Presented by: Najafi AZ, MD. Respiratory tract a common site of occupational injury Two sites: ◦...
64
Presented by: Najafi AZ, MD
-
Upload
marjorie-austin -
Category
Documents
-
view
216 -
download
0
Transcript of Presented by: Najafi AZ, MD. Respiratory tract a common site of occupational injury Two sites: ◦...

Presented by: Najafi AZ, MD

Respiratory tract a common site of occupational injury
Two sites: ◦ Airways◦ Parenchyma
Site of injury depends on:◦ Gas solubility◦ Particle size


History Physical exam Pulmonary function tests:
◦ Spirometry◦ Body plethysmography◦ DLCO
Imaging:◦ Chest X ray◦ HRCT

Short-term exposure to high concentration of gases, fumes, or mists
Generally as an accident Irritation of membranes Chemical pneumonitis ARDS Chmicals:
◦ Formaldehyde◦ Cadmium salts◦ chlorine
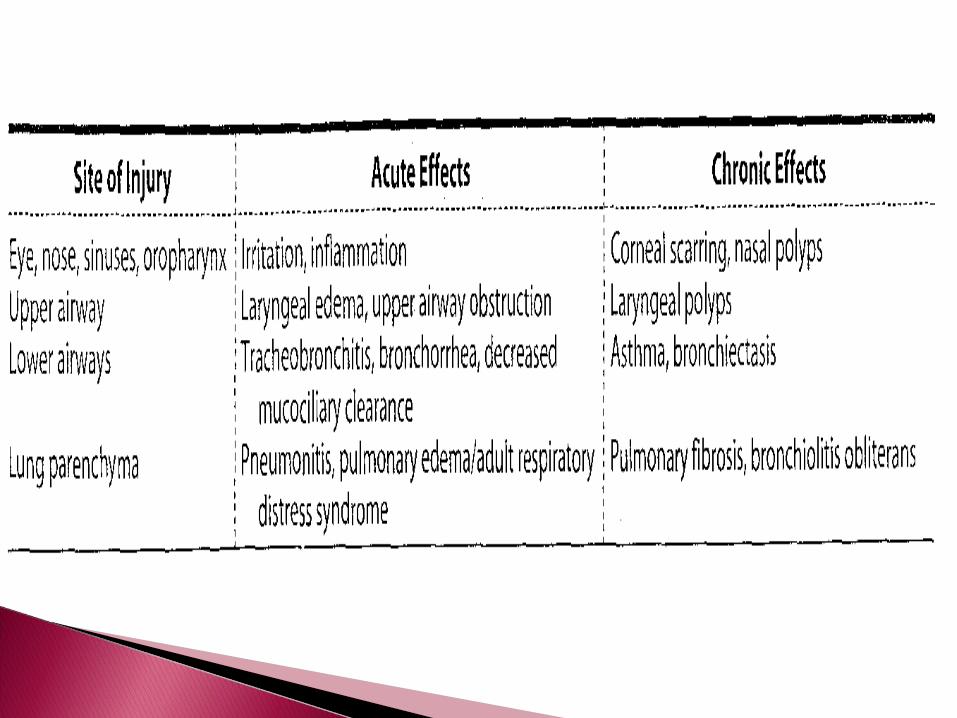

Upper respiratory tract irritation Cough Stridor Hoarseness Wheezing PFT: normal, obstructive, mixed Chest X ray: normal to pulmonary edema

Reversible airway obstruction, with
airway inflammation and bronchial
hyperresponsiveness as a consequence
of occupational exposures


Sensitizer-induced◦ Type 1 immune reaction (IgE)◦ Latent period for sensitization◦ In a percent of workers
Irritant-induced◦ RADS
Without latency Exposure to a high concentration In most workers


History:◦ Hx of dyspnea (exertional), cough, in an episodic
mode, night symptoms Physical exam
◦ wheezing PFT
◦ Spirometry: normal or obstructive◦ BD test: mostly responsive
Chest X ray◦ Not helpful

