Prevention of thrombus embolization during primary percutaneous intervention using a novel mesh...
6
Case Reports Prevention of Thrombus Embolization During Primary Percutaneous Intervention Using a Novel Mesh Covered Stent Ajay Jain, * MD, MRCP , Roshan Weerackody, MRCP , Simon Kennon, and Martin Rothman FRCP , FESC, FACC Embolization of athero-thrombotic material during primary percutaneous coronary intervention is a common cause of periprocedural complication. Methods developed to reduce embolization include thrombus aspiration, and distal protection. We report five cases of primary percutaneous intervention to coronary arteries that contain large amounts of thrombus, using a novel mesh covered stent. The mesh covering of the stent is designed such that it is theoretically able to ensnare thrombus and thus prevent distal migration of embolic material. In all cases, TIMI grade III flow was achieved at the end of the procedure, despite the extensive thrombus burden. ' 2009 Wiley-Liss, Inc. Key words: percutaneous intervention; thrombosis; acute coronary syndrome INTRODUCTION The embolization of degenerative atheromatous ma- terial and thrombus into the distal vascular bed during both planned and emergency percutaneous coronary intervention (PCI), is an important cause of procedural complication, from elevation in markers of myocardial damage to ST elevation myocardial infarction (STEMI) [1]. In the era of primary PCI (PPCI) for STEMI the risk of thrombus propagation is particularly high, and angiographic evidence of embolism is seen to occur in up to 15% of cases [2]. Distal embolization of throm- bus or atheromatous material may result in occlusion of the microvascular bed resulting in suboptimal reper- fusion [3,4]. Debris may be seen to embolise spontane- ously, as a result of instrumentation within the vessel during PCI or as a result of balloon dilatation in patients not suitable for direct stent implantation [5]. Several percutaneous strategies have been developed in attempt to reduce the risk of distal embolization, these include, distal protection devices and thrombus aspiration. Despite the theoretical benefits of distal pro- tection, the effectiveness of these devices in the setting of PPCI for STEMI is not proven. The ‘‘Enhanced Myocardial Efficacy and Recovery by Aspiration of Liberated Debris’’ (EMERALD) trial randomized 500 patients to angioplasty with or without GuardWire dis- tal protection [6]. The use of distal protection provided no benefit in terms of the rapidity of ST-segment reso- lution, final infarct size or the incidence of 6-month major adverse cardiac events (MACE). A similar nega- tive result was found in the ‘‘Protection Devices in PCI Treatment of Myocardial Infarction for Salvage of Endangered Myocardium’’ (PROMISE) trial, which randomized 200 patients undergoing PPCI to protection with or without adjunctive FilterWire [7]. Thrombus aspiration catheters have also been inves- tigated in the setting of primary PCI. Early studies suggested that thrombus aspiration in the setting of STEMI conferred no benefit over conventional therapy. The recent ‘‘Thrombus Aspiration during Percutaneous Coronary Intervention in Acute Myocardial Infarction’’ (TAPAS) study has shown that thrombus aspiration Conflict of interest: Nothing to report. Department of Cardiology, Bart’s and The London NHS Trust, London, UK *Correspondence to: Martin T. Rothman, Bonner Road, Bethnal Green, London, E2 9JX. E-mail: [email protected] Received 14 November 2008; Revision accepted 23 December 2008 DOI 10.1002/ccd.21981 Published online 9 April 2009 in Wiley InterScience (www. interscience.wiley.com). ' 2009 Wiley-Liss, Inc. Catheterization and Cardiovascular Interventions 74:88–93 (2009)
Transcript of Prevention of thrombus embolization during primary percutaneous intervention using a novel mesh...

Case Reports
Prevention of Thrombus Embolization DuringPrimary Percutaneous Intervention Using a
Novel Mesh Covered Stent
Ajay Jain,* MD, MRCP, Roshan Weerackody, MRCP, Simon Kennon,and Martin Rothman FRCP, FESC, FACC
Embolization of athero-thrombotic material during primary percutaneous coronaryintervention is a common cause of periprocedural complication. Methods developed toreduce embolization include thrombus aspiration, and distal protection. We report fivecases of primary percutaneous intervention to coronary arteries that contain largeamounts of thrombus, using a novel mesh covered stent. The mesh covering of thestent is designed such that it is theoretically able to ensnare thrombus and thus preventdistal migration of embolic material. In all cases, TIMI grade III flow was achieved at theend of the procedure, despite the extensive thrombus burden. ' 2009 Wiley-Liss, Inc.
