
Prevalence of Diagnosed Depression in Adolescents With History of Concussion
5
Original article Prevalence of Diagnosed Depression in Adolescents With History of Concussion Sara P. D. Chrisman, M.D., M.P.H. a, b, * , and Laura P. Richardson, M.D., M.P.H. a, b a Division of Adolescent Medicine, Department of Pediatrics, University of Washington, Seattle, Washington b Seattle Children’s Hospital, Center for Child Health Behavior and Development, Seattle, Washington Article history: Received June 25, 2013; Accepted October 8, 2013 Keywords: Adolescents; Concussion; Depression; Traumatic brain injury A B S T R A C T Purpose: Previous studies in adults have suggested concussion and other brain injury presents a risk factor for depression. The goal of our study was to analyze the association between previous concussion and current depression diagnosis in a large nationally representative adolescent data set. Methods: Retrospective cohort study using the National Survey of Children’s Health 2007e2008, a nationally representative survey conducted via random digit dialing. Data were obtained by parental report. We included youth 12e17 years old without a current concussion (N ¼ 36,060), and evaluated the association between previous concussion (binary) and current depression diagnosis (binary) using multiple logistic regression to control for age, sex, parental mental health, and socioeconomic status. Results: After controlling for age, sex, parental mental health, and socioeconomic status, history of concussion was associated with a 3.3-fold greater risk for depression diagnosis (95% CI: 2.0e5.5). Other factors significantly associated with depression diagnosis included poor or fair parental mental health (OR: 3.7, 95% CI: 2.8e4.9), and older age (15e17 years vs. 12e14 years, OR: 1.4, 95% CI: 1.1e1.8). Sex of the subject was not significantly related to depression diagnosis. Being above 200% of the poverty level was associated with approximately a 50% decreased risk of depression diagnosis (95% CI: 35%e70%). Conclusions: History of concussion was associated with a higher prevalence of diagnosed depression in a large nationally representative adolescent data set. Clinicians should screen for depression in their adolescent patients with concussion. Future studies should confirm this as- sociation using prospective methodology and examine potential treatment approaches. Ó 2014 Society for Adolescent Health and Medicine. All rights reserved. IMPLICATIONS AND CONTRIBUTION This is the first study to show a higher rate of depression diagnosis in a national sample of ado- lescents with concussion history. These data suggest clinicians should screen concussed youth for depression, so that they may effectively treat these individuals. Approximately 1.4 million traumatic brain injuries (TBI) occur annually; 75%e90% of these are mild TBI or concussion [1e3]. It was previously thought that youth recovered quickly from concussion, but new evidence suggests symptoms may persist for months or years, particularly after multiple concussions [4]. One of the most concerning symptoms is postconcussive depression. Depression during adolescence is associated with significant morbidity and mortality, including school failure [5], obesity [6], substance abuse [7], and suicide [8]. Data on postconcussive depression comes primarily from the adult literature. Increased diagnoses of depression were found in ex-NFL players with previous concussions, with an odds ratio of 1.5 after controlling for age, education, and substance abuse (18.5% vs. 13.4%, 95% CI 1.2e2.0) [9]. An additional study of ex- NFL players found those with two or more concussions had 1.5 times the risk for lifetime depression, while those with three or more had 3 times greater risk [10]. A study in a health mainte- nance organization in Seattle reported 2 times the risk for depression 2 years after a mild TBI [11]. * Address correspondence to: Sara P. D. Chrisman, M.D., M.P.H., Department of Anesthesiology and Pain Medicine, MB.11.500.3, Seattle Children’s Hospital, 4800 Sandpoint Way NE, Seattle, WA 98104. E-mail address: [email protected] (S.P.D. Chrisman). www.jahonline.org 1054-139X/$ e see front matter Ó 2014 Society for Adolescent Health and Medicine. All rights reserved. http://dx.doi.org/10.1016/j.jadohealth.2013.10.006 Journal of Adolescent Health 54 (2014) 582e586
Transcript of Prevalence of Diagnosed Depression in Adolescents With History of Concussion

Journal of Adolescent Health 54 (2014) 582e586
www.jahonline.org
Original article
Prevalence of Diagnosed Depression in Adolescents With History of Concussion
Sara P. D. Chrisman, M.D., M.P.H. a,b,*, and Laura P. Richardson, M.D., M.P.H. a,baDivision of Adolescent Medicine, Department of Pediatrics, University of Washington, Seattle, Washingtonb Seattle Children’s Hospital, Center for Child Health Behavior and Development, Seattle, Washington
Article history: Received June 25, 2013; Accepted October 8, 2013Keywords: Adolescents; Concussion; Depression; Traumatic brain injury
