PREVENTING CERVICAL CANCER BRYANSTON COUNTRY CLUB 4 th September 2010 Dr Peter C Koll.
64
PREVENTING CERVICAL CANCER BRYANSTON COUNTRY CLUB 4 th September 2010 Dr Peter C Koll
-
Upload
ashtyn-sam -
Category
Documents
-
view
214 -
download
0
Transcript of PREVENTING CERVICAL CANCER BRYANSTON COUNTRY CLUB 4 th September 2010 Dr Peter C Koll.

PREVENTING CERVICAL CANCER
BRYANSTON COUNTRY CLUB
4th September 2010
Dr Peter C Koll

CERVICAL CANCER
•To create the awareness
•To find the resources
•To stimulate the political will
All we need to do is :
Medical breakthroughs have occured
Cervical cancer should not happen

1. Ferlay J, et al. GLOBOCAN 2002 Cancer Incidence, Mortality and Prevalence Worldwide. IARC CancerBase; Lyon, 2004.
Global mortality per annum
Cervical cancer mortality rates worldwide Cases per 100,000 women per year
North America14,500 new cases
6,000 deaths
Latin America72,000 new cases
33,000 deaths
Africa79,000 new cases
62,000 deaths
Asia266,000 new cases
143,000 deaths
Europe60,000 new cases
30,000 deaths
• Worldwide, every 2 minutes a woman dies of cervical cancer1
• The highest burden of disease (up to 80%) occurs in less developed regions1 where there is a lack of effective screening programmes
• This demonstrates a clear medical need for new cervical cancer interventions
< 7.9
< 23.8
< 14.0
< 55.6 < 3.9

Ferlay J, et al. GLOBOCAN 2002 Cancer Incidence, Mortality and Prevalence Worldwide. IARC CancerBase; Lyon; 2004.
The most frequent cancers in women: incidence and mortality
Global data
Incidence Mortality
Age-standardized rate per 100,000
Breast
Cervix
Colon/Rectum
Lung
Stomach
Ovary
Corpus
0 5 10 15 20 25 30 35 40
37.4
16.2
14.6
12.1
10.3
6.6
6.5
Breast
Lung
Cervix
Stomach
Colon/Rectum
Liver
Ovary
0 2 4 6 8 10 12 14
13.2
10.3
9.0
7.9
7.6
5.7
4.0
Age-standardized rate per 100,000

The most frequent cancers in women: incidence and mortality
AfricaIncidence Mortality
Cervix
Breast
Liver
Stomach
Kaposi’ssarcoma
Ovary
Colon/Rectum
0 5 10 15 20 25 30 35
29.3
23.4
6.2
4.9
4.6
4.3
4.2
Cervix
Breast
Liver
Stomach
Kaposi’ssarcoma
Colon/Rectum
Oesophagus
0 5 10 15 20 25
23.1
16.2
6.2
4.6
4.3
3.7
3.2
Ferlay J, et al. GLOBOCAN 2002 Cancer Incidence, Mortality and Prevalence Worldwide. IARC CancerBase; Lyon; 2004.
Age-standardized rate per 100,000 Age-standardized rate per 100,000

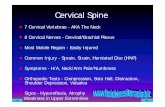
The transformation zone
The transformation zone (squamous metaplasia)
Squamous epithelium
Columnar epithelium
ANATOMY

Pre-Cancerous lesions

Cervical cancer

HISTORY OF Ca Cx PREVENTION
- 1928 George Papanicolaou first described the PAP test --- 81 years ago


Limitations of PAP smear
- Only prevents 70% of cancers
- May miss adenocarcinoma
Endometrium
Uterine cavity
Cervix
Myometrium
Adenocarcinoma
Squamous cell carcinoma
Adenocarcinoma: may beinaccessible to the cervical
smear brush
Squamous cell carcinoma:usually accessible to the cervical
smear brush
AdenocarcinomaSquamous cell carcinoma

Limitations of PAP smear
- May miss adenocarcinoma
- Only prevents 70% of cancers
-Logistics
-Cost
-Treatment
-Recall

