Prevalence of lower urinary tract symptoms in individuals with Down syndrome
6
Prevalence of lower urinary tract symptoms in individuals with Down syndrome * Fla ´via Cristina de Carvalho Mrad a,b, *, Jose´ de Bessa Junior c , Adrianne Maria Berno de Rezende Duarte a , Augusto Alves Pinho Vieira a , Frederico Cantarino Cordeiro Araujo a , Maı ´ra Lorenzo de Sa ´ Camargo a , Sandra Helena Cerrato Tibiric ¸a a , Andre´ Avarese de Figueiredo a , Jose´ Murillo de Bastos Netto a a Federal University of Juiz de Fora, Juiz de Fora, Minas Gerais, Brazil b School of Medical Sciences and Health, Juiz de Fora, Minas Gerais, Brazil c State University of Feira de Santana, Feira de Santana, Bahia, Brazil Received 7 August 2013; accepted 15 February 2014 KEYWORDS Voiding disorder; Dysfunctional voiding symptom score; Down syndrome; Children; Prevalence; Functional constipation Abstract Objectives: Down syndrome (DS), which is caused by the trisomy of chromosome 21, is the most frequent of all genetic syndromes. The current study aims to estimate the prev- alence of lower urinary tract symptoms (LUTS) in individuals with DS buy using the Dysfunc- tional Voiding Symptom Score (DVSS) and correlate with functional constipation, age, and gender, as well as determine the most sensitive and specific factors associated with LUTS. Methods: LUTS was assessed in individuals with DS using a cross-sectional study through the application of a validated and adapted version of the DVSS for the Brazilian population. The presence of functional constipation was evaluated according to the Rome III criteria. Results: Of the 114 individuals assessed, 84 were included in the study (median age 16 5.0 years, 66.7% female). The prevalence of LUTS was 27.3%. The symptoms were more frequent in males (OR 3.0, 95% CI 1.1e8.3, p Z 0.03) and in individuals younger than 10 years of age (OR 5.2, 95% CI 1.8e14, p Z 0.001). Functional constipation was observed in 50% of subjects. It was detected in 95.65% of the individuals with LUTS and 32.78% without LUTS (OR 45.1, 95% CI 5.66 e301, p Z 0.001). The symptom listed in question 8 (“push to pee”) was the most specific in- dicator. When present, this symptom indicated a higher probability of LUTS (LRþ Z 6.3), while the symptom listed in question 4 (“push for bowel movements to come out”) showed high * This work was carried out at the Center for Interdisciplinary Research in Urology, Federal University of Juiz de Fora, Minas Gerais, Jose ´ Lourenc ¸o Kelmer s/n e Campus Universitario, 36036900, Brazil. * Corresponding author. Ludwig Van Beethoven 80, Juiz de Fora, MG 36036634, Brazil. Tel.: þ55 32 8852 6360. E-mail addresses: [email protected] , fl[email protected] (F.C. de Carvalho Mrad). + MODEL Please cite this article in press as: de Carvalho Mrad FC, et al., Prevalence of lower urinary tract symptoms in individuals with Down syndrome, Journal of Pediatric Urology (2014), http://dx.doi.org/10.1016/j.jpurol.2014.02.011 http://dx.doi.org/10.1016/j.jpurol.2014.02.011 1477-5131/ª 2014 Journal of Pediatric Urology Company. Published by Elsevier Ltd. All rights reserved. Journal of Pediatric Urology (2014) xx,1e6
-
Upload
jose-murillo -
Category
Documents
-
view
212 -
download
0
Transcript of Prevalence of lower urinary tract symptoms in individuals with Down syndrome

+ MODEL
Journal of Pediatric Urology (2014) xx, 1e6
Prevalence of lower urinary tract symptomsin individuals with Down syndrome*
Flavia Cristina de Carvalho Mrad a,b,*, Jose de Bessa Junior c,Adrianne Maria Berno de Rezende Duarte a,Augusto Alves Pinho Vieira a,Frederico Cantarino Cordeiro Araujo a,Maıra Lorenzo de Sa Camargo a,Sandra Helena Cerrato Tibirica a,Andre Avarese de Figueiredo a, Jose Murillo de Bastos Netto a
