Presentation Packet - Munson Medical Center · · 2017-11-03• This Live activity,...
94
‘ Presentation Packet
-
Upload
vuongkhanh -
Category
Documents
-
view
219 -
download
3
Transcript of Presentation Packet - Munson Medical Center · · 2017-11-03• This Live activity,...

‘
Presentation
Packet

1
5th Annual Cardiology Update for the Primary Care ProviderNovember 4 2017
20 Cardiologists:10 interventionalists11 imaging experts3 electrophysiologists1 advanced HF
5 Cardiac Surgeons8 Inpatient cardiac APP4 Out pt general card APP2 EP specialty APP116 support staff
High volume cardiac center
• Over 50, 000 patient encounters• 22,878 CV ultrasound procedures• 35,750 provider visits• 378 PAD interventions• 2,492 nuclear studies• 4,053 cardiac cath and PCI procedures• 16,514 device checks• 1,225 pacemakers and ICDs• 380 EP & ablation procedures
2
CME Information
• CME Providers are required to announce faculty and planning committee disclosures prior to any accredited CME activity.
• All of the faculty and planners for this conference report that they have no relevant financial relationships to disclose in the context of the activity.
CME Information
• In order to claim CME credit and get your certificate, please complete the initial electronic SurveyMonkey evaluation. At the end of the evaluation, you will be linked to your CME Certificate of Attendance for downloading and printing.
• The evaluation link is available within our Conference App and will also be emailed to you.
• DO Physicians and AAFP Members, additional post‐activity credit opportunities are available to you. More information will be emailed to you in about 2 weeks.
CME Credits ‐MD
• Munson Medical Center is accredited by the Michigan State Medical Society to provide continuing medical education for physicians.
• Munson Medical Center designates this live activity for a maximum of 6 AMA PRA Category 1 Credit(s)™.Physicians should claim only the credit commensurate with the extent of their participation in the activity.
• To claim credits and receive a Certificate of Attendance, please complete the SurveyMonkeyEvaluation.
3
CME Credits ‐ DO
• Munson Medical Center is accredited by the American Osteopathic Association to provide osteopathic continuing medical education for physicians.
• Munson Medical Center designates this program for a maximum of 6 AOA Category 1‐A Credits and will report CME and specialty credits commensurate with the extent of the physician's participation in this activity.
• To claim credits and receive a Certificate of Attendance, please complete the SurveyMonkey Evaluation.
• An additional 1 AOA Category 1‐A Credit will be awarded to those DO physicians who successfully complete an outcomes evaluation. This special evaluation will be send via email in about two weeks.
CME Credits – AAFP Family Phys.
• This Live activity, Cardiovascular Update for Primary Care Providers, with a beginning date of 11/05/2016, has been reviewed and is acceptable for up to 6.00 Prescribed credits by the American Academy of Family Physicians. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
• To claim credits and receive a Certificate of Attendance, please complete the SurveyMonkey Evaluation.
• An additional 2 AAFP Prescribed Credits will be awarded to those AAFP members who participate in the post‐conference Translation to Practice® exercise. Additional information about this exercise will be emailed in about 2 weeks.
CME Credits – Non‐physicians
• Non‐physician professionals should check with their individual credentialing body to confirm that participation in this CME activity will be recognized for credit.
• Physician Assistants and Nurse Practitioners are eligible to use AMA PRA Category 1 accredited activities toward their certification(s) and/or licensure(s).
• CME Credits can be used to meet the continuing education requirements for Michigan nursing re‐licensure without limitation.

4
Communication & Questions
• www.munsonhealthcare.org/cvupdateapp
Thank You
• Planning committee
‒ Todd Adams‒ Kara Classens‒ Thom Harris‒ Amy Hoge‒ Ian Jones‒ Valerie Schollett‒ Michelle Stawski‒ Mary Tripod
‘
Heart Failure: Preserved Ejection Fraction
Dino Recchia, MD, FACC
Notes:
1
Primary Care Atrial Fibrillation Update:Anticoagulation and Left Atrial Appendage OcclusionGreg Francisco, MD, FACC
DISCLOSURES
• None to declare
2
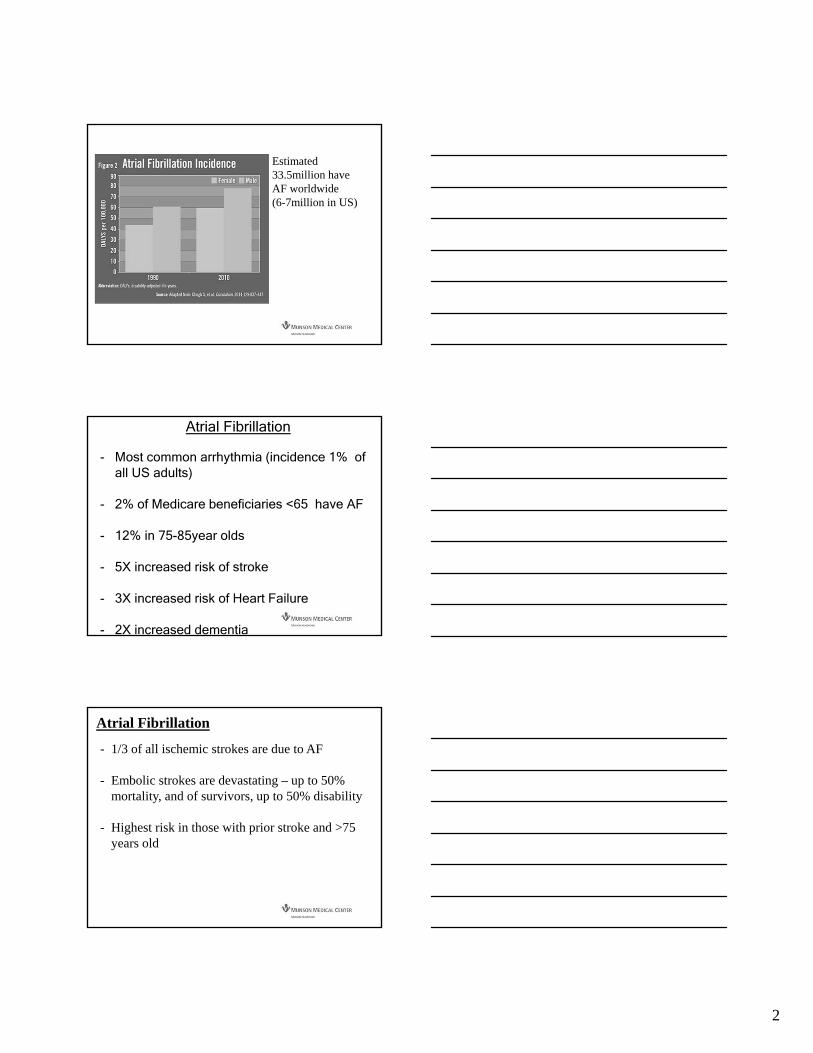
Estimated 33.5million have AF worldwide (6-7million in US)
Atrial Fibrillation
- Most common arrhythmia (incidence 1% of all US adults)
- 2% of Medicare beneficiaries <65 have AF
- 12% in 75-85year olds
- 5X increased risk of stroke
- 3X increased risk of Heart Failure
- 2X increased dementia
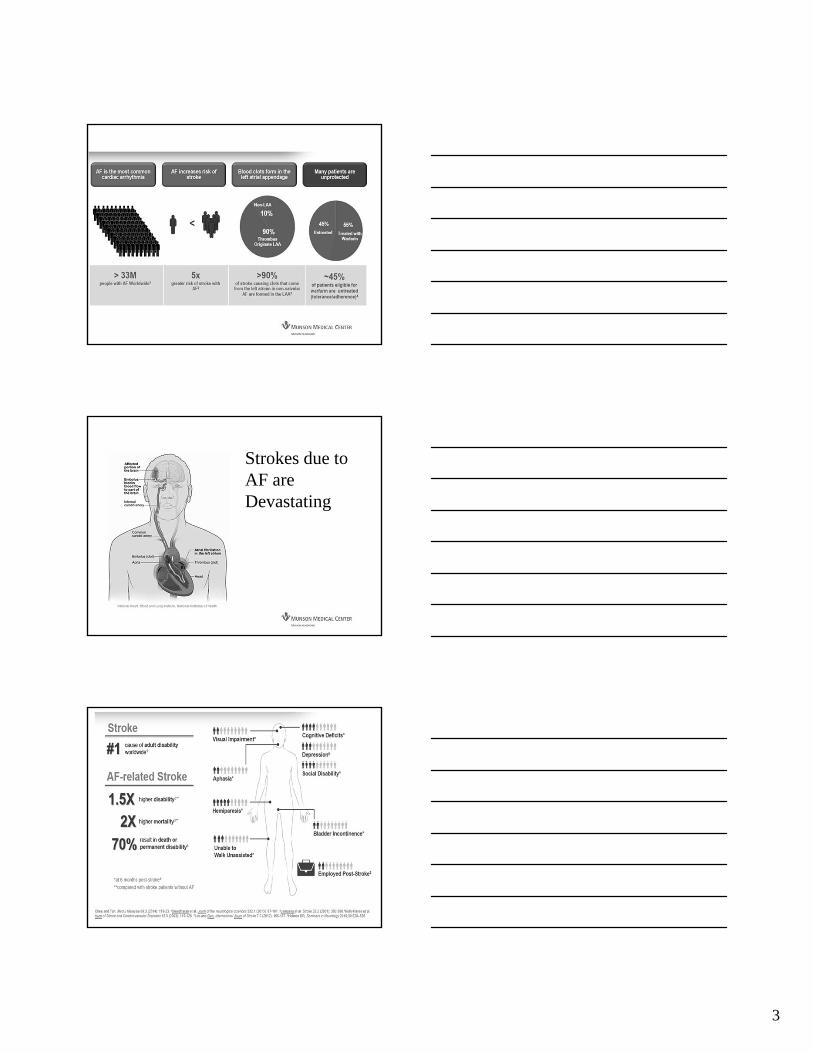
- 1/3 of all ischemic strokes are due to AF
- Embolic strokes are devastating – up to 50% mortality, and of survivors, up to 50% disability
- Highest risk in those with prior stroke and >75 years old
Atrial Fibrillation
3
Strokes due to AF are Devastating
4
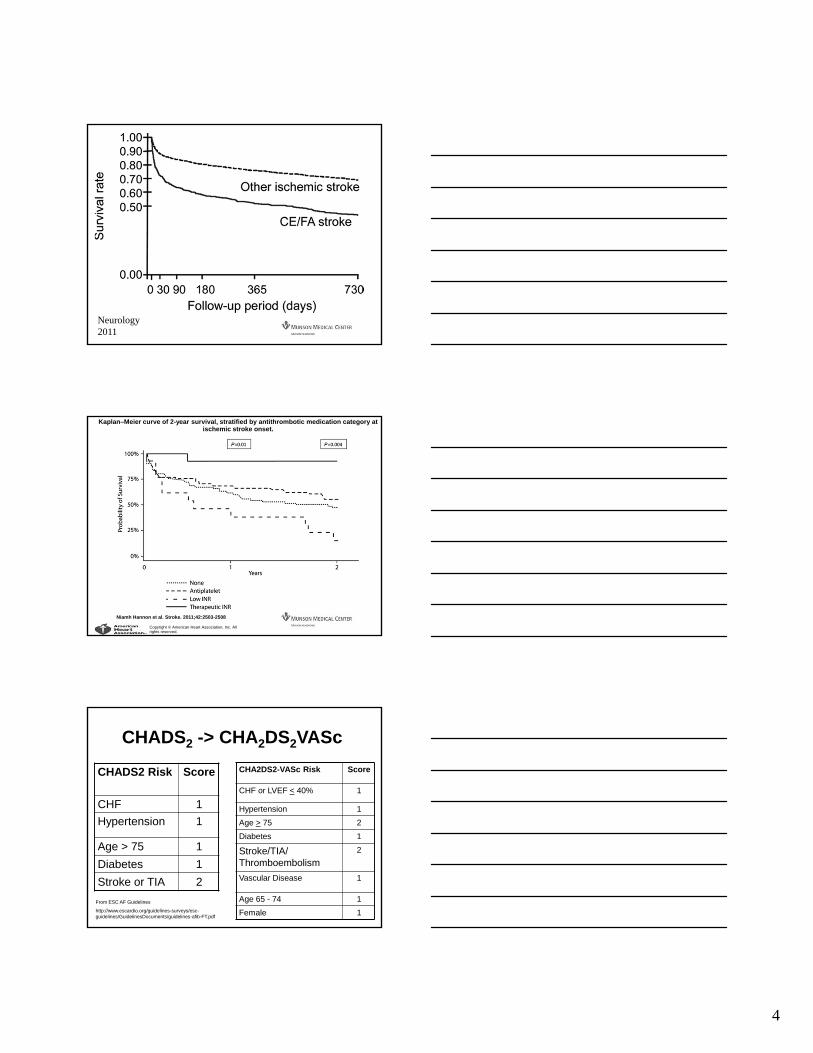
Neurology 2011
Kaplan–Meier curve of 2-year survival, stratified by antithrombotic medication category at ischemic stroke onset.
Niamh Hannon et al. Stroke. 2011;42:2503-2508
Copyright © American Heart Association, Inc. All rights reserved.
CHADS2 -> CHA2DS2VASc
CHA2DS2-VASc Risk Score
CHF or LVEF < 40% 1
Hypertension 1
Age > 75 2
Diabetes 1
Stroke/TIA/ Thromboembolism
2
Vascular Disease 1
Age 65 - 74 1
Female 1
CHADS2 Risk Score
CHF 1
Hypertension 1
Age > 75 1
Diabetes 1
Stroke or TIA 2
From ESC AF Guidelines
http://www.escardio.org/guidelines-surveys/esc-guidelines/GuidelinesDocuments/guidelines-afib-FT.pdf