HISTORY OF Ca Cx PREVENTION
- 1928 George Papanicolaou first described the PAP test --- 81 years ago
- 1983 Harald zur Hausen linked HPV to Ca Cx
- IARC identified HPV DNA in 99.8% of cervical cancer specimens from 25 countries
- Late 1990’s Carcinogenic subtypes of HPV identified
- HPV VACCINES
HPV vaccines, the first vaccines specifically developed
to prevent a cancer

HPV>100 types identified2
~30–40 anogenital2,3
~15–20 oncogenic*,2,3
HPV 16 and HPV 18 types account for the majority of worldwide cervical cancers.4
Nononcogenic** types HPV 6 and 11 are most often
associated with external anogenital warts.3
These two types are responsible for >90% of genital warts.5
Nonenveloped double-stranded DNA virus1
*High risk; ** Low risk
1. Howley PM, Lowy DR. In: Knipe DM, Howley PM, eds. Philadelphia, Pa: Lippincott-Raven; 2001:2197–2229. 2. Schiffman M, Castle PE. Arch Pathol Lab Med. 2003;127:930–934. 3. Wiley DJ, Douglas J, Beutner K, et al. Clin Infect Dis. 2002;35(suppl 2):S210–S224. 4. Muñoz N, Bosch FX, Castellsagué X, et al. Int J Cancer. 2004;111:278–285. 5. Jansen KU, Shaw AR. Annu Rev Med. 2004;55:319–331. 2

HPV Infection and Life Cycle
Normal Epithelium
Cervical Surface
Basement Membrane
Basal (Stem) Cells
Parabasal Cells
Squamous Layer
Mature Squamous
Layer
. .
. .
.
.
.
Infected Epithelium
Adapted from Frazer IH. Nature Rev Immunol. 2004;4:46–54.
Shedding of Virus-Laden Epithelial Cells
Infection of Basal Cells (E1 and E2)
Episomal Viral DNA in Cell Nucleus
(E1 and E2, E6 and E7)
Viral DNA Replication(E6 and E7)
Viral Assembly(L1 and L2)

Why are antibody responses so poor innatural HPV infections?
No viraemia
HPV does not kill keratinocytes
no inflammation
no pro-inflammatory cytokines
poor activation of epithelial antigen presenting cells
Free virus particles are shed from mucosal surfaces with poor exposure to antigen presenting cell (APC)

What are the consequences of this?
Natural infection dose not necessarily confer protection against future disease.
Women remain at risk of persistent HPV infection, throughout their lives .
Persistent HPV infection is the cause of Cervical Cancer

Vaccine HPV type
HPV Types in Cervical Cancer Worldwide
Cancer cases attributed to the most frequent HPV genotypes (%)
HPV genotype
2.32.21.41.31.21.00.70.60.50.3
4.4
53.5
2.6
17.26.7
2.9
0 10 20 30 40 50 60 70 80 90 100
X
Other
82
73
68
39
51
56
59
35
58
52
33
31
45
18
16 53.5 %70.7 %77.4 %80.3 %
Munoz N et al. Int J Cancer 2004;111:278–85.

Central/South America
Northern Africa
North America/Europe
South Asia
16
18
45
31
33
HPV Type
52
Others
*A pooled analysis and multicenter case control study (N = 3607).
1. Muñoz N, Bosch FX, Castellsagué X, et al. Int J Cancer. 2004;111:278–285.
Worldwide Prevalence of HPV Types in Cervical Cancer*,1
58
57
12.6
69.7
14.6
67.6
1752.5
25.7

2.0HPV 591.1HPV 35 3.1HPV 351.9HPV 35
2.2HPV 562.7HPV 56
2.2HPV 56 3.0HPV 583.2HPV 58
1.1HPV 52 3.6HPV 52
3.1HPV 52
2.2HPV 33
4.2HPV 33
4.0HPV 333.2HPV 33
2.3HPV 31
3.4HPV 31
4.5HPV 31
7.4HPV 31
6.8HPV 45
9.0HPV 45 7.9HPV 455.6HPV 4515.0HPV 45
14.6HPV 18 25.7HPV 1812.6HPV 1817.0HPV 1819.1HPV 18
% HPV type% HPV type% %HPV typeHPV type
%
69.7 52.557.067.647.7HPV 16 HPV 16HPV 16HPV 16HPV 16
HPV type
Europe & North America South AsiaCentral-South
AmericaNorthern AfricaSub-Saharan Africa
Adapted from Munoz N et al Int J Cancer 2004;111: 278-85
In 2855 HPV Positive Cervical Cancer Cases & Rank By Region
Prevalence of the 10 most common oncogenic HPV types worldwide