a Federal University of Juiz de Fora, Juiz de Fora, Minas Gerais, Brazilb School of Medical Sciences and Health, Juiz de Fora, Minas Gerais, Brazilc State University of Feira de Santana, Feira de Santana, Bahia, Brazil
Received 7 August 2013; accepted 15 February 2014
KEYWORDSVoiding disorder;Dysfunctional voidingsymptom score;Down syndrome;Children;Prevalence;Functionalconstipation
* This work was carried out at the CLourenco Kelmer s/n e Campus Unive* Corresponding author. Ludwig VanE-mail addresses: fonsecamreis@te
Please cite this article in press as: dsyndrome, Journal of Pediatric Urolo
http://dx.doi.org/10.1016/j.jpurol.201477-5131/ª 2014 Journal of Pediatri
Abstract Objectives: Down syndrome (DS), which is caused by the trisomy of chromosome21, is the most frequent of all genetic syndromes. The current study aims to estimate the prev-alence of lower urinary tract symptoms (LUTS) in individuals with DS buy using the Dysfunc-tional Voiding Symptom Score (DVSS) and correlate with functional constipation, age, andgender, as well as determine the most sensitive and specific factors associated with LUTS.Methods: LUTS was assessed in individuals with DS using a cross-sectional study through theapplication of a validated and adapted version of the DVSS for the Brazilian population. Thepresence of functional constipation was evaluated according to the Rome III criteria.Results: Of the 114 individuals assessed, 84 were included in the study (median age 16 � 5.0years, 66.7% female). The prevalence of LUTS was 27.3%. The symptoms were more frequent inmales (OR 3.0, 95% CI 1.1e8.3, p Z 0.03) and in individuals younger than 10 years of age (OR5.2, 95% CI 1.8e14, pZ 0.001). Functional constipation was observed in 50% of subjects. It wasdetected in 95.65% of the individuals with LUTS and 32.78% without LUTS (OR 45.1, 95% CI 5.66e301, p Z 0.001). The symptom listed in question 8 (“push to pee”) was the most specific in-dicator. When present, this symptom indicated a higher probability of LUTS (LRþ Z 6.3), whilethe symptom listed in question 4 (“push for bowel movements to come out”) showed high
enter for Interdisciplinary Research in Urology, Federal University of Juiz de Fora, Minas Gerais, Josersitario, 36036900, Brazil.Beethoven 80, Juiz de Fora, MG 36036634, Brazil. Tel.: þ55 32 8852 6360.rra.com.br, [email protected] (F.C. de Carvalho Mrad).
e Carvalho Mrad FC, et al., Prevalence of lower urinary tract symptoms in individuals with Downgy (2014), http://dx.doi.org/10.1016/j.jpurol.2014.02.011
14.02.011c Urology Company. Published by Elsevier Ltd. All rights reserved.

2 F.C. de Carvalho Mrad et al.
+ MODEL
Please cite this article in press as: dsyndrome, Journal of Pediatric Urolo
sensitivity and, when absent, indicated a lower probability of LUTS (LRe Z 0.1).Conclusions: LUTS was more prevalent in young males with DS and appeared to improve withage. Functional constipation was strongly associated with LUTS. These findings will contributeto raising the awareness of professionals involved in the follow-up of individuals with DSregarding the clinical manifestations and the need for a standardized investigation of LUTS.ª 2014 Journal of Pediatric Urology Company. Published by Elsevier Ltd. All rights reserved.
Introduction
Down syndrome (DS), which is caused by the trisomy ofchromosome 21, is the most frequent of all genetic syn-dromes [1], with a life expectancy of approximately 60years [2]. The prevalence of 1 per 1000 live births is directlyinfluenced by the age of the mother [3]. Individuals with DShave a well-established increased risk of congenital ab-normalities [4,5], constituting the most prevalent geneticcause of intellectual disability [2]. They have an averagedevelopmental delay of 4 years, and more often haveemotional and behavioral problems (8e23%) than childrenfrom the general population [6].