5
Swedish Study Using a Wide stroke definition140,420 patients
CHADS2vasc = 1 0.5-0.7%/yr for men0.1-0.2%/yr for women
Friberg, JACC 2015
What about Bleeding Risk?

6
HAS BLED
The higher HAS BLED Score, the higher Stroke Risk, too.

7
Warfarin can be Challenging
Dabigatran1 Rivaroxaban2 Apixaban3
Comparator Warfarin Warfarin Warfarin
Total Enrolled Subjects 18,113 14,264 18,201
Trial Design
Randomized, controlled, non-
inferiority (doses of
dabigatran were blinded)
Randomized, controlled, double-blind, non-inferiority
Randomized,controlled, double-blind, non-inferiority
Median Duration of Follow up
2 years 1.94 years 1.8 years
Average CHADS2 Score 2.1 3.5 2.1
Results (primary outcome = stroke or systemic embolism)
Reduction in primary outcomecompared to warfarin
Reduction in primary outcome compared to warfarin
Reduction in primary outcome compared to warfarin

8
TreatmentStudy Drug
Discontinuation RateMajor Bleeding
(rate/year)
Rivaroxaban1 24% 3.6%
Apixaban2 25% 2.1%
Dabigatran3
(150 mg)21% 3.3%
Edoxaban4
(60 mg / 30 mg)33 % / 34% 2.8% / 1.6%
Warfarin1-4 17 – 28% 3.1 – 3.6%
Relatively High Discontinuation Rates with DOACs
Left Atrial Appendage Occlusion:
Watchman Lariat
Atriclip
9
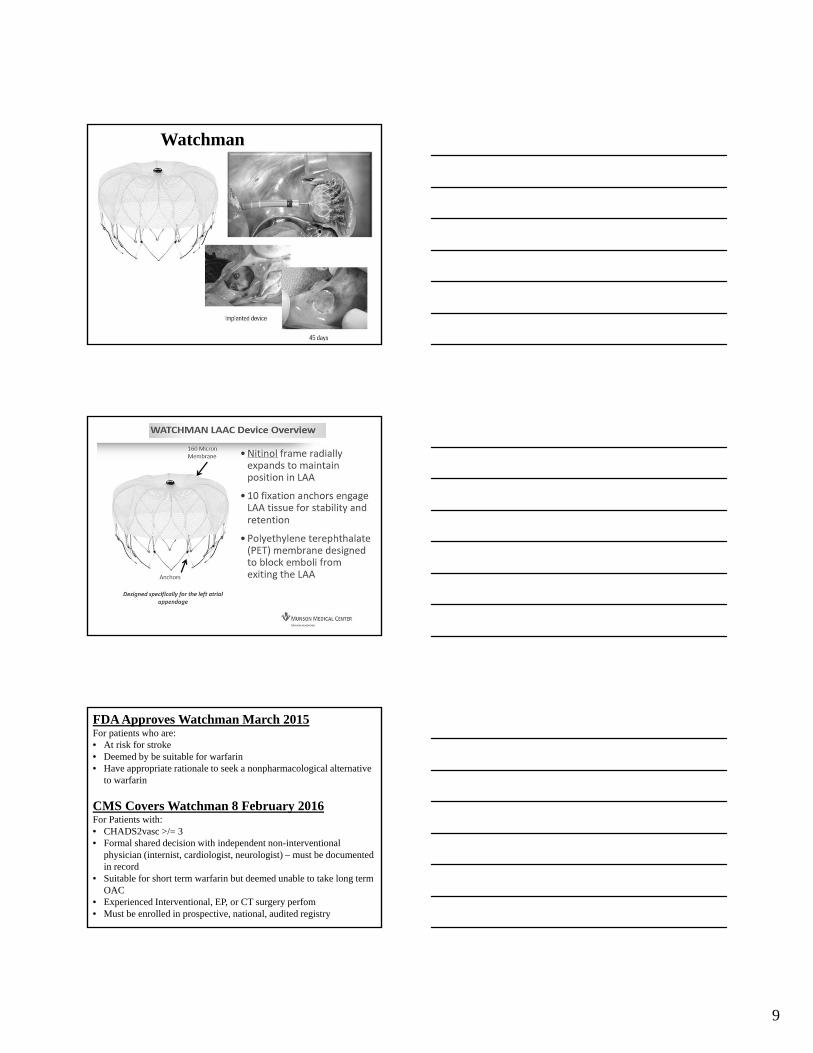
Watchman
FDA Approves Watchman March 2015For patients who are:• At risk for stroke• Deemed by be suitable for warfarin• Have appropriate rationale to seek a nonpharmacological alternative
to warfarin
CMS Covers Watchman 8 February 2016For Patients with:• CHADS2vasc >/= 3• Formal shared decision with independent non-interventional
physician (internist, cardiologist, neurologist) – must be documented in record
• Suitable for short term warfarin but deemed unable to take long term OAC
• Experienced Interventional, EP, or CT surgery perfom • Must be enrolled in prospective, national, audited registry

10
PROTECT AF
CAPRegistry
PREVAIL CAP2Registry Totals
Enrollment 2005-2008 2008-2010 2010-2012 2012-2014
Enrolled 800 566 461 579 2406
Randomized 707 --- 407 --- 1114
WATCHMAN: warfarin (2:1)
463 : 244 566 269 :138 5791877: 382
Mean Follow-up (years)
4.0 3.7 2.2 0.58 N/A
Patient-years 2717 2022 860 332 5931
Warfarin Cessation
Study 45-day 12-month
PROTECT AF 87% >93%
CAP 96% >96%
PREVAIL 92% >99%
PREVAIL Implant Success
No difference between new and experienced operators
Experienced Operators• n=26• 96%
New Operators• n=24• 93%

11
Boersma et al. Heart Rhythm Journal 2017
EWOLUTION: 1 year Real-World Follow-up

12
EWOLUTION: 1 year Real-World Follow-up
Boersma et al. Heart Rhythm Journal 2017
EWOLUTION: 1 year Real-World Follow-up
Boersma et al. Heart Rhythm Journal 2017
Cannot take antiocoagulation
Should not take anticoagulation
Will not take anticoagulation
Recurrent GI Bleeders Dialysis patients Patients living in remote locale
History of Intracranial Bleeding
Stents requiring longtermDAPT
Active lifestyle?
Frequent falls? High HASBLED score? Patient choice?
So who should get a Watchman?