Global burden of HPV- Carcinoma of the cervix
-2002 - 493000 diagnosed -274000 died
- Other HPV Carcinomas-Anal
-Vulvo/vaginal
-Penile
-Oral
-Nasopharangeal
-Abnormal PAP smear -Repeat visits
-Colpomicroscopy
-Biopsy
-Laser/Cone/LEEP/LLETZ
-Financial
-Emotional
-Physical
Morbidity

The most common STD•50% young females aquire it within 3 yrs of sexual debut
• Cumulative detection is 59-82%
• Majority transient in young women – only 10-20% persist for 24 mts
• Peak at 20 sharp decline by 30
• If present after 30 – more likely to be persistent
• ONLY PERSISTENT HIGH RISK HPV CONSTITUTES RISK FOR CIN2 OR 3

Estimated World Burden of HPV-Related Diagnoses Focus on Cervical Disease and Genital Warts
Cervical Cancer: 0.5 million cases/year1
High-grade precancerous lesions: 10 million2
Low-grade cervical lesions: 30 million2
Genital warts: 30 million3
Att
ribu
tabl
e to
onc
ogen
ic H
PV ty
pes
HPV infection: 660 million1
1. World Health Organization, Geneva, Switzerland: World Health Organization; 2005:1–38. 2. World Health Organization. Geneva, Switzerland: World Health Organization; 1999:1–22. 3. World Health Organization. WHO Office of Information. WHO Features. 1990;152:1–6.
Att
ribu
tabl
e to
non
onco
geni
c H
PV ty
pes
Att
ribu
tabl
e to
non
onco
geni
c H
PV ty
pes
2

HPV Infection and Risk of Invasive Cervical Cancer in Selected Countries*,1
*Assays used varied by site.**CI = confidence interval1. Muñoz N, Bosch FX, de Sanjosé S, et al. N Engl J Med. 2003;348:518–527.
0.1 10 100 1000 10,000
Brazil
Mali
Morocco
Paraguay
Philippines
Thailand
Peru
Spain
Colombia
Overall
Odds Ratio (95% CI**)
% HPVPrevalencecases/contro
97.0/17.3
96.9/33.3
97.1/21.6
98.1/19.8
96.4/9.2
96.5/15.7
95.3/17.7
82.4/5.9
78.4/17.5
96.6/15.6
7

Human papillomavirus structureHPV is a relatively small virus containing
double-stranded DNA within a spherical shell (capsid)1
The capsid is composed of two proteins, the ‘late’ or structural proteins L1 and L21
L1 protein pentamer L2 supporting protein
Circular DNA
55 nm
1. Burd EM. Clin Microbiol Rev 2003; 16:1–17.


Virus Like Particle (VLP)
L1 protein pentamer
VLP Looks exactly like the virus but contains no viral DNA
Thus elicits strong immune response without any risk of infection

Active protection via vaccination is mediated by neutralizing antibodies at the cervix
HPV
Cervical canal
Neutralizing antibodies
Blood vessel
Epithelial tear
Basement membrane
Cervicalepithelium
1. Stanley M. Vaccine 2006; 24:S16–S22; 2. Giannini S, et al. Vaccine 2006; 24:5937–5949;
3. Nardelli-Haefliger D, et al. J Natl Cancer Inst 2003; 95:1128–1137; 4. Poncelet S, et al. IPC 2007(poster).

