Presentation1.pptx, ultrasound examination of the 1st trimester pregnancy.
65
ULTRASOUND EXAMINATION OF THE 1 ST TRIMESTER. Dr/ ABD ALLAH NAZEER. MD.
-
Upload
abdellah-nazeer -
Category
Documents
-
view
1.092 -
download
2
Transcript of Presentation1.pptx, ultrasound examination of the 1st trimester pregnancy.
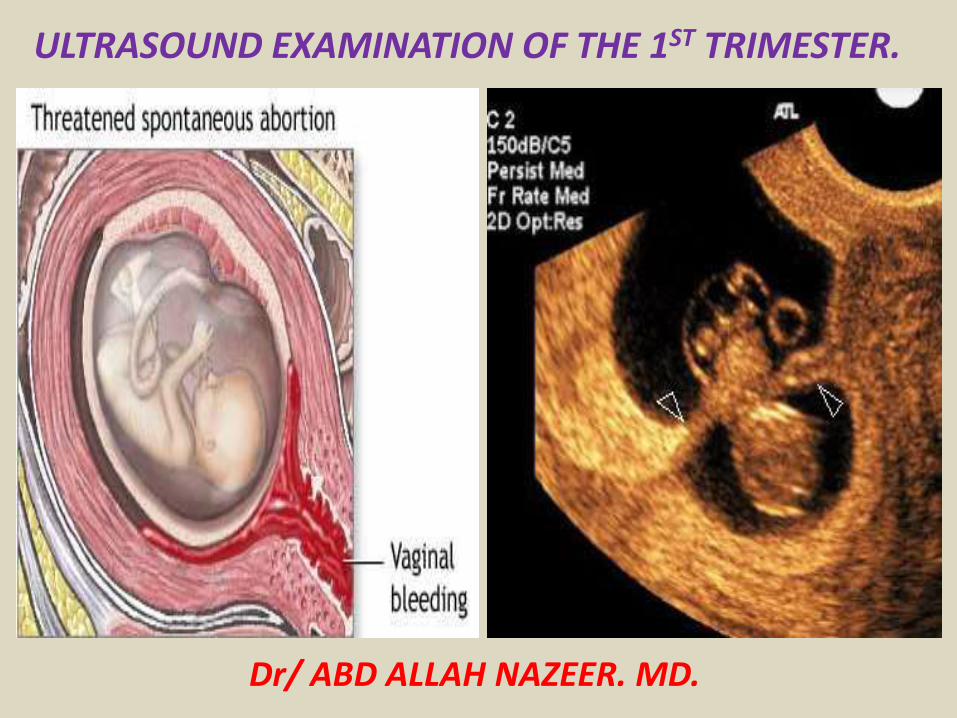
ULTRASOUND EXAMINATION OF THE 1ST TRIMESTER
Dr ABD ALLAH NAZEER MD
FIRST TRIMESTER ULTRASOUND - Normal1ST TRIMESTER ULTRASOUND PROTOCOL
ROLE OF ULTRASOUNDUltrasound is essentially used for assessing gestational age current viability and maternal wellbeing Ultrasound is a valuable diagnostic tool in assessing the following indicationsUnsure of DatesVaginal BleedingPelvic PainExclude an ectopic pregnancyMaternal past historyThreatened MiscarriageNuchal Translucency (11-14 weeks CRL 45-84mm)Patient HistoryGravidityParity (Miscarriage Termination of Pregnancy (TOP))Fertility treatmentDate of Last Menstrual PeriodOther pregnancy HistoryGynecological History
EQUIPMENT SELECTION AND TECHNIQUEModern ultrasound unitCurved linear probe approx 3-7 MHz depending upon maternal factorsTransvaginal probe approx 5-9 MHz (Use of non-latex cover if required)Ensure patient comfort and privacyWarm gel clean towels etcSelect Obstetric preset for appropriate power levels and measurement packagesUse a curvilinear probe (35-6MHZ) with low power to reduce risk of biological effects use of Doppler should be avoided in the 1st trimesterSCANNING TECHNIQUEPATIENT PREPARATION2 hours before the appointment time empty your bladder Over the next hour drink at least 1 liter of water and do not go to the toilet until instructed
lt10 weeks Cervix - assess if closed and measure length between internal and external osLook for bright trophoblastic reaction around sacAssess placental location and distance from internal os (may lie close to os at this stage)Check for retroplacental hemorrhages placental masses etcAssess maternal ovaries adnexae and Pouch Of Douglas (POD)Confirm presence of intrauterine gestation and numberIf multiple pregnancy confirm number of fetuses number of sacs and number of placentas present to determine chorionicity ie MonochorionicMonoamnionic (MCMA)MonochorionicDiamnionic(MCDA)Dichorionic Diamnionic (DCDA)Confirm heart beat(s) amp rate with M-Mode only (Use of Colour or Doppler traces is not recommended in the 1st trimester)Measure CRL to calculate gestational age and Estimated Date of Delivery(EDD)If too early to see the fetal pole measure the average sac diameter
A 1st trimester series should include the following minimum imagesUterus - long transBoth ovariesAdnexaeCervix and Pouch-Of-DouglasGestational sac - Long amp TransYolk sac if visibleFetal poleM mode fetal heartDocument the normal anatomy Any pathology found in 2 planes including measurements
GESTATIONAL SACThe gestational sac(GS) is the earliest sonographic finding in pregnancy It will be difficult to see if the mother has a retroverted uterus or fibroids The GS is an echogenic ring surrounding an anechoic centre An ectopic pregnancy will appear the same but it will not be within the endometrial cavity The GS is not identifiable until approximately 4 12 weeks with a transvaginal scanGestational sac size should be determined by measuring the mean of three diameters These differences rarely effect gestational age dating by more than a day or twoThe following image is using a transvaginal approach the gestational sac can be seen during week 4-5
5 week gestation Yolk Sac Only seen The yolk sac will be visible before a clearly definable embryonic pole
Mean Sac Diameter measurement is used to determine gestational age before a Crown Rump length can be clearly measured The average sac diameter is determined by measuring the length width and height then dividing by 3
The very early embryonic heart will be a subtle flicker This may be measured using M-Mode(avoid Doppler in the first trimester due to risks of bioeffects)Initially the heart rate may be slow
The Crown Rump Length (CRL) measurement in a 6 week gestation A mass of fetal cells separate from the yolk sac first becomes apparent on transvaginal ultrasound just after the 6th week of gestation This mass of cells is known as the fetal pole
YOLK SACThe yolk sac appears during the 5th week It is the second structure to appear after the GS It should be round with an anechoic centre It should not be calcified misshapen or gt5mm from the inner to inner diameter Yolk sacs larger than 6 mm are usually indicative of an abnormal pregnancy Failure to identify (with transvaginal ultrasound) a yolk sac when the gestational sac has grown to 12 mm is also usually indicative of a failed pregnancy
HEART BEATUsing a transvaginal approach the fetal heart beat can be seen flickering before the fetal pole is even identified It will be seen alongside the yolk sac It may be below 100 beats per minute but this will increase to between 120- 180 beats per minute by 7 weeks In the early scans at 5-6 weeks just visualizing a heart beating is the important thing Failure to identify fetal cardiac activity in a fetus whose overall length is greater than 4 mm is an ominous signSometimes there is difficulty distinguishing between the maternal pulse and fetal heart beat Often technicians will take the mothers pulse at the same time to check if it is the fetus or the mothers
CROWN RUMP LENGTH (CRL)The CRL is a reproducible and accurate method for measuring and dating a fetusEarly ultrasonographers used this term (CRL) because early fetuses also adopted the sitting in the chair posture in early pregnancy After 12 weeks the accuracy of CRL in predicting gestational age diminishes and is replaced by measurement of the fetal biparietal diameter In at least some respects the term crown rump length is misleadingThere is no fetal crown and no fetal rump to measure for most of the first trimester Until 53 days from the LMP the most caudad portion of the fetal cell mass is the caudal neurospone followed by the tail Only after 53 days is the fetal rump the most caudal portion of the fetusUntil 60 days from the LMP the most cephalad portion of the fetal cell mass is initially the rostral neurospore and later the cervical flexure After 60 days the fetal head becomes the most cephalad portion of the fetal cell massWhat is really measured during this early development of the fetus is the longest fetal diameterFrom 6 weeks to 9 12 weeks gestational age the fetal CRL grows at a rate of about 1 mm per day
Measure the crown rump length(CRL) to estimate gestational age
At 10 weeks visualize 4 jointed limbs feet and hands
NUCHAL TRANSLUCENCY
From 12 weeks the basic morphology of the fetus is visible
The Nuchal Translucency is used to provide a risk assessment for chromosomal abnormalities specifically Trisomies 1318 and 21 (Downs Syndrome)
The legs are usually crossed at the ankles Confirm the presence and symmetry of the long bones
The correct angle the feet to legs can be confirmed They should be at 90 degrees ie perpendicular or Talipes should be suspected
The humerus radius and ulna and the presence of hands areimaged from 11 weeks
12 week choroids take up most of the space within the ventricles
TWINS Initially twins may be identified as 2 separate gestational sacs (ie diamniotic dichorionic) They may be 2 fetal poles within the same gestational sac (monochorionic) It is easier to determine chorionicity earlier in the pregnancy depending on the chorionicity and amnionicityIt is a sad situation when a vanishing twin occurs which is about 20 of twin pregnancies In these cases one of the twins fails to grow and thrive Instead its development arrests and it is reabsorbed with no evidence at delivery of the twin pregnancy
Monoamniotic Twins Dichorionic diamniotic Twins
TRIPLETS
Triplets with 2 sacs Monoamniotic monochorionic twins and a normal single
GRAPHS TO DETERMINE GESTATIONAL AGEDepending on the age of the gestation these graphs can be used to determine the correct EDD
Mean Sac Diameter measurement is used to determine gestational age before a Crown Rump length can be clearly measured The average sac diameter is determined by measuring the length width and height then dividing by 3
Once a fetal Pole can be visualized the CRL measurement is the most accurate method for dating the pregnancy
COMMON PATHOLOGYThickened Nuchal Translucency(NL)Partial Ovular DetachmentRetained products of conceptionAnembryonic GestationGestational trophoblastic diseaseMiscarriageEctopic PregnancySubchorionic hemorrhageConjoined TwinsAntepartum HemorrhageCheck heart beatCheck causes of bleeding
Thickened Nuchal Translucency (NT)
bull One of the parameters used in sequential screening (SS) for Downrsquos syndrome in first trimester
ndash SS Pregnancy associated plasma protein levels hCG levels NT thickness
bull Measured during 11-14 wks gestational age
bull Seen on sagittal image as increased subcutaneous non-septated fluid in posterior fetal neck
bull Measurement gt3mm usually considered abnormal however exact cut off measurements are dependent on maternal agegestational age
bull Detection rate of screening for Downrsquos Syndrome in first trimester
ndash sequential screening with NT 82-87
ndash NT alone 64-70
Thickened Nuchal Translucency (NT)
Thickened Nuchal Translucency
PARTIAL OVULAR DETACHMENTThe maternal circulation inside the placenta starts peripherally (in the placental margins) and is associated to physiological oxidative phenomena that may lead to membranes rupture and formation The abnormal development of such membranes may result in subchorionic hemorrhage enhancing the predisposition to an adverse gestational outcome at the third trimester (PPROM and PTL)Such abnormality is common and also denominated as subchorionic hemorrhage or trophoblastic hematoma being visualized in more than 18 of cases of threatened miscarriage The presence of fetal heart activity confers an excellent prognosis Clinically subchorionic hemorrhage may course with vaginal bleeding At ultrasonography a crescent-shaped shadow is observed adjacent to the gestational sac with debris Gestational sac compression and consequential deformation may occur In most of cases a two-week follow-up evaluation confirms the hematoma resorption
Retained products of conception are characterized by a
thickened disorganized and heterogeneous endometrium with ill-defined mucosal layers and cavitary line either with or without the presence of gestational sac Clinically the women presents abdominal pain and relative vaginal bleeding(14) In the presence of an intact gestational sac and closed cervix the difficulty in a spontaneous resolution will be higher requiring surgical evacuation
Retained products of conception
Transvaginal sonography without (A) and with (B) color Doppler imaging in a case of RPC with endometrial expansion (arrows)
Images retained products conception
EARLY EMBRYO DEATHSome sonographic findings characterize an embryo death in the first half of the first trimester in early phases before the crown-rump length can be measured The following aspects are highlighted small hyperechoic yolk sac or hydropic yolk sac increased in volume with diameter gt 7 mm or even small amniotic cavity disproportionate to the gestational sac size Before the 9th week small gestational sac may be associated with aneuploidy
Failed early pregnancy
ANEMBRYONIC GESTATIONAt transvaginal ultrasonography the yolk sac should be visualized in a gestational sac with mean diameter gt 10 mm The absence of a yolk sac within the gestational sac with gt 10 mm in mean diameter or the absence of a yolk sac within the gestational sac with gt 16 mm in diameter characterize anembryonic gestation
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
GESTATIONAL TROPHOBLASTIC DISEASEThe typical sonographic finding in most of cases of complete hydatidiform mole is a echogenic intracavitary solid mass with intermingled small cystic loci resembling a snow storm corresponding to the vesicles that macroscopically characterize this condition The higher the gestational age the larger the vesicles visualized as homogeneous anechoic images increasing the method specificity The ultrasonography sensitivity will depend on the gestational age at the moment of the diagnosis Ultrasonography can detect vesicles with gt 2 mm in diameter In early pregnancies with trophoblastic disease the sonographic method accuracy is limited hindering the differentiation of gestational trophoblastic disease from other conditions involving the endometrial cavity
Partial hydatidiform mole offers higher diagnostic difficulty by ultrasonography In a reasonable number of cases this disease presents as an empty gestational sac corresponding to anembryonic gestation or as early embryo death However two criteria have been described in the literature gestational sac transverseanteroposterior diameter ratio gt 15 and cystic changes irregularity of increase in echogenicity of decidualplacenta or myometrial reaction
ECTOPIC PREGNANCYSonographic findings of ectopic pregnancy will vary as a function of the gestational age and site Classically the following sonographic findings are described tubal ring sign adnexal disorganized mass molded to the adnexa andor cul de sac solid organized mass with regular margins mimicking a pediculated myomatous nodule clinically progressing with low β-hCGlevels and presence of a live extrauterine conceptus Uncommon gestational sites may be observed such as abdominal ectopic pregnancy cervical ectopic pregnancy and ectopic pregnancy in a previous Cesarean section pregnancy
Subchorionic hemorrhage (SCH) occurs when there is
perigestational haemorrhage and blood collects between the uterine wall and the chorionic membrane in pregnancy It is a frequent cause of first and second trimester bleedingEpidemiologyIt typically occurs within the first 20 weeks of gestation If seen in the first 10-14 days of gestation they are also sometimes termed implantation bleedsRadiographic featuresUltrasound crescentic collection with elevation of the chorionic membranedepending on the time elapsed since bleeding the collection will have variable echotexture
acute hyperechoic and may be difficult to differentiate from adjacent chorionsubacute-chronic decreasing echogenicity with time
in almost all cases there is extension of the hematoma towards the margin of the placenta
First trimester SCH (subchorionic bleed)
First trimester SCH (subchorionic bleed)
Extensive hematoma in a woman with chronic bleeding
Subchorionic hemorrhage
Conjoined twins are a rare and complex complication of
monozygotic twinning which is associated with high perinatal mortality Early prenatal diagnosis of conjoined twins allows better counselling of the parents regarding the management options including continuation of pregnancy with post-natal surgery termination of pregnancy or selective fetocide in case of a triplet pregnancy With the introduction of high-resolution and transvaginal ultrasound imaging accurate prenatal diagnosis of conjoined twins is possible early in pregnancy Although first-trimester diagnosis of conjoined twins is feasible false-positive cases are common before 10 weeks because earlier in gestation fetal movements are limited and monoamniotic twins may appear conjoined As most parents opt for immediate termination of pregnancy at confirmation of the diagnosis there are limited data on the prenatal follow-up of conjoined twins detailed analysis of case reports where 3D imaging was used indicates that this modality does not improve on the diagnosis made by 2D ultrasound Overall very early prenatal diagnosis and first-trimester 3D imaging provide very little additional practical medical information compared to the 11-14 weeks ultrasound examination
Images of the conjoined twins there are two heads with conjoined body
Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You

FIRST TRIMESTER ULTRASOUND - Normal1ST TRIMESTER ULTRASOUND PROTOCOL
ROLE OF ULTRASOUNDUltrasound is essentially used for assessing gestational age current viability and maternal wellbeing Ultrasound is a valuable diagnostic tool in assessing the following indicationsUnsure of DatesVaginal BleedingPelvic PainExclude an ectopic pregnancyMaternal past historyThreatened MiscarriageNuchal Translucency (11-14 weeks CRL 45-84mm)Patient HistoryGravidityParity (Miscarriage Termination of Pregnancy (TOP))Fertility treatmentDate of Last Menstrual PeriodOther pregnancy HistoryGynecological History
EQUIPMENT SELECTION AND TECHNIQUEModern ultrasound unitCurved linear probe approx 3-7 MHz depending upon maternal factorsTransvaginal probe approx 5-9 MHz (Use of non-latex cover if required)Ensure patient comfort and privacyWarm gel clean towels etcSelect Obstetric preset for appropriate power levels and measurement packagesUse a curvilinear probe (35-6MHZ) with low power to reduce risk of biological effects use of Doppler should be avoided in the 1st trimesterSCANNING TECHNIQUEPATIENT PREPARATION2 hours before the appointment time empty your bladder Over the next hour drink at least 1 liter of water and do not go to the toilet until instructed
lt10 weeks Cervix - assess if closed and measure length between internal and external osLook for bright trophoblastic reaction around sacAssess placental location and distance from internal os (may lie close to os at this stage)Check for retroplacental hemorrhages placental masses etcAssess maternal ovaries adnexae and Pouch Of Douglas (POD)Confirm presence of intrauterine gestation and numberIf multiple pregnancy confirm number of fetuses number of sacs and number of placentas present to determine chorionicity ie MonochorionicMonoamnionic (MCMA)MonochorionicDiamnionic(MCDA)Dichorionic Diamnionic (DCDA)Confirm heart beat(s) amp rate with M-Mode only (Use of Colour or Doppler traces is not recommended in the 1st trimester)Measure CRL to calculate gestational age and Estimated Date of Delivery(EDD)If too early to see the fetal pole measure the average sac diameter
A 1st trimester series should include the following minimum imagesUterus - long transBoth ovariesAdnexaeCervix and Pouch-Of-DouglasGestational sac - Long amp TransYolk sac if visibleFetal poleM mode fetal heartDocument the normal anatomy Any pathology found in 2 planes including measurements
GESTATIONAL SACThe gestational sac(GS) is the earliest sonographic finding in pregnancy It will be difficult to see if the mother has a retroverted uterus or fibroids The GS is an echogenic ring surrounding an anechoic centre An ectopic pregnancy will appear the same but it will not be within the endometrial cavity The GS is not identifiable until approximately 4 12 weeks with a transvaginal scanGestational sac size should be determined by measuring the mean of three diameters These differences rarely effect gestational age dating by more than a day or twoThe following image is using a transvaginal approach the gestational sac can be seen during week 4-5
5 week gestation Yolk Sac Only seen The yolk sac will be visible before a clearly definable embryonic pole
Mean Sac Diameter measurement is used to determine gestational age before a Crown Rump length can be clearly measured The average sac diameter is determined by measuring the length width and height then dividing by 3
The very early embryonic heart will be a subtle flicker This may be measured using M-Mode(avoid Doppler in the first trimester due to risks of bioeffects)Initially the heart rate may be slow
The Crown Rump Length (CRL) measurement in a 6 week gestation A mass of fetal cells separate from the yolk sac first becomes apparent on transvaginal ultrasound just after the 6th week of gestation This mass of cells is known as the fetal pole
YOLK SACThe yolk sac appears during the 5th week It is the second structure to appear after the GS It should be round with an anechoic centre It should not be calcified misshapen or gt5mm from the inner to inner diameter Yolk sacs larger than 6 mm are usually indicative of an abnormal pregnancy Failure to identify (with transvaginal ultrasound) a yolk sac when the gestational sac has grown to 12 mm is also usually indicative of a failed pregnancy
HEART BEATUsing a transvaginal approach the fetal heart beat can be seen flickering before the fetal pole is even identified It will be seen alongside the yolk sac It may be below 100 beats per minute but this will increase to between 120- 180 beats per minute by 7 weeks In the early scans at 5-6 weeks just visualizing a heart beating is the important thing Failure to identify fetal cardiac activity in a fetus whose overall length is greater than 4 mm is an ominous signSometimes there is difficulty distinguishing between the maternal pulse and fetal heart beat Often technicians will take the mothers pulse at the same time to check if it is the fetus or the mothers
CROWN RUMP LENGTH (CRL)The CRL is a reproducible and accurate method for measuring and dating a fetusEarly ultrasonographers used this term (CRL) because early fetuses also adopted the sitting in the chair posture in early pregnancy After 12 weeks the accuracy of CRL in predicting gestational age diminishes and is replaced by measurement of the fetal biparietal diameter In at least some respects the term crown rump length is misleadingThere is no fetal crown and no fetal rump to measure for most of the first trimester Until 53 days from the LMP the most caudad portion of the fetal cell mass is the caudal neurospone followed by the tail Only after 53 days is the fetal rump the most caudal portion of the fetusUntil 60 days from the LMP the most cephalad portion of the fetal cell mass is initially the rostral neurospore and later the cervical flexure After 60 days the fetal head becomes the most cephalad portion of the fetal cell massWhat is really measured during this early development of the fetus is the longest fetal diameterFrom 6 weeks to 9 12 weeks gestational age the fetal CRL grows at a rate of about 1 mm per day
Measure the crown rump length(CRL) to estimate gestational age
At 10 weeks visualize 4 jointed limbs feet and hands
NUCHAL TRANSLUCENCY
From 12 weeks the basic morphology of the fetus is visible
The Nuchal Translucency is used to provide a risk assessment for chromosomal abnormalities specifically Trisomies 1318 and 21 (Downs Syndrome)
The legs are usually crossed at the ankles Confirm the presence and symmetry of the long bones
The correct angle the feet to legs can be confirmed They should be at 90 degrees ie perpendicular or Talipes should be suspected
The humerus radius and ulna and the presence of hands areimaged from 11 weeks
12 week choroids take up most of the space within the ventricles
TWINS Initially twins may be identified as 2 separate gestational sacs (ie diamniotic dichorionic) They may be 2 fetal poles within the same gestational sac (monochorionic) It is easier to determine chorionicity earlier in the pregnancy depending on the chorionicity and amnionicityIt is a sad situation when a vanishing twin occurs which is about 20 of twin pregnancies In these cases one of the twins fails to grow and thrive Instead its development arrests and it is reabsorbed with no evidence at delivery of the twin pregnancy
Monoamniotic Twins Dichorionic diamniotic Twins
TRIPLETS
Triplets with 2 sacs Monoamniotic monochorionic twins and a normal single
GRAPHS TO DETERMINE GESTATIONAL AGEDepending on the age of the gestation these graphs can be used to determine the correct EDD
Mean Sac Diameter measurement is used to determine gestational age before a Crown Rump length can be clearly measured The average sac diameter is determined by measuring the length width and height then dividing by 3
Once a fetal Pole can be visualized the CRL measurement is the most accurate method for dating the pregnancy
COMMON PATHOLOGYThickened Nuchal Translucency(NL)Partial Ovular DetachmentRetained products of conceptionAnembryonic GestationGestational trophoblastic diseaseMiscarriageEctopic PregnancySubchorionic hemorrhageConjoined TwinsAntepartum HemorrhageCheck heart beatCheck causes of bleeding
Thickened Nuchal Translucency (NT)
bull One of the parameters used in sequential screening (SS) for Downrsquos syndrome in first trimester
ndash SS Pregnancy associated plasma protein levels hCG levels NT thickness
bull Measured during 11-14 wks gestational age
bull Seen on sagittal image as increased subcutaneous non-septated fluid in posterior fetal neck
bull Measurement gt3mm usually considered abnormal however exact cut off measurements are dependent on maternal agegestational age
bull Detection rate of screening for Downrsquos Syndrome in first trimester
ndash sequential screening with NT 82-87
ndash NT alone 64-70
Thickened Nuchal Translucency (NT)
Thickened Nuchal Translucency
PARTIAL OVULAR DETACHMENTThe maternal circulation inside the placenta starts peripherally (in the placental margins) and is associated to physiological oxidative phenomena that may lead to membranes rupture and formation The abnormal development of such membranes may result in subchorionic hemorrhage enhancing the predisposition to an adverse gestational outcome at the third trimester (PPROM and PTL)Such abnormality is common and also denominated as subchorionic hemorrhage or trophoblastic hematoma being visualized in more than 18 of cases of threatened miscarriage The presence of fetal heart activity confers an excellent prognosis Clinically subchorionic hemorrhage may course with vaginal bleeding At ultrasonography a crescent-shaped shadow is observed adjacent to the gestational sac with debris Gestational sac compression and consequential deformation may occur In most of cases a two-week follow-up evaluation confirms the hematoma resorption
Retained products of conception are characterized by a
thickened disorganized and heterogeneous endometrium with ill-defined mucosal layers and cavitary line either with or without the presence of gestational sac Clinically the women presents abdominal pain and relative vaginal bleeding(14) In the presence of an intact gestational sac and closed cervix the difficulty in a spontaneous resolution will be higher requiring surgical evacuation
Retained products of conception
Transvaginal sonography without (A) and with (B) color Doppler imaging in a case of RPC with endometrial expansion (arrows)
Images retained products conception
EARLY EMBRYO DEATHSome sonographic findings characterize an embryo death in the first half of the first trimester in early phases before the crown-rump length can be measured The following aspects are highlighted small hyperechoic yolk sac or hydropic yolk sac increased in volume with diameter gt 7 mm or even small amniotic cavity disproportionate to the gestational sac size Before the 9th week small gestational sac may be associated with aneuploidy
Failed early pregnancy
ANEMBRYONIC GESTATIONAt transvaginal ultrasonography the yolk sac should be visualized in a gestational sac with mean diameter gt 10 mm The absence of a yolk sac within the gestational sac with gt 10 mm in mean diameter or the absence of a yolk sac within the gestational sac with gt 16 mm in diameter characterize anembryonic gestation
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
GESTATIONAL TROPHOBLASTIC DISEASEThe typical sonographic finding in most of cases of complete hydatidiform mole is a echogenic intracavitary solid mass with intermingled small cystic loci resembling a snow storm corresponding to the vesicles that macroscopically characterize this condition The higher the gestational age the larger the vesicles visualized as homogeneous anechoic images increasing the method specificity The ultrasonography sensitivity will depend on the gestational age at the moment of the diagnosis Ultrasonography can detect vesicles with gt 2 mm in diameter In early pregnancies with trophoblastic disease the sonographic method accuracy is limited hindering the differentiation of gestational trophoblastic disease from other conditions involving the endometrial cavity
Partial hydatidiform mole offers higher diagnostic difficulty by ultrasonography In a reasonable number of cases this disease presents as an empty gestational sac corresponding to anembryonic gestation or as early embryo death However two criteria have been described in the literature gestational sac transverseanteroposterior diameter ratio gt 15 and cystic changes irregularity of increase in echogenicity of decidualplacenta or myometrial reaction
ECTOPIC PREGNANCYSonographic findings of ectopic pregnancy will vary as a function of the gestational age and site Classically the following sonographic findings are described tubal ring sign adnexal disorganized mass molded to the adnexa andor cul de sac solid organized mass with regular margins mimicking a pediculated myomatous nodule clinically progressing with low β-hCGlevels and presence of a live extrauterine conceptus Uncommon gestational sites may be observed such as abdominal ectopic pregnancy cervical ectopic pregnancy and ectopic pregnancy in a previous Cesarean section pregnancy
Subchorionic hemorrhage (SCH) occurs when there is
perigestational haemorrhage and blood collects between the uterine wall and the chorionic membrane in pregnancy It is a frequent cause of first and second trimester bleedingEpidemiologyIt typically occurs within the first 20 weeks of gestation If seen in the first 10-14 days of gestation they are also sometimes termed implantation bleedsRadiographic featuresUltrasound crescentic collection with elevation of the chorionic membranedepending on the time elapsed since bleeding the collection will have variable echotexture
acute hyperechoic and may be difficult to differentiate from adjacent chorionsubacute-chronic decreasing echogenicity with time
in almost all cases there is extension of the hematoma towards the margin of the placenta
First trimester SCH (subchorionic bleed)
First trimester SCH (subchorionic bleed)
Extensive hematoma in a woman with chronic bleeding
Subchorionic hemorrhage
Conjoined twins are a rare and complex complication of
monozygotic twinning which is associated with high perinatal mortality Early prenatal diagnosis of conjoined twins allows better counselling of the parents regarding the management options including continuation of pregnancy with post-natal surgery termination of pregnancy or selective fetocide in case of a triplet pregnancy With the introduction of high-resolution and transvaginal ultrasound imaging accurate prenatal diagnosis of conjoined twins is possible early in pregnancy Although first-trimester diagnosis of conjoined twins is feasible false-positive cases are common before 10 weeks because earlier in gestation fetal movements are limited and monoamniotic twins may appear conjoined As most parents opt for immediate termination of pregnancy at confirmation of the diagnosis there are limited data on the prenatal follow-up of conjoined twins detailed analysis of case reports where 3D imaging was used indicates that this modality does not improve on the diagnosis made by 2D ultrasound Overall very early prenatal diagnosis and first-trimester 3D imaging provide very little additional practical medical information compared to the 11-14 weeks ultrasound examination
Images of the conjoined twins there are two heads with conjoined body
Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You

