Prevention of Diabetes in African American Communities: Project PROUD Community Trevor Hart, Betty...
36
Prevention of Diabetes in Prevention of Diabetes in African American African American Communities: Communities: Project PROUD Community Project PROUD Community Trevor Hart, Betty Kennedy, Susan Trevor Hart, Betty Kennedy, Susan Peterson, Guido Urizar, Ben Van Peterson, Guido Urizar, Ben Van Voorhees, and Ken Ward Voorhees, and Ken Ward
-
Upload
myron-powell -
Category
Documents
-
view
217 -
download
2
Transcript of Prevention of Diabetes in African American Communities: Project PROUD Community Trevor Hart, Betty...
Prevention of Diabetes in African Prevention of Diabetes in African American Communities:American Communities:
Project PROUD CommunityProject PROUD Community
Trevor Hart, Betty Kennedy, Susan Trevor Hart, Betty Kennedy, Susan Peterson, Guido Urizar, Ben Van Voorhees, Peterson, Guido Urizar, Ben Van Voorhees,
and Ken Wardand Ken Ward

BackgroundBackground African Americans (AA’s) have a greater African Americans (AA’s) have a greater
incidence of diabetes compared to Whitesincidence of diabetes compared to Whites
AA’s suffer diabetes complications AA’s suffer diabetes complications disproportionately relative to Whites:disproportionately relative to Whites: CV disease (heart attacks, stroke)CV disease (heart attacks, stroke) Diabetic retinopathy (blindness)Diabetic retinopathy (blindness) Diabetic nephropathy (kidney failure)Diabetic nephropathy (kidney failure) Peripheral vascular disease (amputations)Peripheral vascular disease (amputations)
Lifestyle interventions delay diabetes onsetLifestyle interventions delay diabetes onset

Limitations of the DPP StudyLimitations of the DPP Study Suggested efficacy in AA’s based on Suggested efficacy in AA’s based on
exploratory post-hoc analysesexploratory post-hoc analyses
DPP lifestyle intervention was an intensive DPP lifestyle intervention was an intensive high-cost medical model delivered by high-cost medical model delivered by professional staffprofessional staff
Design not specifically targeted for AA’s at Design not specifically targeted for AA’s at high risk for diabeteshigh risk for diabetes
In current form, may not be feasible in In current form, may not be feasible in many AA communitiesmany AA communities

Primary Study QuestionPrimary Study Question
We hypothesize that a culturally-We hypothesize that a culturally-appropriate community implementation appropriate community implementation model (Project PROUD) will reduce the model (Project PROUD) will reduce the incidence of Type II Diabetes Mellitus incidence of Type II Diabetes Mellitus (DM) relative to standard care(DM) relative to standard care
Secondary Study QuestionSecondary Study Question
We hypothesize that Project PROUD is cost We hypothesize that Project PROUD is cost effective when savings in long term medical effective when savings in long term medical costs are included ($50,000/quality adjusted costs are included ($50,000/quality adjusted life year)life year)

RecruitmentRecruitment Community-based recruitment conductedCommunity-based recruitment conducted
Six study centers Six study centers DetroitDetroit New OrleansNew Orleans MemphisMemphis OaklandOakland HoustonHouston ChicagoChicago

Study PopulationStudy Population
Inclusion criteria:Inclusion criteria: African American adultsAfrican American adults Age Age >> 25 years 25 years Plasma glucosePlasma glucose
2 hour glucose 140-199 mg/dl (7.8 – 11.1 mmol/L) 2 hour glucose 140-199 mg/dl (7.8 – 11.1 mmol/L)
andand Fasting glucose 95-125 mg/dl (5.3 – 7.0 mmol/L)Fasting glucose 95-125 mg/dl (5.3 – 7.0 mmol/L)
Body Mass Index (BMI) Body Mass Index (BMI) >> 24 kg/m 24 kg/m22

Study PopulationStudy Population
Exclusion criteria:Exclusion criteria: Other member in household enrolledOther member in household enrolled Type I or II diabetesType I or II diabetes Taking medications that alter glucose Taking medications that alter glucose
tolerancetolerance Illness that could seriously reduce life
expectancy

Sample Size AssumptionsSample Size Assumptions
Effect sizesEffect sizes Based on our pilot data, we predict a 30% Based on our pilot data, we predict a 30%
reduction in diabetes incidence in AA’s reduction in diabetes incidence in AA’s randomized in Project PROUD relative to randomized in Project PROUD relative to standard carestandard care
Incidence of 12.1% in standard care groupIncidence of 12.1% in standard care group

Screening and Screening and RecruitmentRecruitment
Step 1 screeningStep 1 screening
Step 2 OGTTStep 2 OGTT
Step 3 start run-inStep 3 start run-in
Step 5 randomizationStep 5 randomization
Number of participantsNumber of participants
160,000160,000
30,00030,000
4,8004,800
4,0004,000
3,260*3,260*
Step 4 end run-inStep 4 end run-in