GARDASIL™ (20/40/40/20 μg) Neutralizing Anti-HPV Immunogenicity
In a double-blind, placebo-controlled, dose-ranging study ofquadrivalent HPV (types 6, 11, 16, 18) L1 VLP vaccine.
1
10
100
1000HPV 6
** * 1
10
100
1000HPV 11
***
7 12 18 24 30 36 54 60
Time Since Vaccination (Months)
10
100
1000
10,000
GM
T w
ith
95
% C
Im
MU
/mL
(L
og
Sc
ale
)
*** 7 12 18 24 30 36 54 60
1
10
100
1000HPV 18
***
HPV 16
Per-Protocol Subjects (GARDASIL)
* vaccinationGARDASIL is a trademark of Merck & Co., Inc., Whitehouse Station, NJ, USA.Adapted from Olsson S-E et al. Vaccine. 2007;25:4931–4939.
7 12 18 24 30 36 54 60 7 12 18 24 30 36 54 60
10

CERVARIX

GARDASIL™ [Quadrivalent Human Papillomavirus (Types 6, 11, 16, 18) Recombinant Vaccine]
GARDASIL: FUTURE I-II End-of-Study ResultsEfficacy Against HPV 6/11/16/18-Related External Genital Lesions1,2
EGL = external genital lesion; VaIN = vaginal intraepithelial neoplasia; VIN = vulvar intraepithelial neoplasia. 1. Haupt RM. ACIP. February 27, 2008. http://www.cdc.gov/vaccines/recs/ACIP/downloads/mtg-slides-feb08/14-3-hpv.pdf. Accessed July 11, 2008. 2. Data on file, MSD ______.
22 0 0
227
193
28 23
0
50
100
150
200
250
HPV 6/11/16/18-Related EGL
GenitalWarts
VIN 1,VaIN 1
VIN 2/3,VaIN 2/3
99%Efficacy (97, 100)
99%Efficacy(96, 100) 100%
Efficacy (86,100)
100%Efficacy (83,100)R
elat
ed C
ases
GARDASIL Placebo
n=7900 n=7902 n=7900 n=7902 n=7900 n=7902n=7900 n=7902
Per-protocol efficacy population, women 16–26 years of age followed up through 3–4 years

HPV 6, 11, 16, or 18-related
GARDASIL Placebo
N Cases N Cases Efficacy 95% CI
PersistentInfection
235 2* 233 45 96% (83, 100)
Disease 235 0 233 6 100% (12, 100)
CIN 1, 2, or 3 235 0 233 3 100% (<0, 100)
Vulvar/vaginal neoplasias or genital warts
235 0 233 3 100% (<0, 100)
GARDASIL™: Durable Protection Through Five Years
A total of 241 subjects were entered into the five-year extension phase of protocol 007.*One case of confirmed persistent infection: HPV 18 DNA detected at months 12 and 18 only (not a case in the five-year extension).*One case of HPV 16 DNA detected at the last visit (month 36); not a subject in the five-year extension phase.GARDASIL is a trademark of Merck & Co., Inc., Whitehouse Station, NJ, USA.
Villa LL, Costa R, Petta R, et al. Br J Cancer. 2006;95:1459–1466.
PPE population; subjects were naïve to HPV types 6, 11, 16, and/or 18
15

nn
87.9 - 1001002906 Month Persistence
72.3 - 10010014012 Month Persistence
32.7 - 100 10070CIN2+
110 61.5 - 100 100CIN1+
95% CI%
Vaccine EfficacyControlHPV VaccineEndpoints*
*Combined analysis initial efficacy study and extended follow-up
ATP analysis for virologic endpoints; ITT analysis for cytologic and CIN endpoints
Presentation Gall S, AACR, Los Angeles, April 14-18, 2007
Up to 5.5 years Substantial Protection against HPV-16/18 infections and CIN outcomes

Disease Cross-Protection Analysis: Efficacy Against CIN 2/3 or AIS in the Generally HPV-Naïve Population
CIN 2/3 or AIS*# of cases GARDASIL
n=4616
# of cases
Placebon=4675
Efficacy 95% CI
HPV 31/45 8 21 62% 10, 85
HPV 31/33/45/52/58
27 48 43% 7, 66
HPV 31/33/35/39/45/51/5
2/56/58/5938 62 38% 6, 60
* Composite endpoints were analyzed (primary endpoints). In analyses for the individual components of the endpoints, efficacy was variable, and there was no evidence of efficacy with respect to HPV 35 and 45-related disease.
Brown D; for the FUTURE Study Group. Poster presented at ICAAC; September 17-20, 2007; Chicago, IL.