EQUIPMENT SELECTION AND TECHNIQUEModern ultrasound unitCurved linear probe approx 3-7 MHz depending upon maternal factorsTransvaginal probe approx 5-9 MHz (Use of non-latex cover if required)Ensure patient comfort and privacyWarm gel clean towels etcSelect Obstetric preset for appropriate power levels and measurement packagesUse a curvilinear probe (35-6MHZ) with low power to reduce risk of biological effects use of Doppler should be avoided in the 1st trimesterSCANNING TECHNIQUEPATIENT PREPARATION2 hours before the appointment time empty your bladder Over the next hour drink at least 1 liter of water and do not go to the toilet until instructed
lt10 weeks Cervix - assess if closed and measure length between internal and external osLook for bright trophoblastic reaction around sacAssess placental location and distance from internal os (may lie close to os at this stage)Check for retroplacental hemorrhages placental masses etcAssess maternal ovaries adnexae and Pouch Of Douglas (POD)Confirm presence of intrauterine gestation and numberIf multiple pregnancy confirm number of fetuses number of sacs and number of placentas present to determine chorionicity ie MonochorionicMonoamnionic (MCMA)MonochorionicDiamnionic(MCDA)Dichorionic Diamnionic (DCDA)Confirm heart beat(s) amp rate with M-Mode only (Use of Colour or Doppler traces is not recommended in the 1st trimester)Measure CRL to calculate gestational age and Estimated Date of Delivery(EDD)If too early to see the fetal pole measure the average sac diameter
A 1st trimester series should include the following minimum imagesUterus - long transBoth ovariesAdnexaeCervix and Pouch-Of-DouglasGestational sac - Long amp TransYolk sac if visibleFetal poleM mode fetal heartDocument the normal anatomy Any pathology found in 2 planes including measurements
GESTATIONAL SACThe gestational sac(GS) is the earliest sonographic finding in pregnancy It will be difficult to see if the mother has a retroverted uterus or fibroids The GS is an echogenic ring surrounding an anechoic centre An ectopic pregnancy will appear the same but it will not be within the endometrial cavity The GS is not identifiable until approximately 4 12 weeks with a transvaginal scanGestational sac size should be determined by measuring the mean of three diameters These differences rarely effect gestational age dating by more than a day or twoThe following image is using a transvaginal approach the gestational sac can be seen during week 4-5
5 week gestation Yolk Sac Only seen The yolk sac will be visible before a clearly definable embryonic pole
Mean Sac Diameter measurement is used to determine gestational age before a Crown Rump length can be clearly measured The average sac diameter is determined by measuring the length width and height then dividing by 3
The very early embryonic heart will be a subtle flicker This may be measured using M-Mode(avoid Doppler in the first trimester due to risks of bioeffects)Initially the heart rate may be slow
The Crown Rump Length (CRL) measurement in a 6 week gestation A mass of fetal cells separate from the yolk sac first becomes apparent on transvaginal ultrasound just after the 6th week of gestation This mass of cells is known as the fetal pole
YOLK SACThe yolk sac appears during the 5th week It is the second structure to appear after the GS It should be round with an anechoic centre It should not be calcified misshapen or gt5mm from the inner to inner diameter Yolk sacs larger than 6 mm are usually indicative of an abnormal pregnancy Failure to identify (with transvaginal ultrasound) a yolk sac when the gestational sac has grown to 12 mm is also usually indicative of a failed pregnancy
HEART BEATUsing a transvaginal approach the fetal heart beat can be seen flickering before the fetal pole is even identified It will be seen alongside the yolk sac It may be below 100 beats per minute but this will increase to between 120- 180 beats per minute by 7 weeks In the early scans at 5-6 weeks just visualizing a heart beating is the important thing Failure to identify fetal cardiac activity in a fetus whose overall length is greater than 4 mm is an ominous signSometimes there is difficulty distinguishing between the maternal pulse and fetal heart beat Often technicians will take the mothers pulse at the same time to check if it is the fetus or the mothers
CROWN RUMP LENGTH (CRL)The CRL is a reproducible and accurate method for measuring and dating a fetusEarly ultrasonographers used this term (CRL) because early fetuses also adopted the sitting in the chair posture in early pregnancy After 12 weeks the accuracy of CRL in predicting gestational age diminishes and is replaced by measurement of the fetal biparietal diameter In at least some respects the term crown rump length is misleadingThere is no fetal crown and no fetal rump to measure for most of the first trimester Until 53 days from the LMP the most caudad portion of the fetal cell mass is the caudal neurospone followed by the tail Only after 53 days is the fetal rump the most caudal portion of the fetusUntil 60 days from the LMP the most cephalad portion of the fetal cell mass is initially the rostral neurospore and later the cervical flexure After 60 days the fetal head becomes the most cephalad portion of the fetal cell massWhat is really measured during this early development of the fetus is the longest fetal diameterFrom 6 weeks to 9 12 weeks gestational age the fetal CRL grows at a rate of about 1 mm per day
Measure the crown rump length(CRL) to estimate gestational age
At 10 weeks visualize 4 jointed limbs feet and hands
NUCHAL TRANSLUCENCY
From 12 weeks the basic morphology of the fetus is visible
The Nuchal Translucency is used to provide a risk assessment for chromosomal abnormalities specifically Trisomies 1318 and 21 (Downs Syndrome)
The legs are usually crossed at the ankles Confirm the presence and symmetry of the long bones
The correct angle the feet to legs can be confirmed They should be at 90 degrees ie perpendicular or Talipes should be suspected
The humerus radius and ulna and the presence of hands areimaged from 11 weeks
12 week choroids take up most of the space within the ventricles
TWINS Initially twins may be identified as 2 separate gestational sacs (ie diamniotic dichorionic) They may be 2 fetal poles within the same gestational sac (monochorionic) It is easier to determine chorionicity earlier in the pregnancy depending on the chorionicity and amnionicityIt is a sad situation when a vanishing twin occurs which is about 20 of twin pregnancies In these cases one of the twins fails to grow and thrive Instead its development arrests and it is reabsorbed with no evidence at delivery of the twin pregnancy
Monoamniotic Twins Dichorionic diamniotic Twins
TRIPLETS
Triplets with 2 sacs Monoamniotic monochorionic twins and a normal single
GRAPHS TO DETERMINE GESTATIONAL AGEDepending on the age of the gestation these graphs can be used to determine the correct EDD
Mean Sac Diameter measurement is used to determine gestational age before a Crown Rump length can be clearly measured The average sac diameter is determined by measuring the length width and height then dividing by 3
Once a fetal Pole can be visualized the CRL measurement is the most accurate method for dating the pregnancy
COMMON PATHOLOGYThickened Nuchal Translucency(NL)Partial Ovular DetachmentRetained products of conceptionAnembryonic GestationGestational trophoblastic diseaseMiscarriageEctopic PregnancySubchorionic hemorrhageConjoined TwinsAntepartum HemorrhageCheck heart beatCheck causes of bleeding
Thickened Nuchal Translucency (NT)
bull One of the parameters used in sequential screening (SS) for Downrsquos syndrome in first trimester
ndash SS Pregnancy associated plasma protein levels hCG levels NT thickness
bull Measured during 11-14 wks gestational age
bull Seen on sagittal image as increased subcutaneous non-septated fluid in posterior fetal neck
bull Measurement gt3mm usually considered abnormal however exact cut off measurements are dependent on maternal agegestational age
bull Detection rate of screening for Downrsquos Syndrome in first trimester
ndash sequential screening with NT 82-87
ndash NT alone 64-70
Thickened Nuchal Translucency (NT)
Thickened Nuchal Translucency
PARTIAL OVULAR DETACHMENTThe maternal circulation inside the placenta starts peripherally (in the placental margins) and is associated to physiological oxidative phenomena that may lead to membranes rupture and formation The abnormal development of such membranes may result in subchorionic hemorrhage enhancing the predisposition to an adverse gestational outcome at the third trimester (PPROM and PTL)Such abnormality is common and also denominated as subchorionic hemorrhage or trophoblastic hematoma being visualized in more than 18 of cases of threatened miscarriage The presence of fetal heart activity confers an excellent prognosis Clinically subchorionic hemorrhage may course with vaginal bleeding At ultrasonography a crescent-shaped shadow is observed adjacent to the gestational sac with debris Gestational sac compression and consequential deformation may occur In most of cases a two-week follow-up evaluation confirms the hematoma resorption
Retained products of conception are characterized by a
thickened disorganized and heterogeneous endometrium with ill-defined mucosal layers and cavitary line either with or without the presence of gestational sac Clinically the women presents abdominal pain and relative vaginal bleeding(14) In the presence of an intact gestational sac and closed cervix the difficulty in a spontaneous resolution will be higher requiring surgical evacuation
Retained products of conception
Transvaginal sonography without (A) and with (B) color Doppler imaging in a case of RPC with endometrial expansion (arrows)
Images retained products conception
EARLY EMBRYO DEATHSome sonographic findings characterize an embryo death in the first half of the first trimester in early phases before the crown-rump length can be measured The following aspects are highlighted small hyperechoic yolk sac or hydropic yolk sac increased in volume with diameter gt 7 mm or even small amniotic cavity disproportionate to the gestational sac size Before the 9th week small gestational sac may be associated with aneuploidy
Failed early pregnancy
ANEMBRYONIC GESTATIONAt transvaginal ultrasonography the yolk sac should be visualized in a gestational sac with mean diameter gt 10 mm The absence of a yolk sac within the gestational sac with gt 10 mm in mean diameter or the absence of a yolk sac within the gestational sac with gt 16 mm in diameter characterize anembryonic gestation
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
GESTATIONAL TROPHOBLASTIC DISEASEThe typical sonographic finding in most of cases of complete hydatidiform mole is a echogenic intracavitary solid mass with intermingled small cystic loci resembling a snow storm corresponding to the vesicles that macroscopically characterize this condition The higher the gestational age the larger the vesicles visualized as homogeneous anechoic images increasing the method specificity The ultrasonography sensitivity will depend on the gestational age at the moment of the diagnosis Ultrasonography can detect vesicles with gt 2 mm in diameter In early pregnancies with trophoblastic disease the sonographic method accuracy is limited hindering the differentiation of gestational trophoblastic disease from other conditions involving the endometrial cavity
Partial hydatidiform mole offers higher diagnostic difficulty by ultrasonography In a reasonable number of cases this disease presents as an empty gestational sac corresponding to anembryonic gestation or as early embryo death However two criteria have been described in the literature gestational sac transverseanteroposterior diameter ratio gt 15 and cystic changes irregularity of increase in echogenicity of decidualplacenta or myometrial reaction
ECTOPIC PREGNANCYSonographic findings of ectopic pregnancy will vary as a function of the gestational age and site Classically the following sonographic findings are described tubal ring sign adnexal disorganized mass molded to the adnexa andor cul de sac solid organized mass with regular margins mimicking a pediculated myomatous nodule clinically progressing with low β-hCGlevels and presence of a live extrauterine conceptus Uncommon gestational sites may be observed such as abdominal ectopic pregnancy cervical ectopic pregnancy and ectopic pregnancy in a previous Cesarean section pregnancy
Subchorionic hemorrhage (SCH) occurs when there is
perigestational haemorrhage and blood collects between the uterine wall and the chorionic membrane in pregnancy It is a frequent cause of first and second trimester bleedingEpidemiologyIt typically occurs within the first 20 weeks of gestation If seen in the first 10-14 days of gestation they are also sometimes termed implantation bleedsRadiographic featuresUltrasound crescentic collection with elevation of the chorionic membranedepending on the time elapsed since bleeding the collection will have variable echotexture
acute hyperechoic and may be difficult to differentiate from adjacent chorionsubacute-chronic decreasing echogenicity with time
in almost all cases there is extension of the hematoma towards the margin of the placenta
First trimester SCH (subchorionic bleed)
First trimester SCH (subchorionic bleed)
Extensive hematoma in a woman with chronic bleeding
Subchorionic hemorrhage
Conjoined twins are a rare and complex complication of
monozygotic twinning which is associated with high perinatal mortality Early prenatal diagnosis of conjoined twins allows better counselling of the parents regarding the management options including continuation of pregnancy with post-natal surgery termination of pregnancy or selective fetocide in case of a triplet pregnancy With the introduction of high-resolution and transvaginal ultrasound imaging accurate prenatal diagnosis of conjoined twins is possible early in pregnancy Although first-trimester diagnosis of conjoined twins is feasible false-positive cases are common before 10 weeks because earlier in gestation fetal movements are limited and monoamniotic twins may appear conjoined As most parents opt for immediate termination of pregnancy at confirmation of the diagnosis there are limited data on the prenatal follow-up of conjoined twins detailed analysis of case reports where 3D imaging was used indicates that this modality does not improve on the diagnosis made by 2D ultrasound Overall very early prenatal diagnosis and first-trimester 3D imaging provide very little additional practical medical information compared to the 11-14 weeks ultrasound examination
Images of the conjoined twins there are two heads with conjoined body
Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You

lt10 weeks Cervix - assess if closed and measure length between internal and external osLook for bright trophoblastic reaction around sacAssess placental location and distance from internal os (may lie close to os at this stage)Check for retroplacental hemorrhages placental masses etcAssess maternal ovaries adnexae and Pouch Of Douglas (POD)Confirm presence of intrauterine gestation and numberIf multiple pregnancy confirm number of fetuses number of sacs and number of placentas present to determine chorionicity ie MonochorionicMonoamnionic (MCMA)MonochorionicDiamnionic(MCDA)Dichorionic Diamnionic (DCDA)Confirm heart beat(s) amp rate with M-Mode only (Use of Colour or Doppler traces is not recommended in the 1st trimester)Measure CRL to calculate gestational age and Estimated Date of Delivery(EDD)If too early to see the fetal pole measure the average sac diameter
A 1st trimester series should include the following minimum imagesUterus - long transBoth ovariesAdnexaeCervix and Pouch-Of-DouglasGestational sac - Long amp TransYolk sac if visibleFetal poleM mode fetal heartDocument the normal anatomy Any pathology found in 2 planes including measurements
GESTATIONAL SACThe gestational sac(GS) is the earliest sonographic finding in pregnancy It will be difficult to see if the mother has a retroverted uterus or fibroids The GS is an echogenic ring surrounding an anechoic centre An ectopic pregnancy will appear the same but it will not be within the endometrial cavity The GS is not identifiable until approximately 4 12 weeks with a transvaginal scanGestational sac size should be determined by measuring the mean of three diameters These differences rarely effect gestational age dating by more than a day or twoThe following image is using a transvaginal approach the gestational sac can be seen during week 4-5
5 week gestation Yolk Sac Only seen The yolk sac will be visible before a clearly definable embryonic pole
Mean Sac Diameter measurement is used to determine gestational age before a Crown Rump length can be clearly measured The average sac diameter is determined by measuring the length width and height then dividing by 3
The very early embryonic heart will be a subtle flicker This may be measured using M-Mode(avoid Doppler in the first trimester due to risks of bioeffects)Initially the heart rate may be slow
The Crown Rump Length (CRL) measurement in a 6 week gestation A mass of fetal cells separate from the yolk sac first becomes apparent on transvaginal ultrasound just after the 6th week of gestation This mass of cells is known as the fetal pole
YOLK SACThe yolk sac appears during the 5th week It is the second structure to appear after the GS It should be round with an anechoic centre It should not be calcified misshapen or gt5mm from the inner to inner diameter Yolk sacs larger than 6 mm are usually indicative of an abnormal pregnancy Failure to identify (with transvaginal ultrasound) a yolk sac when the gestational sac has grown to 12 mm is also usually indicative of a failed pregnancy
HEART BEATUsing a transvaginal approach the fetal heart beat can be seen flickering before the fetal pole is even identified It will be seen alongside the yolk sac It may be below 100 beats per minute but this will increase to between 120- 180 beats per minute by 7 weeks In the early scans at 5-6 weeks just visualizing a heart beating is the important thing Failure to identify fetal cardiac activity in a fetus whose overall length is greater than 4 mm is an ominous signSometimes there is difficulty distinguishing between the maternal pulse and fetal heart beat Often technicians will take the mothers pulse at the same time to check if it is the fetus or the mothers
CROWN RUMP LENGTH (CRL)The CRL is a reproducible and accurate method for measuring and dating a fetusEarly ultrasonographers used this term (CRL) because early fetuses also adopted the sitting in the chair posture in early pregnancy After 12 weeks the accuracy of CRL in predicting gestational age diminishes and is replaced by measurement of the fetal biparietal diameter In at least some respects the term crown rump length is misleadingThere is no fetal crown and no fetal rump to measure for most of the first trimester Until 53 days from the LMP the most caudad portion of the fetal cell mass is the caudal neurospone followed by the tail Only after 53 days is the fetal rump the most caudal portion of the fetusUntil 60 days from the LMP the most cephalad portion of the fetal cell mass is initially the rostral neurospore and later the cervical flexure After 60 days the fetal head becomes the most cephalad portion of the fetal cell massWhat is really measured during this early development of the fetus is the longest fetal diameterFrom 6 weeks to 9 12 weeks gestational age the fetal CRL grows at a rate of about 1 mm per day
Measure the crown rump length(CRL) to estimate gestational age
At 10 weeks visualize 4 jointed limbs feet and hands
NUCHAL TRANSLUCENCY
From 12 weeks the basic morphology of the fetus is visible
The Nuchal Translucency is used to provide a risk assessment for chromosomal abnormalities specifically Trisomies 1318 and 21 (Downs Syndrome)
The legs are usually crossed at the ankles Confirm the presence and symmetry of the long bones
The correct angle the feet to legs can be confirmed They should be at 90 degrees ie perpendicular or Talipes should be suspected
The humerus radius and ulna and the presence of hands areimaged from 11 weeks
12 week choroids take up most of the space within the ventricles
TWINS Initially twins may be identified as 2 separate gestational sacs (ie diamniotic dichorionic) They may be 2 fetal poles within the same gestational sac (monochorionic) It is easier to determine chorionicity earlier in the pregnancy depending on the chorionicity and amnionicityIt is a sad situation when a vanishing twin occurs which is about 20 of twin pregnancies In these cases one of the twins fails to grow and thrive Instead its development arrests and it is reabsorbed with no evidence at delivery of the twin pregnancy
Monoamniotic Twins Dichorionic diamniotic Twins
TRIPLETS
Triplets with 2 sacs Monoamniotic monochorionic twins and a normal single
GRAPHS TO DETERMINE GESTATIONAL AGEDepending on the age of the gestation these graphs can be used to determine the correct EDD
Mean Sac Diameter measurement is used to determine gestational age before a Crown Rump length can be clearly measured The average sac diameter is determined by measuring the length width and height then dividing by 3
Once a fetal Pole can be visualized the CRL measurement is the most accurate method for dating the pregnancy
COMMON PATHOLOGYThickened Nuchal Translucency(NL)Partial Ovular DetachmentRetained products of conceptionAnembryonic GestationGestational trophoblastic diseaseMiscarriageEctopic PregnancySubchorionic hemorrhageConjoined TwinsAntepartum HemorrhageCheck heart beatCheck causes of bleeding
Thickened Nuchal Translucency (NT)
bull One of the parameters used in sequential screening (SS) for Downrsquos syndrome in first trimester
ndash SS Pregnancy associated plasma protein levels hCG levels NT thickness
bull Measured during 11-14 wks gestational age
bull Seen on sagittal image as increased subcutaneous non-septated fluid in posterior fetal neck
bull Measurement gt3mm usually considered abnormal however exact cut off measurements are dependent on maternal agegestational age
bull Detection rate of screening for Downrsquos Syndrome in first trimester
ndash sequential screening with NT 82-87
ndash NT alone 64-70
Thickened Nuchal Translucency (NT)
Thickened Nuchal Translucency
PARTIAL OVULAR DETACHMENTThe maternal circulation inside the placenta starts peripherally (in the placental margins) and is associated to physiological oxidative phenomena that may lead to membranes rupture and formation The abnormal development of such membranes may result in subchorionic hemorrhage enhancing the predisposition to an adverse gestational outcome at the third trimester (PPROM and PTL)Such abnormality is common and also denominated as subchorionic hemorrhage or trophoblastic hematoma being visualized in more than 18 of cases of threatened miscarriage The presence of fetal heart activity confers an excellent prognosis Clinically subchorionic hemorrhage may course with vaginal bleeding At ultrasonography a crescent-shaped shadow is observed adjacent to the gestational sac with debris Gestational sac compression and consequential deformation may occur In most of cases a two-week follow-up evaluation confirms the hematoma resorption
Retained products of conception are characterized by a
thickened disorganized and heterogeneous endometrium with ill-defined mucosal layers and cavitary line either with or without the presence of gestational sac Clinically the women presents abdominal pain and relative vaginal bleeding(14) In the presence of an intact gestational sac and closed cervix the difficulty in a spontaneous resolution will be higher requiring surgical evacuation
Retained products of conception
Transvaginal sonography without (A) and with (B) color Doppler imaging in a case of RPC with endometrial expansion (arrows)
Images retained products conception
EARLY EMBRYO DEATHSome sonographic findings characterize an embryo death in the first half of the first trimester in early phases before the crown-rump length can be measured The following aspects are highlighted small hyperechoic yolk sac or hydropic yolk sac increased in volume with diameter gt 7 mm or even small amniotic cavity disproportionate to the gestational sac size Before the 9th week small gestational sac may be associated with aneuploidy
Failed early pregnancy
ANEMBRYONIC GESTATIONAt transvaginal ultrasonography the yolk sac should be visualized in a gestational sac with mean diameter gt 10 mm The absence of a yolk sac within the gestational sac with gt 10 mm in mean diameter or the absence of a yolk sac within the gestational sac with gt 16 mm in diameter characterize anembryonic gestation
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
GESTATIONAL TROPHOBLASTIC DISEASEThe typical sonographic finding in most of cases of complete hydatidiform mole is a echogenic intracavitary solid mass with intermingled small cystic loci resembling a snow storm corresponding to the vesicles that macroscopically characterize this condition The higher the gestational age the larger the vesicles visualized as homogeneous anechoic images increasing the method specificity The ultrasonography sensitivity will depend on the gestational age at the moment of the diagnosis Ultrasonography can detect vesicles with gt 2 mm in diameter In early pregnancies with trophoblastic disease the sonographic method accuracy is limited hindering the differentiation of gestational trophoblastic disease from other conditions involving the endometrial cavity
Partial hydatidiform mole offers higher diagnostic difficulty by ultrasonography In a reasonable number of cases this disease presents as an empty gestational sac corresponding to anembryonic gestation or as early embryo death However two criteria have been described in the literature gestational sac transverseanteroposterior diameter ratio gt 15 and cystic changes irregularity of increase in echogenicity of decidualplacenta or myometrial reaction
ECTOPIC PREGNANCYSonographic findings of ectopic pregnancy will vary as a function of the gestational age and site Classically the following sonographic findings are described tubal ring sign adnexal disorganized mass molded to the adnexa andor cul de sac solid organized mass with regular margins mimicking a pediculated myomatous nodule clinically progressing with low β-hCGlevels and presence of a live extrauterine conceptus Uncommon gestational sites may be observed such as abdominal ectopic pregnancy cervical ectopic pregnancy and ectopic pregnancy in a previous Cesarean section pregnancy
Subchorionic hemorrhage (SCH) occurs when there is
perigestational haemorrhage and blood collects between the uterine wall and the chorionic membrane in pregnancy It is a frequent cause of first and second trimester bleedingEpidemiologyIt typically occurs within the first 20 weeks of gestation If seen in the first 10-14 days of gestation they are also sometimes termed implantation bleedsRadiographic featuresUltrasound crescentic collection with elevation of the chorionic membranedepending on the time elapsed since bleeding the collection will have variable echotexture
acute hyperechoic and may be difficult to differentiate from adjacent chorionsubacute-chronic decreasing echogenicity with time
in almost all cases there is extension of the hematoma towards the margin of the placenta
First trimester SCH (subchorionic bleed)
First trimester SCH (subchorionic bleed)
Extensive hematoma in a woman with chronic bleeding
Subchorionic hemorrhage
Conjoined twins are a rare and complex complication of
monozygotic twinning which is associated with high perinatal mortality Early prenatal diagnosis of conjoined twins allows better counselling of the parents regarding the management options including continuation of pregnancy with post-natal surgery termination of pregnancy or selective fetocide in case of a triplet pregnancy With the introduction of high-resolution and transvaginal ultrasound imaging accurate prenatal diagnosis of conjoined twins is possible early in pregnancy Although first-trimester diagnosis of conjoined twins is feasible false-positive cases are common before 10 weeks because earlier in gestation fetal movements are limited and monoamniotic twins may appear conjoined As most parents opt for immediate termination of pregnancy at confirmation of the diagnosis there are limited data on the prenatal follow-up of conjoined twins detailed analysis of case reports where 3D imaging was used indicates that this modality does not improve on the diagnosis made by 2D ultrasound Overall very early prenatal diagnosis and first-trimester 3D imaging provide very little additional practical medical information compared to the 11-14 weeks ultrasound examination
Images of the conjoined twins there are two heads with conjoined body
Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You

A 1st trimester series should include the following minimum imagesUterus - long transBoth ovariesAdnexaeCervix and Pouch-Of-DouglasGestational sac - Long amp TransYolk sac if visibleFetal poleM mode fetal heartDocument the normal anatomy Any pathology found in 2 planes including measurements
GESTATIONAL SACThe gestational sac(GS) is the earliest sonographic finding in pregnancy It will be difficult to see if the mother has a retroverted uterus or fibroids The GS is an echogenic ring surrounding an anechoic centre An ectopic pregnancy will appear the same but it will not be within the endometrial cavity The GS is not identifiable until approximately 4 12 weeks with a transvaginal scanGestational sac size should be determined by measuring the mean of three diameters These differences rarely effect gestational age dating by more than a day or twoThe following image is using a transvaginal approach the gestational sac can be seen during week 4-5
5 week gestation Yolk Sac Only seen The yolk sac will be visible before a clearly definable embryonic pole
Mean Sac Diameter measurement is used to determine gestational age before a Crown Rump length can be clearly measured The average sac diameter is determined by measuring the length width and height then dividing by 3
The very early embryonic heart will be a subtle flicker This may be measured using M-Mode(avoid Doppler in the first trimester due to risks of bioeffects)Initially the heart rate may be slow
The Crown Rump Length (CRL) measurement in a 6 week gestation A mass of fetal cells separate from the yolk sac first becomes apparent on transvaginal ultrasound just after the 6th week of gestation This mass of cells is known as the fetal pole
YOLK SACThe yolk sac appears during the 5th week It is the second structure to appear after the GS It should be round with an anechoic centre It should not be calcified misshapen or gt5mm from the inner to inner diameter Yolk sacs larger than 6 mm are usually indicative of an abnormal pregnancy Failure to identify (with transvaginal ultrasound) a yolk sac when the gestational sac has grown to 12 mm is also usually indicative of a failed pregnancy
HEART BEATUsing a transvaginal approach the fetal heart beat can be seen flickering before the fetal pole is even identified It will be seen alongside the yolk sac It may be below 100 beats per minute but this will increase to between 120- 180 beats per minute by 7 weeks In the early scans at 5-6 weeks just visualizing a heart beating is the important thing Failure to identify fetal cardiac activity in a fetus whose overall length is greater than 4 mm is an ominous signSometimes there is difficulty distinguishing between the maternal pulse and fetal heart beat Often technicians will take the mothers pulse at the same time to check if it is the fetus or the mothers
CROWN RUMP LENGTH (CRL)The CRL is a reproducible and accurate method for measuring and dating a fetusEarly ultrasonographers used this term (CRL) because early fetuses also adopted the sitting in the chair posture in early pregnancy After 12 weeks the accuracy of CRL in predicting gestational age diminishes and is replaced by measurement of the fetal biparietal diameter In at least some respects the term crown rump length is misleadingThere is no fetal crown and no fetal rump to measure for most of the first trimester Until 53 days from the LMP the most caudad portion of the fetal cell mass is the caudal neurospone followed by the tail Only after 53 days is the fetal rump the most caudal portion of the fetusUntil 60 days from the LMP the most cephalad portion of the fetal cell mass is initially the rostral neurospore and later the cervical flexure After 60 days the fetal head becomes the most cephalad portion of the fetal cell massWhat is really measured during this early development of the fetus is the longest fetal diameterFrom 6 weeks to 9 12 weeks gestational age the fetal CRL grows at a rate of about 1 mm per day
Measure the crown rump length(CRL) to estimate gestational age
At 10 weeks visualize 4 jointed limbs feet and hands
NUCHAL TRANSLUCENCY
From 12 weeks the basic morphology of the fetus is visible
The Nuchal Translucency is used to provide a risk assessment for chromosomal abnormalities specifically Trisomies 1318 and 21 (Downs Syndrome)
The legs are usually crossed at the ankles Confirm the presence and symmetry of the long bones
The correct angle the feet to legs can be confirmed They should be at 90 degrees ie perpendicular or Talipes should be suspected
The humerus radius and ulna and the presence of hands areimaged from 11 weeks
12 week choroids take up most of the space within the ventricles
TWINS Initially twins may be identified as 2 separate gestational sacs (ie diamniotic dichorionic) They may be 2 fetal poles within the same gestational sac (monochorionic) It is easier to determine chorionicity earlier in the pregnancy depending on the chorionicity and amnionicityIt is a sad situation when a vanishing twin occurs which is about 20 of twin pregnancies In these cases one of the twins fails to grow and thrive Instead its development arrests and it is reabsorbed with no evidence at delivery of the twin pregnancy
Monoamniotic Twins Dichorionic diamniotic Twins
TRIPLETS
Triplets with 2 sacs Monoamniotic monochorionic twins and a normal single
GRAPHS TO DETERMINE GESTATIONAL AGEDepending on the age of the gestation these graphs can be used to determine the correct EDD
Mean Sac Diameter measurement is used to determine gestational age before a Crown Rump length can be clearly measured The average sac diameter is determined by measuring the length width and height then dividing by 3
Once a fetal Pole can be visualized the CRL measurement is the most accurate method for dating the pregnancy
COMMON PATHOLOGYThickened Nuchal Translucency(NL)Partial Ovular DetachmentRetained products of conceptionAnembryonic GestationGestational trophoblastic diseaseMiscarriageEctopic PregnancySubchorionic hemorrhageConjoined TwinsAntepartum HemorrhageCheck heart beatCheck causes of bleeding
Thickened Nuchal Translucency (NT)
bull One of the parameters used in sequential screening (SS) for Downrsquos syndrome in first trimester
ndash SS Pregnancy associated plasma protein levels hCG levels NT thickness
bull Measured during 11-14 wks gestational age
bull Seen on sagittal image as increased subcutaneous non-septated fluid in posterior fetal neck
bull Measurement gt3mm usually considered abnormal however exact cut off measurements are dependent on maternal agegestational age
bull Detection rate of screening for Downrsquos Syndrome in first trimester
ndash sequential screening with NT 82-87
ndash NT alone 64-70
Thickened Nuchal Translucency (NT)
Thickened Nuchal Translucency
PARTIAL OVULAR DETACHMENTThe maternal circulation inside the placenta starts peripherally (in the placental margins) and is associated to physiological oxidative phenomena that may lead to membranes rupture and formation The abnormal development of such membranes may result in subchorionic hemorrhage enhancing the predisposition to an adverse gestational outcome at the third trimester (PPROM and PTL)Such abnormality is common and also denominated as subchorionic hemorrhage or trophoblastic hematoma being visualized in more than 18 of cases of threatened miscarriage The presence of fetal heart activity confers an excellent prognosis Clinically subchorionic hemorrhage may course with vaginal bleeding At ultrasonography a crescent-shaped shadow is observed adjacent to the gestational sac with debris Gestational sac compression and consequential deformation may occur In most of cases a two-week follow-up evaluation confirms the hematoma resorption
Retained products of conception are characterized by a
thickened disorganized and heterogeneous endometrium with ill-defined mucosal layers and cavitary line either with or without the presence of gestational sac Clinically the women presents abdominal pain and relative vaginal bleeding(14) In the presence of an intact gestational sac and closed cervix the difficulty in a spontaneous resolution will be higher requiring surgical evacuation
Retained products of conception
Transvaginal sonography without (A) and with (B) color Doppler imaging in a case of RPC with endometrial expansion (arrows)
Images retained products conception
EARLY EMBRYO DEATHSome sonographic findings characterize an embryo death in the first half of the first trimester in early phases before the crown-rump length can be measured The following aspects are highlighted small hyperechoic yolk sac or hydropic yolk sac increased in volume with diameter gt 7 mm or even small amniotic cavity disproportionate to the gestational sac size Before the 9th week small gestational sac may be associated with aneuploidy
Failed early pregnancy
ANEMBRYONIC GESTATIONAt transvaginal ultrasonography the yolk sac should be visualized in a gestational sac with mean diameter gt 10 mm The absence of a yolk sac within the gestational sac with gt 10 mm in mean diameter or the absence of a yolk sac within the gestational sac with gt 16 mm in diameter characterize anembryonic gestation
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
GESTATIONAL TROPHOBLASTIC DISEASEThe typical sonographic finding in most of cases of complete hydatidiform mole is a echogenic intracavitary solid mass with intermingled small cystic loci resembling a snow storm corresponding to the vesicles that macroscopically characterize this condition The higher the gestational age the larger the vesicles visualized as homogeneous anechoic images increasing the method specificity The ultrasonography sensitivity will depend on the gestational age at the moment of the diagnosis Ultrasonography can detect vesicles with gt 2 mm in diameter In early pregnancies with trophoblastic disease the sonographic method accuracy is limited hindering the differentiation of gestational trophoblastic disease from other conditions involving the endometrial cavity
Partial hydatidiform mole offers higher diagnostic difficulty by ultrasonography In a reasonable number of cases this disease presents as an empty gestational sac corresponding to anembryonic gestation or as early embryo death However two criteria have been described in the literature gestational sac transverseanteroposterior diameter ratio gt 15 and cystic changes irregularity of increase in echogenicity of decidualplacenta or myometrial reaction
ECTOPIC PREGNANCYSonographic findings of ectopic pregnancy will vary as a function of the gestational age and site Classically the following sonographic findings are described tubal ring sign adnexal disorganized mass molded to the adnexa andor cul de sac solid organized mass with regular margins mimicking a pediculated myomatous nodule clinically progressing with low β-hCGlevels and presence of a live extrauterine conceptus Uncommon gestational sites may be observed such as abdominal ectopic pregnancy cervical ectopic pregnancy and ectopic pregnancy in a previous Cesarean section pregnancy
Subchorionic hemorrhage (SCH) occurs when there is
perigestational haemorrhage and blood collects between the uterine wall and the chorionic membrane in pregnancy It is a frequent cause of first and second trimester bleedingEpidemiologyIt typically occurs within the first 20 weeks of gestation If seen in the first 10-14 days of gestation they are also sometimes termed implantation bleedsRadiographic featuresUltrasound crescentic collection with elevation of the chorionic membranedepending on the time elapsed since bleeding the collection will have variable echotexture
acute hyperechoic and may be difficult to differentiate from adjacent chorionsubacute-chronic decreasing echogenicity with time
in almost all cases there is extension of the hematoma towards the margin of the placenta
First trimester SCH (subchorionic bleed)
First trimester SCH (subchorionic bleed)
Extensive hematoma in a woman with chronic bleeding
Subchorionic hemorrhage
Conjoined twins are a rare and complex complication of
monozygotic twinning which is associated with high perinatal mortality Early prenatal diagnosis of conjoined twins allows better counselling of the parents regarding the management options including continuation of pregnancy with post-natal surgery termination of pregnancy or selective fetocide in case of a triplet pregnancy With the introduction of high-resolution and transvaginal ultrasound imaging accurate prenatal diagnosis of conjoined twins is possible early in pregnancy Although first-trimester diagnosis of conjoined twins is feasible false-positive cases are common before 10 weeks because earlier in gestation fetal movements are limited and monoamniotic twins may appear conjoined As most parents opt for immediate termination of pregnancy at confirmation of the diagnosis there are limited data on the prenatal follow-up of conjoined twins detailed analysis of case reports where 3D imaging was used indicates that this modality does not improve on the diagnosis made by 2D ultrasound Overall very early prenatal diagnosis and first-trimester 3D imaging provide very little additional practical medical information compared to the 11-14 weeks ultrasound examination
Images of the conjoined twins there are two heads with conjoined body
Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You

