Presentations of Acute Phenytoin...
7
I: Presentations ofAcutePhenytoinOverdose LARRYB. MELLICK, MD,* J. ALAN MORGAN,DO,t GARYA. MELLICK,DO:!: A 15-year-oldboyingested19.6g (15g verifiable)phenytoin sodiumapproximately fourhoursbeforeemergency department presentation. Thepatientsurvived thesuicideaUempt withonly supportivecare,despitetheingestionof392mg/kganda peak serumlevelof 100.8 g/mL.Awidespectrumofphysical find- ingsconsistent withacutemassive ingestionof phenytoinwas noted.Thiscasereportanda reviewof casesreported in the English literatureofacutesingleanticonvulsant ingestion further delineate theclinicalpresentation ofacutephenytoinoverdose. (AmJ EmergMed1989;7:61-67. @ 1989byW.B.Saunders Company.) Phenytoin has been used as an anticonvulsant since its therapeutic benefit was first reported in the late 1930s.1-3Subsequently, the therapeutic usefulness of this medication has been well established. Following the introduction of phenytoin, reports of various adverse effects and descriptions of gradual and acute intoxications began to appear in the literature. For gradual intoxication, clinical presentation and other adverse effects have been well described. How- ever, the presentation following acute oral overdose and intoxication seems less well delineated. There- fore, in this report the signs and symptoms of acute phenytoin ingestion and intoxication are specifically reviewed. This presentation was accomplished by means of a review of the English literature and our own report of a case of massive ingestion. CASEREPORT On November 15, 1985 a 15-year-old white boy with a history of absence seizures presented to the emergency de- partment (ED) of Brooke Army Medical Center (San Anto- From the 'Emergency Medicine Service, Tripier Army Medical Center, Tripier AMC, HI; the tDepartment of Emergency Medi- cine, USA MEDDAC, Fort Hood, TX; and the :j:Department of Neurology, University of Cincinnati Medical Center, Cincinnati. Manuscript received June 16, 1986; revision accepted February 26,1988. The opinions and assertions contained herein are those of the authors and should not be construed as official or representing the views of the Department of Defense or the Department of the Army. Address reprint requests to Dr Larry B. Mellick: 1888 Walnut Hill Park Dr, Columbus, OH 43232. Key Words: Phenytoin, anticonvulsant overdose. @ 1989 by W.B. Saunders Company. 0735-6757/89/0701-0015$5.00/0 nio, TX) after acutelyingesting a largenumberofphenytoin capsulesover a two-hour period. When awakening the boy for school his parents found him lying on the bedroom floor in a pool of pink vomitus and surrounded by several empty Dilantin (Parke-Davis, Morris Plains, NJ) bottles. History elicitedfromthe familyrevealeda past diagnosisofborder- line schizophrenia and multiple suicide threats over the past week. On presentation the patient demonstrated the following vital signs: BP, 108/80;pulse, 68/min; shallow respirations, 24/min; and temperature, 99.4°P. General physical examina- tion demonstrated a thin and seemingly mute adolescent boy with intermittent body movements best characterized as choreoathetoid. Physical contact with the patient resulted in marked increases in these movements and occasional opisthotonic posturing. The patient would open his eyes to command but did not or could not communicate through speech. The pupils were midposition and reactive to light, and the patient appeared unable to fixate his eyes. Exami- nationof the pharynxwith a tonguebladeresultedin parox- ysms of retching, opisthotonic posturing, and vomiting. Chest examination demonstrated shallow movements of the thorax. The lungs were clear to auscultation. Examination of the heart demonstrated a normal rhythm and no murmurs. The extremities demonstrated brisk, lII-IV/IV, symmetrical deeptendonreflexes,a three-beatankleclonus,andupward going toes. The presence of ataxia or tremor could not be determined because of the dominant choreoathetoid and opisthotonic presentation. Initial treatment in the ED consisted of airway protection by nasotracheal intubation in preparation for gastric lavage with a large-bore tube. Gastric lavage with a total of 4 L normal saline was performed. Subsequently, 300 mL mag- nesium citrate with 60 g charcoal was administered through the lavagetube. Due to the remote possibility of a mixed overdose and the patient's hypoventilation, 3.2 mg naloxone hydrochloride (Narcan; Endo Pharmaceuticals, Inc, Puerto Rico) was administered intravenously (IV). Laboratory data in the ED demonstrated an initial arterial blood gas of pH, 7.406; PC02, 46.8; P02, 90.3; and HC03, 29.4. Serum electrolytes were as follows: sodium, 139;chlo- ride, 101; potassium, 4.0; C02' 27; BUN, II; Cr, 0.1. The Dilantinlevelwas 45 f.Lg/mLon arrival to the ED. The WBC count was 3.3, hemoglobin was 17.2, and hematocrit was 50.7. The chest x-ray demonstrated appropriate nasotracheal tube placement and no evidence of pulmonary aspiration. ECG findings were appropriate for age and demonstrated no conduction or rhythm abnormalities. The patient was admit- ted to the pediatric intensive care unit (ICU) for continued therapy and monitoring. HospitalCourse After admission to the pediatric ICU at Brooke Army Medical Center, the patient required only supportive care. 61
Transcript of Presentations of Acute Phenytoin...