13
Watchman Protocol
1. Watchman performed – general anesthesia; 1 hour procedure2. 1-2 day hospitalization3. 6 weeks anticoagulation 4. 6 week TEE – if no thrombus on atrial side of device and no
leak, then stop anticoagulation5. 4 1/2 months dual antiplatelet therapy (may forego if high
bleeding risk)6. Lifetime baby aspirin if possible7. TEE at 1 year
CASE STUDY:-EV is an 88 year old woman who suffered a stroke and was found to have paroxysmal AF -apixiban was started-Subdural hematoma after a fall 6 months later. Apixiban stopped-Neurosurgeon states that anticoagulation is safe for the short-term, but not preferable for longterm therapy-Watchman was recommended
14
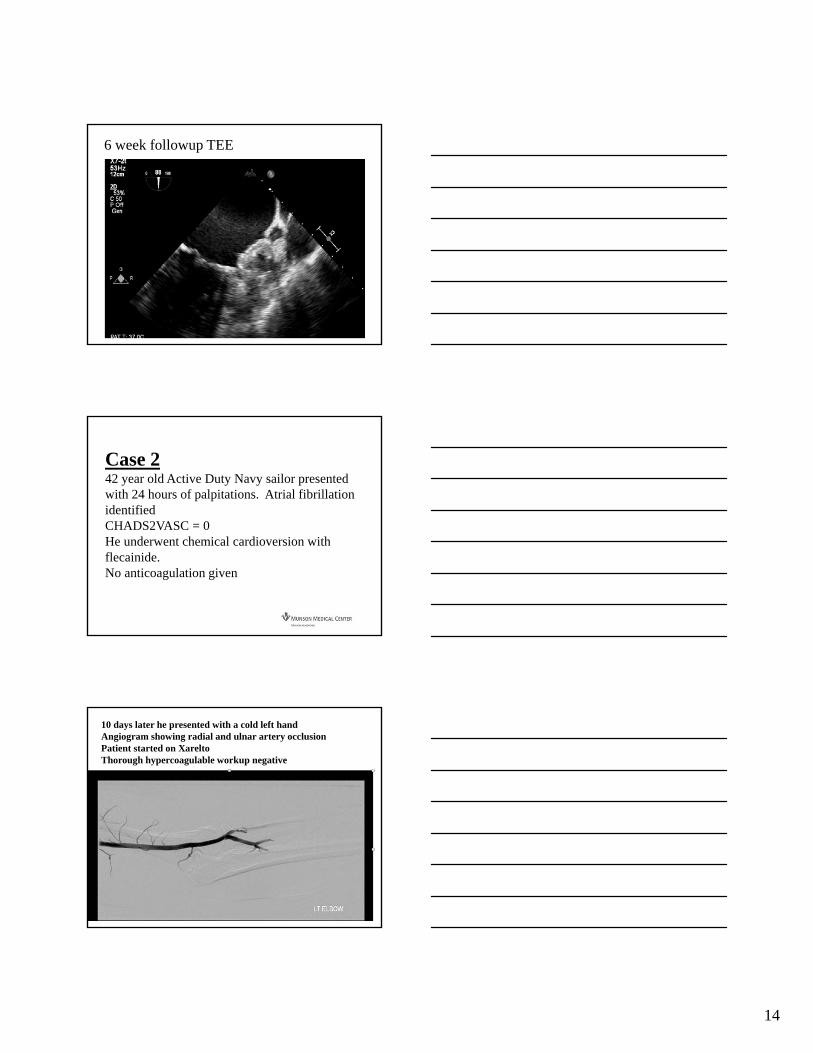
6 week followup TEE
Case 242 year old Active Duty Navy sailor presented with 24 hours of palpitations. Atrial fibrillation identifiedCHADS2VASC = 0He underwent chemical cardioversion with flecainide. No anticoagulation given
10 days later he presented with a cold left handAngiogram showing radial and ulnar artery occlusionPatient started on Xarelto Thorough hypercoagulable workup negative

15
2 years later, on anticoagulation, he awoke with severe flank pain –he was found to have infarcted his right kidney
Watchman recommended for breakthrough embolism on therapy and questions of compliance
Thank you
QUESTIONS?

‘
Heart Failure: Decreased LVEF
Dino Recchia, MD, FACC
Notes:

1
Cholesterol targets and therapyThomas C. Andrews, MD, FACC
2
Still first line therapy!
Statins in secondary prevention
3
• First line therapy: high intensity statin‒ Dose individualized based on baseline LDL‒ Atorvastatin 40 or 80‒ Rosuvastatin 20 or 40
• Second line therapies‒ Statin intolerant or not near goal of LDL <70 mg/dl‒ Ezetimibe plus statin‒ PCSK9 inhibitors
• Monitoring‒ Lipid panel at baseline and 6 weeks post med change‒ Annual (or perhaps semiannual) lipid panels
• assess compliance!

2
Patient one‐liners
Statin intolerance
4
• “I am allergic to all statins”• “When I took that drug, I couldn’t get out of bed”• “Statins are bad for you”• “My memory is bad enough”• “I don’t want to get diabetes”
Are clinicians developing statin‐intolerance tolerance?
Relative risk reduction after MI
5
All cause mortality
46
2421
0
5
10
15
20
25
30
35
40
45
50
Secondary prevention
% mortality reduction
Smoking cessation
Beta blocker
Statin treatment
Myth or reality?
Statin side effects
6
• Hepatitis• Diabetes• Cognitive dysfunction• Renal failure• Peripheral neuropathy• Muscle symptoms

3
ALT>3x ULM/100,000 person‐years
Statin associated hepatitis
7
Treatment Placebo Net risk
Single measure 300 200 100 cases
2 consecutivemeasures
110 40 70 cases
Statins and diabetes
8Sattar N et al, Lancet 2010
Clinical trial data
Statin Odds ratio (95% CI)
Any statin (n=91 140) 1.09 (1.02–1.17)
Atorvastatin (n=7773) 1.14 (0.89–1.46)
Simvastatin (n=18 815) 1.11 (0.97–1.26)
Rosuvastatin (n=24 714) 1.18 (1.04–1.33)
Pravastatin (n=33 627) 1.03 (0.90–1.19)
Lovastatin (n=6211) 0.98 (0.70–1.38)
NNH to causes 1 case of DM: 250NNT to prevent 1 episode of ACS: 25
Statins and renal failure
9
Treatment N Creatinine% Change
Change inGFR
Placebo 371 0.8 -0.3
Rosuvastatin 5 mg10 mg20 mg40 mg
637290914322107
-1.6 -1.4 -1.6 -1.3
1.5 1.6 1.9 1.6
Atorvastatin 10 mg20 mg40 mg80 mg
13941562
221535
-1.5 -1.4 -2.0 -3.8
1.6 1.5 1.9 3.4
Simvastatin 10 mg20 mg40 mg80 mg
1611217
506500
-0.4 -1.4 -1.6 -1.2
0.5 1.4 1.7 1.5
Pravastatin 10 mg20 mg40 mg
159342745
-1.8 -2.1 -0.7
1.81.9 0.8

4
Statin associated peripheral neuropathy
10
Cohort studies
0 1 2 3 4
Anderson JL et al. Am J Cardiol. 2005;95:1097-1099
Corrao G et al. J Epidemiol Community Health. 2004;58:1047-1051
Gaist D et al. Neurology. 2002;58:1333-1337
Gaist D et al. Eur J Clin Pharmacol. 2001;56:931-933
ALL COHORT STUDIES1.8 (1.1-3.4)
5Odds Ratio
12 cases per 100,000 person years
Statins and cognitive function
11Etminan et al. Pharmacotherapy. 2003;23:726‐730
Observational studies
0 1
Hajjar I et al. J Gerontol A Biol Sci Med Sci. 2002;57:408-414
Green RC et al. Neurobiol Aging. 2002;23:S273-S274
Jick H et al. Lancet. 2000;356:1627-1631
Rockwood K et al. Arch Neurol. 2002;59:223-227
ALL COHORT STUDIES
Rodriquez EG et al. J Am Geriatr Soc. 2002;50:1852-1856
Wolozin B et al. Arch Neurol. 2000;57:1439-1443
Yaffe K et al. Arch Neurol. 2002;59:378-384
0.43 (0.31-0.62)
2
Neuropsychiatric testing in heart protection study (simavastatin)
Statins and dementia
12
Measure Simvastatin Placebo
Cognitive impairment 23.7% 24.2%
Dementia 0.3% 0.3%
Psychiatric disorder 0.7% 0.7%
Suicide 0.1% 0.1%

5
Clinical Spectrum
Statin Associated Myopathy
13
• Myalgia‒ Common: 10‐20%‒ Musculoskeletal symptoms with normal CK
• Myositis‒ Uncommon: <1%‒ Musculoskeletal symptoms, CK<3x ULN
• Myopathy‒ Rare: <0.01%‒ Musculoskeletal symptoms, CK 3‐10x ULN
• Rhabdomyolysis‒ 1 per 1 million prescriptions‒ Musculoskeletal symptoms, CK>10x ULN
Management
Statin myopathy
14
• Assess for drug interactions ‒ Most common with lovastatin & simvastatin (P‐450 3A4)
• Grapefruit juice >8 oz/day
• Amlodipine, Amiodarone, others
‒ Fenofibrate instead of gemfibrozil‒ Watch protease inhibitors, cyclosporine
• Assess for Vit D deficiency and hypothyroidism• Consider dose reduction/trial of pravastatin• Consider alternate day dosing
‒ Pravastatin QOD‒ Atorvastatin or rosuvastatin weekly‒ No outcomes data!
Proprotein convertase subtilisin/kexin type 9
PCSK9 inhibitors
15
• Alirocumab (Praluent) and evolocumab (Repatha)—monoclonal antibodies‒ Lower LDL by 60%‒ Reduce Lp(a) up to 36%‒ Regression of plaque volume‒ Prevention of MI and stroke‒ Probable reduction in mortality (meta‐analysis)
• Administration‒ subQ 1‐2 times a month
• Side effects (no muscle toxicity!)‒ Hypersensitivity and site reactions‒ GI (diarrhea)‒ Neurocognitive decline?

6
Summary
Statins in clinical practice
16
• An important part of our armamentarium‒ Serious side effects uncommon‒ “Intolerance” common
• Start with a high intensity statin and modify based on subsequent on‐treatment LDL levels‒ ?Add zetia‒ ?Role of PCSK9 inhibitors
• PCSK9 inhibitors provide an alternative‒ Expensive!‒ Emerging long term outcomes data

1
Beta Blockers In Stable Ischemic Heart DiseaseShould they be continued indefinitely?Benjamin Ebner, MD FACC
Beta Blocker (Brief) Pharmacology Review
2
Adrenergic System
3
• Norepinephrine/Epinephrine from adrenals and nervous system
α2-feedback inhibition
β1- CO
α1-Vasoconstriction
β2-Vasodilation
Bronchodilation

2
Common Beta Blockers
*also produced endothelial dependent vasodilation by enhancing NO release
4
• β1, β2 and α‒ Labetalol‒ Carvedilol
• β1, β2‒ Propranolol‒ Nadolol
• β1 Selective‒ Metoprolol‒ Atenolol‒ Bisoprolol‒ Nebivilol*
• Partial Agonists‒ Pindolol and acebutolol
• Decrease Cardiac Oxygen Use (β1)‒ Heart Rate‒ Contractility‒ Conduction Velocity‒ Relaxation Rate
• Lowers Blood Pressure ‒ ↓ cardiac output‒ ↓ renin release‒ Reflex vasoconstriction
• Unopposed α
Beta Blocker Pharmacology
5
Intolerances of BB
6
• Non‐selective Beta Blockers‒ Bronchoconstriction‒ Claudication
• Fatigue/CNS depression with highly lipophilic‒ Metoprolol/propranolol

3
Clinical Uses of Beta Blockers – A Jack of All Trades
7
• Angina• Heart Failure• Hypertension• Arrhythmia
‒ Atrial and ventricular
• Also‒ HCM‒ Mitral Stenosis‒ Esophageal Varices‒ Migraine‒ Glaucoma‒ Tremor
Beta Blockers for Angina Relief
8
• Decrease Myocardial Oxygen Consumption‒ O2 Supply = O2 Demand
• Multiple RCTs‒ reduce angina frequency‒ time to ischemia ‒ improve exercise capacity
• First Line Treatment of Stable Angina (Class I)
1 receptors 2 receptors
Myocyte hypertrophy and death, dilation, ischemia and arrhythmia
1 receptors
Cardiacsympathetic activity
Sympatheticactivity to kidneys
& blood vessels
CNS sympatheticoutflow
BB in Heart Failure‐Mechanism of Benefit
Adapted from Packer, AHA 2000
VasoconstrictionSodium retention

