Prevent Readmission Heartfailure

of 10
-
Upload
parker-brady -
Category
Documents
-
view
214 -
download
0
Transcript of Prevent Readmission Heartfailure
-
7/31/2019 Prevent Readmission Heartfailure
1/10
OLDER PEOPLE
A randomized controlled trial of a community nurse-supported hospital
discharge programme in older patients with chronic heart failure
Timothy Kwok MD, FRCPDepartment of Medicine & Therapeutics, Prince of Wales Hospital, The Chinese University of Hong Kong, Hong Kong, China
Jenny Lee MSc, MRCPDepartment of Medicine & Therapeutics, Prince of Wales Hospital, The Chinese University of Hong Kong, Hong Kong, China
Jean Woo MD, MA, FRCPDepartment of Medicine & Therapeutics, Prince of Wales Hospital, The Chinese University of Hong Kong, Hong Kong, China
Diana TF Lee RN, PhD
The Nethersole School of Nursing, The Chinese University of Hong Kong, Hong Kong, China
Sian Griffith MA, FRCPSchool of Public Health, The Chinese University of Hong Kong, Hong Kong, China
Submitted for publication: 20 June 2006
Accepted for publication: 22 December 2006
Correspondence:
Professor Timothy Kwok
Department of Medicine & Therapeutics
Prince of Wales Hospital
Hong Kong
China
Telephone: (852)-26076900
E-mail: [email protected]
K W O K T , L E E J , W O O J , L E E T F D & G R I F F I T H S ( 2 0 0 8 )K W OK T , L E E J , W O O J , L E E T F D & G R IF F IT H S ( 2 00 8 ) Journal of Clinical
Nursing 17, 109117
A randomized controlled trial of a community nurse-supported hospital dischargeprogramme in older patients with chronic heart failure
Aims and objectives. To evaluate the effectiveness and cost-effectiveness of a
community nurse-supported hospital discharge programme in preventing hospital
re-admissions, improving functional status and handicap of older patients with
chronic heart failure.
Design. Randomized controlled trial; 105 hospitalized patients aged 60 years or
over with chronic heart failure and history of hospital admission(s) in previous year
were randomly assigned into intervention group (n 49) and control group
(n 56) for six months. Intervention group subjects received community nurse
visits before discharge, within seven days of discharge, weekly for four weeks, then
monthly. Community nurse liaised closely with a designated specialist in hospital
and were accessible to subjects during normal working hours. Control and inter-vention group subjects were followed up in the same specialist medical clinics.
Primary outcome was the rate of unplanned re-admission at six months. Secondary
outcomes were number of unplanned re-admissions, six-minute walking distance,
London Handicap Scale and public health care and personal care costs.
Results. At sixth months, the re-admission rates were not significantly different (46
vs. 57% in control subjects, p 0233, Chi-square test). But the median number of
re-admissions tended to lower in the intervention group (0 vs. 1 in control group,
2008 The Authors. Journal compilation 2008 Blackwell Publishing Ltd 109doi: 10.1111/j.1365-2702.2007.01978.x
-
7/31/2019 Prevent Readmission Heartfailure
2/10
p 0057, Mann Whitney test). Intervention group subjects had less handicap in
independence (median change 0 vs. 05 in control subjects, p 0002, Mann
Whitney test), but there was no difference in six-minute walking distance. There was
no significant group difference in median total public health care and personal care
costs.
Conclusion. Community nurse-supported post-discharge programme was effective
in preserving independence and was probably effective in reducing the number of
unplanned re-admissions. The cost benefits to public health care were not signifi-
cant.
Relevance to clinical practice. Older chronic heart failure patients are likely to
benefit from post-discharge community nurse intervention programmes. More
comprehensive health economic evaluation needs to be undertaken.
Key words: cogestive, community health nursing, cost benefit analysis, heart failure,
older people
Introduction
Chronic heart failure (CHF) is a major health problem of
older people and is associated with recurrent hospital
admissions (Kwok et al. 1999). To account for this, several
factors have been identified. Lack of social support and
psychological maladjustment could contribute to symptoms
and health seeking behaviour. Under use of evidence-based
care for CHF, poor drug and dietary adherence, poor access
to medical care are additional potentially avoidable factors
(Williams & Fitton 1988, Ahmed 2003).
