Preventing Catheter-Associated Urinary Tract Infections June 12, 2013 Bonnie Norrick, MT(ASCP) cm,...
25
Preventing Catheter- Associated Urinary Tract Infections June 12, 2013 Bonnie Norrick, MT(ASCP) cm , EdM, CIC
-
Upload
gilbert-mathews -
Category
Documents
-
view
217 -
download
3
Transcript of Preventing Catheter-Associated Urinary Tract Infections June 12, 2013 Bonnie Norrick, MT(ASCP) cm,...

Preventing Catheter-Associated Urinary Tract Infections June 12, 2013
Bonnie Norrick, MT(ASCP)cm, EdM, CIC

Objectives
• List risks for acquiring a catheter associated urinary tract infection (CAUTI)
• Identify interventions for prevention of CAUTI
• List at least 3 elements in a nurse driven protocol for removing a urinary catheter

Licensed 276 acute care beds Patient days 27,257 for FY 2012; Avg census 77 Observation days 1041 Average length of stay 3.4 days LTC, Hospice, Heart Clinic, Women’s Center,
Occupational Medicine, Sleep Center, Cancer Clinic

Impact of Healthcare Associated Infections (HAI)• According to the Centers for Disease Control
and Infection (CDC), each year– Approximately 1.7 million people develop HAIs– 100,000 people die due to complications of
infections– Between 5 and 10 % of individuals who are
admitted to an acute care hospital will develop at least one HAI
– Costing $4.5-$5.7 billion– 15% of those are CAUTI

Definition of CAUTI
• Catheter-associated UTI (CAUTI): A UTI where an indwelling urinary catheter was in place for >2 calendar days when all elements of the UTI infection criterion were first present together, with day of device placement being Day 1, and
• an indwelling urinary catheter was in place on the date of event,

Definition of CAUTI 2
• at least 1 of the following signs or symptoms: fever (>38°C); suprapubic tenderness*; costovertebral angle pain or tenderness*
• and • a positive urine culture of ≥105 colony-forming units
(CFU)/ml with no more than 2 species of microorganisms. Elements of the criterion must occur within a timeframe that does not exceed a gap of 1 calendar day – *With no other recognized cause

Definition of CAUTI 3
• Patient had an indwelling urinary catheter in place for >2 calendar days and had it removed the day of or the day before all elements of this criterion were first present together
• and at least 1 of the following signs or symptoms: fever (>38°C); urgency*; frequency*; dysuria*; suprapubic tenderness*; costovertebral angle pain or tenderness*
• and a positive urine culture of ≥105 colony-forming units (CFU)/ml with no more than 2 species of microorganisms. Elements of the criterion must occur within a timeframe that does not exceed a gap of 1 calendar day– *With no other recognized cause –

Risks for CAUTI• Duration: Prolonged catheterization > 6 days• Sex: Female gender• Location of insertion: Catheter insertion outside the
operating room– Urology Service
• Overall health– Other active sites of infection – Diabetes– Malnutrition– Elevated creatinine >2.0mg/dl
• Invasive interventions: Ureteral stent• Maintenance of Foley

Our Story: In the Beginning
• Surveillance for CAUTI–Facility wide-medical,
OB and ICU–Use Definitions–Calculate rates? ICU
only, share data

Minimizing the Risks
• Use of silver coated Foley catheter’s in all areas
• Securement device• Placement of tubing and bag in respect of
bladder and floor• Maintain a closed system• Bags emptied appropriately – not overfilled

To Change Requires MeasurementNovember 2008 survey
13 Foley’s reviewed• Tubing kinked 5• Bag on floor 4• Seal Broken 0• Bags overfilled 0• Tubing not secure 11
April 2009 Survey-post education of nurses
22 Foley’s reviewed• Tubing kinked 0• Bag on floor 5• Seal Broken 0• Bags overfilled 0• Tubing not secure 0

Interventions Jan-March 2009• Silver coated catheters• Securement devices (one that stuck)• Visualization of proper positioning of tubing
and collection bag• Method to obtain devices days
Unit WGH Rate NHSN Mean
6 South 7.2 5.7
PCU 5.4 4.7
5th floor 9.5 5.0
4th floor 3.4 5.7
ICU 1.9 3.1

Education
• Aggressive education of staff– Computer based learning
–On hire and annually– Skills day
– Insertion of Foley and peri-care, urine collection
• One on one education– Observation of securement, tubing and bag
position – Inquire-medical necessity?