GESTATIONAL SACThe gestational sac(GS) is the earliest sonographic finding in pregnancy It will be difficult to see if the mother has a retroverted uterus or fibroids The GS is an echogenic ring surrounding an anechoic centre An ectopic pregnancy will appear the same but it will not be within the endometrial cavity The GS is not identifiable until approximately 4 12 weeks with a transvaginal scanGestational sac size should be determined by measuring the mean of three diameters These differences rarely effect gestational age dating by more than a day or twoThe following image is using a transvaginal approach the gestational sac can be seen during week 4-5
5 week gestation Yolk Sac Only seen The yolk sac will be visible before a clearly definable embryonic pole
Mean Sac Diameter measurement is used to determine gestational age before a Crown Rump length can be clearly measured The average sac diameter is determined by measuring the length width and height then dividing by 3
The very early embryonic heart will be a subtle flicker This may be measured using M-Mode(avoid Doppler in the first trimester due to risks of bioeffects)Initially the heart rate may be slow
The Crown Rump Length (CRL) measurement in a 6 week gestation A mass of fetal cells separate from the yolk sac first becomes apparent on transvaginal ultrasound just after the 6th week of gestation This mass of cells is known as the fetal pole
YOLK SACThe yolk sac appears during the 5th week It is the second structure to appear after the GS It should be round with an anechoic centre It should not be calcified misshapen or gt5mm from the inner to inner diameter Yolk sacs larger than 6 mm are usually indicative of an abnormal pregnancy Failure to identify (with transvaginal ultrasound) a yolk sac when the gestational sac has grown to 12 mm is also usually indicative of a failed pregnancy
HEART BEATUsing a transvaginal approach the fetal heart beat can be seen flickering before the fetal pole is even identified It will be seen alongside the yolk sac It may be below 100 beats per minute but this will increase to between 120- 180 beats per minute by 7 weeks In the early scans at 5-6 weeks just visualizing a heart beating is the important thing Failure to identify fetal cardiac activity in a fetus whose overall length is greater than 4 mm is an ominous signSometimes there is difficulty distinguishing between the maternal pulse and fetal heart beat Often technicians will take the mothers pulse at the same time to check if it is the fetus or the mothers
CROWN RUMP LENGTH (CRL)The CRL is a reproducible and accurate method for measuring and dating a fetusEarly ultrasonographers used this term (CRL) because early fetuses also adopted the sitting in the chair posture in early pregnancy After 12 weeks the accuracy of CRL in predicting gestational age diminishes and is replaced by measurement of the fetal biparietal diameter In at least some respects the term crown rump length is misleadingThere is no fetal crown and no fetal rump to measure for most of the first trimester Until 53 days from the LMP the most caudad portion of the fetal cell mass is the caudal neurospone followed by the tail Only after 53 days is the fetal rump the most caudal portion of the fetusUntil 60 days from the LMP the most cephalad portion of the fetal cell mass is initially the rostral neurospore and later the cervical flexure After 60 days the fetal head becomes the most cephalad portion of the fetal cell massWhat is really measured during this early development of the fetus is the longest fetal diameterFrom 6 weeks to 9 12 weeks gestational age the fetal CRL grows at a rate of about 1 mm per day
Measure the crown rump length(CRL) to estimate gestational age
At 10 weeks visualize 4 jointed limbs feet and hands
NUCHAL TRANSLUCENCY
From 12 weeks the basic morphology of the fetus is visible
The Nuchal Translucency is used to provide a risk assessment for chromosomal abnormalities specifically Trisomies 1318 and 21 (Downs Syndrome)
The legs are usually crossed at the ankles Confirm the presence and symmetry of the long bones
The correct angle the feet to legs can be confirmed They should be at 90 degrees ie perpendicular or Talipes should be suspected
The humerus radius and ulna and the presence of hands areimaged from 11 weeks
12 week choroids take up most of the space within the ventricles
TWINS Initially twins may be identified as 2 separate gestational sacs (ie diamniotic dichorionic) They may be 2 fetal poles within the same gestational sac (monochorionic) It is easier to determine chorionicity earlier in the pregnancy depending on the chorionicity and amnionicityIt is a sad situation when a vanishing twin occurs which is about 20 of twin pregnancies In these cases one of the twins fails to grow and thrive Instead its development arrests and it is reabsorbed with no evidence at delivery of the twin pregnancy
Monoamniotic Twins Dichorionic diamniotic Twins
TRIPLETS
Triplets with 2 sacs Monoamniotic monochorionic twins and a normal single
GRAPHS TO DETERMINE GESTATIONAL AGEDepending on the age of the gestation these graphs can be used to determine the correct EDD
Mean Sac Diameter measurement is used to determine gestational age before a Crown Rump length can be clearly measured The average sac diameter is determined by measuring the length width and height then dividing by 3
Once a fetal Pole can be visualized the CRL measurement is the most accurate method for dating the pregnancy
COMMON PATHOLOGYThickened Nuchal Translucency(NL)Partial Ovular DetachmentRetained products of conceptionAnembryonic GestationGestational trophoblastic diseaseMiscarriageEctopic PregnancySubchorionic hemorrhageConjoined TwinsAntepartum HemorrhageCheck heart beatCheck causes of bleeding
Thickened Nuchal Translucency (NT)
bull One of the parameters used in sequential screening (SS) for Downrsquos syndrome in first trimester
ndash SS Pregnancy associated plasma protein levels hCG levels NT thickness
bull Measured during 11-14 wks gestational age
bull Seen on sagittal image as increased subcutaneous non-septated fluid in posterior fetal neck
bull Measurement gt3mm usually considered abnormal however exact cut off measurements are dependent on maternal agegestational age
bull Detection rate of screening for Downrsquos Syndrome in first trimester
ndash sequential screening with NT 82-87
ndash NT alone 64-70
Thickened Nuchal Translucency (NT)
Thickened Nuchal Translucency
PARTIAL OVULAR DETACHMENTThe maternal circulation inside the placenta starts peripherally (in the placental margins) and is associated to physiological oxidative phenomena that may lead to membranes rupture and formation The abnormal development of such membranes may result in subchorionic hemorrhage enhancing the predisposition to an adverse gestational outcome at the third trimester (PPROM and PTL)Such abnormality is common and also denominated as subchorionic hemorrhage or trophoblastic hematoma being visualized in more than 18 of cases of threatened miscarriage The presence of fetal heart activity confers an excellent prognosis Clinically subchorionic hemorrhage may course with vaginal bleeding At ultrasonography a crescent-shaped shadow is observed adjacent to the gestational sac with debris Gestational sac compression and consequential deformation may occur In most of cases a two-week follow-up evaluation confirms the hematoma resorption
Retained products of conception are characterized by a
thickened disorganized and heterogeneous endometrium with ill-defined mucosal layers and cavitary line either with or without the presence of gestational sac Clinically the women presents abdominal pain and relative vaginal bleeding(14) In the presence of an intact gestational sac and closed cervix the difficulty in a spontaneous resolution will be higher requiring surgical evacuation
Retained products of conception
Transvaginal sonography without (A) and with (B) color Doppler imaging in a case of RPC with endometrial expansion (arrows)
Images retained products conception
EARLY EMBRYO DEATHSome sonographic findings characterize an embryo death in the first half of the first trimester in early phases before the crown-rump length can be measured The following aspects are highlighted small hyperechoic yolk sac or hydropic yolk sac increased in volume with diameter gt 7 mm or even small amniotic cavity disproportionate to the gestational sac size Before the 9th week small gestational sac may be associated with aneuploidy
Failed early pregnancy
ANEMBRYONIC GESTATIONAt transvaginal ultrasonography the yolk sac should be visualized in a gestational sac with mean diameter gt 10 mm The absence of a yolk sac within the gestational sac with gt 10 mm in mean diameter or the absence of a yolk sac within the gestational sac with gt 16 mm in diameter characterize anembryonic gestation
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
GESTATIONAL TROPHOBLASTIC DISEASEThe typical sonographic finding in most of cases of complete hydatidiform mole is a echogenic intracavitary solid mass with intermingled small cystic loci resembling a snow storm corresponding to the vesicles that macroscopically characterize this condition The higher the gestational age the larger the vesicles visualized as homogeneous anechoic images increasing the method specificity The ultrasonography sensitivity will depend on the gestational age at the moment of the diagnosis Ultrasonography can detect vesicles with gt 2 mm in diameter In early pregnancies with trophoblastic disease the sonographic method accuracy is limited hindering the differentiation of gestational trophoblastic disease from other conditions involving the endometrial cavity
Partial hydatidiform mole offers higher diagnostic difficulty by ultrasonography In a reasonable number of cases this disease presents as an empty gestational sac corresponding to anembryonic gestation or as early embryo death However two criteria have been described in the literature gestational sac transverseanteroposterior diameter ratio gt 15 and cystic changes irregularity of increase in echogenicity of decidualplacenta or myometrial reaction
ECTOPIC PREGNANCYSonographic findings of ectopic pregnancy will vary as a function of the gestational age and site Classically the following sonographic findings are described tubal ring sign adnexal disorganized mass molded to the adnexa andor cul de sac solid organized mass with regular margins mimicking a pediculated myomatous nodule clinically progressing with low β-hCGlevels and presence of a live extrauterine conceptus Uncommon gestational sites may be observed such as abdominal ectopic pregnancy cervical ectopic pregnancy and ectopic pregnancy in a previous Cesarean section pregnancy
Subchorionic hemorrhage (SCH) occurs when there is
perigestational haemorrhage and blood collects between the uterine wall and the chorionic membrane in pregnancy It is a frequent cause of first and second trimester bleedingEpidemiologyIt typically occurs within the first 20 weeks of gestation If seen in the first 10-14 days of gestation they are also sometimes termed implantation bleedsRadiographic featuresUltrasound crescentic collection with elevation of the chorionic membranedepending on the time elapsed since bleeding the collection will have variable echotexture
acute hyperechoic and may be difficult to differentiate from adjacent chorionsubacute-chronic decreasing echogenicity with time
in almost all cases there is extension of the hematoma towards the margin of the placenta
First trimester SCH (subchorionic bleed)
First trimester SCH (subchorionic bleed)
Extensive hematoma in a woman with chronic bleeding
Subchorionic hemorrhage
Conjoined twins are a rare and complex complication of
monozygotic twinning which is associated with high perinatal mortality Early prenatal diagnosis of conjoined twins allows better counselling of the parents regarding the management options including continuation of pregnancy with post-natal surgery termination of pregnancy or selective fetocide in case of a triplet pregnancy With the introduction of high-resolution and transvaginal ultrasound imaging accurate prenatal diagnosis of conjoined twins is possible early in pregnancy Although first-trimester diagnosis of conjoined twins is feasible false-positive cases are common before 10 weeks because earlier in gestation fetal movements are limited and monoamniotic twins may appear conjoined As most parents opt for immediate termination of pregnancy at confirmation of the diagnosis there are limited data on the prenatal follow-up of conjoined twins detailed analysis of case reports where 3D imaging was used indicates that this modality does not improve on the diagnosis made by 2D ultrasound Overall very early prenatal diagnosis and first-trimester 3D imaging provide very little additional practical medical information compared to the 11-14 weeks ultrasound examination
Images of the conjoined twins there are two heads with conjoined body
Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You

5 week gestation Yolk Sac Only seen The yolk sac will be visible before a clearly definable embryonic pole
Mean Sac Diameter measurement is used to determine gestational age before a Crown Rump length can be clearly measured The average sac diameter is determined by measuring the length width and height then dividing by 3
The very early embryonic heart will be a subtle flicker This may be measured using M-Mode(avoid Doppler in the first trimester due to risks of bioeffects)Initially the heart rate may be slow
The Crown Rump Length (CRL) measurement in a 6 week gestation A mass of fetal cells separate from the yolk sac first becomes apparent on transvaginal ultrasound just after the 6th week of gestation This mass of cells is known as the fetal pole
YOLK SACThe yolk sac appears during the 5th week It is the second structure to appear after the GS It should be round with an anechoic centre It should not be calcified misshapen or gt5mm from the inner to inner diameter Yolk sacs larger than 6 mm are usually indicative of an abnormal pregnancy Failure to identify (with transvaginal ultrasound) a yolk sac when the gestational sac has grown to 12 mm is also usually indicative of a failed pregnancy
HEART BEATUsing a transvaginal approach the fetal heart beat can be seen flickering before the fetal pole is even identified It will be seen alongside the yolk sac It may be below 100 beats per minute but this will increase to between 120- 180 beats per minute by 7 weeks In the early scans at 5-6 weeks just visualizing a heart beating is the important thing Failure to identify fetal cardiac activity in a fetus whose overall length is greater than 4 mm is an ominous signSometimes there is difficulty distinguishing between the maternal pulse and fetal heart beat Often technicians will take the mothers pulse at the same time to check if it is the fetus or the mothers
CROWN RUMP LENGTH (CRL)The CRL is a reproducible and accurate method for measuring and dating a fetusEarly ultrasonographers used this term (CRL) because early fetuses also adopted the sitting in the chair posture in early pregnancy After 12 weeks the accuracy of CRL in predicting gestational age diminishes and is replaced by measurement of the fetal biparietal diameter In at least some respects the term crown rump length is misleadingThere is no fetal crown and no fetal rump to measure for most of the first trimester Until 53 days from the LMP the most caudad portion of the fetal cell mass is the caudal neurospone followed by the tail Only after 53 days is the fetal rump the most caudal portion of the fetusUntil 60 days from the LMP the most cephalad portion of the fetal cell mass is initially the rostral neurospore and later the cervical flexure After 60 days the fetal head becomes the most cephalad portion of the fetal cell massWhat is really measured during this early development of the fetus is the longest fetal diameterFrom 6 weeks to 9 12 weeks gestational age the fetal CRL grows at a rate of about 1 mm per day
Measure the crown rump length(CRL) to estimate gestational age
At 10 weeks visualize 4 jointed limbs feet and hands
NUCHAL TRANSLUCENCY
From 12 weeks the basic morphology of the fetus is visible
The Nuchal Translucency is used to provide a risk assessment for chromosomal abnormalities specifically Trisomies 1318 and 21 (Downs Syndrome)
The legs are usually crossed at the ankles Confirm the presence and symmetry of the long bones
The correct angle the feet to legs can be confirmed They should be at 90 degrees ie perpendicular or Talipes should be suspected
The humerus radius and ulna and the presence of hands areimaged from 11 weeks
12 week choroids take up most of the space within the ventricles
TWINS Initially twins may be identified as 2 separate gestational sacs (ie diamniotic dichorionic) They may be 2 fetal poles within the same gestational sac (monochorionic) It is easier to determine chorionicity earlier in the pregnancy depending on the chorionicity and amnionicityIt is a sad situation when a vanishing twin occurs which is about 20 of twin pregnancies In these cases one of the twins fails to grow and thrive Instead its development arrests and it is reabsorbed with no evidence at delivery of the twin pregnancy
Monoamniotic Twins Dichorionic diamniotic Twins
TRIPLETS
Triplets with 2 sacs Monoamniotic monochorionic twins and a normal single
GRAPHS TO DETERMINE GESTATIONAL AGEDepending on the age of the gestation these graphs can be used to determine the correct EDD
Mean Sac Diameter measurement is used to determine gestational age before a Crown Rump length can be clearly measured The average sac diameter is determined by measuring the length width and height then dividing by 3
Once a fetal Pole can be visualized the CRL measurement is the most accurate method for dating the pregnancy
COMMON PATHOLOGYThickened Nuchal Translucency(NL)Partial Ovular DetachmentRetained products of conceptionAnembryonic GestationGestational trophoblastic diseaseMiscarriageEctopic PregnancySubchorionic hemorrhageConjoined TwinsAntepartum HemorrhageCheck heart beatCheck causes of bleeding
Thickened Nuchal Translucency (NT)
bull One of the parameters used in sequential screening (SS) for Downrsquos syndrome in first trimester
ndash SS Pregnancy associated plasma protein levels hCG levels NT thickness
bull Measured during 11-14 wks gestational age
bull Seen on sagittal image as increased subcutaneous non-septated fluid in posterior fetal neck
bull Measurement gt3mm usually considered abnormal however exact cut off measurements are dependent on maternal agegestational age
bull Detection rate of screening for Downrsquos Syndrome in first trimester
ndash sequential screening with NT 82-87
ndash NT alone 64-70
Thickened Nuchal Translucency (NT)
Thickened Nuchal Translucency
PARTIAL OVULAR DETACHMENTThe maternal circulation inside the placenta starts peripherally (in the placental margins) and is associated to physiological oxidative phenomena that may lead to membranes rupture and formation The abnormal development of such membranes may result in subchorionic hemorrhage enhancing the predisposition to an adverse gestational outcome at the third trimester (PPROM and PTL)Such abnormality is common and also denominated as subchorionic hemorrhage or trophoblastic hematoma being visualized in more than 18 of cases of threatened miscarriage The presence of fetal heart activity confers an excellent prognosis Clinically subchorionic hemorrhage may course with vaginal bleeding At ultrasonography a crescent-shaped shadow is observed adjacent to the gestational sac with debris Gestational sac compression and consequential deformation may occur In most of cases a two-week follow-up evaluation confirms the hematoma resorption
Retained products of conception are characterized by a
thickened disorganized and heterogeneous endometrium with ill-defined mucosal layers and cavitary line either with or without the presence of gestational sac Clinically the women presents abdominal pain and relative vaginal bleeding(14) In the presence of an intact gestational sac and closed cervix the difficulty in a spontaneous resolution will be higher requiring surgical evacuation
Retained products of conception
Transvaginal sonography without (A) and with (B) color Doppler imaging in a case of RPC with endometrial expansion (arrows)
Images retained products conception
EARLY EMBRYO DEATHSome sonographic findings characterize an embryo death in the first half of the first trimester in early phases before the crown-rump length can be measured The following aspects are highlighted small hyperechoic yolk sac or hydropic yolk sac increased in volume with diameter gt 7 mm or even small amniotic cavity disproportionate to the gestational sac size Before the 9th week small gestational sac may be associated with aneuploidy
Failed early pregnancy
ANEMBRYONIC GESTATIONAt transvaginal ultrasonography the yolk sac should be visualized in a gestational sac with mean diameter gt 10 mm The absence of a yolk sac within the gestational sac with gt 10 mm in mean diameter or the absence of a yolk sac within the gestational sac with gt 16 mm in diameter characterize anembryonic gestation
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
GESTATIONAL TROPHOBLASTIC DISEASEThe typical sonographic finding in most of cases of complete hydatidiform mole is a echogenic intracavitary solid mass with intermingled small cystic loci resembling a snow storm corresponding to the vesicles that macroscopically characterize this condition The higher the gestational age the larger the vesicles visualized as homogeneous anechoic images increasing the method specificity The ultrasonography sensitivity will depend on the gestational age at the moment of the diagnosis Ultrasonography can detect vesicles with gt 2 mm in diameter In early pregnancies with trophoblastic disease the sonographic method accuracy is limited hindering the differentiation of gestational trophoblastic disease from other conditions involving the endometrial cavity
Partial hydatidiform mole offers higher diagnostic difficulty by ultrasonography In a reasonable number of cases this disease presents as an empty gestational sac corresponding to anembryonic gestation or as early embryo death However two criteria have been described in the literature gestational sac transverseanteroposterior diameter ratio gt 15 and cystic changes irregularity of increase in echogenicity of decidualplacenta or myometrial reaction
ECTOPIC PREGNANCYSonographic findings of ectopic pregnancy will vary as a function of the gestational age and site Classically the following sonographic findings are described tubal ring sign adnexal disorganized mass molded to the adnexa andor cul de sac solid organized mass with regular margins mimicking a pediculated myomatous nodule clinically progressing with low β-hCGlevels and presence of a live extrauterine conceptus Uncommon gestational sites may be observed such as abdominal ectopic pregnancy cervical ectopic pregnancy and ectopic pregnancy in a previous Cesarean section pregnancy
Subchorionic hemorrhage (SCH) occurs when there is
perigestational haemorrhage and blood collects between the uterine wall and the chorionic membrane in pregnancy It is a frequent cause of first and second trimester bleedingEpidemiologyIt typically occurs within the first 20 weeks of gestation If seen in the first 10-14 days of gestation they are also sometimes termed implantation bleedsRadiographic featuresUltrasound crescentic collection with elevation of the chorionic membranedepending on the time elapsed since bleeding the collection will have variable echotexture
acute hyperechoic and may be difficult to differentiate from adjacent chorionsubacute-chronic decreasing echogenicity with time
in almost all cases there is extension of the hematoma towards the margin of the placenta
First trimester SCH (subchorionic bleed)
First trimester SCH (subchorionic bleed)
Extensive hematoma in a woman with chronic bleeding
Subchorionic hemorrhage
Conjoined twins are a rare and complex complication of
monozygotic twinning which is associated with high perinatal mortality Early prenatal diagnosis of conjoined twins allows better counselling of the parents regarding the management options including continuation of pregnancy with post-natal surgery termination of pregnancy or selective fetocide in case of a triplet pregnancy With the introduction of high-resolution and transvaginal ultrasound imaging accurate prenatal diagnosis of conjoined twins is possible early in pregnancy Although first-trimester diagnosis of conjoined twins is feasible false-positive cases are common before 10 weeks because earlier in gestation fetal movements are limited and monoamniotic twins may appear conjoined As most parents opt for immediate termination of pregnancy at confirmation of the diagnosis there are limited data on the prenatal follow-up of conjoined twins detailed analysis of case reports where 3D imaging was used indicates that this modality does not improve on the diagnosis made by 2D ultrasound Overall very early prenatal diagnosis and first-trimester 3D imaging provide very little additional practical medical information compared to the 11-14 weeks ultrasound examination
Images of the conjoined twins there are two heads with conjoined body
Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You
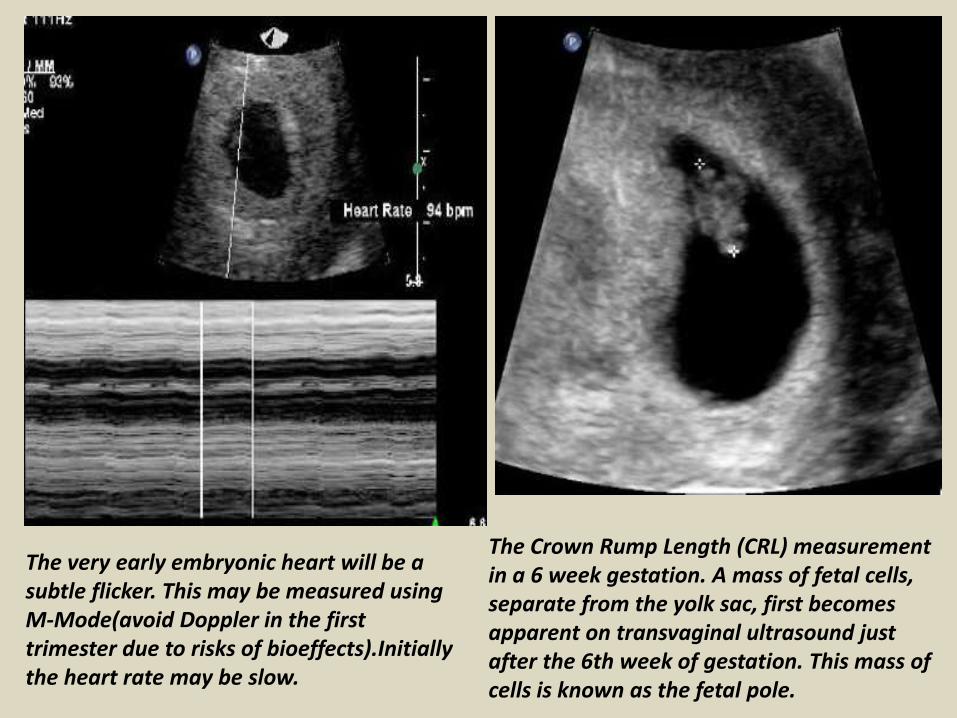
The very early embryonic heart will be a subtle flicker This may be measured using M-Mode(avoid Doppler in the first trimester due to risks of bioeffects)Initially the heart rate may be slow
The Crown Rump Length (CRL) measurement in a 6 week gestation A mass of fetal cells separate from the yolk sac first becomes apparent on transvaginal ultrasound just after the 6th week of gestation This mass of cells is known as the fetal pole
YOLK SACThe yolk sac appears during the 5th week It is the second structure to appear after the GS It should be round with an anechoic centre It should not be calcified misshapen or gt5mm from the inner to inner diameter Yolk sacs larger than 6 mm are usually indicative of an abnormal pregnancy Failure to identify (with transvaginal ultrasound) a yolk sac when the gestational sac has grown to 12 mm is also usually indicative of a failed pregnancy
HEART BEATUsing a transvaginal approach the fetal heart beat can be seen flickering before the fetal pole is even identified It will be seen alongside the yolk sac It may be below 100 beats per minute but this will increase to between 120- 180 beats per minute by 7 weeks In the early scans at 5-6 weeks just visualizing a heart beating is the important thing Failure to identify fetal cardiac activity in a fetus whose overall length is greater than 4 mm is an ominous signSometimes there is difficulty distinguishing between the maternal pulse and fetal heart beat Often technicians will take the mothers pulse at the same time to check if it is the fetus or the mothers
CROWN RUMP LENGTH (CRL)The CRL is a reproducible and accurate method for measuring and dating a fetusEarly ultrasonographers used this term (CRL) because early fetuses also adopted the sitting in the chair posture in early pregnancy After 12 weeks the accuracy of CRL in predicting gestational age diminishes and is replaced by measurement of the fetal biparietal diameter In at least some respects the term crown rump length is misleadingThere is no fetal crown and no fetal rump to measure for most of the first trimester Until 53 days from the LMP the most caudad portion of the fetal cell mass is the caudal neurospone followed by the tail Only after 53 days is the fetal rump the most caudal portion of the fetusUntil 60 days from the LMP the most cephalad portion of the fetal cell mass is initially the rostral neurospore and later the cervical flexure After 60 days the fetal head becomes the most cephalad portion of the fetal cell massWhat is really measured during this early development of the fetus is the longest fetal diameterFrom 6 weeks to 9 12 weeks gestational age the fetal CRL grows at a rate of about 1 mm per day
Measure the crown rump length(CRL) to estimate gestational age
At 10 weeks visualize 4 jointed limbs feet and hands
NUCHAL TRANSLUCENCY
From 12 weeks the basic morphology of the fetus is visible
The Nuchal Translucency is used to provide a risk assessment for chromosomal abnormalities specifically Trisomies 1318 and 21 (Downs Syndrome)
The legs are usually crossed at the ankles Confirm the presence and symmetry of the long bones
The correct angle the feet to legs can be confirmed They should be at 90 degrees ie perpendicular or Talipes should be suspected
The humerus radius and ulna and the presence of hands areimaged from 11 weeks
12 week choroids take up most of the space within the ventricles
TWINS Initially twins may be identified as 2 separate gestational sacs (ie diamniotic dichorionic) They may be 2 fetal poles within the same gestational sac (monochorionic) It is easier to determine chorionicity earlier in the pregnancy depending on the chorionicity and amnionicityIt is a sad situation when a vanishing twin occurs which is about 20 of twin pregnancies In these cases one of the twins fails to grow and thrive Instead its development arrests and it is reabsorbed with no evidence at delivery of the twin pregnancy
Monoamniotic Twins Dichorionic diamniotic Twins
TRIPLETS
Triplets with 2 sacs Monoamniotic monochorionic twins and a normal single
GRAPHS TO DETERMINE GESTATIONAL AGEDepending on the age of the gestation these graphs can be used to determine the correct EDD
Mean Sac Diameter measurement is used to determine gestational age before a Crown Rump length can be clearly measured The average sac diameter is determined by measuring the length width and height then dividing by 3
Once a fetal Pole can be visualized the CRL measurement is the most accurate method for dating the pregnancy
COMMON PATHOLOGYThickened Nuchal Translucency(NL)Partial Ovular DetachmentRetained products of conceptionAnembryonic GestationGestational trophoblastic diseaseMiscarriageEctopic PregnancySubchorionic hemorrhageConjoined TwinsAntepartum HemorrhageCheck heart beatCheck causes of bleeding
Thickened Nuchal Translucency (NT)
bull One of the parameters used in sequential screening (SS) for Downrsquos syndrome in first trimester
ndash SS Pregnancy associated plasma protein levels hCG levels NT thickness
bull Measured during 11-14 wks gestational age
bull Seen on sagittal image as increased subcutaneous non-septated fluid in posterior fetal neck
bull Measurement gt3mm usually considered abnormal however exact cut off measurements are dependent on maternal agegestational age
bull Detection rate of screening for Downrsquos Syndrome in first trimester
ndash sequential screening with NT 82-87
ndash NT alone 64-70
Thickened Nuchal Translucency (NT)
Thickened Nuchal Translucency
PARTIAL OVULAR DETACHMENTThe maternal circulation inside the placenta starts peripherally (in the placental margins) and is associated to physiological oxidative phenomena that may lead to membranes rupture and formation The abnormal development of such membranes may result in subchorionic hemorrhage enhancing the predisposition to an adverse gestational outcome at the third trimester (PPROM and PTL)Such abnormality is common and also denominated as subchorionic hemorrhage or trophoblastic hematoma being visualized in more than 18 of cases of threatened miscarriage The presence of fetal heart activity confers an excellent prognosis Clinically subchorionic hemorrhage may course with vaginal bleeding At ultrasonography a crescent-shaped shadow is observed adjacent to the gestational sac with debris Gestational sac compression and consequential deformation may occur In most of cases a two-week follow-up evaluation confirms the hematoma resorption
Retained products of conception are characterized by a
thickened disorganized and heterogeneous endometrium with ill-defined mucosal layers and cavitary line either with or without the presence of gestational sac Clinically the women presents abdominal pain and relative vaginal bleeding(14) In the presence of an intact gestational sac and closed cervix the difficulty in a spontaneous resolution will be higher requiring surgical evacuation
Retained products of conception
Transvaginal sonography without (A) and with (B) color Doppler imaging in a case of RPC with endometrial expansion (arrows)
Images retained products conception
EARLY EMBRYO DEATHSome sonographic findings characterize an embryo death in the first half of the first trimester in early phases before the crown-rump length can be measured The following aspects are highlighted small hyperechoic yolk sac or hydropic yolk sac increased in volume with diameter gt 7 mm or even small amniotic cavity disproportionate to the gestational sac size Before the 9th week small gestational sac may be associated with aneuploidy
Failed early pregnancy
ANEMBRYONIC GESTATIONAt transvaginal ultrasonography the yolk sac should be visualized in a gestational sac with mean diameter gt 10 mm The absence of a yolk sac within the gestational sac with gt 10 mm in mean diameter or the absence of a yolk sac within the gestational sac with gt 16 mm in diameter characterize anembryonic gestation
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
GESTATIONAL TROPHOBLASTIC DISEASEThe typical sonographic finding in most of cases of complete hydatidiform mole is a echogenic intracavitary solid mass with intermingled small cystic loci resembling a snow storm corresponding to the vesicles that macroscopically characterize this condition The higher the gestational age the larger the vesicles visualized as homogeneous anechoic images increasing the method specificity The ultrasonography sensitivity will depend on the gestational age at the moment of the diagnosis Ultrasonography can detect vesicles with gt 2 mm in diameter In early pregnancies with trophoblastic disease the sonographic method accuracy is limited hindering the differentiation of gestational trophoblastic disease from other conditions involving the endometrial cavity
Partial hydatidiform mole offers higher diagnostic difficulty by ultrasonography In a reasonable number of cases this disease presents as an empty gestational sac corresponding to anembryonic gestation or as early embryo death However two criteria have been described in the literature gestational sac transverseanteroposterior diameter ratio gt 15 and cystic changes irregularity of increase in echogenicity of decidualplacenta or myometrial reaction
ECTOPIC PREGNANCYSonographic findings of ectopic pregnancy will vary as a function of the gestational age and site Classically the following sonographic findings are described tubal ring sign adnexal disorganized mass molded to the adnexa andor cul de sac solid organized mass with regular margins mimicking a pediculated myomatous nodule clinically progressing with low β-hCGlevels and presence of a live extrauterine conceptus Uncommon gestational sites may be observed such as abdominal ectopic pregnancy cervical ectopic pregnancy and ectopic pregnancy in a previous Cesarean section pregnancy
Subchorionic hemorrhage (SCH) occurs when there is
perigestational haemorrhage and blood collects between the uterine wall and the chorionic membrane in pregnancy It is a frequent cause of first and second trimester bleedingEpidemiologyIt typically occurs within the first 20 weeks of gestation If seen in the first 10-14 days of gestation they are also sometimes termed implantation bleedsRadiographic featuresUltrasound crescentic collection with elevation of the chorionic membranedepending on the time elapsed since bleeding the collection will have variable echotexture
acute hyperechoic and may be difficult to differentiate from adjacent chorionsubacute-chronic decreasing echogenicity with time
in almost all cases there is extension of the hematoma towards the margin of the placenta
First trimester SCH (subchorionic bleed)
First trimester SCH (subchorionic bleed)
Extensive hematoma in a woman with chronic bleeding
Subchorionic hemorrhage
Conjoined twins are a rare and complex complication of
monozygotic twinning which is associated with high perinatal mortality Early prenatal diagnosis of conjoined twins allows better counselling of the parents regarding the management options including continuation of pregnancy with post-natal surgery termination of pregnancy or selective fetocide in case of a triplet pregnancy With the introduction of high-resolution and transvaginal ultrasound imaging accurate prenatal diagnosis of conjoined twins is possible early in pregnancy Although first-trimester diagnosis of conjoined twins is feasible false-positive cases are common before 10 weeks because earlier in gestation fetal movements are limited and monoamniotic twins may appear conjoined As most parents opt for immediate termination of pregnancy at confirmation of the diagnosis there are limited data on the prenatal follow-up of conjoined twins detailed analysis of case reports where 3D imaging was used indicates that this modality does not improve on the diagnosis made by 2D ultrasound Overall very early prenatal diagnosis and first-trimester 3D imaging provide very little additional practical medical information compared to the 11-14 weeks ultrasound examination
Images of the conjoined twins there are two heads with conjoined body
Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You
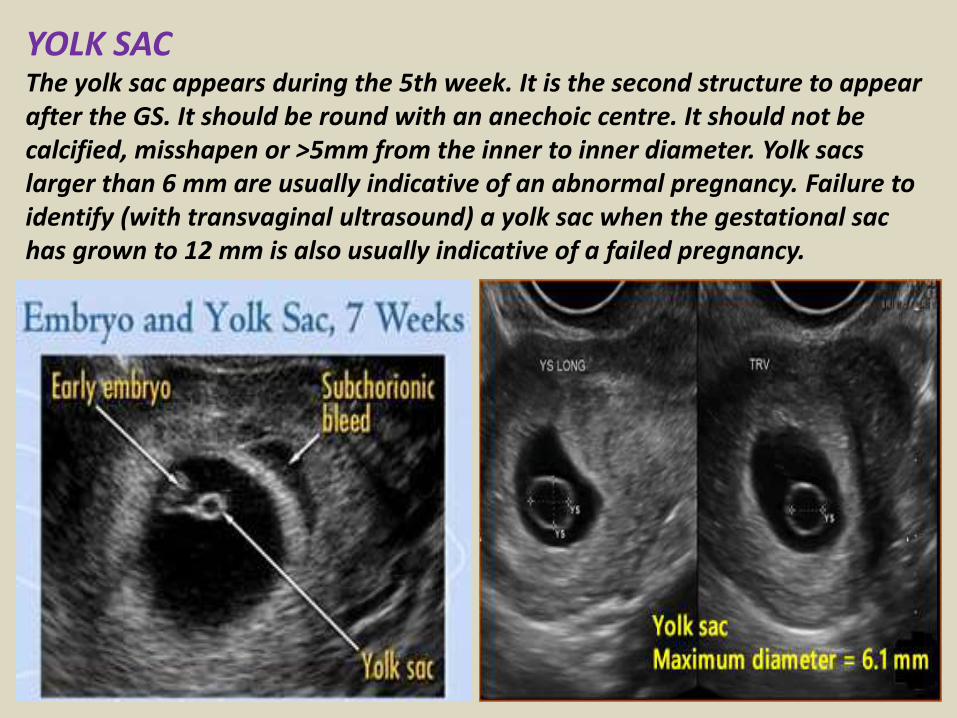
YOLK SACThe yolk sac appears during the 5th week It is the second structure to appear after the GS It should be round with an anechoic centre It should not be calcified misshapen or gt5mm from the inner to inner diameter Yolk sacs larger than 6 mm are usually indicative of an abnormal pregnancy Failure to identify (with transvaginal ultrasound) a yolk sac when the gestational sac has grown to 12 mm is also usually indicative of a failed pregnancy
HEART BEATUsing a transvaginal approach the fetal heart beat can be seen flickering before the fetal pole is even identified It will be seen alongside the yolk sac It may be below 100 beats per minute but this will increase to between 120- 180 beats per minute by 7 weeks In the early scans at 5-6 weeks just visualizing a heart beating is the important thing Failure to identify fetal cardiac activity in a fetus whose overall length is greater than 4 mm is an ominous signSometimes there is difficulty distinguishing between the maternal pulse and fetal heart beat Often technicians will take the mothers pulse at the same time to check if it is the fetus or the mothers
CROWN RUMP LENGTH (CRL)The CRL is a reproducible and accurate method for measuring and dating a fetusEarly ultrasonographers used this term (CRL) because early fetuses also adopted the sitting in the chair posture in early pregnancy After 12 weeks the accuracy of CRL in predicting gestational age diminishes and is replaced by measurement of the fetal biparietal diameter In at least some respects the term crown rump length is misleadingThere is no fetal crown and no fetal rump to measure for most of the first trimester Until 53 days from the LMP the most caudad portion of the fetal cell mass is the caudal neurospone followed by the tail Only after 53 days is the fetal rump the most caudal portion of the fetusUntil 60 days from the LMP the most cephalad portion of the fetal cell mass is initially the rostral neurospore and later the cervical flexure After 60 days the fetal head becomes the most cephalad portion of the fetal cell massWhat is really measured during this early development of the fetus is the longest fetal diameterFrom 6 weeks to 9 12 weeks gestational age the fetal CRL grows at a rate of about 1 mm per day
Measure the crown rump length(CRL) to estimate gestational age
At 10 weeks visualize 4 jointed limbs feet and hands
NUCHAL TRANSLUCENCY
From 12 weeks the basic morphology of the fetus is visible
The Nuchal Translucency is used to provide a risk assessment for chromosomal abnormalities specifically Trisomies 1318 and 21 (Downs Syndrome)
The legs are usually crossed at the ankles Confirm the presence and symmetry of the long bones
The correct angle the feet to legs can be confirmed They should be at 90 degrees ie perpendicular or Talipes should be suspected
The humerus radius and ulna and the presence of hands areimaged from 11 weeks
12 week choroids take up most of the space within the ventricles
TWINS Initially twins may be identified as 2 separate gestational sacs (ie diamniotic dichorionic) They may be 2 fetal poles within the same gestational sac (monochorionic) It is easier to determine chorionicity earlier in the pregnancy depending on the chorionicity and amnionicityIt is a sad situation when a vanishing twin occurs which is about 20 of twin pregnancies In these cases one of the twins fails to grow and thrive Instead its development arrests and it is reabsorbed with no evidence at delivery of the twin pregnancy
Monoamniotic Twins Dichorionic diamniotic Twins
TRIPLETS
Triplets with 2 sacs Monoamniotic monochorionic twins and a normal single
GRAPHS TO DETERMINE GESTATIONAL AGEDepending on the age of the gestation these graphs can be used to determine the correct EDD
Mean Sac Diameter measurement is used to determine gestational age before a Crown Rump length can be clearly measured The average sac diameter is determined by measuring the length width and height then dividing by 3
Once a fetal Pole can be visualized the CRL measurement is the most accurate method for dating the pregnancy
COMMON PATHOLOGYThickened Nuchal Translucency(NL)Partial Ovular DetachmentRetained products of conceptionAnembryonic GestationGestational trophoblastic diseaseMiscarriageEctopic PregnancySubchorionic hemorrhageConjoined TwinsAntepartum HemorrhageCheck heart beatCheck causes of bleeding
Thickened Nuchal Translucency (NT)
bull One of the parameters used in sequential screening (SS) for Downrsquos syndrome in first trimester
ndash SS Pregnancy associated plasma protein levels hCG levels NT thickness
bull Measured during 11-14 wks gestational age
bull Seen on sagittal image as increased subcutaneous non-septated fluid in posterior fetal neck
bull Measurement gt3mm usually considered abnormal however exact cut off measurements are dependent on maternal agegestational age
bull Detection rate of screening for Downrsquos Syndrome in first trimester
ndash sequential screening with NT 82-87
ndash NT alone 64-70
Thickened Nuchal Translucency (NT)
Thickened Nuchal Translucency
PARTIAL OVULAR DETACHMENTThe maternal circulation inside the placenta starts peripherally (in the placental margins) and is associated to physiological oxidative phenomena that may lead to membranes rupture and formation The abnormal development of such membranes may result in subchorionic hemorrhage enhancing the predisposition to an adverse gestational outcome at the third trimester (PPROM and PTL)Such abnormality is common and also denominated as subchorionic hemorrhage or trophoblastic hematoma being visualized in more than 18 of cases of threatened miscarriage The presence of fetal heart activity confers an excellent prognosis Clinically subchorionic hemorrhage may course with vaginal bleeding At ultrasonography a crescent-shaped shadow is observed adjacent to the gestational sac with debris Gestational sac compression and consequential deformation may occur In most of cases a two-week follow-up evaluation confirms the hematoma resorption
Retained products of conception are characterized by a
thickened disorganized and heterogeneous endometrium with ill-defined mucosal layers and cavitary line either with or without the presence of gestational sac Clinically the women presents abdominal pain and relative vaginal bleeding(14) In the presence of an intact gestational sac and closed cervix the difficulty in a spontaneous resolution will be higher requiring surgical evacuation
Retained products of conception
Transvaginal sonography without (A) and with (B) color Doppler imaging in a case of RPC with endometrial expansion (arrows)
Images retained products conception
EARLY EMBRYO DEATHSome sonographic findings characterize an embryo death in the first half of the first trimester in early phases before the crown-rump length can be measured The following aspects are highlighted small hyperechoic yolk sac or hydropic yolk sac increased in volume with diameter gt 7 mm or even small amniotic cavity disproportionate to the gestational sac size Before the 9th week small gestational sac may be associated with aneuploidy
Failed early pregnancy
ANEMBRYONIC GESTATIONAt transvaginal ultrasonography the yolk sac should be visualized in a gestational sac with mean diameter gt 10 mm The absence of a yolk sac within the gestational sac with gt 10 mm in mean diameter or the absence of a yolk sac within the gestational sac with gt 16 mm in diameter characterize anembryonic gestation
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
GESTATIONAL TROPHOBLASTIC DISEASEThe typical sonographic finding in most of cases of complete hydatidiform mole is a echogenic intracavitary solid mass with intermingled small cystic loci resembling a snow storm corresponding to the vesicles that macroscopically characterize this condition The higher the gestational age the larger the vesicles visualized as homogeneous anechoic images increasing the method specificity The ultrasonography sensitivity will depend on the gestational age at the moment of the diagnosis Ultrasonography can detect vesicles with gt 2 mm in diameter In early pregnancies with trophoblastic disease the sonographic method accuracy is limited hindering the differentiation of gestational trophoblastic disease from other conditions involving the endometrial cavity
Partial hydatidiform mole offers higher diagnostic difficulty by ultrasonography In a reasonable number of cases this disease presents as an empty gestational sac corresponding to anembryonic gestation or as early embryo death However two criteria have been described in the literature gestational sac transverseanteroposterior diameter ratio gt 15 and cystic changes irregularity of increase in echogenicity of decidualplacenta or myometrial reaction
ECTOPIC PREGNANCYSonographic findings of ectopic pregnancy will vary as a function of the gestational age and site Classically the following sonographic findings are described tubal ring sign adnexal disorganized mass molded to the adnexa andor cul de sac solid organized mass with regular margins mimicking a pediculated myomatous nodule clinically progressing with low β-hCGlevels and presence of a live extrauterine conceptus Uncommon gestational sites may be observed such as abdominal ectopic pregnancy cervical ectopic pregnancy and ectopic pregnancy in a previous Cesarean section pregnancy
Subchorionic hemorrhage (SCH) occurs when there is
perigestational haemorrhage and blood collects between the uterine wall and the chorionic membrane in pregnancy It is a frequent cause of first and second trimester bleedingEpidemiologyIt typically occurs within the first 20 weeks of gestation If seen in the first 10-14 days of gestation they are also sometimes termed implantation bleedsRadiographic featuresUltrasound crescentic collection with elevation of the chorionic membranedepending on the time elapsed since bleeding the collection will have variable echotexture
acute hyperechoic and may be difficult to differentiate from adjacent chorionsubacute-chronic decreasing echogenicity with time
in almost all cases there is extension of the hematoma towards the margin of the placenta
First trimester SCH (subchorionic bleed)
First trimester SCH (subchorionic bleed)
Extensive hematoma in a woman with chronic bleeding
Subchorionic hemorrhage
Conjoined twins are a rare and complex complication of
monozygotic twinning which is associated with high perinatal mortality Early prenatal diagnosis of conjoined twins allows better counselling of the parents regarding the management options including continuation of pregnancy with post-natal surgery termination of pregnancy or selective fetocide in case of a triplet pregnancy With the introduction of high-resolution and transvaginal ultrasound imaging accurate prenatal diagnosis of conjoined twins is possible early in pregnancy Although first-trimester diagnosis of conjoined twins is feasible false-positive cases are common before 10 weeks because earlier in gestation fetal movements are limited and monoamniotic twins may appear conjoined As most parents opt for immediate termination of pregnancy at confirmation of the diagnosis there are limited data on the prenatal follow-up of conjoined twins detailed analysis of case reports where 3D imaging was used indicates that this modality does not improve on the diagnosis made by 2D ultrasound Overall very early prenatal diagnosis and first-trimester 3D imaging provide very little additional practical medical information compared to the 11-14 weeks ultrasound examination
Images of the conjoined twins there are two heads with conjoined body
Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You

