Columbia Treatment Guidelines –Sexually Transmitted Infections in
Adolescents and Adults. 2014. Available from: http://www.bccdc.ca/NR/rdonlyres/46AC4AC5-96CA-4063-A563-
0BA9F4A0A6E9/0/CPS_BC_STI_Treatment_Guidelines_20112014.pdf
32. Public Health Agency of Canada. Canadian Guidelines on Sexually Transmitted Infections - Section 5 -
Management and Treatment of Specific Infections: Gonococcal Infections. 2015. Available from: http://www.phac-
aspc.gc.ca/std-mts/sti-its/cgsti-ldcits/section-5-6-eng.php#toc361210455
33. New York State Department of Health AIDS Institute. Management of STIs in HIV-infected patients. 2009.
Available from: http://www.hivguidelines.org/clinical-guidelines/adults/management-of-stis-in-hiv-infected-
patients/
34. Kaplan JE, Benson C, Holmes KH, et al. Guidelines for prevention and treatment of opportunistic infections in HIV-
infected adults and adolescents: Recommendations from CDC, the national institutes of health, and the HIV
medicine association of the Infectious Diseases Society of America. MMWR Recomm Rep 2009; 58(RR-4): 1-207;
quiz CE1-4.
35. New York State Department of Health AIDS Institute. Primary Care Approach to the HIV-Infected Patient. 2014.
Available from: http://www.hivguidelines.org/clinical-guidelines/adults/primary-care-approach-to-the-hiv-infected-
patient/
36. U.S. Department of Veterans Affairs. Primary Care of Veterans with HIV. 2011. Available from:
http://www.hiv.va.gov/provider/manual-primary-care/index.asp
37. van der Loeff MFS, Mooij SH, Richel O, de Vries HJ, Prins JM. HPV and Anal Cancer in HIV-Infected Individuals:
A Review. Curr HIV/AIDS Rep 2014; 11(3): 250-262.
38. Panel on Opportunistic Infections in HIV-Infected Adults and Adolescents. Guidelines for the prevention and
treatment of opportunistic infections in HIV-infected adults and adolescents: Recommendations from the Centers for
Disease Control and Prevention, the National Institutes of Health, and the HIV Medicine Association of the
Infectious Diseases Society of America. 2014. Available from:
http://aidsinfo.nih.gov/contentfiles/lvguidelines/adult_oi.pdf
39. BC Centre for Disease Control. HIV Laboratory Testing: a Resource for Health Professionals. 2010. Available from:
http://www.bccdc.ca/NR/rdonlyres/2982E293-BD82-436D-B193-
F929B5CEEBEC/0/HIVTestinginBCResourceDocumentforHealthProfessionalsJune2010.pdf
40. Overton ET, Nurutdinova D, Sungkanuparph S, Seyfried W, Groger RK, Powderly WG. Predictors of immunity
after hepatitis A vaccination in HIV-infected persons. J Viral Hepat 2007; 14(3): 189-193.
41. Jablonowska E, Kudowicz J, Malolepsza E. Efficacy of vaccination against hepatitis A in HIV infected adults from
Lodz region. Preliminary report. Przegl Epidemiol 2008; 62(3): 605-612.
42. Shire NJ, Welge JA, Sherman KE. Efficacy of inactivated hepatitis A vaccine in HIV-infected patients: A
hierarchical bayesian meta-analysis. Vaccine. 2006; 24(3): 272-279.
43. Flynn P, Ruddy B, Wilson C, et al. Improving seroresponse to hepatitis B vaccination in HIV-infected adolescents.
International AIDS Society Conference 2009. Poster abstract No. LBPEB11.
44. Fonseca MO, Pang LW, de Paula Cavalheiro N, Barone AA, Heloisa Lopes M. Randomized trial of recombinant
hepatitis B vaccine in HIV-infected adult patients comparing a standard dose to a double dose. Vaccine 2005;
23(22): 2902-2908.
45. Kim HN, Harrington RD, Van Roompaey SE, Kitahata MM. Independent clinical predictors of impaired response to
hepatitis B vaccination in HIV-infected persons. Int J STD AIDS 2008; 19(9): 600-604.
46. Launay O, Graber S, Gordier E, et al. Immunological efficacy of three-dose schedue of hepatitis A vaccine in HIV
infected adults: HEPAVAC study. J Acquir Immune Defic Syndr 2008; 49(3): 272-275.

52
47. Potsch DFV, Oliveira MLA, Miguel JC, et al. Alternative HBV vaccination schedule leads to higher seroconversion
rates among HIV-infected Brazilian subjects. International AIDS Society Conference 2008. Abstract No.
WEPE0200.
48. Sayana S, Prosser P, Javanbakht M, et al. Improved serological response to double-dose of hepatitis B vaccine in
HIV-infected patients. International AIDS Society Conference 2009. Abstract No. CDB059.
49. BC Centre for Disease Control. Chapter 1. Communicable Disease Control Manual. Chapter 1. Communicable
Disease Control, Hepatitis B. 2009. Available from: http://www.bccdc.ca/NR/rdonlyres/328189F4-2840-44A1-
9D13-D5AB9775B644/0/HepatitisB_Sept_2009.pdf
50. Ghandi RT, Wurcel A, Lee H, et al. Response to hepatitis B vaccine in HIV-1 positive subjects who test positive for
isolated antibody to hepatitis B core antigen: Implications for hepatitis B strategies. J Infect Dis 2005; 191(9): 1435-
1441.
51. Public Health Agency of Canada. Canadian Immunization Guide. Part 4: Active Vaccines – Hepatitis B Vaccine.
Available from: http://www.phac-aspc.gc.ca/publicat/cig-gci/p04-hepb-eng.php#immuno
52. Heffernan RT, Barrett NL, Gallagher KM, et al. Declining incidence of invasive streptococcus pneumoniae
infections among persons with AIDS in an era of highly active antiretroviral therapy, 1995-2000. J Infect Dis 2005;
191(12): 2038-2045.
53. Jordano Q, Falco V, Almirante B, et al. Invasive pneumococcal disease in patients infected with HIV: Still a threat
in the era of highly active antiretroviral therapy. Clin Infect Dis 2004; 38(11): 1623-1628.
54. Nuorti JP, Butler JC, Gelling L, Kool JL, Reingold AL, Vugia DJ. Epidemiologic relation between HIV and
invasive pneumococcal disease in San Francisco County, California. Ann Intern Med 2000; 132(3): 182-190.
55. Redd SC, Rutherford GW,3rd
, Sande MA, et al. The role of human immunodeficiency virus infection in
pneumococcal bacteremia in San Francisco residents. J Infect Dis 1990; 162(5): 1012-1017.
56. Rodriguez-Barradas MC, Goulet J, Brown S, et al. Impact of pneumococcal vaccination on the incidence of
pneumonia by HIV infection status among patients enrolled in the veterans aging cohort 5-site study. Clin Infect Dis
2008; 46(7): 1093-1100..
57. Madeddu G, Porqueddu EM, Cambosu F, et al. Bacterial community acquired pneumonia in HIV-infected inpatients
in the highly active antiretroviral therapy era. Infection 2008; 36(3): 231-236.
58. Malinis M, Myers J, Bordon J, et al. Clinical outcomes of HIV-infected patients hospitalized with bacterial
community-acquired pneumonia. Int J Infect Dis 2010; 14(1): e22-7, doi: 10.1016/j.ijid.2009.03.001.
59. Madeddu G, Laura Fiori M, Stella Mura M. Bacterial community-acquired pneumonia in HIV-infected patients.
Curr Opin Pulm Med 2010; 16(3): 201-207.
60. Lo YC, Lauderdale TL, Chang SY, Hsiao CF, Hung CC, Chang SC. Streptococcus pneumoniae colonization among
patients with human immunodeficiency virus-1 who had received 23-valent polysaccharide pneumococcal vaccine. J
Microbiol Immunol Infect 2009; 42(3): 234-242.
61. Hirschtick RE, Glassroth J, Jordan MC, et al. Bacterial pneumonia in persons infected with the human
immunodeficiency virus. Pulmonary complications of HIV infection study group. N Engl J Med 1995; 333(13): 845-
851.
62. Hung CC, Chang SY, Su CT, et al. A 5-year longitudinal follow-up study of serological responses to 23-valent
pneumococcal polysaccharide vaccination among patients with HIV infection who received highly active
antiretroviral therapy. HIV Med 2010; 11(1): 54-63.
63. Imaz A, Falco V, Penaranda M, et al. Impact of prior pneumococcal vaccination on clinical outcomes in HIV-
infected adult patients hospitalized with invasive pneumococcal disease. HIV Med 2009; 10(6): 356-363.
64. French N, Gordon SB, Mwalukomo T, et al. A Trial of a 7-Valent Pneumococcal Conjugate Vaccine in HIV-
Infected Adults. N Engl J Med 2010; 362(9): 812-822.
65. Feikin DR, Elie CM, Goetz MB, et al. Randomized trial of the quantitative and functional antibody responses to a 7-
valent pneumococcal conjugate vaccine and/or 23-valent polysaccharide vaccine among HIV-infected adults.
Vaccine 2001; 20(3-4): 545-553.
66. Tasslimi A, Sison EJ, Story E, et al. Disappearance of vaccine-type invasive pneumococcal disease and emergence
of serotype 19A in a minority population with a high prevalence of human immunodeficiency virus and low
childhood immunization rates. Clin Vaccine Immunol 2009; 16(8): 1256-1259.
67. Onwubiko C, Swiatlo E, McDaniel LS. Cross-sectional study of nasopharyngeal carriage of streptococcus
pneumoniae in human immunodeficiency virus-infected adults in the conjugate vaccine era. J Clin Microbiol 2008;
46(11): 3621-3625.
68. Lu CL, Hung CC, Chuang YC, et al. Serologic response to primary accination with 7-valent pneumococcal
conjugate vaccine is better than with 23-valent pneumococcal polysaccharide vaccine in HIV-infected patients in the
era of combination antiretroviral therapy. Hum Vaccin Immunother 2014; 9(2): 398-404.

53
69. Lesprit P, Pedrono G, Molina JM, et al. Immunological efficacy of a prime-boost pneumococcal vaccination in HIV-
infected adults. AIDS 2007; 21(18): 2425-34.
70. Lu C, Chang S, Chuang Y, et al. Revaccination with 7-valent pneumococcal conjugate vaccine elicits better
serologic response than 23-valent pneumococcal polysaccharide vaccine in HIV-infected adult patients who have
undergone primary vaccination with 23-valent pneumococcal polysaccharide vaccine in the era of combination
antiretroviral therapy. Vaccine 2014; 32(9): 1031-1035.
71. Crum-Cianflone NF, Huppler Hullsiek K, Roediger M, et al. A randomized clinical trial comparing revaccination
with pneumococcal conjugate vaccine to polysaccharide vaccine among HIV-infected adults. J Infect Dis 2010;
202(7): 1114-1125.
72. Cho B, Stoecker C, Link-Gelles R, Moore MR. Cost-effectiveness of administering 13-valent pneumococcal
conjugate vaccine in addition to 23-valent pneumococcal polysaccharide vaccine to adults with
immunocompromising conditions. Vaccine 2013; 31(50): 6011-6021.
73. National Advisory Committee on Immunization (NACI). Statement on the Use of Conjugate Pneumococcal Vaccine
-13 Valent in Adults (Pneu-C-13). Ottawa: public Health Agency of Canada; 2013: ACS-5.
74. Lin JC, Nichol KL. Excess mortality due to pneumonia or influenza during influenza seasons among persons with
acquired immunodeficiency syndrome. Arch Intern Med 2001; 161(3): 441-446.
75. Tasker SA, Treanor JJ, Paxton WB, Wallace MR. Efficacy of influenza vaccination in HIV-infected persons. A
randomized, double-blind, placebo-controlled trial. Ann Intern Med 1999; 131(6): 430-433.
76. Fine AD, Bridges CB, De Guzman AM, et al. Influenza A among patients with human immunodeficiency virus: An
outbreak of infection at a residential facility in New York City. Clin Infect Dis 2001; 32(12): 1784-1791.
77. Heffelfinger JD, Patel P, Brooks JT, et al. Pandemic influenza: Implications for programs controlling for HIV
infection, tuberculosis, and chronic viral hepatitis. Am J Public Health 2009; 99 Suppl 2: S333-9.
78. National Advisory Committee on Immunization. Recommendations on the use of live, attenuated influenza vaccine
(FluMist®): Supplemental statement on seasonal influenza vaccine 2011-2012. CCDR 2011; 37(ACS-7).
79. BC Centre for Disease Control. Communicable Disease Control Manual. Chapter 2: Immunization, Section VII:
Biological Products. 2014. Available from: http://www.bccdc.ca/dis-cond/comm-manual/CDManualChap2.htm
80. National Advisory Committee on Immunization (NACI). Canadian Immunization Guide. Part 4: Active Vaccines -
Diphtheria Toxoid. Ottawa: Public Health Agency of Canada; 2006. Available from: http://www.phac-
aspc.gc.ca/publicat/cig-gci/p04-dip-eng.php
81. Varughese P. Diphtheria in Canada – surveillance summary. Can Dis Wkly Rep 1978; 4: 65-68.
82. McLean HQ, Fiebelkorn AP, Temte JL, Wallace GS, Centers for Disease Control and Prevention. Prevention of
measles, rubella, congenital rubella syndrome, and mumps, 2013: Summary recommendations of the Advisory
Committee on Immunization Practices (ACIP). MMWR Recomm Rep 2013; 62(RR-04): 1-34.
83. Markowitz LE, Chandler FW, Roldan EO, et al. Fatal measles pneumonia without rash in a child with AIDS. J
Infect Dis 1988; 158(2): 480-483.
84. Palumbo P, Hoyt L, Demasio K, Oleske J, Connor E. Population-based study of measles and measles immunization
in human immunodeficiency virus-infected children. Pediatr Infect Dis J 1992; 11(12): 1008-1014.
85. Kaplan LJ, Daum RS, Smaron M, McCarthy CA. Severe measles in immunocompromised patients. JAMA 1992;
267(9): 1237-1241.
86. Sprauer MA, Markowitz LE, Nicholson JK, et al. Response of human immunodeficiency virus-infected adults to
measles-rubella vaccination. J Acquir Immune Defic Syndr 1993; 6(9): 1013-1016.
87. Abzug MJ, Qin M, Levin MJ, et al. Immunogenicity, immunologic memory, and safety following measles
revaccination in HIV-infected children receiving highly active antiretroviral therapy. J Infect Dis 2012; 206(4): 512-
522.
88. Scott P, Moss WJ, Gilani Z, Low N. Measles Vaccination in HIV-Infected Children: Systematic Review and Meta-
Analysis of Safety and Immunogenicity. J Infect Dis 2011; 204: S164-S178.
89. U.S. Department of Health and Human Services. Guide for HIV/AIDS clinical care. 2014. Available from
http://hab.hrsa.gov/deliverhivaidscare/2014guide.pdf.
90. Public Health Agency of Canada. Canadian Immunization Guide. Part 4: Active Vaccines –Serologic Testing. 2015.
Available from: http://www.phac-aspc.gc.ca/publicat/cig-gci/p04-meas-roug-eng.php#immuno
91. Public Health Agency of Canada. Canadian Immunization Guide. Part 4: Active Vaccines –Varicella (Chickenpox)
Vaccine. 2015. Available from: http://www.phac-aspc.gc.ca/publicat/cig-gci/p04-vari-eng.php
92. National Advisory Committee on Immunization (NACI). Statement on the recommended use of herpes zoster
vaccine. Canada Communicable Disease Report, 36(ACS-1): 1–19. 2010. Available from: http://www.phac-
aspc.gc.ca/publicat/ccdr-rmtc/10vol36/acs-1/index-eng.php

54
93. Oxman MN, Levin MJ, Johnson GR, et al. A vaccine to prevent herpes zoster and postherpetic neuralgia in older
adults. N Engl J Med 2005; 352(22): 2271-2284.
94. Glesby MJ, Moore RD, Chaisson RE. Clinical spectrum of herpes zoster in adults infected with human
immunodeficiency virus. Clin Infect Dis 1995; 21(2): 370-375.
95. Veenstra J, Krol A, van Praag RM, et al. Herpes zoster, immunological deterioration and disease progression in
HIV-1 infection. AIDS 1995; 9(10): 1153-1158.
96. Engels EA, Rosenberg PS, Biggar RJ. Zoster incidence in human immunodeficiency virus-infected hemophiliacs
and homosexual men, 1984-1997. District of Columbia gay cohort study. Multicenter hemophilia cohort study. J
Infect Dis 1999; 180(6): 1784-9.
97. Blank LJ, Polydefkis MJ, Moore RD, Gebo KA. Herpes zoster among persons living with HIV in the current
antiretroviral therapy era. J Acquir Immune Defic Syndr 2012; 61(2): 203-207.
98. Gebo KA, Kalyani R, Moore RD, Polydefkis MJ. The incidence of, risk factors for, and sequelae of herpes zoster
among HIV patients in the highly active antiretroviral therapy era. J Acquir Immune Defic Syndr 2005; 40(2): 169-
174.
99. Weinberg A, Levin MJ, MacGregor RR. Safety and immunogenicity of a live attenuated varicella vaccine in VZV-
seropositive HIV-infected adults. Hum Vaccin 2010; 6(4): 318-321.
100. Benson C, Hua L, Andersen J, et al. Zostavax is generally safe and immunogenic in HIV+ adults virologically
suppressed on ART: results of a phase 2, randomized, double-blind, placebo-controlled trial. Conference on
Retroviruses and Opportunistic Infections, Seattle, Washington, 2012. Abstract No. 96.
101. Baylor MS, Johann-Liang R. Hepatotoxicity associated with nevirapine use. J Acquir Immune Defic Syndr 2004;
35(5): 538-539.
102. Stanley M. Immune responses to human papillomavirus. Vaccine 2006; 24: S16-22.
103. Roy M, Bryson P. Treatment of external genital warts and pre-invasive neoplasia of the lower tract. J Obstet
Gynaecol Can 2007; 29[8]: S37-S41.
104. Hoots BE, Palefsky JM, Pimenta JM, Smith JS. Human Papillomavirus Type Distribution in Anal Cancer and Anal
Intraepithelial Lesions. Int J Cancer 2009; 124(10): 2375-2383.
105. de Sanjose S, Palefsky J. Cervical and anal HPV infections in HIV-positive women and men. Virus Res 2002; 89(2):
201-211.
106. Dartell M, Rasch V, Kahesa C, et al. Human Papillomavirus Prevalence and Type Distribution in 3603 HIV-Positive
and HIV-Negative Women in the General Population of Tanzania: The PROTECT Study. Sex Transm Dis 2012;
39(3): 201-208.
107. Darwich L, Canadas M, Sirera G, et al. Human Papillomavirus Genotype Distribution and Human Papillomavirus 16
and Human Papillomavirus 18 Genomic Integration in Invasive and In Situ Cervical Carcinoma in Human
Immunodeficiency Virus-Infected Women. Int J Gynecol Cancer 2011; 21(8): 1486-1490.
108. Giuliano AR, Palefsky JM, Goldstone S, et al. Efficacy of Quadrivalent HPV Vaccine against HPV Infection and
Disease in Males. N Engl J of Med 2011; 364(5): 401–11.
109. National Advisory Committee on Immunization (NACI). Update on the Recommended Human Papillomavirus
(HPV) Vaccine Immunization Schedule - An Advisory Committee Statement (ACS). Public Health Agency of
Canada. 2015. Available from: http://www.phac-aspc.gc.ca/naci-ccni/acs-dcc/2015/hpv-vph_0215-eng.php
110. Wilkin T, Lee JY, Lensing SY, et al. Safety and Immunogenicity of the Quadrivalent Human Papillomavirus
Vaccine in HIV‐1–Infected Men. J Infect Dis 2010; 202(8): 1246-1253.
111. Piketty C, Kazatchkine MD. Human papillomavirus-related cervical and anal disease in HIV-infected individuals in
the era of highly active antiretroviral therapy. Curr HIV/AIDS Rep 2005; 2(3): 140-145.
112. Wilkin T, Lee JY, Lensing SY, et al. Safety and immunogenicity of the quadrivalent human papillomavirus vaccine
in HIV-1-infected men. J Infect Dis 2010; 202(8): 1246-1253.
113. De Vuyst H, Franceschi S. Human papillomavirus vaccines in HIV-positive men and women. Curr Opin Oncol
2007; 19(5): 470-475.
114. Mujugira A, Morrow RA, Celum C, et al. Performance of the Focus HerpeSelect-2 enzyme immunoassay for the
detection of herpes simplex virus type 2 antibodies in seven African countries. Sex Transm Infect 2011; 87(3): 238-
241.
115. Kojic EM, Kang M, Cespedes MS, et al. Immunogenicity and Safety of a Quadrivalent Human Papillomavirus
Vaccine in HIV-1-Infected Women. Clin Infect Dis 2014; 59(1): 127-135.
116. Money D, Moses E, Raboud J, et al. Immunogenicity of the Quadrivalent HPV Vaccine in HIV Positive Women.
International Workshop on HIV and Women, from Adolescence to Menopause 2015.

55
117. Brisson M, van de Velde N, Franco EL, Drolet M, Boily MC. Incremental Impact of Adding Boys to Current
Human Papillomavirus Vaccination Programs: Role of Herd Immunity. J Infect Dis 2011; 204(3): 372-376.
118. Joint Committee on Vaccination and Immunisation. Interim Statement on HPV Vaccination of Men Who Have Sex
with Men. 2014. Available from:
https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/373531/JCVI_interim_statement_HP
V_vacc.pdf
119. Kim JJ. Targeted Human Papillomavirus Vaccination of Men Who Have Sex with Men in the USA: A Cost-
Effectiveness Modelling Analysis. The Lancet Infect Dis 2010; 10(12): 845-52.
120. HealthLink BC. “BC Immunization Schedules”. 2015. Available from:
http://www.healthlinkbc.ca/toolsvideos/immunization/.