Key words: percutaneous intervention; thrombosis; acute coronary syndrome
INTRODUCTION
The embolization of degenerative atheromatous ma-terial and thrombus into the distal vascular bed duringboth planned and emergency percutaneous coronaryintervention (PCI), is an important cause of proceduralcomplication, from elevation in markers of myocardialdamage to ST elevation myocardial infarction (STEMI)[1]. In the era of primary PCI (PPCI) for STEMI therisk of thrombus propagation is particularly high, andangiographic evidence of embolism is seen to occur inup to 15% of cases [2]. Distal embolization of throm-bus or atheromatous material may result in occlusionof the microvascular bed resulting in suboptimal reper-fusion [3,4]. Debris may be seen to embolise spontane-ously, as a result of instrumentation within the vesselduring PCI or as a result of balloon dilatation inpatients not suitable for direct stent implantation [5].Several percutaneous strategies have been developed
in attempt to reduce the risk of distal embolization,these include, distal protection devices and thrombusaspiration. Despite the theoretical benefits of distal pro-tection, the effectiveness of these devices in the settingof PPCI for STEMI is not proven. The ‘‘EnhancedMyocardial Efficacy and Recovery by Aspiration ofLiberated Debris’’ (EMERALD) trial randomized 500patients to angioplasty with or without GuardWire dis-tal protection [6]. The use of distal protection provided
no benefit in terms of the rapidity of ST-segment reso-lution, final infarct size or the incidence of 6-monthmajor adverse cardiac events (MACE). A similar nega-tive result was found in the ‘‘Protection Devices inPCI Treatment of Myocardial Infarction for Salvage ofEndangered Myocardium’’ (PROMISE) trial, whichrandomized 200 patients undergoing PPCI to protectionwith or without adjunctive FilterWire [7].Thrombus aspiration catheters have also been inves-
tigated in the setting of primary PCI. Early studiessuggested that thrombus aspiration in the setting ofSTEMI conferred no benefit over conventional therapy.The recent ‘‘Thrombus Aspiration during PercutaneousCoronary Intervention in Acute Myocardial Infarction’’(TAPAS) study has shown that thrombus aspiration
Conflict of interest: Nothing to report.
Department of Cardiology, Bart’s and The London NHS Trust,London, UK
*Correspondence to: Martin T. Rothman, Bonner Road, Bethnal
Green, London, E2 9JX.
E-mail: [email protected]
Received 14 November 2008; Revision accepted 23 December 2008
DOI 10.1002/ccd.21981
Published online 9 April 2009 in Wiley InterScience (www.
interscience.wiley.com).
' 2009 Wiley-Liss, Inc.
Catheterization and Cardiovascular Interventions 74:88–93 (2009)

prior to balloon angioplasty and stent implantationimproves TIMI blush score, but the incidence of death,reinfarction, or target-vessel revascularization nor acombination of these events, was not significantly dif-ferent between the group with and the group withoutaspiration [8].An alternative approach to reduce the risk of the lib-
eration of embolic material during primary PCI isthrombus entrapment, in effect blocking embolic mate-rial at source. All intra-coronary stents are suggestedto carry out this function to some extent; however it isclear that the ‘‘pore’’ size in conventional stents is farlarger that the size of particulate matter produced dur-ing PCI with 50% of particles approx 100 lm in diam-eter. Furthermore in the presence of friable thrombus astent is unlikely to effectively reduce the risk ofthrombus propagation. A commercially available prod-uct with the capability to trap embolic material atsource is the MGuardTM stent (InspireMD). TheMGuard is a proprietary metal stent covered with an
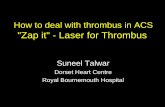
ultra thin, micron level flexible mesh sleeve fabricatedby circular knitting (Fig. 1). During deployment of thestent, the flexible mesh freely expands over the stentstruts, the pores open in parallel with the stent, ‘‘sand-wiching’’ embolic and prothrombotic material betweenthe flexible mesh and the intima. The net has beenengineered such that at optimal balloon expansion thepore size is tailored to optimally reduce embolization.Unlike a ‘‘covered’’ stent, side branches are not obliga-torily occluded, as the mesh theoretically allows nor-mal perfusion into branch vessels.We report five cases of primary PCI in patients pre-
senting with ST elevation myocardial infarction. Ineach case a significant thrombus burden was seen inthe vessel at diagnostic angiography. The lesions weresuccessfully treated by implantation of MGuard stent,without any angiographic evidence of distal emboliza-tion of thrombus. Demographic data, target vessel,TIMI grade flow pre and post intervention, and cardiactroponin I measurements are shown in Table 1.