Post-hospital discharge home visits by nurses, with or
without medical or multidisciplinary support (Rich et al.
1995, Stewart et al. 1999, Blue et al. 2001, McAlister et al.
2004), have been shown to be effective in preventing re-
admission of high-risk patients with CHF. These programmes
have also been shown to be cost-effective (Williams & Fitton
1988, Naylor et al. 1994, Phillips et al. 2004). However,
these studies were performed in developed countries where
older people enjoyed comprehensive coverage of primary and
secondary health care either by insurance or by public
funding.
The publicly funded hospitals in Hong Kong are well
equipped and their charges are nominal. On the contrary,
primary health care is primarily private and not easilyaffordable to many older people. There is, therefore, a big
incentive for the chronic sick to rely on the Accident and
Emergency Departments (A&E) of public hospitals for the
relief of their symptoms. The communication between
hospital doctors and general practitioners is also poor.
For example, on hospital discharge, patients are only given a
summary of medical diagnoses and medication and the
summaries are not directly sent to the general practitioners.
It is, therefore, not surprising that older CHF patients in
Hong Kong have very high re-admission rates (at four weeksas high as 15%) (Kwok et al. 1999). In a local prospective
study of hospital-discharged older medical patients, major
problems in communication about medications and follow-
up arrangement, lack of community support and increase in
functional disabilities were identified (Woo & Cheung 1993).
In view of these problems, we envisaged that the post-
discharge community nursing programme for older CHF
patients had to be more intensive in Hong Kong. We,
therefore, performed a randomized controlled trial to exam-
ine its effectiveness and cost-effectiveness. The hypothesis
was that an intensive post-discharge community nursing
programme will reduce the chance of re-admission by
improving functional status and reducing handicap of older
CHF patients.
Methods
Subjects
Hospital patients with a principal diagnosis of CHF were
recruited from the medical wards in Prince of Wales Hospital
(PWH), a major teaching hospital in Hong Kong. A minority
of subjects were recruited in another acute district generalhospital, Alice Ho Miu Ling Nethersole Hospital (AHNH) in
the same health region. The two hospitals were publicly
funded and provided comprehensive specialist inpatient and
outpatient services for a regional population of one million.
The mean length of stay in the medical departments in these
hospitals was five days. Some frailer CHF patients, who
required a longer period of convalescent care, were dis-
charged to the two convalescent hospitals in the region
T Kwok et al.
110 2008 The Authors. Journal compilation 2008 Blackwell Publishing Ltd
-
7/31/2019 Prevent Readmission Heartfailure
3/10
Shatin and Taipo Hospitals. The inclusion criteria included
age older than 60, residing within the region and had at least
one hospital admission for CHF in the 12 months prior to the
index admission. The exclusion criteria included having
communication problems but without caregivers, residing in
a nursing home and terminal diseases with a life expectancy
of less than six months.
Procedure
Eligible subjects were identified and recruited by a research
nurse (RN) on the day or the day before hospital discharge.
After obtaining written consent from the subjects, the RN
recorded demographic data. Functional status was assessed
by six-minute walking test (Butland et al. 1982). Cognitive
function, psychological state and handicap were assessed by
Abbreviated Mental Test (AMT) (Chu 1999) General Health
Questionnaire (GHQ) (Chi & Boey 1993) and London
Handicap Scale (LHS) (Lo et al. 2001), respectively.General Health Questionnaire is a screening test aimed at
detecting psychological problems in people living in the
community. It has been translated into Chinese and validated
among older Chinese in Hong Kong (Chi et al. 1995). The
score ranges from 030, with scores of six or above indicating
psychological problems. The LHS was developed in the
United Kingdom and had been translated into Chinese and
validated in Hong Kong (Lo et al. 2001). It consisted of one
question for each of the six domains of handicap (mobility,
independence, occupation, social, orientation and economic).
For each domain, there were six progressive levels of
handicap. Higher score indicates higher level of handicap.
In subjects with AMT score less than 6/10, family caregivers
provided information for the handicap scale.
The ward nurses then phoned a second research assistant
who assigned trial grouping according to a random number
table. The group assignment was made known to the
patients.