56
V. Schedule of Care for HIV-positive Individuals
Evidence:
The frequency of clinical and laboratory follow-up of HIV-positive individuals is dependent on
stage of HIV disease, rate of disease progression, overall clinical stability, the presence of co-
morbidities, and the need for other services offered in the clinic. Regular monitoring is important
because individuals engaged in care are more likely to be adherent to their medications and have
improved health outcomes.1 Moreover, risk of virologic failure decreases with duration of viral
suppression.2-4
Recent evidence indicates that, for patients receiving stable antiretroviral therapy
with consistently undetectable plasma viral loads and adequate CD4 cell counts, routine CD4 cell
count monitoring is not medically necessary5; CD4 monitoring in this setting is now optional
according to recent international guidelines.6,7
Since CD4 cell counts have been a cornerstone of
HIV management in the past, patient education around this issue may be necessary to alleviate
stress and confusion, particularly in long-term survivors of HIV. CD4 monitoring should be
resumed if the plasma viral load becomes consistently detectable or if there is any significant
change in the patient’s clinical condition related to HIV or co-morbid conditions.
All antiretroviral agents are associated with potential adverse effects, which can lead patients to
switch or cease therapy.8 Certain factors may increase the risk of adverse effects for some
individuals, such as gender, age, baseline CD4 count, concomitant medical conditions, genetics,
and interactions with other medications. Individuals at a higher risk of developing adverse effects
are often under-represented in clinical trials, resulting in uncertainty around the frequency and
Recommendations:
1. All HIV-positive individuals who are not on antiretroviral therapy should have CD4
cell counts and plasma viral loads (pVL) measured every 3-4 months. (BII)
2. All individuals initiating antiretroviral therapy should have CD4 cell counts and pVL
measured on a monthly basis until pVL is <40 copies/mL, and thereafter monitoring
can occur every 3-4 months. (BII)
3. In clinically stable patients with dependable antiretroviral adherence, once pVL is
consistently <40 copies/mL for two years and CD4 counts are consistently ≥350
cells/mm³, pVL monitoring can occur at intervals of up to six months and CD4
monitoring is optional. (CIII)
4. Safety laboratory parameters (complete blood count, renal and liver function, fasting
lipids, and glucose) should be monitored approximately one month after initiation of
antiretroviral therapy (with the first pVL and CD4 count) and every 3-6 months
thereafter (see Table 6 on p. 57). Monitoring should be undertaken more frequently in
the presence of relevant underlying co-morbid conditions, known potential toxicities of
specific antiretroviral drugs, and/or concomitant medications. (CIII)

57
severity of adverse events in real-life clinical settings. Clearly, the presence of co-morbid
conditions and/or concomitant medications, as well as the known toxicities of certain
antiretroviral medications, need to be taken into consideration when determining the appropriate
frequency of laboratory safety monitoring during antiretroviral therapy.
Age, in particular, is a key factor in determining frequency of follow-up. There has been an
increase in the proportion of HIV-positive individuals who are over the age of 50 years; this
population is more likely to experience a faster progression of HIV disease and is less likely to
be routinely evaluated for antiretroviral therapy.9,10
In addition, higher rates of co-morbid
conditions and antiretroviral toxicities have been observed in older HIV-positive individuals.11,12
This requires a shift from focusing solely on CD4 cell counts, plasma viral loads, and AIDS-
defining illnesses to a more comprehensive care model that is focused on managing a complex,
chronic disease.13
Table 6. Laboratory Monitoring* (Table revised March 2015)
Test Baseline First 2 years
after ART
initiation*
After 2 years on
stable suppressive
ART*
Hematologic
Assessment
Complete blood count (CBC)
with differential and platelet
count
√ With first pVL
(after 1 month),
then every 3-4
months
Every 6 months
HIV plasma
viral load
(pVL)
HIV RNA √ Monthly until <40
copies/mL, then
every 3-4 months
Every 6 months
CD4 cell
count,
absolute and
percentage
√ Monthly until
pVL<40
copies/mL, then
every 3-6 months
Once CD4 is
consistently >350
cells/mm3,
monitoring is
optional
Renal
Function
Creatinine, estimated
glomerular filtration rate
(eGFR), phosphate,
urinalysis, spot urine for
albumin to creatinine ratio
(UACR)
√ With first pVL
(after 1 month),
then every 3-4
months
Every 6 months
Liver Tests Spot urine for albumin to
creatinine ratio (UACR),
alanine aminotransferase
(ALT), aspartate
aminotransferase (AST),
total bilirubin, international
normalized ratio (INR)
√ With first pVL
(after 1 month),
then every 3-4
months
Every 6 months
Table continued on next page…

58
Test Baseline First 2 years
after ART
initiation*
After 2 years on
stable suppressive
ART*
Fasting Lipid
Profile**
Total cholesterol (TC), high
density cholesterol (HDL),
low-density lipoprotein
(LDL), triglycerides (TG),
and/or apolipoprotein B
√ With first pVL
(after 1 month),
then every 6
months
Every 6 months
Blood
Glucose§
Fasting glucose and/or
HbA1C
√ With first pVL
(after 1 month),
then every 6
months
Every 6 months
*Frequency of laboratory monitoring may be adjusted according to medical history of relevant co-morbid
conditions, potential toxicities of specific antiretroviral drugs and concomitant medications, previous or
ongoing laboratory abnormalities, and clinical status. In most cases the timing of safety laboratory
monitoring can be coordinated with monitoring of HIV RNA and CD4 cell counts.
**The Canadian Cardiovascular Society recognizes HIV as a significant risk factor for premature
cardiovascular disease and as an indication for screening for cardiovascular risk factors, including lipids.
In addition, some ARV agents may contribute to dyslipidemia. Apolipoprotein B (apoB) levels should be
monitored, particularly in patients with high triglyceride levels (AIII).14
§ Diabetes mellitus (DM) is more prevalent in the HIV-positive population than in the general population,
particularly in the setting of hepatitis C co-infection. DM risk may be exacerbated by certain antiretroviral
medications. The Canadian Diabetes Association recommends monitoring fasting blood glucose and/or
glycated hemoglobin (HbA1C).15
References
1. Mugavero MJ, Lin HY, Willig JH, et al. Missed visits and mortality among patients establishing initial outpatient
HIV treatment. Clin Infect Dis 2009; 48(2): 248-256.
2. Reekie J, Mocroft A, Ledergerber B, et al. History of viral suppression on combination antiretroviral therapy as a
predictor of virological failure after a treatment change. HIV Med 2010; 11(7): 469-478.
3. Lima VD, Bangsberg DR, Harrigan PR, et al. Risk of viral failure declines with duration of suppression on highly
active antiretroviral therapy irrespective of adherence level. J Acquir Immune Defic Syndr 2010; 55(4): 460-465.
4. Lodwick RK, Smith CJ, Youle M, et al. Stability of antiretroviral regimens in patients with viral suppression. AIDS
2008; 22(9): 1039-1046.
5. Ford N, Meintjes G, Pozniak A, et al. The future role of CD4 cell count for monitoring antiretroviral therapy. Lancet
Infect Dis 2015; 15(2): 241-247.
6. Gunthard HF, Aberg JA, Eron JJ, et al. Antiretroviral treatment of adult HIV infection: 2014 recommendations of
the International Antiviral Society-USA panel. JAMA 2014; 312(4): 410-25.
7. U.S. Department of Health and Human Services. Guidelines for the use of antiretroviral agents in HIV-1-infected
adults and adolescents. 2015:1-288. Available from:
http://aidsinfo.nih.gov/contentfiles/lvguidelines/adultandadolescentgl.pdf
8. O'Brien ME, Clark RA, Besch CL, Myers L, Kissinger P. Patterns and correlates of discontinuation of the initial
HAART regimen in an urban outpatient cohort. J Acquir Immune Defic Syndr 2003; 34(4): 407-414.
9. Kirk JB, Goetz MB. Human immunodeficiency virus in an aging population, a complication of success. J Am
Geriatr Soc 2009; 57(11): 2129-2138.
10. Effros RB, Fletcher CV, Gebo K, et al. Aging and infectious diseases: Workshop on HIV infection and aging: What
is known and future research directions. Clin Infect Dis 2008; 47(4): 542-553.

59
11. Orlando G, Meraviglia P, Valsecchi L, et al. cART durability and causes for treatment switching or discontinuation
in HIV-positive patients older than 50 years of age. J Acquir Immune Defic Syndr 2010; 55(2): e12-4. doi:
10.1097/QAI.0b013e3181ef791b.
12. Shah SS, McGowan JP, Smith C, Blum S, Klein RS. Comorbid conditions, treatment, and health maintenance in
older persons with human immunodeficiency virus infection in New York City. Clin Infect Dis 2002; 35(10): 1238-
1243.
13. Justice AC. HIV and aging: Time for a new paradigm. Curr HIV/AIDS Rep 2010; 7(2): 69-76.
14. Anderson TJ, Gregoire J, Hegele RA, et al. 2012 Update of the Canadian Cardiovascular Society guidelines for the
diagnosis and treatment of dyslipidemia for the prevention of cardiovascular disease in the adult. Can J Cardiol
2013; 29(2): 151-167.
15. Canadian Diabetes Association Clinical Practice Guidelines Expert Committee. Canadian Diabetes Association
2013 Clinical Practice Guidelines for the Prevention and Management of Diabetes in Canada. Can J Diabetes 2013;
37: S1-212.

60
VI. Special Consideration for Women and Transgender† Individuals with HIV
A. Introduction
In Canada in 2012, 23.3% of the 71,300 HIV-positive known cases were among women.1 An
estimate of 1,682 HIV-positive women are known to currently live in British Columbia.2 Women
may inherit social roles and responsibilities as caretakers for extended family members and
friends, and may not give sufficient priority to their own medical care. Furthermore, heterosexual
women frequently face unequal power and socioeconomic relationships with their male partners.
These social factors may increase women’s isolation and depression, and compromise their
adherence.
Transgender populations are disproportionately affected by HIV. A worldwide meta-analysis
shows rates of HIV infections of up to 27% among transgender women (excluding those
involved in sex work).3
The indications for and goals of antiretroviral therapy (ART) are the same for people of any
gender, unless pregnancy is desired.6 Various studies have suggested that sex may influence the
frequency, presentation, and severity of some ART-related adverse events.7 Although data are
limited, evidence also suggests that pharmacokinetics for some ARV drugs may differ between
men and women,8 possibly due to differences between men and women in factors such as body
weight, plasma volume, hormones, gastric emptying time, plasma protein levels, cytochrome P
(CYP) 450 activity, drug transporter function, and excretion activity.9-11
Several studies indicate that women experience metabolic complications associated with ART
use differently than men. These metabolic differences have not been studied in transgender
people, but presumably hormonal therapy could shift metabolic responses into a more male or
female pattern for those using masculinizing or feminizing therapies, respectively. HIV-positive
women are more likely to experience increases in central fat and are at a higher risk of
developing particular patterns of lipodystrophy than their male counterparts.12
However, women
are less likely to have triglyceride elevations on treatment.13
In addition, women have an
increased risk of osteopenia/osteoporosis, particularly after menopause, and this risk may be
exacerbated by HIV and ART.14,15
(See also F. Menopause on p. 64, as well as Section VII: Non-
Infectious Co-morbidities on p. 69).
†
In this section, the term women refers to self-identified women, whose biological sex, external genitalia, or sex
assigned at birth match their gender identity. Transgender women refers to self-identified women, whose biological
sex, external genitalia, or sex assigned at birth does not match the gender by which they identify. Transgender men
refers to self-identified men, whose biological sex, external genitalia, or sex assigned at birth does not match the
gender by which they identify (adapted from United States Centers for Disease Control and Prevention4 and Bauer et
al.5). For more information on the care of transgender individuals, see Transgender Primary Medical Care:
Suggested Guidelines for Clinicians in British Columbia
(http://lgbtqpn.ca/wp-content/uploads/woocommerce_uploads/2014/08/Guidelines-primarycare.pdf).

61
B. Special Considerations Related to Care before, during, and after Pregnancy
Evidence:
Preconception
Approximately 80% of HIV-positive women are of childbearing age. Since perinatal HIV
transmission can be prevented by the appropriate use of antiretroviral therapy, health care
providers should discuss menstrual history, safe sexual practices, pregnancy desires, and
contraceptive practices with their female patients at each visit. The goal of these discussions is to
ensure that patients make informed decisions about pregnancy, contraception, and reproductive
health, and to prevent unintended pregnancies. HIV status of the sexual partner should be
Recommendations:
1. Contraception and pregnancy plans should be discussed with all individuals of
childbearing potential upon initiation of HIV care and routinely thereafter, as
pregnancy may affect the choice and timing of antiretrovirals. (AIII) Contraceptive
counselling should also be included as a critical aspect of postpartum care. (AIII)
2. Preconception counselling in HIV-positive individuals is recommended for anyone
contemplating pregnancy, especially in the setting of HIV-serodiscordant couples.
(BII)
3. Pregnancy in HIV-positive individuals is considered a high risk and complex;
therefore, consultation with or referral to an obstetrician experienced in HIV is highly
recommended. (BIII)
4. All HIV-positive pregnant individuals should be treated with ART for HIV infection,
regardless of their immunologic or virologic status, to prevent infection of their fetus.
(AI) ART should be continued after delivery and reassessed by providers of adult HIV
care. (AII)
5. Breastfeeding is not recommended, regardless of HIV viral load and use of ART, for
HIV-positive individuals in Canada. (AI)
6. Clinicians should avoid prescribing efavirenz, or any new under-studied drug, during
the first trimester of pregnancy, to anyone who wishes to become pregnant, and to
individuals of childbearing potential who are not using effective and consistent
contraception. A pregnancy test should be done before initiation of efavirenz in
individuals of childbearing potential and counselling should be provided on the
potential risk to the fetus while the mother is receiving on efavirenz. (AIII)
7. Clinicians should not prescribe nevirapine to antiretroviral-naïve women or trans-
masculine individuals who have CD4 cell counts >250 cells/mm3, nor start nevirapine
during pregnancy (AI)

62
discussed. Pregnancy history should include the number of pregnancies and outcomes
(miscarriage, ectopic, preterm, term), significant obstetrical complications, number of living
children, and the individual’s general state of health.
In anyone at risk for pregnancy (not using effective and consistent contraception), providers
should carefully review all medications and avoid drugs with potential reproductive toxicity. The
time of greatest risk to the fetus is the first trimester, often before pregnancy is even recognized.
Efavirenz (in Sustiva® and Atripla® as well as generic forms) has been associated with
teratogenic effects in non-human primates, and there are reports of central nervous system
abnormalities in human infants exposed to efavirenz during the first trimester.16
If pregnancy is
desired, preconception counselling with a specialized infectious disease obstetrician is
recommended, especially for HIV serodiscordant couples who can be counselled about ways to
reduce transmission to the uninfected partner while trying to conceive. In British Columbia, such
services can be obtained from the Oak Tree Clinic in Vancouver: www.oaktreeclinic.bc.ca or
604-875-2212.
During pregnancy
Pregnancy in HIV-positive individuals is considered a high risk and complex. Therefore,
consultation with an obstetrician specialising in the management of HIV is recommended. The
use of ART and the resultant reduction of maternal HIV viral load decrease perinatal
transmission of HIV. The goal of ART in pregnancy is to achieve maximal and sustained
suppression of the HIV RNA levels during pregnancy and delivery.17-19
The risk of teratogenic events of efavirenz was recently estimated using data from the Women’s
Interagency HIV Study. The study found that the rate of teratogenic events was 77.26/100,000 in
women exposed to efavirenz, compared with 72.46/100,000 in unexposed women.16
If a pregnant
individual presents after week 12 on efavirenz, it is not recommended to change the regimen, but
rather to refer to an obstetrician who is experienced in managing high risk pregnancies as early
as possible, for neural tube follow-up and further management of HIV in pregnancy.
Nevirapine has been associated with an increased risk of symptomatic, potentially fatal, and
often rash-associated liver toxicity among antiretroviral-naïve individuals. Those with higher
CD4 cell counts appear to be at greatest risk: a meta-analysis of nevirapine-related clinical trials
found that, in women, a CD4 cell count of >250 cells/mm3 at the time of nevirapine initiation
was associated with a 9.8-fold increase in symptomatic hepatic events compared with lower CD4
cell counts.16
Introducing nevirapine during pregnancy resulted in higher rates of toxicity and is
not recommended.20,21
Due to limited data on the use of tenofovir disoproxil fumarate (DF) in human pregnancy and
concerns about potential fetal bone effects, tenofovir DF should be used in pregnancy only after
careful consideration and consultation with an HIV specialist. Potential long-term effects of
newer ART agents on the fetus or newborn are not known.
Post partum (New subsection added August 2015)
Following delivery, clinical, immunologic, and virologic follow-up should continue as
recommended for non-pregnant adults and adolescents. Because use of ART during lactation

63
reduces but does not eliminate the risk of transmission of HIV in breast milk, and because
postnatal transmission can occur despite parental ART, HIV-positive women should also be
counselled to avoid breastfeeding.22
HIV-infected adults should avoid pre-mastication of food
fed to their infants because the practice has been associated with transmission of HIV from
parent to child.23
Considerations regarding continuation of ART for therapeutic indications
during pregnancy are the same as those for ART use in non-pregnant individuals.22,23
Discontinuation of ART postpartum is no longer recommended.6
Several studies have demonstrated that adherence to ART may worsen in the postpartum
period.24,25
Clinicians caring for postpartum individuals who receive ART should specifically
address adherence, including an evaluation of specific facilitators and barriers to adherence.
C. Contraception in the Context of HIV
Evidence:
The incidence and prevalence of gynaecological problems are high among HIV-positive
individuals throughout the course of their HIV disease.26
At the initial patient assessment, a
comprehensive gynaecologic history should be obtained, including menstrual history, sexual
practices, contraceptive history, current status and consistency of contraceptive use, sexually
transmitted infections (STIs) and treatments, and prior abnormal Pap results, including
subsequent tests and treatments. History of gynaecological conditions such as uterine fibroids,
endometriosis, infertility, and surgeries should be obtained. Current gynaecological symptoms
such as vaginal discharge, bleeding, amenorrhea, odour, dysuria, itchiness, dyspareunia, and
pelvic pain should also be assessed. Mid-cycle bleeding and recurrent urinary tract infections
should prompt an evaluation for STIs if appropriate. Most women and transmasculine
individuals with gonorrhoea and chlamydia (GC) infections will be asymptomatic. For
recommendations regarding GC screening, see pp. 35-36 of Section IV: Screening and
Immunization for Selected Co-morbid Infections.
Several protease inhibitors (PIs) and non-nucleoside reverse transcriptase inhibitors (NNRTIs)
have significant drug interactions with combined oral contraceptives. Drug interactions can lead
to a decrease or an increase in blood levels of ethinyl estradiol and/or norethindrone or
norgestimate, which in turn can potentially decrease contraceptive efficacy or increase estrogen-
or progestin-related adverse effects, including thrombo-embolic risk (see Table 7 on p. 65).
Several ritonavir-boosted protease inhibitors (PIs) decrease oral contraceptive estradiol levels.
Although there is minimal information about drug interactions with the use of newer combined
Recommendations:
1. Health care providers should be aware of common interactions between ART and
medications taken for contraception, which may lower contraceptive efficacy and may
result in unintended pregnancy. (AII)
2. Intrauterine devices (IUDs) can be considered as a safe and effective contraception
option for HIV-positive women and adolescents. (BII)

64
hormonal contraceptive methods (e.g. transdermal patch, vaginal ring), an additional or
alternative contraceptive method should also be considered on the basis of established drug
interactions between antiretroviral agents and oral contraceptives. There is limited data on drug
interactions between antiretroviral agents and progestin-only contraceptive methods; however,
recent studies have found no significant changes in antiretroviral drug concentrations of
nelfinavir, nevirapine, or efavirenz when used with depot medroxyprogesterone acetate (DMPA),
and there is no evidence of reduced DMPA effectiveness.27,28
Contraindications to combined
hormonal methods, such as diabetes mellitus, hyperlipidemia, and chronic liver disease, are more
common in HIV-positive individuals. In general, those who are on PIs or NNRTIs should use an
alternative or additional method of contraception (e.g. barrier methods). For a summary of drug-
drug interactions between ARVs and hormonal contraceptives, see Table 7 on p. 65. For
recommendations on the use of hormonal contraceptives among women who are HIV-positive or
at a high risk of acquiring HIV, see the World Health Organization’s 2014 guidance statement
(http://apps.who.int/iris/bitstream/10665/128537/1/WHO_RHR_14.24_eng.pdf). For a list of
interactions between ARVs and hormonal contraceptives, see the tables in the Toronto General
Hospital’s Immunodeficiency Clinic’s guide
(http://www.hivclinic.ca/main/drugs_interact_files/Oral%20Contraceptive-int.pdf).
Regardless of contraception use, condom or other barrier use should be recommended with each
sexual act. Condoms reduce the risk of pregnancy, STIs, and superinfection with different HIV
strains. Barrier methods may reduce risk of HIV infection by approximately 69%,29
but are
associated with high rates of failure and are not welcomed by many men. No randomized trials
comparing the clinical effectiveness of external (male) and internal (female) condoms for the
prevention of HIV have been performed. Use of internal condoms can provide protection from
acquisition and transmission of STIs, although data are limited.30,31
Internal condoms offer an
option for individuals and couples who cannot or will not use the traditional condom. Patients
should be counselled about the greater effectiveness of condoms when used with a second
method of protection.
In the past, intrauterine devices (IUDs) were not considered as an option for contraception due to
fears of pelvic inflammatory disease and infections among immunocompromised women.
However, with improved ARVs and earlier initiation of ART, current evidence supports the
safety and efficacy of IUDs in HIV-positive women, and this option should be considered,
especially for women with CD4 >200 cells/mm3. Cervical infections should be treated prior to
the insertion of the IUD. The data are still sparse. Most studies have focused on non-hormonal
IUDs (copper IUDs); several small studies have found the levonorgestrel-releasing IUDs to be
safe and not associated with increased genital shedding of HIV.33-34
For a more detailed
discussion of recommendations for the use of IUDs among women who are HIV-positive or at a
high risk of acquiring HIV, see the Society of Obstetrician and Gynaecologists of Canada
Committee’s 2014 guidelines on Best Practices to Minimize Risk of Infection With Intrauterine
Device Insertion
(http://sogc.org/guidelines/best-practices-minimize-risk-infection-intrauterine-device-insertion/)
or the WHO’s guidance statement
(http://apps.who.int/iris/bitstream/10665/128537/1/WHO_RHR_14.24_eng.pdf).