Documentation in EMR

Slide 15

Other interventions
• An additional SCIP quality measure began in October 2009 requiring Foley catheter be discontinued on Post Operative Day 1 or Post Operative Day 2. If the Foley remains a reason for continuing urinary catheter must be documented by MD/APN/PA.
• Applied to all surgeries.• Increase use of condom catheters for men.

Rates = infections/device days x 1000
Unit 2010 2011 NHSN Mean
6 South 2.7 0.0 5.7
PCU 0.0 7.2 4.7
5th 1.2 0.0 5.0
4th 0.0 1.5 5.7
ICU 2.0 0.8 3.1
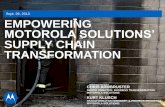
Acute Care Catheter Associated UTI FY 2009-2010 Q3
0.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0
2009 Q1 2009 Q2 2009 Q3 2009 Q4 2010 Q1 2010Q2 2010Q3
infe
ctio
ns
per
100
0 d
evic
e d
ays

Nurse driven protocol-Foley Removal Criteria
• Patient is awake, alert, no problems voiding before the catheter was placed
• Catheter was not placed for urinary retention/obstruction and no recent urological surgery within 3 months
• Patient is able to resume their voiding position• Patient able to cooperate with strict I&O monitoring• No evidence of gross hematuria

Nurse driven protocol-Foley Removal Criteria 2
• Epidural catheter is removed• Patient is not intubated• Patient not admitted with chronic indwelling Foley
catheter• Post-op patient surgery greater than or equal to 48
hours.• Open wounds/excoriation absent or resolved.• Catheter is not a suprapubic catheter
Using the above guidelines, the indwelling (Foley ) catheter will be removed by the RN 48 hours after insertion of the foley unless a specific physician’s order indicates otherwise. Nurse will review reason why foley was initially inserted.

Bladder scan usage
If one of the following is present RN will perform bladder scan. 1. Bladder discomfort
2. Distended bladder
3. Has not voided in 6 hours or at discretion of nurse
4. Post void residual (Not emptying bladder, voiding frequent small volumes)
If urine volume is greater than 250 ml the nurse will call the physician for further instruction such as a straight catherization order. Volumes less that 250 document in nurses notes.

Rates 2012
2013 Risk assessment• Decrease catheter associated UTI
by 50% (1 catheter associated urinary tract infections)
• Devise days will be collected each month for ICU and ICU SD patients.
• Other units devise days will be collected on a rotating schedule.
Unit 2012 NHSN Mean
6 South 0.0 1.6
PCU 0.0 0.5
5th 0.0 1.5
4th 0.7 1.6
ICU 0.0 1.3
ICU SD 1.7 1.8

On Going Initiatives
• Continue rounding on all nursing units• Re-educate Foley removal policy during
rounding• Observe hand off communication between
shifts discussing devices• Identify root cause of each CAUTI

In Summary
• Risk assessment a must, prioritize strategy• Measure• Involve leadership• Celebrate• It’s a Team Effort!

References
• Guideline for Prevention of Catheter-Associated Urinary Tract Infection 2009, Healthcare Infection Control Practices Advisory Committee, Center for Disease Control
• Clarke, K.,Tong, D., Norrick, B., Reduction In catheter-associated urinary tract infection by bundling interventions, International Journal for Quality in Health Care Advance Access, 2012.

Thank you
Any questions? I have the time.
Questions later, email or call.•Bonnie Norrick
–Email [email protected]–Phone 706-845-3180
West Georgia Health- So Healthy Together