I:
PresentationsofAcutePhenytoinOverdose
LARRYB. MELLICK,MD,* J. ALAN MORGAN,DO,tGARYA. MELLICK,DO:!:
A 15-year-oldboyingested19.6g (15g verifiable)phenytoinsodiumapproximatelyfourhoursbeforeemergencydepartmentpresentation.ThepatientsurvivedthesuicideaUemptwithonlysupportivecare,despitetheingestionof 392mg/kganda peakserumlevelof 100.8 g/mL.A widespectrumof physicalfind-ingsconsistentwith acutemassiveingestionof phenytoinwasnoted.Thiscasereportanda reviewof casesreportedin theEnglishliteratureofacutesingleanticonvulsantingestionfurtherdelineatetheclinicalpresentationof acutephenytoinoverdose.(AmJ EmergMed1989;7:61-67.@ 1989byW.B.SaundersCompany.)
Phenytoin has been used as an anticonvulsant sinceits therapeutic benefit was first reported in the late1930s.1-3Subsequently, the therapeutic usefulness ofthis medication has been well established.
Following the introduction of phenytoin, reports ofvarious adverse effects and descriptions of gradual andacute intoxications began to appear in the literature.For gradual intoxication, clinical presentation andother adverse effects have been well described. How-ever, the presentation following acute oral overdoseand intoxication seems less well delineated. There-fore, in this report the signs and symptoms of acutephenytoin ingestion and intoxication are specificallyreviewed. This presentation was accomplished bymeans of a review of the English literature and ourown report of a case of massive ingestion.
CASEREPORT
On November 15, 1985 a 15-year-old white boy with ahistory of absence seizures presented to the emergency de-partment (ED) of Brooke Army Medical Center (San Anto-
From the 'Emergency Medicine Service, Tripier Army MedicalCenter, Tripier AMC, HI; the tDepartment of Emergency Medi-cine, USA MEDDAC, Fort Hood, TX; and the :j:Department ofNeurology, University of Cincinnati Medical Center, Cincinnati.
Manuscript received June 16, 1986; revision accepted February26,1988.
The opinions and assertions contained herein are those of theauthors and should not be construed as official or representingthe views of the Department of Defense or the Department of theArmy.
Address reprint requests to Dr Larry B. Mellick: 1888 Walnut HillPark Dr, Columbus, OH 43232.
Key Words: Phenytoin, anticonvulsant overdose.
@1989 by W.B. Saunders Company.
0735-6757/89/0701-0015$5.00/0
nio, TX) after acutelyingestinga largenumberofphenytoincapsulesover a two-hour period. When awakening the boyfor school his parents found him lying on the bedroom floorin a pool of pink vomitus and surrounded by several emptyDilantin (Parke-Davis, Morris Plains, NJ) bottles. Historyelicitedfromthe familyrevealeda past diagnosisof border-line schizophrenia and multiple suicide threats over the pastweek.
On presentation the patient demonstrated the followingvital signs: BP, 108/80;pulse, 68/min; shallow respirations,24/min;and temperature, 99.4°P. General physical examina-tion demonstrated a thin and seemingly mute adolescent boywith intermittent body movements best characterized aschoreoathetoid. Physical contact with the patient resulted inmarked increases in these movements and occasionalopisthotonic posturing. The patient would open his eyes tocommand but did not or could not communicate throughspeech. The pupils were midposition and reactive to light,and the patient appeared unable to fixate his eyes. Exami-nationof the pharynxwitha tonguebladeresultedin parox-ysms of retching, opisthotonic posturing, and vomiting.Chest examination demonstrated shallow movements of thethorax. The lungs were clear to auscultation. Examination ofthe heart demonstrated a normal rhythm and no murmurs.The extremities demonstrated brisk, lII-IV/IV, symmetricaldeeptendonreflexes,a three-beatankleclonus,andupwardgoing toes. The presence of ataxia or tremor could not bedetermined because of the dominant choreoathetoid andopisthotonic presentation.
Initial treatment in the ED consisted of airway protectionby nasotracheal intubation in preparation for gastric lavagewith a large-bore tube. Gastric lavage with a total of 4 Lnormal saline was performed. Subsequently, 300 mL mag-nesium citrate with 60 g charcoal was administered throughthe lavagetube. Due to the remote possibilityof a mixedoverdose and the patient's hypoventilation, 3.2 mgnaloxonehydrochloride (Narcan; Endo Pharmaceuticals, Inc, PuertoRico) was administered intravenously (IV).
Laboratory data in the ED demonstrated an initial arterialblood gas of pH, 7.406; PC02, 46.8; P02, 90.3; and HC03,29.4. Serum electrolytes were as follows: sodium, 139;chlo-ride, 101; potassium, 4.0; C02' 27; BUN, II; Cr, 0.1. TheDilantin level was 45 f.Lg/mLon arrival to the ED. The WBCcount was 3.3, hemoglobin was 17.2, and hematocrit was50.7.The chest x-ray demonstrated appropriate nasotrachealtube placement and no evidence of pulmonary aspiration.ECG findings were appropriate for age and demonstrated noconduction or rhythm abnormalities. The patient was admit-ted to the pediatric intensive care unit (ICU) for continuedtherapy and monitoring.
HospitalCourseAfter admission to the pediatric ICU at Brooke Army
Medical Center, the patient required only supportive care.
61
AMERICAN JOURNAL OF EMERGENCY MEDICINE. Volume 7, Number 1 . January 1989
Aggressive cathartic and charcoal therapy was continuedthroughout 'hospitalization. The patient's clinical presenta-tion and associated phenytoin levels are presented below.