4
Beta Blockers in Heart Failure
10
• Beta Blockers Improve Survival when LVEF <40%‒ Metoprolol Succinate‒ Bisoprolol‒ Carvedilol
Weak data informing BB in Heart Failure when LVEF >40%
OPTIMIZE HF Registry 11
EF <40 EF >40
HFpEF – 2017 BMJ Meta‐Analysis
12
Beta Blockers only class to improve all cause mortality in Heart Failure with LVEF >40%
3 RCTs- Propranolol, Carvedilol or Nebivilol vs Placebo

5
• 2009 meta‐analysis of 958,000 patients and 108 Trials• BP reduction is important – not the agent
Beta Blockers in Hypertension
13
Beta Blockers After Acute Coronary SyndromeA Story Evolving with the Advent of Reperfusion Therapy
14
Beta Blockers In Pre‐Reperfusion Era
15
• Consistent mortality advantage across many subgroups with AMI
Propranolol vs Placebo in medically managed ACS

6
16
CAPRICORN: Carvedilol After MI with LVEF <40%
• <50% Received Reperfusion
17
• Observational Data‒ Supports use of BB
after MI and Reperfusion
‒ Especially with low EF or Multivessel CAD
Beta Blockers After STEMI In PCI vs Lytic Trial
How Long After AMI should Beta Blockers be Continued?
18

7
Guidelines for BB use in Stable Ischemic Heart Disease
19
• BB prescribed for 3 years post ACS
Class I
*2012 ACC Guidelines on stable ischemic heart disease
• Considered as chronic therapy for other patients with cardiac or vascular disease
Class IIb
Pleiotropic Effect- BB Only Advantage in Recent MI
20
2009 BMJ Meta-analysis of RCTs of Antihypertensives
21
• Observational data of 26,793 started on BB after NSTEMI/STEMI vs Non‐ACS revascularization‒ 3.7 years of follow up
• BB improve outcomes in those with MI‒ Neutral effect without MI
Why Three Years After ACS?

8
Guidelines for BB use in Stable Ischemic Heart Disease
22
• BB prescribed for 3 years post ACS
Class I
*2012 ACC Guidelines on stable ischemic heart disease
• Considered as chronic therapy for other patients with cardiac or vascular disease
Class IIb
Controversial Recommendation For BB In All Patients with CVD
23
• Little data to recommend beta blockers for SIHD‒ LVEF >40%‒ No Recent ACS (>3 years)‒ No Angina
• Represents a very large number of patients‒ Potentially unnecessary prescriptions‒ Exposure to side effects‒ Contributes to pill burden and polypharmacy
24
• REACH Registry Data: No Benefit of Beta Blocker Use in SIHD‒ Observational Data with
propensity matching
Beta Blockers in SIHD ‐ REACH

9
25
Beta Blockers in SIHD – NCDR Data
Registry of >750,000 Medicare Patients• Elective PCI for SIHD• No prior MI• LVEF >40%
Beta blocker • no benefit • more incident HF
Conclusions
26
• Definitely Continue Beta Blockers If‒ LVEF <40%
• Possibly with
‒ LVEF 40‐50%
‒ Normal LVEF and Heart Failure History
‒ < 3 Years Post MI
• Consider stopping if no compelling indication‒ Taper off
Thank You

10
Definition:Stable Ischemic Heart Disease
28
• Obstructive coronary disease‒ Patients with stable angina, silent ischemia or prior
revascularization‒ Normal or abnormal ejection fraction‒ Not patients with recent acute coronary syndrome
• STEMI/NSTEMI/Unstable Angina
1
Venous Disease: More than a cosmetic problem?Andrew Teklinski, MD, MS, FACC
2
Lower Extremity Venous Anatomy
3

2
Perforators
4
Reticular Vein Anatomy
5
Perforators
6
3
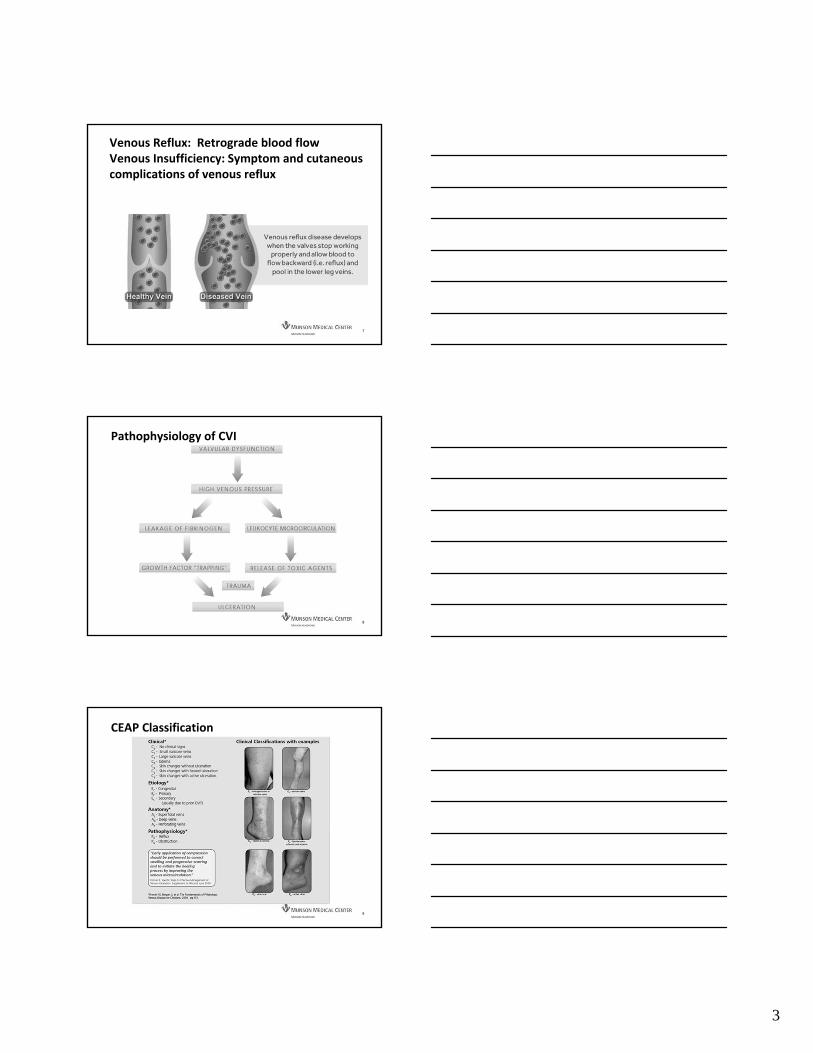
Venous Reflux: Retrograde blood flowVenous Insufficiency: Symptom and cutaneous complications of venous reflux
7
Pathophysiology of CVI
8
CEAP Classification
9
4
10
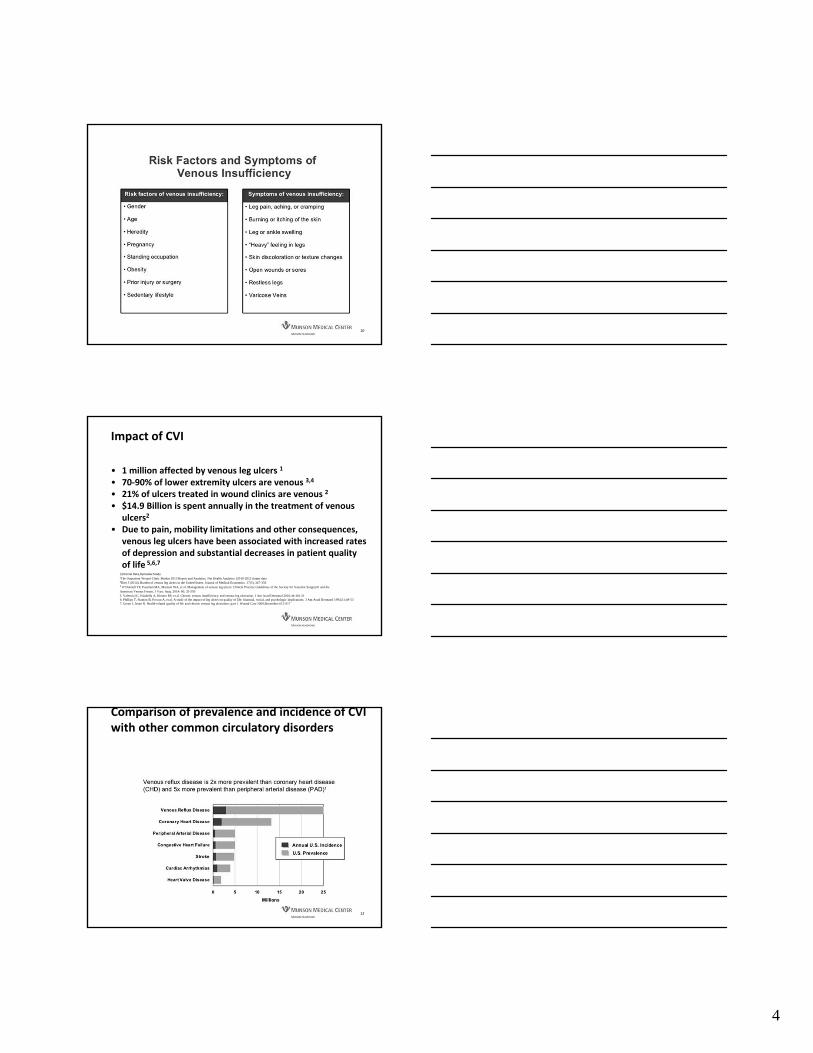
Impact of CVI
• 1 million affected by venous leg ulcers 1
• 70‐90% of lower extremity ulcers are venous 3,4
• 21% of ulcers treated in wound clinics are venous 2
• $14.9 Billion is spent annually in the treatment of venous ulcers2
• Due to pain, mobility limitations and other consequences, venous leg ulcers have been associated with increased rates of depression and substantial decreases in patient quality of life 5,6,7
1Internal Data,Dymedex Study
²The Outpatient Wound Clinic Market 2013 Report and Analytics, Net Health Analytics (2010-2012 claims data³Rice J (2014). Burden of venous leg ulcers in the United States. Journal of Medical Economics. 17(5), 347-356⁴ O’Donnell TF, Passman MA, Marston WA, et al. Management of venous leg ulcers: Clinical Practice Guidelines of the Society for Vascular Surgery® and theAmerican Venous Forum. J Vasc. Surg. 2014: 60; 35-5955. Valencia IC, Falabella A, Kirsner RS, et al. Chronic venous insufficiency and venous leg ulceration. J Am Acad Dermatol 2001;44:401-216. Phillips T, Stanton B, Provan A, et al. A study of the impact of leg ulcers on quality of life: financial, social, and psychologic implications. J Am Acad Dermatol 1994;31:49-537. Green J, Jester R. Health-related quality of life and chronic venous leg ulceration: part 1. Wound Care 2009;December:S12-S17
Comparison of prevalence and incidence of CVI with other common circulatory disorders
12