HEART BEATUsing a transvaginal approach the fetal heart beat can be seen flickering before the fetal pole is even identified It will be seen alongside the yolk sac It may be below 100 beats per minute but this will increase to between 120- 180 beats per minute by 7 weeks In the early scans at 5-6 weeks just visualizing a heart beating is the important thing Failure to identify fetal cardiac activity in a fetus whose overall length is greater than 4 mm is an ominous signSometimes there is difficulty distinguishing between the maternal pulse and fetal heart beat Often technicians will take the mothers pulse at the same time to check if it is the fetus or the mothers
CROWN RUMP LENGTH (CRL)The CRL is a reproducible and accurate method for measuring and dating a fetusEarly ultrasonographers used this term (CRL) because early fetuses also adopted the sitting in the chair posture in early pregnancy After 12 weeks the accuracy of CRL in predicting gestational age diminishes and is replaced by measurement of the fetal biparietal diameter In at least some respects the term crown rump length is misleadingThere is no fetal crown and no fetal rump to measure for most of the first trimester Until 53 days from the LMP the most caudad portion of the fetal cell mass is the caudal neurospone followed by the tail Only after 53 days is the fetal rump the most caudal portion of the fetusUntil 60 days from the LMP the most cephalad portion of the fetal cell mass is initially the rostral neurospore and later the cervical flexure After 60 days the fetal head becomes the most cephalad portion of the fetal cell massWhat is really measured during this early development of the fetus is the longest fetal diameterFrom 6 weeks to 9 12 weeks gestational age the fetal CRL grows at a rate of about 1 mm per day
Measure the crown rump length(CRL) to estimate gestational age
At 10 weeks visualize 4 jointed limbs feet and hands
NUCHAL TRANSLUCENCY
From 12 weeks the basic morphology of the fetus is visible
The Nuchal Translucency is used to provide a risk assessment for chromosomal abnormalities specifically Trisomies 1318 and 21 (Downs Syndrome)
The legs are usually crossed at the ankles Confirm the presence and symmetry of the long bones
The correct angle the feet to legs can be confirmed They should be at 90 degrees ie perpendicular or Talipes should be suspected
The humerus radius and ulna and the presence of hands areimaged from 11 weeks
12 week choroids take up most of the space within the ventricles
TWINS Initially twins may be identified as 2 separate gestational sacs (ie diamniotic dichorionic) They may be 2 fetal poles within the same gestational sac (monochorionic) It is easier to determine chorionicity earlier in the pregnancy depending on the chorionicity and amnionicityIt is a sad situation when a vanishing twin occurs which is about 20 of twin pregnancies In these cases one of the twins fails to grow and thrive Instead its development arrests and it is reabsorbed with no evidence at delivery of the twin pregnancy
Monoamniotic Twins Dichorionic diamniotic Twins
TRIPLETS
Triplets with 2 sacs Monoamniotic monochorionic twins and a normal single
GRAPHS TO DETERMINE GESTATIONAL AGEDepending on the age of the gestation these graphs can be used to determine the correct EDD
Mean Sac Diameter measurement is used to determine gestational age before a Crown Rump length can be clearly measured The average sac diameter is determined by measuring the length width and height then dividing by 3
Once a fetal Pole can be visualized the CRL measurement is the most accurate method for dating the pregnancy
COMMON PATHOLOGYThickened Nuchal Translucency(NL)Partial Ovular DetachmentRetained products of conceptionAnembryonic GestationGestational trophoblastic diseaseMiscarriageEctopic PregnancySubchorionic hemorrhageConjoined TwinsAntepartum HemorrhageCheck heart beatCheck causes of bleeding
Thickened Nuchal Translucency (NT)
bull One of the parameters used in sequential screening (SS) for Downrsquos syndrome in first trimester
ndash SS Pregnancy associated plasma protein levels hCG levels NT thickness
bull Measured during 11-14 wks gestational age
bull Seen on sagittal image as increased subcutaneous non-septated fluid in posterior fetal neck
bull Measurement gt3mm usually considered abnormal however exact cut off measurements are dependent on maternal agegestational age
bull Detection rate of screening for Downrsquos Syndrome in first trimester
ndash sequential screening with NT 82-87
ndash NT alone 64-70
Thickened Nuchal Translucency (NT)
Thickened Nuchal Translucency
PARTIAL OVULAR DETACHMENTThe maternal circulation inside the placenta starts peripherally (in the placental margins) and is associated to physiological oxidative phenomena that may lead to membranes rupture and formation The abnormal development of such membranes may result in subchorionic hemorrhage enhancing the predisposition to an adverse gestational outcome at the third trimester (PPROM and PTL)Such abnormality is common and also denominated as subchorionic hemorrhage or trophoblastic hematoma being visualized in more than 18 of cases of threatened miscarriage The presence of fetal heart activity confers an excellent prognosis Clinically subchorionic hemorrhage may course with vaginal bleeding At ultrasonography a crescent-shaped shadow is observed adjacent to the gestational sac with debris Gestational sac compression and consequential deformation may occur In most of cases a two-week follow-up evaluation confirms the hematoma resorption
Retained products of conception are characterized by a
thickened disorganized and heterogeneous endometrium with ill-defined mucosal layers and cavitary line either with or without the presence of gestational sac Clinically the women presents abdominal pain and relative vaginal bleeding(14) In the presence of an intact gestational sac and closed cervix the difficulty in a spontaneous resolution will be higher requiring surgical evacuation
Retained products of conception
Transvaginal sonography without (A) and with (B) color Doppler imaging in a case of RPC with endometrial expansion (arrows)
Images retained products conception
EARLY EMBRYO DEATHSome sonographic findings characterize an embryo death in the first half of the first trimester in early phases before the crown-rump length can be measured The following aspects are highlighted small hyperechoic yolk sac or hydropic yolk sac increased in volume with diameter gt 7 mm or even small amniotic cavity disproportionate to the gestational sac size Before the 9th week small gestational sac may be associated with aneuploidy
Failed early pregnancy
ANEMBRYONIC GESTATIONAt transvaginal ultrasonography the yolk sac should be visualized in a gestational sac with mean diameter gt 10 mm The absence of a yolk sac within the gestational sac with gt 10 mm in mean diameter or the absence of a yolk sac within the gestational sac with gt 16 mm in diameter characterize anembryonic gestation
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
GESTATIONAL TROPHOBLASTIC DISEASEThe typical sonographic finding in most of cases of complete hydatidiform mole is a echogenic intracavitary solid mass with intermingled small cystic loci resembling a snow storm corresponding to the vesicles that macroscopically characterize this condition The higher the gestational age the larger the vesicles visualized as homogeneous anechoic images increasing the method specificity The ultrasonography sensitivity will depend on the gestational age at the moment of the diagnosis Ultrasonography can detect vesicles with gt 2 mm in diameter In early pregnancies with trophoblastic disease the sonographic method accuracy is limited hindering the differentiation of gestational trophoblastic disease from other conditions involving the endometrial cavity
Partial hydatidiform mole offers higher diagnostic difficulty by ultrasonography In a reasonable number of cases this disease presents as an empty gestational sac corresponding to anembryonic gestation or as early embryo death However two criteria have been described in the literature gestational sac transverseanteroposterior diameter ratio gt 15 and cystic changes irregularity of increase in echogenicity of decidualplacenta or myometrial reaction
ECTOPIC PREGNANCYSonographic findings of ectopic pregnancy will vary as a function of the gestational age and site Classically the following sonographic findings are described tubal ring sign adnexal disorganized mass molded to the adnexa andor cul de sac solid organized mass with regular margins mimicking a pediculated myomatous nodule clinically progressing with low β-hCGlevels and presence of a live extrauterine conceptus Uncommon gestational sites may be observed such as abdominal ectopic pregnancy cervical ectopic pregnancy and ectopic pregnancy in a previous Cesarean section pregnancy
Subchorionic hemorrhage (SCH) occurs when there is
perigestational haemorrhage and blood collects between the uterine wall and the chorionic membrane in pregnancy It is a frequent cause of first and second trimester bleedingEpidemiologyIt typically occurs within the first 20 weeks of gestation If seen in the first 10-14 days of gestation they are also sometimes termed implantation bleedsRadiographic featuresUltrasound crescentic collection with elevation of the chorionic membranedepending on the time elapsed since bleeding the collection will have variable echotexture
acute hyperechoic and may be difficult to differentiate from adjacent chorionsubacute-chronic decreasing echogenicity with time
in almost all cases there is extension of the hematoma towards the margin of the placenta
First trimester SCH (subchorionic bleed)
First trimester SCH (subchorionic bleed)
Extensive hematoma in a woman with chronic bleeding
Subchorionic hemorrhage
Conjoined twins are a rare and complex complication of
monozygotic twinning which is associated with high perinatal mortality Early prenatal diagnosis of conjoined twins allows better counselling of the parents regarding the management options including continuation of pregnancy with post-natal surgery termination of pregnancy or selective fetocide in case of a triplet pregnancy With the introduction of high-resolution and transvaginal ultrasound imaging accurate prenatal diagnosis of conjoined twins is possible early in pregnancy Although first-trimester diagnosis of conjoined twins is feasible false-positive cases are common before 10 weeks because earlier in gestation fetal movements are limited and monoamniotic twins may appear conjoined As most parents opt for immediate termination of pregnancy at confirmation of the diagnosis there are limited data on the prenatal follow-up of conjoined twins detailed analysis of case reports where 3D imaging was used indicates that this modality does not improve on the diagnosis made by 2D ultrasound Overall very early prenatal diagnosis and first-trimester 3D imaging provide very little additional practical medical information compared to the 11-14 weeks ultrasound examination
Images of the conjoined twins there are two heads with conjoined body
Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You

CROWN RUMP LENGTH (CRL)The CRL is a reproducible and accurate method for measuring and dating a fetusEarly ultrasonographers used this term (CRL) because early fetuses also adopted the sitting in the chair posture in early pregnancy After 12 weeks the accuracy of CRL in predicting gestational age diminishes and is replaced by measurement of the fetal biparietal diameter In at least some respects the term crown rump length is misleadingThere is no fetal crown and no fetal rump to measure for most of the first trimester Until 53 days from the LMP the most caudad portion of the fetal cell mass is the caudal neurospone followed by the tail Only after 53 days is the fetal rump the most caudal portion of the fetusUntil 60 days from the LMP the most cephalad portion of the fetal cell mass is initially the rostral neurospore and later the cervical flexure After 60 days the fetal head becomes the most cephalad portion of the fetal cell massWhat is really measured during this early development of the fetus is the longest fetal diameterFrom 6 weeks to 9 12 weeks gestational age the fetal CRL grows at a rate of about 1 mm per day
Measure the crown rump length(CRL) to estimate gestational age
At 10 weeks visualize 4 jointed limbs feet and hands
NUCHAL TRANSLUCENCY
From 12 weeks the basic morphology of the fetus is visible
The Nuchal Translucency is used to provide a risk assessment for chromosomal abnormalities specifically Trisomies 1318 and 21 (Downs Syndrome)
The legs are usually crossed at the ankles Confirm the presence and symmetry of the long bones
The correct angle the feet to legs can be confirmed They should be at 90 degrees ie perpendicular or Talipes should be suspected
The humerus radius and ulna and the presence of hands areimaged from 11 weeks
12 week choroids take up most of the space within the ventricles
TWINS Initially twins may be identified as 2 separate gestational sacs (ie diamniotic dichorionic) They may be 2 fetal poles within the same gestational sac (monochorionic) It is easier to determine chorionicity earlier in the pregnancy depending on the chorionicity and amnionicityIt is a sad situation when a vanishing twin occurs which is about 20 of twin pregnancies In these cases one of the twins fails to grow and thrive Instead its development arrests and it is reabsorbed with no evidence at delivery of the twin pregnancy
Monoamniotic Twins Dichorionic diamniotic Twins
TRIPLETS
Triplets with 2 sacs Monoamniotic monochorionic twins and a normal single
GRAPHS TO DETERMINE GESTATIONAL AGEDepending on the age of the gestation these graphs can be used to determine the correct EDD
Mean Sac Diameter measurement is used to determine gestational age before a Crown Rump length can be clearly measured The average sac diameter is determined by measuring the length width and height then dividing by 3
Once a fetal Pole can be visualized the CRL measurement is the most accurate method for dating the pregnancy
COMMON PATHOLOGYThickened Nuchal Translucency(NL)Partial Ovular DetachmentRetained products of conceptionAnembryonic GestationGestational trophoblastic diseaseMiscarriageEctopic PregnancySubchorionic hemorrhageConjoined TwinsAntepartum HemorrhageCheck heart beatCheck causes of bleeding
Thickened Nuchal Translucency (NT)
bull One of the parameters used in sequential screening (SS) for Downrsquos syndrome in first trimester
ndash SS Pregnancy associated plasma protein levels hCG levels NT thickness
bull Measured during 11-14 wks gestational age
bull Seen on sagittal image as increased subcutaneous non-septated fluid in posterior fetal neck
bull Measurement gt3mm usually considered abnormal however exact cut off measurements are dependent on maternal agegestational age
bull Detection rate of screening for Downrsquos Syndrome in first trimester
ndash sequential screening with NT 82-87
ndash NT alone 64-70
Thickened Nuchal Translucency (NT)
Thickened Nuchal Translucency
PARTIAL OVULAR DETACHMENTThe maternal circulation inside the placenta starts peripherally (in the placental margins) and is associated to physiological oxidative phenomena that may lead to membranes rupture and formation The abnormal development of such membranes may result in subchorionic hemorrhage enhancing the predisposition to an adverse gestational outcome at the third trimester (PPROM and PTL)Such abnormality is common and also denominated as subchorionic hemorrhage or trophoblastic hematoma being visualized in more than 18 of cases of threatened miscarriage The presence of fetal heart activity confers an excellent prognosis Clinically subchorionic hemorrhage may course with vaginal bleeding At ultrasonography a crescent-shaped shadow is observed adjacent to the gestational sac with debris Gestational sac compression and consequential deformation may occur In most of cases a two-week follow-up evaluation confirms the hematoma resorption
Retained products of conception are characterized by a
thickened disorganized and heterogeneous endometrium with ill-defined mucosal layers and cavitary line either with or without the presence of gestational sac Clinically the women presents abdominal pain and relative vaginal bleeding(14) In the presence of an intact gestational sac and closed cervix the difficulty in a spontaneous resolution will be higher requiring surgical evacuation
Retained products of conception
Transvaginal sonography without (A) and with (B) color Doppler imaging in a case of RPC with endometrial expansion (arrows)
Images retained products conception
EARLY EMBRYO DEATHSome sonographic findings characterize an embryo death in the first half of the first trimester in early phases before the crown-rump length can be measured The following aspects are highlighted small hyperechoic yolk sac or hydropic yolk sac increased in volume with diameter gt 7 mm or even small amniotic cavity disproportionate to the gestational sac size Before the 9th week small gestational sac may be associated with aneuploidy
Failed early pregnancy
ANEMBRYONIC GESTATIONAt transvaginal ultrasonography the yolk sac should be visualized in a gestational sac with mean diameter gt 10 mm The absence of a yolk sac within the gestational sac with gt 10 mm in mean diameter or the absence of a yolk sac within the gestational sac with gt 16 mm in diameter characterize anembryonic gestation
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
GESTATIONAL TROPHOBLASTIC DISEASEThe typical sonographic finding in most of cases of complete hydatidiform mole is a echogenic intracavitary solid mass with intermingled small cystic loci resembling a snow storm corresponding to the vesicles that macroscopically characterize this condition The higher the gestational age the larger the vesicles visualized as homogeneous anechoic images increasing the method specificity The ultrasonography sensitivity will depend on the gestational age at the moment of the diagnosis Ultrasonography can detect vesicles with gt 2 mm in diameter In early pregnancies with trophoblastic disease the sonographic method accuracy is limited hindering the differentiation of gestational trophoblastic disease from other conditions involving the endometrial cavity
Partial hydatidiform mole offers higher diagnostic difficulty by ultrasonography In a reasonable number of cases this disease presents as an empty gestational sac corresponding to anembryonic gestation or as early embryo death However two criteria have been described in the literature gestational sac transverseanteroposterior diameter ratio gt 15 and cystic changes irregularity of increase in echogenicity of decidualplacenta or myometrial reaction
ECTOPIC PREGNANCYSonographic findings of ectopic pregnancy will vary as a function of the gestational age and site Classically the following sonographic findings are described tubal ring sign adnexal disorganized mass molded to the adnexa andor cul de sac solid organized mass with regular margins mimicking a pediculated myomatous nodule clinically progressing with low β-hCGlevels and presence of a live extrauterine conceptus Uncommon gestational sites may be observed such as abdominal ectopic pregnancy cervical ectopic pregnancy and ectopic pregnancy in a previous Cesarean section pregnancy
Subchorionic hemorrhage (SCH) occurs when there is
perigestational haemorrhage and blood collects between the uterine wall and the chorionic membrane in pregnancy It is a frequent cause of first and second trimester bleedingEpidemiologyIt typically occurs within the first 20 weeks of gestation If seen in the first 10-14 days of gestation they are also sometimes termed implantation bleedsRadiographic featuresUltrasound crescentic collection with elevation of the chorionic membranedepending on the time elapsed since bleeding the collection will have variable echotexture
acute hyperechoic and may be difficult to differentiate from adjacent chorionsubacute-chronic decreasing echogenicity with time
in almost all cases there is extension of the hematoma towards the margin of the placenta
First trimester SCH (subchorionic bleed)
First trimester SCH (subchorionic bleed)
Extensive hematoma in a woman with chronic bleeding
Subchorionic hemorrhage
Conjoined twins are a rare and complex complication of
monozygotic twinning which is associated with high perinatal mortality Early prenatal diagnosis of conjoined twins allows better counselling of the parents regarding the management options including continuation of pregnancy with post-natal surgery termination of pregnancy or selective fetocide in case of a triplet pregnancy With the introduction of high-resolution and transvaginal ultrasound imaging accurate prenatal diagnosis of conjoined twins is possible early in pregnancy Although first-trimester diagnosis of conjoined twins is feasible false-positive cases are common before 10 weeks because earlier in gestation fetal movements are limited and monoamniotic twins may appear conjoined As most parents opt for immediate termination of pregnancy at confirmation of the diagnosis there are limited data on the prenatal follow-up of conjoined twins detailed analysis of case reports where 3D imaging was used indicates that this modality does not improve on the diagnosis made by 2D ultrasound Overall very early prenatal diagnosis and first-trimester 3D imaging provide very little additional practical medical information compared to the 11-14 weeks ultrasound examination
Images of the conjoined twins there are two heads with conjoined body
Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You
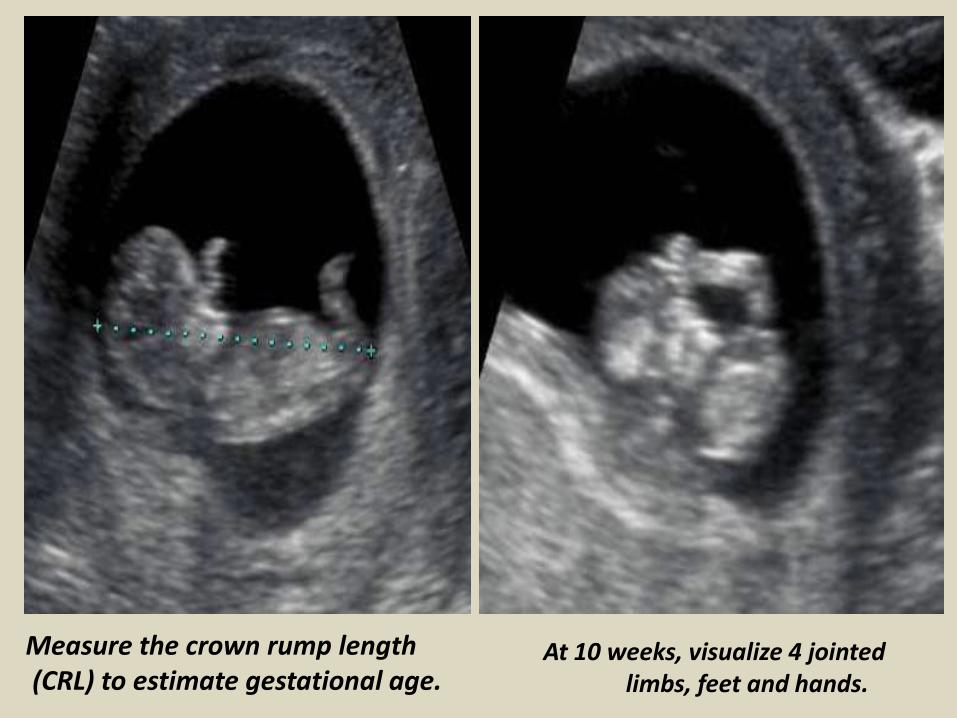
Measure the crown rump length(CRL) to estimate gestational age
At 10 weeks visualize 4 jointed limbs feet and hands
NUCHAL TRANSLUCENCY
From 12 weeks the basic morphology of the fetus is visible
The Nuchal Translucency is used to provide a risk assessment for chromosomal abnormalities specifically Trisomies 1318 and 21 (Downs Syndrome)
The legs are usually crossed at the ankles Confirm the presence and symmetry of the long bones
The correct angle the feet to legs can be confirmed They should be at 90 degrees ie perpendicular or Talipes should be suspected
The humerus radius and ulna and the presence of hands areimaged from 11 weeks
12 week choroids take up most of the space within the ventricles
TWINS Initially twins may be identified as 2 separate gestational sacs (ie diamniotic dichorionic) They may be 2 fetal poles within the same gestational sac (monochorionic) It is easier to determine chorionicity earlier in the pregnancy depending on the chorionicity and amnionicityIt is a sad situation when a vanishing twin occurs which is about 20 of twin pregnancies In these cases one of the twins fails to grow and thrive Instead its development arrests and it is reabsorbed with no evidence at delivery of the twin pregnancy
Monoamniotic Twins Dichorionic diamniotic Twins
TRIPLETS
Triplets with 2 sacs Monoamniotic monochorionic twins and a normal single
GRAPHS TO DETERMINE GESTATIONAL AGEDepending on the age of the gestation these graphs can be used to determine the correct EDD
Mean Sac Diameter measurement is used to determine gestational age before a Crown Rump length can be clearly measured The average sac diameter is determined by measuring the length width and height then dividing by 3
Once a fetal Pole can be visualized the CRL measurement is the most accurate method for dating the pregnancy
COMMON PATHOLOGYThickened Nuchal Translucency(NL)Partial Ovular DetachmentRetained products of conceptionAnembryonic GestationGestational trophoblastic diseaseMiscarriageEctopic PregnancySubchorionic hemorrhageConjoined TwinsAntepartum HemorrhageCheck heart beatCheck causes of bleeding
Thickened Nuchal Translucency (NT)
bull One of the parameters used in sequential screening (SS) for Downrsquos syndrome in first trimester
ndash SS Pregnancy associated plasma protein levels hCG levels NT thickness
bull Measured during 11-14 wks gestational age
bull Seen on sagittal image as increased subcutaneous non-septated fluid in posterior fetal neck
bull Measurement gt3mm usually considered abnormal however exact cut off measurements are dependent on maternal agegestational age
bull Detection rate of screening for Downrsquos Syndrome in first trimester
ndash sequential screening with NT 82-87
ndash NT alone 64-70
Thickened Nuchal Translucency (NT)
Thickened Nuchal Translucency
PARTIAL OVULAR DETACHMENTThe maternal circulation inside the placenta starts peripherally (in the placental margins) and is associated to physiological oxidative phenomena that may lead to membranes rupture and formation The abnormal development of such membranes may result in subchorionic hemorrhage enhancing the predisposition to an adverse gestational outcome at the third trimester (PPROM and PTL)Such abnormality is common and also denominated as subchorionic hemorrhage or trophoblastic hematoma being visualized in more than 18 of cases of threatened miscarriage The presence of fetal heart activity confers an excellent prognosis Clinically subchorionic hemorrhage may course with vaginal bleeding At ultrasonography a crescent-shaped shadow is observed adjacent to the gestational sac with debris Gestational sac compression and consequential deformation may occur In most of cases a two-week follow-up evaluation confirms the hematoma resorption
Retained products of conception are characterized by a
thickened disorganized and heterogeneous endometrium with ill-defined mucosal layers and cavitary line either with or without the presence of gestational sac Clinically the women presents abdominal pain and relative vaginal bleeding(14) In the presence of an intact gestational sac and closed cervix the difficulty in a spontaneous resolution will be higher requiring surgical evacuation
Retained products of conception
Transvaginal sonography without (A) and with (B) color Doppler imaging in a case of RPC with endometrial expansion (arrows)
Images retained products conception
EARLY EMBRYO DEATHSome sonographic findings characterize an embryo death in the first half of the first trimester in early phases before the crown-rump length can be measured The following aspects are highlighted small hyperechoic yolk sac or hydropic yolk sac increased in volume with diameter gt 7 mm or even small amniotic cavity disproportionate to the gestational sac size Before the 9th week small gestational sac may be associated with aneuploidy
Failed early pregnancy
ANEMBRYONIC GESTATIONAt transvaginal ultrasonography the yolk sac should be visualized in a gestational sac with mean diameter gt 10 mm The absence of a yolk sac within the gestational sac with gt 10 mm in mean diameter or the absence of a yolk sac within the gestational sac with gt 16 mm in diameter characterize anembryonic gestation
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
GESTATIONAL TROPHOBLASTIC DISEASEThe typical sonographic finding in most of cases of complete hydatidiform mole is a echogenic intracavitary solid mass with intermingled small cystic loci resembling a snow storm corresponding to the vesicles that macroscopically characterize this condition The higher the gestational age the larger the vesicles visualized as homogeneous anechoic images increasing the method specificity The ultrasonography sensitivity will depend on the gestational age at the moment of the diagnosis Ultrasonography can detect vesicles with gt 2 mm in diameter In early pregnancies with trophoblastic disease the sonographic method accuracy is limited hindering the differentiation of gestational trophoblastic disease from other conditions involving the endometrial cavity
Partial hydatidiform mole offers higher diagnostic difficulty by ultrasonography In a reasonable number of cases this disease presents as an empty gestational sac corresponding to anembryonic gestation or as early embryo death However two criteria have been described in the literature gestational sac transverseanteroposterior diameter ratio gt 15 and cystic changes irregularity of increase in echogenicity of decidualplacenta or myometrial reaction
ECTOPIC PREGNANCYSonographic findings of ectopic pregnancy will vary as a function of the gestational age and site Classically the following sonographic findings are described tubal ring sign adnexal disorganized mass molded to the adnexa andor cul de sac solid organized mass with regular margins mimicking a pediculated myomatous nodule clinically progressing with low β-hCGlevels and presence of a live extrauterine conceptus Uncommon gestational sites may be observed such as abdominal ectopic pregnancy cervical ectopic pregnancy and ectopic pregnancy in a previous Cesarean section pregnancy
Subchorionic hemorrhage (SCH) occurs when there is
perigestational haemorrhage and blood collects between the uterine wall and the chorionic membrane in pregnancy It is a frequent cause of first and second trimester bleedingEpidemiologyIt typically occurs within the first 20 weeks of gestation If seen in the first 10-14 days of gestation they are also sometimes termed implantation bleedsRadiographic featuresUltrasound crescentic collection with elevation of the chorionic membranedepending on the time elapsed since bleeding the collection will have variable echotexture
acute hyperechoic and may be difficult to differentiate from adjacent chorionsubacute-chronic decreasing echogenicity with time
in almost all cases there is extension of the hematoma towards the margin of the placenta
First trimester SCH (subchorionic bleed)
First trimester SCH (subchorionic bleed)
Extensive hematoma in a woman with chronic bleeding
Subchorionic hemorrhage
Conjoined twins are a rare and complex complication of
monozygotic twinning which is associated with high perinatal mortality Early prenatal diagnosis of conjoined twins allows better counselling of the parents regarding the management options including continuation of pregnancy with post-natal surgery termination of pregnancy or selective fetocide in case of a triplet pregnancy With the introduction of high-resolution and transvaginal ultrasound imaging accurate prenatal diagnosis of conjoined twins is possible early in pregnancy Although first-trimester diagnosis of conjoined twins is feasible false-positive cases are common before 10 weeks because earlier in gestation fetal movements are limited and monoamniotic twins may appear conjoined As most parents opt for immediate termination of pregnancy at confirmation of the diagnosis there are limited data on the prenatal follow-up of conjoined twins detailed analysis of case reports where 3D imaging was used indicates that this modality does not improve on the diagnosis made by 2D ultrasound Overall very early prenatal diagnosis and first-trimester 3D imaging provide very little additional practical medical information compared to the 11-14 weeks ultrasound examination
Images of the conjoined twins there are two heads with conjoined body
Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You