The initial phenytoin level obtained in the ED was 45fJ..g/mL.Peaking of the anticonvulsant level at 100.8fJ..g/mLoccurred in the afternoon of the second day. Throughout thefirst three days of hospitalization the patient's condition var-ied between combativeness, agitation, and responsivenessonly to pain. During periods of severe agitation, diazepamwas intermittently required to calm the patient. The phenyt-oin level obtained in the early morning of the third day was87.0 fJ..g/mL.By the fourth day of admission he became lesscombative and was responsive to verbal stimuli. Serum lev-els on day 4 were 65.4 fJ..g/mLat 10AMand 55.0 fJ..g/mL12hours later. On day 5, the patient was oriented, eating, andambulatory, despite being markedly ataxic. Serum levelsmeasured 12hours apart were 42.6 fJ..g/mLand 42.4 fJ..g/mL.At that time he related that he had ingested 196pills at 2 AMon the day of admission. Nystagmus, both horizontal andvertical, persisted until day 7 (serum level, 26.4 fJ..g/mL).After eight days of hospitalization the patient was trans-ferred to a residential psychiatric facility.
Serious potential consequences of overdose did not occurin this case. Our patient demonstrated no hypotension orcardiac arrhythmia as a consequence of the massive phenyt-oin ingestion.4 A febrile response did occur on the secondday of hospitalization. Because the intubated patient hadother potential sources of temperature elevation (ie, at-electasis) that were not specifically investigated by physi-cians in the ICU, we cannot attribute this finding to phenyt-oin intoxication. Nevertheless, fevers have been describedin cases of acute phenytoin intoxications.5.6
Laboratory documentation of the patient's condition dem-onstrated several abnormalities. These included mild liverfunction and marked creatine kinase (CK) abnormalities(probably caused by agitation and associated muscletrauma). The highest levels, documented on November 18,were as follows: CK, 6,267 U/L; LDH, 2247U/L; total bil-irubin, 1.4 mg/dL; unconjugated bilirubin, 0.9 mg/dL;SGOT, 171.These abnormalities resolved gradually over theremaininghospitalization. Several ECGs obtained during thecourse of hospitalization demonstrated no abnormalities inrhythm or conduction.
METHODS
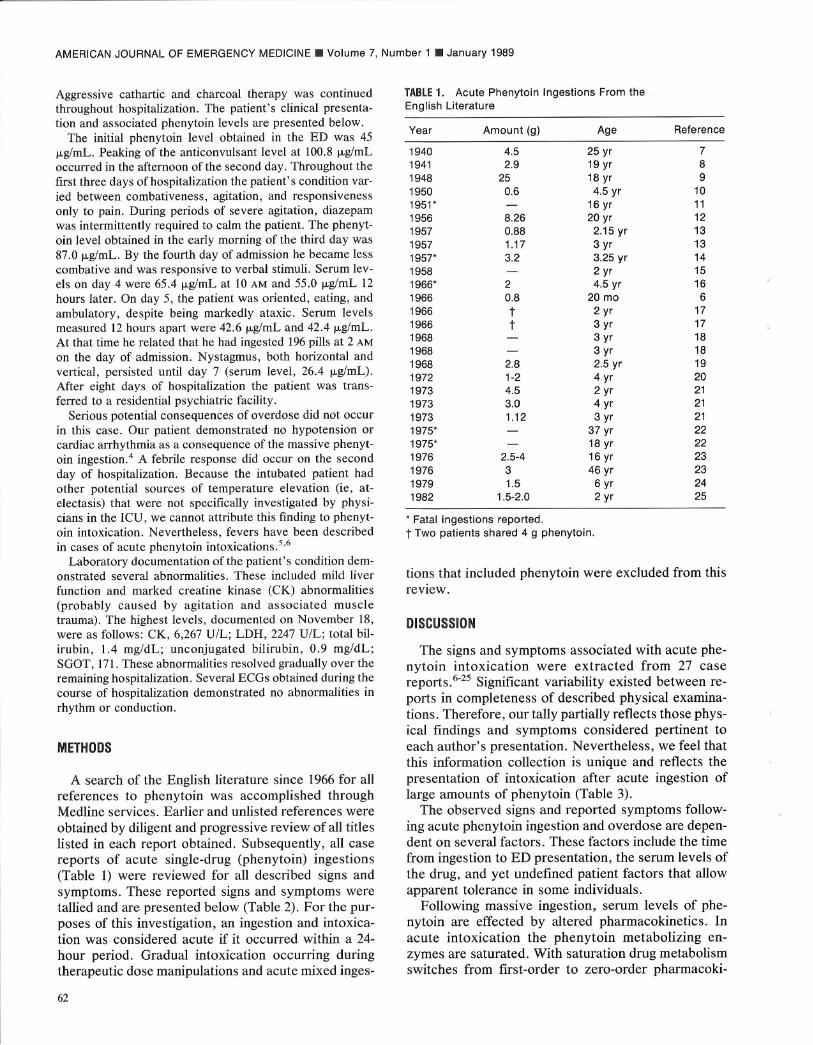
A search of the English literature since 1966for allreferences to phenytoin was accomplished throughMedline services. Earlier and unlisted references wereobtained by diligent and progressive review of all titleslisted in each report obtained. Subsequently, all casereports of acute single-drug (phenytoin) ingestions(Table 1) were reviewed for all described signs andsymptoms. These reported signs and symptoms weretallied and are presented below (Table 2). For the pur-poses of this investigation, an ingestion and intoxica-tion was considered acute if it occurred within a 24-hour period. Gradual intoxication occurring duringtherapeutic dose manipulations and acute mixed inges-
62
TABLE1. AcutePhenytoin Ingestions From theEnglish Literature
" Fatal ingestions reported.t Two patients shared 4 g phenytoin.
tions that included phenytoin were excluded from thisreview.