CASE REPORTS
Case 1
A 53 year old patient presented with 48 h history ofintermittent chest pain at rest. The patient reported noprevious cardiac symptoms and was a current smoker.On the day of admission she had suffered severe painat rest and an ECG showed anterior STEMI. The diag-nostic angiogram showed a segment of severe stenosisextending from proximal to mid LAD, with adherentthrombus (Fig. 2, panel A). After guide wire passagebeyond the stenosis, the lesion was treated by directimplantation of two overlapping MGuard stents (3.253 19 mm and 3.5 3 12 mm), without predilatation ofthe lesion. Following stent deployment, there wasTIMI III flow and normal myocardial blush, with noangiographic evidence of distal embolization of throm-bus (Fig. 2, panel B).
Case 2
A 56 year old man was admitted with left sidedchest pain. Initial ECG showed infero-lateral STEMI.Angiography showed severe stenosis in the mid portion
Fig. 1. MGuard stent, with balloon expanded, showing meshcovering.
TABLE I. Table of Culprit Vessel and TIMI Grade of Flow Before and After PrimaryPercutaneous Intervention With MGuard Stent
Case no Age Indication
Culprit
vessel Pre-TIMI Post-TIMI
Post PCI
troponin
1 53 Anterior STEMI LAD 2 3 0.1
2 56 Infero-lateral STEMI Cx 2 3 0.28
3 70 Inferior STEMI RCA 2 3 0.09
4 41 Anterior STEMI LAD 0 3 2.49
5 37 Inferior STEMI RCA 2 3 4.33
Prevention of Thrombus Embolization 89
Catheterization and Cardiovascular Interventions DOI 10.1002/ccd.Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).

of the circumflex artery, with large adherent thrombus(Fig. 3, panel A). A 3.5 3 19 mm MGuard stent wasdirectly implanted across the stenosis without balloonpredilatation. The angiogram following stent implanta-tion suggested residual thrombus at the distal end ofthe stent. This was covered with a further 3.5 3 12mm MGuard stent. The final angiographic appearance
was excellent with TIMI III flow and no angiographicevidence of distal embolization (Fig. 3, panel B).
Case 3
A 70 year old woman with recent onset angina wasadmitted with crescendo angina. The ECG showed in-
Fig. 3. Angiogram showing a tight stenosis in the circumflex coronary artery with adherentthrombus, before and after MGuard stent implantation.
Fig. 2. Angiogram showing a tight stenosis in the proximal left anterior descending coronaryartery with adherent thrombus, before and after MGuard stent implantation.
90 Jain et al.
Catheterization and Cardiovascular Interventions DOI 10.1002/ccd.Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).

ferior STEMI. The diagnostic angiogram showedsevere mid-vessel disease in RCA with extensiveattached thrombus, and TIMI II flow in the target ves-sel (Fig. 4, panel A). The lesion was crossed with awire and following this a 4 3 24 mm MGuard stentwas implanted, this resulted in restoration of TIMI
grade III flow, without angiographic evidence of distalembolization (Fig. 4, panel B).
Case 4
A 41 year old female smoker, with no prior history ofcardiac illness, presented with a 1 h history of chest
Fig. 5. Angiogram showing a thrombotic occlusion of the left anterior descending artery,before and after MGuard stent implantation.
Fig. 4. Angiogram showing thrombus in the right coronary artery, before and after MGuardstent implantation.
Prevention of Thrombus Embolization 91
Catheterization and Cardiovascular Interventions DOI 10.1002/ccd.Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).

pain at rest, the ECG showed anterior STEMI. Sheunderwent diagnostic angiography, which confirmedthrombotic occlusion of the proximal LAD (Fig. 5,panel A). Anterograde flow was restored after passageof a 0.014 @ angioplasty guidewire, but chest pain andST segment elevation on the ECG persisted. The steno-sis in LAD was predilated and treated with 3.5 3 24mm LiberteTM bare metal stent. This resulted in distaldisplacement of thrombus; this was visible as mobilethrombus adherent to the exit of the stent. In an attemptto avoid distal embolization, this area was covered with3.5 3 12 mm MGuard stent. The final result was excel-lent with TIMI III flow within LAD, no visible throm-bus within the treated vessel, and no angiographic evi-dence of distal embolization (Fig. 5, panel B).