A B S T R A C TIMPLICATIONS AND
Purpose: Previous studies in adults have suggested concussion and other brain injury presents arisk factor for depression. The goal of our study was to analyze the association between previousconcussion and current depression diagnosis in a large nationally representative adolescentdata set.Methods: Retrospective cohort study using the National Survey of Children’s Health 2007e2008, anationally representative survey conducted via random digit dialing. Data were obtained byparental report. We included youth 12e17 years old without a current concussion (N ¼ 36,060),and evaluated the association between previous concussion (binary) and current depressiondiagnosis (binary) using multiple logistic regression to control for age, sex, parental mental health,and socioeconomic status.Results: After controlling for age, sex, parental mental health, and socioeconomic status, history ofconcussion was associated with a 3.3-fold greater risk for depression diagnosis (95% CI: 2.0e5.5).Other factors significantly associated with depression diagnosis included poor or fair parentalmental health (OR: 3.7, 95% CI: 2.8e4.9), and older age (15e17 years vs. 12e14 years, OR: 1.4, 95%CI: 1.1e1.8). Sex of the subject was not significantly related to depression diagnosis. Being above200% of the poverty level was associated with approximately a 50% decreased risk of depressiondiagnosis (95% CI: 35%e70%).Conclusions: History of concussion was associated with a higher prevalence of diagnoseddepression in a large nationally representative adolescent data set. Clinicians should screen fordepression in their adolescent patients with concussion. Future studies should confirm this as-sociation using prospective methodology and examine potential treatment approaches.
� 2014 Society for Adolescent Health and Medicine. All rights reserved.
* Address correspondence to: Sara P. D. Chrisman, M.D., M.P.H., Department ofAnesthesiology and Pain Medicine, MB.11.500.3, Seattle Children’s Hospital,4800 Sandpoint Way NE, Seattle, WA 98104.
E-mail address: [email protected] (S.P.D. Chrisman).
1054-139X/$ e see front matter � 2014 Society for Adolescent Health and Medicine. All rights reserved.http://dx.doi.org/10.1016/j.jadohealth.2013.10.006
CONTRIBUTION
This is the first study toshow a higher rate ofdepression diagnosis in anational sample of ado-lescents with concussionhistory. These data suggestclinicians should screenconcussed youth fordepression, so that theymay effectively treat theseindividuals.
Approximately 1.4 million traumatic brain injuries (TBI) occurannually; 75%e90% of these are mild TBI or concussion [1e3]. Itwas previously thought that youth recovered quickly fromconcussion, but new evidence suggests symptoms may persistfor months or years, particularly after multiple concussions [4].One of the most concerning symptoms is postconcussivedepression. Depression during adolescence is associated with
significant morbidity and mortality, including school failure [5],obesity [6], substance abuse [7], and suicide [8].
Data on postconcussive depression comes primarily from theadult literature. Increased diagnoses of depressionwere found inex-NFL players with previous concussions, with an odds ratio of1.5 after controlling for age, education, and substance abuse(18.5% vs. 13.4%, 95% CI 1.2e2.0) [9]. An additional study of ex-NFL players found those with two or more concussions had 1.5times the risk for lifetime depression, while those with three ormore had 3 times greater risk [10]. A study in a health mainte-nance organization in Seattle reported 2 times the risk fordepression 2 years after a mild TBI [11].

S.P.D. Chrisman and L.P. Richardson / Journal of Adolescent Health 54 (2014) 582e586 583
Data from youth with mild TBI are more limited. One study ofa clinical population found an 11% incidence of novel depressionin youth 6 months following mild TBI, but these were only insubjects with abnormal brain imaging [12]. Studies of depressionfollowingmild TBI are complicated by the fact that risk factors formild TBI (such as low socioeconomic status or family history ofmental health issues) are also associated with depression. Tomore clearly understand the risk for depression following mildTBI requires a comparative population and adequate measure-ment of potential confounding factors. One study of youth in ahealth maintenance organization in Seattle found twice the riskfor depression following mild TBI after controlling for potentialconfounding, but only for youth without previous psychiatricissues [13]. Another study in the same organization found a 1.7-fold greater risk of depression for youth following any TBI [14].The one prospective study of depression and TBI in youth [15]found similar amounts of depressive symptoms when com-paring youth with Mild I TBI (no intracranial hemorrhage) toarm-injured controls 2 years after injury, but 5% of the Mild I TBIpatients were diagnosed with major depressive disordercompared with 0% of arm-injured controls.