All subjects were followed up by designated geriatricians or
cardiologists in their respective hospital medical clinics. The
interval of clinic appointment ranged from 612 weeks on
average. When the subjects were re-admitted, they were
assessed by either a geriatrician or a cardiologist for reasons ofre-admission. The primary and secondary causes of re-admis-
sion were categorized as follows: exacerbation of existing
disorder, new but related event, new unrelated event, elective,
admission with no deterioration, social/psychological prob-
lems, drug-related problems and dietary non-compliance.
After six months of trial, subjects had their functional and
psychosocial status re-assessed, as in the baseline, at the
follow-up clinics. The RN was not aware of the
randomization grouping of the subjects. All hospital admis-
sions, including attendance to the A&E, throughout Hong
Kong were traced by an electronic database maintained by
the Hospital Authority which operated all publicly funded
hospitals in Hong Kong.
Intervention group
The subjects were visited by a designated community nurse
(CN) before they were discharged from the hospital. The
objectives were to provide health counselling, such as drug
compliance, dietary advice and to encourage subjects to
contact CN via a telephone hotline during office hours when
they developed symptoms. The CN carried a pager and a
mobile phone. The trained clerk, who answered the hotline,
relayed the message from the subjects to the CN via the
pager.
The subjects were then visited by the CN at home within
seven days of discharge. During the home visits, the CN
checked vital signs and signs for poor control of CHF ankleswelling, dyspnoea and basal crepitation on auscultation.
Medications were checked and compliance encouraged.
Avoidance of salty and high fat foods and regular physical
exercise were promoted. Home care and day care services
were arranged if social support was found to be insufficient.
The CN thereafter performed home visits at weekly
intervals for another four weeks and monthly after that.
The CN liaised closely with either a geriatrician or a
cardiologist in their respective hospitals. After liaison, the
CN could alter medication regime, arrange urgent hospital
outpatient appointments and clinical admission. When sub-
jects were re-admitted, the CN visited the patients in the
hospital and provided background information to attending
doctors. Subjects who refused further home visits were
monitored by the CN by telephone.
Control group
The control subjects received usual medical and social care,
except that they were followed up in the hospital outpatient
clinics by the same group of designated geriatrician or car-
diologist.
Ethics approval
The study was approved by the Research Ethics Committee
of the Chinese University of Hong Kong.
Sample size calculation
According to the results from a pilot study of 49 older CHF
patients discharged from PWH, the re-admission rate at six
Older people Post-discharge program in heart failure
2008 The Authors. Journal compilation 2008 Blackwell Publishing Ltd 111
-
7/31/2019 Prevent Readmission Heartfailure
4/10
months was 69%, a sample size of 50 per group was estimated
to have 80% chance of detecting a 40% relative reduction in
re-admission rate at a confidence interval of 0 95.
Statistical analysis
The primary outcome was the percentage of subjects who
ever had unplanned hospital re-admissions within six calen-
dar months of discharge. The secondary outcomes included
the following: number of unplanned hospital re-admissions,
changes in six-minute walking test and LHS domain scores.
Comparison of proportion of subjects with re-admissions
was made by Chi-square test. As the secondary outcome
variables were not normally distributed, Mann Whitney
U test was used for group comparison. Because LHS has six
domains, p-value has to be
-
7/31/2019 Prevent Readmission Heartfailure
5/10
At the six-month follow-up, 44 in the intervention group
and 46 in the control group were available for re-assessment
for the six-minute walking test and LHS scores (Table 2).
When compared with the control subjects, the intervention
group subjects became significantly less limited in independ-
ence (median change in LHS independence domain score 0 vs.
05, p < 0005, Mann Whitney test). The change in
functional status of the subjects, as reflected by the six-
minute walking test, was not different between the groups.
The group comparison of costs to public health care system
was shown in Table 3. One intervention group subject andtwo control group subjects had missing records of outpatient
attendance and were therefore excluded. The median
community nursing costs in the intervention group was
HK$2 391 per subject. The median total public health costs
as a result of hospital stay and emergency care attendances
were significantly lower in intervention group than in control
group (HK$5 229 vs. HK$20 916, p 0048). However, the
total public health care costs were not significantly different.