65
Table 7. Hormonal Contraceptives and ARV Interactions (New table added August 2015, adapted from University of Liverpool).
Protease Inhibitors NNRTIs Integrase Inhibitors NRTIs
ATV/r DRV/r FPV/r IDV/r LPV/r SQV/r EFV ETV NVP RPV MVC DTG EVG/c RAL ABC FTC 3TC TDF ZDV
Estrogen
Ethinylestradiol Estradiol Progestins
Desogestrel Drospirenone Dydrogestrone Etonogestrel Gestodene Levonorgestrel Medroxy-
progesterone (IM)
Medroxy-
progesterone (oral)
Norelgestromin Norethisterone
(Norethindrone)
Norgestimate Norgestrel Other
Levonogestrel (EC) Mifepristone Ulipristal
Text Legend Colour Legend
Potential increased exposure to the hormone No clinically significant interaction expected
Potential decreased exposure to the hormone Potential interaction which may require a dose adjustment or close monitoring
No significant effect Potential interaction predicted to be of weak intensity. No dosage adjustment required.
Potential increased exposure of HIV drug

66
D. Screening for Cervical and Breast Cancer in HIV-positive Individuals
Evidence:
Abnormal cervical cytology is ten times more prevalent in HIV-positive individuals compared
with the general population, and is associated with the presence of Human Papilloma Virus
(HPV) infection and the degree of immune dysfunction. More frequent Pap smears should be
considered in the following circumstances:
If there is a previous history of an abnormal Pap smear (atypical squamous cells, either of
unknown significance [ASC-US] or low grade intraepithelial lesion [LSIL], or high grade
[ASC-H, or HSIL], or squamous carcinoma)
In those with known HPV infection
In those with CD4 <200 cells/mm3
In HIV-positive individuals who have had a hysterectomy, and history of abnormal
cervical cytology before or at the time of the procedure. These individuals are at an
increased risk for pathological lesion and should undergo screening with vault Pap
smears.35
Although the appropriate interval for screening has not been established, it is
reasonable to follow guidelines similar to those for those who have not undergone a
hysterectomy, or once yearly.
For transgender patients on testosterone, make sure to mark this on the cytology requisition for
accurate results. Screening for STIs (including gonorrhea, chlamydia, trichomonas, bacterial
vaginosis, syphilis, and herpes) should be performed at routine gynaecological visits and when
symptomatic or considered at risk. For more details about BC cervical screening
recommendations for women and transgender people in the general population, see the BC
Cancer Agency’s website (http://www.screeningbc.ca/Cervix/default.htm).
Recommendations:
1. Cervical Pap smear should be done for any individual with a cervix starting at age 21
or 3 years after first sexual contact, whichever occurs first. For those eligible HIV-
positive individuals cervical screening should be done upon initiation of care, and
should be repeated 6 months later. If results are normal in both tests, cervical Pap
smear should be done annually thereafter. (AI) If Pap smear results are abnormal, the
individual should be referred for colposcopy and directed biopsy, as recommended by
the BC Cancer Agency, with further treatment as indicated by results. (AII)
2. Breast cancer screening for HIV-positive people should follow provincial guidelines
for the general population. (AII) Consider screening in transgender women on long-
term hormone replacement >5 years, and in transgender men and others who may have
had mastectomy for non-cancer related reasons.

67
Breast cancer risk is not increased in HIV-positive individuals and therefore screening should
follow provincial guidelines for those who are not infected with HIV (see the BC Cancer
Agency’s Physician Protocol for Screening Mammograms,
http://www.screeningbc.ca/NR/rdonlyres/AA527AF1-6F8E-40DE-84DA-
E2397FC29C9D/68351/SMPPhysicianProtocolsVersionFebruary2014Web.pdf). For guidelines
on breast cancer screening among transgender individuals who are HIV-positive, see the
Canadian Cancer Agency’s website
(http://convio.cancer.ca/site/PageServer?pagename=SSL_ON_T_Home#.VaBZE-t9SXv).
E. Human Papillomavirus (HPV)
See Section IV: Screening and Immunization for Selected Co-morbid Infections, Part 2:
Immunization, H. Human Papillomavirus (HPV) (pp. 45-46).
F. Menopause
Evidence:
An increasing number of HIV-positive women are living past menopausal age or are becoming
infected when they are over 50. In Canada, women over 50 years of age constitute 8.5% of the
HIV-positive population.36
Menopause may be diagnosed clinically as 12 months of amenorrhea
in a woman over age 45 years in the absence of other biological or physiological causes.37
There
are currently no randomized controlled trials delineating the use of hormonal replacement
therapy in HIV-positive women. There are conflicting data on the effect of HIV on menopausal
age and symptoms. Factors that can influence menopausal symptoms, including smoking, stress,
drug use, low body mass index, and race/ethnicity, are also relatively more prevalent among
HIV-positive populations. A review of age at menopause in HIV-positive women did not find
conclusive data to affirm early menopause in HIV-positive women. However, sample size was
limited in these studies and larger studies are required to determine if there is early ovarian
failure in HIV-positive women, and whether it is related to the virus, to antiretrovirals, to
lifestyle, or to genetic factors.38
There is an increased risk of premature bone loss (osteopenia and osteoporosis) during and after
menopause. The prevalence of osteoporosis in HIV-positive women is three times greater
Recommendations:
1. Hormone replacement therapy may be considered in patients who experience severe
menopausal symptoms (i.e. vasomotor symptoms and vaginal dryness) but should
generally be used only for a limited period of time and at the lowest effective doses.
(BII)
2. Hormone replacement for HIV-positive transgender individuals should be provided in
consultation with an endocrinologist or other clinician who has experience providing
endocrine care to transgender individuals.

68
compared with HIV-uninfected women in the same age group in the United States.14
The
pathogenesis of the reduced bone mineral density noted in HIV-positive individuals is most
likely multi-factorial, with risk increased by some ART (tenofovir DF, efavirenz, protease
inhibitors), as well as by HIV itself. Traditional risk factors for osteoporosis, including smoking,
menstrual irregularities (oligomenorrhea and amenorrhea), substance abuse, and low body
weight, are more common in HIV-positive individuals. As per provincial guidelines, periodic
bone density screening every 3-5 years starting at age 50 (or at any age if there is a fragility
fracture) should be offered to postmenopausal women (in BC, the Medical Services Plan [MSP]
covers every 3 years), especially if they are receiving tenofovir DF.39
For additional information
on management of bone loss please refer to the discussion on bone health in Section VII: Non-
infectious Co –morbidities (pp. 72-73).
Sexual practices in menopausal women are not well described. In a study from the British
Columbia Centre for Disease Control (BCCDC), 53% of 48 women who self-identified as
menopausal reported being sexually active in the previous 6 months, and 30% of them reported
having unprotected sex.40
Thus, it is important for physicians to discuss safer sex practices with
individuals of all ages and to consider HIV diagnosis in women above the age of 45 years and
those who are menopausal.
References
1. Public Health Agency of Canada. Population-Specific HIV/AIDS Status Report: People Living with HIV/AIDS.
Chapter 2 – Epidemiological Profile of HIV and AIDS in Canada. 2015. http://www.phac-aspc.gc.ca/aids-
sida/publication/ps-pd/people-personnes/chapter-chapitre-2-eng.php#a2-3
2. BC Centre for Excellence in HIV/AIDS. HIV monitoring quarterly report for British Columbia: Second Quarter.
Updated Nov 28, 2014. Available from:
http://www.cfenet.ubc.ca/sites/default/files/uploads/publications/centredocs/monitoring_bc_2013q2_updated_2014-
nov-28-2.pdf
3. Baral SD, Poteat T, Stromdahl S, Wirtz AL, Guadamuz TE, Beyrer C. Worldwide burden of HIV in transgender
women: a systematic review and meta-analysis. The Lancet Infect Dis 2013; 13(3): 214-222.
4. US Centers for Disease Control and Prevention (CDC). HIV Among Transgender People.
http://www.cdc.gov/hiv/group/gender/transgender/index.html
5. Bauer GR, Travers R, Scanlon K, Coleman TA. High heterogeneity of HIV-related sexual risk among transgender
people in Ontario, Canada: a province-wide respondent-driven sampling survey. BMC Pub Health 2012; 12: 292.
6. U.S. Department of Health and Human Services. Guidelines for the use of antiretroviral agents in HIV-1-infected
adults and adolescents. 2014:1-161. Available from:
http://www.aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf.
7. Clark RA, Squires KE. Gender-specific considerations in the antiretroviral management of HIV-infected women.
Expert Rev Anti Infect Ther 2005; 3(2): 213-227.
8. Loutfy MR, Walmsley SL, Klein MB, Raboud J, Tseng AL, Blitz SL, Pick N, et al. Factors affecting antiretroviral
pharmacokinetics in HIV-infected women with virologic suppression on combination antiretroviral therapy: a cross-
sectional study. BMC Infect Dis 2013; 3(13): 256.
9. Gandhi M, Aweeka F, Greenblatt RM, Blaschke TF. Sex differences in pharmacokinetics and pharmacodynamics.
Annu Rev Pharmacol Toxicol 2004; 44: 499-523.
10. Floridia M, Giuliano M, Palmisano L, Vella S. Gender differences in the treatment of HIV infection. Pharmacol Res
2008; 58(3-4): 173-192.
11. Ofotokun I, Chuck SK, Hitti JE. Antiretroviral pharmacokinetic profile: a review of sex differences. Gend Med
2007; 4(2): 106-119.
12. Galli M, Veglia F, Angarano G, et al. Gender differences in antiretroviral drug-related adipose tissue alterations.
Women are at higher risk than men and develop particular lipodystrophy patterns. J Acquir Immune Defic Syndr
2003; 34: 58-61.

69
13. Thiebaut R, Dequae-Merchadou L, Ekouevi DK, et al. Incidence and risk factors of severe hypertriglyceridaemia in
the era of highly active antiretroviral therapy: The Aquitaine cohort, France, 1996-99. HIV Med 2001; 2: 84-88.
14. Brown TT, Qaqish RB. Antiretroviral therapy and the prevalence of osteopenia and osteoporosis: A meta-analytic
review. AIDS 2006; 20: 2165-2174.
15. Yin M, Dobkin J, Brudney K, et al. Bone mass and mineral metabolism in HIV+ postmenopausal women.
Osteoporos Int 2005; 16: 1345-1352.
16. Hsu H, Rydzak C, Cotich K, et al. Quantifying the risks and benefits of efavirenz use in HIV-infected women of
childbearing age in the USA. HIV Med 2010.
17. Ioannidis JP, Abrams EJ, Ammann A, et al. Perinatal transmission of human immunodeficiency virus type 1 by
pregnant women with RNA virus loads <1000 copies/ml. J Infect Dis 2001; 183(4): 539-545.
18. Mofenson LM, Lambert JS, Stiehm ER, et al; for Pediatric AIDS Clinical Trials Group Study 185 Team. Risk
factors for perinatal transmission of human immunodeficiency virus type 1 in women treated with zidovudine. N
Engl J Med 1999; 341(6): 385-393.
19. Garcia PM, Kalish LA, Pitt J, et al; for the Women and Infants Transmission Study Group. Maternal levels of
plasma human immunodeficiency virus type 1 RNA and the risk of perinatal transmission. N Engl J Med 1999;
341(6): 394-402.
20. van Schalkwyk JE, Alimenti A, Khoo D, et al. Serious toxicity associated with continuous nevirapine-based
HAART in pregnancy. BJOG 2008; 115: 1297-1302.
21. Hitti J, Frenkel LM, Stek AM, et al. Maternal toxicity with continuous nevirapine in pregnancy: Results from
PACTG 1022. J Acquir Immune Defic Syndr 2004; 36: 772-776.
22. Department of Human and Health Services. Recommendations for Use of Antiretroviral Drugs in Pregnant HIV-1-
Infected Women for Maternal Health and Interventions to Reduce Perinatal HIV Transmission in the United States.
2014. Available at: http://aidsinfo.nih.gov/contentfiles/lvguidelines/perinatalgl.pdf
23. Gaur AH, Freimanis-Hance L, Dominguez K, et al. Knowledge and practice of prechewing/prewarming food by
HIV- infected women. Pediatrics 2011; 127(5): e1206-1211.
24. Nachega JB, Uthman OA, Anderson J, Peltzer K, Wampold S, Cotton MF, et al. Adherence to antiretroviral therapy
during and after pregnancy in low-income, middle-income, and high-income countries: a systematic review and
meta-analysis. AIDS 2012; 26: 2039-52.
25. Kaida A, Forrest J, Money D, Burdge D, Forbes J, Fernandes K, et al. Antiretroviral adherence during pregnancy
and postpartum among HIV-positive women enrolled in the Drug Treatment Program in British Columbia, Canada.
Paper presented at: 18th Annual Canadian Conference on HIV/AIDS Research; April 23-26, 2009; Vancouver. Can
J Infect Dis Med Microbiol 2009; 20(B): 25B.
26. Minkoff HL, Eisenberger-Matiyahu D, Feldman J, Burk R, Clarke L. Prevalence and incidence of gynecologic
disorder among women infected with HIV. Am J obstet Gynecol 1990; 180: 824-836.
27. Nanda K, Amaral E, Hays M, Viscola MA, Mehta N, Bahamondes L. Pharmacokinetic interactions between depot
medroxyprogesterone acetate and combination antiretroviral therapy. Fertil Steril 2008; 90: 965-971.
28. Watts DH, Park JG, Cohn SE, et al. Safety and tolerability of depot medroxyprogesterone acetate among HIV-
infected women on antiretroviral therapy: ACTG A5093. Contraception
29. 2008; 77: 84-90.
30. Weller SC. A meta-analysis of condom effectiveness in reducing sexually transmitted HIV. Soc Sci Med 1993; 36:
1635-1644.
31. Vijayakumar G, Mabude Z, Smit J, Beksinska M, Lurie M. A review of female-condom effectiveness: Patterns of
use and impact on protected sex acts and STI incidence. Int J STD AIDS 2006; 17: 652-659.
32. French PP, Latka M, Gollub EL, Rogers C, Hoover DR, Stein ZA. Use-effectiveness of the female versus male
condom in preventing sexually transmitted disease in women. Sex Transm Dis 2003; 30: 433-439.
33. Heikinheimo O, Lehtovirta P, Aho I, Ristola M, Paavonen J. The levonorgestrel-releasing intrauterine system in
human immunodeficiency virus-infected women: a 5-year follow-up study. Am J Obstet Gynecol 2011; 204(2): 126
e121-124.
34. Heikinheimo O, Lahteenmaki P. Contraception and HIV infection in women. Hum Reprod Update 2009; 15(2): 165-
176.
35. Lehtovirta P, Paavonen J, Heikinheimo O. Experience with the levonorgestrel-releasing intrauterine system among
HIV- infected women. Contraception 2007; 75(1): 37-39.
36. Paramsothy P, Duerr A, Heilig CM, et al. Abnormal vaginal cytology in HIV-infected and at-risk women after
hysterectomy. J Acquir Immune Defic Syndr. 2004; 35: 484-491.

70
37. Public Health Agency of Canada. HIV and AIDS in Canada: Surveillance report to December 31, 2012. Centre for
Communicable Diseases and Infection Control: Public Health Agency of Canada; 2013. Available from:
http://publications.gc.ca/collections/collection_2014/aspc-phac/HP37-2-2012-eng.pdf
38. Burger HG. Unpredictable endocrinology of the menopause transition: clinical, diagnostic and management
implications. Menopause Int 2011; 17(4): 153-154.
39. Conde DM, Pinto-Neto AM, Costa-Paiva L. Age at menopause of HIV-infected women: A review. Gynecol
Endocrinol 2008; 24: 84-86.
40. Yin MT, Zhang CA, McMahon DJ, Ferris DC, Irani D, Colon I, Cremers S, Shane E. Higher rates of bone loss in
postmenopausal HIV-infected women: a longitudinal study. J Clin Endocrinol Metab 2011; 97(2): 554-562.
41. Pick NOG. Sexual lifestyle behaviour of menopausal HIV+ women compared to reproductive age group peers.
Canadian Association for HIV Research. 2007.

71
VII. Common Non-Infectious Co-Morbidities (New Subsections March 2015)
A. Introduction
A number of conditions not traditionally associated with AIDS, including cardiovascular and
renal disease, are exacerbated in the presence of uncontrolled HIV replication.1 Therefore,
despite the potential for long-term complications due to chronic antiretroviral therapy, the
benefits outweigh the potential risks in HIV-positive individuals who are appropriately treated
and monitored.2 To this end, clinical and laboratory assessment of relevant co-morbid conditions
should be performed at baseline before initiation of antiretroviral therapy and during follow-up.
Screening for long-term complications of antiretroviral therapy is described in Appendix 5 (pp.
112-113).
The frequency of lab monitoring for antiretroviral toxicity depends on the known potential
toxicities of specific drugs, concomitant medications, and underlying co-morbid conditions. Lab
monitoring may occur every four weeks after initiation of therapy, decreasing to up to every six
months after stabilization of the patient on their antiretroviral regimen.3 In most cases the timing
of safety laboratory monitoring can be coordinated with monitoring of HIV RNA and CD4 cell
counts.
B. Cardiovascular disease
Evidence:
As in the general population, cardiovascular disease (CVD) is a common cause of morbidity and
mortality in HIV-positive individuals. It was the second most common cause of death in the
HIV-positive participants of the SMART trial (after non-AIDS defining cancers).1 Uncontrolled
HIV infection, including during antiretroviral therapy interruption, is associated with an
unfavourable lipid profile and increased risk of cardiovascular events.1,4
However, antiretrovirals
are also associated with increased CVD risk, with the rate of cardiovascular events increasing by
16% per year of exposure to antiretroviral therapy, particularly protease inhibitors.5 This
Recommendations:
1. All HIV-positive individuals should be screened for risk of cardiovascular disease at
least annually, and modifiable cardiovascular risk factors should be addressed where
possible. (AI)
2. Assess fasting lipids (total, HDL, LDL cholesterol, and triglycerides) or apolipoprotein
B at baseline and every six months once patient begins antiretroviral therapy. (AIII)
3. An electrocardiogram (ECG) should be performed at baseline and monitored
periodically (at intervals determined by the degree of risk) in patients taking protease
inhibitors and/or rilpivirine with other PR- or QTc-prolonging drugs. (CIII)

72
antiretroviral-induced risk is not entirely explained by drug-induced dyslipidemia. The
antiretroviral-associated risk of CVD has decreased with the use of newer antiretroviral regimens
but can still be significant in patients with HIV, especially in the presence of other cardiovascular
risk factors, such as age and smoking.6,7
The Canadian Cardiovascular Society Guidelines
(http://www.onlinecjc.ca/article/S0828-282X%2812%2901510-3/pdf) recognizes HIV as a
significant risk factor for premature CVD and an indication for screening for cardiovascular risk
factors, including lipids.8 Antiretroviral therapy should not be stopped due to concern over
perceived high cardiovascular risk, e.g. to correct dyslipidemia.2,5
Apolipoprotein B (apoB) measurement is subject to less laboratory error than LDL cholesterol,
particularly in patients with hypertriglyceridemia (as often seen in HIV); therefore, this
parameter should be monitored where available and used as a treatment target (as an alternative
to LDL) per the Canadian Cardiovascular Society Guidelines.8
In the absence of a history of
severe hypertriglyceridemia, an apoB measurement can be used instead of fasting LDL
cholesterol for the assessment of cardiovascular risk and monitoring of patients on treatment.
Elevated levels of some inflammatory biomarkers, notably high-sensitivity C-reactive protein
(hsCRP), are independently associated with a higher risk of myocardial infarction in the HIV-
positive population, as in the general population.9,10
However, the interpretation of hsCRP can be
complicated in the setting of the chronic inflammatory state associated with HIV infection.
Although antiretroviral therapy reduces the levels of these biomarkers, they can remain elevated
compared with those of HIV-negative individuals. The clinical utility of these biomarkers for
initiation or monitoring therapy in the setting of HIV is unknown.
Despite the impact of antiretroviral therapy and HIV infection itself, traditional CVD risk factors
(including age, smoking, and gender) remain the most important contributors to CVD in this
population. The Framingham Risk Score, which has been validated in Canada, is the
recommended tool for assessing total CVD risk, but may underestimate cardiovascular risk in the
setting of HIV infection.8,11
The Reynolds Risk Score (www.reynoldsriskscore.org), which
incorporates family history and hsCRP as well as traditional cardiovascular risk factors, may be a
more accurate alternative, but has not yet been validated in a Canadian population nor in HIV.8
Regardless of underlying cardiovascular risk, modifiable risk factors should be aggressively
addressed in all HIV-positive individuals as in the general population, including smoking,
sedentary lifestyle, and excess weight.8 Smoking cessation is particularly critical and has been
demonstrated to reduce clinical CV events in a large HIV-positive population.2,12
Dyslipidemia,
where present, should be managed according to current general population guidelines, taking into
account potentially significant drug-drug interactions between lipid-lowering agents and
antiretrovirals (e.g. statins and protease inhibitors) (www.hiv-druginteractions.org).8 Of note,
HIV-positive individuals may not reach desirable lipid targets with conventional statin therapy
and combination therapy may be necessary.13
Some older HIV protease inhibitors (specifically saquinavir and lopinavir/ritonavir) were
associated with PR interval prolongation or QTc interval prolongation.14-16
Cardiac conduction
abnormalities may become clinically significant when a ritonavir-boosted protease inhibitor is
co-administered with one or more QTc-prolonging drugs such as methadone, quetiapine,