Current health (during the last 4 weeks)
If you run or climb stairs fast do you ever:•Cough?•Wheeze?•Get tight in the chest?
Yes/noYes/noYes/no
Is you sleep ever broken by:•Wheeze?•Difficulty with breathing?
Yes/noYes/no
Do you ever wake up in the morning with:•wheeze?•Difficulty with breathing?
Yes/noYes/no
Do you ever wheeze:•If you are in a smoky room?•If you are in a very dusty place?
Yes/noYes/no

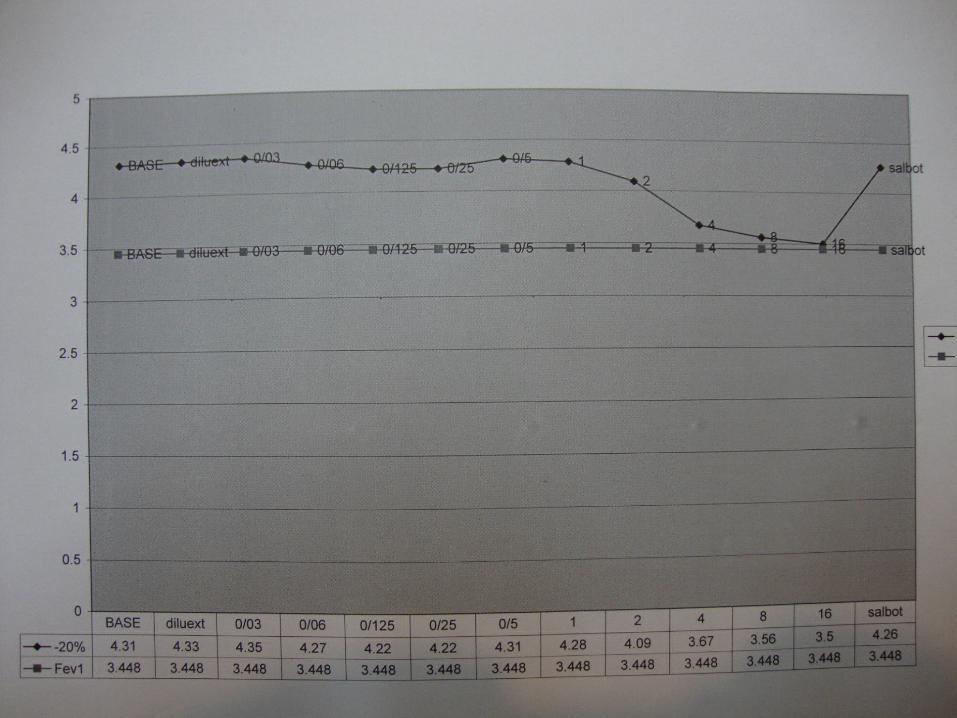
I. Occupational symptoms.II. Serial P.E.FIII. Serial spirometryIV. Challenge test



Reduction or elimination of exposure Beta agonists corticosteriods
1. Substitution2. Ventilation3. Change of procedure4. Restriction of employment5. Free from smoke6. Accidental education7. Environmental screening8. Protective devices

A type of O-ILDs. Due to inhalation and deposition of mineral
dust within lung parenchyma. Induce tissue reaction May cause disruption of alveolar
architecture or collagen fibrosis.

Deposition of mineral dusts in lung tissue. Presence of parenchymal tissue reaction Positive chest x-ray findings
PFT may be abnormal depending on the stage and severity and complications.

Benign:◦ Asymptomatic◦ Normal spirometric findings
Collageneous:◦ Symptomatic◦ Abnormal spirometric findings
Sufficient and reasonable exposure. (intensity and duration)
Positive chest x-ray findings (good quality is required)
No other concomitant diseases that mimic pneumoconiosis.

