Prevention of preeclampsia Jim Roberts. Introduction The NICHD/NHLBI will soon begin a very large (9...
31
Prevention of Prevention of preeclampsia preeclampsia Jim Roberts
-
Upload
cathleen-bailey -
Category
Documents
-
view
214 -
download
0
Transcript of Prevention of preeclampsia Jim Roberts. Introduction The NICHD/NHLBI will soon begin a very large (9...

Prevention of Prevention of preeclampsiapreeclampsia
Jim Roberts
IntroductionIntroduction
The NICHD/NHLBI will soon begin a very large (9 to 12,000 women) and very expensive study of antioxidant therapy to attempt to prevent the pregnancy complication, preeclampsia.
What background data and principles should guide such a study?

GoalsGoals
What is preeclampsia?Prior attempts to prevent
preeclampsia• What can we learn?
Principles to guide preventive therapyRationale for antioxidant therapy Skeleton of study design (work in
progress)

PreeclampsiaPreeclampsia
Clinical (pregnancy specific syndrome)HypertensionProteinuria
ImpactLeading cause of maternal mortality5 fold increase in perinatal mortality15% of preterm births

Treatment of Treatment of PreeclampsiaPreeclampsia
Delivery!Delivery!
Usually prevents maternal mortality.
Does not prevent maternal morbidity.
Can result in iatrogenic prematurity.

Treatment of Treatment of PreeclampsiaPreeclampsia
The best treatment is prevention!

Preeclampsia Preeclampsia ProphylaxisProphylaxis
HistoryHistory• Salt restriction• Salt supplementation• Protein restriction• Protein
supplementation• Eat less• Eat more• Rest less• Rest more• etc., etc., etc. ...

Principles of Principles of ProphylaxisProphylaxis
• Successful preventive therapy requires:–Sufficient understanding of the disease to direct strategy
–The ability to identify patients at enough risk to justify prophylaxis
• “Prophylactic” treatment may actually be early therapy.
• Preventive therapy must prevent the disease and not merely the diagnosis of the disease.

““Decreasing the Diagnosis”Decreasing the Diagnosis”
Preeclampsia is diagnosed by:• increased blood pressure• proteinuriaThese are not important pathophysiological features!
Drugs which lower BP or prevents proteinuria will reduce the dx.
Have not prevented the disorder only the diagnosis.

Calcium Calcium SupplementationSupplementation
RationaleRationaleHypocalcuria in preeclampsia
? antedates disease Increased intracytoplasmic calcium
platelets: basal yes/nostimulated yes/no
Epidemiologylow calcium diets => more preeclampsia(South and Central America and Africa)

Calcium SupplementationCalcium SupplementationClinical trials and meta-analysisClinical trials and meta-analysis
OR for developing preeclampsia
Marya 1987 Villar 1987 Lopez-Jaramillo 1989 Lopez-Jaramillo 1989 Montanaro 1990 Villar 1990 Beilzan 1991 Cong 1993 Sanchez- Ramos 1994 Pooled Estimate
Favors Calcium Favors Control
0.001 0.01 0.1 1 10

Calcium Calcium SupplementationSupplementation
Clinical trials and meta-analysisClinical trials and meta-analysis
Summary:• Preeclampsia reduced (OR = 0.38)• “PIH” reduced (OR = 0.3)• Blood pressure reduced (5.4 /
3.44)
“The minimal expense and negligible risk ... may justify administration of calcium to even the low risk cohort.”

Calcium Calcium SupplementationSupplementation
NIH trialNIH trial
Design• 4600 low risk nulliparous women• Randomized to 2 gms Ca++ or placebo• Assess calcium intake predelivery• Assess urinary calcium in a subset

Calcium Calcium SupplementationSupplementation
NIH trialNIH trial
Ca++(2295)
Placebo(2294)
RR(95% CI)
Preeclampsia 6.9% 7.3% 0.94(0.76, 1.16)
mild 4.7% 4.8% 0.99(0.76, 1.28)
severe 2.2% 2.6% 0.85(0.78, 1.01)
transient BP a 15.3% 17.3% 0.88(.78, 1.01)
all BP a 22.2% 26.4% 0.9(0.81, 1.00)