73
macrolides, quinolones, and/or azoles (for a full list, see the CredibleMeds website at
https://www.crediblemeds.org/index.php), or PR-prolonging drugs (e.g. digitalis, calcium
channel blockers, anti-arrhythmics, and beta-blockers). Also, the non-nucleoside reverse
transcriptase inhibitor rilpivirine was associated with QTc prolongation at daily doses of 75 mg
or 150 mg, although this does not appear to be a problem at the 25 mg daily dose currently in
use.17-19
An electrocardiogram (ECG) should be performed at baseline before starting a ritonavir-
boosted protease inhibitor and/or rilpivirine with one or more PR- or QTc-prolonging drugs. A
repeat ECG should be performed approximately five half-lives after starting the relevant drug,
i.e. approximately two days after starting atazanavir/ritonavir, three days after starting
darunavir/ritonavir, or ten days after starting rilpivdirine. In addition, an ECG should be done
after the addition or dose increase of any other QTc-prolonging drug and at times of increased
risk (e.g. hypokalemia, hypomagnesemia). Repeat ECG monitoring should be performed at
intervals determined by the degree of risk, i.e. whether the QTc is short (<0.41 seconds),
borderline (0.42-0.44 seconds), or prolonged (>0.45 seconds).20
C. Insulin resistance (IR) and diabetes mellitus (DM)
Evidence:
Diabetes mellitus (DM) is more prevalent in the HIV-positive population than in the general
population, particularly in those who are co-infected with hepatitis C.2,21,22
Insulin resistance (IR)
is associated with use of some nucleoside reverse transcriptase inhibitors and protease inhibitors,
but may be transient; clinical hyperglycemia is less common than dyslipidemia in this setting,
occurring in less than 5% of protease inhibitor-treated individuals. The evidence is inconclusive
that switching antiretrovirals will improve glucose tolerance.2 Traditional risk factors for DM
remain relevant in HIV-positive individuals. HbA1c may be monitored as an alternative to
fasting blood glucose, particularly if fasting status is difficult to ascertain; however, HbA1c can
be misleading in certain anemic conditions (e.g. iron deficiency) and in situations where
erythrocyte half-life is reduced (e.g. recent transfusion, hemolysis, or blood loss) or increased
(e.g. asplenia).2, 23
Recommendations:
1. Fasting blood glucose (FBG) and/or glycated hemoglobin (HbA1c) should be
performed in all HIV-positive individuals at baseline and at six-month intervals during
antiretroviral therapy. Abnormalities in fasting glucose and/or HbA1c should be
evaluated and managed according to the Canadian Diabetes Society guidelines
(http://guidelines.diabetes.ca/). (AIII)
2. Initial management of blood glucose abnormalities in HIV-positive individuals
involves lifestyle changes (weight loss, diet, exercise). (AIII)
3. Oral anti-glycemic agents and injectable anti-glycemic agents (insulin, glucagon-like
peptide-1[GLP-1] receptor agonists) should be used as required, keeping in mind drug
interactions with some antiretrovirals. (AIII)

74
D. Bone disease
Evidence:
HIV-positive individuals are at a greater risk of fractures than non-infected individuals.24
The
loss of bone density associated with normal aging is accelerated by HIV infection and by
exposure to antiretrovirals.25
The role of specific antiretrovirals in causing bone loss is
controversial and inconsistent; however, most recent evidence points to tenofovir DF and
possibly ritonavir-boosted protease inhibitors as the leading culprits.26,27
Efavirenz has also been
implicated as a contributor to low bone mass, mediated through its effect on vitamin D
metabolism.28
There are currently no validated or widely accepted North American guidelines for screening,
assessing, monitoring, or treating low bone mineral density (BMD) in HIV-positive individuals.
When using dual energy X-ray absorptiometry (DXA) scan data to assess BMD in HIV-positive
individuals, clinicians should use caution in the interpretation of T-scores, and the Z-score is
probably preferable in this population.29
Osteoporosis cannot be diagnosed using DXA alone in
Recommendations:
1. Clinicians should undertake preventive measures for bone loss in all HIV-positive
individuals, including weight-bearing exercises, maintaining ideal weight, reducing
smoking and alcohol consumption, and optimizing vitamin D and calcium intake (in
the form of diet and supplements). (AIII)
2. Vitamin D supplementation should be considered for all HIV-positive individuals (e.g.
1000-2000 IU/day). (BIII)
3. Clinicians should consider performing a baseline dual energy X-ray absorptiometry
(DXA) scan to assess bone mineral density for HIV-positive women who are post-
menopausal and in all HIV positive men aged 50 years and older, and in patients of
any age with a history of fragility fractures or significant risk factors for osteoporosis
(http://www.osteoporosis.ca/health-care-professionals/guidelines/) (BIII).
4. DXA scan should be repeated at intervals according to local provincial guidelines.
(BIII)
5. For HIV-positive transgender people who have undergone gender-affirming
interventions, such as hormone therapy or gonadectomy, clinicians should refer to
appropriate resources for guidance on osteoporosis screening. (CIII)
6. If decreased bone density is diagnosed, secondary causes such as hypogonadism,
alcoholism, glucocorticoid exposure, and vitamin D deficiency should be investigated
and treated appropriately, including referral to a specialist if necessary. (AIII)

75
men aged less than 50 years or in premenopausal women; in fact, many experts feel that a DXA
scan is generally not indicated in this population unless patients have a fragility fracture or
another risk factor – although in this context, HIV may be considered a sufficient risk
factor.26,30,31
With or without DXA results, a patient’s ten-year risk of fracture can be assessed using the
WHO Fracture Risk Assessment tool (http://www.sheffield.ac.uk/FRAX/); however, this
instrument has not been validated for use in patients with HIV.
For HIV-positive transgender people, different methods of prevention and screening for
osteoporosis are needed, depending on the type and duration of gender-affirming interventions,
such as hormone therapy or gonadectomy. Clinicians should refer to appropriate resources for
guidance (http://transhealth.ucsf.edu/trans?page=protocol-screening#S6X). For HIV-positive
transgender people who have not undergone any medical or surgical transition, clinicians should
follow guidelines based on birth sex.
Most HIV patients have low vitamin D levels, as does the general North American population;
therefore, there is insufficient evidence to support routine measurement of vitamin D levels in
HIV-positive individuals.32,33
While there is no consensus regarding the optimal dose in the
setting of HIV, supplementation with vitamin D at doses of 1000 to 2000 international units (IU)
daily is inexpensive, safe, and not associated with known interactions with antiretroviral drugs. If
dietary calcium intake is inadequate, a calcium supplement should be considered, taking into
consideration potential interactions with antiretrovirals.
E. Renal disease
Evidence:
Renal dysfunction is frequently seen in HIV-positive individuals, especially as they age. The risk
for renal disease is increased by black race, age over 50 years, past or family history of kidney
Recommendations:
1. Due to the risk of renal disease related to HIV and antiretroviral medications, it is
recommended that blood pressure and laboratory assessment of renal function (serum
creatinine and phosphate, estimated glomerular filtration rate [eGFR], urinalysis for
protein and sediment, and spot urine for albumin to creatinine ratio [UACR]) should be
performed in all HIV-positive individuals at baseline and every 3-4 months after
starting antiretrovirals, increasing to six-month intervals when stable (depending on
degree of risk). (AIII)
2. In case of renal dysfunction, clinicians should adjust doses of medications, including
antiretrovirals that are cleared by the kidney. An exception is tenofovir DF, which
should be avoided in patients with or at high risk of renal disease, and replaced with
another agent in the presence of clinically significant renal dysfunction. (AII)

76
disease, advanced HIV disease (low CD4 nadir), nephrotoxic medication use including
recreational drugs, and certain co-morbidities (including diabetes mellitus, hypertension,
hepatitis B or C, and other liver disease).34
Classic HIV-associated nephropathy (HIVAN), due to
direct infection of renal epithelial cells with HIV, is relatively uncommon in British Columbia. It
is seen almost exclusively in blacks of West African or Haitian descent in association with
advanced HIV disease; as such, it is an indication for starting antiretroviral therapy regardless of
CD4 count.3 Despite a small potential for nephrotoxicity, overall large studies show that current
antiretroviral therapy is beneficial for renal function.1,35
Numerous forms of acute and chronic renal disease are seen in the setting of HIV:
HIV-related, e.g. thrombotic microangiopathy, immune complex glomerulonephritis, IgA
nephropathy
Secondary to co-morbid conditions, e.g. hepatitis B/C, hypertension, diabetes mellitus
Related to nephrotoxic medications (notably nonsteroidal anti-inflammatory drugs) including
some antiretrovirals, notably tenofovir DF and some ritonavir-boosted protease inhibitors53-56
Drug interactions, e.g. ritonavir-boosted protease inhibitors/statins (rhabdomyolysis and
myoglobinuria)
Certain etiologies of renal disease may also be related to antiretrovirals, specifically:
Risk of tubular dysfunction and renal phosphate wasting with tenofovir DF, especially in
patients with other risk factors or eGFR <90 mL/min at baseline34,40
Other NRTIs (didanosine, stavudine, and lamivudine) rarely associated with tubular disorders
Nephrolithiasis risk with indinavir and, less commonly, with atazanavir.41,42
Patients should
be advised to maintain adequate hydration to prevent kidney stones during treatment with
atazanavir or indinavir (the latter agent is not recommended in current treatment guidelines3).
Rarely, acute interstitial nephropathy with reversible acute renal failure has been described in
association with hypersensitivity reactions to abacavir, efavirenz, and atazanavir43
Establishing the etiology of renal dysfunction in HIV-positive individuals can be difficult as it is
often multi-factorial. Referral to a nephrologist and possibly renal biopsy may be required for a
definitive diagnosis, especially in cases where drug-related nephrotoxicity is suspected. Any
renal function abnormalities identified at screening should be investigated and managed
appropriately as in the general population. Some antiretrovirals (specifically all NRTIs except
abacavir) are renally cleared and may require dosage adjustment if renal function is abnormal.
For some drugs with low nephrotoxic potential (e.g. lamivudine), the beneficial effect of dose
adjustment has not been proven. However, tenofovir DF is renally cleared and is also a
nephrotoxin; this drug should be avoided in patients with renal disease or at high risk. If renal
dysfunction occurs during antiretroviral therapy, tenofovir DF should be discontinued if possible
and replaced with another agent (e.g. abacavir if HLA-B*5701 negative) rather than dose-
reduced.
Certain antiretroviral agents (dolutegravir, rilpivirine, raltegravir) and pharmacokinetic
enhancers (ritonavir, cobicistat) affect renal tubular creatinine transporters resulting in decreased
tubular creatinine secretion and increased serum creatinine levels.18,19,44-48
This is manifested as a
factitious increase in serum creatinine during the initial 2-4 weeks of therapy, without an effect
on true glomerular filtration rate. After the initial increase, serum creatinine levels remain stable

77
at the new higher level as long as the agent is continued. The mean increase in creatinine to be
expected on starting any of these agents is around 10-12 μmol/L for dolutegravir, rilpivirine, or
cobicistat, and approximately 5 μmol/L for raltegravir or ritonavir. If the serum creatinine
increase is much greater than expected (e.g. 20-30 μmol/L), is accompanied by any other signs of
renal dysfunction (e.g. proteinuria), or continues to increase after the first four weeks of a new
therapy, further renal investigations should be undertaken and nephrology referral should be
considered.
F. Hypogonadism (New subsection added March 2015)
Evidence
In the pre-highly active antiretroviral therapy (pre-HAART) era, hypogonadism was identified as
an important contributor to loss of lean body and muscle mass, the hallmarks of AIDS-associated
wasting, as well as decreased bone mineral density.49
While less prevalent in the HAART era,
low testosterone levels are still present in a significant minority of HIV-positive men.50
Symptoms suggestive of testosterone deficiency include decreased libido, erectile dysfunction,
hot flashes and sweats, weight loss, reduced muscle strength or exercise capacity, fragility
fractures, sleep disturbance, fatigue, and depression. HIV-positive men presenting with one or
more of these symptoms should be screened with a morning free testosterone level, and low
levels should be confirmed on repeat testing.2 An estimated bioavailable testosterone
measurement may be helpful to assess certain individuals, specifically obese men with borderline
low total testosterone levels. Normal serum testosterone levels in women are unknown.
Testosterone replacement therapy (TRT) is indicated only for men with symptomatic low
testosterone levels, and should be prescribed according to current guidelines, preferably in
consultation with an endocrinologist or other specialist.51
In HIV-positive men with
Recommendations:
1. HIV-positive men presenting with symptoms of hypogonadism (decreased libido,
erectile dysfunction, reduced bone mass or low trauma fractures, hot flashes or sweats,
weight loss, reduced muscle strength or exercise capacity, sleep disturbance, fatigue,
or depression) may be assessed with a morning serum total testosterone level; an
abnormal testosterone level should be confirmed with repeat testing. An estimated
bioavailable testosterone measurement may be helpful to assess certain individuals,
including obese men with borderline low total testosterone levels. (AII)
2. Testosterone replacement is indicated only for symptomatic men with total
testosterone levels less than 10 mmol/L, and should be prescribed in consultation with
a specialist. (AII)
3. Hormone replacement for HIV-positive transgender individuals should be provided in
consultation with an endocrinologist or other clinician who has experience providing
endocrine care to transgender individuals. (CIII)

78
hypogonadism, TRT has been shown to improve mood, energy, libido, muscle strength, and
body composition (specifically, decreasing fat and increasing muscle mass), without adverse
effects on viral load or CD4 cell count.49
However, there are no reliable data demonstrating that
TRT improves muscle mass, in excess of that achieved by physical exercise, or overall physical
function in men with HIV.52
Potential side effects of TRT include acne, male pattern balding, and sleep apnea. More serious
potential adverse effects include myocardial infarction (due to erythrocytosis) and prostate
cancer. TRT is contraindicated in men with acute coronary syndrome or prostate cancer. The
long-term safety of TRT is unknown; the need for ongoing TRT should be reassessed at least
every six months.51
G. Neurocognitive Impairment (New subsection added March 2015)
Evidence:
HIV can affect the central nervous system (CNS), impacting cognitive function (e.g. memory,
reasoning, planning, solving problems, attention, concentration) and activities of daily living.
Fortunately, the incidence of severe cognitive impairment in the form of HIV-associated
dementia has declined significantly since the advent of antiretroviral therapy. However, milder
forms of neurocognitive impairment remain prevalent, even in the presence of virologic
suppression, and can have a significant impact on quality of life and adherence to HIV
medications.53
HIV-positive individuals with impairment in two or more cognitive domains and mild to
moderate impairment in daily functioning, in the absence of confounding conditions, may be
diagnosed with mild neurocognitive disorder.54
Potential underlying conditions that need to be
ruled out include (see https://online.epocrates.com/u/2911900)55
:
Psychiatric conditions, e.g. depression
Alcohol and other substance use
CNS infections, e.g. encephalitis, meningitis, neurosyphilis
CNS lymphoma
Cerebrovascular disease
History of head trauma
Endocrine disorders e.g. thyroid disease, hypogonadism
Recommendations:
1. Antiretroviral therapy to suppress plasma viral load should be started early and
administered continuously, to prevent or minimize HIV-related neurocognitive
impairment. (AII)
2. HIV-positive individuals presenting with cognitive complaints that affect their daily
functioning should be investigated to rule out relevant underlying conditions. (AII)

79
Nutritional deficiencies
Side effects of antiretrovirals or other medications
HIV-positive individuals presenting with significant cognitive complaints (affecting their work
performance, housekeeping, and/or social functioning) should have their plasma HIV viral load
assessed, and antiretroviral therapy started or adjusted as necessary to ensure good adherence and
consistent viral suppression. Those already receiving suppressive antiretroviral therapy should
have investigations to rule out the above conditions, including brain computed tomography
(CT)/magnetic resonance imaging (MRI) and lumbar puncture for cerebrospinal fluid (CSF)
examination if appropriate.55,56
This should be done in consultation with a neurologist. A full
evaluation by a neuropsychologist, if available, may be needed to delineate the pattern and extent
of the neurocognitive deficit.
In the absence of relevant underlying conditions, neurocognitive impairment in HIV may be
related to CSF viral “escape”, i.e. presence of detectable HIV RNA in CSF despite undetectable
viral load in plasma. Limited evidence exists that adjusting the antiretroviral therapy regimen to
include agents with better CSF penetration can stabilize or improve neurocognitive function in
this setting. Referral to a physician with expertise in the management of HIV is advised in these
situations. Full suppression of plasma viral replication remains the most important target, for
both prevention and treatment of HIV-related cognitive disorders.
H. Lung Disease (New subsection added March 2015)
Evidence:
Compared to the general population, HIV-positive patients have a greater risk for chronic
obstructive pulmonary disease (COPD), and are prone to develop it at a younger age, even taking
into account the relatively high rates of smoking in this population.57-59
COPD should be
managed according to current Canadian Thoracic Society guidelines (available at
Recommendations:
1. Smoking cessation should be strongly encouraged in all HIV-positive patients, because
they are at a higher risk for chronic obstructive pulmonary disease (COPD) and lung
cancer than smokers who do not have HIV. (AI)
2. A chest X-ray should be performed at baseline in all HIV-positive patients. Once
infection has been treated or ruled out, patients with persistently abnormal chest X-ray
findings should be investigated and referred to a respiratory specialist if necessary. (AI)
3. A diagnosis of COPD should be considered, and spirometry performed as a screening
test, among HIV-positive patients of any age presenting with persistent respiratory
complaints, especially those with additional risk factors such as smoking. COPD
should be managed according to current Canadian Thoracic Society guidelines
(http://www.respiratoryguidelines.ca/); however, concomitant use of inhaled steroids
with ritonavir or cobicistat should be avoided if possible. (AII)

80
http://www.respiratoryguidelines.ca/), including an aggressive plan for smoking cessation. The
use of all inhaled steroids should be avoided if possible in patients receiving ritonavir or
cobicistat as part of their antiretroviral therapy regimen, due to the risk of adrenal suppression
and iatrogenic Cushing’s syndrome.60,61
Beclometasone cannot be recommended as a “safer”
alternative in this setting; a recent systematic review showed this agent has no clinical effect in
COPD.62
If combination inhaled steroids/long-acting beta-agonist (LABA) inhalers are necessary
for the management of severe COPD symptoms, consideration should be given to switching
patients off of regimens containing ritonavir or cobicistat. Salmeterol is not recommended with
concomitant ritonavir or cobicistat in HIV-positive patients with COPD because of elevated
salmeterol levels that may increase the risk of cardiovascular adverse events63
; however, other
single-agent LABAs (e.g. indacaterol, formoterol) can be used safely in this setting.
A chest X-ray should be performed at baseline in all HIV-positive patients. As HIV confers an
increased risk of lung cancer, HIV care providers should have a low threshold for performing a
chest X-ray or chest computerized tomography (CT) in the presence of significant respiratory
symptoms, particularly in smokers.64-66
After appropriate management of infectious etiologies,
consultation with a respiratory specialist is advisable to investigate persistent symptoms or
abnormal imaging findings.
I. Liver Disease/Cirrhosis (New subsection added March 2015)
Evidence:
Chronic liver disease is a leading cause of morbidity and mortality among HIV-positive
individuals.67,68
Due to shared routes of transmission, a significant proportion of HIV-positive
individuals are co-infected with Hepatitis B and/or C virus.68-70
See also Section IV, Part 1 (pp.
33-35) Other important etiologies of liver disease in HIV-positive individuals include alcoholic
hepatitis, non-alcoholic steatohepatitis (NASH), and drug-induced hepatotoxicity.68,71-73
Due to
HIV being well-controlled with antiretroviral therapy, opportunistic infections of the liver are
now uncommon.
Recommendations:
1. Liver enzymes and liver function should be assessed in all HIV-positive individuals at
baseline and every 3-4 months after starting antiretrovirals, increasing to six-month
intervals when stable (AIII).
2. All HIV-positive individuals with cirrhosis who are co-infected with Hepatitis B and/or
C should be screened for hepatocellular carcinoma every six months using ultrasound
(AII).
3. All HIV-positive individuals with cirrhosis should be referred for a baseline
gastroscopy to screen for esophageal varices (AII).