In 2009, the Washington State Legislature passed the LystedtLaw [16], requiring all athletes to be evaluated by a clinician ifsuspected of having a concussion. This and similar laws havecaused an influx of concussed patients into primary care offices[17]. The goal of our study was to examine prevalence of diag-nosed depression in youth with a history of concussion using anationally representative sample that would allow us to controlfor potential confounding. If concussion is associated with asignificant increased risk of depression, clinicians shouldmonitor more carefully for the development of depression whenmanaging concussed youth.
Methods
Data source
The National Survey of Children’s Health 2007 [18] is a tele-phone survey of parents administrated by theMaternal and ChildHealth Bureau, U.S. Department of Health and Human Services.The survey was conducted in several waves, and we used datafrom the 2007e2008 survey only. Phone numbers were selectedby random digit dialing to identify households with one or morechildren under 18 years old, and one of those children wasrandomly selected to be discussed. If respondents reported nochildren under 18 years old lived in the household, the interviewwas stopped. The interview was conducted with the parent orcaregiver, and interviews were completed in 66% of householdsidentified with children, for a total of 91,642 surveys. Surveyswere conducted in English and Spanish. The surveywas designedto collect a nationally representative sample of the noninstitu-tionalized population aged 0e17 years, with at least 1,700 sur-veys per state. A wide range of topics were covered including (1)medical insurance coverage; (2) child and family demographics;(3) parental physical and mental health; (4) child physical andmental health; (5) school performance; and (6) neighborhooddescription.
Variables
The primary outcome was a current diagnosis of depression.Parents were asked whether their child had ever been diagnosed
with depression by a clinician, and were prompted with thisinformation: “Depression is an illness that involves the body,mood, and thoughts. It is marked by persistent sadness or ananxious or empty mood. It affects how a person feels, and theway a person eats, sleeps, and functions.” Parents were thenasked whether their child suffered depression currently or onlyin the past, and the outcome we chose was “current” depression.Subjects with previous depression diagnosis were included inthe sample as not having current depression. Our predictor ofinterest was history of brain injury or concussion. Parents wereasked whether their child had ever been diagnosed with a braininjury or concussion, and were prompted with this information:“A concussion is an injury of the brain that causes a briefdisruption in brain function. Brain tumors should not beconsidered brain injuries.” Parents were then asked whether thebrain injury was current or in the past, and we only includedsubjects with previous brain injury. For simplicity in this study,we use the term “concussion” to describe these injuries ratherthan “concussion or other brain injury” as the question specif-ically mentioned concussion. Data suggest that the preponder-ance of brain injuries suffered by youth are mild brain injuries, orconcussions [19].
Potential confounders of the relationship between previousconcussion and current depression were selected based onliterature review, and included age [20], sex [21], parental mentalhealth [22,23], and poverty level [24]. We generated a binary agevariable (15e17 years old vs. 12e14 years old), and a binaryparental mental health variable (poor or fair vs. excellent, verygood, or good). Sex (female vs. male) was available in the data setand poverty level (�100%, >100% to �200%, >200% to �400%,>400%) was constructed by the staff at the National Survey ofChildren’s Health using annual household income and the totalnumber of persons living in the household, with the 2007Department of Health and Human Services poverty thresholdguidelines as a reference. Either annual income or number ofpersons in the household was missing for>10% of the subjects inthe data set, and thus multiply imputed data constructed by theresearchers at the National Survey for Children’s Health wereused for analysis [25]. These data contained five imputations foreach subject.
Sample
For this study we examined only 12e17-year-olds, becausethis was our population of interest.
