
PRETERM BIRTH AND ABORTION Mary L Davenport, MD, FACOG Magnificat Maternal Health Program July...
51
PRETERM BIRTH AND ABORTION Mary L Davenport, MD, FACOG Magnificat Maternal Health Program July 31-August 3, 2013 Medical Women’s International Association Seoul, Korea
-
Upload
jason-hines -
Category
Documents
-
view
215 -
download
1
Transcript of PRETERM BIRTH AND ABORTION Mary L Davenport, MD, FACOG Magnificat Maternal Health Program July...

PRETERM BIRTH AND ABORTION
Mary L Davenport, MD, FACOGMagnificat Maternal Health Program July 31-August 3, 2013 Medical Women’s International Association Seoul, Korea © 2013

Disclosure
There are no commercial products mentioned in this lecture nor is support being supplied by any vendor, agency, or governmental grant or agent.
Preterm Birth and Abortion• Introduction▫Frequency of preterm birth▫Risk factors▫Biological pathways
•Studies on preterm birth and abortion▫Meta-analyses▫Recent studies▫Medical vs surgical abortion
•Conclusion

Preterm Birth: World-wide•15,000,000 preterm births annually world-wide; one in
10 world-wide• Leading cause of newborn death•Second cause of death (after pneumonia) of children
under 5•Fourth Millennium Goal: reducing mortality rate in
children under 5 by two thirds between 1990 and 2015; preterm birth is a big factor
•Assessing gestational age in low-resource settings difficult; low birth weight used as proxy
Back S et al. Bull World Health Organ, 2010

Preterm Birth: under 37 weeks
•Extremely preterm < 28 weeks•Very preterm 28-32 weeks•Moderate to late preterm 32 to <37
weeks



60% of preterm births occur in Sub-Saharan Africa and Southern Asia
Nour N. “Preterm delivery and the MDG.” Rev Obstet Gynecol, 2012.
South Africa
More than eight out of ten births are preterm – less than 37 weeks.
WHO 2012, The Global Action Report on Preterm Birth
Preterm Birth: High vs Low Income Nations
•High income nations▫50% of 24 week babies survive▫90% of <28 week babies survive
• Low resource nations▫50 % survival does not occur until 32 weeks▫90% of <28 babies die within a few days
Nour N. “Preterm delivery and the MDG.” Rev Obstet Gynecol, 2012.

In the USA we have come a long way….
Patrick Bouvier KennedyAugust 7-9, 1963
• Born by cesarean section at 34 ½ weeks gestation
• 2.11 Kg (4 lb10 ½ oz)• Died of hyaline membrane
disease• Accelerated research in
surfactant, CPAP, respiratory therapies
• 2013: Survival nearly 100% at 32 weeks gestation

Preterm Birth: USA•210,000 births annually•12% of all births are preterm•2% are Very Preterm Births (<32 weeks) ▫Leading cause of neonatal death▫At risk for lifelong respiratory, visual, cognitive complications
•Preterm birth has risen 20 % in past two decades•Estimated annual cost $26 Billion•Average cost $51,600 per infantMarch of Dimes, Peristats.Hamilton B et al. CDC Vital Statistics Reports, 2012. Behrman,E et al. Preterm Birth: Consequence, Causes and Prevention. 2007