81
HIV-positive individuals who are co-infected with HBV and/or HCV have a relatively rapid rate
of progression to cirrhosis compared to HIV-negative individuals with viral hepatitis.74,75
Once
cirrhotic, this population also has a higher rate of hepatic decompensation and hepatocellular
carcinoma.85,76
HCV and HBV in HIV-positive individuals should be managed according to
current guidelines to prevent cirrhosis (http://www.hcvguidelines.org/full-report/unique-patient-
populations-hivhcv-coinfection-box-summary-recommendations-hivhcv;
http://aidsinfo.nih.gov/contentfiles/lvguidelines/glchunk/glchunk_25.pdf).
HIV-positive individuals with confirmed cirrhosis should undergo routine hepatocellular
carcinoma surveillance with ultrasound every six months (see Table 6 on p. 57).77,78
These
individuals should also undergo a baseline gastroscopy to screen for varices.77,79
Serum alpha-
fetoprotein (AFP) monitoring lacks adequate sensitivity and specificity for hepatocellular
carcinoma surveillance and is no longer recommended.78
Cirrhosis in HIV-positive individuals
should be managed in collaboration with experts in liver diseases.
J. Cancer (New subsection added March 2015)
Evidence:
The incidence of AIDS-defining cancers, Kaposi's sarcoma, and non-Hodgkin’s lymphoma, has
markedly decreased in the highly active antiretroviral therapy era (with the exception of invasive
cervical cancer which has remained relatively unchanged), while non-AIDS-defining cancers
have become more common.80-82
This is attributable at least in part to the increasing risk of
malignancy as the HIV-positive population ages.
In general, people living with HIV are not at a greater risk of common cancers (breast,
colorectal, ovary, prostate) than their age-matched HIV-negative counterparts.83
Screening for
these cancers in HIV-positive patients should follow current provincial recommendations for the
general population.
However, even after controlling for relevant risk factors such as smoking, HIV-positive
individuals are at a higher risk for lung cancer (see Section VII, H. Lung Disease, p. 77) and
cancers attributable to infectious etiologies, specifically83,84
:
Anogenital and oropharyngeal cancers, secondary to Human Papilloma Virus (HPV)82
– see
Section IV (pp. 45-46)
Lymphoma, secondary to Epstein-Barr Virus (EBV)85
Recommendations:
1. In HIV-positive patients, screening for breast, colorectal, ovary, and prostate cancers
should follow current provincial recommendations for the general population. (BII)
2. HIV-positive patients may be at increased risk for lung cancer, HPV-related cancers
(oropharyngeal, cervical, anal), and hepatocellular cancer as compared to the general
population. Increased surveillance for these cancers is recommended. (AII)

82
Hepatocellular cancer, related to hepatitis B and C viruses (HBV and HCV)86
– see Section
VII, I. Liver disease (pp. 78-79)
Recommendations for cancer screening in HIV-positive individuals are summarized in Table 8
below.
Table 8. Recommendations for cancer screening in HIV-positive individuals (adapted from 2014
EACS Guidelines)
Cancer Population Screening test Baseline Screening
interval
Comments
Anal Men who have
sex with men
(MSM)
Digital rectal
exam
√ 1-3 years Anal Pap test may
be considered where
available, but not
standard of care (see
Section IV[F] (p.
36)
Breast Women Mammography Follow
standard BC
guidelines*
Follow standard
BC guidelines*
See Section VI (pp.
64-65)
Cervical† Women Pap test √ Repeat at 6
months; if both
tests normal,
repeat annually
Patients with
abnormal Pap test
should be referred
for colposcopy†; see
Section VI (pp. 63-
65)
Colorectal Men and
women 50-74
years
Fecal immuno-
chemical test
(FIT)
Follow
standard BC
guidelines
2 years‡ Patients with
abnormal FIT test
should be referred
for colonoscopy‡
Hepatocellular HCV+
Abdominal
ultrasound
ä - (unless
cirrhosis present)
HCV+ with
cirrhosis; or
HBV+
regardless of
fibrosis stage
√ 6 months
Non-cirrhotic,
HBV- and
HCV-
- -
Lung All Chest X-ray √ - Consider chest CT
specially in smokers
Prostate Men >50 years Digital rectal
exam
√ 1-3 years Use of the prostate-
specific antigen
(PSA) test for
screening is
controversial¶,**
* http://www.screeningbc.ca/Breast/ForHealthProfessionals/Eligibility.htm
† http://www.screeningbc.ca/Cervix/ForHealthProfessionals/Default.htm
‡ http://www.screeningbc.ca/Colon/ForHealthProfessionals/ProgramDetails.htm

83
§ Hull M, Klein M, Shafran S, Tseng A, Giguere P, Cote P, Poliquin M, Cooper C, The CIHR Canadian HIV Trials
Network HIV/Hepatitis C Management and Treatment Guidelines Working Group. Can J of Infect Dis Med
Microbiol 2013; 24(4): 217-238.
¶ Bell N, Gorber SC, Shane A, Joffres M, Singh H, Dickinson J, Shaw E, Dunfield L, Tonelli M, Canadian Task
Force on Preventive Health Care. Recommendations on screening for prostate cancer with the prostate-specific
antigen test. CMAJ 2014; 186(16): 1225-1234.
** Prostate Cancer Canada. Prostate Cancer Canada reminds men that early detection using ‘Smart Screening’ for
prostate cancer can save lives. Oct. 27, 2014. Available from http://www.prostatecancer.ca/In-The-
News/Foundation-News-Releases/Test#.VHkAl2fityI
References
1. Strategies for Management of Antiretroviral Therapy (SMART) Study Group, El-Sadr WM, Lundgren JD, et al.
CD4+ count-guided interruption of antiretroviral treatment. N Engl J Med 2006; 355(22): 2283-2296.
2. Aberg JA, Gallant JE, Ghanem KG, et al. Primary care guidelines for the management of persons infected with
human immunodeficiency virus: 2013 update by the HIV Medicine Association of the Infectious Diseases Society of
America. Clin Infect Dis 2014; 58(1): e1-e34. doi: 10.1093/cid/cit665.
3. Gunthard HF, Aberg JA, Eron JJ, et al. Antiretroviral treatment of adult HIV infection: 2014 recommendations of
the International Antiviral Society-USA panel. JAMA 2014; 312(4): 410-425.
4. Phillips AN, Carr A, Neuhaus J, et al. Interruption of antiretroviral therapy and risk of cardiovascular disease in
persons with HIV-1 infection: Exploratory analyses from the SMART trial. Antivir Ther 2008; 13(2): 177-187.
5. DAD Study Group, Friis-Moller N, Reiss P, et al. Class of antiretroviral drugs and the risk of myocardial infarction.
N Engl J Med 2007; 356(17): 1723-1735.
6. Currier JS, Lundgren JD, Carr A, et al. Epidemiological evidence for cardiovascular disease in HIV-infected patients
and relationship to highly active antiretroviral therapy. Circulation 2008; 118(2): e29-35. doi:
10.1161/CIRCULATIONAHA.107.189624.
7. Currier JS. Update on cardiovascular complications in HIV infection. Top HIV Med 2009; 17(3): 98-103.
8. Anderson TJ, Gregoire J, Hegele RA, et al. 2012 Update of the Canadian Cardiovascular Society guidelines for the
diagnosis and treatment of dyslipidemia for the prevention of cardiovascular disease in the adult. Can J Cardiol
2013; 29(2): 151-167.
9. Triant VA, Meigs JB, Grinspoon SK. Association of C-reactive protein and HIV infection with acute myocardial
infarction. J Acquir Immune Defic Syndr 2009; 51(3): 268-273.
10. Ridker PM, Danielson E, Fonseca FA, et al. Rosuvastatin to prevent vascular events in men and women with
elevated C-reactive protein. N Engl J Med 2008; 359(21): 2195-2207.
11. Law MG, Friis-Moller N, El-Sadr WM, et al. The use of the Framingham equation to predict myocardial infarctions
in HIV-infected patients: Comparison with observed events in the D:A:D study. HIV Med 2006; 7(4): 218-230.
12. Petomenous K, Worm S, Reiss P, et al. Rates of cardiovascular disease following smoking cessation in patients with
HIV infection: Results from the DAD study. HIV Med 2011; 12(7): 412-421.
13. Johns KW, Bennett MT, Bondy GP. Are HIV-positive patients resistant to statin therapy? Lipids Health Dis 2007; 6:
27.
14. Soliman EZ, Lundgren JD, Roediger MP, et al. Boosted protease inhibitors and the electrocardiographic measures of
QT and PR durations. AIDS 2011; 25(3): 367-377.
15. U.S. Food and Drug Administration. Labeling changes for Kaletra reflecting new QT/QTC interval and PR interval
prolongation information. April 2009. Available from:
http://www.fda.gov/forpatients/illness/hivaids/history/ucm151081.htm#2009.
16. U.S. Food and Drug Administration. Invirase (saquinavir): On-going safety review of clinical trial data. February
2010. Available from:
http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm201563.htm.
17. Pozniak AL, Morales-Ramirez J, Katabira E, et al. Efficacy and safety of TMC278 in antiretroviral-naïve HIV-1
patients: week 96 results of a phase IIb randomized trial. AIDS 2010: 24(1): 55-65.
18. Molina J-M, Cahn P, Grinsztejn B, et al. Rilpivirine versus efavirenz with tenofovir and emtricitabine in treatment-
naïve adults infected with HIV-1 (ECHO): a phase 3 randomised double-blind active-controlled trial. Lancet 2011;
378(9787): 238-246.

84
19. Cohen CJ, Andrade-Villanueva J, Clotet B, et al. Rilpivirine versus efavirenz with two background nucleoside or
nucleotide reverse transcriptase inhibitors in treatment-naïve adults infected with HIV-1 (THRIVE): a phase 3,
randomized, non-inferiority trial. Lancet 2011: 378(9787): 229-237.
20. Zareba W, Lin DA. Antipsychotic drugs and QT interval prolongation. Psychiatr Q 2003; 74(3): 291-306.
21. Brown TT, Li X, Cole SR, et al. Cumulative exposure to nucleoside analogue reverse transcriptase inhibitors is
associated with insulin resistance markers in the multicenter AIDS cohort study. AIDS 2005; 19(13): 1375-1383.
22. Jain MK, Araqki C, Fischbach L, et al. Hepatitis C is associated with Type 2 diabetes mellitus in HIV-infected
persons without traditional risk factors. HIV Med 2007; 8(8): 491-497.
23. Canadian Diabetes Association Clinical Practice Guidelines Expert Committee. Canadian Diabetes Association
2013 Clinical Practice Guidelines for the Prevention and Management of Diabetes in Canada. Can J Diabetes 2013;
37: S1-S212.
24. Triant VA, Brown TT, Lee H, Grinspoon SK. Fracture prevalence among human immunodeficiency virus (HIV)-
infected versus non-HIV-infected patients in a large U.S. healthcare system. J Clin Endocrinol Metab 2008; 93(9):
3499-3504.
25. Grund B, Peng G, Gibert CL, et al. Continuous antiretroviral therapy decreases bone mineral density. AIDS 2009;
23(12): 1519-1529.
26. McComsey GA, Tebas P, Shane E, et al. Bone disease in HIV infection: A practical review and recommendations
for HIV care providers. Clin Infect Dis 2010; 51(8): 937-946.
27. Bedimo R, Maalouf NM, Zhang S, Drechsler H, Tebas P. Osteoporotic fracture risk associated with cumulative
exposure to tenofovir and other antiretroviral agents. AIDS 2012; 26(7): 825-831.
28. Fabbriciani G, De Socio GVL. Efavirenz and bone health. AIDS 2009; 23(9): 1181.
29. Guillemi S, Harris M, Bondy GP, et al. Prevalence of bone mineral density abnormalities and related risk factors in
an ambulatory HIV clinic population. J Clin Densitom 2010; 13(4): 456-461.
30. The International Society for Clinical Densitometry (ISCD). 2013 ISCD Official Positions– Adult.2013. Available
from: http://www.iscd.org/official-positions/2013-iscd-official-positions-adult/.
31. Papaioannou A, Morin S, Cheung AM, et al. 2010 clinical practice guidelines for the diagnosis and management of
osteoporosis in Canada: Summary. CMAJ 2010; 182(17): 1864-1873.
32. Mueller NJ, Fux CA, Ledergerber B, et al. High prevalence of severe vitamin D deficiency in combined
antiretroviral therapy-naive and successfully treated Swiss HIV patients. AIDS 2010; 24(8): 1127-1134.
33. Holick MF. Vitamin D deficiency. N Engl J Med 2007; 357(3): 266-281.
34. Gupta SK, Eustace JA, Winston JA, et al. Guidelines for the management of chronic kidney disease in HIV-infected
patients: Recommendations of the HIV Medicine Association of the Infectious Diseases Society of America. Clin
Infect Dis 2005; 40(11): 1559-1585.
35. Jones R, Stebbing J, Nelson M, et al. Renal dysfunction with tenofovir disoproxil fumarate-containing highly active
antiretroviral therapy regimens is not observed more frequently: A cohort and case-control study. J Acquir Immune
Defic Syndr 2004; 37(4): 1489-1495.
36. Mocroft A, Kirk O, Reiss P, et al. Estimated glomerular filtration rate, chonic kidney disease and antiretroviral drug
use in HIV-positive patients. AIDS 2010; 24(11): 1667-1678.
37. Scherzer R, Estrella M, Li Y, et al. Association of tenofovir exposure with kidney disease risk in HIV infection.
AIDS 2012; 26(7): 867-875.
38. Ryom L, Mocroft A, Kirk O, et al. Association between antiretroviral exposure and renal impairment among HIV-
positive persons with normal baseline renal function: the D:A:D Study. J Infect Dis 2013; 207(9): 1359-1369.
39. Rockwood N, Mandalia S, Sirokosta J, Gazzard B, Nelson M. A comparative analysis of risk factors associated with
renal impairment and highly active antiretroviral therapy. J Antivir Antiretrovir 2012; 4: 21-25.
40. Harris M., Zalunardo N., Bonner S. Use of estimated glomerular filtration rate (GFR) to predict renal toxicity in
patients receiving tenofovir DF (TDF). 11th Conference on Retroviruses and Opportunistic Infections 2004.
41. Kopp JB, Miller KD, Mican JA, et al. Crystalluria and urinary tract abnormalities associated with indinavir. Ann
Intern Med 1997; 127(2): 119-125.
42. Rockwood N, Mandalia S, Bower M, Gazzard B, Nelson M. Ritonavir-boosted atazanavir exposure is associated
with an increased rate of renal stones compared to efavirenz, ritonavir-boosted lopinavir and ritonavir-boosted
darunavir. AIDS 2011; 25(13): 1671-1673.
43. Izzedine H, Harris, M, Perazella MA. Managing the nephrotoxic effects of HAART. Nat Rev Nephrol 2009; 5: 563-
573.
44. Koteff J, Borland J, Chen S, et al. A phase 1 study to evaluate the effect of dolutegravir on renal function via
measurement of iohexol and para-aminohippurate clearance in healthy subjects. Br J Clin Pharm 2013; 75(4): 990-
996.

85
45. Lepist-EI, Zhang X, Hao J, et al. Contribution of the organic ion transporter OAT2 to the renal active tubular
secretion of creatinine and mechanism for serum creatinine elevations caused by cobicistat. Kidney Int 2014; 86(2):
350-357.
46. DeJesus E, Rockstroh J, Henry K, et al. Co-formulated elvitegravir, cobicistat, emtricitabine, and tenofovir
disoproxil fumarate versus ritonavir-boosted atazanavir plus co-formulated emtricitabine and tenofovir disoproxil
fumarate for initial treatment of HIV-1 infection: a randomised, double-blind, phase 3, non-inferiority trial. Lancet
2012; 379(9835): 2429-2438.
47. Sax PE, DeJesus E, Mills A, et al. Co-formulated elvitegravir, cobicistat, emtricitabine, and tenofovir disoproxil
fumarate versus co-formulated efavirenz, emtricitabine and tenofovir for initial treatment of HIV-1 infection: a
randomised, double-blind, phase 3 trial, analysis of results after 48 weeks. Lancet 2012; 379(9835): 2439-2448.
48. Curtis LD, Min S, Nichols G, et al. Once-daily dolutegravir (DTG; GSK1349572) has a renal safety profile
comparable to raltegravir (RAL) and efavirenz in antiretroviral-naïve adults: 48 weeks results from SPRING-2
(ING113086) and SINGLE (ING114467). International AIDS Society Conference 2013. Abstract No. TUPE282.
49. Dobs A. Role of testosterone in maintaining lean body mass and bone density in HIV-infected patients. Int J
Impotence Res 2003; 15 Suppl 4: S21-25.
50. Rietschel P, Corcoran C, Stanly T, Basgoz N, Klibanski A, Grinspoon S. Prevalence of hypogonadism among men
with weight loss related to Human Immunodeficiency Virus infection who were receiving highly active
antiretroviral therapy. Clin Infect Dis 2000; 31(5): 1240-1244.
51. Bhasin S, Cunningham GR, Hayes FJ, et al. Testosterone therapy in men with androgen deficiency syndromes: an
Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab 2010; 95(6): 2536-59.
52. Grinspoon S, Corcoran C, Parlman K, et al. Effects of testosterone and progressive resistance training in eugonadal
men with AIDS wasting. A randomized, controlled trial. Ann Intern Med 2000; 133(5): 348-355.
53. The Mind Exchange Working Group. Assessment, Diagnosis, and Treatment of HIV-Associated Neurocognitive
Disorder: A Consensus Report of the Mind Exchange Program. Clin Infect Dis 2013; 56 (7): 1004-1017.
54. Antinori A, Arendt G, Becker JT, et al. Updated research nosology for HIV-associated neurocognitive disorders.
Neurol 2007; 69(18): 1789-1799.
55. Brouillette M-J, Hull M, Harris M. Evaluation of HIV-related mental status changes. BMJ Publishing Group.
Available from: https://online.epocrates.com/u/2911900
56. European AIDS Clinical Society (EACS). Guidelines Version 7.1, November 2014. Available from:
http://www.eacsociety.org/files/guidelines-7.1-english.pdf
57. Crothers K, Huang L, Goulet JL, et al. HIV infection and risk for incident pulmonary diseases in the combination
antiretroviral therapy era. Am J Resp Crit Care Med 2011; 183(3): 388-395.
58. Madeddu G, Fois AG, Calia GM, et al. Chronic obstructive pulmonary disease: An emerging co-morbidity in HIV-
infected patients in the HAART era? Infection 2012; 41(2): 347-353.
59. Leung JM, Liu JC, Mtambo A, et al. The determinants of poor respiratory health status in adults living with Human
Immunodeficiency Virus infection. AIDS Patient Care STDs 2014; 28(5): 240-247.
60. Foisy M, Yakiwchuk EM, Ciu I, Singh AE. Adrenal suppression and Cushing’s syndrome secondary to an
interaction between ritonavir and fluticasone: a review of the literature. HIV Med 2008; 9(6): 389-96.
61. Stribild Product Monograph. Gilead Sciences Canada Inc., February 2014.
62. De Coster DA, Jones M, Thakrar N. Beclometasone for chronic obstructive pulmonary disease. Cochrane Database
of Systematic Reviews 2013; 10: CD009769.
63. U.S. Department of Health and Human Services. Guidelines for the use of antiretroviral agents in HIV-1-infected
adults and adolescents. 2014:1-161. Available from:
http://www.aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf
64. Sigel K, Wisnevsky J, Gordon K, et al. HIV as an independent risk factor for incident lung cancer. AIDS 2012;
26(8): 1017-1025.
65. Kirk GD, Merlo C, O’Driscoll P, et al. HIV infection is associated with an increased risk for lung cancer,
independent of smoking. Clin Infect Dis 2007; 45(1): 103-110.
66. National Lung Screening Trial Research Team. Results of Initial Low-Dose Computed Tomographic Screening for
Lung Cancer. N Engl J Med 2013; 368(21): 1980-1991.
67. Weber R, Sabin CA, Friis-Moller N, et al. Liver-related deaths in persons infected with the human
immunodeficiency virus: the D:A:D study. Arch Intern Med 2006; 166(15): 1632-1641.
68. Salmon-Ceron D, Lewden C, Morlat P, et al. Liver disease as a major cause of death among HIV infected patients:
role of hepatitis C and B viruses and alcohol. J Hepatol 2005; 42(6): 799-805.
69. Koziel MJ, Peters MG. Viral hepatitis in HIV infection. N Engl J Med 2007; 356(14): 1445-1454.

86
70. Rosenthal E, Pialoux G, Bernard N, et al. Liver-related mortality in human-immunodeficiency-virus-infected
patients between 1995 and 2003 in the French GERMIVIC Joint Study Group Network (MORTAVIC 2003 study). J
Viral Hepat 2007; 14(3): 183-188.
71. Joshi D, O'Grady J, Dieterich D, Gazzard B, Agarwal K. Increasing burden of liver disease in patients with HIV
infection. Lancet 2011; 377 (9772): 1198-209.
72. Chaudhry AA, Sulkowski MS, Chander G, Moore RD. Hazardous drinking is associated with an elevated aspartate
aminotransferase to platelet ratio index in an urban HIV-infected clinical cohort. HIV Med 2009; 10(3): 133-142.
73. Soriano V, Barreiro P, Sherman KE. The changing epidemiology of liver disease in HIV patients. AIDS Rev 2013;
15(1): 25-31.
74. Giordano TP, Kramer JR, Souchek J, Richardson P, El-Serag HB. Cirrhosis and hepatocellular carcinoma in HIV-
infected veterans with and without the hepatitis C virus: a cohort study, 1992-2001. Arch Intern Med 2004; 164(21):
2349-2354.
75. Colin JF, Cazals-Hatem D, Loriot MA, et al. Influence of human immunodeficiency virus infection on chronic
hepatitis B in homosexual men. Hepatology 1999; 29(4): 1306-1310.
76. Graham CS, Baden LR, Yu E, et al. Influence of human immunodeficiency virus infection on the course of hepatitis
C virus infection: a meta-analysis. Clin Infect Dis 2001; 33(4): 562-569.
77. Hull M, Shafran S, Tseng A, Giguère P, Klein MB, Cooper C. CIHR Canadian HIV Trials Network Co-infection
and Concurrent Diseases Core: Updated Canadian guidelines for the treatment of hepatitis C infection in HIV-
hepatitis C coinfected adults. Can J Infect Dis Med Microbiol 2014; 25(6): 311-320.
78. Bruix J, Sherman M, American Association of the Study of Liver Diseases. Management of hepatocellular
carcinoma: An update. Hepatology 2011; 53(3): 1020-1022.
79. Garcia-Tsao G, Sanyal AJ, Grace ND, et al. Prevention and management of gastroesophageal varices and variceal
hemorrhage in cirrhosis. Hepatology 2007; 46(3): 922-938.
80. Engels EA, Biggar RJ, Hall HI, et al. Cancer risk in people infected with human immunodeficiency virus in the
United States. Int J Cancer 2008; 123(1): 187-194..
81. Silverberg MJ, Abrams DI. AIDS-defining and non-AIDS-defining malignancies: cancer occurrence in the
antiretroviral therapy era. Curr Opin Oncol 2007; 19(5): 446-451.
82. Chaturvedi AK, Madeleine MM, Biggar RJ, Engels EA. Risk of human papillomavirus-associated cancers among
persons with AIDS. J Natl Cancer Inst 2009; 101(16): 1120-1130.
83. Grulich AE, van Leeuwen MT, Falster MO, Vajdic CM. Incidence of cancers in people with HIV/AIDS compared
with immunosuppressed transplant recipients: a meta-analysis. Lancet 2007; 370(9581): 59-67.
84. Sigel K, Wisnevsky J, Gordon K, et al. HIV as an independent risk factor for incident lung cancer. AIDS 2012;
26(8): 1017-1025.
85. Grogg KL, Miller RF, Dogan A. HIV infection and lymphoma. J Clin Pathol 2007; 60(12): 1365-1372.
86. Macdonald DC, Nelson M, Bower M, Powles T. Hepatocellular carcinoma, human immunodeficiency virus and
viral hepatitis in the HAART era. World J Gastroenterol 2008; 14(11): 1657–1663.