Analysis
We modeled the unadjusted relationship between theprimary predictor (previous concussion) and current depres-sion (binary variable, yes/no) using logistic regression togenerate odds ratios and 95% confidence intervals. We alsogenerated individual logistic regression models to assess thestrength of the relationship between each potentialconfounder (age, sex, parental mental health, and povertylevel) and current depression. We then created a multivariatelogistic regression model to calculate adjusted odds ratios and95% confidence intervals for the relationship between thepredictor of interest (previous concussion) and the outcome(current depression diagnosis), while controlling for potentialconfounders. We chose the potential confounders a prioribased on previous literature, and thus they were retained in
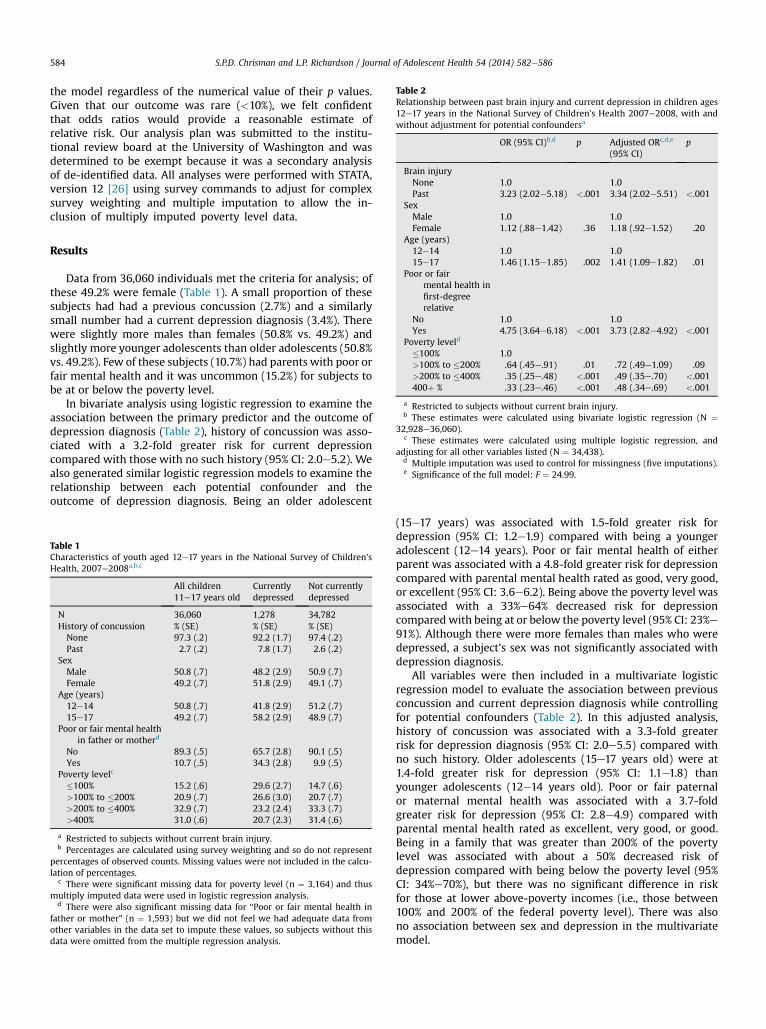
Table 2Relationship between past brain injury and current depression in children ages12e17 years in the National Survey of Children’s Health 2007e2008, with andwithout adjustment for potential confoundersa
OR (95% CI)b,d p Adjusted ORc,d,e
(95% CI)p
Brain injuryNone 1.0 1.0Past 3.23 (2.02e5.18) <.001 3.34 (2.02e5.51) <.001
SexMale 1.0 1.0
S.P.D. Chrisman and L.P. Richardson / Journal of Adolescent Health 54 (2014) 582e586584
the model regardless of the numerical value of their p values.Given that our outcome was rare (<10%), we felt confidentthat odds ratios would provide a reasonable estimate ofrelative risk. Our analysis plan was submitted to the institu-tional review board at the University of Washington and wasdetermined to be exempt because it was a secondary analysisof de-identified data. All analyses were performed with STATA,version 12 [26] using survey commands to adjust for complexsurvey weighting and multiple imputation to allow the in-clusion of multiply imputed poverty level data.
Female 1.12 (.88e1.42) .36 1.18 (.92e1.52) .20Age (years)12e14 1.0 1.015e17 1.46 (1.15e1.85) .002 1.41 (1.09e1.82) .01
Poor or fairmental health infirst-degreerelative
No 1.0 1.0Yes 4.75 (3.64e6.18) <.001 3.73 (2.82e4.92) <.001
Poverty leveld
�100% 1.0>100% to �200% .64 (.45e.91) .01 .72 (.49e1.09) .09>200% to �400% .35 (.25e.48) <.001 .49 (.35e.70) <.001400þ % .33 (.23e.46) <.001 .48 (.34e.69) <.001
a Restricted to subjects without current brain injury.b These estimates were calculated using bivariate logistic regression (N ¼
32,928e36,060).c These estimates were calculated using multiple logistic regression, and
adjusting for all other variables listed (N ¼ 34,438).d Multiple imputation was used to control for missingness (five imputations).e Significance of the full model: F ¼ 24.99.
Results
Data from 36,060 individuals met the criteria for analysis; ofthese 49.2% were female (Table 1). A small proportion of thesesubjects had had a previous concussion (2.7%) and a similarlysmall number had a current depression diagnosis (3.4%). Therewere slightly more males than females (50.8% vs. 49.2%) andslightly more younger adolescents than older adolescents (50.8%vs. 49.2%). Few of these subjects (10.7%) had parents with poor orfair mental health and it was uncommon (15.2%) for subjects tobe at or below the poverty level.