Table 1 Baseline characteristics of
intervention (community nursing) and
control group subjects*
Intervention (n 49) Control (n 56)
Male 22 (45%) 25 (45%)
Age (years) 795 66 768 70
Live alone 15 (31%) 10 (18%)
CSSA 23 (47%) 14 (25%)
Six-minute walking test (m) 1207 620 1185 625
Abbr eviated Mental Test (max. 10) 86 14 87 13
General Health Questionnaire (max. 30) 56 37 61 33
London Handicap Scale (max. 6)
Mobility 3 (2, 3) 3 (3, 3)
Independence 3 (2, 3) 3 (2, 3)
Occupation 3 (3, 4) 3 (3, 4)
Social 2 (2, 2) 2 (2, 2)
Orientation 2 (2, 2) 2 (2, 2)
Economic 3 (3, 4) 3 (2, 3)
Left ventricular EF
-
7/31/2019 Prevent Readmission Heartfailure
6/10
The medical and social costs paid by the subjects were
shown in Table 4. One intervention and two control group
subjects who attended the six month follow-up had missing
personal cost data. There was no significant group difference
in the total health and social care costs to the patients.
However, only 17 out of 49 intervention group subjects
(34%) paid for CN visits: 24 by CSSA, one by civil service
pension scheme, eight by research grant because of refusal topay. To exclude the confounding effect of waivers, the
personal cost analysis was repeated after excluding those
eligible for CSSA or civil service pension in both groups and
on the assumption that all those subjects who had to pay for
CN paid by themselves. The median cost of CN visits per
subject was HK$385 (quartile range 330, 578). The median
total personal costs (medical and social included) of the
intervention (n 21) and control (n 32) group subjects
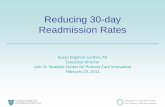
Randomized
(n = 105)
Intervention(n = 49)
Control(n = 56)
Completed(n = 44)
Completed(n = 46)
Dropout(one moved )
Dropout(one moved,one cancer)
Six month
follow-up
Died
(n = 8)Died
(n = 4)
Readmitted
(n = 19)
Not readmitted
(n = 25)Readmitted
(n = 24)
Not readmitted
(n = 22) Figure 1 Flow diagram of major outcomes
of randomized subjects.
Table 3 Comparison of total public health
costs per person in six months between
intervention (community nursing) and
control groups*
Cost item Intervention (n 48) Control (n 54)
Hospital bed and emergency care 5 229 (0, 33 384) 20 916 (534, 72 312)
Outpatient clinic 1 365 (910, 1 544) 1 365 (533, 1 365)
Community nursing 2 391 (1 600, 3 050) 0 (0, 0)
Total 10 186 (3 785, 37 962) 21 599 (1 978, 73 449)
*HK$ presented as median (interquartile range).
Table 4 Medical and social care costs to subjects in six months*
Cost item
Intervention
(n 43) Control (n 44)
Outpatient clinic 0 (0, 132) 132 (0, 132)
Travel to clinics/hospital 100 (38, 150) 75 (33, 144)
Hospital stay 0 (0, 136) 0 (0, 527)
Community nurse 0 (0, 330) 0 (0, 0)
Private doctor 0 (0, 360) 0 (0, 608)Social services 0 (0, 10) 0 (0, 0)
Total 513 (213, 2 407) 775 (184, 2 107)
*HK$ presented as median (25th, 75th percentile); 12 control and 22
intervention group subjects had all charges waived because of com-
prehensive social security assistance or retired civil servant status;
seven intervention group subjects had community nurse visits paid by
research fund.Home help, meals on wheel, day care centre, escort for medical
follow-up.
T Kwok et al.
114 2008 The Authors. Journal compilation 2008 Blackwell Publishing Ltd
-
7/31/2019 Prevent Readmission Heartfailure
7/10
were HK$1 457 (589, 4 011) and 922 (193, 2 269), respect-
ively. The difference was not significant (P 0118, Mann
Whitney U test).
Discussion
Our results demonstrated that an intensive post-discharge
community nursing intervention programme for older CHF
patients could not reduce the chance of re-admissions in six
months, but was probably effective in reducing the number of
unplanned re-admissions. The latter is consistent with the
results of other similar trials overseas. The low drop out rate
in the intervention group reflects an overall good acceptance
of the intervention.