5
CVI Treatment Data
13
Venous insufficiency exam is an anatomic and functional study. Not the same as a venous ultrasound, which is mostly anatomic
Diagnostics: Ultrasound
14
Venous Duplex is the main stay of diagnosis Duplex is utilized to – Make the diagnosis– Identify level of disease– Identify segments of disease– Identify the pathophysiology– Rule out DVT/SVT– Guide therapy for superficial venous reflux – Provide post‐procedure follow up
Useful for reticular vein examination
Vein Light
15

6
Ablation: Useful for long, straight segments
Treatment Modalities
16
Thermal ablation
17
Phlebectomy: Useful for symptomatic varicose veins
Treatment Modalities
18

7
Treatment Modalities
19
Sclerotherapy: Useful for reticular veins and tortuous superficial veins
2020
Response of ulcers to ablation
30
20
10
0-100-80 -60 -40 -20 0 20 40 60 80 100
Vein Ablation
Percent treatment timeBEFORE ablation
Percent treatment timeAFTER ablation
Ulc
er s
ize
(cm
2 )
.
1 Howard M. Kimmel et al. An Evidence-Based Algorithm for Treating Venous Leg Ulcers Utilizing the Cochrane Database of Systematic Reviews. WOUNDS 2013;25(9):242-250
GSV- Great saphenous veinSSV- Small saphenous veinPTPV- Posterior tibial perforator veinAll veins
Ablation method used was radiofrequency ablation
2121
Results of Perforator Ablation
8
2222
Benefits of evidence & guidelines based care¹
• Venous leg ulcer outcomes are optimized when patients receive multidisciplinary care and evidence-based wound management.
• Dermatology, geriatrics, podiatry, and surgery are just a few specialties that may be utilized to improve outcomes.¹
• Significant decreases in healing time and costs are associated with guideline adherence.
• Among veterans with VLUs, those who receive guideline-concordant wound care are 2.5 times more likely to achieve wound healing than are those who receive non-concordant care.¹
¹ Howard M. Kimmel et al. An Evidence-Based Algorithm for Treating Venous Leg Ulcers Utilizing the Cochrane Database of Systematic Reviews. WOUNDS 2013;25(9):242-250
Summary
23
• CVI is a common, yet often overlooked disease
• Significant financial burden to the healthcare system
• Negatively affects quality of life and may result in disability and need for chronic medical care
• Multidisciplinary treatment is effective in relieving the symptoms and managing the complications of CVI
• Venous disease is more than cosmetic
‘
Orthostatic Hypotension
James Fox, MD, FACC
Notes:

11/2/2017
1
CONGENITAL HEART CENTER
Bicuspid Aortic ValveMore Than Two Sides to the Story
Mark Norris MD, MS
CONGENITAL HEART CENTER
2
Bicuspid Aortic Valve and Associated Conditions
• No disclosures• Any discussion of off label medication use will be highlighted
Adult Congenital Heart Program•2 ACHD cardiologists•1 ACHD fellow•2 NP providers•2 RN team members
CONGENITAL HEART CENTER
CONGENITAL HEART CENTER
3
CONGENITAL HEART CENTER
• Few health conditions affect ½-1% of the population
• Put another way of all fans attending the MSU vs. U of Michigan game this year (112,432):
• About 11,000 have a bicuspid valve or associated aortopathy
• About 80,000 went home wet and sad
Bicuspid Aortic Valve

11/2/2017
2
CONGENITAL HEART CENTER
4
CONGENITAL HEART CENTER
• Two functional aortic valve leaflets
• Fusion of two leaflets or appearance of two smooth leaflets
– Right / Left coronary cusp fusion
– Right / Non – coronary cusp fusion
• Much more rare single leaflet, unicuspid valve
Bicuspid Aortic Valve
CONGENITAL HEART CENTER
5
CONGENITAL HEART CENTER
• Increased risk for calcific aortic stenosis
• Increased risk for aortic insufficiency
• More likely to be progressive than normal valve
• Increased risk for endocarditis
– Antibiotic prophylaxis is not recommended
– Great Britain experience
Bicuspid Aortic Valve
CONGENITAL HEART CENTER
6
CONGENITAL HEART CENTER
• Early Systolic Ejection Click
– Doming valve with sail-like pop
• Aortic stenosis and/or insufficiency murmurs
• Aortic dilation is generally undetectable
– S2 may be prominent
Bicuspid Aortic Valve – Physical Exam

11/2/2017
3
CONGENITAL HEART CENTER
7
CONGENITAL HEART CENTER
• The is not a valve condition only
• The entire ascending aorta is at risk for dilation
– Aortic Sinus
– Tubular Ascending Aorta
– “Root”
• Mechanism is uncertain
– Hereditary tissue difference
• Cystic Medial Necrosis
– Hemodynamic consequent
– Can occur with normal valve function
Bicuspid Aortic Valve – Associated Aortopathy
CONGENITAL HEART CENTER
8
CONGENITAL HEART CENTER
• Autosomal dominant pattern with variable penetrance
• Valve pathology alone appears in 10% of first degree relatives
• Aortopathy with tricommisural valve occurs in more
– Clinically Silent
Bicuspid Aortic Valve - Hereditary Nature
CONGENITAL HEART CENTER
9
CONGENITAL HEART CENTER
11/2/2017
4
CONGENITAL HEART CENTER
10
CONGENITAL HEART CENTER
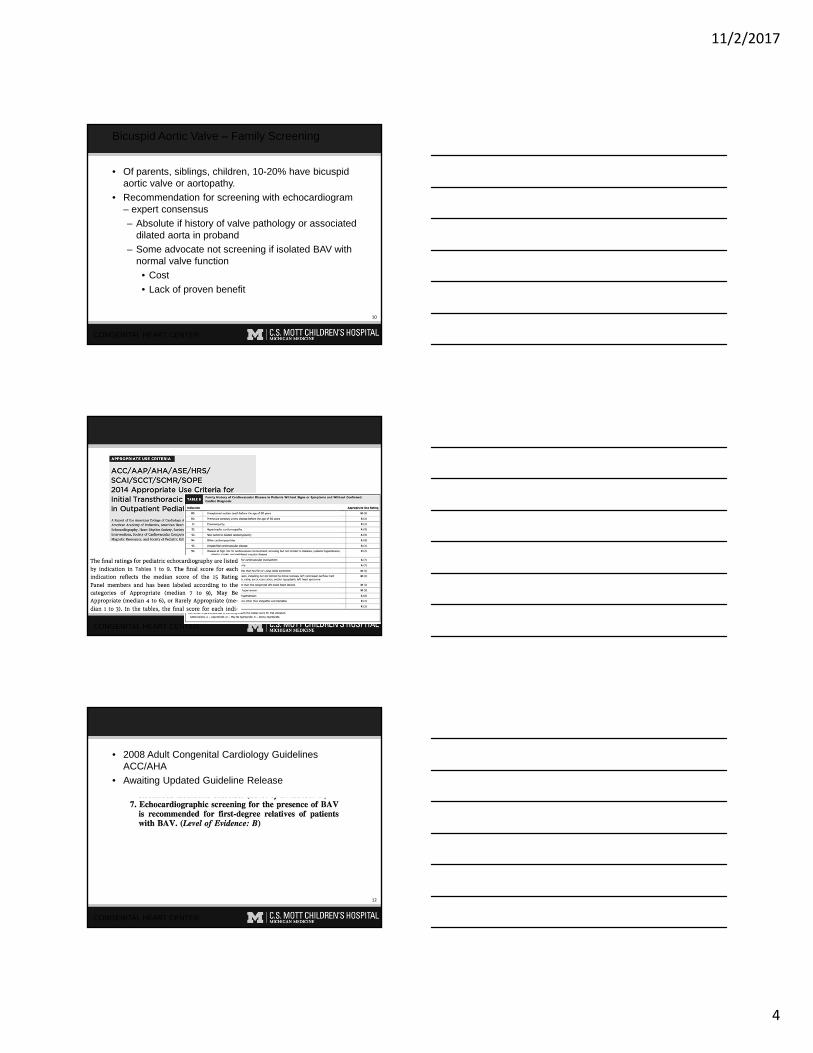
• Of parents, siblings, children, 10-20% have bicuspid aortic valve or aortopathy.
• Recommendation for screening with echocardiogram – expert consensus
– Absolute if history of valve pathology or associated dilated aorta in proband
– Some advocate not screening if isolated BAV with normal valve function
• Cost
• Lack of proven benefit
Bicuspid Aortic Valve – Family Screening
CONGENITAL HEART CENTER
11
CONGENITAL HEART CENTER
CONGENITAL HEART CENTER
12
CONGENITAL HEART CENTER
• 2008 Adult Congenital Cardiology Guidelines ACC/AHA
• Awaiting Updated Guideline Release

11/2/2017
5
CONGENITAL HEART CENTER
13
CONGENITAL HEART CENTER
• Echocardiography
• Aortic stenosis / regurgitation parameters
• Vascular assessment of entire ascending aorta
– If unable, then CT or MRI
Bicuspid Aortic Valve – Assessment
CONGENITAL HEART CENTER
14
CONGENITAL HEART CENTER
CONGENITAL HEART CENTER
15
CONGENITAL HEART CENTER

11/2/2017
6
CONGENITAL HEART CENTER
16
CONGENITAL HEART CENTER
ACC Valve Guidelines 2014
CONGENITAL HEART CENTER
17
CONGENITAL HEART CENTER
• Aortic Dilation is Progressive
• Risk for Dissection / Rupture
– Similar to other aortopathy
• Previous guidelines recommended aortic root replacement in BAV for diameter >50 mm
• 2014 guidelines recommend >55 mm for ALL
– Revised consensus with Thoracic Surgery is >55mm with consideration of surgery at 50 mm. (Broadly written 2A recommendation)
Bicuspid Aortic Valve - Aortopathy
CONGENITAL HEART CENTER
18
CONGENITAL HEART CENTER
• No evidence of benefit if normal BP
– Previous attempts to treat with beta-blockade or ARB with low BP goals
• Anti-hypertensive - Goal of normal blood pressure
• SBE antibiotic prophylaxis is NOT recommended
Bicuspid Aortic Valve – Medical Therapy