In bivariate analysis using logistic regression to examine theassociation between the primary predictor and the outcome ofdepression diagnosis (Table 2), history of concussion was asso-ciated with a 3.2-fold greater risk for current depressioncompared with those with no such history (95% CI: 2.0e5.2). Wealso generated similar logistic regression models to examine therelationship between each potential confounder and theoutcome of depression diagnosis. Being an older adolescent
Table 1Characteristics of youth aged 12e17 years in the National Survey of Children’sHealth, 2007e2008a,b,c
All children11e17 years old
Currentlydepressed
Not currentlydepressed
N 36,060 1,278 34,782History of concussion % (SE) % (SE) % (SE)None 97.3 (.2) 92.2 (1.7) 97.4 (.2)Past 2.7 (.2) 7.8 (1.7) 2.6 (.2)
SexMale 50.8 (.7) 48.2 (2.9) 50.9 (.7)Female 49.2 (.7) 51.8 (2.9) 49.1 (.7)
Age (years)12e14 50.8 (.7) 41.8 (2.9) 51.2 (.7)15e17 49.2 (.7) 58.2 (2.9) 48.9 (.7)
Poor or fair mental healthin father or motherd
No 89.3 (.5) 65.7 (2.8) 90.1 (.5)Yes 10.7 (.5) 34.3 (2.8) 9.9 (.5)
Poverty levelc
�100% 15.2 (.6) 29.6 (2.7) 14.7 (.6)>100% to �200% 20.9 (.7) 26.6 (3.0) 20.7 (.7)>200% to �400% 32.9 (.7) 23.2 (2.4) 33.3 (.7)>400% 31.0 (.6) 20.7 (2.3) 31.4 (.6)
a Restricted to subjects without current brain injury.b Percentages are calculated using survey weighting and so do not represent
percentages of observed counts. Missing values were not included in the calcu-lation of percentages.
c There were significant missing data for poverty level (n ¼ 3,164) and thusmultiply imputed data were used in logistic regression analysis.
d There were also significant missing data for “Poor or fair mental health infather or mother” (n ¼ 1,593) but we did not feel we had adequate data fromother variables in the data set to impute these values, so subjects without thisdata were omitted from the multiple regression analysis.
(15e17 years) was associated with 1.5-fold greater risk fordepression (95% CI: 1.2e1.9) compared with being a youngeradolescent (12e14 years). Poor or fair mental health of eitherparent was associated with a 4.8-fold greater risk for depressioncompared with parental mental health rated as good, very good,or excellent (95% CI: 3.6e6.2). Being above the poverty level wasassociated with a 33%e64% decreased risk for depressioncompared with being at or below the poverty level (95% CI: 23%e91%). Although there were more females than males who weredepressed, a subject’s sex was not significantly associated withdepression diagnosis.
All variables were then included in a multivariate logisticregression model to evaluate the association between previousconcussion and current depression diagnosis while controllingfor potential confounders (Table 2). In this adjusted analysis,history of concussion was associated with a 3.3-fold greaterrisk for depression diagnosis (95% CI: 2.0e5.5) compared withno such history. Older adolescents (15e17 years old) were at1.4-fold greater risk for depression (95% CI: 1.1e1.8) thanyounger adolescents (12e14 years old). Poor or fair paternalor maternal mental health was associated with a 3.7-foldgreater risk for depression (95% CI: 2.8e4.9) compared withparental mental health rated as excellent, very good, or good.Being in a family that was greater than 200% of the povertylevel was associated with about a 50% decreased risk ofdepression compared with being below the poverty level (95%CI: 34%e70%), but there was no significant difference in riskfor those at lower above-poverty incomes (i.e., those between100% and 200% of the federal poverty level). There was alsono association between sex and depression in the multivariatemodel.

S.P.D. Chrisman and L.P. Richardson / Journal of Adolescent Health 54 (2014) 582e586 585
Discussion
In this secondary analysis of data from the National Surveyof Children’s Health we found that history of concussion wasassociatedwith greater than a 3-fold risk of a current diagnosis ofdepression, even after controlling for age, sex, parental mentalhealth, and socioeconomic status. This study adds to the evi-dence for an association between concussion and depression[9e15] and is the first study to find such an association in a largenationally representative data set. Although there was little in-formation about timing of the depression diagnosis in this sur-vey, making it difficult to draw conclusions regarding causality, itis suggestive of a need to more closely monitor this populationfor depression.
We found a much stronger association between brain injuryand depression than a previous study byMassagli and colleagues[13]. Massagli and colleagues utilized an administrative data setrather than parental report, and thus there were significant dif-ferences in themanner inwhich our two studies defined both theexposure (concussion) and the outcome (depression diagnosis).Using ICD-9 codes for concussion or brain injury most likelyproduces an underestimate of the true brain-injured population,given that previous studies have shown that most youth withmild brain injury do not present to clinical care [19]. Massagli andcolleagues also reported only on depression diagnoses from ICD-9 codes, and prior research has shown that pediatricians often donot code for depression or mental health conditions [27]. Thus,parental report may identify additional depressed youth whowere diagnosed with depression, but for whom no visit code fordepression was used.