The subjects were well matched except that the interven-
tion group had more financial hardship. This might have had
a negative influence on the rate of public health care
utilization in the intervention group.
As expected for older CHF subjects, only a third of thesubjects had systolic heart failure. Consistent with clinical
practice at the time of the study, the great majority of CHF
patients were on diuretics and the use of angiotensin
converting inhibitor (ACEI) and beta blockers was limited.
It is noteworthy that the use of ACEI and beta blockers has
been associated with less re-admission in CHF patients
(Fowler et al. 2001, Abarca et al. 2004). The change of
medication after recruitment was unfortunately not docu-
mented in this study. However, as both groups were managed
by the same specialist outpatient clinics, significant differ-
ences in medication use were unlikely.
Although the intervention did not significantly reduce the
chance of admission within six months, it reduced the
number of unplanned admissions. The lower mortality rates
of the intervention group subjects (83 vs. 148% in control
subjects) suggested that the CN intervention did not delay
hospital admissions when they were needed. A meta-analysis
showed that post-discharge CN interventions, when com-
bined with specialist medical support, can reduce mortality of
CHF patients (McAlister et al. 2004).
Community nurse intervention did not improve functional
status of the CHF patients. However, relative to the control
group who showed deterioration in the independence domainof handicap, CN intervention helped to maintain the level of
independence. The educational and advisory role of the CN
had probably helped the patients and the family caregivers to
better manage the disease and its associated disabilities.
The CN might have been effective in preventing some
admissions by enhancing the interface between hospital
services and the medical needs of CHF patients and possibly
by improving the self-management of the disease by the
patients or the family members. There was still room for
improvement as a few intervention group subjects were still
re-admitted for dietary non-adherence and drug-related
problems.
The CN intervention can potentially be more effective if
they can have training in two important areas of self-
management of CHF, namely diet and exercise. There is good
evidence that regular physical exercise is beneficial to the
exercise tolerance of CHF patients (Smart & Marwick 2004),
even in advanced age and in the home setting (Corvera-Tindel
et al. 2004). CNs are in a good position to motivate older
patients to perform physical exercises that suit their lifestyle.
However, they require training in the prescription of physical
exercise and information about locally available exercise
programmes. Salty diet is a common problem in older people,
particularly in those with CHF. Simple advice to restrict salt
is usually not adequate to change behaviour in the long term
(Gonzalez et al. 2005). More training in dietetic approaches
in gradual salt restriction is needed.The high rate of re-admissions for reasons which may or
may not be related to CHF suggests that this group of
patients requires close medical supervision. Unfortunately,
most subjects in both groups relied primarily on specialist
outpatient clinics, but, the frequency of specialist outpatient
clinic is necessarily limited because of the workload in
hospitals and patients may not welcome that. The cost data
showed that the cost of transport to outpatient clinic
comprised a significant proportion of their health care costs.
Moreover, many older people have trouble finding their way
round the hospital clinics, therefore requiring family
members to escort them.
Primary health care clinics which are more locally access-
ible should play a major role in the follow-up of these high-
risk individuals in the community. This is indeed the case in
most Western countries, but our data confirmed that the use
of primary health care was minimal (data not shown). This
highlights the under use or inaccessibility of primary health
care for at risk older people. As in public hospitals, the
government general outpatient clinics (GOPD) had low
charges which were waived in those on CSSA, but to be seen
at the clinics, one had to queue for a consultation quota early
in the morning. This is not feasible for an ill older person. Inthe last two years, the Hospital Authority has taken over the
administration of the GOPD. This opens up the possibility of
arranging follow-up in GOPD upon hospital discharge and
the sharing of clinical data via the HA territory-wise
computerized client management system (CMS).