11/2/2017
7
CONGENITAL HEART CENTER
19
CONGENITAL HEART CENTER
• Based on valve pathology and aortic dimensions
Bicuspid Aortic Valve – Exercise Recommendations
CONGENITAL HEART CENTER
20
CONGENITAL HEART CENTER
• Genetic
– Turner Syndrome
• Left Side of the Heart – Multi Level Obstruction
– Aortic Coarctation
– Mitral stenosis
Bicuspid Aortic Valve – Associated Conditions
CONGENITAL HEART CENTER
21
CONGENITAL HEART CENTER
• XO genetic material loss
• Short stature, webbed neck
• Coarctation
• Partial Anomalous Pulmonary Venous Return
– Pulmonary vein connecting to systemic vein instead of to the left atrium
• All should have vascular anatomy checked
– CT / MRI/MRA
Turner Syndrome

11/2/2017
8
CONGENITAL HEART CENTER
22
CONGENITAL HEART CENTER
Coarctation
Bicuspid Aortic Valve
Coarctation and Bicuspid Aortic Valve
50% 6%
CONGENITAL HEART CENTER
23
CONGENITAL HEART CENTER
• Discrete vs Long Segment Narrowing of Thoracic Aorta from Transverse to Descending
• Repair may be end-to-end discrete resection vslonger segment patch augmentation
• Higher risk for aortic dilation when present with bicuspid aortic valve
Coarctation of the Aorta
CONGENITAL HEART CENTER
24
CONGENITAL HEART CENTER
• Diagram / Echo
Coarctation of Aorta

11/2/2017
9
CONGENITAL HEART CENTER
25
CONGENITAL HEART CENTER
• Even ideal infant repairs are long-term risks
• Hypertension
• Accelerated Coronary Diseaes
• Recoarctation
• Cerebral Aneurysm
Coarctation of Aorta
CONGENITAL HEART CENTER
26
CONGENITAL HEART CENTER
• Long term cardiac follow-up is appropriate
• Life style modification
• Modifiable Risk Factor attack
Coarctation of the Aorta
CONGENITAL HEART CENTER
27
CONGENITAL HEART CENTER
• Very few cardiac conditions are “Fixed” or “Cured”
• Other than simple ASD, PDA, muscular VSD repair or spontaneous closure in infancy or early childhood, some cardiac follow-up is recommended
Life Long Congenital Cardiac Follow-up

11/2/2017
10
CONGENITAL HEART CENTER
28
CONGENITAL HEART CENTER
CONGENITAL HEART CENTER
29
CONGENITAL HEART CENTER
CONGENITAL HEART CENTER
30
CONGENITAL HEART CENTER

11/2/2017
11
CONGENITAL HEART CENTER
31
CONGENITAL HEART CENTER
CONGENITAL HEART CENTER
32
CONGENITAL HEART CENTER
CONGENITAL HEART CENTER
33
CONGENITAL HEART CENTER
Adult Congenital Heart Program
Mark Norris MD, MS
• (734) 232-2673
• (877) 720-3983

11/2/2017
12
CONGENITAL HEART CENTER
34
CONGENITAL HEART CENTER
CONGENITAL HEART CENTER
35
CONGENITAL HEART CENTER

‘
Crytogenic Shock: A Cardiologist's Perspective
James Fox, MD, FACC
Notes:

1
Update in Cardio‐oncologyThomas C. Andrews, MD, FACC
Need for elective referral
Cardio‐oncology
2
• Evaluation for possible late effects of treatment‒ Anthracycline exposure‒ Prior radiation (particularly mantle)‒ CHF symptoms
• Patients with multiple myeloma‒ Light chain disease‒ Screen for cardiac amyloidosis
• Patients with carcinoid tumors‒ Valvular heart disease
Carcinoid syndrome
• 67 year old with metastatic carcinoid tumor• Oct 2016: nausea, vomiting, diarrhea
‒ Multiple large liver tumors, up to 4 cm, biopsy proven carcinoid. Also lung involvement
‒ Primary in the terminal ileum resected
• Nov 2016: start monthly lanreotide‒ Clinical response of lung, liver tumor
• Home destroyed by hurricane Harvey, moved to MI from Houston

2
Carcinoid syndrome
4
Tricuspid regurgitation
Carcinoid syndrome
5
Aortic regurgitation
Carcinoid syndrome
• Right sided valvular lesions most common‒ TR‒ PS/PI
• Left sided valvular involvement with PFO or poorly controlled disease.‒ Pure AI and/or MR
• Associated with liver disease and high urinary 5‐HIAA levels

3
Carcinoid heart disease
• Carcinoid heart disease with Class 3 symptoms mean survival is less than 1 year.
• Treatment of choice is TVR/PVR‒ Operative mortality 6‐10% (Mayo)‒ Bioprosthetic valves usually chosen
• Early degeneration
• Importance of disease control with somatostatin analogues
Patients in need of urgent referral
Cardio‐oncology
8
• Established cardiovascular disease‒ Cardio‐toxic treatment under consideration‒ Poorly controlled symptoms‒ Major surgery contemplated
• New cardiovascular symptoms during treatment‒ Heart failure/drop in EF‒ Angina‒ Arrhythmias
• Treatment with VEGF inhibitors‒ Bevacizumab, others‒ HTN management
Inhibitors of VEGF and hypertension
• 63 year old female with thoracic aortic aneurysm and metastatic clear cell carcinoma of the kidney to lungs (Stage III)
• Jan 2017: Nephrectomy with 15cm tumor locally invasive
• June 2017: Multiple lung nodules. CT guided biopsy confirms metastatic disease
• Therapy started with Votrient (pazopanib)
4
Inhibitors of VEGF and hypertension
• BP elevated up to 190/126 at home• Management by oncology
‒ Metoprolol stopped‒ lisinopril 10mg added‒ Votrient dose reduced by 25%
• Urgent cardio‐oncology consult
Inhibitors of VEGF and hypertension
• PMx‒ Ascending thoracic aortic aneurysm measuring up to 4.0
cm.‒ Baseline echo: EF 60%, grade 1 diastolic dysfunction,
cLVH, dilated ascending aorta with mild aortic insufficiency.
‒ Lipids: LDL 122, HDL 52
• Soc Hx‒ Distant history of smoking‒ Rare alcohol
Inhibitors of VEGF and hypertension
• Physical exam‒ BP 120/86, HR 66‒ BMI 36‒ Normal cardiovascular exam
• EKG‒ QTc 460 msec‒ nonspecific ST‐T wave changes

5
Inhibitors of VEGF and hypertension
• VEGF inhibitors commonly cause HTN, proteinuria and renal dysfunction
• Incidence reported 40% for pazopanib, similar for bevacizumab (avastin)‒ Elevations of up to 30 mmHg (systolic and diastolic)
reported in some trials)‒ No current way to predict this response
• Mechanisms‒ Decrease in nitric oxide production‒ Endothelial cell damage and dysfunction
Inhibitors of VEGF and hypertension
• Treatment goal is <140/90• Monitor BP minimally weekly during first cycle of
therapy, then regularly thereafter• Start BP medication if above target, or if >20mmHg
from baseline• ACEI and dihydropyridine CCBs commonly used for
treatment• BP can fall quickly when TKIs are discontinued
When to refer
Cardio‐oncology
15
• Elective referrals‒ Evaluation for possible late effects of treatment‒ Patients with multiple myeloma‒ Patients with carcinoid tumors
• Urgent referrals‒ Established cardiovascular disease‒ New cardiovascular symptoms during treatment‒ Treatment with VEGF inhibitors
• Contact info‒ [email protected]‒ 972‐672‐6504‒ MMC page operator
1
Aortic Valve diseaseNick Slocum, MD, FACCMichael Howe, MD, FACC
11.4.17
2
• No financial relationships / disclosures
Should anyone get a mechanical aortic valve?
3
• Controversial‒ Lack of standard definitions for valve deterioration in the
surgical literature.
• Changing practice‒ More receiving bioprosthetic valves (registry data)
‒ Adults < 50yo undergoing AVR‒ 1997 vs 2014
‒ 14% vs 47% bioprosthetic
2
Should anyone get a mechanical aortic valve?
4
• Bioprosthetic vs. Mechanical
• Anticoagulation • Lifetime stroke risk (higher in mech valves)• Reoperation : 25% vs. 10% at 12 yrs
Should anyone get a mechanical aortic valve?
5
• “Consider the risk‐benefit balance of a mechanical versus a bioprosthetic valve based on anticoagulation and bleeding risk considerations, the risk of structural valve deterioration and redo surgery and expected patient longevity.” (BMJ AHA)
Should anyone get a mechanical aortic valve?
6
• Yes• <55 yo “consider” mechanical
‒ Risks, benefits, lifestyle
• Child bearing women?‒ Mechanical valve + pregnancy is challenging

3
How often should I get an echo in AS?
7
• Changing symptoms or physical exam• Asymptomatic AS
‒ Mild every 3‐5yrs‒ Moderate 1‐2 yrs‒ Severe 1 year
Mitral Valve diseaseNick Slocum, MD
11.4.17
How often should I get echos in mitral dz?
9
• Changing symptoms or physical exam• Asymptomatic MR
‒ Mild every 3‐5yrs‒ Moderate 1‐2 yrs‒ Severe 6‐12months (* more frequent than AS)
• Under cardiology guidance an exercise echo could be considered in the asymptomatic severe pt to further risk stratify.
4
Who should be considered for a MitraClip?
10
• Percutaneous approach for treatment of severe symptomatic degenerative MR in high risk surgical patients.
• Objective is palliation of symptoms and reduction in CHF related admissions.
• Goal is to reduce MR by 2‐3 grades. A successful procedure is severe MR mild.
• Procedure is done under general anesthesia and Echo guided.
Who should be considered for a MitraClip?
11
• Current indication is for Degenerative MR.
• We have been evaluating through the Structural Heart Clinic patients with an indication for mitral valve surgery but thought to be high risk for surgery.
• Patients seen by both cardiology and CT surgery to evaluate candidacy.
Who should be considered for a MitraClip?
12
• Severe degenerative MR
• High risk for surgery
• Significant (heart failure) symptoms

5
13
14
15

Break-out
Sessions

11/2/2017
1
Atrial Fibrillation
Robert Kennedy, MD, FHRSRebecca Eichberger, FNP‐C
www.HRSonline.org
2017 HRS/EHRA/ECAS/APRHS/SOLAECE Expert Consensus Statement on Catheter and Surgical Ablation of Atrial Fibrillation
• Gerhard Hindricks, MD and Young‐Hoon Kim, MD, PhD
• 33 million people have AF world wide
• 3–5 million people in the United States
• By 2050, app. 8 million people will be affected in the United States
• AF increases risk of stroke on average 5-fold
• AF increases heart failure, dementia, and total mortality
• 450000 hospitalizations in the United States
• 90000 deaths related to AF in the United States
Significance of AF

11/2/2017
2
AF Definitions: Speaking the Same Language…
Anatomy of the LA and AF
• Obesity
• Sleep apnea
• Hypertension
• Diabetes
• Alcohol
• Exercise
• Control of risk factors has a significant impact on AF burden
Risk Factors and Their Interaction with AF
Comorbidity Association with AF
Heart failure vs. none HR 1.43 (95% CI 0.85–2.40)
Hypertension (treated) vs. none HR 1.32 (95% CI 1.08–1.60)
ObesityNone (BMI <25 kg/m²)
Overweight (BMI 25–30 kg/m²)
Obese (BMI ≥31 kg/m²)
HR:
1.00 (reference)
1.13 (95% CI 0.87–1.46)
1.37 (95% CI 1.05–1.78)
Diabetes mellitus vs. none HR 1.25 (95% CI 0.98–1.60)
Obstructive sleep apnea vs. none HR 2.18 (95% CI 1.34–3.54)
Chronic obstructive pulmonary diseaseFEV1 ≥80%
FEV1 60–80%
FEV1 <60%
RR:
1.00 (reference)
1.28 (95% CI 0.79–2.06)
2.53 (95% CI 1.45–4.42)

11/2/2017
3
Case Study: 58 year old male with persistent AF failing Multaq and Norpace.
ARREST‐AF• Study objective was to
evaluate the impact of risk factor and weight management on AF ablation
LEGACY‒ Study objective was to
evaluate the long term impact of weight loss and weight fluctuation on rhythm control in obese individuals with AF.
8
LEGACY
9Pathak, R. K. et al. J Am Coll Cardiology. 2015; et al. J Am Coll Cardiol. 2015; 65(20) 2159-69.