Kangaroo Care
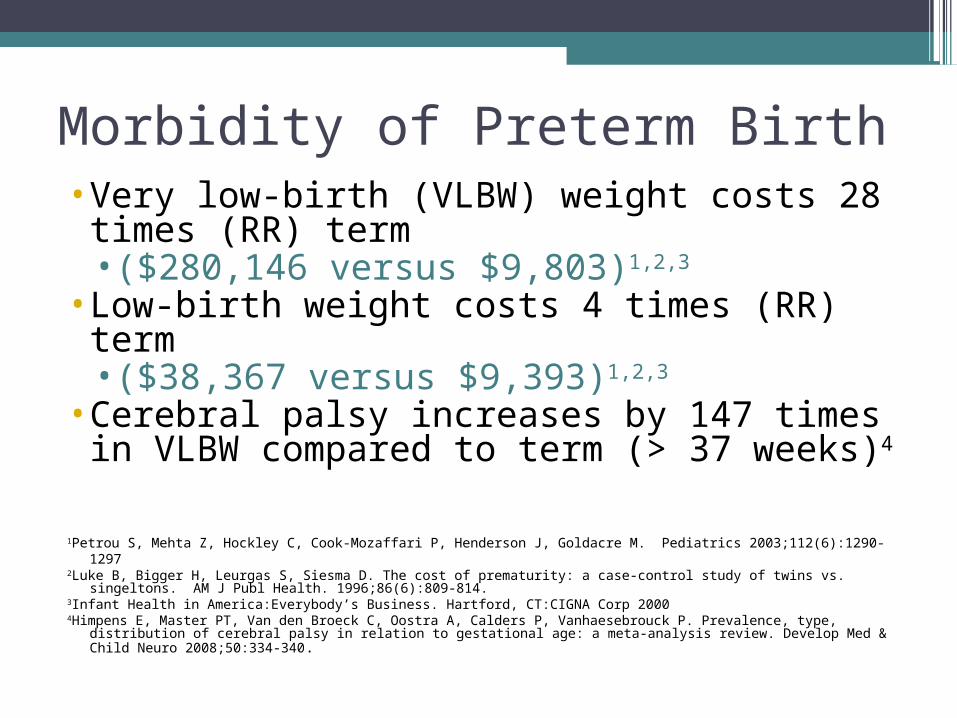
Morbidity of Preterm Birth• Very low-birth (VLBW) weight costs 28 times
(RR) term•($280,146 versus $9,803)1,2,3
• Low-birth weight costs 4 times (RR) term•($38,367 versus $9,393)1,2,3
• Cerebral palsy increases by 147 times in VLBW compared to term (> 37 weeks)4
1Petrou S, Mehta Z, Hockley C, Cook-Mozaffari P, Henderson J, Goldacre M. Pediatrics 2003;112(6):1290-12972Luke B, Bigger H, Leurgas S, Siesma D. The cost of prematurity: a case-control study of twins vs. singeltons. AM J Publ Health.
1996;86(6):809-814.3Infant Health in America:Everybody’s Business. Hartford, CT:CIGNA Corp 20004Himpens E, Master PT, Van den Broeck C, Oostra A, Calders P, Vanhaesebrouck P. Prevalence, type, distribution of cerebral
palsy in relation to gestational age: a meta-analysis review. Develop Med & Child Neuro 2008;50:334-340 .
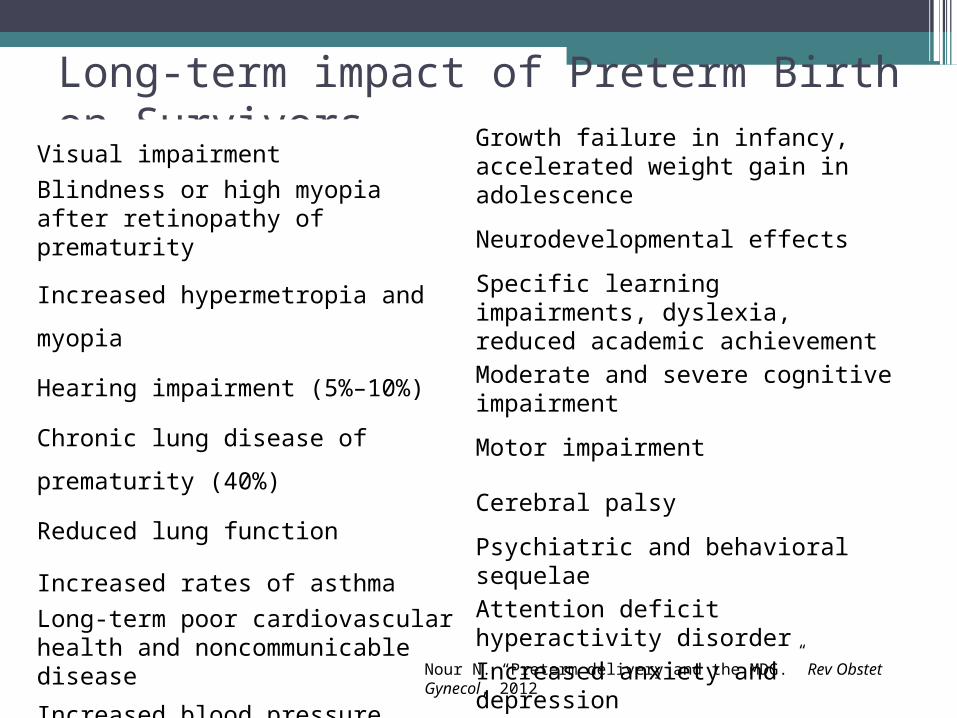
Long-term impact of Preterm Birth on SurvivorsVisual impairment
Blindness or high myopia after retinopathy of prematurity
Increased hypermetropia and myopia
Hearing impairment (5%–10%)
Chronic lung disease of prematurity (40%)
Reduced lung function
Increased rates of asthma
Long-term poor cardiovascular health and noncommunicable disease
Increased blood pressure, diabetes, pre-eclampsia
Growth failure in infancy, accelerated weight gain in adolescence
Neurodevelopmental effects
Specific learning impairments, dyslexia, reduced academic achievement
Moderate and severe cognitive impairment
Motor impairment
Cerebral palsy
Psychiatric and behavioral sequelae
Attention deficit hyperactivity disorder
Increased anxiety and depression
Nour N. “Preterm delivery and the MDG.” Rev Obstet Gynecol, 2012