NUCHAL TRANSLUCENCY
From 12 weeks the basic morphology of the fetus is visible
The Nuchal Translucency is used to provide a risk assessment for chromosomal abnormalities specifically Trisomies 1318 and 21 (Downs Syndrome)
The legs are usually crossed at the ankles Confirm the presence and symmetry of the long bones
The correct angle the feet to legs can be confirmed They should be at 90 degrees ie perpendicular or Talipes should be suspected
The humerus radius and ulna and the presence of hands areimaged from 11 weeks
12 week choroids take up most of the space within the ventricles
TWINS Initially twins may be identified as 2 separate gestational sacs (ie diamniotic dichorionic) They may be 2 fetal poles within the same gestational sac (monochorionic) It is easier to determine chorionicity earlier in the pregnancy depending on the chorionicity and amnionicityIt is a sad situation when a vanishing twin occurs which is about 20 of twin pregnancies In these cases one of the twins fails to grow and thrive Instead its development arrests and it is reabsorbed with no evidence at delivery of the twin pregnancy
Monoamniotic Twins Dichorionic diamniotic Twins
TRIPLETS
Triplets with 2 sacs Monoamniotic monochorionic twins and a normal single
GRAPHS TO DETERMINE GESTATIONAL AGEDepending on the age of the gestation these graphs can be used to determine the correct EDD
Mean Sac Diameter measurement is used to determine gestational age before a Crown Rump length can be clearly measured The average sac diameter is determined by measuring the length width and height then dividing by 3
Once a fetal Pole can be visualized the CRL measurement is the most accurate method for dating the pregnancy
COMMON PATHOLOGYThickened Nuchal Translucency(NL)Partial Ovular DetachmentRetained products of conceptionAnembryonic GestationGestational trophoblastic diseaseMiscarriageEctopic PregnancySubchorionic hemorrhageConjoined TwinsAntepartum HemorrhageCheck heart beatCheck causes of bleeding
Thickened Nuchal Translucency (NT)
bull One of the parameters used in sequential screening (SS) for Downrsquos syndrome in first trimester
ndash SS Pregnancy associated plasma protein levels hCG levels NT thickness
bull Measured during 11-14 wks gestational age
bull Seen on sagittal image as increased subcutaneous non-septated fluid in posterior fetal neck
bull Measurement gt3mm usually considered abnormal however exact cut off measurements are dependent on maternal agegestational age
bull Detection rate of screening for Downrsquos Syndrome in first trimester
ndash sequential screening with NT 82-87
ndash NT alone 64-70
Thickened Nuchal Translucency (NT)
Thickened Nuchal Translucency
PARTIAL OVULAR DETACHMENTThe maternal circulation inside the placenta starts peripherally (in the placental margins) and is associated to physiological oxidative phenomena that may lead to membranes rupture and formation The abnormal development of such membranes may result in subchorionic hemorrhage enhancing the predisposition to an adverse gestational outcome at the third trimester (PPROM and PTL)Such abnormality is common and also denominated as subchorionic hemorrhage or trophoblastic hematoma being visualized in more than 18 of cases of threatened miscarriage The presence of fetal heart activity confers an excellent prognosis Clinically subchorionic hemorrhage may course with vaginal bleeding At ultrasonography a crescent-shaped shadow is observed adjacent to the gestational sac with debris Gestational sac compression and consequential deformation may occur In most of cases a two-week follow-up evaluation confirms the hematoma resorption
Retained products of conception are characterized by a
thickened disorganized and heterogeneous endometrium with ill-defined mucosal layers and cavitary line either with or without the presence of gestational sac Clinically the women presents abdominal pain and relative vaginal bleeding(14) In the presence of an intact gestational sac and closed cervix the difficulty in a spontaneous resolution will be higher requiring surgical evacuation
Retained products of conception
Transvaginal sonography without (A) and with (B) color Doppler imaging in a case of RPC with endometrial expansion (arrows)
Images retained products conception
EARLY EMBRYO DEATHSome sonographic findings characterize an embryo death in the first half of the first trimester in early phases before the crown-rump length can be measured The following aspects are highlighted small hyperechoic yolk sac or hydropic yolk sac increased in volume with diameter gt 7 mm or even small amniotic cavity disproportionate to the gestational sac size Before the 9th week small gestational sac may be associated with aneuploidy
Failed early pregnancy
ANEMBRYONIC GESTATIONAt transvaginal ultrasonography the yolk sac should be visualized in a gestational sac with mean diameter gt 10 mm The absence of a yolk sac within the gestational sac with gt 10 mm in mean diameter or the absence of a yolk sac within the gestational sac with gt 16 mm in diameter characterize anembryonic gestation
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
GESTATIONAL TROPHOBLASTIC DISEASEThe typical sonographic finding in most of cases of complete hydatidiform mole is a echogenic intracavitary solid mass with intermingled small cystic loci resembling a snow storm corresponding to the vesicles that macroscopically characterize this condition The higher the gestational age the larger the vesicles visualized as homogeneous anechoic images increasing the method specificity The ultrasonography sensitivity will depend on the gestational age at the moment of the diagnosis Ultrasonography can detect vesicles with gt 2 mm in diameter In early pregnancies with trophoblastic disease the sonographic method accuracy is limited hindering the differentiation of gestational trophoblastic disease from other conditions involving the endometrial cavity
Partial hydatidiform mole offers higher diagnostic difficulty by ultrasonography In a reasonable number of cases this disease presents as an empty gestational sac corresponding to anembryonic gestation or as early embryo death However two criteria have been described in the literature gestational sac transverseanteroposterior diameter ratio gt 15 and cystic changes irregularity of increase in echogenicity of decidualplacenta or myometrial reaction
ECTOPIC PREGNANCYSonographic findings of ectopic pregnancy will vary as a function of the gestational age and site Classically the following sonographic findings are described tubal ring sign adnexal disorganized mass molded to the adnexa andor cul de sac solid organized mass with regular margins mimicking a pediculated myomatous nodule clinically progressing with low β-hCGlevels and presence of a live extrauterine conceptus Uncommon gestational sites may be observed such as abdominal ectopic pregnancy cervical ectopic pregnancy and ectopic pregnancy in a previous Cesarean section pregnancy
Subchorionic hemorrhage (SCH) occurs when there is
perigestational haemorrhage and blood collects between the uterine wall and the chorionic membrane in pregnancy It is a frequent cause of first and second trimester bleedingEpidemiologyIt typically occurs within the first 20 weeks of gestation If seen in the first 10-14 days of gestation they are also sometimes termed implantation bleedsRadiographic featuresUltrasound crescentic collection with elevation of the chorionic membranedepending on the time elapsed since bleeding the collection will have variable echotexture
acute hyperechoic and may be difficult to differentiate from adjacent chorionsubacute-chronic decreasing echogenicity with time
in almost all cases there is extension of the hematoma towards the margin of the placenta
First trimester SCH (subchorionic bleed)
First trimester SCH (subchorionic bleed)
Extensive hematoma in a woman with chronic bleeding
Subchorionic hemorrhage
Conjoined twins are a rare and complex complication of
monozygotic twinning which is associated with high perinatal mortality Early prenatal diagnosis of conjoined twins allows better counselling of the parents regarding the management options including continuation of pregnancy with post-natal surgery termination of pregnancy or selective fetocide in case of a triplet pregnancy With the introduction of high-resolution and transvaginal ultrasound imaging accurate prenatal diagnosis of conjoined twins is possible early in pregnancy Although first-trimester diagnosis of conjoined twins is feasible false-positive cases are common before 10 weeks because earlier in gestation fetal movements are limited and monoamniotic twins may appear conjoined As most parents opt for immediate termination of pregnancy at confirmation of the diagnosis there are limited data on the prenatal follow-up of conjoined twins detailed analysis of case reports where 3D imaging was used indicates that this modality does not improve on the diagnosis made by 2D ultrasound Overall very early prenatal diagnosis and first-trimester 3D imaging provide very little additional practical medical information compared to the 11-14 weeks ultrasound examination
Images of the conjoined twins there are two heads with conjoined body
Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You
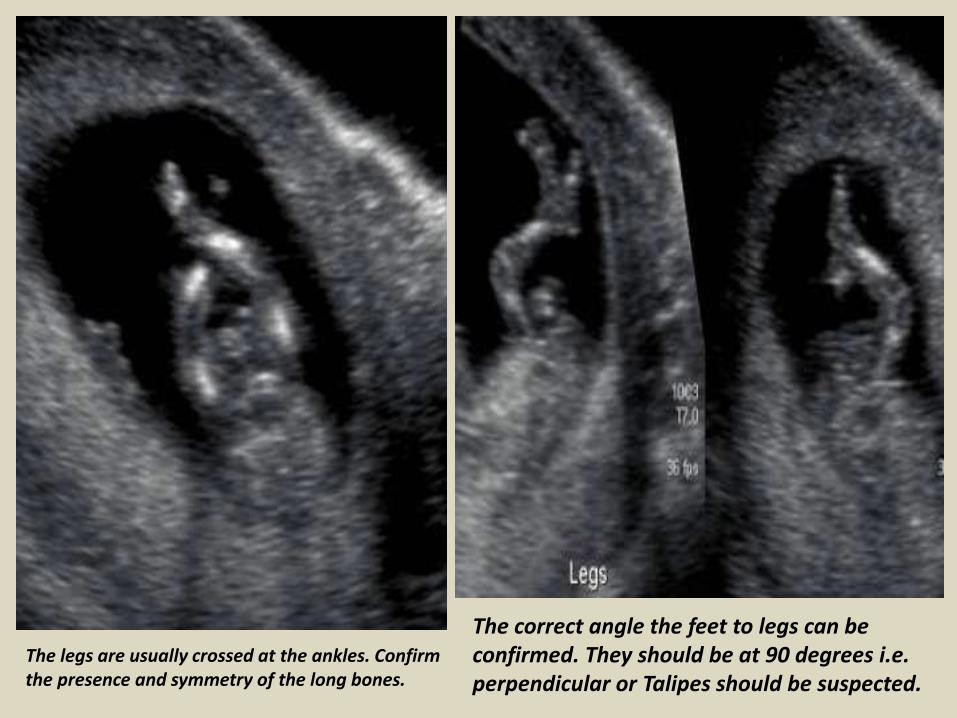
The legs are usually crossed at the ankles Confirm the presence and symmetry of the long bones
The correct angle the feet to legs can be confirmed They should be at 90 degrees ie perpendicular or Talipes should be suspected
The humerus radius and ulna and the presence of hands areimaged from 11 weeks
12 week choroids take up most of the space within the ventricles
TWINS Initially twins may be identified as 2 separate gestational sacs (ie diamniotic dichorionic) They may be 2 fetal poles within the same gestational sac (monochorionic) It is easier to determine chorionicity earlier in the pregnancy depending on the chorionicity and amnionicityIt is a sad situation when a vanishing twin occurs which is about 20 of twin pregnancies In these cases one of the twins fails to grow and thrive Instead its development arrests and it is reabsorbed with no evidence at delivery of the twin pregnancy
Monoamniotic Twins Dichorionic diamniotic Twins
TRIPLETS
Triplets with 2 sacs Monoamniotic monochorionic twins and a normal single
GRAPHS TO DETERMINE GESTATIONAL AGEDepending on the age of the gestation these graphs can be used to determine the correct EDD
Mean Sac Diameter measurement is used to determine gestational age before a Crown Rump length can be clearly measured The average sac diameter is determined by measuring the length width and height then dividing by 3
Once a fetal Pole can be visualized the CRL measurement is the most accurate method for dating the pregnancy
COMMON PATHOLOGYThickened Nuchal Translucency(NL)Partial Ovular DetachmentRetained products of conceptionAnembryonic GestationGestational trophoblastic diseaseMiscarriageEctopic PregnancySubchorionic hemorrhageConjoined TwinsAntepartum HemorrhageCheck heart beatCheck causes of bleeding
Thickened Nuchal Translucency (NT)
bull One of the parameters used in sequential screening (SS) for Downrsquos syndrome in first trimester
ndash SS Pregnancy associated plasma protein levels hCG levels NT thickness
bull Measured during 11-14 wks gestational age
bull Seen on sagittal image as increased subcutaneous non-septated fluid in posterior fetal neck
bull Measurement gt3mm usually considered abnormal however exact cut off measurements are dependent on maternal agegestational age
bull Detection rate of screening for Downrsquos Syndrome in first trimester
ndash sequential screening with NT 82-87
ndash NT alone 64-70
Thickened Nuchal Translucency (NT)
Thickened Nuchal Translucency
PARTIAL OVULAR DETACHMENTThe maternal circulation inside the placenta starts peripherally (in the placental margins) and is associated to physiological oxidative phenomena that may lead to membranes rupture and formation The abnormal development of such membranes may result in subchorionic hemorrhage enhancing the predisposition to an adverse gestational outcome at the third trimester (PPROM and PTL)Such abnormality is common and also denominated as subchorionic hemorrhage or trophoblastic hematoma being visualized in more than 18 of cases of threatened miscarriage The presence of fetal heart activity confers an excellent prognosis Clinically subchorionic hemorrhage may course with vaginal bleeding At ultrasonography a crescent-shaped shadow is observed adjacent to the gestational sac with debris Gestational sac compression and consequential deformation may occur In most of cases a two-week follow-up evaluation confirms the hematoma resorption
Retained products of conception are characterized by a
thickened disorganized and heterogeneous endometrium with ill-defined mucosal layers and cavitary line either with or without the presence of gestational sac Clinically the women presents abdominal pain and relative vaginal bleeding(14) In the presence of an intact gestational sac and closed cervix the difficulty in a spontaneous resolution will be higher requiring surgical evacuation
Retained products of conception
Transvaginal sonography without (A) and with (B) color Doppler imaging in a case of RPC with endometrial expansion (arrows)
Images retained products conception
EARLY EMBRYO DEATHSome sonographic findings characterize an embryo death in the first half of the first trimester in early phases before the crown-rump length can be measured The following aspects are highlighted small hyperechoic yolk sac or hydropic yolk sac increased in volume with diameter gt 7 mm or even small amniotic cavity disproportionate to the gestational sac size Before the 9th week small gestational sac may be associated with aneuploidy
Failed early pregnancy
ANEMBRYONIC GESTATIONAt transvaginal ultrasonography the yolk sac should be visualized in a gestational sac with mean diameter gt 10 mm The absence of a yolk sac within the gestational sac with gt 10 mm in mean diameter or the absence of a yolk sac within the gestational sac with gt 16 mm in diameter characterize anembryonic gestation
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
GESTATIONAL TROPHOBLASTIC DISEASEThe typical sonographic finding in most of cases of complete hydatidiform mole is a echogenic intracavitary solid mass with intermingled small cystic loci resembling a snow storm corresponding to the vesicles that macroscopically characterize this condition The higher the gestational age the larger the vesicles visualized as homogeneous anechoic images increasing the method specificity The ultrasonography sensitivity will depend on the gestational age at the moment of the diagnosis Ultrasonography can detect vesicles with gt 2 mm in diameter In early pregnancies with trophoblastic disease the sonographic method accuracy is limited hindering the differentiation of gestational trophoblastic disease from other conditions involving the endometrial cavity
Partial hydatidiform mole offers higher diagnostic difficulty by ultrasonography In a reasonable number of cases this disease presents as an empty gestational sac corresponding to anembryonic gestation or as early embryo death However two criteria have been described in the literature gestational sac transverseanteroposterior diameter ratio gt 15 and cystic changes irregularity of increase in echogenicity of decidualplacenta or myometrial reaction
ECTOPIC PREGNANCYSonographic findings of ectopic pregnancy will vary as a function of the gestational age and site Classically the following sonographic findings are described tubal ring sign adnexal disorganized mass molded to the adnexa andor cul de sac solid organized mass with regular margins mimicking a pediculated myomatous nodule clinically progressing with low β-hCGlevels and presence of a live extrauterine conceptus Uncommon gestational sites may be observed such as abdominal ectopic pregnancy cervical ectopic pregnancy and ectopic pregnancy in a previous Cesarean section pregnancy
Subchorionic hemorrhage (SCH) occurs when there is
perigestational haemorrhage and blood collects between the uterine wall and the chorionic membrane in pregnancy It is a frequent cause of first and second trimester bleedingEpidemiologyIt typically occurs within the first 20 weeks of gestation If seen in the first 10-14 days of gestation they are also sometimes termed implantation bleedsRadiographic featuresUltrasound crescentic collection with elevation of the chorionic membranedepending on the time elapsed since bleeding the collection will have variable echotexture
acute hyperechoic and may be difficult to differentiate from adjacent chorionsubacute-chronic decreasing echogenicity with time
in almost all cases there is extension of the hematoma towards the margin of the placenta
First trimester SCH (subchorionic bleed)
First trimester SCH (subchorionic bleed)
Extensive hematoma in a woman with chronic bleeding
Subchorionic hemorrhage
Conjoined twins are a rare and complex complication of
monozygotic twinning which is associated with high perinatal mortality Early prenatal diagnosis of conjoined twins allows better counselling of the parents regarding the management options including continuation of pregnancy with post-natal surgery termination of pregnancy or selective fetocide in case of a triplet pregnancy With the introduction of high-resolution and transvaginal ultrasound imaging accurate prenatal diagnosis of conjoined twins is possible early in pregnancy Although first-trimester diagnosis of conjoined twins is feasible false-positive cases are common before 10 weeks because earlier in gestation fetal movements are limited and monoamniotic twins may appear conjoined As most parents opt for immediate termination of pregnancy at confirmation of the diagnosis there are limited data on the prenatal follow-up of conjoined twins detailed analysis of case reports where 3D imaging was used indicates that this modality does not improve on the diagnosis made by 2D ultrasound Overall very early prenatal diagnosis and first-trimester 3D imaging provide very little additional practical medical information compared to the 11-14 weeks ultrasound examination
Images of the conjoined twins there are two heads with conjoined body
Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You

The humerus radius and ulna and the presence of hands areimaged from 11 weeks
12 week choroids take up most of the space within the ventricles
TWINS Initially twins may be identified as 2 separate gestational sacs (ie diamniotic dichorionic) They may be 2 fetal poles within the same gestational sac (monochorionic) It is easier to determine chorionicity earlier in the pregnancy depending on the chorionicity and amnionicityIt is a sad situation when a vanishing twin occurs which is about 20 of twin pregnancies In these cases one of the twins fails to grow and thrive Instead its development arrests and it is reabsorbed with no evidence at delivery of the twin pregnancy
Monoamniotic Twins Dichorionic diamniotic Twins
TRIPLETS
Triplets with 2 sacs Monoamniotic monochorionic twins and a normal single
GRAPHS TO DETERMINE GESTATIONAL AGEDepending on the age of the gestation these graphs can be used to determine the correct EDD
Mean Sac Diameter measurement is used to determine gestational age before a Crown Rump length can be clearly measured The average sac diameter is determined by measuring the length width and height then dividing by 3
Once a fetal Pole can be visualized the CRL measurement is the most accurate method for dating the pregnancy
COMMON PATHOLOGYThickened Nuchal Translucency(NL)Partial Ovular DetachmentRetained products of conceptionAnembryonic GestationGestational trophoblastic diseaseMiscarriageEctopic PregnancySubchorionic hemorrhageConjoined TwinsAntepartum HemorrhageCheck heart beatCheck causes of bleeding
Thickened Nuchal Translucency (NT)
bull One of the parameters used in sequential screening (SS) for Downrsquos syndrome in first trimester
ndash SS Pregnancy associated plasma protein levels hCG levels NT thickness
bull Measured during 11-14 wks gestational age
bull Seen on sagittal image as increased subcutaneous non-septated fluid in posterior fetal neck
bull Measurement gt3mm usually considered abnormal however exact cut off measurements are dependent on maternal agegestational age
bull Detection rate of screening for Downrsquos Syndrome in first trimester
ndash sequential screening with NT 82-87
ndash NT alone 64-70
Thickened Nuchal Translucency (NT)
Thickened Nuchal Translucency
PARTIAL OVULAR DETACHMENTThe maternal circulation inside the placenta starts peripherally (in the placental margins) and is associated to physiological oxidative phenomena that may lead to membranes rupture and formation The abnormal development of such membranes may result in subchorionic hemorrhage enhancing the predisposition to an adverse gestational outcome at the third trimester (PPROM and PTL)Such abnormality is common and also denominated as subchorionic hemorrhage or trophoblastic hematoma being visualized in more than 18 of cases of threatened miscarriage The presence of fetal heart activity confers an excellent prognosis Clinically subchorionic hemorrhage may course with vaginal bleeding At ultrasonography a crescent-shaped shadow is observed adjacent to the gestational sac with debris Gestational sac compression and consequential deformation may occur In most of cases a two-week follow-up evaluation confirms the hematoma resorption
Retained products of conception are characterized by a
thickened disorganized and heterogeneous endometrium with ill-defined mucosal layers and cavitary line either with or without the presence of gestational sac Clinically the women presents abdominal pain and relative vaginal bleeding(14) In the presence of an intact gestational sac and closed cervix the difficulty in a spontaneous resolution will be higher requiring surgical evacuation
Retained products of conception
Transvaginal sonography without (A) and with (B) color Doppler imaging in a case of RPC with endometrial expansion (arrows)
Images retained products conception
EARLY EMBRYO DEATHSome sonographic findings characterize an embryo death in the first half of the first trimester in early phases before the crown-rump length can be measured The following aspects are highlighted small hyperechoic yolk sac or hydropic yolk sac increased in volume with diameter gt 7 mm or even small amniotic cavity disproportionate to the gestational sac size Before the 9th week small gestational sac may be associated with aneuploidy
Failed early pregnancy
ANEMBRYONIC GESTATIONAt transvaginal ultrasonography the yolk sac should be visualized in a gestational sac with mean diameter gt 10 mm The absence of a yolk sac within the gestational sac with gt 10 mm in mean diameter or the absence of a yolk sac within the gestational sac with gt 16 mm in diameter characterize anembryonic gestation
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
GESTATIONAL TROPHOBLASTIC DISEASEThe typical sonographic finding in most of cases of complete hydatidiform mole is a echogenic intracavitary solid mass with intermingled small cystic loci resembling a snow storm corresponding to the vesicles that macroscopically characterize this condition The higher the gestational age the larger the vesicles visualized as homogeneous anechoic images increasing the method specificity The ultrasonography sensitivity will depend on the gestational age at the moment of the diagnosis Ultrasonography can detect vesicles with gt 2 mm in diameter In early pregnancies with trophoblastic disease the sonographic method accuracy is limited hindering the differentiation of gestational trophoblastic disease from other conditions involving the endometrial cavity
Partial hydatidiform mole offers higher diagnostic difficulty by ultrasonography In a reasonable number of cases this disease presents as an empty gestational sac corresponding to anembryonic gestation or as early embryo death However two criteria have been described in the literature gestational sac transverseanteroposterior diameter ratio gt 15 and cystic changes irregularity of increase in echogenicity of decidualplacenta or myometrial reaction
ECTOPIC PREGNANCYSonographic findings of ectopic pregnancy will vary as a function of the gestational age and site Classically the following sonographic findings are described tubal ring sign adnexal disorganized mass molded to the adnexa andor cul de sac solid organized mass with regular margins mimicking a pediculated myomatous nodule clinically progressing with low β-hCGlevels and presence of a live extrauterine conceptus Uncommon gestational sites may be observed such as abdominal ectopic pregnancy cervical ectopic pregnancy and ectopic pregnancy in a previous Cesarean section pregnancy
Subchorionic hemorrhage (SCH) occurs when there is
perigestational haemorrhage and blood collects between the uterine wall and the chorionic membrane in pregnancy It is a frequent cause of first and second trimester bleedingEpidemiologyIt typically occurs within the first 20 weeks of gestation If seen in the first 10-14 days of gestation they are also sometimes termed implantation bleedsRadiographic featuresUltrasound crescentic collection with elevation of the chorionic membranedepending on the time elapsed since bleeding the collection will have variable echotexture
acute hyperechoic and may be difficult to differentiate from adjacent chorionsubacute-chronic decreasing echogenicity with time
in almost all cases there is extension of the hematoma towards the margin of the placenta
First trimester SCH (subchorionic bleed)
First trimester SCH (subchorionic bleed)
Extensive hematoma in a woman with chronic bleeding
Subchorionic hemorrhage
Conjoined twins are a rare and complex complication of
monozygotic twinning which is associated with high perinatal mortality Early prenatal diagnosis of conjoined twins allows better counselling of the parents regarding the management options including continuation of pregnancy with post-natal surgery termination of pregnancy or selective fetocide in case of a triplet pregnancy With the introduction of high-resolution and transvaginal ultrasound imaging accurate prenatal diagnosis of conjoined twins is possible early in pregnancy Although first-trimester diagnosis of conjoined twins is feasible false-positive cases are common before 10 weeks because earlier in gestation fetal movements are limited and monoamniotic twins may appear conjoined As most parents opt for immediate termination of pregnancy at confirmation of the diagnosis there are limited data on the prenatal follow-up of conjoined twins detailed analysis of case reports where 3D imaging was used indicates that this modality does not improve on the diagnosis made by 2D ultrasound Overall very early prenatal diagnosis and first-trimester 3D imaging provide very little additional practical medical information compared to the 11-14 weeks ultrasound examination
Images of the conjoined twins there are two heads with conjoined body
Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You

TWINS Initially twins may be identified as 2 separate gestational sacs (ie diamniotic dichorionic) They may be 2 fetal poles within the same gestational sac (monochorionic) It is easier to determine chorionicity earlier in the pregnancy depending on the chorionicity and amnionicityIt is a sad situation when a vanishing twin occurs which is about 20 of twin pregnancies In these cases one of the twins fails to grow and thrive Instead its development arrests and it is reabsorbed with no evidence at delivery of the twin pregnancy
Monoamniotic Twins Dichorionic diamniotic Twins
TRIPLETS
Triplets with 2 sacs Monoamniotic monochorionic twins and a normal single
GRAPHS TO DETERMINE GESTATIONAL AGEDepending on the age of the gestation these graphs can be used to determine the correct EDD
Mean Sac Diameter measurement is used to determine gestational age before a Crown Rump length can be clearly measured The average sac diameter is determined by measuring the length width and height then dividing by 3
Once a fetal Pole can be visualized the CRL measurement is the most accurate method for dating the pregnancy
COMMON PATHOLOGYThickened Nuchal Translucency(NL)Partial Ovular DetachmentRetained products of conceptionAnembryonic GestationGestational trophoblastic diseaseMiscarriageEctopic PregnancySubchorionic hemorrhageConjoined TwinsAntepartum HemorrhageCheck heart beatCheck causes of bleeding
Thickened Nuchal Translucency (NT)
bull One of the parameters used in sequential screening (SS) for Downrsquos syndrome in first trimester
ndash SS Pregnancy associated plasma protein levels hCG levels NT thickness
bull Measured during 11-14 wks gestational age
bull Seen on sagittal image as increased subcutaneous non-septated fluid in posterior fetal neck
bull Measurement gt3mm usually considered abnormal however exact cut off measurements are dependent on maternal agegestational age
bull Detection rate of screening for Downrsquos Syndrome in first trimester
ndash sequential screening with NT 82-87
ndash NT alone 64-70
Thickened Nuchal Translucency (NT)
Thickened Nuchal Translucency
PARTIAL OVULAR DETACHMENTThe maternal circulation inside the placenta starts peripherally (in the placental margins) and is associated to physiological oxidative phenomena that may lead to membranes rupture and formation The abnormal development of such membranes may result in subchorionic hemorrhage enhancing the predisposition to an adverse gestational outcome at the third trimester (PPROM and PTL)Such abnormality is common and also denominated as subchorionic hemorrhage or trophoblastic hematoma being visualized in more than 18 of cases of threatened miscarriage The presence of fetal heart activity confers an excellent prognosis Clinically subchorionic hemorrhage may course with vaginal bleeding At ultrasonography a crescent-shaped shadow is observed adjacent to the gestational sac with debris Gestational sac compression and consequential deformation may occur In most of cases a two-week follow-up evaluation confirms the hematoma resorption
Retained products of conception are characterized by a
thickened disorganized and heterogeneous endometrium with ill-defined mucosal layers and cavitary line either with or without the presence of gestational sac Clinically the women presents abdominal pain and relative vaginal bleeding(14) In the presence of an intact gestational sac and closed cervix the difficulty in a spontaneous resolution will be higher requiring surgical evacuation
Retained products of conception
Transvaginal sonography without (A) and with (B) color Doppler imaging in a case of RPC with endometrial expansion (arrows)
Images retained products conception
EARLY EMBRYO DEATHSome sonographic findings characterize an embryo death in the first half of the first trimester in early phases before the crown-rump length can be measured The following aspects are highlighted small hyperechoic yolk sac or hydropic yolk sac increased in volume with diameter gt 7 mm or even small amniotic cavity disproportionate to the gestational sac size Before the 9th week small gestational sac may be associated with aneuploidy
Failed early pregnancy
ANEMBRYONIC GESTATIONAt transvaginal ultrasonography the yolk sac should be visualized in a gestational sac with mean diameter gt 10 mm The absence of a yolk sac within the gestational sac with gt 10 mm in mean diameter or the absence of a yolk sac within the gestational sac with gt 16 mm in diameter characterize anembryonic gestation
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
GESTATIONAL TROPHOBLASTIC DISEASEThe typical sonographic finding in most of cases of complete hydatidiform mole is a echogenic intracavitary solid mass with intermingled small cystic loci resembling a snow storm corresponding to the vesicles that macroscopically characterize this condition The higher the gestational age the larger the vesicles visualized as homogeneous anechoic images increasing the method specificity The ultrasonography sensitivity will depend on the gestational age at the moment of the diagnosis Ultrasonography can detect vesicles with gt 2 mm in diameter In early pregnancies with trophoblastic disease the sonographic method accuracy is limited hindering the differentiation of gestational trophoblastic disease from other conditions involving the endometrial cavity
Partial hydatidiform mole offers higher diagnostic difficulty by ultrasonography In a reasonable number of cases this disease presents as an empty gestational sac corresponding to anembryonic gestation or as early embryo death However two criteria have been described in the literature gestational sac transverseanteroposterior diameter ratio gt 15 and cystic changes irregularity of increase in echogenicity of decidualplacenta or myometrial reaction
ECTOPIC PREGNANCYSonographic findings of ectopic pregnancy will vary as a function of the gestational age and site Classically the following sonographic findings are described tubal ring sign adnexal disorganized mass molded to the adnexa andor cul de sac solid organized mass with regular margins mimicking a pediculated myomatous nodule clinically progressing with low β-hCGlevels and presence of a live extrauterine conceptus Uncommon gestational sites may be observed such as abdominal ectopic pregnancy cervical ectopic pregnancy and ectopic pregnancy in a previous Cesarean section pregnancy
Subchorionic hemorrhage (SCH) occurs when there is
perigestational haemorrhage and blood collects between the uterine wall and the chorionic membrane in pregnancy It is a frequent cause of first and second trimester bleedingEpidemiologyIt typically occurs within the first 20 weeks of gestation If seen in the first 10-14 days of gestation they are also sometimes termed implantation bleedsRadiographic featuresUltrasound crescentic collection with elevation of the chorionic membranedepending on the time elapsed since bleeding the collection will have variable echotexture
acute hyperechoic and may be difficult to differentiate from adjacent chorionsubacute-chronic decreasing echogenicity with time
in almost all cases there is extension of the hematoma towards the margin of the placenta
First trimester SCH (subchorionic bleed)
First trimester SCH (subchorionic bleed)
Extensive hematoma in a woman with chronic bleeding
Subchorionic hemorrhage
Conjoined twins are a rare and complex complication of
monozygotic twinning which is associated with high perinatal mortality Early prenatal diagnosis of conjoined twins allows better counselling of the parents regarding the management options including continuation of pregnancy with post-natal surgery termination of pregnancy or selective fetocide in case of a triplet pregnancy With the introduction of high-resolution and transvaginal ultrasound imaging accurate prenatal diagnosis of conjoined twins is possible early in pregnancy Although first-trimester diagnosis of conjoined twins is feasible false-positive cases are common before 10 weeks because earlier in gestation fetal movements are limited and monoamniotic twins may appear conjoined As most parents opt for immediate termination of pregnancy at confirmation of the diagnosis there are limited data on the prenatal follow-up of conjoined twins detailed analysis of case reports where 3D imaging was used indicates that this modality does not improve on the diagnosis made by 2D ultrasound Overall very early prenatal diagnosis and first-trimester 3D imaging provide very little additional practical medical information compared to the 11-14 weeks ultrasound examination
Images of the conjoined twins there are two heads with conjoined body
Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You
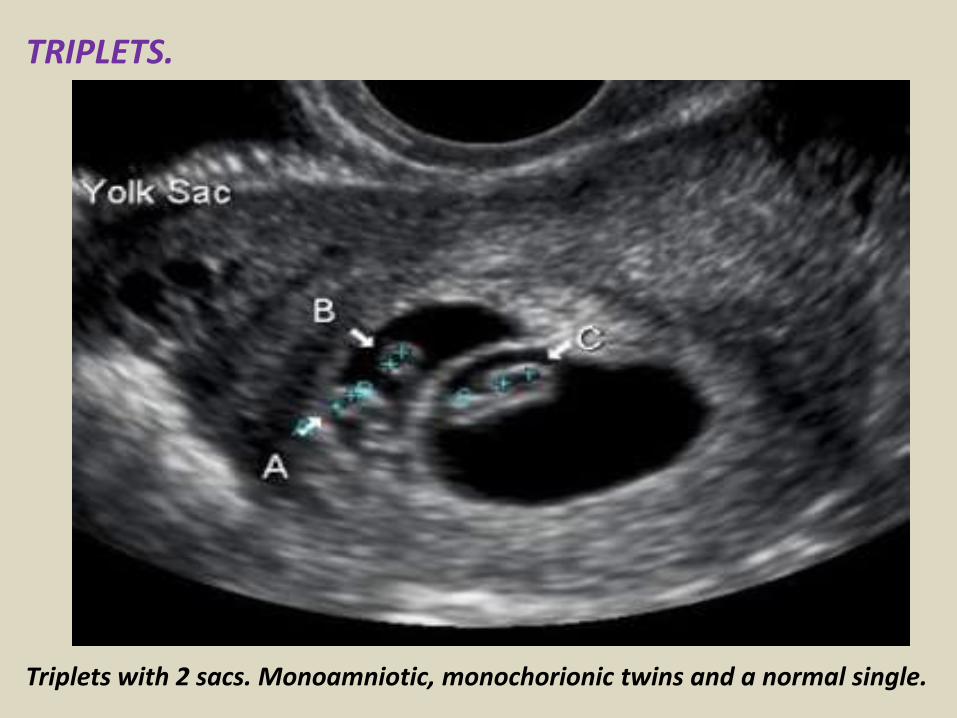
TRIPLETS
Triplets with 2 sacs Monoamniotic monochorionic twins and a normal single
GRAPHS TO DETERMINE GESTATIONAL AGEDepending on the age of the gestation these graphs can be used to determine the correct EDD
Mean Sac Diameter measurement is used to determine gestational age before a Crown Rump length can be clearly measured The average sac diameter is determined by measuring the length width and height then dividing by 3
Once a fetal Pole can be visualized the CRL measurement is the most accurate method for dating the pregnancy
COMMON PATHOLOGYThickened Nuchal Translucency(NL)Partial Ovular DetachmentRetained products of conceptionAnembryonic GestationGestational trophoblastic diseaseMiscarriageEctopic PregnancySubchorionic hemorrhageConjoined TwinsAntepartum HemorrhageCheck heart beatCheck causes of bleeding
Thickened Nuchal Translucency (NT)
bull One of the parameters used in sequential screening (SS) for Downrsquos syndrome in first trimester
ndash SS Pregnancy associated plasma protein levels hCG levels NT thickness
bull Measured during 11-14 wks gestational age
bull Seen on sagittal image as increased subcutaneous non-septated fluid in posterior fetal neck
bull Measurement gt3mm usually considered abnormal however exact cut off measurements are dependent on maternal agegestational age
bull Detection rate of screening for Downrsquos Syndrome in first trimester
ndash sequential screening with NT 82-87
ndash NT alone 64-70
Thickened Nuchal Translucency (NT)
Thickened Nuchal Translucency
PARTIAL OVULAR DETACHMENTThe maternal circulation inside the placenta starts peripherally (in the placental margins) and is associated to physiological oxidative phenomena that may lead to membranes rupture and formation The abnormal development of such membranes may result in subchorionic hemorrhage enhancing the predisposition to an adverse gestational outcome at the third trimester (PPROM and PTL)Such abnormality is common and also denominated as subchorionic hemorrhage or trophoblastic hematoma being visualized in more than 18 of cases of threatened miscarriage The presence of fetal heart activity confers an excellent prognosis Clinically subchorionic hemorrhage may course with vaginal bleeding At ultrasonography a crescent-shaped shadow is observed adjacent to the gestational sac with debris Gestational sac compression and consequential deformation may occur In most of cases a two-week follow-up evaluation confirms the hematoma resorption
Retained products of conception are characterized by a
thickened disorganized and heterogeneous endometrium with ill-defined mucosal layers and cavitary line either with or without the presence of gestational sac Clinically the women presents abdominal pain and relative vaginal bleeding(14) In the presence of an intact gestational sac and closed cervix the difficulty in a spontaneous resolution will be higher requiring surgical evacuation
Retained products of conception
Transvaginal sonography without (A) and with (B) color Doppler imaging in a case of RPC with endometrial expansion (arrows)
Images retained products conception
EARLY EMBRYO DEATHSome sonographic findings characterize an embryo death in the first half of the first trimester in early phases before the crown-rump length can be measured The following aspects are highlighted small hyperechoic yolk sac or hydropic yolk sac increased in volume with diameter gt 7 mm or even small amniotic cavity disproportionate to the gestational sac size Before the 9th week small gestational sac may be associated with aneuploidy
Failed early pregnancy
ANEMBRYONIC GESTATIONAt transvaginal ultrasonography the yolk sac should be visualized in a gestational sac with mean diameter gt 10 mm The absence of a yolk sac within the gestational sac with gt 10 mm in mean diameter or the absence of a yolk sac within the gestational sac with gt 16 mm in diameter characterize anembryonic gestation
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
GESTATIONAL TROPHOBLASTIC DISEASEThe typical sonographic finding in most of cases of complete hydatidiform mole is a echogenic intracavitary solid mass with intermingled small cystic loci resembling a snow storm corresponding to the vesicles that macroscopically characterize this condition The higher the gestational age the larger the vesicles visualized as homogeneous anechoic images increasing the method specificity The ultrasonography sensitivity will depend on the gestational age at the moment of the diagnosis Ultrasonography can detect vesicles with gt 2 mm in diameter In early pregnancies with trophoblastic disease the sonographic method accuracy is limited hindering the differentiation of gestational trophoblastic disease from other conditions involving the endometrial cavity
Partial hydatidiform mole offers higher diagnostic difficulty by ultrasonography In a reasonable number of cases this disease presents as an empty gestational sac corresponding to anembryonic gestation or as early embryo death However two criteria have been described in the literature gestational sac transverseanteroposterior diameter ratio gt 15 and cystic changes irregularity of increase in echogenicity of decidualplacenta or myometrial reaction
ECTOPIC PREGNANCYSonographic findings of ectopic pregnancy will vary as a function of the gestational age and site Classically the following sonographic findings are described tubal ring sign adnexal disorganized mass molded to the adnexa andor cul de sac solid organized mass with regular margins mimicking a pediculated myomatous nodule clinically progressing with low β-hCGlevels and presence of a live extrauterine conceptus Uncommon gestational sites may be observed such as abdominal ectopic pregnancy cervical ectopic pregnancy and ectopic pregnancy in a previous Cesarean section pregnancy
Subchorionic hemorrhage (SCH) occurs when there is
perigestational haemorrhage and blood collects between the uterine wall and the chorionic membrane in pregnancy It is a frequent cause of first and second trimester bleedingEpidemiologyIt typically occurs within the first 20 weeks of gestation If seen in the first 10-14 days of gestation they are also sometimes termed implantation bleedsRadiographic featuresUltrasound crescentic collection with elevation of the chorionic membranedepending on the time elapsed since bleeding the collection will have variable echotexture
acute hyperechoic and may be difficult to differentiate from adjacent chorionsubacute-chronic decreasing echogenicity with time
in almost all cases there is extension of the hematoma towards the margin of the placenta
First trimester SCH (subchorionic bleed)
First trimester SCH (subchorionic bleed)
Extensive hematoma in a woman with chronic bleeding
Subchorionic hemorrhage
Conjoined twins are a rare and complex complication of
monozygotic twinning which is associated with high perinatal mortality Early prenatal diagnosis of conjoined twins allows better counselling of the parents regarding the management options including continuation of pregnancy with post-natal surgery termination of pregnancy or selective fetocide in case of a triplet pregnancy With the introduction of high-resolution and transvaginal ultrasound imaging accurate prenatal diagnosis of conjoined twins is possible early in pregnancy Although first-trimester diagnosis of conjoined twins is feasible false-positive cases are common before 10 weeks because earlier in gestation fetal movements are limited and monoamniotic twins may appear conjoined As most parents opt for immediate termination of pregnancy at confirmation of the diagnosis there are limited data on the prenatal follow-up of conjoined twins detailed analysis of case reports where 3D imaging was used indicates that this modality does not improve on the diagnosis made by 2D ultrasound Overall very early prenatal diagnosis and first-trimester 3D imaging provide very little additional practical medical information compared to the 11-14 weeks ultrasound examination
Images of the conjoined twins there are two heads with conjoined body
Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You