Private clinics are widely available in Hong Kong, but this
group of patients might have found them unaffordable. For
those who can afford it, the private doctors can potentially be
Older people Post-discharge program in heart failure
2008 The Authors. Journal compilation 2008 Blackwell Publishing Ltd 115
-
7/31/2019 Prevent Readmission Heartfailure
8/10
more helpful if they can have access to clinical information
about the patients. At present, all hospital patients are
provided with a computer-generated discharge note showing
the diagnoses and medication. The detailed discharge sum-
mary is deliberately withheld from the patients because of
confidentiality issues. Patients can request medical reports
but, they are charged a significant fee and the procedures
normally take a few weeks. This administrative culture of
non-disclosure hinders the free flow of clinical information
which is critically important if doctors in the community are
expected to participate in chronic disease management. Pilot
programmes allowing selected private general practitioners to
gain access to their regular patients clinical information in
the CMS via the internet are under way.
The CN programme was probably effective in reducing
the costs of hospital stay and emergency care attendance,
but when the costs of CN were considered, the net gain in
public health care costs was not significant. In contrast,
most overseas post-discharge CN programmes were shownto be cost effective (McAlister et al. 2004). Admittedly, this
trial was under-powered to detect a small reduction in
health care costs. Nevertheless, this CN programme might
have been more cost effective if less home visits were made.
The number of home visits in this programme was greater
than in most previous trials which emphasized predischarge
face-to-face hospital visits and post-discharge phone follow-
ups more (Naylor et al. 1994, Krumholz et al. 2002). Apart
from the need to have an early home visit for an initial
assessment and formulation of management plan, the need
for further visits will largely depend on the resources and
physical condition of the patients. The greater use of
telephone follow-up and empowerment of patients and their
families in disease management may reduce the need for
home visits, therefore enhancing the cost-effectiveness of the
programme.
The costs to the patients were not overall increased by CN
intervention. However, a CN visit cost HK$55 in Hong Kong
at the time (the charge was increased to HK$80 in 2003).
After excluding those who were eligible for waived charges,
the cost of CN visits was a significant proportion of the total
health care costs paid by the patients. Further cost analysis
confirmed that the CN intervention tended to increase theoverall cost of care to the patients. It was, therefore, not
surprising that a significant proportion of subjects who had to
pay refused to do so. In Hong Kong, only those with net asset
of less than HK$30 000 were eligible for comprehensive
social security assistance which included waiving of all
charges from public services. However, there are many at
risk older people who are not eligible for CSSA, but have
meagre monthly incomes. This seriously questions the
rationale of charging for community health services which
can potentially reduce overall health care costs.
The strength of this trial is that it was the first randomized
controlled trial of CN intervention in CHF patients in Hong
Kong where the primary health care is not well organized.
The outcomes in functional status and handicap and cost
analysis were considered at the same time. The main
limitation was the small sample size which only allowed the
detection of a major effect of CN intervention. The subjects
had multiple medical problems and high mortality. In the cost
analysis, the hospital and clinic costs were all standardized.
The indirect costs to patients were not considered. More
comprehensive cost analysis is warranted.
Conclusion
We concluded that post-discharge visits by CNs in older
chronic cardiac failure patients were not effective in reducing
the chance of re-admission within a six month period. But,they were effective in preserving independence and were
probably effective in reducing the number of unplanned re-
admissions. More comprehensive health economic evaluation
needs to be undertaken.
Acknowledgements
We would like to express our gratitude to the participating
community nursing teams, Ms Eliza Lau, Dr Chan Chi Kin,
and Prof John Sanderson. The research was funded by the
Health Services Research Committee/Health Care & Promo-
tion Fund (HSRC/HCPF) of Hong Kong.
Statement of Competing Interests
None.
Contributions
Study design: KT, LTFD; data collection and analysis: KT,
WJ; manuscript preparation: KT, LJ, GS, WJ.
References
Abarca J, Malone DC, Armstrong EP & Zachry WM III (2004) An-
giotensin-convertingenzyme inhibitortherapy in patients withheart
failure enrolled in a managed care organization: effect on costs and
probability of hospitalization. Pharmacotherapy 24, 351357.
Ahmed A (2003) American College of Cardiology/American Heart
Association Chronic Heart Failure Evaluation and Management
guidelines: relevance to geriatric practice. Journal of the American
Geriatrics Society 51, 123126.
T Kwok et al.
116 2008 The Authors. Journal compilation 2008 Blackwell Publishing Ltd
-
7/31/2019 Prevent Readmission Heartfailure
9/10
Blue L, Lang E, McMurray JJ, Davie AP, McDonagh TA, Murdoch
DR, Petrie MC, Connolly E, Norrie J, Round CE, Ford I &
Morrison CE. (2001) Randomized controlled trial of specialist
nurse intervention in heart failure. British Medical Journal 323,
715718.