The investigation of urological abnormalities in in-dividuals with DS is not yet well established. Several relatedstudies indicate an elevated prevalence of abnormalities,such as renal agenesis, hydronephrosis, ureteropelvicjunction obstruction, posterior urethral valves, hypospadiasand lower urinary tract symptoms (LUTS) [4,7e12].
LUTS are classified according to their relation to thevoiding and/or storage phase of bladder function, and if itthere is coexistence with functional constipation it isnamed bladder bowel dysfunction (BBD) [13,14]. There isgreat concern in the diagnosis and administration of earlytreatment to prevent urinary tract infections and lesions ofthe upper urinary tract [13]. This concern is also relevant inindividuals with DS. Nevertheless, additional difficultiesarise in diagnosing LUTS in children with DS since theircaregivers often assume that such situations arise as aconsequence of their delayed psychomotor development[6,15].
LUTS affect both the child and the family socially,emotionally, and behaviorally. This places the child at riskfor social isolation, peer conflict, and teasing [16].
The current study aims to estimate the prevalence ofLUTS in individuals with DS and the correlations of thesesymptoms with functional constipation, age, and genderusing the Dysfunctional Voiding Symptom Score (DVSS) [17]adapted and validated for the Brazilian population by Cal-ado et al. [18].
Patients and methods
This cross-sectional study was carried out from February2010 to March 2012, during which 114 individuals with DSwho were regularly attending a specialized clinic for DSwere assessed.
The exclusion criteria were current urogenital disorder,untreated hypothyroidism, current use of medicationsknown to interfere in bladder or sphincter function, andthose that were still using diapers. We chose to stratify the
e Carvalho Mrad FC, et al., Prevgy (2014), http://dx.doi.org/10.1
sample into individuals 10 years old or younger and in-dividuals older than 10 years of age because the DVSS is forchildren younger than 10 years of age.
The interview for the application of the DVSS was con-ducted in a private environment (physician’s office).
The DVSS [17] includes 10 quantitative and qualitativeurological variables assessed by age-appropriate questionsfor children and has been used widely with confirmedreliability and validity as an objective instrument to gradevoiding disorder in children. Each subject, with the help oftheir parents, answered the 10 questions of the validatedBrazilian language version of the Dysfunctional VoidingScore Symptom questionnaire [18].
The first 10 questions of the DVSS assess daytime in-continence, volume of urine leakage, urinary frequency,holding maneuvers, bowel habit, urgency, voiding fre-quency, straining voiding, and dysuria, which are eachscored on a scale of 0e3 (0 almost never, 1 less than halfthe time, 2 about half the time and 3 almost every time). Inquestion 10, the answers were dichotomic: yes for a scoreof 3 and no for a score of 0. The individuals or their parentswere asked if they had experienced any stressful situationsin the previous month. The cut-off values to indicate thepresence of LUTS were >6 for females and >9 for males. Toour knowledge, this is the first study applying the DVSS inindividuals with DS.
All of the included patients were submitted to non-invasive urodynamics. Renal and bladder ultrasound eval-uating urological abnormalities and post-voiding residual,uroflowmetry were performed, and a voiding diary waskept. The cut-off value for post-void residual urine wasclassed as elevated if it was 10% greater than the expectbladder capacity for the age of the child.
The presence of functional constipation was evaluatedaccording to the Rome III criteria [19].
To evaluate present or past urinary tract infection (UTI)or bacteriuria, urine cultures were performed in all pa-tients, and all of the individuals responsible for the patientswere asked if their child had experienced any episodes ofUTI.