In a prospective evaluation of depression following TBI ofvarying severity, O’Connor and colleagues [15] found that theirmost mildly injured patients (brain injury symptoms withnormal imaging) had no significant differences in depressivesymptoms at 3,12, or 24months comparedwith injured controls,but did have a numerically increased rate of depression diagnosis(5% vs. 0%). Although these results are in a similar direction toour findings, no statistical testing was conducted to evaluate thesignificance of this difference.
There are many potential explanations for this observed as-sociation between concussion and depression. It is possible thisassociation is due to diagnostic bias, or in other words concus-sion may lead to increased physician visits because so few ado-lescents visit physicians [28] and this could cause increaseddiagnosis of depression. It is also possible that both depressionand concussion occur secondary to confounding factors we wereunable to control for in this analysis [29]. It could also be true thatthis association actually represents diagnostic confusion,because many of the symptoms of concussion (sleep difficulties,irritability, and fatigue) are also symptoms of depression. Somehave even suggested that symptoms of concussion (such as sleepdisruption) may lead to depression, and a recent study found anassociation between sleep difficulties and depressive symptomseven a year after brain injury [30,31].
It is important to point out that these data were collected in amanner that limits our ability to draw conclusions regarding thedirection of the association between concussion and depression,and more work is needed to validate this association with pro-spective methodology. However, at minimum, this findingmeritsadditional screening in the concussed adolescent population andfurther discussion regarding concussion management. Currentconcussion consensus guidelines [32] recommend that “in the
early stages of concussion, youth should not engage in physical orcognitive activities that result in an increase in symptoms.” Un-fortunately, many clinicians have interpreted this statement tomean that return to activity should not begin until symptomshave completely resolved. Such relative social isolation [33] andincrease in sedentary behavior [34] can lead to depressivesymptoms. A recent article found little data supporting rest as atreatment for prolonged concussive symptoms [35] and specif-ically stated that if “normal activities are restricted for extendedperiods of time, they [youth] are at risk for secondary problemssuch as physical deconditioning, anxiety and stress, milddepression, and irritability.”
The approach of waiting until symptoms resolve to beginreturn to physical activity is more conservative than the treat-ment used for patients with more severe traumatic brain injury(TBI), where patients are entered into physical rehabilitationprograms because of brain-injured symptoms, not despite them.New data suggests patients with severe TBI who receive earlierintervention fare even better than those for whom rehabilitationis delayed [36]. A recent review [37] framed this well: “In med-icine, rest is often prescribed by default when the presentingcondition is poorly understood.” As we learn more aboutconcussive injury, we are finding that although some rest is good,too much rest may be detrimental. A few studies suggest thatphysical activity interventions for concussion, where youth areslowly returned to activity even while symptomatic, may bemore effective than rest [35,37].
One of the advantages of our study was the use of a largenationally representative data set, which allowed us greaterpower to detect differences and better representation of thegeneral population. This data set also contained detailed infor-mation about socioeconomic status and parental mental health,which provided us a means to examine the association betweenbrain injury and depression diagnosis while minimizing thesepotential confounders. Previous studies such as those by Mas-sagli and colleagues [13] and O’Connor and colleagues [15] wereundertaken using clinical samples or administrative data sets,both of which contain bias. Patients are only included in thosesamples if they seek care, and many patients with concussion ordepression do not seek care.
One of the main weaknesses of the present study is that itrelied on retrospective parent report. There is always concernregarding memory bias in retrospective studies, but in additionto those concerns we have added the complexity of determiningthe exposure and the outcome simultaneously. We haveattempted tominimize these issues by examining the associationbetween “previous” concussion and “current” depression, but itis still possible that the association we describe is due to reversecausality. In other words, we cannot rule out the possibility thatsome of these youth were depressed before their concussion.However, if there is an increased prevalence of depression in thepopulation of youth who have suffered a concussion comparedwith those who have never had a concussion, this still suggests aneed for enhanced screening in this population. It is expectedthat diagnosed depression would underestimate true depressionin this population, but this should only decrease our associationrather than generate a spurious association.