11/2/2017
4
10Pathak, R. K. et al. J Am Coll Cardiol. 2015; 65(20): 2159-69
11Pathak, R. K. et al. J Am Coll Cardiol. 2015; 65(20): 2159-69.
12

11/2/2017
5
Atrial Fibrillation Ladder
13
Age
Obesity
Sleep apnea
HTN
ETOH
Diabetes
Misc/Genetics
AFIB
Indications for AF Ablation
Indications for AF Ablation

11/2/2017
6
Indications for AF Ablation
**A decision to perform AF ablation in an asymptomatic patient requires additional discussion with the patient because the potential benefits of the procedure for the patient without symptoms are uncertain.
Indications for AF Ablation
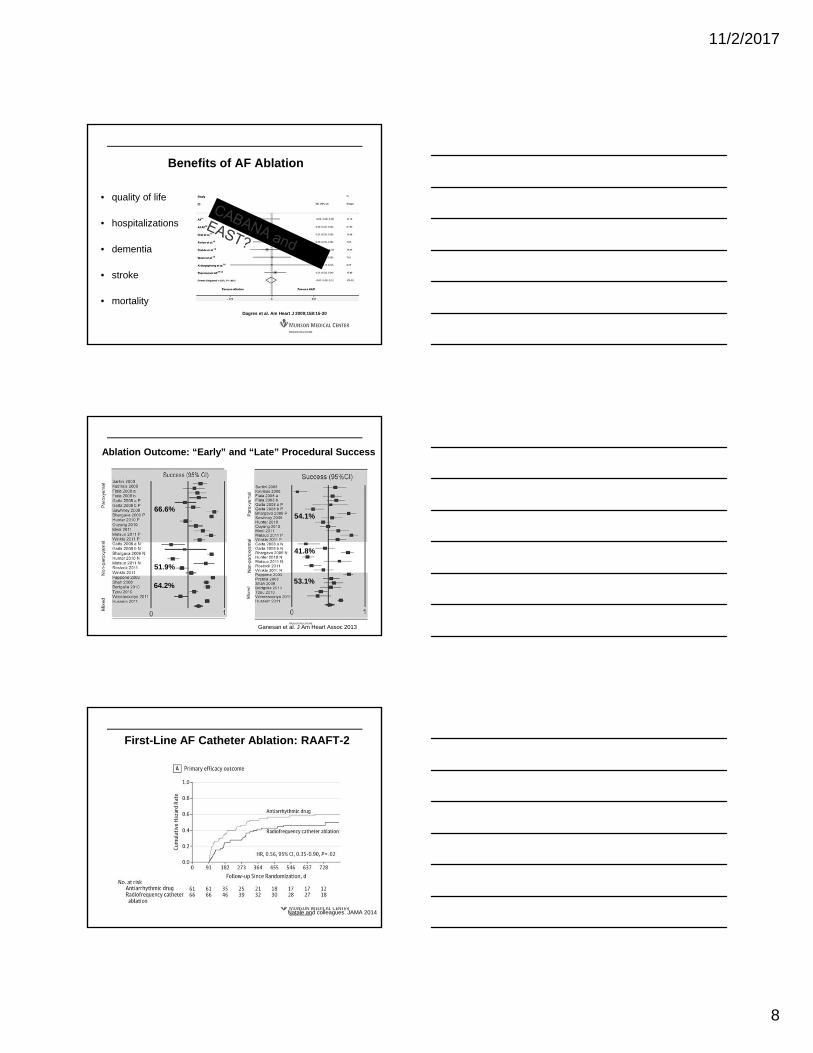
• quality of life
• hospitalizations
• dementia
• stroke
• mortality
Benefits of AF Ablation
Reynolds et al. Circ Cardiovasc Qual Outcomes 2010;3:615-623

11/2/2017
7
• quality of life
• hospitalizations
• dementia
• stroke
• mortality
Benefits of AF Ablation
Depression Anxiety
Physical component Mental component
AF Abl.
AA Drugs
Sang et al. Clin Cardiol 2013
• quality of life
• hospitalizations
• dementia
• stroke
• mortality
Benefits of AF Ablation
>9.000 patients~40% CHADS≥2
Reynolds et al. Circ Cardiovasc Qual Outcomes 2012;5:171-181
• quality of life
• hospitalizations
• dementia
• stroke
• mortality
Benefits of AF Ablation
Dagres et al. Am Heart J 2009;158:15-20
11/2/2017
8
• quality of life
• hospitalizations
• dementia
• stroke
• mortality
Benefits of AF Ablation
Dagres et al. Am Heart J 2009;158:15-20
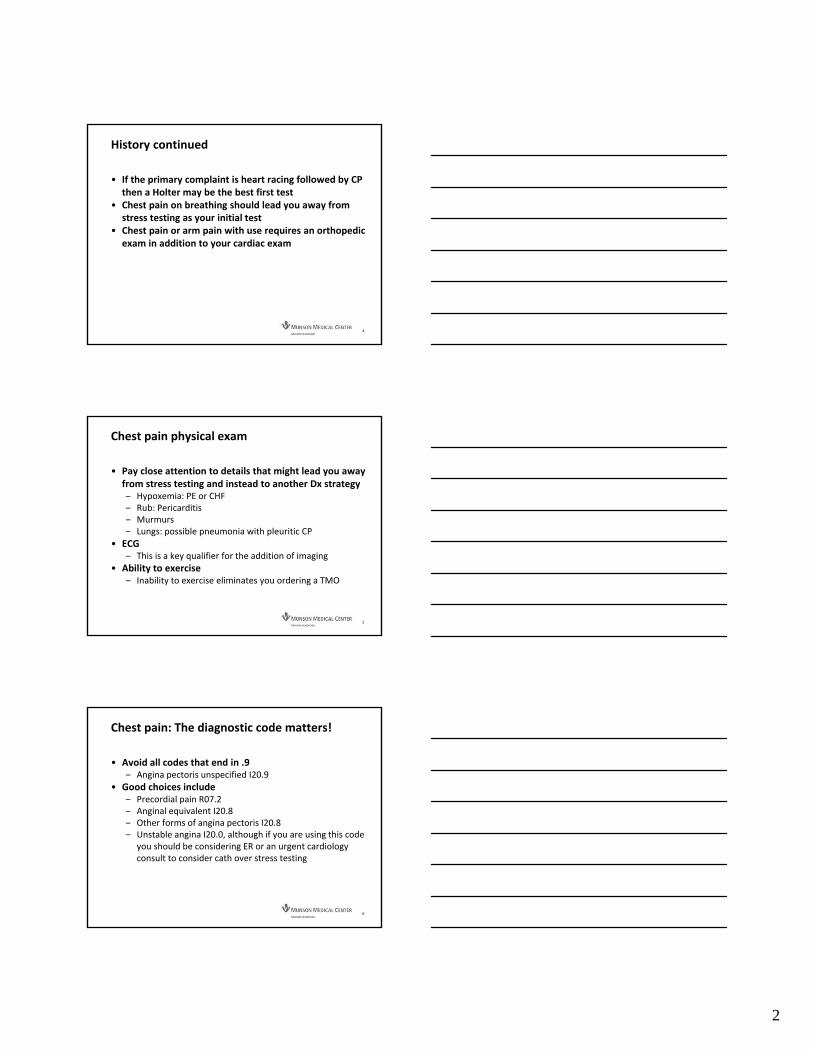
Ganesan et al. J Am Heart Assoc 2013
Ablation Outcome: “Early” and “Late” Procedural Success
66.6%
51.9%
64.2%
54.1%
41.8%
53.1%
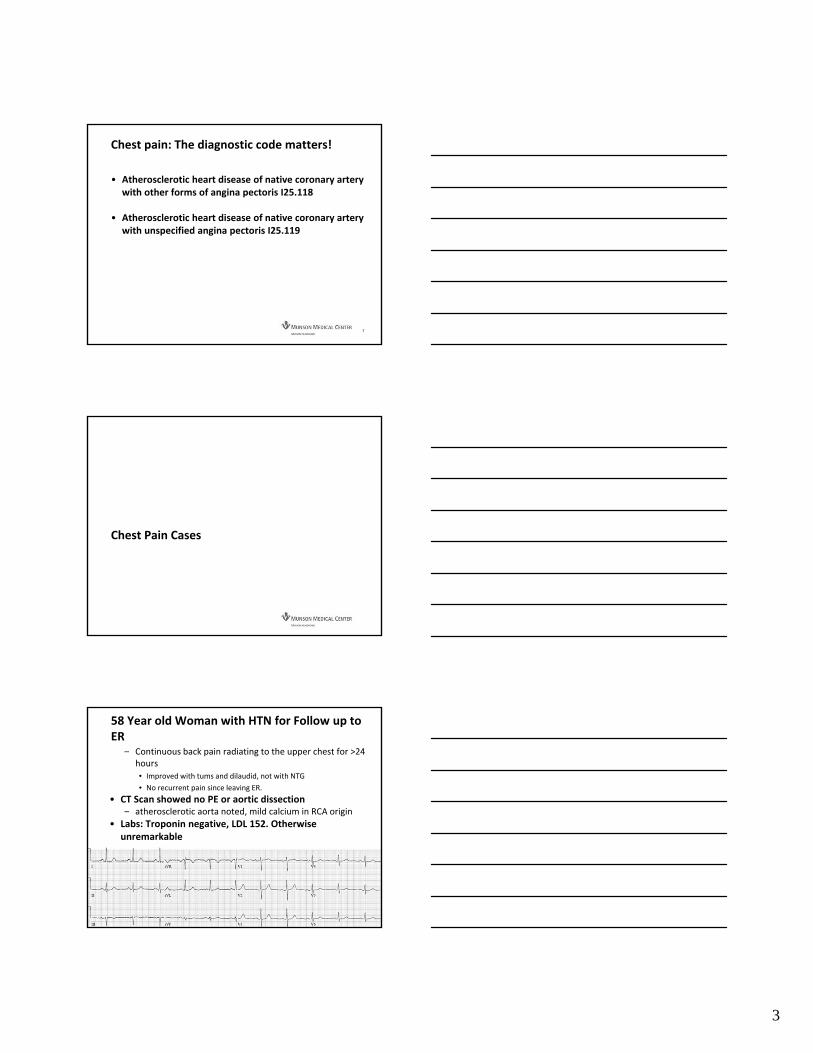
First-Line AF Catheter Ablation: RAAFT-2
Natale and colleagues. JAMA 2014