The data were expressed as the mean � standard devi-ation (SD), median, and interquartile ranges, or absolutevalues and fractions. The Student t test or the Man-neWhitney test was used to compare continuous variables,while the categorical variables were compared using theFisher exact test. Pearson’s correlation analysis was used todescribe the associations. The odds ratio was used todescribe the magnitude of the association between theabsence or presence of LUTS and gender and age. Thepositive predictive value (PPV) and negative predictivevalue (NPV) were determined for the group of 10 questionsof the DVSS as a means to evaluate the most sensitive and/
alence of lower urinary tract symptoms in individuals with Down016/j.jpurol.2014.02.011

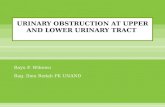
Figure 2 Prevalence of urinary tract symptoms in Downsyndrome (DS) individuals stratified by age.
Lower urinary tract symptoms in Down syndrome 3
+ MODEL
or specific symptoms and to describe the diagnostic accu-racy of the questions. For all the statistical procedures, the95% confidence interval (CI) was applied; the significancelevel was p < 0.05. The data were processed usingcommercially available statistical software (GRAPH padPrism, version 6.00 for Windows).
The current study (protocol number 1960.019.2010) wasapproved by the Ethics Committee of the Federal Universityof Juiz de Fora, and all parents or those responsible for thepatients signed an informed consent form.
Results
Of the 114 individuals assessed, 84were included in the study(28 males and 56 females). The median age of the subjectswas 16 (range 9e22) � 5.0 years (range 4e30 years). Of theindividuals who were excluded, one girl was diagnosed withWest syndrome, two subjects had a posterior urethral valve,and 27 subjects were still wearing diapers.
The overall prevalence of LUTS was 27.3% (23/84). Themean score of the DVSS was 12.4 � 4.4 in individuals withDS with LUTS and 2.5 � 2.7 in individuals without LUTS(p < 0.001).
When compared by gender, the prevalence of LUTS wassignificantly higher in males than in females. LUTS werepresent in 42.8% (12/28) of the males and 19.6% (11/56) ofthe females (OR 3.0, 95% CI 1.1e8.3, p Z 0.03).
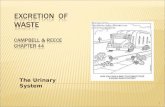
There was an inverse association between age and theDVSS score (R Z �0.27, 95% CI e0.46 to �0.06, p Z 0.01)(Fig. 1).
The median age in patients with LUTS, 9 (8e11) years,was significantly lower than in asymptomatic subjects 18(11e28) years (p < 0.01).
LUTS was observed in 14 (60.8%) patients who were 10years old or younger, and in nine (39.1%) patients older than10 years of age (OR 5.2, 95% CI 1.8e14, p Z 0.001) (Fig. 2).
Figure 1 Correlation among age individuals with Down syn-drome (DS) and Dysfunctional Voiding Symptom Score (DVSS).
Please cite this article in press as: de Carvalho Mrad FC, et al., Prevsyndrome, Journal of Pediatric Urology (2014), http://dx.doi.org/10.1
The symptom mentioned in question 8 of the DVSS(“Does your son/daughter need to push to pee?”) was themost specific to indicate LUTS, with a specificity of 91.8%(95% CI 81.9e97.2). When present, this symptom indicateda higher probability of LUTS (LRþZ 6.3; PPVZ 70.5%). Thesymptom referred to in question 4 (“Does your son/daughter need to push for his/her bowel movements tocome out?) was the most sensitive, with a sensitivity of86.9% (95% CI 66.4e97.2) and if absent, it indicated a lowprobability of LUTS (LRe Z 0.1; NPV Z 92.6%) in thispopulation. As these questions are known to be more spe-cific and sensitive, more attention could be paid to themwhen the whole score is close to the cut-off value.
Table 1 presents a description of the sample (generaland stratified by gender) in accordance with the urinarysymptoms assessed by the DVSS and the p value for eachquestion.
Functional constipation (characterized according toRome III criteria) was observed in 50% of subjects (42/84)and strongly associated with LUTS. It was presented in95.65% (22/23) of the individuals with LUTS and 32.78% (20/61) without LUTS (OR 45.1, 95% CI 5.6e301, p Z 0.001).