Asking parents about a diagnosis of “concussion or other braininjury” is also likely to generate an underestimate of true injury,because parents may not know about mild brain injury, and/ormild brain injuries may go undiagnosed [19]. To place this incontext, a recent survey that utilized youth self-report of brain

S.P.D. Chrisman and L.P. Richardson / Journal of Adolescent Health 54 (2014) 582e586586
injured symptoms after head impact, suggested a prevalence of20.2% for brain injury [38]. It is not surprising that the numbers inour studywould be somuch less, given thatweare both relyingonparental report and asking only about diagnosed concussion.
An additional limitation of this study was that data were notavailable regarding timing of when the concussions occurred.Very different factors would be suspected to explain this asso-ciation if depression occurred soon after the concussive injuryrather than later on. Perhaps in future editions of the NationalSurvey of Children’s Health the authors will consider askingabout timing of the diagnoses they discuss; this could proveuseful for many purposes beyond this study. Future studies willneed to address this issue of prospective data.
In summary, this study adds to the evidence that there is anassociation between depression and concussion in youth. Clini-cians caring for youth with concussion should be aware of thisassociation and should screen youth for depressive symptoms.More work is needed using prospective studies with youth tounderstand the pathways that mediate this association and toexplore treatment possibilities.
Funding Sources
This research was supported by a National Institutes of HealthLoan Repayment Grant.
References
[1] Centers for Disease Control and Prevention (CDC). Nonfatal traumatic braininjuries from sports and recreation activitiesdUnited States, 2001e2005.MMWR Morb Mortal Wkly Rep 2007;56:733e7.
[2] Langlois JA, Rutland-Brown W, Wald MM. The epidemiology and impact oftraumatic brain injury: A brief overview. J Head Trauma Rehabil 2006;21:375e8.
[3] Thurman DJ, Branche CM, Sniezek JE. The epidemiology of sports-relatedtraumatic brain injuries in the United States: Recent developments.J Head Trauma Rehabil 1998;13:1e8.
[4] Meares S, Shores EA, Taylor AJ, et al. Mild traumatic brain injury does notpredict acute postconcussion syndrome. J Neurol Neurosurg Psychiatry2008;79:300e6.
[5] Fletcher JM. Adolescent depression: Diagnosis, treatment, and educationalattainment. Health Econ 2008;17:1215e35.
[6] Richardson LP, Davis R, Poulton R, et al. A longitudinal evaluation ofadolescent depression and adult obesity. Arch Pediatr Adolesc Med 2003;157:739e45.
[7] Saluja G, Iachan R, Scheidt PC, et al. Prevalence of and risk factors fordepressive symptoms among young adolescents. Arch Pediatr Adolesc Med2004;158:760e5.
[8] Lewinsohn PM, Hops H, Roberts RE, et al. Adolescent psychopathology: I.Prevalence and incidence of depression and other DSM-III-R disorders inhigh school students. J Abnorm Psychol 1993;102:133e44.
[9] Holsinger T, Steffens DC, Phillips C, et al. Head injury in early adulthood andthe lifetime risk of depression. Arch Gen Psychiatry 2002;59:17e22.
[10] Guskiewicz KM, Marshall SW, Bailes J, et al. Recurrent concussion and riskof depression in retired professional football players. Med Sci Sports Exerc2007;39:903e9.
[11] Fann JR, Burlington B, Leonetti A, et al. Psychiatric illness following trau-matic brain injury in an adult health maintenance organization population.Arch Gen Psychiatry 2004;61:53e61.
[12] Max JE, Keatley E, Wilde EA, et al. Depression in children and adolescentsin the first 6 months after traumatic brain injury. Int J Dev Neurosci 2012;30:239e45.
[13] Massagli TL, Fann JR, Burington BE, et al. Psychiatric illness after mild trau-matic brain injury in children. Arch Phys Med Rehabil 2004;85:1428e34.
[14] Zatzick DF, Grossman DC. Association between traumatic injury and psy-chiatric disorders and medication prescription to youths aged 10e19.Psychiatr Serv 2011;62:264e71.
[15] O’Connor SS, Zatzick DF, Wang J, et al. Association between posttraumaticstress, depression, and functional impairments in adolescents 24 monthsafter traumatic brain injury. J Trauma Stress 2012;25:264e71.
[16] Chopp F, Owen B, Gregoire C. Youth sportsdhead injury policies.Engrossed House bill 1824. Available at: https://docs.google.com/viewer?url¼http%3A%2F%2Fapps.leg.wa.gov%2Fdocuments%2Fbilldocs%2F2009-10%2FPdf%2FBills%2FHouse%2520Bills%2F1824.E.pdf.
[17] Bakhos LL, Lockhart GR, Myers R, Linakis JG. Emergency department visitsfor concussion in young child athletes. Pediatrics 2010;126:e550e6. http://dx.doi.org/10.1542/peds.2009-3101.