Silicosis Asbestosis Coal-workers’ pneumoconiosis

Silicosis
A collagenous pneumoconiosis caused by inhalation of respirable (0.2 – 10 µm ) free crystalline silicon dioxide ( SiO2 ).
Chronic diffuse interstitial fibronodular lung disease.
High-dose and long-time inhalation is required. A strict dose-response relationship is present
Cumulative exposure Intensity × duration

Removal of stone Hard rock mining Tunnel drilling Stone quarrying
Processing stone or sand Stone crushing Granite carving


MinningFoundry
workSand
blastingCeramics
Abrasive use of silica or sand Abrasive blasting Foundry casting Knife sharpening
Production of fine silica powder


Utilization of sand or silica powder◦ Glass manufacture◦ Plastic manufacture◦ Paint manufacture◦ Pottery◦ Ceramic manufacture◦ Construction work

Chronic bronchitis Emphysema Silicosis Tuberculosis Lung cancer Collagen vascular diseases

Chronic simple ( classic ) silicosis
Chronic complicated ( PMF ) silicosis
Accelerated silicosis
Acute silicosis

Moderate long-time exposure (at least 10 yr) to less than 30% quartz
Symptoms and signs:◦ Mostly asymptomatic◦ Chronic productive cough or DOE due to chronic bronchitis◦ Progressive DOE and dry cough (late finding)◦ Ph. exam normal or crackles◦ PFT: normal or restrictive (mainly) obstructive or mixed pattern◦ CXRay: small (<1 cm), round nodules predominantly in upper
lobes, hilar lymphadenopathy and calcification
Progressive massive fibrosis Tuberculosis(3-fold to 20-fold)
Pulmonary and extrapulmonary Typical and atypical mycobacteria
Immune-mediated Scleroderma (m/c) SLE, RA , … Renal (GN, nephrotic syndrome)(usually in heavy exposure)
Lung cancer Fungal diseases
Cryptococcus Blastomycosis coccidiopmycosis
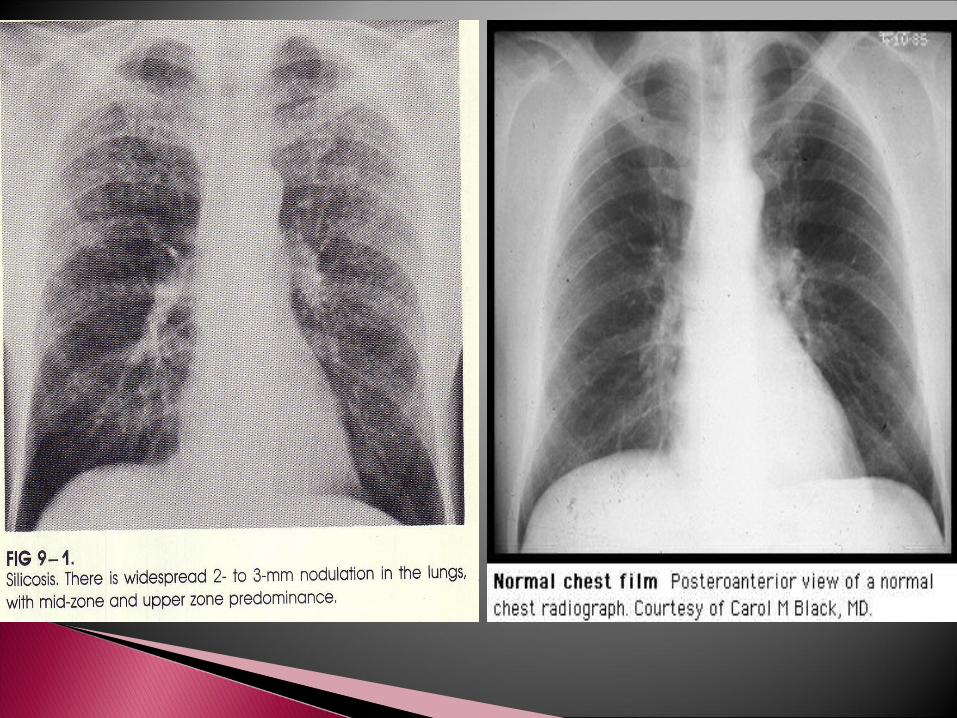