A significant residual urinary volume was observed in21.7% (5/23) patients with LUTS and none of the asymp-tomatic (pZ 0.04), and one male presented with unilateralhydronephrosis grade II. Bacteriuria was diagnosed in 17.3%(4/23) patients with LUTS and 3.2% (2/61) asymptomaticones (p < 0.001).
Discussion
The prevalence of LUTS in individuals with DS found in thepresent study was 27.3%, in accordance with others studiesthat have demonstrated 20e30% of children have dysfunc-tional voiding [20,21]. Our findings were also similar to thestudy of Vaz et al. [22], including 739 Brazilian typicallydeveloped students, in which the prevalence of LUTS wasestimated to be 21.8%.
The tool used in this study consists of an adapted andvalidated version of the DVSS [17] for the Brazilian popu-lation, performed by Calado et al. [18]. This instrumentprovides a reliable score for the numeric gradation of uri-nary symptoms in children and provides structured quanti-tative data that allow standardization of the LUTSdiagnosis. It is important to consider the lack of existenceof a specific tool to investigate urinary symptoms in in-dividuals with DS.
alence of lower urinary tract symptoms in individuals with Down016/j.jpurol.2014.02.011

Table 1 Description of symptoms in individuals with Down syndrome (DS) with and without LUTS stratified by gender.
Question Variable With LUTS (n Z 23) Without LUTS (n Z 61) p value
T % M % F % T % M % F %
1 Daytime incontinence 56.5 54.5 63.6 9.80 0.0 11.1 <0.0012 Volume of urine leakage 52.2 54.5 50 8.20 0.0 11.1 <0.0013 Frequency of Evacuation 65.2 50 81.8 21.3 11.7 24.4 <0.0014 Push bowel movements 87.0 83.3 90 36.1 23.5 40.0 <0.0015 Low urinary frequency 78.3 81.8 83.3 16.4 13.3 16.5 <0.0016 Holding maneuvers 78.3 83.3 90.9 39.3 35.2 42.0 0.0017 Urgency 56.5 81.8 63.6 23.0 11.7 22.0 0.0038 Straining voiding 52.2 54.5 41.6 8.20 8.30 8.80 <0.0019 Dysuria 34.8 25.0 16.6 8.20 0.00 10.5 0.00310 Stressful events 26.1 15.0 16.0 16.4 14.0 12.0 0.313
LUTS Z lower urinary tract symptoms; DS Z Down syndrome.
4 F.C. de Carvalho Mrad et al.
+ MODEL
There are few studies on the investigation of LUTS inindividuals with DS, and none has applied the DVSS. Handelet al. [9] radiologically and urodynamically evaluated 26male patients with DS and found a prevalence of 15% forLUTS. In another retrospective study, using urodynamicinvestigation in 24 individuals with DS, the prevalence ofLUTS was found to be 45.8% [10]. In two systematic reviewsintending to estimate the prevalence of urological abnor-malities and comorbidities associated with DS, an increasedprevalence of LUTS was also observed [4,11]. The widerange of different methodologies used to evaluate LUTSmay explain the discrepancies related to the prevalence ofLUTS. Thus, standardization of methodologies is necessaryfor the diagnosis of LUTS.
LUTS were found to be more prevalent in male in-dividuals with DS (42.8%) than in females (19.6%), which isconsistent with the results reported by Burgu et al. [23].However, this finding disagrees with other results reportedin the literature for typically developing children, in whicheither a higher prevalence of LUTS was found in femaleindividuals [22] or no significant difference between gen-ders was found [24].
In the present study, we opted to stratify the sampleinto individuals 10 years old or younger, and older than 10years of age because the DVSS is for children younger than10 years of age. However, even in an adult life, 23% of in-dividuals with DS showed cognitive limitations, with diffi-culty performing daily life activities, including personalhygiene and toilet use [6]. Thus, the DVSS was applied to allindividuals with DS, regardless of their age.