Butland RJA, Pang J, Gross ER et al. (1982) Two, six and 12 minute
walking tests in respiratory disease. British Medical Journal 284,
16071608.
Chi I (1995) Mental health of the old-old in Hong Kong. ClinicalGerontologist 15, 3144.
Chu LW, Pei CKW, Ho MH & Chan PT. (1995) Validation of the
abbreviated mental test (Hong Kong version) in the elderly medical
patient. Hong Kong Medical Journal 1, 207211.
Corvera-Tindel T, Doering LV, Woo MA, Khan S & Dracup K
(2004) Effects of a home walking exercise program on functional
status and symptoms in heart failure. The American Heart Journal
147, 339346.
Fowler MB, Vera-Llonch M, Oster G, Bristow MR, Cohn JN, Co-
lucci WS, Gilbert EM, Lukas MA, Lacey MJ, Richner R, Young ST
& Packer M (2001) Influence of carvedilol on hospitalizations in
heart failure: incidence, resource utilization and costs. U.S.
Carvedilol Heart Failure Study Group. Journal of the American
College of Cardiology 37, 16921699.
Gonzalez B, Lupon J, Herreros J, Urrutia A, Altimir S, Coll R, Prats
M & Valle V (2005) Patients education by nurse: what we really
do achieve? European Journal of Cardiovascular Nursing 4, 107
111.
Krumholz HM, Amatruda J, Smith GL, Mattera JA, Roumanis SA,
Radford MJ, Crombie P & Vaccarino V (2002) Randomized trial
of an education and support intervention to prevent readmission of
patients with heart failure. Journal of the American College of
Cardiology 39, 8389.
Kwok T, Lau E, Woo J, Luk JKH, Sham A, Wong E & Lee SH (1999)
The incidence of and risk factors for hospital readmission in older
medical patients in Hong Kong a cohort study. Journal of the
Royal College of Physicians of London 33, 153156.
Lo R, Harwood R, Woo J, Yeung F & Ebrahim S (2001) Cross-
cultural validation of the London handicap scale in Hong Kong
Chinese. Clinical Rehabilitation 15, 177185.
McAlister FA, Stewart S, Ferrua S & McMurray JJV (2004) Multi-
disciplinary strategies for management of heart failure patients at
high risk for admission: a systemic review of randomized trials.
Journal of the American College of Cardiology 44, 810819.Naylor M, Brooten D, Jones R, Ravizzo-Mourey R, Mezey M &
Pauly M (1994) Comprehensive discharge planning for the hospi-
talized elderly: a randomised clinical trial. Annals of Internal
Medicine 120, 9991006.
Phillips CO, WrightSM, Kern DE, SingaRM, ShepperdS & Rubin HR
(2004) Comprehensive discharge planning with post discharge sup-
port for olderpatients with congestive heartfailure: a meta-analysis.
Journal of the American Medical Association 291, 13581367.
Rich MW, Beckham V, Wittenberg C, Leven CL, Freedland KE &
Carney RM (1995) A multidisciplinary intervention to prevent the
readmission of elderly patients with congestive heart failure. The
New England Journal of Medicine 333, 11901195.
Smart N & Marwick TH (2004) Exercise training for patients with
heart failure: a systematic review of factors that improve mortality
and morbidity. The American Journal of Medicine 116, 693706.
Stewart S, Marley JE & Horowitz JD (1999) Effects of a multi-
disciplinary, home-based intervention on unplanned readmissions
and survival among patients with chronic congestive heart failure:
a randomized controlled study. Lancet354, 10771083.
Williams EI & Fitton F (1988) Factors affecting early unplanned
readmission of elderly patients to hospital. British Medical Journal
297, 784787.
Woo J & Cheung A (1993) A survey of elderly people discharged
from hospital. Journal of Hong Kong Medical Association 45,
291297.
Older people Post-discharge program in heart failure
2008 The Authors. Journal compilation 2008 Blackwell Publishing Ltd 117
-
7/31/2019 Prevent Readmission Heartfailure
10/10