Cross Protection Cervarix® showed significant type-specific efficacy
against pre-cancers (CIN 2+) associated with HPV types beyond 16 and 18
Vaccine efficacy was:100% for HPV 31/45 against CIN2+ 68.2% for the 5 most frequent oncogenic types
(31,33,45,52,58)
68.4% for the 10 most frequent oncogenic types (31,33,35,39,45,51,52,56,58,59)
Cervarix® showed vaccine efficacy of 77.7% for 14 oncogenic types, including HPV 16 and 18 measured as a composite endpoint

No clinically meaningful differences between study groups with respect to:
Medically significant conditions • Serious Adverse Events • New onset chronic disease and new onset autoimmune
diseases• Pregnancy outcomes
SAFETY

WHICH ONE ?
• Both safe• Both very effective• Both equally effective in preventing Ca Cx
• Only two undisputed facts: 1) Gardasil protects against 6 and 11 2) Cervarix is cheaper

The Gardasil argument
1) Proven protection against vulval and vaginal carcinoma
2) Protection against 6 and 11

GARDASILHPV 6 & 11
HPV Types 6 and 11 responsible for >90% of anogenital warts1
Estimated lifetime risk of developing genital warts ~10%2,3
External genital warts are very contagious.Infectivity >75%

RRP
Age distribution is bimodal with peaks at1: 2 to 4 years of age (childhood-onset) 20 to 40 years of age (adult-onset)
HPV Types 6 and 11 cause ~100% of both juvenile- and adult-onset RRP.2
Papillomas are stratified squamous epithelial masses that can obstruct the airway if not removed.3
Although histologically benign, RRP causes significant morbidity and mortality due to recurrent nature.3
Could require surgery under general anesthesia as frequently as every few weeks
Possible causative role of RRP in head and neck cancers3-5
RRP is rare.6
GARDASIL™ is not indicated for RRP.1. Derkay CS. Laryngoscope. 2001;111:57–69. 2. Lacey CJN, Lowndes CM, Shah KV. Vaccine. 2006;24S3:S3/35–S3/41. 3. Abramson AL, Nouri M, Mullooly V, Fisch G, Steinberg BM. J Med Virol. 2004;72:473–477. 4. Steinberg BM, DiLorenzo TP. Cancer Metastasis Rev. 1996;15:91–112. 5. Szentirmay Z, Pólus K, Tamás L, et al. Cancer and Metastasis Reviews. 2005;24:19–34. 6. Derkay CS, Darrow DH. Ann Otol Rhinol Laryngol. 2006;115:1–11.

The Cervarix argument
1. Higher antibody levels
2. Higher number of memory b cells
3. Higher antibody levels in cervical mucous
4. Better cross protection data

Cervarix®
Gardasi™
p<0.0001
HPV-16 and 18 Neutralising antibody responses:
Geometric Mean Titers
TVC* = at least 1 dose received
GM
T (
ED
50
)
31715 8682 188613732
1:GSKBio_WWMA_DoF018_3_2009
3.7 -fold
7.3 -fold
HPV 16** HPV 18**

Memory B cells
The frequency of antigen-specific memory B-cells in responders was significantly higher (2.7-fold) in the Cervarix® group than in the Gardasil™ group for both HPV 16 and HPV 18 (women aged 18–45 years, p<0.0001).