LUTS decrease in both genders between 4.5 and 9.5years [25]. This present study has shown that in individualswith DS who are older than 10 years, the chance of LUTS isfive times lower than in those who are 10 years old oryounger. Hence, in this study, and in others, a tendency ofthe reduction of symptoms with the progression of age isobserved. This is in agreement with Rihtman et al. [15],who reported that, as they grow older, individuals with DSshow better motor and cognitive skills, which could lead toa better urinary pattern, especially if appropriate in-terventions are provided.
The mean DVSS value was significantly higher in in-dividuals with DS with LUTS than in those individualswithout LUTS (12.4 � 4.4 and 2.5 � 2.7, respectively).
Please cite this article in press as: de Carvalho Mrad FC, et al., Prevsyndrome, Journal of Pediatric Urology (2014), http://dx.doi.org/10.1
Burgu et al. [23] assessed the DVSS score in children withattention deficit hyperactivity disorder and showed resultssimilar to those presented here, although the surveyedpopulations were different. The total mean DVSS score foreach group was 11.1 � 2.9 and 3.2 � 1.3, respectively.
DS is the most frequent genetic cause of intellectualdisability [2]. It is therefore important to compare thisstudy with others involving children with cognitive impair-ments. Yang et al. [26] evaluated 51 children with intel-lectual disability, and the prevalence of voiding disorderwas found to be 35.2%. Individuals with intellectualdisability have difficulty describing their urinary symptoms.Hence, studies that focus on estimating the prevalence ofLUTS in individuals with intellectual disability are impor-tant to guide caregivers and reduce associated morbidities.The prevalence of neurobehavioral disorders [27e29] intypically developing children and teenagers is approxi-mately 10e15% [23] in contrast to 23% in individuals with DS[6]. In both groups with neurobehavioral disorders, it can benoted that there is an increase in LUTS [10,11,23,24,29],which is in accordance with the results shown in this study.Factors that contribute to LUTS in individuals with DS areabnormal bowel habit, lack of guidance to caregivers aboutthe age of toilet training and also as a consequence ofdelayed psychomotor development.
In this study, functional constipation (characterized ac-cording to Rome III criteria) was detected in 95.65% of in-dividuals with LUTS and in 32.78% of individuals withoutLUTS. This confirms that when the symptom mentioned inquestion 4 of the DVSS (“Does your son/daughter need topush for his/her bowel movements to come out?”) waspresent, there was a higher probability of LUTS, with asensitivity of 86.96%. These findings corroborate the resultsfound by Burgers et al. [30], who evaluated 113 childrenwith LUTS. More than 50% of these children presented withfunctional constipation. Thus, the evaluation of bowelhabits is recommended as part of the assessment of chil-dren with LUTS for diagnosing BBD [16,30]. It is importantto report that one of the individuals included in our studywas diagnosed with Hirschsprung’s disease.
Among the DS children with LUTS, 21.7% had incompletebladder emptying and 17.3% had bacteriuria. One malepresented with unilateral hydronephrosis grade II. Yanget al. [26] conducted a study in children with intellectual
alence of lower urinary tract symptoms in individuals with Down016/j.jpurol.2014.02.011

Lower urinary tract symptoms in Down syndrome 5
+ MODEL
disabilities and found that 35% of the participants hadvoiding disorder, and, of these, 38% had residual urinaryvolume and 11% had bacteriuria.
One bias of this study is that there were 10 individualsolder than 4 years of age (median age 4.6 � 1.0 years) whowere still not toilet trained, a fact that could be related toLUTS, and these individuals were not included in the study.However, no studies have shown at what age the individualswith DS acquire toilet training, and the DVSS is a ques-tionnaire for children who are not in diapers.
Although the guidelines for the clinical monitoring ofsubjects with DS that were developed by Bull [31] do notrecommend screening for routine urological abnormalitiesin newborns with DS and do not even mention urologicalscreening in any other age group, based on the lack ofstudies in the literature, we believe that this recommen-dation should be reconsidered given the high prevalence ofLUTS in individuals with DS. Therefore, an accurate inves-tigation during the clinical consultation should be stimu-lated to diagnose and prevent the consequences of LUTS,depicted mainly by urinary infections and injuries of theupper urinary tract.