GRAPHS TO DETERMINE GESTATIONAL AGEDepending on the age of the gestation these graphs can be used to determine the correct EDD
Mean Sac Diameter measurement is used to determine gestational age before a Crown Rump length can be clearly measured The average sac diameter is determined by measuring the length width and height then dividing by 3
Once a fetal Pole can be visualized the CRL measurement is the most accurate method for dating the pregnancy
COMMON PATHOLOGYThickened Nuchal Translucency(NL)Partial Ovular DetachmentRetained products of conceptionAnembryonic GestationGestational trophoblastic diseaseMiscarriageEctopic PregnancySubchorionic hemorrhageConjoined TwinsAntepartum HemorrhageCheck heart beatCheck causes of bleeding
Thickened Nuchal Translucency (NT)
bull One of the parameters used in sequential screening (SS) for Downrsquos syndrome in first trimester
ndash SS Pregnancy associated plasma protein levels hCG levels NT thickness
bull Measured during 11-14 wks gestational age
bull Seen on sagittal image as increased subcutaneous non-septated fluid in posterior fetal neck
bull Measurement gt3mm usually considered abnormal however exact cut off measurements are dependent on maternal agegestational age
bull Detection rate of screening for Downrsquos Syndrome in first trimester
ndash sequential screening with NT 82-87
ndash NT alone 64-70
Thickened Nuchal Translucency (NT)
Thickened Nuchal Translucency
PARTIAL OVULAR DETACHMENTThe maternal circulation inside the placenta starts peripherally (in the placental margins) and is associated to physiological oxidative phenomena that may lead to membranes rupture and formation The abnormal development of such membranes may result in subchorionic hemorrhage enhancing the predisposition to an adverse gestational outcome at the third trimester (PPROM and PTL)Such abnormality is common and also denominated as subchorionic hemorrhage or trophoblastic hematoma being visualized in more than 18 of cases of threatened miscarriage The presence of fetal heart activity confers an excellent prognosis Clinically subchorionic hemorrhage may course with vaginal bleeding At ultrasonography a crescent-shaped shadow is observed adjacent to the gestational sac with debris Gestational sac compression and consequential deformation may occur In most of cases a two-week follow-up evaluation confirms the hematoma resorption
Retained products of conception are characterized by a
thickened disorganized and heterogeneous endometrium with ill-defined mucosal layers and cavitary line either with or without the presence of gestational sac Clinically the women presents abdominal pain and relative vaginal bleeding(14) In the presence of an intact gestational sac and closed cervix the difficulty in a spontaneous resolution will be higher requiring surgical evacuation
Retained products of conception
Transvaginal sonography without (A) and with (B) color Doppler imaging in a case of RPC with endometrial expansion (arrows)
Images retained products conception
EARLY EMBRYO DEATHSome sonographic findings characterize an embryo death in the first half of the first trimester in early phases before the crown-rump length can be measured The following aspects are highlighted small hyperechoic yolk sac or hydropic yolk sac increased in volume with diameter gt 7 mm or even small amniotic cavity disproportionate to the gestational sac size Before the 9th week small gestational sac may be associated with aneuploidy
Failed early pregnancy
ANEMBRYONIC GESTATIONAt transvaginal ultrasonography the yolk sac should be visualized in a gestational sac with mean diameter gt 10 mm The absence of a yolk sac within the gestational sac with gt 10 mm in mean diameter or the absence of a yolk sac within the gestational sac with gt 16 mm in diameter characterize anembryonic gestation
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
GESTATIONAL TROPHOBLASTIC DISEASEThe typical sonographic finding in most of cases of complete hydatidiform mole is a echogenic intracavitary solid mass with intermingled small cystic loci resembling a snow storm corresponding to the vesicles that macroscopically characterize this condition The higher the gestational age the larger the vesicles visualized as homogeneous anechoic images increasing the method specificity The ultrasonography sensitivity will depend on the gestational age at the moment of the diagnosis Ultrasonography can detect vesicles with gt 2 mm in diameter In early pregnancies with trophoblastic disease the sonographic method accuracy is limited hindering the differentiation of gestational trophoblastic disease from other conditions involving the endometrial cavity
Partial hydatidiform mole offers higher diagnostic difficulty by ultrasonography In a reasonable number of cases this disease presents as an empty gestational sac corresponding to anembryonic gestation or as early embryo death However two criteria have been described in the literature gestational sac transverseanteroposterior diameter ratio gt 15 and cystic changes irregularity of increase in echogenicity of decidualplacenta or myometrial reaction
ECTOPIC PREGNANCYSonographic findings of ectopic pregnancy will vary as a function of the gestational age and site Classically the following sonographic findings are described tubal ring sign adnexal disorganized mass molded to the adnexa andor cul de sac solid organized mass with regular margins mimicking a pediculated myomatous nodule clinically progressing with low β-hCGlevels and presence of a live extrauterine conceptus Uncommon gestational sites may be observed such as abdominal ectopic pregnancy cervical ectopic pregnancy and ectopic pregnancy in a previous Cesarean section pregnancy
Subchorionic hemorrhage (SCH) occurs when there is
perigestational haemorrhage and blood collects between the uterine wall and the chorionic membrane in pregnancy It is a frequent cause of first and second trimester bleedingEpidemiologyIt typically occurs within the first 20 weeks of gestation If seen in the first 10-14 days of gestation they are also sometimes termed implantation bleedsRadiographic featuresUltrasound crescentic collection with elevation of the chorionic membranedepending on the time elapsed since bleeding the collection will have variable echotexture
acute hyperechoic and may be difficult to differentiate from adjacent chorionsubacute-chronic decreasing echogenicity with time
in almost all cases there is extension of the hematoma towards the margin of the placenta
First trimester SCH (subchorionic bleed)
First trimester SCH (subchorionic bleed)
Extensive hematoma in a woman with chronic bleeding
Subchorionic hemorrhage
Conjoined twins are a rare and complex complication of
monozygotic twinning which is associated with high perinatal mortality Early prenatal diagnosis of conjoined twins allows better counselling of the parents regarding the management options including continuation of pregnancy with post-natal surgery termination of pregnancy or selective fetocide in case of a triplet pregnancy With the introduction of high-resolution and transvaginal ultrasound imaging accurate prenatal diagnosis of conjoined twins is possible early in pregnancy Although first-trimester diagnosis of conjoined twins is feasible false-positive cases are common before 10 weeks because earlier in gestation fetal movements are limited and monoamniotic twins may appear conjoined As most parents opt for immediate termination of pregnancy at confirmation of the diagnosis there are limited data on the prenatal follow-up of conjoined twins detailed analysis of case reports where 3D imaging was used indicates that this modality does not improve on the diagnosis made by 2D ultrasound Overall very early prenatal diagnosis and first-trimester 3D imaging provide very little additional practical medical information compared to the 11-14 weeks ultrasound examination
Images of the conjoined twins there are two heads with conjoined body
Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You

COMMON PATHOLOGYThickened Nuchal Translucency(NL)Partial Ovular DetachmentRetained products of conceptionAnembryonic GestationGestational trophoblastic diseaseMiscarriageEctopic PregnancySubchorionic hemorrhageConjoined TwinsAntepartum HemorrhageCheck heart beatCheck causes of bleeding
Thickened Nuchal Translucency (NT)
bull One of the parameters used in sequential screening (SS) for Downrsquos syndrome in first trimester
ndash SS Pregnancy associated plasma protein levels hCG levels NT thickness
bull Measured during 11-14 wks gestational age
bull Seen on sagittal image as increased subcutaneous non-septated fluid in posterior fetal neck
bull Measurement gt3mm usually considered abnormal however exact cut off measurements are dependent on maternal agegestational age
bull Detection rate of screening for Downrsquos Syndrome in first trimester
ndash sequential screening with NT 82-87
ndash NT alone 64-70
Thickened Nuchal Translucency (NT)
Thickened Nuchal Translucency
PARTIAL OVULAR DETACHMENTThe maternal circulation inside the placenta starts peripherally (in the placental margins) and is associated to physiological oxidative phenomena that may lead to membranes rupture and formation The abnormal development of such membranes may result in subchorionic hemorrhage enhancing the predisposition to an adverse gestational outcome at the third trimester (PPROM and PTL)Such abnormality is common and also denominated as subchorionic hemorrhage or trophoblastic hematoma being visualized in more than 18 of cases of threatened miscarriage The presence of fetal heart activity confers an excellent prognosis Clinically subchorionic hemorrhage may course with vaginal bleeding At ultrasonography a crescent-shaped shadow is observed adjacent to the gestational sac with debris Gestational sac compression and consequential deformation may occur In most of cases a two-week follow-up evaluation confirms the hematoma resorption
Retained products of conception are characterized by a
thickened disorganized and heterogeneous endometrium with ill-defined mucosal layers and cavitary line either with or without the presence of gestational sac Clinically the women presents abdominal pain and relative vaginal bleeding(14) In the presence of an intact gestational sac and closed cervix the difficulty in a spontaneous resolution will be higher requiring surgical evacuation
Retained products of conception
Transvaginal sonography without (A) and with (B) color Doppler imaging in a case of RPC with endometrial expansion (arrows)
Images retained products conception
EARLY EMBRYO DEATHSome sonographic findings characterize an embryo death in the first half of the first trimester in early phases before the crown-rump length can be measured The following aspects are highlighted small hyperechoic yolk sac or hydropic yolk sac increased in volume with diameter gt 7 mm or even small amniotic cavity disproportionate to the gestational sac size Before the 9th week small gestational sac may be associated with aneuploidy
Failed early pregnancy
ANEMBRYONIC GESTATIONAt transvaginal ultrasonography the yolk sac should be visualized in a gestational sac with mean diameter gt 10 mm The absence of a yolk sac within the gestational sac with gt 10 mm in mean diameter or the absence of a yolk sac within the gestational sac with gt 16 mm in diameter characterize anembryonic gestation
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
GESTATIONAL TROPHOBLASTIC DISEASEThe typical sonographic finding in most of cases of complete hydatidiform mole is a echogenic intracavitary solid mass with intermingled small cystic loci resembling a snow storm corresponding to the vesicles that macroscopically characterize this condition The higher the gestational age the larger the vesicles visualized as homogeneous anechoic images increasing the method specificity The ultrasonography sensitivity will depend on the gestational age at the moment of the diagnosis Ultrasonography can detect vesicles with gt 2 mm in diameter In early pregnancies with trophoblastic disease the sonographic method accuracy is limited hindering the differentiation of gestational trophoblastic disease from other conditions involving the endometrial cavity
Partial hydatidiform mole offers higher diagnostic difficulty by ultrasonography In a reasonable number of cases this disease presents as an empty gestational sac corresponding to anembryonic gestation or as early embryo death However two criteria have been described in the literature gestational sac transverseanteroposterior diameter ratio gt 15 and cystic changes irregularity of increase in echogenicity of decidualplacenta or myometrial reaction
ECTOPIC PREGNANCYSonographic findings of ectopic pregnancy will vary as a function of the gestational age and site Classically the following sonographic findings are described tubal ring sign adnexal disorganized mass molded to the adnexa andor cul de sac solid organized mass with regular margins mimicking a pediculated myomatous nodule clinically progressing with low β-hCGlevels and presence of a live extrauterine conceptus Uncommon gestational sites may be observed such as abdominal ectopic pregnancy cervical ectopic pregnancy and ectopic pregnancy in a previous Cesarean section pregnancy
Subchorionic hemorrhage (SCH) occurs when there is
perigestational haemorrhage and blood collects between the uterine wall and the chorionic membrane in pregnancy It is a frequent cause of first and second trimester bleedingEpidemiologyIt typically occurs within the first 20 weeks of gestation If seen in the first 10-14 days of gestation they are also sometimes termed implantation bleedsRadiographic featuresUltrasound crescentic collection with elevation of the chorionic membranedepending on the time elapsed since bleeding the collection will have variable echotexture
acute hyperechoic and may be difficult to differentiate from adjacent chorionsubacute-chronic decreasing echogenicity with time
in almost all cases there is extension of the hematoma towards the margin of the placenta
First trimester SCH (subchorionic bleed)
First trimester SCH (subchorionic bleed)
Extensive hematoma in a woman with chronic bleeding
Subchorionic hemorrhage
Conjoined twins are a rare and complex complication of
monozygotic twinning which is associated with high perinatal mortality Early prenatal diagnosis of conjoined twins allows better counselling of the parents regarding the management options including continuation of pregnancy with post-natal surgery termination of pregnancy or selective fetocide in case of a triplet pregnancy With the introduction of high-resolution and transvaginal ultrasound imaging accurate prenatal diagnosis of conjoined twins is possible early in pregnancy Although first-trimester diagnosis of conjoined twins is feasible false-positive cases are common before 10 weeks because earlier in gestation fetal movements are limited and monoamniotic twins may appear conjoined As most parents opt for immediate termination of pregnancy at confirmation of the diagnosis there are limited data on the prenatal follow-up of conjoined twins detailed analysis of case reports where 3D imaging was used indicates that this modality does not improve on the diagnosis made by 2D ultrasound Overall very early prenatal diagnosis and first-trimester 3D imaging provide very little additional practical medical information compared to the 11-14 weeks ultrasound examination
Images of the conjoined twins there are two heads with conjoined body
Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You

Thickened Nuchal Translucency (NT)
bull One of the parameters used in sequential screening (SS) for Downrsquos syndrome in first trimester
ndash SS Pregnancy associated plasma protein levels hCG levels NT thickness
bull Measured during 11-14 wks gestational age
bull Seen on sagittal image as increased subcutaneous non-septated fluid in posterior fetal neck
bull Measurement gt3mm usually considered abnormal however exact cut off measurements are dependent on maternal agegestational age
bull Detection rate of screening for Downrsquos Syndrome in first trimester
ndash sequential screening with NT 82-87
ndash NT alone 64-70
Thickened Nuchal Translucency (NT)
Thickened Nuchal Translucency
PARTIAL OVULAR DETACHMENTThe maternal circulation inside the placenta starts peripherally (in the placental margins) and is associated to physiological oxidative phenomena that may lead to membranes rupture and formation The abnormal development of such membranes may result in subchorionic hemorrhage enhancing the predisposition to an adverse gestational outcome at the third trimester (PPROM and PTL)Such abnormality is common and also denominated as subchorionic hemorrhage or trophoblastic hematoma being visualized in more than 18 of cases of threatened miscarriage The presence of fetal heart activity confers an excellent prognosis Clinically subchorionic hemorrhage may course with vaginal bleeding At ultrasonography a crescent-shaped shadow is observed adjacent to the gestational sac with debris Gestational sac compression and consequential deformation may occur In most of cases a two-week follow-up evaluation confirms the hematoma resorption
Retained products of conception are characterized by a
thickened disorganized and heterogeneous endometrium with ill-defined mucosal layers and cavitary line either with or without the presence of gestational sac Clinically the women presents abdominal pain and relative vaginal bleeding(14) In the presence of an intact gestational sac and closed cervix the difficulty in a spontaneous resolution will be higher requiring surgical evacuation
Retained products of conception
Transvaginal sonography without (A) and with (B) color Doppler imaging in a case of RPC with endometrial expansion (arrows)
Images retained products conception
EARLY EMBRYO DEATHSome sonographic findings characterize an embryo death in the first half of the first trimester in early phases before the crown-rump length can be measured The following aspects are highlighted small hyperechoic yolk sac or hydropic yolk sac increased in volume with diameter gt 7 mm or even small amniotic cavity disproportionate to the gestational sac size Before the 9th week small gestational sac may be associated with aneuploidy
Failed early pregnancy
ANEMBRYONIC GESTATIONAt transvaginal ultrasonography the yolk sac should be visualized in a gestational sac with mean diameter gt 10 mm The absence of a yolk sac within the gestational sac with gt 10 mm in mean diameter or the absence of a yolk sac within the gestational sac with gt 16 mm in diameter characterize anembryonic gestation
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
GESTATIONAL TROPHOBLASTIC DISEASEThe typical sonographic finding in most of cases of complete hydatidiform mole is a echogenic intracavitary solid mass with intermingled small cystic loci resembling a snow storm corresponding to the vesicles that macroscopically characterize this condition The higher the gestational age the larger the vesicles visualized as homogeneous anechoic images increasing the method specificity The ultrasonography sensitivity will depend on the gestational age at the moment of the diagnosis Ultrasonography can detect vesicles with gt 2 mm in diameter In early pregnancies with trophoblastic disease the sonographic method accuracy is limited hindering the differentiation of gestational trophoblastic disease from other conditions involving the endometrial cavity
Partial hydatidiform mole offers higher diagnostic difficulty by ultrasonography In a reasonable number of cases this disease presents as an empty gestational sac corresponding to anembryonic gestation or as early embryo death However two criteria have been described in the literature gestational sac transverseanteroposterior diameter ratio gt 15 and cystic changes irregularity of increase in echogenicity of decidualplacenta or myometrial reaction
ECTOPIC PREGNANCYSonographic findings of ectopic pregnancy will vary as a function of the gestational age and site Classically the following sonographic findings are described tubal ring sign adnexal disorganized mass molded to the adnexa andor cul de sac solid organized mass with regular margins mimicking a pediculated myomatous nodule clinically progressing with low β-hCGlevels and presence of a live extrauterine conceptus Uncommon gestational sites may be observed such as abdominal ectopic pregnancy cervical ectopic pregnancy and ectopic pregnancy in a previous Cesarean section pregnancy
Subchorionic hemorrhage (SCH) occurs when there is
perigestational haemorrhage and blood collects between the uterine wall and the chorionic membrane in pregnancy It is a frequent cause of first and second trimester bleedingEpidemiologyIt typically occurs within the first 20 weeks of gestation If seen in the first 10-14 days of gestation they are also sometimes termed implantation bleedsRadiographic featuresUltrasound crescentic collection with elevation of the chorionic membranedepending on the time elapsed since bleeding the collection will have variable echotexture
acute hyperechoic and may be difficult to differentiate from adjacent chorionsubacute-chronic decreasing echogenicity with time
in almost all cases there is extension of the hematoma towards the margin of the placenta
First trimester SCH (subchorionic bleed)
First trimester SCH (subchorionic bleed)
Extensive hematoma in a woman with chronic bleeding
Subchorionic hemorrhage
Conjoined twins are a rare and complex complication of
monozygotic twinning which is associated with high perinatal mortality Early prenatal diagnosis of conjoined twins allows better counselling of the parents regarding the management options including continuation of pregnancy with post-natal surgery termination of pregnancy or selective fetocide in case of a triplet pregnancy With the introduction of high-resolution and transvaginal ultrasound imaging accurate prenatal diagnosis of conjoined twins is possible early in pregnancy Although first-trimester diagnosis of conjoined twins is feasible false-positive cases are common before 10 weeks because earlier in gestation fetal movements are limited and monoamniotic twins may appear conjoined As most parents opt for immediate termination of pregnancy at confirmation of the diagnosis there are limited data on the prenatal follow-up of conjoined twins detailed analysis of case reports where 3D imaging was used indicates that this modality does not improve on the diagnosis made by 2D ultrasound Overall very early prenatal diagnosis and first-trimester 3D imaging provide very little additional practical medical information compared to the 11-14 weeks ultrasound examination
Images of the conjoined twins there are two heads with conjoined body
Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You
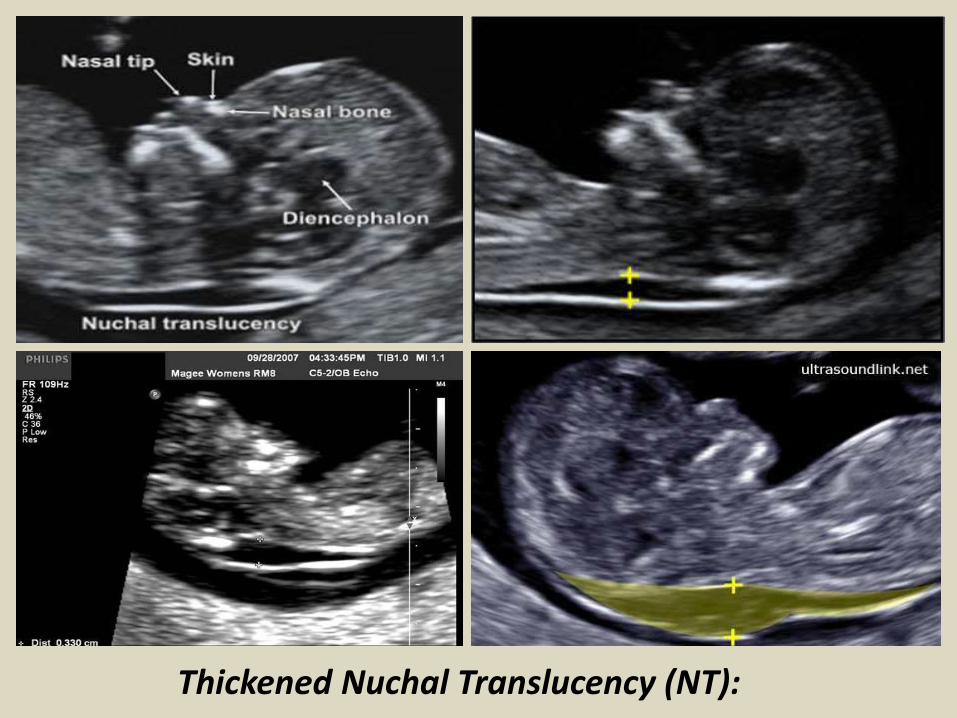
Thickened Nuchal Translucency (NT)
Thickened Nuchal Translucency
PARTIAL OVULAR DETACHMENTThe maternal circulation inside the placenta starts peripherally (in the placental margins) and is associated to physiological oxidative phenomena that may lead to membranes rupture and formation The abnormal development of such membranes may result in subchorionic hemorrhage enhancing the predisposition to an adverse gestational outcome at the third trimester (PPROM and PTL)Such abnormality is common and also denominated as subchorionic hemorrhage or trophoblastic hematoma being visualized in more than 18 of cases of threatened miscarriage The presence of fetal heart activity confers an excellent prognosis Clinically subchorionic hemorrhage may course with vaginal bleeding At ultrasonography a crescent-shaped shadow is observed adjacent to the gestational sac with debris Gestational sac compression and consequential deformation may occur In most of cases a two-week follow-up evaluation confirms the hematoma resorption
Retained products of conception are characterized by a
thickened disorganized and heterogeneous endometrium with ill-defined mucosal layers and cavitary line either with or without the presence of gestational sac Clinically the women presents abdominal pain and relative vaginal bleeding(14) In the presence of an intact gestational sac and closed cervix the difficulty in a spontaneous resolution will be higher requiring surgical evacuation
Retained products of conception
Transvaginal sonography without (A) and with (B) color Doppler imaging in a case of RPC with endometrial expansion (arrows)
Images retained products conception
EARLY EMBRYO DEATHSome sonographic findings characterize an embryo death in the first half of the first trimester in early phases before the crown-rump length can be measured The following aspects are highlighted small hyperechoic yolk sac or hydropic yolk sac increased in volume with diameter gt 7 mm or even small amniotic cavity disproportionate to the gestational sac size Before the 9th week small gestational sac may be associated with aneuploidy
Failed early pregnancy
ANEMBRYONIC GESTATIONAt transvaginal ultrasonography the yolk sac should be visualized in a gestational sac with mean diameter gt 10 mm The absence of a yolk sac within the gestational sac with gt 10 mm in mean diameter or the absence of a yolk sac within the gestational sac with gt 16 mm in diameter characterize anembryonic gestation
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
GESTATIONAL TROPHOBLASTIC DISEASEThe typical sonographic finding in most of cases of complete hydatidiform mole is a echogenic intracavitary solid mass with intermingled small cystic loci resembling a snow storm corresponding to the vesicles that macroscopically characterize this condition The higher the gestational age the larger the vesicles visualized as homogeneous anechoic images increasing the method specificity The ultrasonography sensitivity will depend on the gestational age at the moment of the diagnosis Ultrasonography can detect vesicles with gt 2 mm in diameter In early pregnancies with trophoblastic disease the sonographic method accuracy is limited hindering the differentiation of gestational trophoblastic disease from other conditions involving the endometrial cavity
Partial hydatidiform mole offers higher diagnostic difficulty by ultrasonography In a reasonable number of cases this disease presents as an empty gestational sac corresponding to anembryonic gestation or as early embryo death However two criteria have been described in the literature gestational sac transverseanteroposterior diameter ratio gt 15 and cystic changes irregularity of increase in echogenicity of decidualplacenta or myometrial reaction
ECTOPIC PREGNANCYSonographic findings of ectopic pregnancy will vary as a function of the gestational age and site Classically the following sonographic findings are described tubal ring sign adnexal disorganized mass molded to the adnexa andor cul de sac solid organized mass with regular margins mimicking a pediculated myomatous nodule clinically progressing with low β-hCGlevels and presence of a live extrauterine conceptus Uncommon gestational sites may be observed such as abdominal ectopic pregnancy cervical ectopic pregnancy and ectopic pregnancy in a previous Cesarean section pregnancy
Subchorionic hemorrhage (SCH) occurs when there is
perigestational haemorrhage and blood collects between the uterine wall and the chorionic membrane in pregnancy It is a frequent cause of first and second trimester bleedingEpidemiologyIt typically occurs within the first 20 weeks of gestation If seen in the first 10-14 days of gestation they are also sometimes termed implantation bleedsRadiographic featuresUltrasound crescentic collection with elevation of the chorionic membranedepending on the time elapsed since bleeding the collection will have variable echotexture
acute hyperechoic and may be difficult to differentiate from adjacent chorionsubacute-chronic decreasing echogenicity with time
in almost all cases there is extension of the hematoma towards the margin of the placenta
First trimester SCH (subchorionic bleed)
First trimester SCH (subchorionic bleed)
Extensive hematoma in a woman with chronic bleeding
Subchorionic hemorrhage
Conjoined twins are a rare and complex complication of
monozygotic twinning which is associated with high perinatal mortality Early prenatal diagnosis of conjoined twins allows better counselling of the parents regarding the management options including continuation of pregnancy with post-natal surgery termination of pregnancy or selective fetocide in case of a triplet pregnancy With the introduction of high-resolution and transvaginal ultrasound imaging accurate prenatal diagnosis of conjoined twins is possible early in pregnancy Although first-trimester diagnosis of conjoined twins is feasible false-positive cases are common before 10 weeks because earlier in gestation fetal movements are limited and monoamniotic twins may appear conjoined As most parents opt for immediate termination of pregnancy at confirmation of the diagnosis there are limited data on the prenatal follow-up of conjoined twins detailed analysis of case reports where 3D imaging was used indicates that this modality does not improve on the diagnosis made by 2D ultrasound Overall very early prenatal diagnosis and first-trimester 3D imaging provide very little additional practical medical information compared to the 11-14 weeks ultrasound examination
Images of the conjoined twins there are two heads with conjoined body
Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You

Thickened Nuchal Translucency
PARTIAL OVULAR DETACHMENTThe maternal circulation inside the placenta starts peripherally (in the placental margins) and is associated to physiological oxidative phenomena that may lead to membranes rupture and formation The abnormal development of such membranes may result in subchorionic hemorrhage enhancing the predisposition to an adverse gestational outcome at the third trimester (PPROM and PTL)Such abnormality is common and also denominated as subchorionic hemorrhage or trophoblastic hematoma being visualized in more than 18 of cases of threatened miscarriage The presence of fetal heart activity confers an excellent prognosis Clinically subchorionic hemorrhage may course with vaginal bleeding At ultrasonography a crescent-shaped shadow is observed adjacent to the gestational sac with debris Gestational sac compression and consequential deformation may occur In most of cases a two-week follow-up evaluation confirms the hematoma resorption
Retained products of conception are characterized by a
thickened disorganized and heterogeneous endometrium with ill-defined mucosal layers and cavitary line either with or without the presence of gestational sac Clinically the women presents abdominal pain and relative vaginal bleeding(14) In the presence of an intact gestational sac and closed cervix the difficulty in a spontaneous resolution will be higher requiring surgical evacuation
Retained products of conception
Transvaginal sonography without (A) and with (B) color Doppler imaging in a case of RPC with endometrial expansion (arrows)
Images retained products conception
EARLY EMBRYO DEATHSome sonographic findings characterize an embryo death in the first half of the first trimester in early phases before the crown-rump length can be measured The following aspects are highlighted small hyperechoic yolk sac or hydropic yolk sac increased in volume with diameter gt 7 mm or even small amniotic cavity disproportionate to the gestational sac size Before the 9th week small gestational sac may be associated with aneuploidy
Failed early pregnancy
ANEMBRYONIC GESTATIONAt transvaginal ultrasonography the yolk sac should be visualized in a gestational sac with mean diameter gt 10 mm The absence of a yolk sac within the gestational sac with gt 10 mm in mean diameter or the absence of a yolk sac within the gestational sac with gt 16 mm in diameter characterize anembryonic gestation
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
GESTATIONAL TROPHOBLASTIC DISEASEThe typical sonographic finding in most of cases of complete hydatidiform mole is a echogenic intracavitary solid mass with intermingled small cystic loci resembling a snow storm corresponding to the vesicles that macroscopically characterize this condition The higher the gestational age the larger the vesicles visualized as homogeneous anechoic images increasing the method specificity The ultrasonography sensitivity will depend on the gestational age at the moment of the diagnosis Ultrasonography can detect vesicles with gt 2 mm in diameter In early pregnancies with trophoblastic disease the sonographic method accuracy is limited hindering the differentiation of gestational trophoblastic disease from other conditions involving the endometrial cavity
Partial hydatidiform mole offers higher diagnostic difficulty by ultrasonography In a reasonable number of cases this disease presents as an empty gestational sac corresponding to anembryonic gestation or as early embryo death However two criteria have been described in the literature gestational sac transverseanteroposterior diameter ratio gt 15 and cystic changes irregularity of increase in echogenicity of decidualplacenta or myometrial reaction
ECTOPIC PREGNANCYSonographic findings of ectopic pregnancy will vary as a function of the gestational age and site Classically the following sonographic findings are described tubal ring sign adnexal disorganized mass molded to the adnexa andor cul de sac solid organized mass with regular margins mimicking a pediculated myomatous nodule clinically progressing with low β-hCGlevels and presence of a live extrauterine conceptus Uncommon gestational sites may be observed such as abdominal ectopic pregnancy cervical ectopic pregnancy and ectopic pregnancy in a previous Cesarean section pregnancy
Subchorionic hemorrhage (SCH) occurs when there is
perigestational haemorrhage and blood collects between the uterine wall and the chorionic membrane in pregnancy It is a frequent cause of first and second trimester bleedingEpidemiologyIt typically occurs within the first 20 weeks of gestation If seen in the first 10-14 days of gestation they are also sometimes termed implantation bleedsRadiographic featuresUltrasound crescentic collection with elevation of the chorionic membranedepending on the time elapsed since bleeding the collection will have variable echotexture
acute hyperechoic and may be difficult to differentiate from adjacent chorionsubacute-chronic decreasing echogenicity with time
in almost all cases there is extension of the hematoma towards the margin of the placenta
First trimester SCH (subchorionic bleed)
First trimester SCH (subchorionic bleed)
Extensive hematoma in a woman with chronic bleeding
Subchorionic hemorrhage
Conjoined twins are a rare and complex complication of
monozygotic twinning which is associated with high perinatal mortality Early prenatal diagnosis of conjoined twins allows better counselling of the parents regarding the management options including continuation of pregnancy with post-natal surgery termination of pregnancy or selective fetocide in case of a triplet pregnancy With the introduction of high-resolution and transvaginal ultrasound imaging accurate prenatal diagnosis of conjoined twins is possible early in pregnancy Although first-trimester diagnosis of conjoined twins is feasible false-positive cases are common before 10 weeks because earlier in gestation fetal movements are limited and monoamniotic twins may appear conjoined As most parents opt for immediate termination of pregnancy at confirmation of the diagnosis there are limited data on the prenatal follow-up of conjoined twins detailed analysis of case reports where 3D imaging was used indicates that this modality does not improve on the diagnosis made by 2D ultrasound Overall very early prenatal diagnosis and first-trimester 3D imaging provide very little additional practical medical information compared to the 11-14 weeks ultrasound examination
Images of the conjoined twins there are two heads with conjoined body
Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You