Risk factors for preterm birth• Previous preterm delivery• Uterine distension• Cervical trauma• Infection• Placental issues• Abdominal surgery during
pregnancy• Fetal anomaly• Chronic diseases • Demographic: maternal age (<
18 or > 40 ), black race, genotype
• Low interconceptional interval
• Social: nutrition, smoking, substance abuse
• Psychosocial: anxiety, depression, stress
• Occupational: physical exertion, standingnet
• Genetic
•Abortion???
Robinson J et al. “Risk factors for preterm birth,” UptoDate. 2012

WHO: “Born Too Soon”, 2012
• WHO “The Global Action Report on Preterm Birth report on PTB” in 2012
• No mention of abortion as a risk factor on page 20 of report.
• In fact, no mention of abortion at all as a PTB risk factor in the world or as an explanation for rising PTB rates
WHO 2012, “The Global Action Report on Preterm Birth”, p 20.

Preterm labor: biological pathways
QUIESENCE•Progesterone, prostacyclin (PGI2), nitric oxide, relaxin, and parathyroid hormone-related peptide contractions•These substances increase cAMP•Inhibit release of calcium from intracellular stores•Inhibit MLKC
ACTIVATION•Increased levels of CAP’s (contraction-associated proteins); cytokines;•Activated by myometrial stretch •Leads to activation of CRH (corticotropin-releasing hormone) and withdrawal of progesterone•Increased levels of prostaglandins
Behrman,E et al. Preterm Birth: Consequence, Causes and Prevention. National Academies Press, 2007
Biological pathways to preterm birth: Inflammation•Gene-environment interactions may be responsible for pathology;
genetic polymorphisms may play a role in inducing a harmful inflammatory response
•Caucasians: Factor V Leiden (FVL) was significantly associated with PTB (OR 2.6, 95% CI 1.31-5.17)
•African-Americans: significant associations with polymorphisms in the maternal interleukin IL-12 gene and the fetal IL-2RB receptor
Holst D et al. Eur J Obstet Gynecol Reprod Biol. 2008Velez DR et al. PLoS One. 2008Velez DR et al. Am J Obstet Gynecol. 2009.
ACOG, WHO and the medical community have disregarded the link between abortion and preterm birth.
•135 studies* have demonstrated an association between abortion and preterm birth
•No studies show lower rate of preterm birth after abortion•Studies from diverse locations world-wide•Most pronounced association with very preterm birth and
multiple abortion•Some ethnic groups are disproportionately impacted:
Africans and African Americans
*as of February,2013