DISCUSSION
The signs and symptoms associated with acute phe-nytoin intoxication were extracted from 27 casereports.6-25Significant variability existed between re-ports in completeness of described physical examina-tions. Therefore, our tally partially reflects those phys-ical findings and symptoms considered pertinent toeach author's presentation. Nevertheless, we feel thatthis information collection is unique and reflects thepresentation of intoxication after acute ingestion oflarge amounts of phenytoin (Table 3).
The observed signs and reported symptoms follow-ing acute phenytoin ingestion and overdose are depen-dent on several factors. These factors include the timefrom ingestion to ED presentation, the serum levels ofthe drug, and yet undefined patient factors that allowapparent tolerance in some individuals.
Following massive ingestion, serum levels of phe-nytoin are effected by altered pharmacokinetics. Inacute intoxication the phenytoin metabolizing en-zymes are saturated. With saturation drug metabolismswitches from first-order to zero-order pharmacoki-
Year Amount (g) Age Reference
1940 4.5 25 yr 71941 2.9 19 yr 81948 25 18 yr 91950 0.6 4.5 yr 101951" - 16 yr 111956 8.26 20 yr 121957 0.88 2.15 yr 131957 1.17 3 yr 131957" 3.2 3.25 yr 141958 - 2 yr 151966" 2 4.5 yr 161966 0.8 20 mo 61966 t 2 yr 171966 t 3 yr 171968 - 3 yr 181968 - 3 yr 181968 2.8 2.5 yr 191972 1-2 4 yr 201973 4.5 2 yr 211973 3.0 4 yr 211973 1.12 3 yr 211975" - 37 yr 221975" - 18 yr 221976 2.5-4 16 yr 231976 3 46 yr 231979 1.5 6 yr 241982 1.5-2.0 2 yr 25
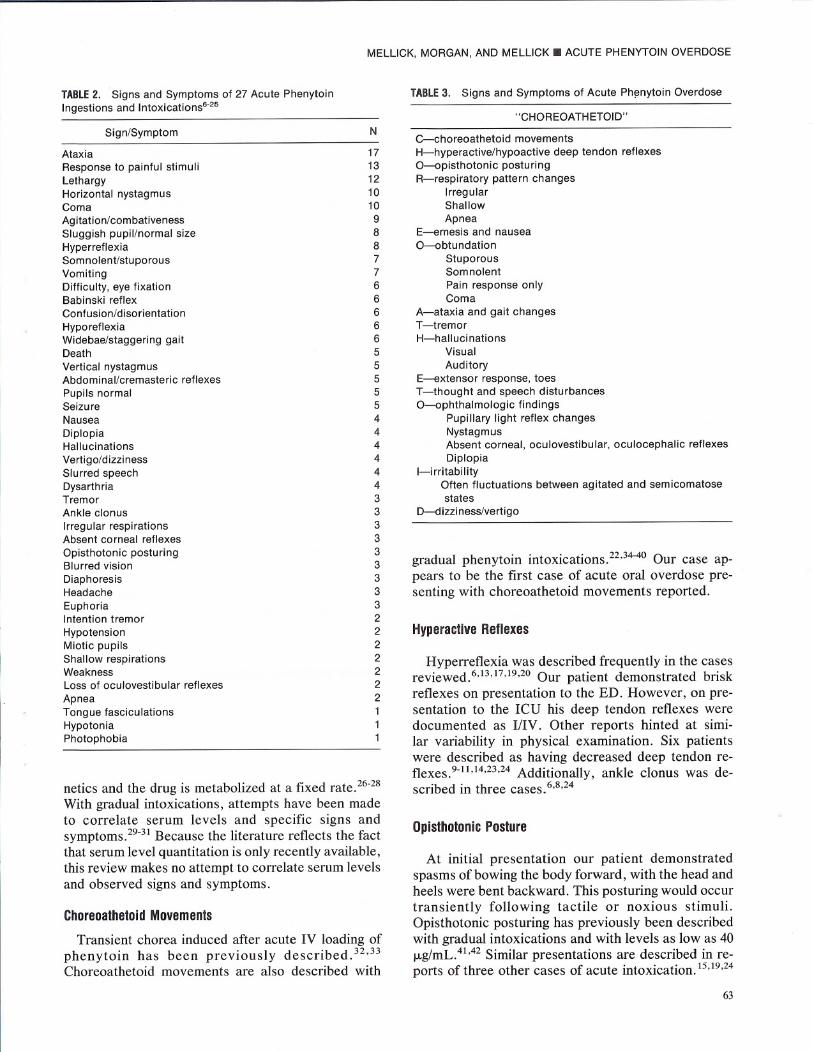
TABLE2. Signs and Symptoms of 27 Acute PhenytoinIngestions and Intoxications6-25
Sign/Symptom
AtaxiaResponse to painful stimuliLethargyHorizontal nystagmusComaAgitation/combativenessSluggish pupil/normal sizeHyperreflexiaSomnolent/stuporousVomitingDifficulty, eye fixationBabinski reflexConfusion/disorientationHyporeflexiaWidebae/staggering gaitDeathVertical nystagmusAbdominal/cremasteric reflexesPupils normalSeizureNauseaDiplopiaHallucinations
Vertigo/dizzinessSlurred speechDysarthriaTremorAnkle clonus
Irregular respirationsAbsent corneal reflexesOpisthotonic posturingBlurred vision
DiaphoresisHeadacheEuphoriaIntention tremorHypotensionMiotic pupilsShallow respirationsWeaknessLoss of oculovestibular reflexesApneaTongue fasciculationsHypotoniaPhotophobia
netics and the drug is metabolized at a fixed rate.26-28With gradual intoxications, attempts have been madeto correlate serum levels and specific signs andsymptoms.29-31Because the literature reflects the factthat serum level quantitation is only recently available,this review makes no attempt to correlate serum levelsand observed signs and symptoms.