Conclusions
There is a high prevalence of LUTS in younger males withDS, and the symptoms tend to improve as these individualsgrow older. LUTS are frequently associated with functionalconstipation in these individuals. These findings willcontribute to raising the awareness of professionalsinvolved in the follow-up of individuals with DS regardingthe clinical manifestations and the need for a standardizedinvestigation of LUTS.
Conflict of interest
None.
Funding
None.
Acknowledgments
We are grateful to all the participants for their dedicationand perseverance and the Ambulatory InterdisciplinaryTeam of Down Syndrome of the Department of Health ofChildren and Adolescents (Unified Health System e SUS-Brazil).
References
[1] Hulten MA, Patel SD, Westgren M, Papadogiannakis N,Jonsson AM, Jonasson J, et al. On the paternal origin of tri-somy 21 Down syndrome. Mol Cytogenet 2010;3:4.
[2] Perluigi M, Butterfield DA. Oxidative stress and Down syn-drome: a route toward Alzheimer-like dementia. Curr Ger-ontol Geriatr Res; 2012:10. Article ID 724904.
Please cite this article in press as: de Carvalho Mrad FC, et al., Prevsyndrome, Journal of Pediatric Urology (2014), http://dx.doi.org/10.1
[3] Gusman R, Campos C, Lopez-Fernandez E, Casado A. Bio-markers of age effect on renal function in Down syndrome.Biomarkers 2011;16(8):679e85.
[4] Weijerman ME, de Winter JP. Clinical practice. The care ofchildren with Down syndrome. Eur J Pediatr 2010;169:1445e52.
[5] Glasson EJ, Dye DE, Bittles AH. The triple challenges associatedwith age-related comorbidities in Down syndrome. J IntellectDisabil Res; 2013. http://dx.doi.org/10.1111/jir.12026.
[6] Van Gameren-Oosterom HB, Fekkes M, Buitendijk SE,Mohangoo JB, Bruil J, Van Wouwe JP. Development, problembehavior, and quality of life in a population based sample ofeight-year-old children with Down syndrome. PLoS One 2011;6:e21879.
[7] Ahmed S. Vesico-ureteric reflux in Down’s syndrome: poorprognosis. Aust N Z J Surg 1990;60:113e6.
[8] Ariel L, Wells TR, Landing BH, Singer DB. The urinary system inDown syndrome: a study of 124 autopsy cases. Pediatr Pathol1991;11:879e88.
[9] Handel LN, Barqawi A, Checa G, Furness III PD, Koyle MA.Males with Down’s syndrome and nonneurogenic neurogenicbladder. J Urol 2003;169:646e9.
[10] Ebert AK, Brookman-Amissah S, Rosch WH. Urological mani-festations of Down syndrome: significance and long-termcomplications e our own patient cohort with an overview.Urol A 2008;47:337e41.
[11] Mercer ES, Broecker B, Smith EA, Kirsch AJ, Scherz HC,Massad CA. Urological manifestations of Down syndrome. JUrol 2004;171:1250e3.
[12] Kupferman JC, Druschel CM, Kupchik GS. Increased preva-lence of renal and urinary tract anomalies in children withDown syndrome. Pediatrics 2009;124:615e21.
[13] Neveus T, Von Gontard A, Hoebeke P, Hjalmas K, Bauer S,Bower W, et al. The standardization of terminology of lowerurinary tract function in children and adolescents: report fromthe Standardisation Committee of the International Children’sContinence Society. J Urol 2006;176:314e24.
[14] Burguers RE, Mugie SM, Chase J, Cooper CS, Von Gontard A,Ritting CS, et al. Management of functional constipation inchildren with lower urinary tract symptoms: report from theStandardization Committee of the International Children’sContinence Society. J Urol 2013;190:29e36 [Review].
[15] Rihtman T, Tekuzener E, Parush S, Tenenbaum A, Bachrach SJ,Ornoy A. Are the cognitive functions of children with Downsyndrome related to their participation? Dev Med Child Neurol2010;52:72e8.