Case 5
A 37 year old man with no preceding cardiac his-tory had collapsed after feeling unwell, ECG showedinferior STEMI. Angiography showed severe stenosisin mid RCA disease with considerable thrombus bur-den (Fig. 6, panel A). The lesion was treated by directimplantation of two overlapping 4 3 12 mm MGuardstents. The final angiographic appearance was excellentwith no residual stenosis, and no evidence of distalembolization of thrombus (Fig. 6, panel B).
DISCUSSION
The use of the flexible knitted mesh coveredMGuard stent has several theoretical advantages over
conventional embolic protection, and atherectomy devi-
ces. The embolic protection function of the stent is
deployed at the time of PCI, and as the mesh is on the
stent, there remains an enduring effect after the inter-
vention. The MGuard stent is delivered by conven-
tional means, meaning that delivery is rapid, with no
need for specialist training.
Use of conventional thrombectomy devices allrequire crossing of the thrombus burdened lesion witha guide wire. Filter wires, wherein the guide wireembodies some form of capture technology are bulkierthan a guide wire alone and in themselves may causeembolization. These devices may also not providecomplete capture of thrombus, either because of lim-ited capacity or because the device does not capture100% of all the debris as it passes the capture technol-ogy. Thrombectomy devices track a guide wire thatmust be placed across the lesion and they use aspira-tion as they cross the lesion territory, they are bulkyand may themselves cause embolization. Aspirationdevices that attempt to remain upstream, proximal tothe thrombus still require a guide wire across the terri-tory with thrombus. These devices then attempt toaspirate directly or use a Venturi effect to aspirate.These techniques are not always reliable and occasion-ally the high flow of aspirate may of itself causeembolization. These distal protection devices are de-pendent upon the presence of a suitable anatomy, alanding zone for the device, adequate vessel calibre,and the position of side branches. In contrast the
Fig. 6. Angiogram showing a stenosis in right coronary artery with significant thrombus bur-den, before and after MGuard stent implantation.
92 Jain et al.
Catheterization and Cardiovascular Interventions DOI 10.1002/ccd.Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).

MGuard stent is used as per a conventional stent, andnot constrained by similar anatomical considerations.We report five cases of STEMI in which percutane-
ous intervention using an MGuard stent to ‘‘thrombusrich’’ lesions was successful, without angiographic evi-dence of distal embolization. A randomized controlledtrial of the mesh covered stent versus conventionaltherapy in PPCI for STEMI is warranted.
REFERENCES
1. Ioannidis JP, Karvouni E, Katritsis DG. Mortality risk conferred
by small elevations of creatine kinase-MB isoenzyme after percu-
taneous coronary intervention. J Am Coll Cardiol 2003;42:1406–
1411.
2. Henriques JP, Zijlstra F, Ottervanger JP, et al. Incidence and
clinical significance of distal embolization during primary
angioplasty for acute myocardial infarction. Eur Heart J 2002;23:
1112–1117.
3. Topol EJ, Yadav JS. Recognition of the importance of emboliza-
tion in atherosclerotic vascular disease. Circulation 2000;101:
570–580.
4. Kotani J, Nanto S, Mintz GS, et al. Plaque gruel of atheromatous
coronary lesion may contribute to the no-reflow phenomenon in
patients with acute coronary syndrome. Circulation 2002;106:
1672–1677.
5. Katritsis DG, Korovesis S, Karvouni E, Giazitzoglou E, Theo-
dorou S, et al. Direct versus predilatation drug-eluting stenting: a
randomized clinical trial. J Invasive Cardiol 2006;18:475–479.
6. Stone GW, Webb J, Cox DA, Brodie BR, Qureshi M, et al. Dis-
tal microcirculatory protection during percutaneous coronary
intervention in acute ST-segment elevation myocardial infarction:
a randomized controlled trial. JAMA 2005;293:1063–1072.
7. Gick M, Jander N, Bestehorn HP, Kienzle RP, Ferenc M, et al.
Randomized evaluation of the effects of filter-based distal protec-
tion on myocardial perfusion and infarct size after primary percu-
taneous catheter intervention in myocardial infarction with and
without ST-segment elevation. Circulation 2005;112:1462–1469.
8. Svilaas T, Vlaar PJ, van DHI, Diercks GF, de Smet BJ, et al.
Thrombus aspiration during primary percutaneous coronary inter-
vention. N Engl J Med 2008;358:557–567.
Prevention of Thrombus Embolization 93
Catheterization and Cardiovascular Interventions DOI 10.1002/ccd.Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).