Why the Discrepancies?Why the Discrepancies?Calcium Trial SpecificCalcium Trial Specific
Wrong amount of calcium? • not likely
Compliance?
Poor definitions in the meta-analysis?
Supplement ≠ dietary calcium
Different populations?• much more Ca++ deficient
Aspirin for Aspirin for PreeclampsiaPreeclampsia
RationaleRationale“Prostacyclin thromboxane imbalance”
Prostacyclinvasodilator inhibits platelet aggregationmade by endothelium
Thromboxanevasoconstrictor aggregates plateletsmade by platelets

Aspirin for Aspirin for PreeclampsiaPreeclampsia
RationaleRationale“Prostacyclin thromboxane
imbalance”
In preeclampsia the ratio of prostacyclin to thromboxane is reduced (as predicted by the hypothesis)
But ...These agents have very short half
lives (i.e. they do not function as hormones)

Aspirin for Aspirin for PreeclampsiaPreeclampsia
RationaleRationale
“Prostacyclin thromboxane imbalance”
Aspirin given daily, in low doses, preferentially inhibits
thromboxane synthesis.
Aspirin for Aspirin for PreeclampsiaPreeclampsia
Clinical TrialsClinical TrialsIn the mid 1980’s several trials
suggested benefit (less preeclampsia, reduced IUGR, fewer C-sections) in high risk patients.
Quality of trials varied (e.g. historical controls, non-blind etc.)
There were, however, several controlled trials suggesting benefits.

Aspirin for Aspirin for PreeclampsiaPreeclampsia
Meta-analysisMeta-analysisIn 1991 metaanalysis of 6 highest
quality studies (= 394)concluded that ASA:
1. Reduced the incidence of preeclampsia
RR = 0.35 (0.22 - 0.55)2. Reduced the risk of IUGR
RR = 0.56 (0.36 - 0.88)3. Reduced the risk of C-section
RR = 0.34 (0.25 - 0.48)
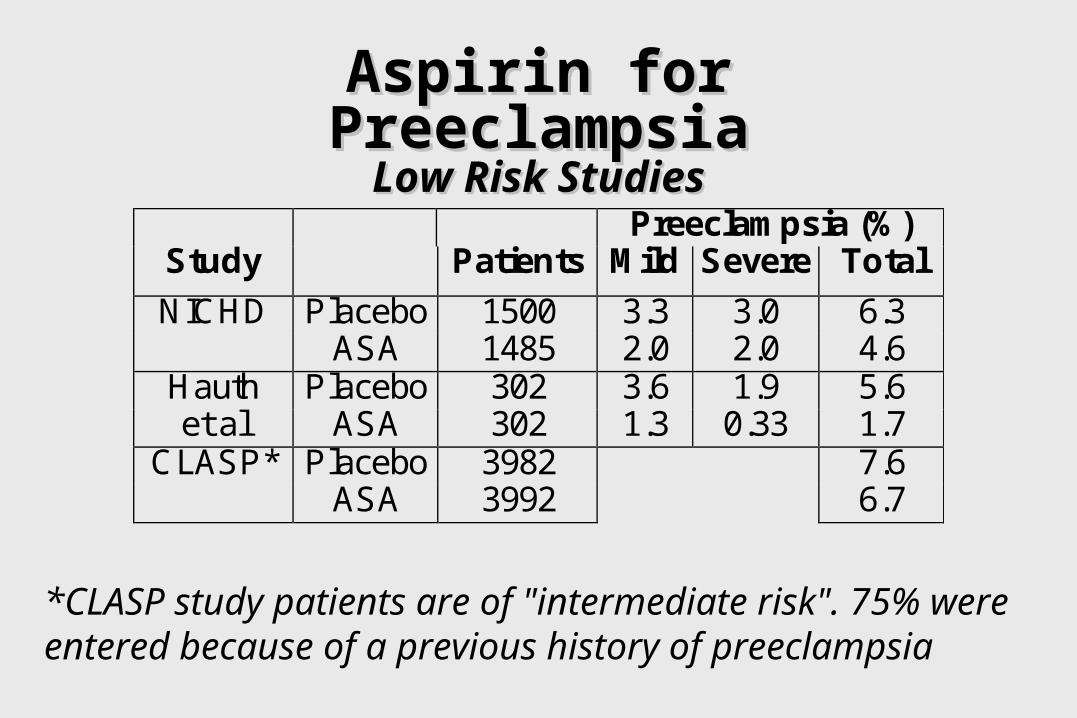
Aspirin for Aspirin for PreeclampsiaPreeclampsiaLow Risk StudiesLow Risk Studies
Preeclampsia (%)Study Patients Mild Severe Total
NICHD Placebo 1500 3.3 3.0 6.3ASA 1485 2.0 2.0 4.6
Hauth Placebo 302 3.6 1.9 5.6et al ASA 302 1.3 0.33 1.7
CLASP* Placebo 3982 7.6ASA 3992 6.7
*CLASP study patients are of "intermediate risk". 75% were entered because of a previous history of preeclampsia

Aspirin for Aspirin for PreeclampsiaPreeclampsia
The NIH High Risk StudyThe NIH High Risk StudyIncidence of
Preeclampsia %Risk Group n ASA PlaceboPregestationalDiabetes
462 18 22
Hypertension 763 26 25Multifetalgestation
678 12 16
Previouspreeclampsia
600 17 19
All groups 2503 18 20

Aspirin for Aspirin for PreeclampsiaPreeclampsia
Cochranne MetanalysisCochranne Metanalysis35,000 women have taken ASA in RCT!
reduced preterm birthreduced perinatal mortalitystatisticaly but ? Clinically significant
Why so small an effect?Subsets?Wrong dose?Wrong time in gestation?Wrong time of day?

Why the Discrepancies?Why the Discrepancies?General metaanalysis vs. trialGeneral metaanalysis vs. trial
GIGO (garbage in = garbage out)
Publication bias• small negative trials do not get published (or submitted)
(at time of CLASP there were as many patients in unpublished studies as there were in the
positive trials cited in the 1991 meta-analysis)

Why the Discrepancies?Why the Discrepancies?General meta-analysis vs. trialGeneral meta-analysis vs. trial
Although the limitations of metaanalysis likely explain discrepancy, a caution is necessary.
• In large trials population is much less homogeneous than single center trials.
• Preeclampsia is heterogeneous.
• Perhaps only certain subsets benefit from a specific therapy.

What have we learned?What have we learned?
Meta-analysis is not a substitute for large clinical trials.
In testing preventive therapy for preeclampsia some marker of perinatal well being is the appropriate outcome.
It may be necessary to identify subsets of preeclamptic patients for effective early therapy.

Future DirectionsFuture Directions Identifying targets for therapyIdentifying targets for therapy
Preeclampsia:• manifests many pathophysiological
changes?cause or effect?
• is present before evident disease
• ends when pregnancy ends
• is likely the convergence of several pathways with a common
endpoint

Future DirectionsFuture Directions Identifying targets for therapyIdentifying targets for therapy
Future trials should be guided by well established pathophysiological features.
• Biologically plausible antecedent of maternal/perinatal mortality/morbidity
• Present before disease• Returns to normal after
pregnancy
• May only be pertinent to a subset of preeclamptic women

Future DirectionsFuture DirectionsEffects on perinatal outcomeEffects on perinatal outcome
Signs of preeclampsia are not an important part of physiology.
As an inherited disease, predicts survival value of the disorder.
It is possible to mask the diagnosis without affecting relevant pathophysiology.

Future DirectionsFuture DirectionsEffects on perinatal outcomeEffects on perinatal outcome
Future clinical trials:• must be large enough to detect adverse
fetal/neonatal outcome
• should have as primary outcome an endpoint relevant to neonatal well-being

Future DirectionsFuture DirectionsEffects on perinatal outcomeEffects on perinatal outcome
Future clinical trials:• must be large enough to detect adverse
fetal/neonatal outcome
• should have as primary outcome an endpoint relevant to neonatal well-being
• Admit our knowledge is limited and also collect mechanistic data (without compromising trial)