87
VIII. Optimizing Adherence to Antiretroviral Therapy
Evidence:
High levels of adherence to antiretroviral therapy (≥95%) are necessary to ensure the optimum
effect of treatment on HIV disease progression.1 Sub-optimal adherence leads to a high
probability of the development of drug resistance. Early engagement and retention in care is
critical to helping patients achieve high levels of adherence and treatment success.2
Patients should be educated on the importance of maintaining adherence to HIV treatment and
they should be encouraged to inform all their care providers of their HIV treatment when they
are transferring care. HIV medications are not routinely entered onto Pharmanet when
medications are dispensed in B.C.
There is a dearth of information on how to effectively assess patient readiness for HIV treatment
in terms of patient ability to adhere to antiretroviral therapy.3 Adherence counselling training for
clinic team members has been proposed as a method to improve understanding about the
challenges associated with adherence and strategies to reduce adherence-related barriers.4
Depression and substance abuse are common co-morbidities in persons living with HIV infection
and are important barriers to HIV treatment adherence and care. It is important to identify
patients with depression because treating depression can improve adherence to antiretroviral
therapy.5
Recommendations:
1. All HIV-positive individuals should have timely access to routine and urgent care that
is linguistically and culturally appropriate to patient needs. (BII)
2. An interprofessional team model, with a primary provider for each patient, should be
utilized to promote trusting relationships between the patient and their health care team
members. (BII)
3. Clinicians should involve patients in antiretroviral regimen selection. Clinicians should
ensure that patients understand treatment goals and are motivated to initiate and
maintain adherence to antiretroviral therapy. (BII)
4. Clinicians should educate and support patients to help maintain adherence to
antiretroviral therapy by positively reinforcing treatment success. (BII)
5. Potential behavioural, structural, and psycho-social barriers to adherence and
engagement in care, such as mental illness or substance abuse, should be identified and
addressed in collaboration with appropriate providers. These barriers may change with
time and should be re-evaluated on an ongoing basis by all health care team members.
(BIII)

88
Adherence to therapy is a dynamic process and should be evaluated at each clinic visit to
facilitate early intervention and support to patients where necessary.6 Mixed results have been
observed regarding the effects of directly observed therapy on adherence and clinical outcomes
in hard-to-treat populations.7,8
A comprehensive model of HIV care that addresses medical and
social issues is essential for providing care to marginalized populations.5,9-12
If appropriate,
simplification of therapy (e.g. decreased number of daily doses, fixed-dose combinations) may
enhance adherence to antiretroviral therapy.13
Patients who consent may also benefit from the use
of adherence tools (e.g. pill boxes, reminder devices) and the involvement of community partners
(e.g. HIV service organizations, community health representatives).
References
1. Lima VD, Gill VS, Yip B, Hogg RS, Montaner JS, Harrigan PR. Increased resilience to the development of drug
resistance with modern boosted protease inhibitor-based highly active antiretroviral therapy. J Infect Dis 2008;
198(1): 51-58.
2. Thompson MA, Mugavero MJ, Amico KR, et al. Guidelines for improving entry into and retention in care and
antiretroviral adherence for persons with HIV: evidence-based recommendations from an International Association
of Physicians in AIDS Care panel. Ann Intern Med 2012; 156(11): 817-833.
3. Grimes RM, Grimes DE. Readiness: The state of the science (or the lack thereof). Curr HIV/AIDS Rep 2010; 7(4):
245-252.
4. Wilson IB, Laws MB, Safren SA, et al. Provider-focused intervention increases adherence-related dialogue but does
not improve antiretroviral therapy adherence in persons with HIV. J Acquir Immune Defic Syndr 2010; 53(3): 338-
347.
5. Sayles JN, Wong MD, Kinsler JJ, Martins D, Cunningham WE. The association of stigma with self-reported access
to medical care and antiretroviral therapy adherence in persons living with HIV/AIDS. J Gen Intern Med 2009;
24(10): 1101-1108.
6. Glass TR, Battegay M, Cavassini M, et al. Longitudinal analysis of patterns and predictors of changes in self-
reported adherence to antiretroviral therapy: Swiss HIV cohort study. J Acquir Immune Defic Syndr 2010; 54(2):
197-203.
7. Berg KM, Litwin A, Li X, Heo M, Arnsten JH. Directly observed antiretroviral therapy improves adherence and
viral load in drug users attending methadone maintenance clinics: A randomized controlled trial. Drug Alcohol
Depend 2010; 113(2-3): 192-199.
8. Hart JE, Jeon CY, Ivers LC, et al. Effect of directly observed therapy for highly active antiretroviral therapy on
virologic, immunologic, and adherence outcomes: A meta-analysis and systematic review. J Acquir Immune Defic
Syndr 2010; 54(2): 167-179.
9. Mugavero MJ, Lin HY, Willig JH, et al. Missed visits and mortality among patients establishing initial outpatient
HIV treatment. Clin Infect Dis 2009; 48(2): 248-256.
10. Vervoort SC, Grypdonck MH, de Grauwe A, Hoepelman AI, Borleffs JC. Adherence to HAART: Processes
explaining adherence behavior in acceptors and non-acceptors. AIDS Care 2009; 21(4): 431-438.
11. Royal SW, Kidder DP, Patrabansh S, et al. Factors associated with adherence to highly active antiretroviral therapy
in homeless or unstably housed adults living with HIV. AIDS Care 2009; 21(4): 448-455.
12. Sevelius J, Patouhas E, Keatley J et al. Barriers and Facilitators to Engagement and Retention in Care among
Transgender Women Living with Human Immunodeficiency Virus. Ann Behav Med 2014; 47(1): 5-16.
13. Nachega JB, Parienti JJ, Uthman OA, et al. Lower pill burden and once-daily dosing antiretroviral treatment
regimens for HIV infection: a meta-analysis of randomized controlled trials. Clin Infect Dis 2014; 58(9): 1297-1307.

89
IX. Special Consideration for HIV-positive Individuals with Addictions
Evidence:
There is a significant prevalence of illicit substance use among HIV-positive individuals.1
Substance abuse is associated with decreased access to and use of health care, reduced likelihood
of being prescribed antiretrovirals, and reduced adherence to antiretrovirals.2 HIV-positive
individuals should be asked about substance use annually, even if their baseline screen result is
negative. Commonly used substances include tobacco, alcohol, marijuana, heroin, cocaine, and
methamphetamines. Asking about the use and abuse of prescription opiates and benzodiazepines
is also important.
Individuals with a known history of substance dependence are at a high risk for relapse,
particularly when stressed by a new diagnosis of HIV or by its complications. Interventions to
improve the medical care of HIV-positive individuals who are substance-dependent should
include integration of drug abuse treatment with HIV primary care.3 Clinicians should be
familiar with the range of substance use treatment programs and services in their area. There is
some evidence that integrating harm reduction interventions within HIV care settings is
beneficial, and that a supervised injection facility can positively influence access to care for
HIV-positive people who inject drugs (PWID).4
Methadone maintenance therapy (MMT) is another intervention that has been shown to increase
access and adherence to antiretroviral drug treatment among PWID.5,6
Clinicians should closely
monitor HIV-positive individuals who are concurrently receiving antiretroviral therapy and
MMT. There are a number of drug-drug interactions between most antiretrovirals and
methadone.7 Buprenorphine (co-formulated with naloxone in Suboxone®) is also increasingly
Recommendations:
1. All HIV-positive individuals should be asked about substance use at baseline and at
least annually thereafter. Those with a history of substance use should be re-evaluated
for drug and alcohol use at least quarterly. (CIII)
2. Clinicians should offer and support a variety of substance use treatment options for
HIV-positive substance users, including abstinence, a reduction in use, and safer use
strategies. (CIII)
3. HIV-positive substance users receiving methadone or buprenorphine while on
antiretroviral therapy should be monitored for potential drug-drug interactions. (AII)
4. Substance users are at a high risk for multiple co-morbid medical and mental health
conditions, such as hepatitis B and C virus infection, tuberculosis, skin and soft tissue
infections, recurrent bacterial pneumonia, endocarditis, and depression. Primary care
providers of HIV-positive substance users should be familiar with the prevention,
diagnosis, and treatment of these co-morbidities. (BII)

90
being used for opioid use disorder but information regarding its interaction with antiretrovirals is
currently limited.8, 9
However, based on the available studies, buprenorphine has a more
favourable drug interaction profile compared to methadone. For a complete list of interactions
between antiretrovirals and other medications, please refer to Table 19 (a,b,c,d) in the DHHS
2015 guidelines (http://aidsinfo.nih.gov/contentfiles/lvguidelines/adultandadolescentgl.pdf) or
seek advice from a pharmacist with antiretroviral expertise if you practice in BC (call the St.
Paul’s HIV Pharmacy at 1-888-511-6222).
There are a number of common co-morbidities among HIV-positive substance users. Serologic
evidence of past hepatitis B virus (HBV) and hepatitis C virus (HCV) infection has been found in
more than two thirds of long-term users of injection drugs.10,11
HIV-related tuberculosis has been
closely associated with injection drug use, partly due to the high endemic levels of latent
Mycobacterium tuberculosis infection in the population groups in which substance users are
concentrated, such as the urban poor.12
Several studies have documented an elevated risk of
bacterial pneumonia in HIV-positive individuals who use drugs.13-15
The most common injection
drug use related infectious disease complications are skin and soft tissue infections, which
include cellulitis and abscesses.16-18
Endocarditis is independently associated with HIV infection
among PWID.17
High rates of depressive disorders have also been reported among those with a
substance use disorder.19,20
Familiarity with the prevention, diagnosis and treatment of these co-
morbidities in HIV-positive substance users is an essential component of their comprehensive
HIV care.
References
1. Galvan FH, Burnam MA, Bing EG. Co-occurring psychiatric symptoms and drug dependence or heavy drinking
among HIV-positive people. J Psychoactive Drugs 2003; 35 Suppl 1: 153-160.
2. Bruce RD, Altice FL. Clinical care of the HIV-infected drug user. Infect Dis Clin North Am 2007; 21(1): 149-179.
3. Knowlton AR, Arnsten JH, Eldred LJ, et al. Antiretroviral use among active injection-drug users: The role of
patient-provider engagement and structural factors. AIDS Patient Care STDS 2010; 24(7): 421-428.
4. Krusi A, Small W, Wood E, Kerr T. An integrated supervised injecting program within a care facility for HIV-
positive individuals: A qualitative evaluation. AIDS Care 2009; 21(5): 638-644.
5. Clarke S, Keenan E, Ryan M, Barry M, Mulcahy F. Directly observed antiretroviral therapy for injection drug users
with HIV infection. AIDS Read 2002; 12(7): 305-7, 312-316.
6. Spire B, Lucas GM, Carrieri MP. Adherence to HIV treatment among IDUs and the role of opioid substitution
treatment (OST). Int J Drug Policy 2007; 18(4): 262-270.
7. Bruce RD, Altice FL, Gourevitch MN, Friedland GH. Pharmacokinetic drug interactions between opioid agonist
therapy and antiretroviral medications: Implications and management for clinical practice. J Acquir Immune Defic
Syndr 2006; 41(5): 563-572.
8. Gruber VA, McCance-Katz EF. Methadone, buprenorphine, and street drug interactions with antiretroviral
medications. Curr HIV/AIDS Rep 2010; 7(3): 152-160.
9. Bruce RD, McCance-Katz E, Kharasch ED, Moody DE, Morse GD. Pharmacokinetic interactions between
buprenorphine and antiretroviral medications. Clin Infect Dis 2006; 43 Suppl 4: S216-223.
10. Stimmel B, Vernace S, Schaffner F. Hepatitis B surface antigen and antibody. A prospective study in asymptomatic
drug abusers. JAMA 1975; 234(11): 1135-1138.
11. Donahue JG, Nelson KE, Munoz A, et al. Antibody to hepatitis C virus among cardiac surgery patients, homosexual
men, and intravenous drug users in Baltimore, Maryland. Am J Epidemiol 1991; 134(10): 1206-1211.
12. O'Connor PG, Selwyn PA, Schottenfeld RS. Medical care for injection-drug users with human immunodeficiency
virus infection. N Engl J Med 1994; 331(7): 450-459.
13. Farizo KM, Buehler JW, Chamberland ME, et al. Spectrum of disease in persons with human immunodeficiency
virus infection in the united states. JAMA 1992; 267(13): 1798-1805.

91
14. Selwyn PA, Feingold AR, Hartel D, et al. Increased risk of bacterial pneumonia in HIV-infected intravenous drug
users without AIDS. AIDS 1988; 2(4): 267-272.
15. Willocks L, Cowan F, Brettle RP, Emmanuel FX, Flegg PJ, Burns S. The spectrum of chest infections in HIV-
positive patients in Edinburgh. J Infect 1992; 24(1): 37-42.
16. Palepu A, Tyndall MW, Leon H, et al. Hospital utilization and costs in a cohort of injection drug users. CMAJ 2001;
165(4): 415-420.
17. Spijkerman IJ, van Ameijden EJ, Mientjes GH, Coutinho RA, van den Hoek A. Human immunodeficiency virus
infection and other risk factors for skin abscesses and endocarditis among injection drug users. J Clin Epidemiol
1996; 49(10): 1149-1154.
18. Gordon RJ, Lowy FD. Bacterial infections in drug users. N Engl J Med 2005; 353(18): 1945-1954.
19. Valverde EE, Purcell DW, Waldrop-Valverde D, et al. Correlates of depression among HIV-positive women and
men who inject drugs. J Acquir Immune Defic Syndr 2007; 46 Suppl 2: S96-100. doi:
10.1097/QAI.0b013e318157683b.
20. Rabkin JG, Johnson J, Lin SH, et al. Psychopathology in male and female HIV-positive and negative injecting drug
users: Longitudinal course over 3 years. AIDS 1997; 11(4): 507-515.

92
X. Special Consideration for Individuals with Advanced HIV – Opportunistic
Infection & Prophylaxis
Despite efforts to expand HIV testing and the accessibility of effective antiretroviral therapy in
British Columbia, a number of individuals still present to medical care at an advanced stage of
HIV disease. Others may not access medical care including antiretroviral therapy, or be unable to
adhere to it consistently. Such individuals may have a low CD4 cell count, which places them at
risk for opportunistic infections (OIs), and indeed an OI is often the presenting feature that brings
them into medical care. Once the acute OI has been treated, primary prophylaxis for other
common OIs may be appropriate if the CD4 cell count remains low. Following immune
reconstitution with antiretroviral therapy, primary prophylaxis can often be discontinued once the
patient is clinically stable and has established consistent adherence. For more information on
Immune Reconstitution Inflammatory Syndrome (IRIS) in HIV-infected patients, refer to the
BC-CfE Therapeutic Guidelines (http://www.cfenet.ubc.ca/therapeutic-guidelines/adult).
Indications for prophylaxis, agents of choice, and criteria for discontinuing and restarting
primary prophylaxis for Pneumocystis Jirovecii pneumonia (PJP), Toxoplasma, Mycoplasma
(M.) tuberculosis, and Mycobacterium Avium Complex (MAC) are shown in Table 9 on p. 93.
References
1. Kaplan JE, Benson C, Holmes KK, et al. Guidelines for prevention and treatment of opportunistic infections in HIV-
infected adults and adolescents: Recommendations from Centers for Disease Control and Prevention, the National
Institutes of Health, and the HIV Medicine Association of the Infectious Diseases Society of America. 2015.
Available from: https://aidsinfo.nih.gov/contentfiles/lvguidelines/adult_oi.pdf

93
Table 9: Prophylaxis to prevent first episode of opportunistic disease, and criteria for when to discontinue or restart primary prophylaxis
for adults and adolescents with HIV infection (Table updated March 2015, adapted from http://aidsinfo.nih.gov/guidelines 2013)1
Pathogen* Indication First choice Alternative Criteria for
discontinuing
primary prophylaxis
Criteria for
restarting
primary
prophylaxis
Pneumocystis
Jerovecii Pneumonia
(PJP)
(previously PCP)
CD4 cell count <200
cells/mm3 or
oropharyngeal candidiasis
or CD4 cell count <14%
or history of AIDS-
defining illness or CD4
cell count >200 but <250
cells/ mm3 if monitoring
CD4 cell count every 1-3
months is not possible
Trimethoprim-
sulfamethoxazole (TMP-
SMX)*, 1 double strength
(DS) per os (by mouth)
(PO) daily; or 1 single
strength (SS) PO daily
• TMP-SMX* 1 DS PO
3 times a week; or
• Dapsone* 100 mg PO
daily or 50 mg PO bid;
or
• Dapsone 50 mg PO
daily + (pyrimethamine
50 mg + leucovorin 25
mg ) PO weekly; or
• Atovaquone 1500 mg
PO daily; or
• Aerosolized
pentamidine 300 mg via
Respirgard® II
nebulizer every month
CD4 cell count >200
cells/mm3 for >3
months in response to
antiretroviral therapy
(ART) or CD4 cell
count 100-200
cells/mm3 for >3
months in response to
ART, and HIV RNA
<40 copies/mL230
CD4 cell count <200
cells/mm3, if HIV
RNA>40 copies/mL;
or CD4 <100 cells/mm
3
if HIV RNA
<40 copies/mL
Toxoplasma gondii
encephalitis
Toxoplasma IgG positive
patients with CD4 cell
count <100 cells/mm3
Seronegative patients
receiving PCP prophylaxis
not active against
toxoplasmosis should have
toxoplasma serology
retested if CD4 cell count
declines to <100
cells/mm3. Prophylaxis
should be initiated if
seroconversion occurred
Trimethoprim-
sulfamethoxazole (TMP-
SMX)*, 1 DS PO daily
• TMP-SMX* 1 DS PO
3 times a week; or
• TMP-SMX 1 SS PO
daily; or
• Dapsone* 50 mg PO
daily + (pyrimethamine
50 mg + leucovorin 25
mg) PO weekly; or
• atovaquone 1500 mg
PO daily
CD4 cell count >200
cells/mm3 for >3
months in response to
ART
CD4 cell count
< 100-200 cells/mm3

94
Mycobacterium
tuberculosis
infection (TB)
[Treatment of latent
TB infection (LTBI)]
• (+) diagnostic test for
LTBI, no evidence of
active TB, and no prior
history of treatment for
active or latent TB
• Or, close contact with a
person with infectious
pulmonary TB and no
evidence of active TB,
regardless of screening
diagnostic test result for
LTBI
• Or a history of untreated
or inadequately treated
healed TB (i.e. old fibrotic
lesions) regardless of
diagnostic tests for LTBI
and no evidence of active
TB
Isoniazid (INH) 300 mg
PO daily or 900 mg PO
twice a week for 9 months
– both plus pyridoxine 25
mg PO daily
Rifampin (RIF) 600 mg
PO daily x 4 months; or
Rifabutin 300 mg po
daily (dose adjusted
based on concomitant
ART) x 4 months
(For persons exposed to
drug-resistant TB,
selection of drugs after
consultation with public
health authorities)
Not applicable Not Applicable
Disseminated
Mycobacterium
avium complex
(MAC) disease
CD4 cell count <50
cells/mm3 after ruling out
active MAC infection¶
Azithromycin 1200 mg
PO once weekly or
Clarithromycin 500 mg
PO bid or
Azithromycin 600 mg PO
twice weekly
Rifabutin 300 mg PO
daily (dosage
adjustment based on
drug-drug interactions
with ART); rule out
active TB before
starting RFB
CD4 cell count >100
cells/mm3 for >3
months in response to
ART
CD4 cell count
<50 cells/mm3
* Screening for Glucose-6-phosphate Dehydrogenase (G6PD) deficiency for patients with a predisposing racial or ethnic background may be relevant to prevent
hemolysis after exposure to oxidant drugs such as dapsone and trimethoprim-sulfamethoxazole ¶ For asymptomatic patients, MAC prophylaxis can be started after drawing a mycobacterial blood culture. Symptomatic patients should wait for the results of
blood culture before starting MAC prophylaxis.