Meta-analysis by Shah, et al 2009 •Screened 834 papers•Excluded 765 for lack of data and
objectivity; retrieved 69 citations•37 included studies
•18 studies with Low Birth Weight (LBW)•22 studies for preterm birth (PTB)•3 studies for small for gestational age
(SGA)

Meta-analysis by Shah, et al 2009 18 LBW Studies No abortions vs induced abortions•No abortion vs 1
IAB •18 studies•280,529 patients•OR 1.35 [1.20-
1.52]
•No abortions vs > 1 IAB•5 studies of 18•49,347 patients•OR 1.72 [1.45-
2.04]

Meta-analysis by Shah, et al 200922 PTB StudiesNo abortions vs induced abortions•No abortion vs 1
IAB 22 studies•268,379 patients•OR 1.36 [1.24-
1.50]
•No abortions vs > 1 IAB•7 studies of 22•158,421 patients•1.93 [1.38-2.71]
Meta-analysis by Swingle, et al 2009• Meta-analyses of literature 1995-2007• Pro-abortion and pro-life authors• 7,891 titles, 349 abstracts, 130 papers• 30 abortion and 26 SAB papers included• Analyzed data from 12 induced and 9 SAB
papers
Meta-analysis by Swingle, et al 2009• 12 studies used to calculate common OR’s for
induced abortion• 1 induced abortion 1.25 OR [1.03-1.48] increased risk
preterm birth < 37 weeks• > 1 induced abortion 1.51 OR [1.21-1.75] increased
risk preterm birth < 37 weeks

Meta-analysis by Swingle, et al 2009• 4 studies available for common OR’s for induced
abortion < 32 weeks (very preterm birth)• Common OR 1.64 [1.38-1.91]• Increased very preterm delivery rate of 64%• Similar to other literature’s findings