ChoreoathetoidMovements
Transient chorea induced after acute IV loading ofphenytoin has been previously described. 32,33Choreoathetoid movements are also described with
MELLICK, MORGAN, AND MELLICK. ACUTE PHENYTOIN OVERDOSE
TABLE3. Signs and Symptoms of Acute Ph~nytoin Overdose
,'CHOREOATHETOID"N
17131210109887766666555554444443333333332222222111
C-choreoathetoid movementsH-hyperactive/hypoactive deep tendon reflexesO-opisthotonic posturingR-respiratory pattern changes
IrregularShallowApnea
E-emesis and nauseaO-obtundation
StuporousSomnolentPain response onlyComa
A-ataxia and gait changesT-tremorH-hallucinations
VisualAuditory
E-extensor response, toesT-thought and speech disturbancesO-ophthalmologic findings
Pupillary light reflex changesNystagmusAbsent corneal, oculovestibular, oculocephalic reflexesDiplopia
I-irritabilityOften fluctuations between agitated and semicomatosestates
D-dizziness/vertigo
gradual phenytoin intoxications.22.34-4oOur case ap-pears to be the first case of acute oral overdose pre-senting with choreoathetoid movements reported.
HyperactiveReflexes
Hyperreflexia was described frequently in the casesreviewed.6,13.17.19,20Our patient demonstrated briskreflexes on presentation to the ED. However, on pre-sentation to the ICU his deep tendon reflexes weredocumented as IIIV. Other reports hinted at simi-lar variability in physical examination. Six patientswere described as having decreased deep tendon re-flexes.9-1l,14.23,24Additionally, ankle clonus was de-scribed in three cases. 6,8,24
OpisthotonicPosture
At initial presentation our patient demonstratedspasms of bowing the body forward, with the head andheels were bent backward. This posturing would occurtransiently following tactile or noxious stimuli.Opisthotonic posturing has previously been describedwith gradual intoxications and with levels as low as 40JJ.g/mL.41,42Similar presentations are described in re-ports of three other cases of acute intoxication.15.19,24
63

AMERICAN JOURNAL OF EMERGENCY MEDICINE. Volume 7, Number 1 . January 1989
RespiratoryPatternChanges
Irregular and shallow respirations were described inthree and two patients, respectively. 13,15,19Our patientdemonstrated very shallow respirations and arterialblood gas findings consistent with a mild ventilatorydeficiency. Apnea resulting in a fatal CNS insult wasreportedfollowingan isolatedphenytoinoverdose.16
Emesis
Vomiting was a dominant finding in our patient'spresentation. A gag stimulus considered minimal re-sulted in prolonged retching, Other reports indicatethat vomiting is common following acute phenytoinintoxication.8,9,12-14,16,20Nausea was described in fourcase reports,8-10,12
Obtundation
Mental status changes were frequently reportedin the literature, A spectrum of changes weredescribed, commonly occurring in individual patients.Descriptive terminology included the following: leth-argy6,7,13-15,17,20,2\ responsive only to painfulstimuli 11,13-17,19,21,23-25;comatose7, 11,16,19,23,24,43;andsomnolent or stuporous.l0,17,20,21,23-25Our patientdemonstrated similar changes in level of conscious-ness. Even at the highest documented levels responseto painful stimuliwas described. However, applicationof the Glasgow Coma Scale to the reported patientswould have provided greater descriptive consistencyand clarity. Of special significance for the evaluationof comatose patients was the reported losses of ocu-locephalic, oculovestibular, and corneal reflexes in pa-tients reported by Spector et ae3 and absent cornealreflexes reported by Tenckhoff et al.19Unfortunately,these examinations were not performed or docu-mented in most of the cases reported.
Seizures associated with gradual phenytoin toxicityhave been reported,28,44,45,46Five patients with acuteintoxication had evidence of transient seizureactivity.6,14,15,21,24However, the relationship betweenseizures and phenytoin toxicity in these patients is notclear. One patient had seizures associated with fever;in fact, in this case the phenytoin was administeredacutely and at excessive doses because of the onset ofseizures with a high fever, At admission the patienthad a temperature of 105°F.6Another patient had whatwas thought to be a seizure 48 hours after overdose.This 6-year-old girl with marked opisthotonic postur-ing had a "generalized tonic spasm. ,,24Another childwith uncontrollable seizures while on chronic phenyt-oin administration had seizures 15 to 18 hours afteradmission for a fatal overdose. 14True seizure activity
64
verified by EEG studies occurred in a two-year-oldboy withno previoushistoryof seizures.15 Duringtheprevious day this patient had experienced hypotensionfollowing dialysis, which was treated with levartere-nol. Later in the hospitalization he was reported to behyponatremic. Another patient with no previous his-tory of seizures was described by his mother as havingquick, generalized jerking movements just before hispresentation for admission. No other evidence or ver-ificationof a possibleseizureevent was available.21
Ataxia
This finding was most frequently documented.Ataxia occurred in 17of the reported acute phenytoinintoxications.6,8-10,12,13,16-21,23This finding is com-monly reported in cases of gradual intoxication. In an-other six cases a wide-base or staggering gait wasdescribed.8,10,12,13,20,24
Tremor
"Tremor" was described in three cases.8,10,24An-other two patients demonstrated intention tremor.9,12
Hallucinations
Auditory or visual hallucinations were reported infour cases. 10,12,13,18
ExtensorToe Responses
The presence of a Babinski reflex was reported rel-atively frequently. 9,13,19,24Our patient demonstratedan extensor toe response at the time of presentation tothe ED. Babinski reflexes have also been reportedwith gradual intoxication.42
Thoughtand Speech Disturbances
A euphoric state was described in three of 27patients8,9,12;while confusion or disorientation wasdocumented in reports of six cases. S,10,13,18Speech ab-normalities, such as slurred speechS-l0,12 anddysarthria,8,12,23were not infrequent findings.