PARTIAL OVULAR DETACHMENTThe maternal circulation inside the placenta starts peripherally (in the placental margins) and is associated to physiological oxidative phenomena that may lead to membranes rupture and formation The abnormal development of such membranes may result in subchorionic hemorrhage enhancing the predisposition to an adverse gestational outcome at the third trimester (PPROM and PTL)Such abnormality is common and also denominated as subchorionic hemorrhage or trophoblastic hematoma being visualized in more than 18 of cases of threatened miscarriage The presence of fetal heart activity confers an excellent prognosis Clinically subchorionic hemorrhage may course with vaginal bleeding At ultrasonography a crescent-shaped shadow is observed adjacent to the gestational sac with debris Gestational sac compression and consequential deformation may occur In most of cases a two-week follow-up evaluation confirms the hematoma resorption
Retained products of conception are characterized by a
thickened disorganized and heterogeneous endometrium with ill-defined mucosal layers and cavitary line either with or without the presence of gestational sac Clinically the women presents abdominal pain and relative vaginal bleeding(14) In the presence of an intact gestational sac and closed cervix the difficulty in a spontaneous resolution will be higher requiring surgical evacuation
Retained products of conception
Transvaginal sonography without (A) and with (B) color Doppler imaging in a case of RPC with endometrial expansion (arrows)
Images retained products conception
EARLY EMBRYO DEATHSome sonographic findings characterize an embryo death in the first half of the first trimester in early phases before the crown-rump length can be measured The following aspects are highlighted small hyperechoic yolk sac or hydropic yolk sac increased in volume with diameter gt 7 mm or even small amniotic cavity disproportionate to the gestational sac size Before the 9th week small gestational sac may be associated with aneuploidy
Failed early pregnancy
ANEMBRYONIC GESTATIONAt transvaginal ultrasonography the yolk sac should be visualized in a gestational sac with mean diameter gt 10 mm The absence of a yolk sac within the gestational sac with gt 10 mm in mean diameter or the absence of a yolk sac within the gestational sac with gt 16 mm in diameter characterize anembryonic gestation
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
GESTATIONAL TROPHOBLASTIC DISEASEThe typical sonographic finding in most of cases of complete hydatidiform mole is a echogenic intracavitary solid mass with intermingled small cystic loci resembling a snow storm corresponding to the vesicles that macroscopically characterize this condition The higher the gestational age the larger the vesicles visualized as homogeneous anechoic images increasing the method specificity The ultrasonography sensitivity will depend on the gestational age at the moment of the diagnosis Ultrasonography can detect vesicles with gt 2 mm in diameter In early pregnancies with trophoblastic disease the sonographic method accuracy is limited hindering the differentiation of gestational trophoblastic disease from other conditions involving the endometrial cavity
Partial hydatidiform mole offers higher diagnostic difficulty by ultrasonography In a reasonable number of cases this disease presents as an empty gestational sac corresponding to anembryonic gestation or as early embryo death However two criteria have been described in the literature gestational sac transverseanteroposterior diameter ratio gt 15 and cystic changes irregularity of increase in echogenicity of decidualplacenta or myometrial reaction
ECTOPIC PREGNANCYSonographic findings of ectopic pregnancy will vary as a function of the gestational age and site Classically the following sonographic findings are described tubal ring sign adnexal disorganized mass molded to the adnexa andor cul de sac solid organized mass with regular margins mimicking a pediculated myomatous nodule clinically progressing with low β-hCGlevels and presence of a live extrauterine conceptus Uncommon gestational sites may be observed such as abdominal ectopic pregnancy cervical ectopic pregnancy and ectopic pregnancy in a previous Cesarean section pregnancy
Subchorionic hemorrhage (SCH) occurs when there is
perigestational haemorrhage and blood collects between the uterine wall and the chorionic membrane in pregnancy It is a frequent cause of first and second trimester bleedingEpidemiologyIt typically occurs within the first 20 weeks of gestation If seen in the first 10-14 days of gestation they are also sometimes termed implantation bleedsRadiographic featuresUltrasound crescentic collection with elevation of the chorionic membranedepending on the time elapsed since bleeding the collection will have variable echotexture
acute hyperechoic and may be difficult to differentiate from adjacent chorionsubacute-chronic decreasing echogenicity with time
in almost all cases there is extension of the hematoma towards the margin of the placenta
First trimester SCH (subchorionic bleed)
First trimester SCH (subchorionic bleed)
Extensive hematoma in a woman with chronic bleeding
Subchorionic hemorrhage
Conjoined twins are a rare and complex complication of
monozygotic twinning which is associated with high perinatal mortality Early prenatal diagnosis of conjoined twins allows better counselling of the parents regarding the management options including continuation of pregnancy with post-natal surgery termination of pregnancy or selective fetocide in case of a triplet pregnancy With the introduction of high-resolution and transvaginal ultrasound imaging accurate prenatal diagnosis of conjoined twins is possible early in pregnancy Although first-trimester diagnosis of conjoined twins is feasible false-positive cases are common before 10 weeks because earlier in gestation fetal movements are limited and monoamniotic twins may appear conjoined As most parents opt for immediate termination of pregnancy at confirmation of the diagnosis there are limited data on the prenatal follow-up of conjoined twins detailed analysis of case reports where 3D imaging was used indicates that this modality does not improve on the diagnosis made by 2D ultrasound Overall very early prenatal diagnosis and first-trimester 3D imaging provide very little additional practical medical information compared to the 11-14 weeks ultrasound examination
Images of the conjoined twins there are two heads with conjoined body
Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You
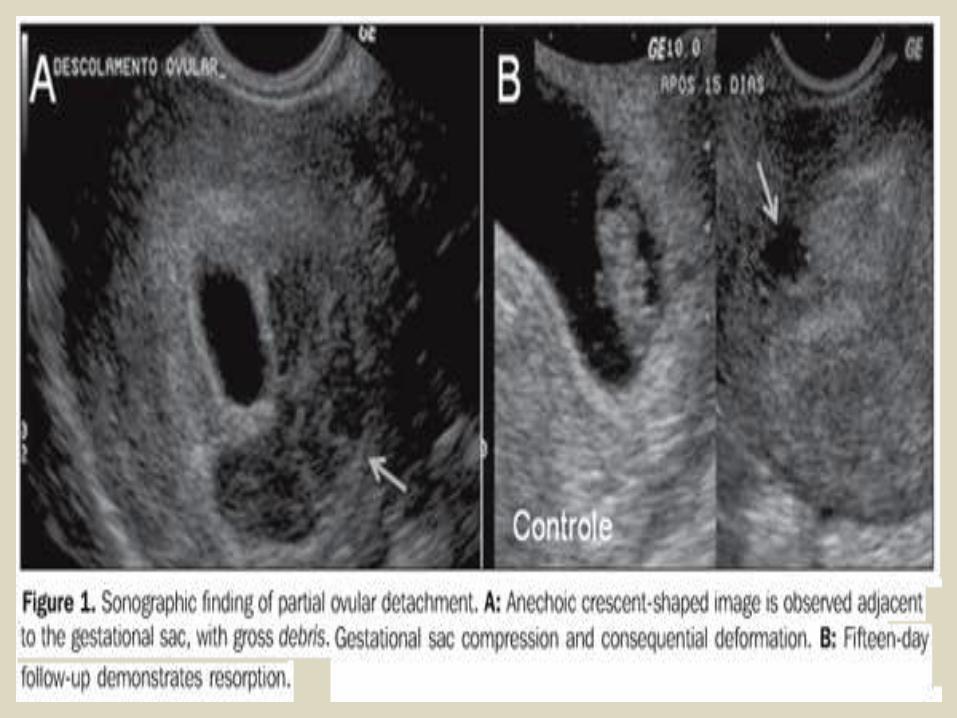
Retained products of conception are characterized by a
thickened disorganized and heterogeneous endometrium with ill-defined mucosal layers and cavitary line either with or without the presence of gestational sac Clinically the women presents abdominal pain and relative vaginal bleeding(14) In the presence of an intact gestational sac and closed cervix the difficulty in a spontaneous resolution will be higher requiring surgical evacuation
Retained products of conception
Transvaginal sonography without (A) and with (B) color Doppler imaging in a case of RPC with endometrial expansion (arrows)
Images retained products conception
EARLY EMBRYO DEATHSome sonographic findings characterize an embryo death in the first half of the first trimester in early phases before the crown-rump length can be measured The following aspects are highlighted small hyperechoic yolk sac or hydropic yolk sac increased in volume with diameter gt 7 mm or even small amniotic cavity disproportionate to the gestational sac size Before the 9th week small gestational sac may be associated with aneuploidy
Failed early pregnancy
ANEMBRYONIC GESTATIONAt transvaginal ultrasonography the yolk sac should be visualized in a gestational sac with mean diameter gt 10 mm The absence of a yolk sac within the gestational sac with gt 10 mm in mean diameter or the absence of a yolk sac within the gestational sac with gt 16 mm in diameter characterize anembryonic gestation
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
GESTATIONAL TROPHOBLASTIC DISEASEThe typical sonographic finding in most of cases of complete hydatidiform mole is a echogenic intracavitary solid mass with intermingled small cystic loci resembling a snow storm corresponding to the vesicles that macroscopically characterize this condition The higher the gestational age the larger the vesicles visualized as homogeneous anechoic images increasing the method specificity The ultrasonography sensitivity will depend on the gestational age at the moment of the diagnosis Ultrasonography can detect vesicles with gt 2 mm in diameter In early pregnancies with trophoblastic disease the sonographic method accuracy is limited hindering the differentiation of gestational trophoblastic disease from other conditions involving the endometrial cavity
Partial hydatidiform mole offers higher diagnostic difficulty by ultrasonography In a reasonable number of cases this disease presents as an empty gestational sac corresponding to anembryonic gestation or as early embryo death However two criteria have been described in the literature gestational sac transverseanteroposterior diameter ratio gt 15 and cystic changes irregularity of increase in echogenicity of decidualplacenta or myometrial reaction
ECTOPIC PREGNANCYSonographic findings of ectopic pregnancy will vary as a function of the gestational age and site Classically the following sonographic findings are described tubal ring sign adnexal disorganized mass molded to the adnexa andor cul de sac solid organized mass with regular margins mimicking a pediculated myomatous nodule clinically progressing with low β-hCGlevels and presence of a live extrauterine conceptus Uncommon gestational sites may be observed such as abdominal ectopic pregnancy cervical ectopic pregnancy and ectopic pregnancy in a previous Cesarean section pregnancy
Subchorionic hemorrhage (SCH) occurs when there is
perigestational haemorrhage and blood collects between the uterine wall and the chorionic membrane in pregnancy It is a frequent cause of first and second trimester bleedingEpidemiologyIt typically occurs within the first 20 weeks of gestation If seen in the first 10-14 days of gestation they are also sometimes termed implantation bleedsRadiographic featuresUltrasound crescentic collection with elevation of the chorionic membranedepending on the time elapsed since bleeding the collection will have variable echotexture
acute hyperechoic and may be difficult to differentiate from adjacent chorionsubacute-chronic decreasing echogenicity with time
in almost all cases there is extension of the hematoma towards the margin of the placenta
First trimester SCH (subchorionic bleed)
First trimester SCH (subchorionic bleed)
Extensive hematoma in a woman with chronic bleeding
Subchorionic hemorrhage
Conjoined twins are a rare and complex complication of
monozygotic twinning which is associated with high perinatal mortality Early prenatal diagnosis of conjoined twins allows better counselling of the parents regarding the management options including continuation of pregnancy with post-natal surgery termination of pregnancy or selective fetocide in case of a triplet pregnancy With the introduction of high-resolution and transvaginal ultrasound imaging accurate prenatal diagnosis of conjoined twins is possible early in pregnancy Although first-trimester diagnosis of conjoined twins is feasible false-positive cases are common before 10 weeks because earlier in gestation fetal movements are limited and monoamniotic twins may appear conjoined As most parents opt for immediate termination of pregnancy at confirmation of the diagnosis there are limited data on the prenatal follow-up of conjoined twins detailed analysis of case reports where 3D imaging was used indicates that this modality does not improve on the diagnosis made by 2D ultrasound Overall very early prenatal diagnosis and first-trimester 3D imaging provide very little additional practical medical information compared to the 11-14 weeks ultrasound examination
Images of the conjoined twins there are two heads with conjoined body
Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You
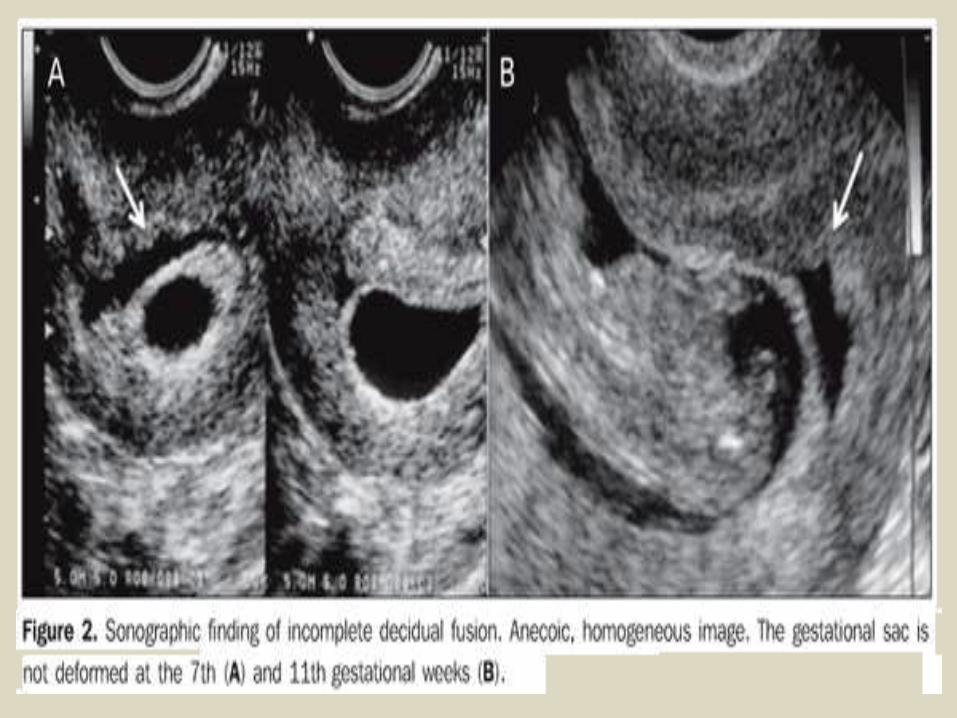
Retained products of conception
Transvaginal sonography without (A) and with (B) color Doppler imaging in a case of RPC with endometrial expansion (arrows)
Images retained products conception
EARLY EMBRYO DEATHSome sonographic findings characterize an embryo death in the first half of the first trimester in early phases before the crown-rump length can be measured The following aspects are highlighted small hyperechoic yolk sac or hydropic yolk sac increased in volume with diameter gt 7 mm or even small amniotic cavity disproportionate to the gestational sac size Before the 9th week small gestational sac may be associated with aneuploidy
Failed early pregnancy
ANEMBRYONIC GESTATIONAt transvaginal ultrasonography the yolk sac should be visualized in a gestational sac with mean diameter gt 10 mm The absence of a yolk sac within the gestational sac with gt 10 mm in mean diameter or the absence of a yolk sac within the gestational sac with gt 16 mm in diameter characterize anembryonic gestation
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
GESTATIONAL TROPHOBLASTIC DISEASEThe typical sonographic finding in most of cases of complete hydatidiform mole is a echogenic intracavitary solid mass with intermingled small cystic loci resembling a snow storm corresponding to the vesicles that macroscopically characterize this condition The higher the gestational age the larger the vesicles visualized as homogeneous anechoic images increasing the method specificity The ultrasonography sensitivity will depend on the gestational age at the moment of the diagnosis Ultrasonography can detect vesicles with gt 2 mm in diameter In early pregnancies with trophoblastic disease the sonographic method accuracy is limited hindering the differentiation of gestational trophoblastic disease from other conditions involving the endometrial cavity
Partial hydatidiform mole offers higher diagnostic difficulty by ultrasonography In a reasonable number of cases this disease presents as an empty gestational sac corresponding to anembryonic gestation or as early embryo death However two criteria have been described in the literature gestational sac transverseanteroposterior diameter ratio gt 15 and cystic changes irregularity of increase in echogenicity of decidualplacenta or myometrial reaction
ECTOPIC PREGNANCYSonographic findings of ectopic pregnancy will vary as a function of the gestational age and site Classically the following sonographic findings are described tubal ring sign adnexal disorganized mass molded to the adnexa andor cul de sac solid organized mass with regular margins mimicking a pediculated myomatous nodule clinically progressing with low β-hCGlevels and presence of a live extrauterine conceptus Uncommon gestational sites may be observed such as abdominal ectopic pregnancy cervical ectopic pregnancy and ectopic pregnancy in a previous Cesarean section pregnancy
Subchorionic hemorrhage (SCH) occurs when there is
perigestational haemorrhage and blood collects between the uterine wall and the chorionic membrane in pregnancy It is a frequent cause of first and second trimester bleedingEpidemiologyIt typically occurs within the first 20 weeks of gestation If seen in the first 10-14 days of gestation they are also sometimes termed implantation bleedsRadiographic featuresUltrasound crescentic collection with elevation of the chorionic membranedepending on the time elapsed since bleeding the collection will have variable echotexture
acute hyperechoic and may be difficult to differentiate from adjacent chorionsubacute-chronic decreasing echogenicity with time
in almost all cases there is extension of the hematoma towards the margin of the placenta
First trimester SCH (subchorionic bleed)
First trimester SCH (subchorionic bleed)
Extensive hematoma in a woman with chronic bleeding
Subchorionic hemorrhage
Conjoined twins are a rare and complex complication of
monozygotic twinning which is associated with high perinatal mortality Early prenatal diagnosis of conjoined twins allows better counselling of the parents regarding the management options including continuation of pregnancy with post-natal surgery termination of pregnancy or selective fetocide in case of a triplet pregnancy With the introduction of high-resolution and transvaginal ultrasound imaging accurate prenatal diagnosis of conjoined twins is possible early in pregnancy Although first-trimester diagnosis of conjoined twins is feasible false-positive cases are common before 10 weeks because earlier in gestation fetal movements are limited and monoamniotic twins may appear conjoined As most parents opt for immediate termination of pregnancy at confirmation of the diagnosis there are limited data on the prenatal follow-up of conjoined twins detailed analysis of case reports where 3D imaging was used indicates that this modality does not improve on the diagnosis made by 2D ultrasound Overall very early prenatal diagnosis and first-trimester 3D imaging provide very little additional practical medical information compared to the 11-14 weeks ultrasound examination
Images of the conjoined twins there are two heads with conjoined body
Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You

Transvaginal sonography without (A) and with (B) color Doppler imaging in a case of RPC with endometrial expansion (arrows)
Images retained products conception
EARLY EMBRYO DEATHSome sonographic findings characterize an embryo death in the first half of the first trimester in early phases before the crown-rump length can be measured The following aspects are highlighted small hyperechoic yolk sac or hydropic yolk sac increased in volume with diameter gt 7 mm or even small amniotic cavity disproportionate to the gestational sac size Before the 9th week small gestational sac may be associated with aneuploidy
Failed early pregnancy
ANEMBRYONIC GESTATIONAt transvaginal ultrasonography the yolk sac should be visualized in a gestational sac with mean diameter gt 10 mm The absence of a yolk sac within the gestational sac with gt 10 mm in mean diameter or the absence of a yolk sac within the gestational sac with gt 16 mm in diameter characterize anembryonic gestation
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
GESTATIONAL TROPHOBLASTIC DISEASEThe typical sonographic finding in most of cases of complete hydatidiform mole is a echogenic intracavitary solid mass with intermingled small cystic loci resembling a snow storm corresponding to the vesicles that macroscopically characterize this condition The higher the gestational age the larger the vesicles visualized as homogeneous anechoic images increasing the method specificity The ultrasonography sensitivity will depend on the gestational age at the moment of the diagnosis Ultrasonography can detect vesicles with gt 2 mm in diameter In early pregnancies with trophoblastic disease the sonographic method accuracy is limited hindering the differentiation of gestational trophoblastic disease from other conditions involving the endometrial cavity
Partial hydatidiform mole offers higher diagnostic difficulty by ultrasonography In a reasonable number of cases this disease presents as an empty gestational sac corresponding to anembryonic gestation or as early embryo death However two criteria have been described in the literature gestational sac transverseanteroposterior diameter ratio gt 15 and cystic changes irregularity of increase in echogenicity of decidualplacenta or myometrial reaction
ECTOPIC PREGNANCYSonographic findings of ectopic pregnancy will vary as a function of the gestational age and site Classically the following sonographic findings are described tubal ring sign adnexal disorganized mass molded to the adnexa andor cul de sac solid organized mass with regular margins mimicking a pediculated myomatous nodule clinically progressing with low β-hCGlevels and presence of a live extrauterine conceptus Uncommon gestational sites may be observed such as abdominal ectopic pregnancy cervical ectopic pregnancy and ectopic pregnancy in a previous Cesarean section pregnancy
Subchorionic hemorrhage (SCH) occurs when there is
perigestational haemorrhage and blood collects between the uterine wall and the chorionic membrane in pregnancy It is a frequent cause of first and second trimester bleedingEpidemiologyIt typically occurs within the first 20 weeks of gestation If seen in the first 10-14 days of gestation they are also sometimes termed implantation bleedsRadiographic featuresUltrasound crescentic collection with elevation of the chorionic membranedepending on the time elapsed since bleeding the collection will have variable echotexture
acute hyperechoic and may be difficult to differentiate from adjacent chorionsubacute-chronic decreasing echogenicity with time
in almost all cases there is extension of the hematoma towards the margin of the placenta
First trimester SCH (subchorionic bleed)
First trimester SCH (subchorionic bleed)
Extensive hematoma in a woman with chronic bleeding
Subchorionic hemorrhage
Conjoined twins are a rare and complex complication of
monozygotic twinning which is associated with high perinatal mortality Early prenatal diagnosis of conjoined twins allows better counselling of the parents regarding the management options including continuation of pregnancy with post-natal surgery termination of pregnancy or selective fetocide in case of a triplet pregnancy With the introduction of high-resolution and transvaginal ultrasound imaging accurate prenatal diagnosis of conjoined twins is possible early in pregnancy Although first-trimester diagnosis of conjoined twins is feasible false-positive cases are common before 10 weeks because earlier in gestation fetal movements are limited and monoamniotic twins may appear conjoined As most parents opt for immediate termination of pregnancy at confirmation of the diagnosis there are limited data on the prenatal follow-up of conjoined twins detailed analysis of case reports where 3D imaging was used indicates that this modality does not improve on the diagnosis made by 2D ultrasound Overall very early prenatal diagnosis and first-trimester 3D imaging provide very little additional practical medical information compared to the 11-14 weeks ultrasound examination
Images of the conjoined twins there are two heads with conjoined body
Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You
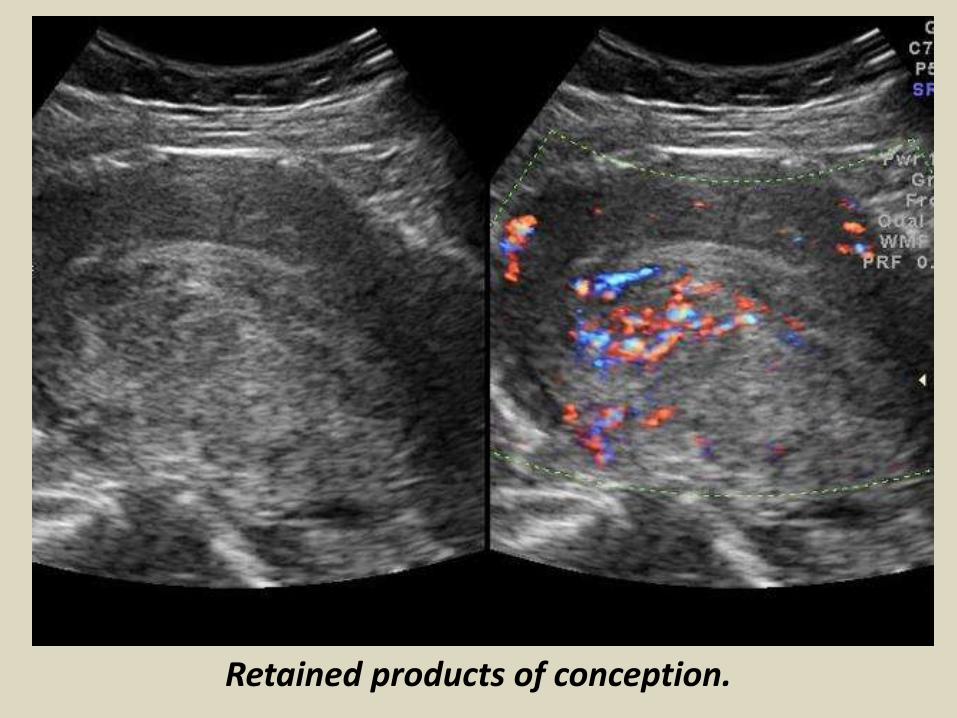
Images retained products conception
EARLY EMBRYO DEATHSome sonographic findings characterize an embryo death in the first half of the first trimester in early phases before the crown-rump length can be measured The following aspects are highlighted small hyperechoic yolk sac or hydropic yolk sac increased in volume with diameter gt 7 mm or even small amniotic cavity disproportionate to the gestational sac size Before the 9th week small gestational sac may be associated with aneuploidy
Failed early pregnancy
ANEMBRYONIC GESTATIONAt transvaginal ultrasonography the yolk sac should be visualized in a gestational sac with mean diameter gt 10 mm The absence of a yolk sac within the gestational sac with gt 10 mm in mean diameter or the absence of a yolk sac within the gestational sac with gt 16 mm in diameter characterize anembryonic gestation
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
GESTATIONAL TROPHOBLASTIC DISEASEThe typical sonographic finding in most of cases of complete hydatidiform mole is a echogenic intracavitary solid mass with intermingled small cystic loci resembling a snow storm corresponding to the vesicles that macroscopically characterize this condition The higher the gestational age the larger the vesicles visualized as homogeneous anechoic images increasing the method specificity The ultrasonography sensitivity will depend on the gestational age at the moment of the diagnosis Ultrasonography can detect vesicles with gt 2 mm in diameter In early pregnancies with trophoblastic disease the sonographic method accuracy is limited hindering the differentiation of gestational trophoblastic disease from other conditions involving the endometrial cavity
Partial hydatidiform mole offers higher diagnostic difficulty by ultrasonography In a reasonable number of cases this disease presents as an empty gestational sac corresponding to anembryonic gestation or as early embryo death However two criteria have been described in the literature gestational sac transverseanteroposterior diameter ratio gt 15 and cystic changes irregularity of increase in echogenicity of decidualplacenta or myometrial reaction
ECTOPIC PREGNANCYSonographic findings of ectopic pregnancy will vary as a function of the gestational age and site Classically the following sonographic findings are described tubal ring sign adnexal disorganized mass molded to the adnexa andor cul de sac solid organized mass with regular margins mimicking a pediculated myomatous nodule clinically progressing with low β-hCGlevels and presence of a live extrauterine conceptus Uncommon gestational sites may be observed such as abdominal ectopic pregnancy cervical ectopic pregnancy and ectopic pregnancy in a previous Cesarean section pregnancy
Subchorionic hemorrhage (SCH) occurs when there is
perigestational haemorrhage and blood collects between the uterine wall and the chorionic membrane in pregnancy It is a frequent cause of first and second trimester bleedingEpidemiologyIt typically occurs within the first 20 weeks of gestation If seen in the first 10-14 days of gestation they are also sometimes termed implantation bleedsRadiographic featuresUltrasound crescentic collection with elevation of the chorionic membranedepending on the time elapsed since bleeding the collection will have variable echotexture
acute hyperechoic and may be difficult to differentiate from adjacent chorionsubacute-chronic decreasing echogenicity with time
in almost all cases there is extension of the hematoma towards the margin of the placenta
First trimester SCH (subchorionic bleed)
First trimester SCH (subchorionic bleed)
Extensive hematoma in a woman with chronic bleeding
Subchorionic hemorrhage
Conjoined twins are a rare and complex complication of
monozygotic twinning which is associated with high perinatal mortality Early prenatal diagnosis of conjoined twins allows better counselling of the parents regarding the management options including continuation of pregnancy with post-natal surgery termination of pregnancy or selective fetocide in case of a triplet pregnancy With the introduction of high-resolution and transvaginal ultrasound imaging accurate prenatal diagnosis of conjoined twins is possible early in pregnancy Although first-trimester diagnosis of conjoined twins is feasible false-positive cases are common before 10 weeks because earlier in gestation fetal movements are limited and monoamniotic twins may appear conjoined As most parents opt for immediate termination of pregnancy at confirmation of the diagnosis there are limited data on the prenatal follow-up of conjoined twins detailed analysis of case reports where 3D imaging was used indicates that this modality does not improve on the diagnosis made by 2D ultrasound Overall very early prenatal diagnosis and first-trimester 3D imaging provide very little additional practical medical information compared to the 11-14 weeks ultrasound examination
Images of the conjoined twins there are two heads with conjoined body
Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You

EARLY EMBRYO DEATHSome sonographic findings characterize an embryo death in the first half of the first trimester in early phases before the crown-rump length can be measured The following aspects are highlighted small hyperechoic yolk sac or hydropic yolk sac increased in volume with diameter gt 7 mm or even small amniotic cavity disproportionate to the gestational sac size Before the 9th week small gestational sac may be associated with aneuploidy
Failed early pregnancy
ANEMBRYONIC GESTATIONAt transvaginal ultrasonography the yolk sac should be visualized in a gestational sac with mean diameter gt 10 mm The absence of a yolk sac within the gestational sac with gt 10 mm in mean diameter or the absence of a yolk sac within the gestational sac with gt 16 mm in diameter characterize anembryonic gestation
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
GESTATIONAL TROPHOBLASTIC DISEASEThe typical sonographic finding in most of cases of complete hydatidiform mole is a echogenic intracavitary solid mass with intermingled small cystic loci resembling a snow storm corresponding to the vesicles that macroscopically characterize this condition The higher the gestational age the larger the vesicles visualized as homogeneous anechoic images increasing the method specificity The ultrasonography sensitivity will depend on the gestational age at the moment of the diagnosis Ultrasonography can detect vesicles with gt 2 mm in diameter In early pregnancies with trophoblastic disease the sonographic method accuracy is limited hindering the differentiation of gestational trophoblastic disease from other conditions involving the endometrial cavity
Partial hydatidiform mole offers higher diagnostic difficulty by ultrasonography In a reasonable number of cases this disease presents as an empty gestational sac corresponding to anembryonic gestation or as early embryo death However two criteria have been described in the literature gestational sac transverseanteroposterior diameter ratio gt 15 and cystic changes irregularity of increase in echogenicity of decidualplacenta or myometrial reaction
ECTOPIC PREGNANCYSonographic findings of ectopic pregnancy will vary as a function of the gestational age and site Classically the following sonographic findings are described tubal ring sign adnexal disorganized mass molded to the adnexa andor cul de sac solid organized mass with regular margins mimicking a pediculated myomatous nodule clinically progressing with low β-hCGlevels and presence of a live extrauterine conceptus Uncommon gestational sites may be observed such as abdominal ectopic pregnancy cervical ectopic pregnancy and ectopic pregnancy in a previous Cesarean section pregnancy
Subchorionic hemorrhage (SCH) occurs when there is
perigestational haemorrhage and blood collects between the uterine wall and the chorionic membrane in pregnancy It is a frequent cause of first and second trimester bleedingEpidemiologyIt typically occurs within the first 20 weeks of gestation If seen in the first 10-14 days of gestation they are also sometimes termed implantation bleedsRadiographic featuresUltrasound crescentic collection with elevation of the chorionic membranedepending on the time elapsed since bleeding the collection will have variable echotexture
acute hyperechoic and may be difficult to differentiate from adjacent chorionsubacute-chronic decreasing echogenicity with time
in almost all cases there is extension of the hematoma towards the margin of the placenta
First trimester SCH (subchorionic bleed)
First trimester SCH (subchorionic bleed)
Extensive hematoma in a woman with chronic bleeding
Subchorionic hemorrhage
Conjoined twins are a rare and complex complication of
monozygotic twinning which is associated with high perinatal mortality Early prenatal diagnosis of conjoined twins allows better counselling of the parents regarding the management options including continuation of pregnancy with post-natal surgery termination of pregnancy or selective fetocide in case of a triplet pregnancy With the introduction of high-resolution and transvaginal ultrasound imaging accurate prenatal diagnosis of conjoined twins is possible early in pregnancy Although first-trimester diagnosis of conjoined twins is feasible false-positive cases are common before 10 weeks because earlier in gestation fetal movements are limited and monoamniotic twins may appear conjoined As most parents opt for immediate termination of pregnancy at confirmation of the diagnosis there are limited data on the prenatal follow-up of conjoined twins detailed analysis of case reports where 3D imaging was used indicates that this modality does not improve on the diagnosis made by 2D ultrasound Overall very early prenatal diagnosis and first-trimester 3D imaging provide very little additional practical medical information compared to the 11-14 weeks ultrasound examination
Images of the conjoined twins there are two heads with conjoined body
Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You
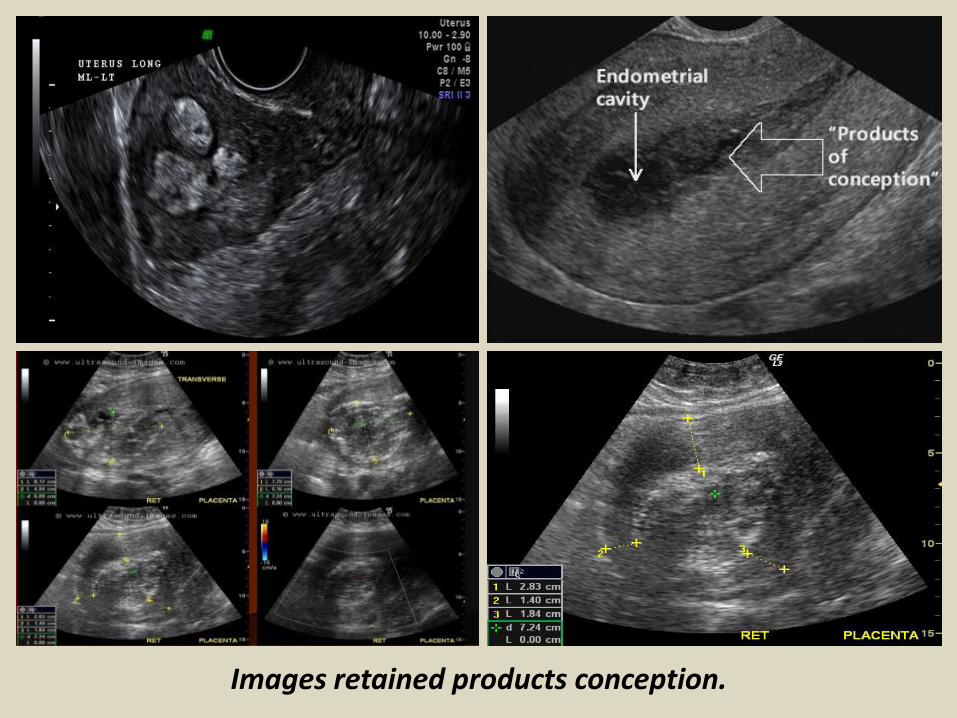
Failed early pregnancy
ANEMBRYONIC GESTATIONAt transvaginal ultrasonography the yolk sac should be visualized in a gestational sac with mean diameter gt 10 mm The absence of a yolk sac within the gestational sac with gt 10 mm in mean diameter or the absence of a yolk sac within the gestational sac with gt 16 mm in diameter characterize anembryonic gestation
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
GESTATIONAL TROPHOBLASTIC DISEASEThe typical sonographic finding in most of cases of complete hydatidiform mole is a echogenic intracavitary solid mass with intermingled small cystic loci resembling a snow storm corresponding to the vesicles that macroscopically characterize this condition The higher the gestational age the larger the vesicles visualized as homogeneous anechoic images increasing the method specificity The ultrasonography sensitivity will depend on the gestational age at the moment of the diagnosis Ultrasonography can detect vesicles with gt 2 mm in diameter In early pregnancies with trophoblastic disease the sonographic method accuracy is limited hindering the differentiation of gestational trophoblastic disease from other conditions involving the endometrial cavity
Partial hydatidiform mole offers higher diagnostic difficulty by ultrasonography In a reasonable number of cases this disease presents as an empty gestational sac corresponding to anembryonic gestation or as early embryo death However two criteria have been described in the literature gestational sac transverseanteroposterior diameter ratio gt 15 and cystic changes irregularity of increase in echogenicity of decidualplacenta or myometrial reaction
ECTOPIC PREGNANCYSonographic findings of ectopic pregnancy will vary as a function of the gestational age and site Classically the following sonographic findings are described tubal ring sign adnexal disorganized mass molded to the adnexa andor cul de sac solid organized mass with regular margins mimicking a pediculated myomatous nodule clinically progressing with low β-hCGlevels and presence of a live extrauterine conceptus Uncommon gestational sites may be observed such as abdominal ectopic pregnancy cervical ectopic pregnancy and ectopic pregnancy in a previous Cesarean section pregnancy
Subchorionic hemorrhage (SCH) occurs when there is
perigestational haemorrhage and blood collects between the uterine wall and the chorionic membrane in pregnancy It is a frequent cause of first and second trimester bleedingEpidemiologyIt typically occurs within the first 20 weeks of gestation If seen in the first 10-14 days of gestation they are also sometimes termed implantation bleedsRadiographic featuresUltrasound crescentic collection with elevation of the chorionic membranedepending on the time elapsed since bleeding the collection will have variable echotexture
acute hyperechoic and may be difficult to differentiate from adjacent chorionsubacute-chronic decreasing echogenicity with time
in almost all cases there is extension of the hematoma towards the margin of the placenta
First trimester SCH (subchorionic bleed)
First trimester SCH (subchorionic bleed)
Extensive hematoma in a woman with chronic bleeding
Subchorionic hemorrhage
Conjoined twins are a rare and complex complication of
monozygotic twinning which is associated with high perinatal mortality Early prenatal diagnosis of conjoined twins allows better counselling of the parents regarding the management options including continuation of pregnancy with post-natal surgery termination of pregnancy or selective fetocide in case of a triplet pregnancy With the introduction of high-resolution and transvaginal ultrasound imaging accurate prenatal diagnosis of conjoined twins is possible early in pregnancy Although first-trimester diagnosis of conjoined twins is feasible false-positive cases are common before 10 weeks because earlier in gestation fetal movements are limited and monoamniotic twins may appear conjoined As most parents opt for immediate termination of pregnancy at confirmation of the diagnosis there are limited data on the prenatal follow-up of conjoined twins detailed analysis of case reports where 3D imaging was used indicates that this modality does not improve on the diagnosis made by 2D ultrasound Overall very early prenatal diagnosis and first-trimester 3D imaging provide very little additional practical medical information compared to the 11-14 weeks ultrasound examination
Images of the conjoined twins there are two heads with conjoined body
Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You