Two studies from 2012 Watson, et al: very preterm births (20- 31⁶ weeks)
• Case control study from Australia; 603 cases and 796 controls from 2002-2004
• Findings:• Terminations
• 1 abortion OR 2.11 (1.3,3.4) p<0.002; AOR 2.02 (1.2,3.3) p<0.004• > 1 abortion OR 4.4 (1.9,9.1) p<0.001; AOR 3.50 (1.6,7.9) p<0.002
• SAB’s• 1 SAB OR 2.06(1.4,3.1) p<0.001; AOR 2.03(1.4,3.1) p<0.001• > 1 SAB OR 3.01(1.8,5.0) p<0.001; AOR 2.82(1.7,4.8) p<0.001
Watson LF, Rayner JA, Forster D.. Midwifery 2012
Two studies from 2012 Watson, et al: Conclusions Two groups of risks• Lifestyle factors – being single, separated or divorced, smoking
and drug use, as well as a history of pregnancy termination• Pre-existing medical conditions–prior preterm birth, a history
of miscarriage, bleeding in prior pregnancies, and diabetes• “Our aim is that by presenting the findings summarised
together, the data may be helpful for those providing care to women antenatally, particularly when taking medical histories in early pregnancy or in pre-pregnancy clinics.” i.e. Elective abortion is HIGH RISK factor for PTB and need to be AWARE as physicians and patients!
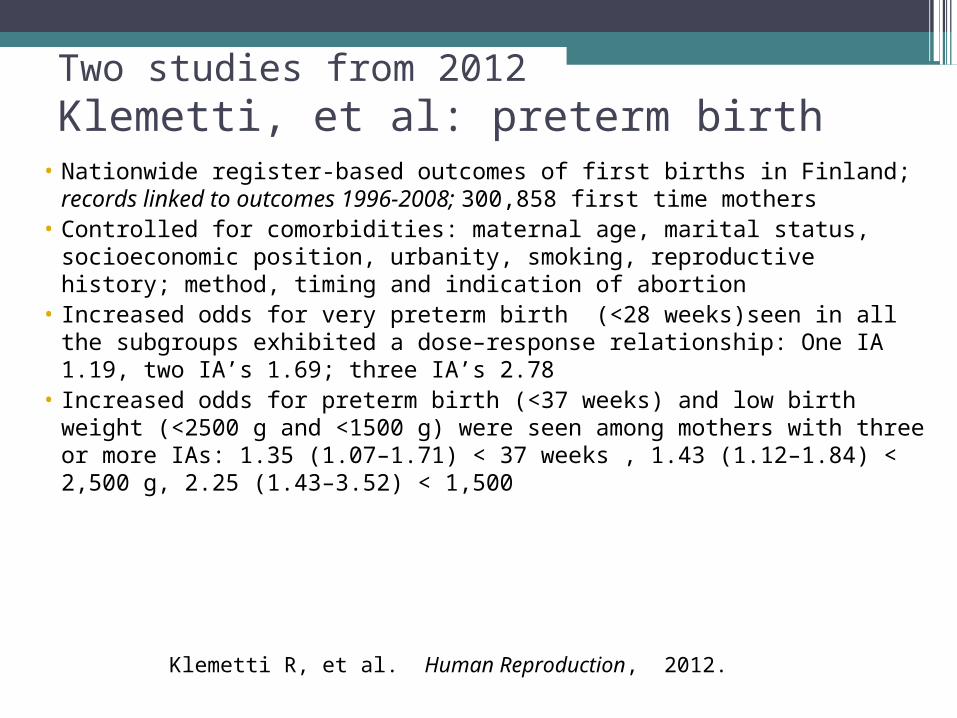
Two studies from 2012 Klemetti, et al: preterm birth
• Nationwide register-based outcomes of first births in Finland; records linked to outcomes 1996-2008; 300,858 first time mothers
• Controlled for comorbidities: maternal age, marital status, socioeconomic position, urbanity, smoking, reproductive history; method, timing and indication of abortion
• Increased odds for very preterm birth (<28 weeks)seen in all the subgroups exhibited a dose–response relationship: One IA 1.19, two IA’s 1.69; three IA’s 2.78
• Increased odds for preterm birth (<37 weeks) and low birth weight (<2500 g and <1500 g) were seen among mothers with three or more IAs: 1.35 (1.07–1.71) < 37 weeks , 1.43 (1.12–1.84) < 2,500 g, 2.25 (1.43–3.52) < 1,500
Klemetti R, et al. Human Reproduction, 2012.

Two studies from 2012
Klemetti, et al: preterm birthConclusions:•“In terms of public health and practical implications, health education should contain information of the potential health hazards of repeat IAs, including very preterm birth and low birth weight in subsequent pregnancies.”•“Health care professionals should be informed about the potential risks of repeat IAs on infant outcomes in subsequent pregnancy.”

Two studies from 2012
Klemetti, et al: preterm birth• Final Thought by researchers:
“Observational studies like ours, however large and well-controlled, will not prove causality.”
• Same thing said by tobacco research.

Bradford Hill Criteria•Developed to draw causal inference
from epidemiological association • In 1964, the US Surgeon General
applied the newly developed Bradford Hill criteria for causality to the cigarette lung cancer link epidemiologic studies to warn the public
•Tobacco-lung cancer link known since the 1940’s•A response to politicized “tobacco science”
Criteria for drawing a causal inference from epidemiological association: abortion and preterm birth fulfill many criteria•Timing: abortion occurs before preterm birth•Dose effect: risk is higher with more exposure•Consistency of effect: demonstrated in many
populations•Strength of association: more association with
very preterm birth•Biological plausibility: abortion leads to chronic
inflammation and cervical incompetence