95
XI. Psycho-Social Implications of HIV Infection
A coordinated interdisciplinary care approach is an important aspect of primary care for HIV-
positive individuals. Best practices for delivering this care, including testing and treatment, must
be informed by an array of psycho-social considerations that stem from the reality of the lives of
HIV-positive individuals. The impact of these considerations depends on individual
circumstances and on an individual’s stage within the HIV disease trajectory.
From a clinical perspective, the continuum of HIV care has been summarized as: (1) HIV
diagnosis; (2) linked to HIV care; (3) retained in HIV care; (4) on antiretroviral therapy (ART);
(5) adherent to ART; and (6) achieving a suppressed viral load.1 These stages have also been
turned into indicators, collectively known as the cascade of care, that can serve as a tool for
improving the delivery and quality of HIV care. In BC, these indicators reveal disparities and
thus potential opportunities for improvement.1 Preventing losses at each step of the cascade will
benefit the individual (decrease morbidity and mortality), the community (decrease HIV
transmissions) and the system (save costs of new infections and cost of acute care utilization).2-4
A. Model of care
Evidence:
The collaborative and interdisciplinary chronic disease model of care should strengthen and
support self-care while assuring effective medical care, prevention and health maintenance.5 The
process should be dynamic and continuous, beginning with mutual respect, dialogue, and the
establishment of mutually desired and obtainable goals, and progressing through stages to
improve adherence, optimize health and increase survival.5-9
It is essential to this type of health
care management that collaborative definitions of problems, goals, and planning are clearly
established with the patient always at the centre to improve health outcomes.5,7-11
In addition to having an interdisciplinary team approach, free HIV care should foster the
development of a strong and trusting patient-provider relationship, preferably between the patient
and a primary case manager.12,13
Trust and confidentiality are also essential on the part of care
providers. Although confidentiality of all medical information is always mandatory, it is
particularly important for HIV-positive individuals due to HIV-related stigma. Issues of trust and
other barriers to care can impact an individual’s risk of acquiring HIV and can also impact the
care of those who are HIV-positive.12,13
Recommendation:
1. HIV care and patient education should be provided in a socially, culturally and gender
appropriate manner using a patient-centred, collaborative, and interdisciplinary
chronic disease care model which fosters trusting patient-provider relationships and
improves retention in care. (CIII)

96
B. Linkage to and retention in care (New subsection May 2015)
Evidence:
Timely access to care is important for any health condition but especially important in the case of
HIV, where delayed treatment can have serious consequences for the individual and others
through unintended disease transmission.2,14
In British Columbia, all residents are eligible for
care and treatment of HIV free of charge. Care providers who are faced with the ethical dilemma
of caring for any person not eligible for treatment or care (visitors and/or persons residing in
Canada illegally) should contact the BC Centre for Excellence in HIV/AIDS to advocate on the
person’s behalf for coverage of the cost of medical treatment.
HIV-positive individuals who are not linked to and retained in care may face significant barriers
to achieving optimal treatment outcomes.15
In some settings, interventions such as case
management and intensive outreach that aim to improve linkage to care and sustained
engagement can help support better treatment outcomes.16
As needs vary from one social and
clinical context to another, more research evaluating what interventions work and where is
needed.16
Quality improvement involves routine data collection and cycles of planning, change, and
feedback to improve processes and outcomes. Incorporating quality improvement methods in
HIV care can provide useful feedback throughout cycles of change, including the
implementation of an intervention, and help close gaps in care.17
For more information on best
practices for quality improvement and evaluation of HIV care and services, please consult the
resources available on the HIV Continuum of Care Collaborative website
(http://stophivaids.ca/hiv-continuum-collaborative/) or contact the BC Centre for Excellence in
HIV/AIDS by phone at 604-806-8477.
Recommendations:
1. All HIV-positive individuals should have timely access to routine primary care and
treatment. (BII)
2. Case management for individuals with a new HIV diagnosis is recommended. (BII)
3. Intensive outreach for individuals not engaged in medical care within 6 months of a
new HIV diagnosis may be considered. (CIII)
4. Clinical and non-clinical providers are strongly encouraged to incorporate quality
improvement strategies that focus on improving delivery and quality of HIV care to
HIV-positive individuals. (CIII)

97
C. Peer and social support
Evidence:
Stigma, isolation, and marginalization are common realities in the lives of HIV-positive
individuals. Ensuring access to social and emotional support for affected individuals is a crucial
part of HIV primary care.11
Moreover, clinicians should ensure that the individual’s basic
determinants of health, such as food security and access to adequate housing, are fulfilled.
Patients should also be connected to peer support whenever possible. Peer support programs
have proven successful in reducing harmful health behaviours, improving disease management,
and improving depression outcomes.18,19
Peer support programs can also help improve linkages
to and retention in care.16
AIDS service organizations (ASOs) are excellent starting points for
many of these services. The Canadian AIDS Treatment and Information Exchange
(http://catie.ca, 1-800-263-1638) is a national organization that provides useful support and
information as well as a searchable listing of regional ASOs. Please refer to the Contact List (p.
105) for a list of provincial ASOs.
D. Youth (New subsection added March 2015)
Evidence:
Advances in antiretroviral therapy have resulted in the increasing survival of HIV-positive
individuals, allowing those infected to live near normal life expectancies, yet those under 30
years of age continue to have suboptimal rates of retention at each stage across the cascade of
care.20-23
Recommendations:
1. Clinicians should perform thorough assessments of the social circumstances of HIV-
positive individuals at baseline and re-evaluate annually. (CIII)
2. All individuals living with HIV should be offered a referral to an AIDS service
organization (ASO) for counselling, social, and peer support. (CIII)
3. Peer support workers should be identified and utilized to help improve patient
outcomes. (CIII)
Recommendation:
1. In view of the suboptimal rates of retention youth experience at each stage of the
cascade of care, consideration should be given to the unique psycho-social issues that
youth face when developing their care and treatment plan. (CIII)

98
Clinicians providing care to both prenatally- and behaviourally-infected youth should be
cognizant of the many psycho-social issues that affect retention in care and medication
adherence rates, including stigma, discrimination, loss of family members, body dysmorphia,
safer sex negotiation, and general feelings of youth invincibility. It is important that youth play
an active role in their health care planning to increase autonomy and capacity. When possible,
newer technologies, such as texting medication reminders, should be utilized to improve
adherence.24,25
For more information on adherence to antiretroviral therapy, please refer to
Section VIII. Optimizing Adherence to Antiretroviral Therapy on p. 85.
References
1. BC Centre for Excellence in HIV/AIDS. HIV Monitoring Quarterly Report for British Columbia. Fourth Quarter
2014. Available from: http://www.cfenet.ubc.ca/sites/default/files/uploads/publications/centredocs/bc-monitoring-
report-14q4-final-2015-mar-10.pdf
2. Montaner JS, Lima VD, Barrios R, et al. Association of Highly Active Antiretroviral Therapy Coverage, Population
Viral Load, and Yearly New HIV Diagnoses in British Columbia, Canada: A Population-Based Study. Lancet 2010;
376(9740): 532-539.
3. Nosyk B, Montaner JS, Colley G, et al. The Cascade of HIV Care in British Columbia, Canada, 1996–2011: A
Population-Based Retrospective Cohort Study. Lancet Infect Dis 2014; 14(1): 40-49.
4. Lourenço L, Lima VD, Heath K, et al. Process Monitoring of an HIV Treatment as Prevention Program in British
Columbia, Canada. J Acquir Immune Defic Syndr 2014; 67(3): e94-109. doi: 10.1097/QAI.0000000000000293.
5. Beal J, Orrick J, Alfonso K, Rathore M. HIV/AIDS primary care guide. Florida: Crown House Publishing; 2006.
6. U.S. Department of Health and Human Services. Guidelines for the use of antiretroviral agents in HIV-1-infected
adults and adolescents. 2014:1-161. Available from:
http://www.aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf
7. Hecht FM, Wilson IB, Wu AW, Cook RL, Turner BJ. Optimizing care for persons with HIV infection. society of
general internal medicine AIDS task force. Ann Intern Med 1999; 131(2): 136-143.
8. Washington DL, Bowles J, Saha S, et al. Transforming clinical practice to eliminate racial-ethnic disparities in
healthcare. J Gen Intern Med 2008; 23(5): 685-691.
9. Stone VE. Optimizing the care of minority patients with HIV/AIDS. Clin Infect Dis 2004; 38(3): 400-404.
10. Pelzang, R. Time to learn: Understanding patient-centred care. Br J Nurs 2010; 19(14): 912-917.
11. U.S. Department of Health and Human Services. A guide to primary care for people with HIV/AIDS. 2004.
Available from: http://www.hab.hrsa.gov/tools/primarycareguide/index.htm
12. Schneider J, Kaplan SH, Greenfield S, Li W, Wilson IB. Better physician-patient relationships are associated with
higher reported adherence to antiretroviral therapy in patients with HIV infection. J Gen Intern Med 2004; 19(11):
1096-1103.
13. Dugdale DC, Epstein R, Pantilat SZ. Time and the patient-physician relationship. J Gen Intern Med 1999; 14 Suppl
1: S34-40.
14. Johnston KM, Levy AR, Lima VD, et al. Expanding access to HAART: A cost-effective approach for treating and
preventing HIV. AIDS 2010; 24(12): 1929-1935.
15. Gardner EM, McLees MP, Steiner JF, Del Rio C, Burman WJ. The spectrum of engagement in HIV care and its
relevance to test-and-treat strategies for prevention of HIV infection. Clin Infect Dis 2011; 52(6): 793-800.
16. Zuniga JM, Young B. Achieving Improvements across the HIV Treatment Cascade: A Clinical Management
Algorithm Based on IAPAC’s Entry into and Retention in Care and Antiretroviral Therapy Adherence Guidelines. J
Int Assoc Provid AIDS Care 2013; 12(1): 15-17.
17. Centers for Disease Control and Prevention, Health Resources and Services Administration, National Institutes of
Health, American Academy of HIV Medicine, Association of Nurses in AIDS Care, International Association of
Providers of AIDS Care, the National Minority AIDS Council, and Urban Coalition for HIV/AIDS Prevention
Services. Recommendations for HIV Prevention with Adults and Adolescents with HIV in the United States, 2014.
2014. Available from: http://stacks.cdc.gov/view/cdc/26062.
18. Rapid Response Service. Rapid Response: How to support and facilitate peer engagement in service provision roles.
Toronto, ON: Ontario HIV Treatment Network; December 2013. 2013. Available from:
http://www.ohtn.on.ca/Pages/Knowledge-Exchange/Rapid-Responses/Documents/RR76.pdf
19. Dennis CL. Peer support within a health care context: a concept analysis. Int J Nurs Stud 2003; 40(3): 321-32.

99
20. Canadian AIDS Treatment Information Exchange (CATIE). HIV in Canada: A Primer for Service Providers. 2014.
Available from: http://www.catie.ca/en/hiv-canada/2/2-3/2-3-6
21. Canadian AIDS Treatment Information Exchange (CATIE). Fact Sheet - The Epidemiology of HIV in Youth. 2013.
Available from: http://www.catie.ca/en/fact-sheets/epidemiology/epidemiology-hiv-youth
22. Public Health Agency of Canada. Population-Specific Status Report: HIV/AIDS and other Sexually Transmitted and
Blood Borne Infections Among Youth in Canada. Ottawa, Canada: Centre for Communicable Diseases and
Infection Control Public Health Agency of Canada; 2014. 2014. Available from: http://librarypdf.catie.ca/pdf/ATI-
20000s/26485.pdf
23. Statistics Canada. Aboriginal Peoples in Canada: First Nations People, Métis and Inuit. Ottawa, Canada: Social and
Aboriginal Statistics Division, Statistics Canada; 2011. 2011. Available from: http://www12.statcan.gc.ca/nhs-
enm/2011/as-sa/99-011-x/99-011-x2011001-eng.cfm.
24. U.S. Department of Health and Human Services. Guidelines for the use of antiretroviral agents in HIV-1-infected
adults and adolescents. 2014: 1-161. Available from:
http://www.aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf.
25. Belzar M, Naar-King S, Olson J, Clark, Sarr M, and the Adolescent Trials Network for HIV/AIDS Interventions. A
pilot study using cell phone interactions to improve HIV medication adherence in adolescents who have previously
failed antiretroviral therapy. Society for Adolescent Health and Medicine Annual Meeting. 2013.

100
Table 10: Other Guidelines related to the care of HIV-positive individuals
Topic/Title URL Issuing Agency
Antiretroviral Therapy
Therapeutic Guidelines for
Antiretroviral (ARV) Treatment of
Adult HIV Infection (2013)
http://www.cfenet.ubc.ca/therapeutic-
guidelines/adult
BC Centre for Excellence in
HIV/AIDS
Guidelines for HIV Infected and
Exposed Children
http://www.cfenet.ubc.ca/therapeutic-
guidelines/pediatric
BC Centre for Excellence in
HIV/AIDS
Accidental Exposure Guidelines http://www.cfenet.ubc.ca/therapeutic-
guidelines/accidental-exposure
BC Centre for Excellence in
HIV/AIDS
Antiretroviral Treatment of Adult
HIV Infection: 2014
Recommendations
http://jama.jamanetwork.com/article.aspx?ar
ticleid=1889146
International Antiretroviral
Society, US Panel
Antiretroviral Drug Resistance
Testing in Adult HIV-1 Infection:
2008 Recommendations
http://www.iasusa.org/pub/resistance2008.p
df
International Antiretroviral
Society, US Panel
Drug Interactions Charts, HIV
Drug Interactions.org
http://www.hiv-
druginteractions.org/interactions.aspx
Liverpool HIV Pharmacology
Group, University of
Liverpool
Drug Interaction Tables,
Immunodeficiency Clinic
http://www.hivclinic.ca/main/drugs_interact.
html
Toronto General Hospital,
University Health Network
Guidelines for the Use of
Antiretroviral Agents in HIV-
Infected Adults and Adolescents
(2015)
http://aidsinfo.nih.gov/contentfiles/lvguideli
nes/adultandadolescentgl.pdf
U.S. Department of Health
and Human Services
https://www.crediblemeds.org/index.php CredibleMeds
Cancer
Cervical Cancer http://www.screeningbc.ca/Cervix/default.ht
m
http://www.screeningbc.ca/Cervix/ForHealth
Professionals/Default.htm
BC Cancer Agency
Physician Protocol for Screening
Mammograms
http://www.screeningbc.ca/NR/rdonlyres/A
A527AF1-6F8E-40DE-84DA-
E2397FC29C9D/68351/SMPPhysicianProto
colsVersionFebruary2014Web.pdf
BC Cancer Agency
Trans People http://convio.cancer.ca/site/PageServer?page
name=SSL_ON_T_Home#.VaBZE-t9SXv
Canadian Cancer Agency
Breast Cancer http://www.screeningbc.ca/Breast/ForHealth
Professionals/Eligibility.htm
BC Cancer Society
Colon Cancer http://www.screeningbc.ca/Colon/ForHealth
Professionals/ProgramDetails.htm
BC Cancer Society
Recommendations on screening for
prostate cancer with the prostate-
specific antigen test
http://www.cmaj.ca/content/186/16/1225
or http://canadiantaskforce.ca/ctfphc-
guidelines/2014-prostate-cancer/
Canadian Task Force on
Preventive Health Care
Cardiovascular
Canadian Hypertension Education
Program Recommendations for
Blood Pressure Measurement,
Diagnosis, Assessment of Risk,
Prevention, and Treatment of
Hypertension (2014)
http://www.onlinecjc.ca/article/S0828-
282X%2814%2900070-1/pdf
Canadian Hypertension
Education Program

101
Topic/Title URL Issuing Agency
Update of the Canadian
Cardiovascular Society Guidelines
for the Diagnosis and Treatment of
Dyslipidemia for the Prevention of
Cardiovascular Disease in the
Adult (2012)
http://www.onlinecjc.ca/article/S0828-
282X%2812%2901510-3/pdf
Canadian Cardiovascular
Society
Contraception
Interactions between
Antiretrovirals (ARVs) and
Hormonal Contraceptives
http://www.hivclinic.ca/main/drugs_interact
_files/Oral%20Contraceptive-int.pdf
Toronto General Hospital,
Immunodeficiency Clinic
Hormonal contraceptive methods
for
women at high risk of HIV and
living with HIV (2014)
http://apps.who.int/iris/bitstream/10665/128
537/1/WHO_RHR_14.24_eng.pdf
World Health Organization
Best Practices to Minimize Risk of
Infection with Intrauterine Device
Insertion
http://sogc.org/guidelines/best-practices-
minimize-risk-infection-intrauterine-device-
insertion/
Society of Obstetricians and
Gynaecologists of Canada
Diabetes
Diabetes Clinic Practice Guidelines
2013
http://guidelines.diabetes.ca/ Canadian Diabetes
Association
Hepatitis B and Co-infection
Practice Guidelines http://www.aasld.org/practiceguidelines/doc
uments/bookmarked%20practice%20guideli
nes/chronic_hep_b_update_2009%208_24_2
009.pdf
American Association for the
Study of Liver Disease
Hepatitis B in Chapter I -
Management of Specific Diseases
http://www.bccdc.ca/NR/rdonlyres/328189F
4-2840-44A1-9D13-
D5AB9775B644/0/HepatitisB_Sept_2009.p
df
BC Centre for Disease Control
British HIV Association guidelines
for the management of hepatitis
viruses in adults infected with HIV
2013
http://www.bhiva.org/documents/Guidelines
/Hepatitis/2013/HepatitisGuidelines2013.pdf
British HIV Association
EACS Guidelines Version 7.1 http://www.eacsociety.org/files/guidelines-
7.1-english.pdf
European AIDS Clinical
Society
EASL Clinical Practice Guidelines http://www.easl.eu/research/our-
contributions/clinical-practice-guidelines
European Association for the
Study of the Liver
Hepatitis C and Co-infection
Recommendations for Testing,
Managing and Treating Hepatitis C
http://www.hcvguidelines.org/full-
report/unique-patient-populations-hivhcv-
coinfection-box-summary-
recommendations-hivhcv
American Association for the
Study of Liver Diseases
BHIVA guidelines for the
management of hepatitis viruses in
adults infected with HIV 2013
(updated September 2014)
http://www.bhiva.org/hepatitis-
guidelines.aspx
British HIV Association
An update on the management of
chronic hepatitis C: 2015
consensus guidelines from the
Canadian Association for the Study
of the Liver
http://www.liver.ca/files/Professional_Educa
tion___Partnerships/Information___Resourc
es_for_HCP/CASL_Hep_C_Consensus_Gui
delines_Update_-_Jan_2015.pdf
Canadian Association for the
Study of the Liver

102
Topic/Title URL Issuing Agency
British HIV Association guidelines
for the management of hepatitis
viruses in adults infected with HIV
2013
http://www.eacsociety.org/guidelines/eacs-
guidelines/eacs-guidelines.html
European AIDS Clinical
Society
Care of patients co-infected with
HIV and hepatitis C virus: 2007
updated recommendations from the
HCV–HIV International Panel
http://www.matecmichigan.com/resource/10
.Hepatitis/C%20Care%20of%20patients%20
coinfected%20with%20HIV%20and%20HC
V%202007.pdf
International AIDS Society
Hepatitis C Co-infection
Guidelines 2007
CIHR Canadian HIV Trials
Network Co-infection and
Concurrent Diseases Core:
Canadian guidelines for
management and treatment of
HIV/hepatitis C co-infection in
adults
http://www.pulsus.com/pdfs/15871_hull.pdf M. Hull et al. on behalf of the
Canadian HIV Trials Network
HIV/Hepatitis C Management
and Treatment Guidelines
Working Group
Immunization
Immunization Program http://www.bccdc.ca/dis-cond/comm-
manual/CDManualChap2.htm
BC Centre for Disease Control
Communicable Disease Control
Manual. Chapter 2: Immunization,
Section VII: Biological Products
(2014)
http://www.bccdc.ca/NR/rdonlyres/528C4C
20-F2F8-4333-9927-
E8DC455A5E76/0/SectionVII_BiologicalPr
oducts_February2015.pdf
BC Centre for Disease Control
Canadian Immunization Guide
(2014)
http://www.phac-aspc.gc.ca/publicat/cig-
gci/index-eng.php
Public Health Agency of
Canada, National Advisory
Committee on Immunization
Update the Recommended Human
Papillomavirus (HPV) Vaccine
Immunization Schedule
http://www.phac-aspc.gc.ca/naci-ccni/acs-
dcc/2015/hpv-vph_0215-eng.php
Public Health Agency of
Canada, National Advisory
Committee on Immunization
Interim Statement on HPV
Vaccination of Men Who Have Sex
with Men (2014)
https://www.gov.uk/government/uploads/sys
tem/uploads/attachment_data/file/373531/JC
VI_interim_statement_HPV_vacc.pdf
Joint Committee on
Vaccination and Immunisation
Laboratory Testing
HIV Laboratory Testing: a
Resource for Health Professionals
(2010)
http://www.bccdc.ca/NR/rdonlyres/2982E29
3-BD82-436D-B193-
F929B5CEEBEC/0/HIVTestinginBCResour
ceDocumentforHealthProfessionalsJune2010
BC Centre for Disease Control
IGRA Testing Guidelines
http://www.bccdc.ca/NR/rdonlyres/F34F072
5-9087-457D-8059-
F30BE18946C4/0/TB_manual_IGRA_guide
lines.pdf
BC Centre for Disease Control
HIV testing, reporting, counselling
and follow-up, and guidelines on
point of care testing
http://www.bccdc.ca/dis-cond/comm-
manual/CDManualChap5.htm
BC Centre for Disease Control
Update: Diagnostic, monitoring
and resistance laboratory tests for
HIV (2014)
http://www.hivguidelines.org/wp-
content/uploads/2014/01/diagnostic-
monitoring-and-resistance-laboratory-tests-
for-hiv.pdf
New York State Department
of Health AIDS Institute
Living with HIV
Healthy Living Manual (2012) http://positivelivingbc.org/wp-
content/uploads/2015/03/healthylivingmanu
al2012_0.pdf
Positive Living Society of
British Columbia

103
Topic/Title URL Issuing Agency
Nutrition
A practical guide to nutrition for
people living with HIV (2007)
http://www.catie.ca/en/practical-
guides/nutrition
Canadian AIDS Treatment
Information Exchange
Opportunistic Infections
Therapeutic Guidelines for
Opportunistic Infections (2009)
http://www.cfenet.ubc.ca/therapeutic-
guidelines/opportunistic-infection
BC Centre for Excellence in
HIV/AIDS
Guidelines for the prevention and
treatment of opportunistic
infections in HIV-infected adults
and adolescents
http://aidsinfo.nih.gov/contentfiles/lvguideli
nes/adult_oi.pdf
Centers for Disease Control
and Prevention, the National
Institutes of Health, and the
HIV Medicine Association of
the Infectious Diseases
Society of America
1993 Revised Classification system
for HIV infection and expanded
surveillance case definition for
AIDS among adolescents and
adults.
http://www.cdc.gov/mmwr/preview/mmwrht
ml/00018871.htm
US Centers for Disease
Control and Prevention
Osteoporosis
Clinical practice guidelines for the
diagnosis and management of
osteoporosis in Canada (2010)
http://www.cmaj.ca/cgi/rapidpdf/cmaj.10077
1v1?ijkey=ab94499c2341afa8cc5a2577e9d6
c9d4b78ea7bb&keytype2=tf_ipsecsha
or http://www.osteoporosis.ca/health-care-
professionals/guidelines/
The Scientific Advisory
Council of Osteoporosis
Canada
Fracture Risk Assessment tool
http://www.sheffield.ac.uk/FRAX/ World Health Organization
General Prevention and Screening:
Musculoskeletal Health
http://transhealth.ucsf.edu/trans?page=proto
col-screening#S6X
Centre of Excellence for
Transgender Health,
University of California San
Francisco
Peer Support
How to support and facilitate peer
engagement in service provision
roles (2013)
http://www.ohtn.on.ca/Pages/Knowledge-
Exchange/Rapid-
Responses/Documents/RR76.pdf
Ontario HIV Treatment
Network
Pregnancy
British Columbia Guidelines for
the Care of HIV-positive Pregnant
Women and Interventions to
Reduce Perinatal Transmission
http://www.cfenet.ubc.ca/therapeutic-
guidelines/pregnant-women
BC Centre for Excellence in
HIV/AIDS
Canadian consensus guidelines for
the management of pregnant HIV-
positive women and their offspring
http://www.bcwomens.ca/NR/rdonlyres/FD
DFFBBA-F070-494F-8A01-
12B19397B2BF/66470/guidelines.pdf
Canadian HIV Trials Network
Working Group on Vertical
HIV Transmission
Guidelines for the Care of Pregnant
Women Living With HIV and
Interventions to Reduce Perinatal
Transmission
http://sogc.org/guidelines/guidelines-care-
pregnant-women-living-hiv-interventions-
reduce-perinatal-transmission-executive-
summary/)
Society of Obstetricians and
Gynaecologists of Canada
Recommendations for Use of
Antiretroviral Drugs in Pregnant
HIV-1-Infected Women for
Maternal Health and Interventions
to Reduce Perinatal HIV
Transmission in the United States
http://aidsinfo.nih.gov/contentfiles/lvguideli
nes/perinatalgl.pdf
U.S. Department of Human
and Health Services

104
Topic/Title URL Issuing Agency
Nutrition
Primary care guidelines for the
management of persons infected
with human immunodeficiency
virus (2014)
http://www.idsociety.org/uploadedFiles/IDS
A/Guidelines-
Patient_Care/PDF_Library/HIV%20Primary
%20Care.pdf
HIV Medicine Association of
the Infectious Diseases
Society of America
Primary Care Approach to the
HIV-infected Patient (2014)
http://www.hivguidelines.org/wp-
content/uploads/2014/11/primary-care-
approach-to-the-hiv-infected-patient.pdf
New York State Department
of Health AIDS Institute
A Guide to Primary Care for
People With HIV/AIDS (2004)
http://www.hab.hrsa.gov/tools/primarycareg
uide/index.htm
U.S Department of Health and
Human Services
Guide for HIV/AIDS clinical care
(2014)
http://hab.hrsa.gov/deliverhivaidscare/2014g
uide.pdf
U.S Department of Health and
Human Services
Primary Care of Veterans with HIV
(2011)
http://www.hiv.va.gov/provider/manual-
primary-care/index.asp
U.S. Department of Veterans
Affairs
Transgender Primary Medical
Care: Suggested Guidelines for
Clinicians in British Columbia
(2014)
http://lgbtqpn.ca/wp-
content/uploads/woocommerce_uploads/201
4/08/Guidelines-primarycare.pdf
Transcend Transgender
Support & Education Society
and Vancouver Coastal Health
Renal
Clinical Practice Guideline for the
Management of Chronic Kidney
Disease in Patients Infected With
HIV: 2014 Update
http://cid.oxfordjournals.org/content/early/2
014/09/12/cid.ciu617.full.pdf+html
HIV Medicine Association of
the Infectious Diseases
Society of America
Respiratory
COPD guidelines http://www.respiratoryguidelines.ca/ Canadian Thoracic Society
Sexually Transmitted Infections
British Columbia Treatment
Guidelines: Sexualy Transmitted
Infections in Adolescents and
Adults (2014)
http://www.bccdc.ca/NR/rdonlyres/46AC4A
C5-96CA-4063-A563-
0BA9F4A0A6E9/0/CPS_BC_STI_Treatmen
t_Guidelines_20112014.pdf
BC Centre for Disease Control
Sexually Transmitted Infections
(Section I)
http://www.bccdc.ca/dis-cond/comm-
manual/CDManualChap5.htm
BC Centre for Disease Control
Canadian Guidelines on Sexually
Transmitted Infections (2014)
http://www.phac-aspc.gc.ca/std-mts/sti-
its/cgsti-ldcits/index-eng.php
Public Health Agency of
Canada. Expert Working
Group for the Canadian
Guidelines on Sexually
Transmitted Infections.
Management of STIs in HIV-
infected patients (2009)
http://www.hivguidelines.org/clinical-
guidelines/adults/management-of-stis-in-hiv-
infected-patients/
New York State Department
of Health AIDS Institute
Tuberculosis
Tuberculosis Manual: Interferon
Gamma Release Assay Testing
Guideline for Diagnosis of Latent
Tuberculosis Infection by
Physicians (2014)
http://www.bccdc.ca/NR/rdonlyres/F34F072
5-9087-457D-8059-
F30BE18946C4/0/TB_manual_IGRA_guide
lines.pdf
BC Centre for Disease Control
Canadian Tuberculosis Standards
(2014)
http://www.respiratoryguidelines.ca/sites/all/
files/Canadian_TB_Standards_7th_Edition_
ENG.pdf
Public Health Agency of
Canada and Canadian Lung
Association

105
CONTACT LIST (Revised March 2015)
Provincial HIV/AIDS Service Organizations
Organization Local Number Other Number Website
BC Centre for Excellence in
HIV/AIDS For HIV treatment and management or
guideline inquiries
604-806-8477 HIV/AIDS Treatment
Program Information Line
604-806-8515 Drug Resistance Testing
1-800-517-1119
www.cfenet.ubc.ca
REACH Telephone Line Rapid Expert Advice and Consultation in
HIV – a 24 hour line available to connect
all physicians, nurses and pharmacists in
BC to infectious disease specialists, GP
HIV specialists or HIV-experienced
pharmacists
604-681-5748
1-800-665-7677
N/A
RACE Telephone Line Rapid Access to Consultative Expertise –
a provincial shared care telephone advice
line for family physicians. When calling,
request BC-CfE for HIV primary care.
604-696-2131
1-877-696-2131
N/A
St. Paul’s Hospital
Pharmacy To reach an HIV-experienced pharmacist
if you practice in British Columbia.
1-888-511-6222
N/A
BC-CfE HIV Preceptorship
Training Program
604-806-8415 N/A www.education.cfenet.ubc.ca
Email: [email protected]
BC Centre for Disease
Control For HIV testing and other STI inquiries
604-707-5600 N/A www.bccdc.ca
Oak Tree Clinic Inquiries regarding specialized HIV care
for HIV-positive women, pregnant
women, partners, children, and youth
604-875-2212 1-888-711-3030 www.bcwomens.ca/Services/H
ealthServices/OakTreeClinic/
Organization Local Number Other Number Website
Positive Living Society of BC
604-893-2200 1-800-994-AIDS www.positivelivingbc.org
Positive Women’s Network 604-692-3000
1-866-692-3001
www.pwn.bc.ca
YouthCO HIV & Hep C
Society
604-688-1441 1-877-968-8426 www.youthco.org
Healing Our Spirit, BC
Aboriginal HIV/AIDS Society
604-879-8884 1-866-745-8884 www.healingourspirit.org
Western Canadian Paediatric
AIDS Society
604-684-1701 N/A www.campmoomba.com
Pacific AIDS Network (PAN) 604-569-1998
N/A www.pacificaidsnetwork.org

106
APPENDICES
Appendix 1: AIDS-defining conditions* (New Appendix added March 2015)
(Require concurrent positive HIV serology to be diagnostic of AIDS)
Bacterial pneumonia, recurrent
Candidiasis (esophageal, bronchi, trachea or lungs)
Cervical cancer, invasive
Coccidioidomycosis (disseminated or extrapulmonary)
Cryptococcosis (extrapulmonary)
Cryptosporidiosis (chronic intestinal)
Cytomegalovirus disease (other than liver, spleen, nodes)
Cytomegalovirus retinitis (with loss of vision)
Encephalopathy, HIV-related (dementia)
Herpes simplex virus (chronic ulcers or bronchitis, pneumonitis or esophagitis)
Isosporiasis, chronic intestinal
Kaposi sarcoma
Lymphoma (Burkitt, immunoblastic, primary in brain)
Mycobacterium avium complex or M. kansasii (disseminated or extrapulmonary)
Mycobacterium of other species (disseminated or extrapulmonary)
Mycobacterium tuberculosis (pulmonary, disseminated or extrapulmonary)
Pneumocystis jiroveci (formerly carinii) pneumonia
Progressive multifocal leukoencephalopathy
Salmonella septicemia, recurrent
Toxoplasmosis of brain
Wasting syndrome due to HIV
*Adapted from Canadian Guidelines on Sexually Transmitted Infections, Public Health Agency
of Canada (http://www.phac-aspc.gc.ca/std-mts/sti-its/cgsti-ldcits/section-5-8-eng.php#table-3)
with data from Health and Welfare Canada. Revision of the CDC surveillance case definition for
acquired immunodeficiency syndrome. CDWR 1987;13-38:169–177; and from Revision of the
surveillance case definition for AIDS in Canada. CCDR 1993;19-15:116–117.

107
Appendix 2: Signs and symptoms associated with HIV Seroconversion Syndrome/Acute
Retroviral Syndrome and their frequency*
Fever (80%)
Tired or fatigued (78%)
Malaise (68%)
Arthralgias (54%)
Headache (54%)
Loss of appetite (54%)
Rash (51%)
Night sweats (51%)
Myalgias (49%)
Nausea (49%)
Diarrhea (46%)
Fever and rash (46%)
Pharyngitis (44%)
Oral ulcers (37%)
Stiff neck (34%)
Weight loss (>5 lb; 2.5 kg) (32%)
Confusion (25%)
Photophobia (24%)
Vomiting (12%)
Infected gums (10%)
Sores on anus (5%)
Sores on genitals (2%)
*Adapted from HIV Clinical Resource, New York State Department of Health AIDS Institute
(http://www.hivguidelines.org/clinical-guidelines/adults/diagnosis-and-management-of-acute-
hiv-infection/) with data from Hecht FM, Busch MP, Rawal B, et al. Use of laboratory tests and
clinical symptoms for identification of primary HIV infection. AIDS 2002;16:1119-1129.

108
Appendix 3: HIV-Related History (Appendix updated March 2015)
General
History
Review sources of past medical care; obtain medical records whenever possible
Past hospitalizations, past and current illnesses
Tuberculosis history
o Possible recent exposure to tuberculosis
o History of positive purified protein derivative (PPD), Mycobacterium tuberculosis (TB)
disease, or treatment of latent TB infection
History of hepatitis A, B and C
Current prescription and non-prescription medicines, including complementary and alternative
medicines and hormones
Vaccination history including hepatitis A and B series, pneumococcal vaccine, flu shots,
tetanus
Reproductive history, including pregnancies, births, termination of pregnancy; current
contraceptive use and needs
Partner information for disclosure of HIV status
Allergies
Travel history/place of birth
Occupational history and hobbies
Pets/animal exposures
HIV Related
History
HIV exposure history
o Date and place of the diagnosis
o Route of exposure, if known
Most recent viral load and CD4 cell count
Seroconversion illness
Nadir CD4 cell count and peak viral load
Drug-resistance testing (Genotype)
Current and previous antiretroviral regimens and date of initiation of ARV therapy
Previous adverse ARV drug reactions
Opportunistic infections
Previous adverse reactions to drugs used for opportunistic infection prophylaxis
Providers who have been involved in the patient’s HIV treatment
Patient’s understanding of HIV disease and treatment
Mental
Health
History
Mental health diagnoses, especially:
o Depression
o Anxiety
o Post-traumatic stress disorder
o Suicidal/violent behaviour
o Severe and persistent mental illness
Psychotropic medications
Past psychiatric hospitalizations
Contact information for mental health providers if applicable

109
*Adapted from: Primary Care Approach to the HIV-Infected Patient. Office of the Medical Director, New
York State Department of Health AIDS Institute. November 2014.
Substance
Use History
Types of drugs; past and current use
o Street drugs—marijuana, cocaine, heroin, methamphetamine, ecstasy, etc.
o Illicit use of prescription drugs
o Alcohol
o Tobacco
Frequency of use and usual route of administration
Risk behaviours—drug/needle sharing, exchanging sex for drugs, sexual risk-taking while
under the influence of drugs or alcohol
History of treatment and barriers to treatment
Sexual
History
Current sexual activity
History of sexually transmitted infections—syphilis, herpes simplex, genital warts, chlamydia,
gonorrhea, chancroid
Sexual practices—vaginal, anal, oral
Gender identity
Past and current partners
Risk behaviour assessment, including use of latex or polyurethane barriers, number of partners
Psycho-social
Assessment
Housing status
Employment and insurance status
Educational level
Family and partner contacts
Stability of personal relationships
o Domestic violence screening
Immigration status
Review of
Systems
Constitutional—weight loss, malaise, fevers, night sweats, changes in appetite, changes in
sleep, adenopathy
Eyes—change in vision, including blurry vision, double vision, flashes of light, or loss of
vision
Ears, nose, throat—dysphagia, odynophagia, hearing loss, discharge, dental pain, periodontal
disease, oral herpes simplex, oral thrush, oral hairy leukoplakia
Pulmonary—cough, dyspnea at rest or on exertion, hemoptysis, sputum
Cardiac—chest pain, palpitations, heart murmur
Abdominal—nausea, vomiting, diarrhea, constipation, blood per rectum, hemorrhoids
Genitourinary:
o Vaginal or penile discharge, vaginal pain, dysuria, genital/rectal warts (Human Papilloma
Virus), classic and atypical herpes simplex virus
o Obstetrics/gynaecology - menstrual status, bleeding, infections, last Pap test and result
o Anal Pap status
Extremities—muscle wasting, muscle weakness, muscle pain, joint swelling
Neurologic—cognitive changes; tingling, burning, pain, or numbness in the extremities;
weakness

110
Appendix 4: HIV-Related Physical Examination (Appendix updated March 2015)
Blood Pressure, Weight, and
Symptoms 2
Assess at each visit
Pain Assessment
Assess at each visit
General Body habitus, obesity, wasting, lipodystrophy, frailty, and ambulatory
ability.
Ophthalmologic If possible perform or refer for a funduscopic examination3 when CD4 cell
count <50 cells/mm3
Pallor or icterus
Head, Ears, Nose, Throat
Sinus infection, odynophagia, dysphagia, hearing loss . parotid
enlargement
Oral Oral candidiasis (thrush), hairy leukoplakia (examine lateral borders of
tongue), Kaposi’s sarcoma, gingival disease, aphthous ulcers
Dermatologic Rash, pruritus, psoriasis, molluscum contagiosum, seborrheic dermatitis,
Kaposi’s sarcoma, onychomycosis, diffuse folliculitis with pruritus,
melanoma, medication-related rash, cutaneous fungal infections, purpura,
petechial, herpes simplex and zoster infections.
Lymph Nodes 4 Generalized or localized lymphadenopathy.
Endocrinologic Abnormal subcutaneous fat redistribution
Thyroid gland assessment
Pulmonary
Lung fields for wheezes, rhonchi, rales, or dullness
Cardiac Examination Heart rhythm, heart murmur, click, or rub, peripheral edema, peripheral
pulses.
Abdominal Hepatosplenomegaly, multiple lipomata in the subcutaneous fat, increased
visceral fat, abdominal masses or tumours, tenderness.
Genital Genitourinary - vaginal or penile discharge, vaginal pain, ulcerative genital
disease - venereal warts
Obstetrics/gynaecology - careful pelvic examination (refer to Section VI:
Special Consideration for Women and Transgender Individuals with HIV)
Rectal Visible anal lesions or evidence of skin abnormality around the anus,
ulcers, warts, fissures, haemorrhoids, tumors
Digital rectal exam

111
Musculoskeletal
Extremities, muscle wasting
Joint inflammatory changes
Neuropsychiatric Reflex, sensory, motor, and gait abnormalities
Signs of multifocal motor and sensory nerve abnormalities, especially
peripheral neuropathy
Cranial nerves
Cognitive status examination, attention, memory, speech problems
Mental health and substance use assessment
*Adapted from: Primary Care Approach to the HIV-Infected Patient. Office of the Medical Director, New
York State Department of Health AIDS Institute. November 2014.
1
Assessment of symptoms may require direct questioning because patients may not consider
their symptoms important until after the symptoms have already caused significant morbidity. 2 Except where indicated, each element should be performed at baseline and at least annually.
3 Patients with CD4 cell counts <50 cells/mm
3 should be examined by an ophthalmologist at
baseline and every 6 months. 4 Significant abnormalities may present as clusters of large nodes, asymmetry, tenderness, or
sudden increase in size or firmness of nodes.

112
Appendix 5: Screening for non-infectious comorbid conditions in HIV-positive individuals (Appendix updated March 2015,
Adapted from EACS guidelines for Prevention and Management of Non-infectious Co-morbidities in HIV, version 7.0)
Assessment Pre-ART baseline Follow-up on ART* Comments
General
Medical
History
Personal and family
history of relevant
comorbid conditions (e.g.
premature cardiovascular
disease, hypertension,
diabetes, osteoporosis,
liver disease, chronic
kidney disease)
+
Update all at each visit
(<q 6mos)
Concomitant medications +
Lifestyle (smoking,
alcohol, recreational
drugs, diet, exercise)
+
Cardiovascular
disease
Risk assessment
(Framingham risk score)
+
At each visit
(<q 6mos) Framingham Risk Score may underestimate risk in HIV
Consider using Reynolds Risk Score
Consider measuring apolipoprotein B especially in
patients with hypertriglyceridemia
Manage hypertension and dyslipidemia per general
population guidelines; NB potential drug interactions
with ART
Address modifiable risk factors where possible
Monitor ECG if receiving protease inhibitors and/or
rilpivirine with concomitant agents associated with
cardiac conduction abnormalities
Blood pressure + <q 6mos
Fasting lipids (total,
HDL, and LDL
cholesterol, triglycerides)
or apolipoprotein B
+ q6 mo
Diabetes Fasting blood sugar or
HbA1C
+ Q 6 months Manage blood glucose abnormalities per Diabetes
Canada guidelines, with lifestyle changes first (weight
loss, diet, exercise)
NB potential drug interactions with ART

113
Appendix 5: Screening for non-infectious comorbid conditions in HIV-positive individuals (Continued)
Assessment Pre-ART baseline Follow-up on ART* Comments
Bone disease
(osteopenia/
osteoporosis)
Osteoporosis risk
assessment (family
history, exercise, weight,
smoking, alcohol,
calcium and vitamin D
intake)
+
At each visit (<q
6months) FRAX not validated for use in Canada or in patients
with HIV
Recommend supplementation with Vitamin D 1000-
2000 IU/day for prevention
Recommend calcium supplementation if dietary intake
inadequate
Perform DXA in HIV+ patients of any age with a
history of fragility fractures or significant risk factors
for osteoporosis
Fracture risk assessment
(FRAX)
+ At each visit (<q 6
months)
DXA scan + for post-
menopausal women,
men age >50 years
Intervals determined
by BC guidelines
Renal disease Risk assessment
including nephrotoxic
medications
+ <q 6months
Increased risk for renal disease associated with family
history, black race, age >50 years, advanced HIV
disease (low CD4 nadir), diabetes, hypertension,
hepatitis B/C, other liver disease, concomitant
nephrotoxic medications including NSAIDs and some
recreational drugs
Increased risk of renal toxicity with certain
antiretrovirals, particularly tenofovir DF and indinavir,
also possibly with atazanavir, lopinavir/ritonavir
Diagnosis of abnormalities may require referral to a
nephrologist and possible renal biopsy
Blood pressure
+ <q 6months
Serum creatinine and
eGFR; urinalysis; spot
urine for albumin to
creatinine ratio
+ q3-4 mo initially, then
q6 mo when stable
Hypogonadism Morning serum total
testosterone
+ Only in
symptomatic men
Only in symptomatic
men Symptoms may include decreased libido, erectile
dysfunction, reduced bone mass or low trauma fractures,
hot flashes or sweats, weight loss, reduced muscle
strength or exercise capacity, sleep disturbance, fatigue,
or depression
Lung disease Chest X-ray + If symptomatic consider chest CT in presence of significant symptoms,
especially in smokers
Liver disease Abdominal ultrasound + (if HBV+ or
HCV+)
Q 6 mo if HBV+ (any
stage fibrosis) or
HCV+ with cirrhosis

114
* Frequency of laboratory monitoring may be adjusted according medical history of relevant co-morbid conditions, potential toxicities of specific
antiretroviral drugs and concomitant medications, previous or ongoing laboratory abnormalities, and clinical status.
ART, antiretroviral therapy
CT, computed tomography
DXA, dual energy absorptiometry
ECG, electrocardiogram
eGFR, estimated glomerular filtration rate
HbA1C, glycated hemoglobin
NSAIDs, non-steroidal anti-inflammatory drugs