[16] Thibodeau BA, Metcalfe P, Koop P, Moore P. Urinary inconti-nence and quality of life in children. J Pediatr Urol 2013;9:78e93.
[17] Farhat W, Bagli DJ, Capolicchio G, O’Reilly S, Merguerian PA,Khoury A, et al. The dysfunctional voiding scoring system:quantitative standardization of dysfunctional voiding symp-toms in children. J Urol 2000;164:1011e5.
[18] Calado AA, Araujo EM, Barroso Jr U, Netto JM, Filho MZ,Macedo Jr A, et al. Cross-cultural adaptation of the dysfunc-tional voiding score symptom (DVSS) questionnaire for Bra-zilian children. Int Braz J Urol 2010;36:458e63.
[19] Rasquim A, Di Lorenzo C, Forbes D, Guiraldes E, Hyams JS,Staiano A, et al. Childhood functional gastrointestinal disor-ders: children/adolescents. Gastroenterology 2006;130:1527e37.
[20] Barroso Jr U, Tourinho R, Lordelo P, Hoebeke P, Chase J. Elec-trical stimulation for lower urinary tract dysfunction in chil-dren: a systematic review of the literature. Neurourol Urodyn2011;30:1429e36.
[21] Koenig JF, McKenna PH. Biofeedback therapy of dysfunctionalvoiding in children. Curr Urol Rep 2011;12:144e52 [Review].
alence of lower urinary tract symptoms in individuals with Down016/j.jpurol.2014.02.011
6 F.C. de Carvalho Mrad et al.
+ MODEL
[22] Vaz GT, Vasconcelos MM, Oliveira EA, Ferreira AL,Magalhaes PG, Silva FM, et al. Prevalence of lower urinarytract symptoms in school-age children. Pediatr Nephrol 2012;27:597e603.
[23] Burgu B, Aydogdu O, Gurkan K, Uslu R, Soygur T. Lower urinarytract conditions in children with attention deficit hyperac-tivity disorder: correlation of symptoms based on validatedscoring systems. J Urol 2011;185:663e8.
[24] Von Gontard A, Baeyens D, Van Hoecke E, Warzak WJ,Bachmann C. Psychological and psychiatric issues in urinaryand fecal incontinence. J Urol 2011;185:1432e6.
[25] Heron J, Joinson C, Croudace T, Von Gontard A. Trajectoriesof daytime wetting and soiling in a United Kingdom 4 to 9-year-old population birth cohort study. J Urol 2008;179:1970e5.
[26] Yang PY, Meng NH, Chou EC. Voiding dysfunctions in childrenwith mental retardation. Neurourol Urodyn 2010;29:1272e5.
Please cite this article in press as: de Carvalho Mrad FC, et al., Prevsyndrome, Journal of Pediatric Urology (2014), http://dx.doi.org/10.1
[27] American Psychiatric Association. Diagnostic and statisticalmanual of mental disorders. 4th ed. Washington DC: AmericanPsychiatric Association; 2000. text revision.
[28] Rutter M. World health Organization. Multiaxial classificationof child and adolescent psychiatric disorders: the ICD-10classification of mental and behavioural disorders in childrenand adolescents. Cambridge: Cambridge University Press;2008.
[29] Yang TK, Guo YJ, Chen SC, Chang HC, Yang HJ, Huang KH.Correlation between symptoms of voiding dysfunction andattention deficit disorder with hyperactivity in children withlower urinary tract symptoms. J Urol 2012;187:656e61.
[30] Burgers R, de Jong TP, Visser M, Di Lorenzo C, Dijkgraaf MG,Benninga MA. Functional defecation disorders in children withlower urinary tract symptoms. J Urol 2013;189:1886e91.
[31] Bull MJ, Committee on Genetics. Health supervision for chil-dren with Down syndrome. Pediatrics 2011;128:393e406.
alence of lower urinary tract symptoms in individuals with Down016/j.jpurol.2014.02.011