More medical abortions: An important trend•44,000,000 abortions world-wide in 2008•Medical abortion – mifepristone and misoprostol or
misoprostol alone - is increasing as a proportion of all abortions internationally – legal and clandestine
•USA: 17% of all nonhospital abortions, 25% of abortions < 9 weeks in 2008
•European countries: medical abortions as percentage of abortions: Scotland 2012 77%, Sweden 2011 75%, Denmark 2011 56%, Finland 2011 89%
International perspectives on global and reproducitve health; Vol 38, no 1. March 2012
Changes in association of abortion and preterm birth: Scotland 1980-2008•Historical cohort study of 732,719 first births >24
weeks•Preterm delivery <37 weeks declined over time•Surgical without use of cervical pre-treatment
decreased from 31% to 0.4%; medical abortions increased from 18% to 68% during this period
•Previous abortion associated with preterm birth most prevalent 1980-1983 (OR 1.32 [1.21–1.43]) ; overall OR (1.12 [1.09–1.16])
Oliver-Williams C et al. PLoS Medicine, 2013

Changes in association of abortion and preterm birth: Scotland 1980-2008
Oliver-Williams C et al. PLoS Medicine, 2013

Changes in association of abortion and preterm birth: Scotland 1980-2008•Headlines – “Modern methods of abortion not
associated with preterm births.” • “Maternal abortion no longer associated with
preterm birth.”•Authors: “We speculate that modernising abortion
methods may be an effective long-term strategy to reduce global rates of preterm birth.”
Is this really true?Other studies show no difference in PTB between
medical and surgical abortion.

Oliver-Williams C et al. PLoS Medicine, 2013
Medical and surgical abortion: China 1998-2001•Compared birth outcomes in women with one prior
medical or surgical abortion vs no abortions▫4,925 women with no history of induced abortion ▫4,931 women with one mifepristone-induced abortion▫4,800 women with one previous surgical abortion ▫Lost to follow up <1%
• No significant differences comparing medical and surgical abortion in risk of preterm delivery (28-37 weeks), frequency of low birth weight
Chen A et al. Am. J. Epidemiol. 2004

Medical vs surgical abortion: Finland 2000-2009•All primigravid women with one prior induced
abortion and singleton delivery •Population-based register study•Medical (n = 3441) or surgical (n = 4853)
abortion; total 8294•No statistically significant difference in risk of
preterm birth with medical vs surgical abortion▫4.0% risk with medical abortion▫4.9% risk surgical abortion
Mannisto J et al. BJOG. 2013
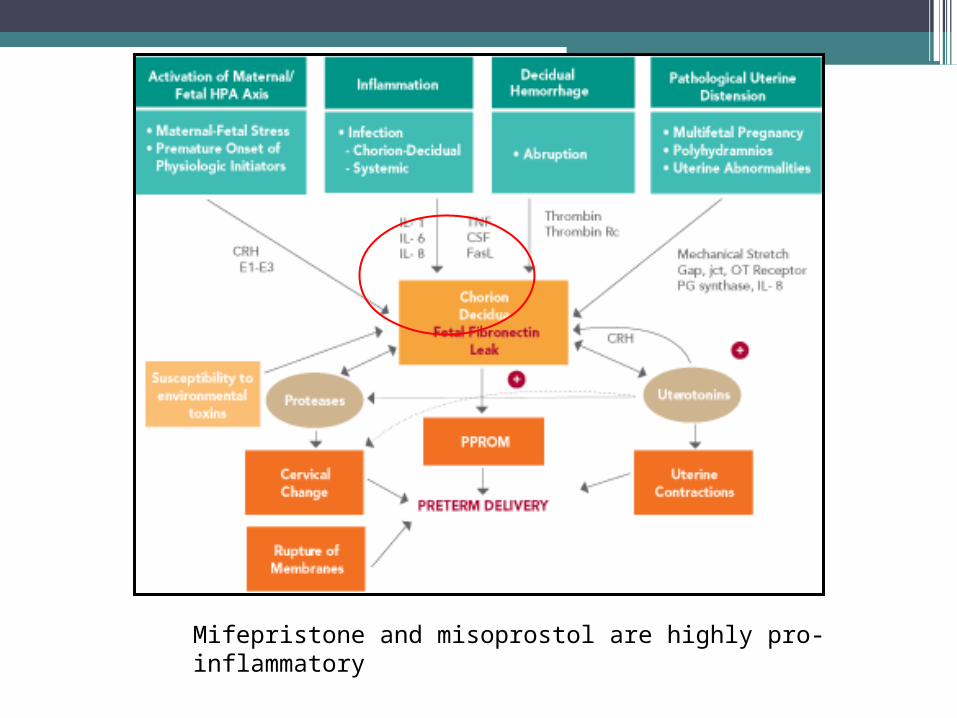
Mifepristone and misoprostol are highly pro-inflammatory