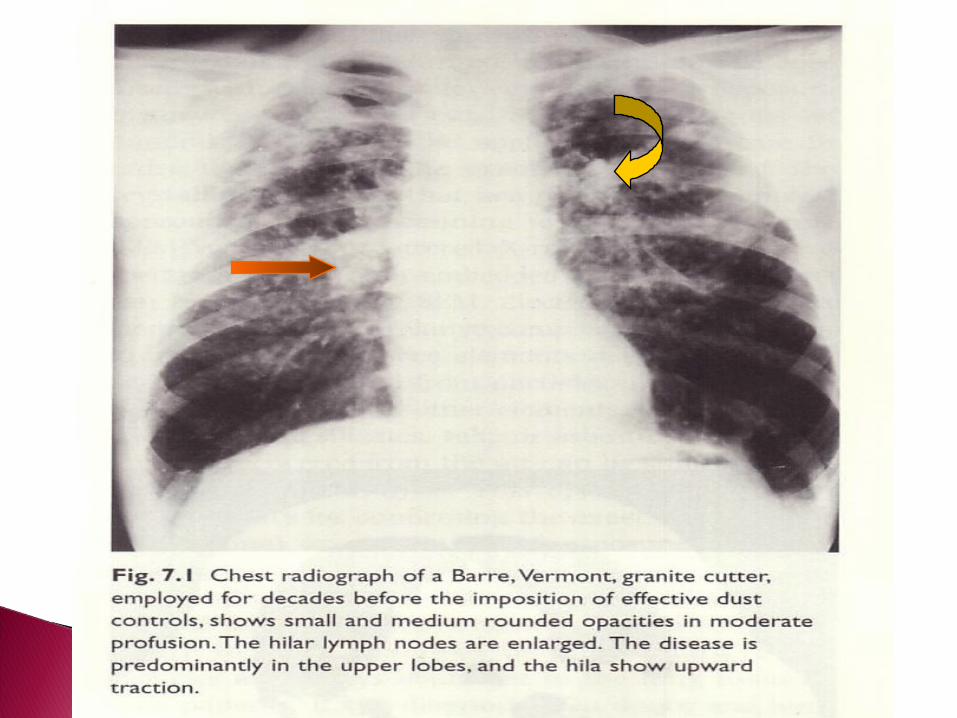

SilicosisCalcified lymph nodes
Upper lobe nodules

Incidence of TB is greater in accelerated Incidence of TB is greater in accelerated or acute Silicosisor acute Silicosis
Silica exp. in the absence of silicosis is Silica exp. in the absence of silicosis is risk factor for TBrisk factor for TB
Silica exp. : Risk for TB Silica exp. : Risk for TB Radiographic changes in silicosis Radiographic changes in silicosis frequency of TB frequency of TB Silica exp. & TB: Death 4 yrs earlier Silica exp. & TB: Death 4 yrs earlier
than TB alone than TB alone

Dx : rapid worsening of CXR, decline in Dx : rapid worsening of CXR, decline in lung function suspicion for TBlung function suspicion for TB
regular PPD skin test (yearly )regular PPD skin test (yearly )
PPD(+) without active TB , indicated at PPD(+) without active TB , indicated at least 1 yr INH prophylaxis.least 1 yr INH prophylaxis.

11-History of silica exp.-History of silica exp.
22-Chest radiography consist with silicosis.-Chest radiography consist with silicosis.
33-R/O other illness that mimic silicosis. -R/O other illness that mimic silicosis.
HRCT & Lung biopsy (open) if …HRCT & Lung biopsy (open) if …

Product substitution of silica with less Product substitution of silica with less toxic particlestoxic particles
Engineering control of dust Engineering control of dust concentration concentration
Appropriate use of respiratory Appropriate use of respiratory protective devicesprotective devices
Medical screening: Medical screening: questionnaire, CXR, spirometryquestionnaire, CXR, spirometry
DiagnosisDiagnosis of silicosis Remove of silicosis Remove Regular CXR and PPD skin test Regular CXR and PPD skin test Steroid helpful in Acute S. or Steroid helpful in Acute S. or
autoimmune dis. (+ INH prophylaxis)autoimmune dis. (+ INH prophylaxis) Whole lung lavage for acute silicosis ?Whole lung lavage for acute silicosis ? Tetrandrine Tetrandrine Lung trasplantationLung trasplantation