RandomizationRandomization
Stratified randomization by study centerStratified randomization by study center
Sample size 1630 in each arm of the study = 3260Sample size 1630 in each arm of the study = 3260 Project PROUD (community implementation of DPP)Project PROUD (community implementation of DPP) Control (standard care)Control (standard care)

Design and ProtocolDesign and Protocol
Project PROUD (n=1630)
Standard Care Standard Care (n=1630)(n=1630)
BaselineBaseline Year 1Year 1 Year 3Year 3 Year 5Year 5
Year 4Year 4Year 2Year 2 Year 6Year 6

Outcome MeasuresOutcome Measures Primary OutcomePrimary Outcome
Diabetes diagnosis (assessed annually)Diabetes diagnosis (assessed annually)
Secondary OutcomeSecondary Outcome Physical Activity LevelPhysical Activity Level Usual caloric intakeUsual caloric intake Body Mass Index (BMI)Body Mass Index (BMI) HbA1cHbA1c
All measures will be administered on the same All measures will be administered on the same schedules to both groupsschedules to both groups

Key Aspects of Project PROUDKey Aspects of Project PROUD
Weight loss and physical activity goalsWeight loss and physical activity goals
Lifestyle coachesLifestyle coaches
Intensive, ongoing interventionIntensive, ongoing intervention Core curriculumCore curriculum Supervised exercise sessionsSupervised exercise sessions Maintenance programMaintenance program

ComponentComponent DPPDPP PROUDPROUDIntervention Case Intervention Case ManagersManagers
University-Trained Health University-Trained Health InterventionistsInterventionists
Trained Community Health Trained Community Health Educators – African Educators – African
AmericanAmerican
INTERVENTION COMPONENTSINTERVENTION COMPONENTS

Community Members as Peer Health EducatorsCommunity Members as Peer Health Educators
Project PROUD CommunityProject PROUD Community

ComponentComponent DPPDPP PROUDPROUDIntervention Case Intervention Case ManagersManagers
University-Trained Health University-Trained Health InterventionistsInterventionists
Trained Community Health Trained Community Health Educators – African Educators – African
AmericanAmerican
SettingSetting Health ClinicHealth Clinic ChurchesChurches

ComponentComponent DPPDPP PROUDPROUDIntervention Case Intervention Case ManagersManagers
University-Trained Health University-Trained Health InterventionistsInterventionists
Trained Community Health Trained Community Health Educators – African Educators – African
AmericanAmerican
SettingSetting Health ClinicHealth Clinic ChurchesChurches
DietDiet Non-ethnic specific foodsNon-ethnic specific foods Soul food pyramid, Soul food pyramid, cooking demonstrationscooking demonstrations

Project PROUD CommunityProject PROUD Community Nutrition EducationNutrition Education
Introduction to the Lifestyle Balance ProgramIntroduction to the Lifestyle Balance Program Record Keeping of Food and Exercise DiaryRecord Keeping of Food and Exercise Diary Getting Started Losing WeightGetting Started Losing Weight
Healthy EatingHealthy Eating
Tip the Calorie BalanceTip the Calorie Balance
Four Keys to Healthy Eating OutFour Keys to Healthy Eating Out
You Can Manage StressYou Can Manage Stress
Ways to Stay MotivatedWays to Stay Motivated
Diet and Physical Activity Self MonitoringDiet and Physical Activity Self Monitoring

ComponentComponent DPPDPP PROUDPROUDIntervention Case Intervention Case ManagersManagers
University-Trained Health University-Trained Health InterventionistsInterventionists
Trained Community Health Trained Community Health Educators – African Educators – African
AmericanAmerican
SettingSetting Health ClinicHealth Clinic ChurchesChurches
DietDiet Non-ethnic specific foodsNon-ethnic specific foods Soul food pyramid, Soul food pyramid, cooking demonstrationscooking demonstrations
ExerciseExercise Brisk WalkingBrisk Walking Brisk WalkingBrisk Walking
DancingDancing
Gospel AerobicsGospel Aerobics

ComponentComponent DPPDPP PROUDPROUDIntervention Case Intervention Case ManagersManagers
University-Trained Health University-Trained Health InterventionistsInterventionists
Trained Community Health Trained Community Health Educators – African Educators – African
AmericanAmerican
SettingSetting Health ClinicHealth Clinic ChurchesChurches
DietDiet Non-ethnic specific foodsNon-ethnic specific foods Soul food pyramid, Soul food pyramid, cooking demonstrationscooking demonstrations
ExerciseExercise Brisk WalkingBrisk Walking Brisk WalkingBrisk Walking
DancingDancing
Gospel AerobicsGospel Aerobics
Adherence StrategiesAdherence Strategies Problem-solvingProblem-solving
ReinforcementsReinforcements
Healthy neighborhood Healthy neighborhood options, ethnic-specific options, ethnic-specific
recipes/cookbooksrecipes/cookbooks