Medical abortion: high failure rate•Studied all Finnish women undergoing abortion < 9
weeks gestation 2000-2006•42,619 abortions: medical 22,368 and surgical 20,251•Adverse events four times higher with medical
abortions; 20% vs 5.6%•Rate of hemorrhage 15.6%•Surgical (re)evacuation 5.9% of medical abortions;
1.9% of surgical abortions (P<.001)
Niinnimaki, M. et al. Obstet Gynecol. 2009.
China: Repeated medical abortions and the risk of preterm birth in the subsequent pregnancy •Cohort study of 7 hospitals in Chendu 2006-2009•Delivery outcomes known in 18,323▫1 surgical abortion 40% increase PTB▫3 or more surgical abortions 62% increase in PTB▫Combined medical surgical abortion increase of 212%
(20% of medical IAB had surgical evacuation)•69% increase in PTB with surgical evacuation < 7 weeks•360% increase in PTB with med-surg abortion < 7 weeks
Liao H et al. Arch Gynecol Obstet . 2011.

Israel: Clinical, surgical and histopathologic outcomes following failed medical abortion
• Medical-surgical abortions are associated with significant necrosis and inflammation▫ 104 surgical abortions vs 104 medical-surgical abortions▫ Inflammation quantified by immunohistochemical stains for T and B
lymphocytes and macrophages; necrosis evaluated morphologically▫ Abnormal findings more frequent in the med-surg group; 10.9% vs 1.9%
• Most frequent abnormality in the case group was the presence of intimately adherent products of conception, necessitating sharp curettage
• “The long term consequences of curettage following failed medical abortion warrant further investigation.”
Fuchs N et al. Int J Gynaecol Obstet. 2012

Conclusions• Induced abortion increases preterm birth rates
substantially in latest large studies and meta analyses; 135 studies now with statistical significance (February, 2013)
• Medical abortion does NOT eliminate risk of preterm birth
• Preterm birth increases risk for cognitive, visual and other deficits substantially; cerebral palsy by 147 times
• Health care-neonatal costs increased by billions• Patients, governments and health care
organizations need to know consequences and costs related to induced abortion


With thanks toByron C. Calhoun, MD, FACOG, FACS, MBAProfessor and Vice Chair, Obstetrics and GynecologyWest Virginia University-CharlestonCharleston, West Virginia, USA

ReferencesBack S et al. Bull World Health Organ, 2010Behrman,E et al. Preterm Birth: Consequence, Causes and Prevention. National Academies Press,
2007 Calhoun BC. Abortion and Preterm Birth: Why Medical Journals Aren’t Giving Us the Truth. IORG
Briefing Paper. 2012.Calhoun BC, Shadigian E, Rooney B. Induced abortion: cost consequences of an attributable risk
for preterm birth and its impact on informed consent and medical malpractice. J Repro Med 2007;52.
Chen A, YuanW, Meirik O, Wang X. Wu S, Zhou L, Luo L, Gao E, and Cheng Y. Mifepristone-induced early abortion and outcome of subsequent wanted pregnancy. Am. J. Epidemiol. 2004. Vol. 160, No. 2
Fuchs N, Maymon R, Ben-Ami I, Mendlovic S,Schneider D, Pansky M, Halperin R . Clinical, surgical, and histopathologic outcomes following failed medical
abortion. Int J Gynaecol Obstetrics. 2012;117.Hamilton B et al. CDC Vital Statistics Reports, 2012Hill AB. The environment and disease: Association or causation? Proceed Roy Soc Medicine –
London1965:58.Himpens E, Master PT, Van den Broeck C, Oostra A, Calders P, Vanhaesebrouck P. Prevalence, type,
distribution of cerebral palsy in relation to gestational age: a meta-analysis review. Develop Med Child Neurol. 2008. Vol 50.
Holst D, Garnier Y. Preterm birth and inflammation- the role of genetic polymorphisms. Eur J Obstet Gynecol Biol. 2008:1.