ANEMBRYONIC GESTATIONAt transvaginal ultrasonography the yolk sac should be visualized in a gestational sac with mean diameter gt 10 mm The absence of a yolk sac within the gestational sac with gt 10 mm in mean diameter or the absence of a yolk sac within the gestational sac with gt 16 mm in diameter characterize anembryonic gestation
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
GESTATIONAL TROPHOBLASTIC DISEASEThe typical sonographic finding in most of cases of complete hydatidiform mole is a echogenic intracavitary solid mass with intermingled small cystic loci resembling a snow storm corresponding to the vesicles that macroscopically characterize this condition The higher the gestational age the larger the vesicles visualized as homogeneous anechoic images increasing the method specificity The ultrasonography sensitivity will depend on the gestational age at the moment of the diagnosis Ultrasonography can detect vesicles with gt 2 mm in diameter In early pregnancies with trophoblastic disease the sonographic method accuracy is limited hindering the differentiation of gestational trophoblastic disease from other conditions involving the endometrial cavity
Partial hydatidiform mole offers higher diagnostic difficulty by ultrasonography In a reasonable number of cases this disease presents as an empty gestational sac corresponding to anembryonic gestation or as early embryo death However two criteria have been described in the literature gestational sac transverseanteroposterior diameter ratio gt 15 and cystic changes irregularity of increase in echogenicity of decidualplacenta or myometrial reaction
ECTOPIC PREGNANCYSonographic findings of ectopic pregnancy will vary as a function of the gestational age and site Classically the following sonographic findings are described tubal ring sign adnexal disorganized mass molded to the adnexa andor cul de sac solid organized mass with regular margins mimicking a pediculated myomatous nodule clinically progressing with low β-hCGlevels and presence of a live extrauterine conceptus Uncommon gestational sites may be observed such as abdominal ectopic pregnancy cervical ectopic pregnancy and ectopic pregnancy in a previous Cesarean section pregnancy
Subchorionic hemorrhage (SCH) occurs when there is
perigestational haemorrhage and blood collects between the uterine wall and the chorionic membrane in pregnancy It is a frequent cause of first and second trimester bleedingEpidemiologyIt typically occurs within the first 20 weeks of gestation If seen in the first 10-14 days of gestation they are also sometimes termed implantation bleedsRadiographic featuresUltrasound crescentic collection with elevation of the chorionic membranedepending on the time elapsed since bleeding the collection will have variable echotexture
acute hyperechoic and may be difficult to differentiate from adjacent chorionsubacute-chronic decreasing echogenicity with time
in almost all cases there is extension of the hematoma towards the margin of the placenta
First trimester SCH (subchorionic bleed)
First trimester SCH (subchorionic bleed)
Extensive hematoma in a woman with chronic bleeding
Subchorionic hemorrhage
Conjoined twins are a rare and complex complication of
monozygotic twinning which is associated with high perinatal mortality Early prenatal diagnosis of conjoined twins allows better counselling of the parents regarding the management options including continuation of pregnancy with post-natal surgery termination of pregnancy or selective fetocide in case of a triplet pregnancy With the introduction of high-resolution and transvaginal ultrasound imaging accurate prenatal diagnosis of conjoined twins is possible early in pregnancy Although first-trimester diagnosis of conjoined twins is feasible false-positive cases are common before 10 weeks because earlier in gestation fetal movements are limited and monoamniotic twins may appear conjoined As most parents opt for immediate termination of pregnancy at confirmation of the diagnosis there are limited data on the prenatal follow-up of conjoined twins detailed analysis of case reports where 3D imaging was used indicates that this modality does not improve on the diagnosis made by 2D ultrasound Overall very early prenatal diagnosis and first-trimester 3D imaging provide very little additional practical medical information compared to the 11-14 weeks ultrasound examination
Images of the conjoined twins there are two heads with conjoined body
Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You

IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
GESTATIONAL TROPHOBLASTIC DISEASEThe typical sonographic finding in most of cases of complete hydatidiform mole is a echogenic intracavitary solid mass with intermingled small cystic loci resembling a snow storm corresponding to the vesicles that macroscopically characterize this condition The higher the gestational age the larger the vesicles visualized as homogeneous anechoic images increasing the method specificity The ultrasonography sensitivity will depend on the gestational age at the moment of the diagnosis Ultrasonography can detect vesicles with gt 2 mm in diameter In early pregnancies with trophoblastic disease the sonographic method accuracy is limited hindering the differentiation of gestational trophoblastic disease from other conditions involving the endometrial cavity
Partial hydatidiform mole offers higher diagnostic difficulty by ultrasonography In a reasonable number of cases this disease presents as an empty gestational sac corresponding to anembryonic gestation or as early embryo death However two criteria have been described in the literature gestational sac transverseanteroposterior diameter ratio gt 15 and cystic changes irregularity of increase in echogenicity of decidualplacenta or myometrial reaction
ECTOPIC PREGNANCYSonographic findings of ectopic pregnancy will vary as a function of the gestational age and site Classically the following sonographic findings are described tubal ring sign adnexal disorganized mass molded to the adnexa andor cul de sac solid organized mass with regular margins mimicking a pediculated myomatous nodule clinically progressing with low β-hCGlevels and presence of a live extrauterine conceptus Uncommon gestational sites may be observed such as abdominal ectopic pregnancy cervical ectopic pregnancy and ectopic pregnancy in a previous Cesarean section pregnancy
Subchorionic hemorrhage (SCH) occurs when there is
perigestational haemorrhage and blood collects between the uterine wall and the chorionic membrane in pregnancy It is a frequent cause of first and second trimester bleedingEpidemiologyIt typically occurs within the first 20 weeks of gestation If seen in the first 10-14 days of gestation they are also sometimes termed implantation bleedsRadiographic featuresUltrasound crescentic collection with elevation of the chorionic membranedepending on the time elapsed since bleeding the collection will have variable echotexture
acute hyperechoic and may be difficult to differentiate from adjacent chorionsubacute-chronic decreasing echogenicity with time
in almost all cases there is extension of the hematoma towards the margin of the placenta
First trimester SCH (subchorionic bleed)
First trimester SCH (subchorionic bleed)
Extensive hematoma in a woman with chronic bleeding
Subchorionic hemorrhage
Conjoined twins are a rare and complex complication of
monozygotic twinning which is associated with high perinatal mortality Early prenatal diagnosis of conjoined twins allows better counselling of the parents regarding the management options including continuation of pregnancy with post-natal surgery termination of pregnancy or selective fetocide in case of a triplet pregnancy With the introduction of high-resolution and transvaginal ultrasound imaging accurate prenatal diagnosis of conjoined twins is possible early in pregnancy Although first-trimester diagnosis of conjoined twins is feasible false-positive cases are common before 10 weeks because earlier in gestation fetal movements are limited and monoamniotic twins may appear conjoined As most parents opt for immediate termination of pregnancy at confirmation of the diagnosis there are limited data on the prenatal follow-up of conjoined twins detailed analysis of case reports where 3D imaging was used indicates that this modality does not improve on the diagnosis made by 2D ultrasound Overall very early prenatal diagnosis and first-trimester 3D imaging provide very little additional practical medical information compared to the 11-14 weeks ultrasound examination
Images of the conjoined twins there are two heads with conjoined body
Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You
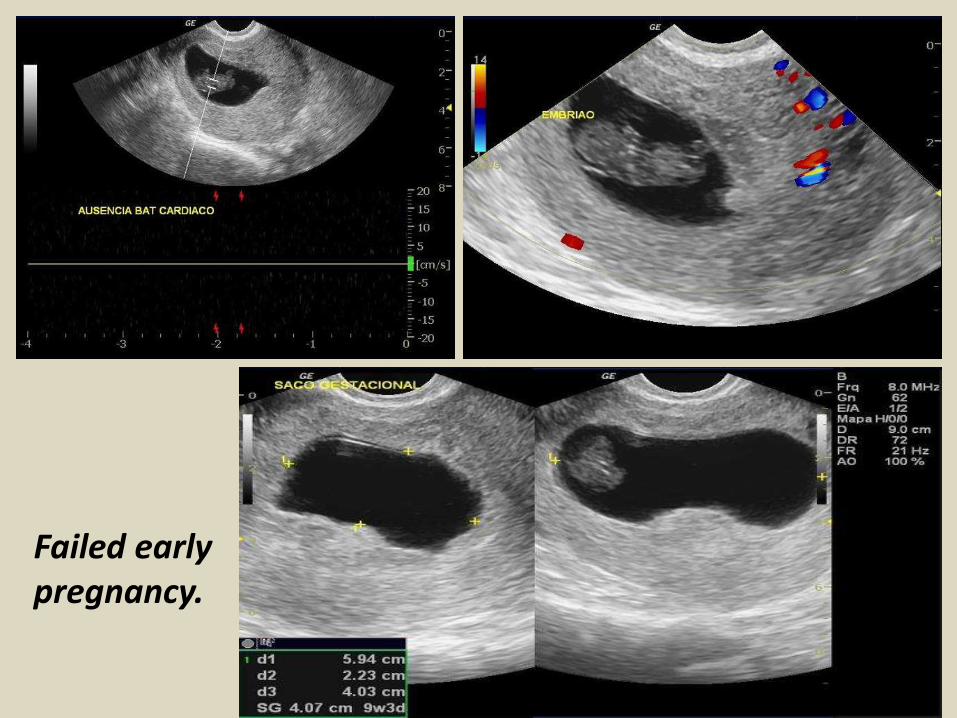
IMAGES FOR ANEMBRYONIC PREGNANCY (BLIGHTED OVUM PREGNANCY)
GESTATIONAL TROPHOBLASTIC DISEASEThe typical sonographic finding in most of cases of complete hydatidiform mole is a echogenic intracavitary solid mass with intermingled small cystic loci resembling a snow storm corresponding to the vesicles that macroscopically characterize this condition The higher the gestational age the larger the vesicles visualized as homogeneous anechoic images increasing the method specificity The ultrasonography sensitivity will depend on the gestational age at the moment of the diagnosis Ultrasonography can detect vesicles with gt 2 mm in diameter In early pregnancies with trophoblastic disease the sonographic method accuracy is limited hindering the differentiation of gestational trophoblastic disease from other conditions involving the endometrial cavity
Partial hydatidiform mole offers higher diagnostic difficulty by ultrasonography In a reasonable number of cases this disease presents as an empty gestational sac corresponding to anembryonic gestation or as early embryo death However two criteria have been described in the literature gestational sac transverseanteroposterior diameter ratio gt 15 and cystic changes irregularity of increase in echogenicity of decidualplacenta or myometrial reaction
ECTOPIC PREGNANCYSonographic findings of ectopic pregnancy will vary as a function of the gestational age and site Classically the following sonographic findings are described tubal ring sign adnexal disorganized mass molded to the adnexa andor cul de sac solid organized mass with regular margins mimicking a pediculated myomatous nodule clinically progressing with low β-hCGlevels and presence of a live extrauterine conceptus Uncommon gestational sites may be observed such as abdominal ectopic pregnancy cervical ectopic pregnancy and ectopic pregnancy in a previous Cesarean section pregnancy
Subchorionic hemorrhage (SCH) occurs when there is
perigestational haemorrhage and blood collects between the uterine wall and the chorionic membrane in pregnancy It is a frequent cause of first and second trimester bleedingEpidemiologyIt typically occurs within the first 20 weeks of gestation If seen in the first 10-14 days of gestation they are also sometimes termed implantation bleedsRadiographic featuresUltrasound crescentic collection with elevation of the chorionic membranedepending on the time elapsed since bleeding the collection will have variable echotexture
acute hyperechoic and may be difficult to differentiate from adjacent chorionsubacute-chronic decreasing echogenicity with time
in almost all cases there is extension of the hematoma towards the margin of the placenta
First trimester SCH (subchorionic bleed)
First trimester SCH (subchorionic bleed)
Extensive hematoma in a woman with chronic bleeding
Subchorionic hemorrhage
Conjoined twins are a rare and complex complication of
monozygotic twinning which is associated with high perinatal mortality Early prenatal diagnosis of conjoined twins allows better counselling of the parents regarding the management options including continuation of pregnancy with post-natal surgery termination of pregnancy or selective fetocide in case of a triplet pregnancy With the introduction of high-resolution and transvaginal ultrasound imaging accurate prenatal diagnosis of conjoined twins is possible early in pregnancy Although first-trimester diagnosis of conjoined twins is feasible false-positive cases are common before 10 weeks because earlier in gestation fetal movements are limited and monoamniotic twins may appear conjoined As most parents opt for immediate termination of pregnancy at confirmation of the diagnosis there are limited data on the prenatal follow-up of conjoined twins detailed analysis of case reports where 3D imaging was used indicates that this modality does not improve on the diagnosis made by 2D ultrasound Overall very early prenatal diagnosis and first-trimester 3D imaging provide very little additional practical medical information compared to the 11-14 weeks ultrasound examination
Images of the conjoined twins there are two heads with conjoined body
Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You
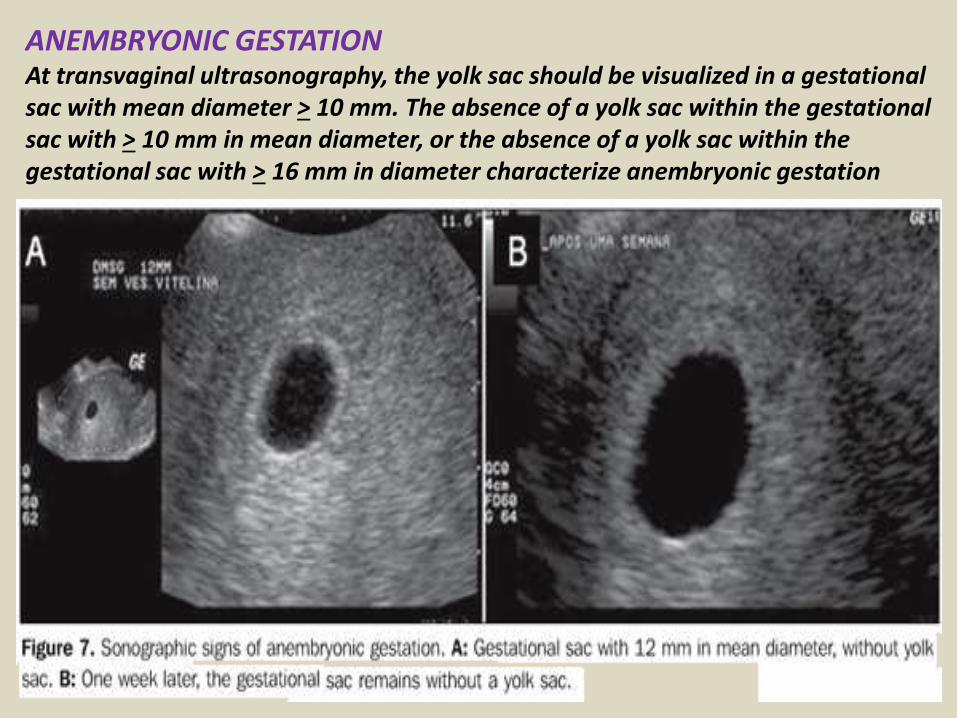
GESTATIONAL TROPHOBLASTIC DISEASEThe typical sonographic finding in most of cases of complete hydatidiform mole is a echogenic intracavitary solid mass with intermingled small cystic loci resembling a snow storm corresponding to the vesicles that macroscopically characterize this condition The higher the gestational age the larger the vesicles visualized as homogeneous anechoic images increasing the method specificity The ultrasonography sensitivity will depend on the gestational age at the moment of the diagnosis Ultrasonography can detect vesicles with gt 2 mm in diameter In early pregnancies with trophoblastic disease the sonographic method accuracy is limited hindering the differentiation of gestational trophoblastic disease from other conditions involving the endometrial cavity
Partial hydatidiform mole offers higher diagnostic difficulty by ultrasonography In a reasonable number of cases this disease presents as an empty gestational sac corresponding to anembryonic gestation or as early embryo death However two criteria have been described in the literature gestational sac transverseanteroposterior diameter ratio gt 15 and cystic changes irregularity of increase in echogenicity of decidualplacenta or myometrial reaction
ECTOPIC PREGNANCYSonographic findings of ectopic pregnancy will vary as a function of the gestational age and site Classically the following sonographic findings are described tubal ring sign adnexal disorganized mass molded to the adnexa andor cul de sac solid organized mass with regular margins mimicking a pediculated myomatous nodule clinically progressing with low β-hCGlevels and presence of a live extrauterine conceptus Uncommon gestational sites may be observed such as abdominal ectopic pregnancy cervical ectopic pregnancy and ectopic pregnancy in a previous Cesarean section pregnancy
Subchorionic hemorrhage (SCH) occurs when there is
perigestational haemorrhage and blood collects between the uterine wall and the chorionic membrane in pregnancy It is a frequent cause of first and second trimester bleedingEpidemiologyIt typically occurs within the first 20 weeks of gestation If seen in the first 10-14 days of gestation they are also sometimes termed implantation bleedsRadiographic featuresUltrasound crescentic collection with elevation of the chorionic membranedepending on the time elapsed since bleeding the collection will have variable echotexture
acute hyperechoic and may be difficult to differentiate from adjacent chorionsubacute-chronic decreasing echogenicity with time
in almost all cases there is extension of the hematoma towards the margin of the placenta
First trimester SCH (subchorionic bleed)
First trimester SCH (subchorionic bleed)
Extensive hematoma in a woman with chronic bleeding
Subchorionic hemorrhage
Conjoined twins are a rare and complex complication of
monozygotic twinning which is associated with high perinatal mortality Early prenatal diagnosis of conjoined twins allows better counselling of the parents regarding the management options including continuation of pregnancy with post-natal surgery termination of pregnancy or selective fetocide in case of a triplet pregnancy With the introduction of high-resolution and transvaginal ultrasound imaging accurate prenatal diagnosis of conjoined twins is possible early in pregnancy Although first-trimester diagnosis of conjoined twins is feasible false-positive cases are common before 10 weeks because earlier in gestation fetal movements are limited and monoamniotic twins may appear conjoined As most parents opt for immediate termination of pregnancy at confirmation of the diagnosis there are limited data on the prenatal follow-up of conjoined twins detailed analysis of case reports where 3D imaging was used indicates that this modality does not improve on the diagnosis made by 2D ultrasound Overall very early prenatal diagnosis and first-trimester 3D imaging provide very little additional practical medical information compared to the 11-14 weeks ultrasound examination
Images of the conjoined twins there are two heads with conjoined body
Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You

ECTOPIC PREGNANCYSonographic findings of ectopic pregnancy will vary as a function of the gestational age and site Classically the following sonographic findings are described tubal ring sign adnexal disorganized mass molded to the adnexa andor cul de sac solid organized mass with regular margins mimicking a pediculated myomatous nodule clinically progressing with low β-hCGlevels and presence of a live extrauterine conceptus Uncommon gestational sites may be observed such as abdominal ectopic pregnancy cervical ectopic pregnancy and ectopic pregnancy in a previous Cesarean section pregnancy
Subchorionic hemorrhage (SCH) occurs when there is
perigestational haemorrhage and blood collects between the uterine wall and the chorionic membrane in pregnancy It is a frequent cause of first and second trimester bleedingEpidemiologyIt typically occurs within the first 20 weeks of gestation If seen in the first 10-14 days of gestation they are also sometimes termed implantation bleedsRadiographic featuresUltrasound crescentic collection with elevation of the chorionic membranedepending on the time elapsed since bleeding the collection will have variable echotexture
acute hyperechoic and may be difficult to differentiate from adjacent chorionsubacute-chronic decreasing echogenicity with time
in almost all cases there is extension of the hematoma towards the margin of the placenta
First trimester SCH (subchorionic bleed)
First trimester SCH (subchorionic bleed)
Extensive hematoma in a woman with chronic bleeding
Subchorionic hemorrhage
Conjoined twins are a rare and complex complication of
monozygotic twinning which is associated with high perinatal mortality Early prenatal diagnosis of conjoined twins allows better counselling of the parents regarding the management options including continuation of pregnancy with post-natal surgery termination of pregnancy or selective fetocide in case of a triplet pregnancy With the introduction of high-resolution and transvaginal ultrasound imaging accurate prenatal diagnosis of conjoined twins is possible early in pregnancy Although first-trimester diagnosis of conjoined twins is feasible false-positive cases are common before 10 weeks because earlier in gestation fetal movements are limited and monoamniotic twins may appear conjoined As most parents opt for immediate termination of pregnancy at confirmation of the diagnosis there are limited data on the prenatal follow-up of conjoined twins detailed analysis of case reports where 3D imaging was used indicates that this modality does not improve on the diagnosis made by 2D ultrasound Overall very early prenatal diagnosis and first-trimester 3D imaging provide very little additional practical medical information compared to the 11-14 weeks ultrasound examination
Images of the conjoined twins there are two heads with conjoined body
Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You

Subchorionic hemorrhage (SCH) occurs when there is
perigestational haemorrhage and blood collects between the uterine wall and the chorionic membrane in pregnancy It is a frequent cause of first and second trimester bleedingEpidemiologyIt typically occurs within the first 20 weeks of gestation If seen in the first 10-14 days of gestation they are also sometimes termed implantation bleedsRadiographic featuresUltrasound crescentic collection with elevation of the chorionic membranedepending on the time elapsed since bleeding the collection will have variable echotexture
acute hyperechoic and may be difficult to differentiate from adjacent chorionsubacute-chronic decreasing echogenicity with time
in almost all cases there is extension of the hematoma towards the margin of the placenta
First trimester SCH (subchorionic bleed)
First trimester SCH (subchorionic bleed)
Extensive hematoma in a woman with chronic bleeding
Subchorionic hemorrhage
Conjoined twins are a rare and complex complication of
monozygotic twinning which is associated with high perinatal mortality Early prenatal diagnosis of conjoined twins allows better counselling of the parents regarding the management options including continuation of pregnancy with post-natal surgery termination of pregnancy or selective fetocide in case of a triplet pregnancy With the introduction of high-resolution and transvaginal ultrasound imaging accurate prenatal diagnosis of conjoined twins is possible early in pregnancy Although first-trimester diagnosis of conjoined twins is feasible false-positive cases are common before 10 weeks because earlier in gestation fetal movements are limited and monoamniotic twins may appear conjoined As most parents opt for immediate termination of pregnancy at confirmation of the diagnosis there are limited data on the prenatal follow-up of conjoined twins detailed analysis of case reports where 3D imaging was used indicates that this modality does not improve on the diagnosis made by 2D ultrasound Overall very early prenatal diagnosis and first-trimester 3D imaging provide very little additional practical medical information compared to the 11-14 weeks ultrasound examination
Images of the conjoined twins there are two heads with conjoined body
Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You

First trimester SCH (subchorionic bleed)
First trimester SCH (subchorionic bleed)
Extensive hematoma in a woman with chronic bleeding
Subchorionic hemorrhage
Conjoined twins are a rare and complex complication of
monozygotic twinning which is associated with high perinatal mortality Early prenatal diagnosis of conjoined twins allows better counselling of the parents regarding the management options including continuation of pregnancy with post-natal surgery termination of pregnancy or selective fetocide in case of a triplet pregnancy With the introduction of high-resolution and transvaginal ultrasound imaging accurate prenatal diagnosis of conjoined twins is possible early in pregnancy Although first-trimester diagnosis of conjoined twins is feasible false-positive cases are common before 10 weeks because earlier in gestation fetal movements are limited and monoamniotic twins may appear conjoined As most parents opt for immediate termination of pregnancy at confirmation of the diagnosis there are limited data on the prenatal follow-up of conjoined twins detailed analysis of case reports where 3D imaging was used indicates that this modality does not improve on the diagnosis made by 2D ultrasound Overall very early prenatal diagnosis and first-trimester 3D imaging provide very little additional practical medical information compared to the 11-14 weeks ultrasound examination
Images of the conjoined twins there are two heads with conjoined body
Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You

First trimester SCH (subchorionic bleed)
Extensive hematoma in a woman with chronic bleeding
Subchorionic hemorrhage
Conjoined twins are a rare and complex complication of
monozygotic twinning which is associated with high perinatal mortality Early prenatal diagnosis of conjoined twins allows better counselling of the parents regarding the management options including continuation of pregnancy with post-natal surgery termination of pregnancy or selective fetocide in case of a triplet pregnancy With the introduction of high-resolution and transvaginal ultrasound imaging accurate prenatal diagnosis of conjoined twins is possible early in pregnancy Although first-trimester diagnosis of conjoined twins is feasible false-positive cases are common before 10 weeks because earlier in gestation fetal movements are limited and monoamniotic twins may appear conjoined As most parents opt for immediate termination of pregnancy at confirmation of the diagnosis there are limited data on the prenatal follow-up of conjoined twins detailed analysis of case reports where 3D imaging was used indicates that this modality does not improve on the diagnosis made by 2D ultrasound Overall very early prenatal diagnosis and first-trimester 3D imaging provide very little additional practical medical information compared to the 11-14 weeks ultrasound examination
Images of the conjoined twins there are two heads with conjoined body
Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You

Extensive hematoma in a woman with chronic bleeding
Subchorionic hemorrhage
Conjoined twins are a rare and complex complication of
monozygotic twinning which is associated with high perinatal mortality Early prenatal diagnosis of conjoined twins allows better counselling of the parents regarding the management options including continuation of pregnancy with post-natal surgery termination of pregnancy or selective fetocide in case of a triplet pregnancy With the introduction of high-resolution and transvaginal ultrasound imaging accurate prenatal diagnosis of conjoined twins is possible early in pregnancy Although first-trimester diagnosis of conjoined twins is feasible false-positive cases are common before 10 weeks because earlier in gestation fetal movements are limited and monoamniotic twins may appear conjoined As most parents opt for immediate termination of pregnancy at confirmation of the diagnosis there are limited data on the prenatal follow-up of conjoined twins detailed analysis of case reports where 3D imaging was used indicates that this modality does not improve on the diagnosis made by 2D ultrasound Overall very early prenatal diagnosis and first-trimester 3D imaging provide very little additional practical medical information compared to the 11-14 weeks ultrasound examination
Images of the conjoined twins there are two heads with conjoined body
Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You

Subchorionic hemorrhage
Conjoined twins are a rare and complex complication of
monozygotic twinning which is associated with high perinatal mortality Early prenatal diagnosis of conjoined twins allows better counselling of the parents regarding the management options including continuation of pregnancy with post-natal surgery termination of pregnancy or selective fetocide in case of a triplet pregnancy With the introduction of high-resolution and transvaginal ultrasound imaging accurate prenatal diagnosis of conjoined twins is possible early in pregnancy Although first-trimester diagnosis of conjoined twins is feasible false-positive cases are common before 10 weeks because earlier in gestation fetal movements are limited and monoamniotic twins may appear conjoined As most parents opt for immediate termination of pregnancy at confirmation of the diagnosis there are limited data on the prenatal follow-up of conjoined twins detailed analysis of case reports where 3D imaging was used indicates that this modality does not improve on the diagnosis made by 2D ultrasound Overall very early prenatal diagnosis and first-trimester 3D imaging provide very little additional practical medical information compared to the 11-14 weeks ultrasound examination
Images of the conjoined twins there are two heads with conjoined body
Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You
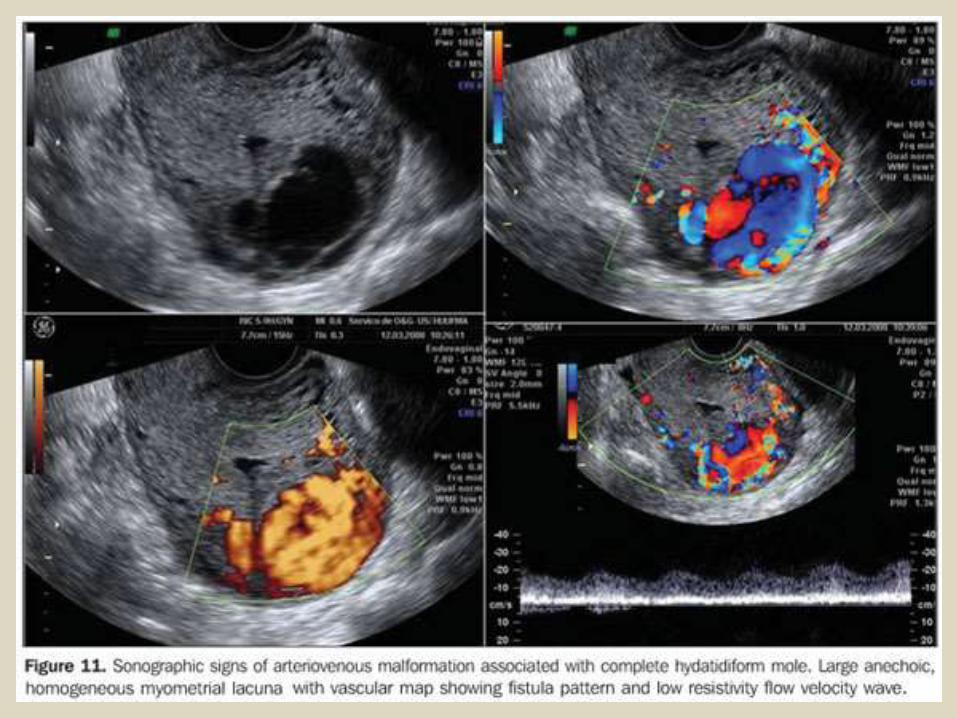
Conjoined twins are a rare and complex complication of
monozygotic twinning which is associated with high perinatal mortality Early prenatal diagnosis of conjoined twins allows better counselling of the parents regarding the management options including continuation of pregnancy with post-natal surgery termination of pregnancy or selective fetocide in case of a triplet pregnancy With the introduction of high-resolution and transvaginal ultrasound imaging accurate prenatal diagnosis of conjoined twins is possible early in pregnancy Although first-trimester diagnosis of conjoined twins is feasible false-positive cases are common before 10 weeks because earlier in gestation fetal movements are limited and monoamniotic twins may appear conjoined As most parents opt for immediate termination of pregnancy at confirmation of the diagnosis there are limited data on the prenatal follow-up of conjoined twins detailed analysis of case reports where 3D imaging was used indicates that this modality does not improve on the diagnosis made by 2D ultrasound Overall very early prenatal diagnosis and first-trimester 3D imaging provide very little additional practical medical information compared to the 11-14 weeks ultrasound examination
Images of the conjoined twins there are two heads with conjoined body
Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You

Images of the conjoined twins there are two heads with conjoined body
Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You

Images of the conjoined twins
Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You

Conjoined twins Ultrasound images of fetuses joined at the pelvis and chest with separate heads
Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You

Three-dimensional sonogram showing the conjoined twins of the thoraco-omphalopagus type
First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You

First Trimester BleedingMiscarriage Molar ChangesMiscarriage is defined as the loss of a pregnancy prior to the completion of 24 weeks gestation and the main maternal symptoms are bleeding and pain If a fetal HR has been detected the risk of spontaneous miscarriage in singletons is 122
Threatened Pregnancy Failure
Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You

Threatened Pregnancy Failure
An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You

An incomplete miscarriage
CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You

CONCLUSIONFirst trimester obstetric abnormalities are identified by screening studies or in cases of abnormal vaginal bleeding with the objective of determining the gestation viability Transvaginal ultrasonography is the method of choice in the evaluation of first trimester pregnancy In the presence of vaginal bleeding this method is highly specific in the determination of the conceptus viability most of times clearly defining the etiological process involved in the clinical condition The knowledge of the sonographic findings that characterize each condition is essential for determining an appropriate clinical approach in these cases
Thank You

Thank You

![Presentation1.pptx [repaired]](https://static.fdocuments.in/doc/165x107/58a9e64c1a28ab36018b4839/presentation1pptx-repaired-58ac0f71a4da9.jpg)





![Presentation1[1].pptx manoj](https://static.fdocuments.in/doc/165x107/577d26051a28ab4e1ea0162b/presentation11pptx-manoj.jpg)