ComponentComponent DPPDPP PROUDPROUDIntervention Case Intervention Case ManagersManagers
University-Trained Health University-Trained Health InterventionistsInterventionists
Trained Community Health Trained Community Health Educators – African Educators – African
AmericanAmerican
SettingSetting Health ClinicHealth Clinic ChurchesChurches
DietDiet Non-ethnic specific foodsNon-ethnic specific foods Soul food pyramid, Soul food pyramid, cooking demonstrationscooking demonstrations
ExerciseExercise Brisk WalkingBrisk Walking Brisk walkingBrisk walking
DancingDancing
Gospel AerobicsGospel Aerobics
Adherence StrategiesAdherence Strategies Problem-solvingProblem-solving
ReinforcementsReinforcements
Healthy neighborhood Healthy neighborhood options, ethnic-specific options, ethnic-specific
recipes/cookbooksrecipes/cookbooks
Ethnically targeted Ethnically targeted materialsmaterials
Materials not targeted for Materials not targeted for African-AmericansAfrican-Americans
African-American specific African-American specific materials (e.g., materials (e.g.,
testimonials, illustrations, testimonials, illustrations, stories)stories)
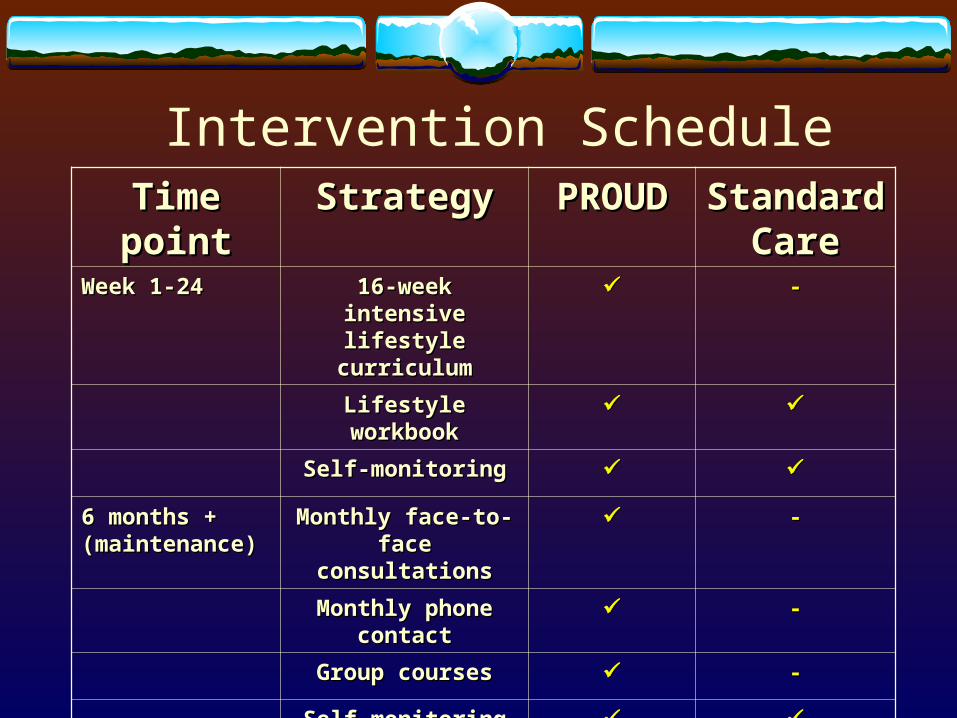
Time pointTime point StrategyStrategy PROUDPROUD Standard Standard CareCare
Week 1-24Week 1-24 16-week intensive 16-week intensive lifestyle curriculumlifestyle curriculum
--
Lifestyle workbookLifestyle workbook
Self-monitoringSelf-monitoring
6 months + 6 months + (maintenance)(maintenance)
Monthly face-to-face Monthly face-to-face consultationsconsultations
--
Monthly phone Monthly phone contactcontact
--
Group coursesGroup courses --
Self-monitoringSelf-monitoring
Annual remindersAnnual reminders
Intervention Schedule

Treatment FidelityTreatment Fidelity Treatment DeliveryTreatment Delivery
1-week initial training for lifestyle counselors1-week initial training for lifestyle counselors Weekly rounds to discuss casesWeekly rounds to discuss cases Review 3 audiotapes of sessionsReview 3 audiotapes of sessions
Treatment ReceiptTreatment Receipt Follow-up adherence checklist covering goals of Follow-up adherence checklist covering goals of
session (coach session (coach andand participant) participant)
Treatment EnactmentTreatment Enactment Weight assessment each meeting Weight assessment each meeting Assessment of activity level and caloric intakeAssessment of activity level and caloric intake

Ascertainment of Response Ascertainment of Response VariablesVariables
Training of AssessorsTraining of Assessors Major assessments (6 mo and 1 year) Major assessments (6 mo and 1 year)
conducted by independent study staff at local conducted by independent study staff at local clinicsclinics
Assessors blinded to conditionAssessors blinded to condition
Trained to assess behavior and biological Trained to assess behavior and biological variablesvariables

Adverse EventsAdverse Events Based on the DPP we will monitor for Based on the DPP we will monitor for
adverse events in both study armsadverse events in both study arms
Musculoskeletal symptomsMusculoskeletal symptoms
HospitalizationsHospitalizationsLength of stay and diagnosisLength of stay and diagnosis
DeathsDeathsCause of deathCause of death

Data AnalysisData Analysis Interim MonitoringInterim Monitoring
After 2 years of the study and every year following After 2 years of the study and every year following until end of studyuntil end of study
Primary AnalysisPrimary Analysis Comparison of Diabetes Incidence between Project Comparison of Diabetes Incidence between Project
PROUD and Standard Care conditionsPROUD and Standard Care conditions Time to outcome assessed using life-table methodsTime to outcome assessed using life-table methods
Secondary AnalysisSecondary Analysis Pair-wise comparisons of secondary outcomesPair-wise comparisons of secondary outcomes

Secondary Outcome: Secondary Outcome: Cost EffectivenessCost Effectiveness
PurposePurpose: to determine if Project PROUD is cost : to determine if Project PROUD is cost effective when savings in long term medical effective when savings in long term medical costs are included ($50,000/quality adjusted life costs are included ($50,000/quality adjusted life year)year)
Decision analysis model projecting results of Decision analysis model projecting results of Project PROUD into the general populationProject PROUD into the general population
We will examine the cost effectiveness of this We will examine the cost effectiveness of this project under different assumptionsproject under different assumptions

Model AssumptionsModel Assumptions Efficacy: Study results relative to standard careEfficacy: Study results relative to standard care
Costs (Project PROUD & standard care): all costs Costs (Project PROUD & standard care): all costs not related to research implementationnot related to research implementation
Costs (Medical): medical costs of diabetes and or Costs (Medical): medical costs of diabetes and or complications treatmentcomplications treatment
Costs (Non-Medical): We will include estimates Costs (Non-Medical): We will include estimates of productivity gained for those not diagnosed of productivity gained for those not diagnosed with DMwith DM

Cost Effectiveness AnalysisCost Effectiveness Analysis Outcome: costs/quality adjusted life year gained Outcome: costs/quality adjusted life year gained
by intervention compared to standard careby intervention compared to standard care
First analysis: based on efficacy and costs in First analysis: based on efficacy and costs in interventionintervention
Second analysis: sensitivity analysis based on Second analysis: sensitivity analysis based on reasonable range of values for efficacy and costs reasonable range of values for efficacy and costs anticipated in actual implementation conditions.anticipated in actual implementation conditions.

Methodologic IssuesMethodologic Issues Unit of randomizationUnit of randomization
Procedures designed to limit cross-arm Procedures designed to limit cross-arm contaminationcontamination
Selection of diabetes incidence as primary Selection of diabetes incidence as primary endpointendpoint
Use of African American churches as Use of African American churches as intervention sitesintervention sites

Other designs considered: 2-armOther designs considered: 2-arm
Eligible participantsEligible participants
RandomizedRandomized
DPP DPP Project PROUDProject PROUD
Pros – Replicate DPP in African AmericansPros – Replicate DPP in African AmericansCons– Small expected effect – sample size approaches infinityCons– Small expected effect – sample size approaches infinity

Other designs considered: 3-armOther designs considered: 3-arm
Eligible participantsEligible participants
RandomizedRandomized
Standard careStandard care DPPDPP Project PROUDProject PROUD
Pros – Replicate DPP in African AmericansPros – Replicate DPP in African AmericansCons– Resource intensiveCons– Resource intensive

Proposed Design: 2-armProposed Design: 2-arm
Eligible participantsEligible participants
RandomizedRandomized
Standard Care Standard Care Project PROUD Project PROUD
ACKNOWLEDGEMENTSACKNOWLEDGEMENTS
Group 1 would like to thank the following Group 1 would like to thank the following faculty for assisting us in designing faculty for assisting us in designing project PROUD Community:project PROUD Community:
Dr. Ron AbelesDr. Ron Abeles Dr. Jim BlumenthalDr. Jim Blumenthal Dr. Lynda PowellDr. Lynda Powell Dr. Michael ProschanDr. Michael Proschan