11/2/2017
9
Catheter Ablation of AF: MANTRA-PAF Trial at 5 yrs.
Nielsen et al. 2016Hakalahti A et al.; Europace 2015

1
Chest Pain in the officeTodd Adams DOBenjamin Ebner MD
Chest pain in the office
2
• Brief focused history‒ Red flags?
• Yes to ER
• No continue to full exam
• Should you check a triage troponin in the office??
Chest H & P
3
• The key to avoiding a discussion with AIM is the details‒ Having these details in your note will in many cases
eliminate you need to participate in “peer to peer” discussions
• Describe the discomfort including severity on 0‐10 scale.
• Describe location of discomfort including radiation of symptoms
• Describe context of symptoms‐ rest/exertional or both• Describe associated symptoms• Include risk factors
2
History continued
4
• If the primary complaint is heart racing followed by CP then a Holter may be the best first test
• Chest pain on breathing should lead you away from stress testing as your initial test
• Chest pain or arm pain with use requires an orthopedic exam in addition to your cardiac exam
Chest pain physical exam
5
• Pay close attention to details that might lead you away from stress testing and instead to another Dx strategy‒ Hypoxemia: PE or CHF‒ Rub: Pericarditis‒ Murmurs‒ Lungs: possible pneumonia with pleuritic CP
• ECG‒ This is a key qualifier for the addition of imaging
• Ability to exercise‒ Inability to exercise eliminates you ordering a TMO
Chest pain: The diagnostic code matters!
6
• Avoid all codes that end in .9‒ Angina pectoris unspecified I20.9
• Good choices include‒ Precordial pain R07.2‒ Anginal equivalent I20.8‒ Other forms of angina pectoris I20.8‒ Unstable angina I20.0, although if you are using this code
you should be considering ER or an urgent cardiology consult to consider cath over stress testing
3
Chest pain: The diagnostic code matters!
7
• Atherosclerotic heart disease of native coronary artery with other forms of angina pectoris I25.118
• Atherosclerotic heart disease of native coronary artery with unspecified angina pectoris I25.119
Chest Pain Cases
58 Year old Woman with HTN for Follow up to ER
9
‒ Continuous back pain radiating to the upper chest for >24 hours• Improved with tums and dilaudid, not with NTG
• No recurrent pain since leaving ER.
• CT Scan showed no PE or aortic dissection ‒ atherosclerotic aorta noted, mild calcium in RCA origin
• Labs: Troponin negative, LDL 152. Otherwise unremarkable
4
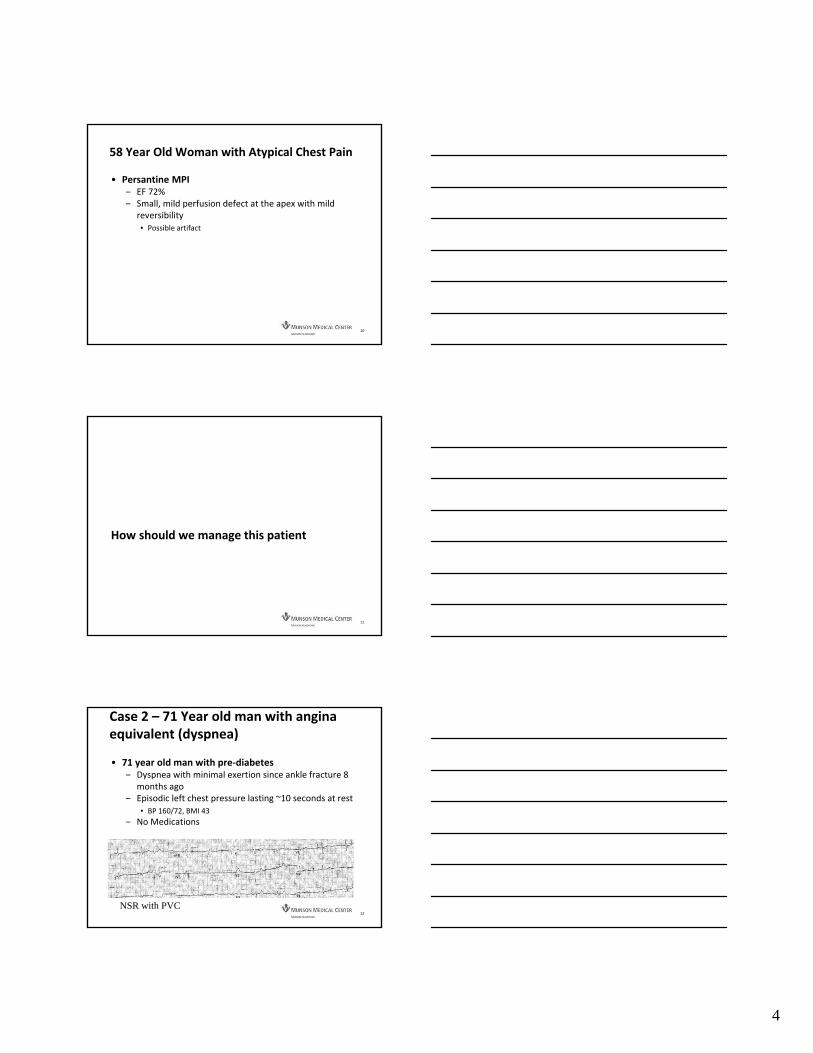
58 Year Old Woman with Atypical Chest Pain
10
• Persantine MPI‒ EF 72%‒ Small, mild perfusion defect at the apex with mild
reversibility• Possible artifact
How should we manage this patient
11
Case 2 – 71 Year old man with angina equivalent (dyspnea)
12
• 71 year old man with pre‐diabetes ‒ Dyspnea with minimal exertion since ankle fracture 8
months ago‒ Episodic left chest pressure lasting ~10 seconds at rest
• BP 160/72, BMI 43
‒ No Medications
NSR with PVC

5
Case 2
13
• Stress MPI ‒ 6 minutes on Bruce protocol (7 METS)‒ 88% PMHR‒ Ventricular ectopy including triplets with exercise‒ No ST Changes, No Angina
• Duke Treadmill Score of 6
‒ Inferior infarct pattern (12% of LV) with LVEF of 45%
How should we manage this patient?
14
Case 3
15
• 76 year diabetic man with new shortness of breath on exertion – Class II after a transient episode a brief episode of chest pain three weeks ago
• Exam BP 142/71, HR 71‒ Well appearing, lungs clear, no JVD, no edema

6
76 Year Old Diabetic Man with Recent Chest Pain
16
• Echo LVEF 40%, anterior infarct, LV Thrombus• Moderate‐Severe MR.• Current Meds
‒ Atenolol 50‒ Lisinopril 5‒ Insulin/Glipizide
How should we manage this patient?
17

1
Breakout Session – SyncopeGreg Francisco, MD, FACCJames Fox, MD, FACC
DISCLOSURES
• None to declare
The Case of the Passing Out Pilot
• A 26 year old male USMC helicopter pilot presents for recurrent syncope.
• Episode occurred while standing at a blackboard giving a brief to his squadron – little prodrome
• 2 prior episodes 1 and 3 years prior – similar circumstances
• Previous workup included echocardiogram, tilt-table test, 30 day event monitor – all normal

2
• Another 30 day monitor is ordered• Patient is grounded from flying• 30 day event monitor is normal – no events• 1 week after mailing the monitor back another
episode occurs while seated at computer
Workup?
Syncope: “A symptom that presents with an abrupt, transient, complete loss of consciousness, associated with inability to maintain postural tone, with rapid and spontaneous recovery.”
Up to 40% have experienced an episodeUp to 13% have had recurrent syncope

3
Causes:
• Neurocardiogenic (vasovagal); • Reflex-mediated (cough, micturition, etc)• Orthostatic hypotension
• Arrhythmic – brady (sick sinus/complete heart block); tachy –VT, VF, AF
• Structural – aortic stenosis; atrial myxoma (rare)
Other noncardiac – hemorrhage, pulmonary embolism
Nonsyncope – seizure, hypoglycemia, pseudosyncope, narcolepsy
Cardiac Causes more likely Noncardiac Causes more likely
Older age (>60) Younger age
Male sex Female sex
History of MI, structural heart disease, arrhythmia, or reduced EF or congenital heart disease
No known cardiac disease
Syncope during exertion Syncope only in standing position
Syncope in supine position Positional change from supine to standing
Low # of syncope episodes Frequent syncope
Absence of prodrome Presence of prodrome: nausea, vomiting, feeling warmth
Abnormal cardiac exam Triggers: dehydration, pain, blood draw, cough, laugh, micturition, defecation, deglutition
Family history of inheritable conditions or premature SCD (<50)

4
Workup begins with a good history and physical, and ECG
Other Tests to consider:1) Echocardiogram – if structural heart disease considered2) Stress test – if syncope during exercise3) Monitoring – based on frequency and severity of syncope:
holter – 24hevent monitor – 14-30 daysImplantable loop recorder – 3 years
4) Tilt-Table Testing – if vasovagal syncope suspected5) Targeted lab tests6) EP study, carotid duplex, brain MRI – all low yield
Implantable loop recorder – injectable, minimally invasive – 3 year battery
2 months after loop recorder placed, our pilot suffered another episode associated with a 14 second asystole

5
Vasovagal Syncope
Treatment of Vasovagal Syncope
Driving Restrictions/Recommendations after syncope:
Know your state’s lawsMichigan DOT: No driving for 6months unless a letter recommending return to driving is provided by a “medical examiner”Secretary of State (not the physician) decides whether a patient can resume driving
California – no driving for 6months. May drive at 3months with document stating a physician is monitoring
Commercial Driver’s License – regulated by FMCSA – fairly straightforward guidance, with some room for waiver

6
Thank you
QUESTIONS?

‘
Breakout Session – ECG Pearls
Dino Recchia, MD, FACC
Thomas Andrews, MD, FACC
Notes: