PREVIEW OF EMT/EMR PEDIATRIC EMERGENCIES POWERPOINT TRAINING PRESENTATION
24
PREVIEW OF EMT/EMR PEDIATRIC EMERGENCIES POWERPOINT TRAINING PRESENTATION
-
Upload
bruce-vincent -
Category
Education
-
view
92 -
download
0
Transcript of PREVIEW OF EMT/EMR PEDIATRIC EMERGENCIES POWERPOINT TRAINING PRESENTATION

PREVIEW OF
EMT/EMR PEDIATRIC EMERGENCIESPOWERPOINT TRAINING
PRESENTATION

GENERAL CONSIDERATIONSMany components of the initial evaluation can be
done by careful observation without touching the patientWhen appropriate, utilize the parent/guardian to help the infant or child be more comfortable with your exam & treatmentCommunicating with scared, concerned parents &
family is important when caring for an ill infant or child
Continue assessment until care is transferred

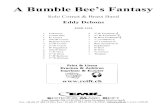
Subarachnoidspace

AIRWAY COMPAIRED TO AN ADULTS
Smaller in diameter & shorter in lengthJaw is smaller with infant’s tongue taking up
more room in the oropharynxInfants are nasal breathersTracheal cartilage is softer & more collapsibleEpiglottis of infants & toddlers is long, floppy,
narrow & extends at a 450 angle into airway

ABDOMINAL DIFFERENCE
Less-developed abdominal muscles & organs situated more anteriorly, therefore less protection of rib cageLiver & spleen are proportionally largerImplications for the health care provider
Seemingly insignificant forces can cause serious internal injuryLiver, spleen, and kidneys are more frequently injuredMultiple organ injury common

EXTREMITIES AS COMPAIRED TO AN ADULTS
Bones are softerOpen growth plates are weaker
than ligaments & tendons, so injury to growth plate can result in length discrepancies
Drawing byBruce Blaus

NERVOUS SYSTEM AND SPINAL COLUMN COMPARED TO AN ADULT’S
Brain tissue & vascular system is more fragile & prone to bleeding from injury
Subarachnoid space is relatively smaller, with less cushioning effect for brain
Pediatric brain requires nearly twice the cerebral blood flow as does an adult’sBrain & spinal cord less well protected

IMPLICATIONS FOR THE HEALTHCARE PROVIDER
The large cerebral blood flow requirement increases risk of hypoxia; hypoxia and hypotension in a child with a head injury can cause ongoing damageHead momentum may result in bruising and damage to the brain Spinal cord injuries less commonCervical spine injuries more commonly ligamentous injuries

GROWTH & DEVELOPMENT IN INFANCY BIRTH TO TWO MONTHS
Cognitive developmentCrying form of communicationInfants cry for obvious reasons such as
hunger and needing to be changedWhen obvious reasons for crying have been
addressed, persistent crying can be a sign of significant illness

IMPLICATIONS FOR THE HEALTH CARE PROVIDER
Persistent crying or irritability in a 0 to 2month-old can be a symptom of serious illnessInfants sleep a lot, however should arouse easily; inability to arouse a baby should be considered an emergencyHead control is limited

IMPLICATIONS FOR THE HEALTHCARE PROVIDER
They not like to be separated from parentsThey do not want an oxygen mask (do NOT
blow in face) Need to be kept warm - make sure hands
and stethoscope are warmed before touching child

GROWTH & DEVELOPMENTEIGHTEEN TO TWENTY-FOUR MONTHS
Physical developmentImproved gait and balanceBegin to run and climb
Cognitive developmentBegin to understand cause and effectBegin to label objectsTen to 15 words becomes 100 by 24 months
Emotional developmentClinginess with parentsAttachment to a special object, like a blanket

IMPLICATIONS FOR THE HEALTH CARE PROVIDER
Persistent crying or irritability can be a symptom of serious illness
Allow a child to hold objects of importance to them (e.g., blanket)
Children no longer require shoulder rolls to limit flexion of the neck when bag-valve-mask ventilating or intubating
Painful procedures make lasting impressions

GENERAL CONSIDERATIONS OF ASSESSMENT
Many components of the initial evaluation can be done by careful observation without touching the patient
When appropriate, utilize the parent/guardian to help the infant or child be more
comfortable with your exam and therapies

PREPARING FOR ARRIVAL
Assembling age-appropriate equipmentReviewing age-appropriate vital signs and anticipated development

PATIENT ASSESSMENT
“Pediatric Assessment Triangle” consists ofGeneralComponentsPossible physiologic state

GENERAL
Provides a 15- to 30-second assessment of theseverity of the patient’s illness or injury
Use prior to addressing “the ABCs”Does not require touching the
patient, just looking and listening

FOCUSED HISTORY
Symptoms and durationFeverActivity levelRecent eating, drinking, and urine output historyHistory of vomiting, diarrhea, or abdominal painNote any rashes
Medications taking and medication allergiesPast medical problems or chronic illnessesKey events leading to the injury or illness

ASSESSMENT
HistoryPhysical findings
Are respirations within normal limitsLabored breathingAbnormal chest rise & fallTripod positioning

SPECIFIC CONDITIONS
MeningitisAltered mental statusClosed head injury
Bleeding inside skullFractures

ALTERED MENTAL STATUS
Primarily caused by Hypoglycemia PoisoningSeizure InfectionHead trauma HypoxiaShock Fatigue
Cause should be determined for appropriate care
Have understanding of normal mental status

MANAGEMENT
Altered mental statusAssess for need to protect airwayAssess and intervene for increased
intracranialSupplemental oxygen as necessary

MOTOR VEHICLE PASSENGERS
Unrestrained passengers have head and neck injuries
Restrained passengers have abdominal and lower spine injuriesStruck while riding bicycle - head injury, spinal
injury, abdominal injuryPedestrian struck by vehicle - abdominal injury
with internal bleeding, possible painful, swollen, deformed thigh, head injury

To purchase this presentation go to www.bravetraining.com
Or tap the above link