OphthalmologicDisturbances
Information useful in the differential evaluation ofcomatose patients is that pupil size was most com-monly normal and that light reflexes were eithersluggish,6,7,12,13,18,19,21,23 absent,14 or nor-maI.7,10,13,19,21Miotic pupils were described in two ofthe 27 patients.ll,16 Interestingly, both of the patientswith miotic pupils died. A third death14was reportedin a patient described as having absent pupillary re-flexes. We might speculate that miosis either resulted

from an unknown mixed ingestion or was a conse-quence of therapeutic interventions in these patients.The other and less clear alternative is that miosis oc-curs at more toxic serum levels of phenytoin.
Diplopia was reported in four patients,8,9,12,19whereas difficulty with eye fixation was reported inSiX.8,12,23,24As mentioned previously, opthalmoplegiahas been described with acute oral and IV intoxica-tions.Z3 Blurred vision was also reported.8,10,12
Descriptions of nystagmus are common in reports ofchronic intoxication.43,47,48This finding was also com-mon in cases of acute intoxication. Horizontal and ver-tical nystagmus was present in our patient. Horizontalnystagmus occurred in ten patients,8,IZ,13,ZO,ZI,Z3andvertical nystagmus was documented in five.6,9,IZ,19Asin our patient, bidirectional nystagmus was often seenin the same patient.6,9,IZ,19
Irritability
Irritability, agitation, or combativeness was de-scribed in nine patients.lO,IZ,13,15,16,ZO,ZI,Z3On arrival atthe ED our patient demonstrated marked agitation inresponse to minimalexternal stimuli. Simple touchingalone would result in choreoathetoid movements andopisthotonic posturing. Additionally, his hospitalcourse was characterized by intermittent agitation re-quiring the use of restraints. At other times the patientwas responsive only to painful stimuli. Diazepam wasused intermittently by physicians in the ICU duringperiods of extreme agitation; we are unable to delin-eate its exact role in the patient's clinical presentation.Nevertheless, other reports (of cases in which diaze-pam was not used) implied similar fluctuations be-tween agitated and depressed mental states.
Dizziness
Dizziness or vertigo was reported in four cases.7-9,18Our patient also complained of dizziness.
Death
Our patient survived following a massive ingestion;however, deaths are reported in the literature.ll,14,16,ZZA review of these cases suggests that therapeutic in-terventions or limited capabilities for monitoring andsupport of metabolic and respiratory complicationsmay have had a role in the outcome. Large doses ofamphetamine (2.88g), caffeine (72g), and nikethamide(144 g) were administered in one patient who devel-oped cardiac irritability and ventricular arrhythmia be-fore death. II In the second case (patient aged 3 years,4 months), reported in 1956, a total 375 mg caffeinewas administered early in the hospitalization. This pa-tient died quietly 34 hours after ingestion of 3.2 g phe-nytoin (220mg/kg).The report does not describe mon-
MELLICK, MORGAN, AND MELLICK. ACUTE PHENYTOIN OVERDOSE
itoring or documentation of metabolic or respiratorystatus. Supportive measures included IV fluid, gammaglobulin, and antibiotic administration. Documenta-tion of the mechanism of death, as well as descriptionsof attempted resuscitative interventions, are absentfrom the report. 14The third death, reported in 1966,occurred in a 4.5-year-old girl who ingested 2 g phe-nytoin. After 48 hours an episode of apnea occurredand the patient was intubated. Subsequently, she wastransferred to a university hospital where her pupilswere noted to be fixed and dilated. Because of "irre-versible brain damage," the respirator was eventuallystopped and the patient died.16
Other deaths following phenytoin overdoses havebeen described more recently. Coutselinis et al verybriefly report two adults (aged 37 and 18 years) onchronic therapy who were found dead and had post-mortem blood levels of 45 and 48 ,...g/mL.zzThe Na-tional Capital Poison Center has also reported deathsfollowing acute ingestions of phenytoin.49-51Impor-tantly, all three of these ingestions were associatedwith other chemical substances or drugs. The 1983re-port describes an adult who ingested phenytoin, phe-nobarbital, and carbamazepine.49 The adult death re-ported in the 1984report also involved phenobarbitaland carbamazepine.50 In the 1985 summary a 3-year-old boy died following the ingestion of six ormore phenytoin capsules. However, the patient's tox-icology screen also demonstrated benzyl alcohol. As-sociated metabolic derangements were also signifi-cant. Laboratory findings included sodium, 125mEq/L; potassium, 2.9 mEq/L; arterial pH, 7.3; and PCOz,30 mmHg. Diabetes insipidus developed 24 hourspostingestion.51 Nevertheless, 6,826 nonfatal expo-sures to phenytoin were reported over 4 years.49-52
Our patient survived with only supportive care fol-lowing the reported ingestion of 196 phenytoin cap-sules (100mg each). This dosage could not be verifiedbeyond the 150capsules definitely known to be in thepatient's possession. If the patient's account is accu-rate, the amount ingested was 392 mg/kg. However,the amount of phenytoin vomited shortly after inges-tion and following presentation to the ED is unknown.If emesis had not lowered the total phenytoin load andthe patient had not been discovered so soon after in-gesting the drug, a different presentation and outcomemight have occurred. However, survival has been re-ported after a mixed acute ingestion including 21 gphenytoin5 and after a pure ingestion of 25g.9Our casereport supports phenytoin's reputation for relativelymild toxicity and successful therapeutic outcomes de-spite large oral ingestions.