Mucosal HPV antibody response in cervicovaginal secretion (CVS)
Positivity rates for anti-HPV-16/18 neutralizing antibodies in CVS frequencies were higher for Cervarix®.
81.3% vs 50.9% for HPV 1633.3% vs 8.8% for HPV 18

Thus, we have two teams of international immunoligical heavyweights sending us different messages !
RESULT


REMEMBER
• Both safe• Both very effective• Both equally effective in preventing Ca Cx
• Only two undisputed facts: 1) Gardasil protects against 6 and 11 2) Cervarix is cheaper

So, which one ?Short answer: -it doesn’t matterIf can’t make up mind: -toss a coin -Either way, you won’t be wrongFor goodness sake VACCINATE

WHO AND WHEN

Cumulative Risk of Any HPV Infection by Age in Women*,1
Cum
ulat
ive
Ris
k of
HP
V I
nfec
tion
(%
)Age at Baseline
N=1610
Years
0
10
20
30
40
50
0 1 2 3 4 5
15–1920–24
25–2930–4445+
*In a cohort of Colombian women1. Adapted from Muñoz N, Méndez F, Posso H, et al. J Infect Dis. 2004;190:2077–2087. Reprinted with permission from The University of Chicago Press. Copyright © 2004 by the Infectious Diseases Society of America. All rights reserved.
8

WHO AND WHEN•Before sexual debut ?9-13 “screen yourselves-vaccinate your daughters”
BUT•20 years to see any impact
•30-40 years to see benefit on Ca Cx
THEREFORE•May consider “catch up” vaccination for all sexually active women
•We know its effective and safe in older women (10-55)•We know very few carry both 16 and 18
•We know most HPV infections are transient
SUGGESTS SIGNIFICANT BENEFIT FOR ALL SEXUALLY ACTIVE WOMEN

WHO AND WHEN
•In other words, vaccinating all sexually active women will probably :
•Reduce Ca Cx
•Reduce repeat visits and smears
•Reduce colposcopies
•Reduce destructive cervical procedures and the obstetric complications associated with them
•Reduce hysterectomies for pre-invasive cervical lesions
And consequently reduce the -
•Psychological
•Physical
•Financial
- Morbidity and mortality associated with them

WHO AND WHEN
• NOT only pre sexual debut
• NOT only up to 26 • NOT only the promiscuous
• Current PAP status irrelevant
• Current HPV status irrelevant

WHO AND WHEN•? Males - Controvercial
•? Pre vaccination HPV test - Not necessary
•? Boosters - Not needed to 7.3 years trials ongoing but look promising for long term
•? Prev abn PAP
•? Pregnancy
•? Lactation
•? Current abn PAP
- Vaccinate
- Vaccinate
- Postpone
- Benefit vs Risk

PSYCOLOGICAL ASPECTS
Parents don’t mind
Vaccination does not change sexual behavior (ie promiscuity)
Vaccination does not change sexual practice (ie safe sex)

Screening to prevent Ca Cx
• PAP remains the mainstay of screening
• Importance of PAP even after vaccination
• What is the place of HPV testing?

SCREENING
Potential use of HPV testing:
1) Primary screening
2) Triange of abn PAP
3) Test of cure

SCREENING
How good are PAPs ?
(Pooled European and Canadian studies)
Sensitivity 53%
Specificity 96%How good is HPV testing ?
Sensitivity almost 100%
Specificity very lowLogic for primary HPV screen

HPV is common (80%)Only 10 to 20% persistOnly some of the persistent HPV lead to High-Gr SilPeak at 20 sharp decline by 30Only persistent HPV is a problem but current tests
only show presence
HPV TESTING - Problems

TRIANGE OF ABN PAP
ASCUS 43% HPV PositiveLSil 76% HPV PositiveTherefore only worthwhile in ASCUSLow-Gr Sil needs ColposcopyIn ASCUS HC2 identifies 37% more CIN2 than repeat
cytology

TEST OF CURE
Sweedish study looked at longterm incidence/mortality following treatment for CIN3
Showed lifelong increased risk of invasive Ca that accelerated with age.
We thus need better Risk stratification of these patients

TEST OF CURE
6 months post treatment HPV test showed 99% sensitivity
Cytology + HPV 100%Good test of cureLonger follow up needed

LIQUID BASED CYTOLOGY
No convincing evidence of better detection of High-Gr SilTwo advantages:
1) Reflex HPV test if ASCUS found
2) Better in automated screeningWhat will it’s place be in future?

Take home message
• Vaccinate all women 10 to 50
• Vaccinate boys on request
• Continue screening after vaccination