[18] Child and Adolescent Health Measurement Initiative (CAHMI), 2007,National Survey of Children’s Health Indicator Data Set, Data ResourceCenter for Child and Adolescent Health, Available at: www.childhealthdata.org.
[19] Centers for Disease Control and Prevention (CDC). Report to Congress onmild traumatic brain injury in the United States: Steps to prevent a seriouspublic health problem. Available at: www.cdc.gov/ncipc/pub-res/mtbi/mtbireport.pdf.
[20] Birmaher B, Brent DA, Benson RS. Summary of the practice parameters forthe assessment and treatment of children and adolescents with depressivedisorders. American Academy of Child and Adolescent Psychiatry. J AmAcad Child Adolesc Psychiatry 1998;37:1234e8.
[21] Mc Guinness TM, Dyer JG, Wade EH. Gender differences inadolescent depression. J Psychosoc Nurs Ment Health Serv 2012;50:17e20.
[22] Gureje O, Oladeji B, Hwang I, et al. Parental psychopathology and the riskof suicidal behavior in their offspring: Results from the World MentalHealth surveys. Mol Psychiatry 2011;16:1221e33. http://dx.doi.org/10.1038/mp.2010.111.
[23] Hirshfeld-Becker DR, Micco JA, Henin A, et al. Psychopathology in adoles-cent offspring of parents with panic disorder, major depression, or both: A10-year follow-up. Am J Psychiatry 2012;169:1175e84.
[24] McLaughlin KA, Costello EJ, Leblanc W, et al. Socioeconomic status andadolescent mental disorders. Am J Public Health 2012;102:1742e50.http://dx.doi.org/10.2105/AJPH.2011.300477.
[25] Blumberg SJ, Foster EB, Frasier AM, et al. Design and operation of the Na-tional Survey of Children’s Health, 2007. Vital Health Stat 2012;1:1e149.
[26] StataCorp. Stata statistical software: Release 12. College Station, TX:Author; 2011.
[27] Rushton JL, Felt BT, Roberts MW. Coding of pediatric behavioral and mentaldisorders. Pediatrics 2002;110(1 Pt 1):e8.
[28] Nordin JD, Solberg LI, Parker ED. Adolescent primary care visit patterns.Ann Fam Med 2010;8:511e6. http://dx.doi.org/10.1370/afm.1188.
[29] Fewell Z, Davey Smith G, Sterne JA. The impact of residual and unmeasuredconfounding in epidemiologic studies: A simulation study. Am J Epidemiol2007;166:646e55.
[30] Fogelberg DJ, Hoffman JM, Dikmen S, et al. Association of sleep and co-occurring psychological conditions at 1 year after traumatic brain injury.Arch Phys Med Rehabil 2012;93:1313e8.
[31] Krystal AD. Psychiatric disorders and sleep. Neurol Clin 2012;30:1389e413.
[32] Harmon KG, Drezner JA, Gammons M, et al. American medical Society forsports medicine position statement: Concussion in sport. Br J Sports Med2013;47:15e26.
[33] Witvliet M, Brendgen M, van Lier PA, et al. Early adolescent depressivesymptoms: Prediction from clique isolation, loneliness, and perceived so-cial acceptance. J Abnorm Child Psychol 2010;38:1045e56. http://dx.doi.org/10.1007/s10802-010-9426-x.
[34] Teychenne M, Ball K, Salmon J. Sedentary behavior and depression amongadults: A review. Int J Behav Med 2010;17:246e54. http://dx.doi.org/10.1007/s12529-010-9075-z.
[35] Schneider KJ, Iverson GL, Emery CA, et al. The effects of rest and treatmentfollowing sport-related concussion: A systematic review of the literature.Br J Sports Med 2013;47:304e7. http://dx.doi.org/10.1136/bjsports-2013-092190.
[36] Andelic N, Bautz-Holter E, Ronning P, et al. Does an early onset andcontinuous chain of rehabilitation improve the long-term functionaloutcome of patients with severe traumatic brain injury? J Neurotrauma2012;29:66e74. http://dx.doi.org/10.1089/neu.2011.1811.
[37] Silverberg ND, Iverson GL. Is rest after concussion “the best medicine?”:Recommendations for activity resumption following concussion in ath-letes, civilians, and military service members. J Head Trauma Rehabil 2013;28:250e9. http://dx.doi.org/10.1097/HTR.0b013e31825ad658.
[38] Ilie G, Boak A, Adlaf EM, et al. Prevalence and correlates of traumatic braininjuries among adolescents. JAMA 2013;309:2550e2. http://dx.doi.org/10.1001/jama.2013.6750.


