Crystalline silica (quartz, cristobalite) is Crystalline silica (quartz, cristobalite) is carcinogen (group 1 IARC)carcinogen (group 1 IARC)
Silicosis is associated with autoimmune Silicosis is associated with autoimmune disease (RA, SLE, Scleroderma)disease (RA, SLE, Scleroderma)


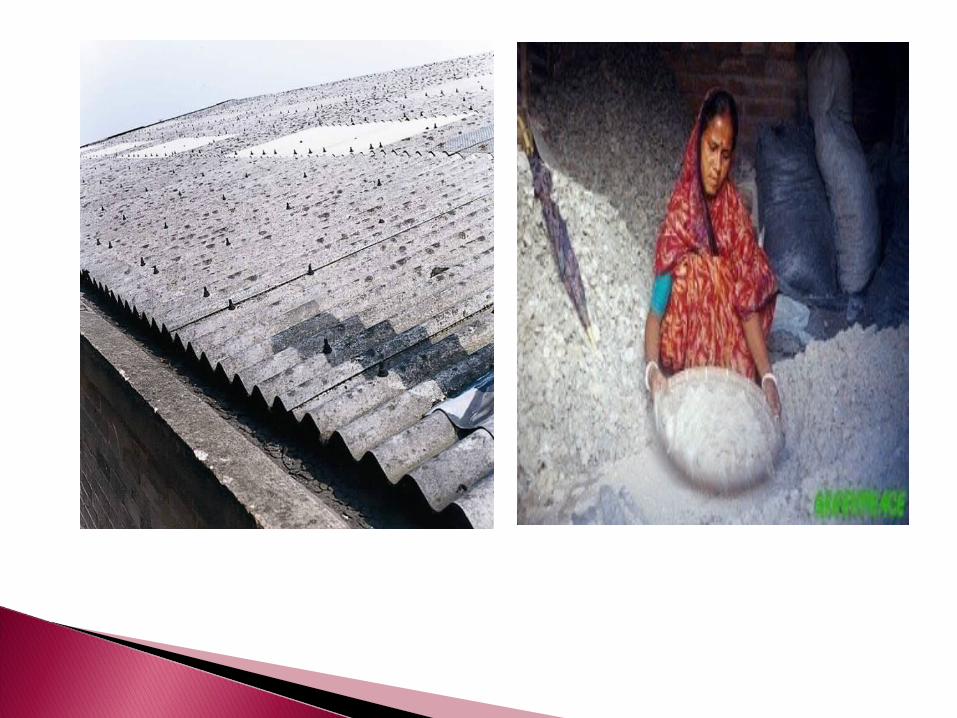
Pipe coveringAsbestos clothCementsRoofing materials
Clinical presentation: exertional dyspnea,, cough, chest pain, clubbing
• X Ray: reticular veiling lower lobes, ground glass
pleural changes, PMF in mixed exposure,
• Lung fx: restrictive, diffusion↓, hypoxemia,



Coal worker's pneumoconiosis (CWP) can be defined as the accumulation of coal dust in the lungs and the tissue's reaction to its presence:
simple CWP (SCWP) pulmonary massive fibrosis (PMF)


Radiology: nodular veiling upper lung zones, nodules > 1 cm indicative of
PMF
• Lung fx: normal – simple type restrictive – complicated type • Prognosis: simple type – good complicated type – cardio-respiratoryfailure

Immunologically mediated inflammatory disease of lung parenchyma caused by some organic dusts


History◦ Acute: cough, fever, chills, malaise, dyspnea after
an acute exposure◦ Chronic
Physical exam”◦ Basilar inspiratory crackles
PFT:◦ Restrictive or mixed pattern, low DLCO
CXray: ◦ normal, reticulonodular pattern, infiltration

Avoidance of exposure Corticosteroids

OCCUPATIONAL LUNG OCCUPATIONAL LUNG
DISEASES ARE DISEASES ARE
PREVENTABLEPREVENTABLE

Complex exposures






![LW Claude Monet Attunement (Farhad Najafi)[1]](https://static.fdocuments.in/doc/165x107/577d21031a28ab4e1e9444f0/lw-claude-monet-attunement-farhad-najafi1.jpg)