CONCLUSION
In order to better delineate the many signs andsymptoms that develop following ingestion of large
65
AMERICAN JOURNAL OF EMERGENCY MEDICINE. Volume 7, Number 2. March 1989
amounts of phenytoin a review of the literature wasperformed. Our review demonstrated that the mostcommon signs and symptoms are ataxia, nystagmus,hyperreflexia, vomiting, Babinski reflexes, disorienta-tion, normal pupillary size with sluggish light reflexes,and central signs of both combativeness and markedmental status depression. Additionally, we describedthe presence of choreoathetoid movements and veri-fied previous reports of opisthotonic posturing in casesof acute phenytoin ingestion and intoxication. We alsohighlighted the previously reported losses of oculo-cephalic, oculovestibular, and corneal reflexes follow-ing acute intoxications. In addition, we questionedwhether phenytoin toxicity had any role in causing oraggravatingseizure activity. Finally, we described oneof the largest acute phenytoin ingestions, with subse-quent survival, reported to date. Our information sup-ports phenytoin's reputation for minimal mortality orlong-term morbidity.
REFERENCES
1. Merritt HH, Putnam TJ: Sodium diphenyl hydantoinate in thetreatment of convulsive disorders. JAMA 1938;111:1068-1073
2. Kimball OP, Horan TN: The use of Dilantin in the treatmentof epilepsy. Ann Intern Med 1939;13:787-793
3. Frankel SI: Dilantin sodium in the treatment of epilepsy.JAMA 1940;114:1320-1321
4. Blumsohn D, Seabrook M: Oral diphenylhydantoin sodiumand cardiovascular toxicity. S Afr Med J 1970;44:1207-1208
5. Theil GB, Richter RW, Powell MR, et al: Acute Dilantin poi-soning. Neurology 1961;11:138-142
6. Klein JP: Diphenylhydantoin intoxication associated withhyperglycemia. J Pediatr 1966;69:463-465
7. Robinson LJ: Case of acute poisoning from Dilantin sodiumwith recovery. JAMA 1940;115:289-290
8. Aring CD, Rosenbaum M: Ingestion of large doses of Dilan-tin sodium. Arch Neurol Psychiatry 1941;45:265-270
9. Nauth-Misir TN: A case of gross overdosage of soluble phe-nytoin. Br Med J 1948;2:646
10. Price WC, Frank ME: Accidental acute Dilantin poisoning:Report of a case with complete recovery in a nonepilepticchild. J Pediatr 1950;36:652-655
11. Tichner JB, Enselberg CD: Suicidal Dilantin (sodium diphe-nylhydantoin) poisoning: A case report. N Engl J Med1951;245:723-725
12. Grosz HJ: Dilantin intoxication-With a report of one case.Am Pract Digest Treat 1956;7:1633-1636
13. Moling JH, Posch JJ: Acute diphenylhydantoin intoxication.Pediatrics 1957;20:877-880
14. Petty CS, Muelling RJ, Sindell HW: Accidental, fatal poison-ing with diphenylhydantoin (Dilantin). J Forensic Sci1957;2:279-286
15. Schreiner GE: Hemodialysis in acute poisoning. Arch InternMed 1958;102:896-913
16. Laubscher FA: Fatal diphenylhydantoin poisoning: A casereport. JAMA 1966;198:1120-1121
17. Schulte CJ, Good TA: Acute intoxication due to methsuxi-mide and diphenylhydantoin. J Pediatr 1966;68:635-637
18. Patel J, Crichton JU: The neurologic hazards of diphenylhy-dantoin in childhood. J Pediatr 1968;73:676-684
66
19. Tenckhoff H, Sherrard DJ, Hickman RO, et al: Acute diphe-nylhydantoin intoxication. Am J Dis Child 1968;116:422-425
20. Holcomb R, Lynn R, Harvey B, et al: Intoxication with 5,5-diphenylhydantoin (Dilantin). J Pediatr 1972;80:627-632
21. Wilder BJ, Buchanan RA, Serrano EE: Correlation of acutediphenylhydantoin intoxication with plasma levels andmetabolite excretion. Neurology 1973;23:1329-1332
22. Coutselinis A, Dimopoulos G, Varsami P: Fatal intoxicationwith diphenylhydantoin: Report of two cases. ForensicSci 1975;6:131-133
23. Spector RH, Davidoff RA, Schwartzman RJ: Phenytoin-induced ophthalmoplegia. Neurology 1976;26:1031-1034
24. Wilson JT, Huff JG, Kilroy AW: Prolonged toxicity followingacute phenytoin overdose in a child. J Pediatr 1979;95:135-138
25. Lindahl S, Westerling D: Detoxification with peritoneal dial-ysis and blood exchange after diphenylhydantoin intoxi-cation. Acta Paediatr Scand 1982;71:665-666