ReferencesInfant Health in America: Everybody’s Business. Hartford, CT:CIGNA Corp 2000International perspectives on global and reproductive health. 38:1. 2012.Klemetti R, Gissler M, Niinimaki M, Hemminki E. Birth outcomes after induced abortion: a
nationwide register-based study of first births in Finland. Human Reproduction, 2012Liao H, Wei Q, Duan L, Ge J, Zhou Y, Zeng W. Repeated medical abortions and the risk of
preterm birth in subsequent pregnancies. Arch Gynecol Obstet 2011;289. Luke B, Bigger H, Leurgas S, Siesma D. The cost of prematurity: a case-control study of twins vs.
singletons. AM J Publ Health. 1996:86.Männistö J, Mentula M, Bloigu A, Hemminki E, Gissler M, Heikinheimo O, Niinimäki
M. Medical versus surgical termination of pregnancy in primigravid women—is the next delivery differently at risk? A population-based register study. BJOG 2013:120
McCaffrey M. Abortion’s impact on prematurity. Family North Carolina, 2013.March of Dimes. Peristats, as found at:
http://www.marchofdimes.com/peristats/Peristats.aspxNiinimäki M, Pouta A, Bloigu A, Gissler M, Hemminki E, Suhonen S, Heikinheimo O.
Immediate complications after medical compared with surgical termination of pregnancy. Obstet Gynecol. 2009 ;114.
Nour N. Preterm delivery and the MDG. Rev Obstet Gynecol, 2012;5.Oliver-Williams C, Fleming M, Monteath K, Wood AM, et al. Changes in Association
between Previous Therapeutic Abortion and Preterm Birth in Scotland, 1980 to 2008: A Historical Cohort Study. PLoS Med 2013; 10.

ReferencesPetrou S, Mehta Z, Hockley C, Cook-Mozaffari P, Henderson J, Goldacre M. Pediatrics 2003;112.Rooney B, Calhoun B. Induced abortion and risk of later preterm births. J Am Phys Surg. 2003;8. Robinson J et al. Risk factors for preterm birth. UptoDate. 2012. 8:2Shah PS, Zao J. Induced termination of pregnancy and low birthweight and preterm birth: a systematic review and meta-analysis. BJOG 2009;116 Swingle HM, Colaizy TT, Zimmerman MB, Morriss FH. Abortion and the risk of subsequent preterm birth: A systematic review with meta-analyses. J Repro Med .2009; 54. Velez DR, Fortunato SJ, Thorsen P, Lombardi SJ, Williams SM, Menon R. Preterm birth in Caucasians is associated with coagulation and inflammation pathway gene variants. PLoSOne. 2008:3.Velez, DR, Fortunato S, Thorsen P, Lombardi SJ, Williams SM, Menon R. Spontaneous preterm birth in
African Americans is associated with infection and inflammatory response gene variants. Am J Obstet Gynecol. 2009: 200Watson LF, Rayner JA, Forster D. Identifying risk factors for very preterm birth: A reference for clinicians. Midwifery 2012WHO 2012, The Global Action Report on Preterm Birth.Zhou W, Sorenson HT, Olsen J. Induced Abortion and Subsequent Pregnancy Duration. Obstetrics & Gynecology 1999;94.


