26. Haddad LM, Winchester J (eds): Clinical Management ofPoisoning and Drug Overdose. Philadelphia, Saunders,1983
27. Gill MA, Kern JW, Kane KJ, et al: Phenytoin overdose kinet-ics. West J Med 1978;128:246-248
28. Atkinson AJ, Shaw JM: Pharmacokinetic study of patientwith diphenylhydantoin toxicity. Clin Pharmacol Ther1973;14:521-528
29. Kutt H, Winters W, Fletcher M: Diphenylhydantoin metabo-lism, blood levels, and toxicity. Arch Neuro11964;11 :642-648
30. Gerber N, Lynn R, Oates J: Acute intoxication with 5,5-diphenylhydantoin (Dilantin) associated with impairmentof biotransformation: Plasma levels and urinary metabo-lites; and studies in healthy volunteers. Ann Intern Med1972;77:765-771
31. Booker HE, Darcey B: Serum concentrations of free diphe-nylhydantoin and their relationship to clinical intoxica-tion. Epilepsia (Amst) 1973;14:177-184
32. Filloux F, Thompson JA: Transient chorea induced by phe-nytoin. J Pediatr 1987;110:639-641
33. Howie DL, Crumrine PK: Phenytoin-induced movement dis-order associated with intravenous administration for sta-tus epilepticus. Clin Pediatr 1985;24:467-469
34. Rosenblum E, Rodichok L, Hanson P: Movement disorder asa manifestation of diphenylhydantoin toxicity. Pediatrics1974;54:364-366
35. Ahmad S, Laidlaw J, Haughton GW, et al: Involuntary move-ments caused by phenytoin intoxication in epileptic pa-tients. J Neurol Neurosurg Psychiatry 1975;38:225-231
36. Chalhub EG, DeVivo DC: Phenytoin-induced choreoatheto-sis. J Pediatr 1976;89:153-154
37. Krishnamoorthy KS, Zalneraitis EL, Young RSK, et al: Phe-nytoin-induced choreoathetosis in infancy: Case reportsand a review. Pediatrics 1983;72:831-834
38. Shuttleworth E, Wise G, Paulson G: Choreoathetosis anddiphenylhydantoin intoxication. JAM A 1974;230:1170-1171
39. Chadwick D, Reynolds EH, Marsden CD: Anticonvulsant-induced dyskinesias: A comparison with dyskinesias in-duced by neuroleptics, J Neurol Neurosurg Psychiatry1976;39:1210-1218
40. Nausieda PA, Koller WC, Klawano HL, et al: Phenytoin andchoreic movements. N Engl J Med 1978;298:1093-1094
41. Kooiker JC, Sumi SM: Movement disorder as a manifesta-tion of diphenylhydantoin intoxication. Neurology 1974;24:68-71
42. Jan JE, Kliman MR: Extrapyramidal disturbance and vascu-lar changes during diphenylhydantoin intoxication. CanMed Assoc 1974;111:636-641
43. Nozue M, Mizuno M, Kaga K: Neurotological findings in di-phenylhydantoin intoxication. Ann Otolaryngol 1973;82:389-394
44. Kutt H, Winters W, Scherman R, et al: Diphenylhydantoinand phenobarbital toxicity. Arch Neuro11964;11 :649-656
45. Ivanainen M, Viukari M: Serum-phenytoin, seizures, andelectroencephalography. Lancet 1977;16:860
46. Levy LL, Fenichel GM: Diphenylhydantoin activated sei-zures. Neurology 1965;15:716-722
47. Riker WK, Downes H, Olsen GO, et al: Conjugate lateral gazenystagmus and free phenytoin concentrations in plasma:Lack of correlation. Epilepsia 1978;19:93-98
MELLICK, MORGAN, AND MELLICK. ACUTE PHENYTOIN OVERDOSE
48. Campbell W: Periodic alternating nystagmus in phenytoinintoxication. Arch NeuroI1980;37:178-180
49. Litovitz T, Veltri J: 1983 annual report of the American As-sociation of Poison Control Centers national data collec-tion systems. Am J Emerg Med 1984;3:423-450
50. Litovitz T, Normann So Veltri J: 1984 annual report of theAmerican Association of Poison Control Centers nationaldata collection systems. Am J Emerg Med 1985;4:427-458
51. Litovitz T, Martin T, Schmitz B: 1985 annual report of theAmerican Association of Poison Control Centers nationaldata collection systems. Am J Emerg Med 1986;5:405-445
52. Veltri J, Litovitz T: 1982 annual report of the American As-sociation of Poison Control Centers national data collec-tion systems. Am J Emerg Med 1983;2:420-443
67















![[Product Monograph Template - Standard] · PRODUCT MONOGRAPH . PrDILANTIN® (30 mg Extended Phenytoin Sodium Capsules, Manufacturer Standard) (100 mg Extended Phenytoin Sodium Capsules](https://static.fdocuments.in/doc/165x107/5bd5671d09d3f2733e8b8a3f/product-monograph-template-standard-product-monograph-prdilantin-30.jpg)


