
Presentation for EPEMED Webinar (11-27-12) Final
36
COMMUNICATING THE POTENTIAL OF PERSONALISED MEDICINE TO STAKEHOLDERS IN EUROPE From Complexity to Clarity: EPEMED Webinar November 27 th , 2012 Stig Albinus APCO Worldwide
-
Upload
stig-albinus -
Category
Documents
-
view
300 -
download
6
Transcript of Presentation for EPEMED Webinar (11-27-12) Final
COMMUNICATING THE POTENTIAL OF PERSONALISED MEDICINE TO STAKEHOLDERS IN EUROPE
From Complexity to Clarity:
EPEMED WebinarNovember 27th, 2012Stig AlbinusAPCO Worldwide

2
Overview of Presentation• Setting the stage: Complexity or confusion?• European healthcare landscape • How to advance adoption of personalised
medicine – learning from other disruptive technologies
• Five hypotheses about change• Four thought starters about communications
strategies• Desired future stakeholder perceptions• Opportunities for EPEMED and its members

3
Complexity or Confusion?

EUROPEAN HEALTH CARE LANDSCAPE AND STAKEHOLDER INSIGHTS
4

5
EU Health and Pharmaceutical Policy Today
Trends & ChallengesSustainability of European healthcare systems under threat:• Strong focus on cost-containment with healthcare reform and European austerity measures• Changing demographics – ageing population• Lack of recognition of the value of innovation
Role and influence of policy makers and payer audiences continue to grow:• Rapid and unpredictable changes in government pricing policies• HTA evaluation to inform reimbursement decisions
EU Pharmaceutical Policy & Legislation EU Medical Devices Legislation
• Reflection process on PM• Revision Transparency Directive• Review Data Protection Directive• EMA Reflection papers and Consultations
on Genomics and PM
• Recast of Medical Devices Directives and IVD Directive

6
EU Stakeholder Insights about Personalised Medicine
• 70% of primary care physicians, neurologists and cardiologists expect personalised medicine to become routine in their own clinical practice within five years (EU and US survey)
– 37% of oncologists claim to be ‘very familiar’ with personalised medicine and only 6% of other specialists and 5% of PCPs
– “Eye for pharma” website, 16 October 2012 http://social.eyeforpharma.com/patients/personalised-medicine-%E2%80%93-through-eyes-physician
• Personalised healthcare will deliver improved health outcomes (64% of 840 respondents)
– Absence of clear regulatory guidelines is causing delay in marketing and authorisation of personalised health care products and services (over 60% of respondents)
– Healthcare spending will increase short term - 5 years (58% of respondents), but will decrease long-term - 15 years (46% of respondents)
– Europe-wide cooperation will be necessary for the development and adoption of personalised healthcare (80 % of respondents)
– “Health for All, Care for You,” Karolinska Institutet Survey on the Promise of Personalised Healthcare in Europe, 2010) http://www.sciencebusiness.net/pdfs/PM_survey_results.pdf
7
EU Stakeholder Initiatives Around Personalised Medicine
• Some European hospitals are engaged in the development of new imaging technology and genetic tools, mostly in cancer, but state “major challenges including learning curve for doctors and consumer behavior”
– http://www.hope.be/05eventsandpublications/docpublications/88_personalised_medicine/88_HOPE-PWC_Publication-Personalised-Medicine_February_2012.pdf
• Few initiatives at the Member State government level – Ireland one exception citing personalised medicine as key area for commercialisation
– “Research Prioritisation Report” recommends “mapping exercise to identify areas of strength and opportunity, e.g., personalised medicine/diagnostics, biomarkers…”
– http://www.forfas.ie/media/ffs20120301-Research_Prioritisation_Exercise_Report.pdf
• Patients and patient organizations are largely absent from the public debate – with the exception of cancer advocacy groups

8
EU/US Comparisons• While there are many similarities, the single-payer European
healthcare systems may provide a better foundation for personalised medicine, particularly population-based strategies
– There are however large variations across Member States
• European austerity measures will short term represent a significant challenge for investing in personalised medicine
• Multi-tiered US health care system may enable advances in personalized medicine
– However limited to better funded health plans, integrated delivery systems and upscale markets

9
Key Stakeholder Overview• Hope, but limited understanding
– Continued general belief in the promise, but major obstacles due to limited understanding
• Oncology is still the main focus, but less obvious– Growing controversy about the reality of the promise
• Questions about physician readiness and clinical utility– GPs believe PM will eventually change medical practice, but limited experience
• Consumer privacy concerns– Consumers are hopeful, but concerned about privacy implications
• Policymakers on the fence– Policymakers are not clear about the relevance short term – Still waiting for the
Commission’s …omics report!• Cost is a concern
– General concerns about increase in costs short-term• There is a huge information and communication gap
– Limited, if any information in general consumer and business media

10
BIG PROMISE
“Personalised medicine offer tremendous opportunities for better care and raise high expectations”
John Dalli, Former EU Health Commissioner
Reduce medical errors
Improve patient outcomes
Reduce total healthcare spending over 15 years
“Health for All, Care for You,.” Karolinska Institutet Survey on
the Promise of Personalised Healthcare in Europe, 2010
Summary of Opportunities and Challenges for Personalised
Medicine in Europe
BIG OBSTACLES
Research, technology and standards
Lack of common EU policy and regulatory framework
Financial and reimbursement
Lack of education of physicians and patients
“European Perspectives in Personalised Medicine”, European Commission, 12-13 May, 2011

HOW TO ADVANCE ADOPTION OF PERSONALISED MEDICINE?
11

12
Hypothesis #1: Social Change is a Real Barrier
• While there are scientific, regulatory and financial obstacles to advancing personalised medicine, the major barrier to unlocking its potential is the human factor:
– Personalised medicine represents a powerful, disruptive and radical change of social and cultural interactions and communications among all stakeholders in all aspects of the health care delivery chain
– A typical example of moving a hot technology from the laboratory to market– Particularly in a conservative sector such as health care
“ For the technology to be fully implemented and integrated across the healthcare value chain, stakeholders recognised both scientific and structural hurdles that needed to be overcome. In fact, without a “basic understanding of human biology and disease mechanisms” the majority of the stakeholders failed to see a smooth transformation from the traditional healthcare paradigm to personalised healthcare.
“
“Health for All, Care for You,.” Karolinska Institutet Survey on the Promise of Personalised Healthcare in Europe, 2010)

13
From Newton to iPad
Apple Newton1987
Apple iPad2010

14
Typical Adoption Cycle for Disruptive Innovation
AWA
RE
NE
SS
AC
CE
PT
A
DO
PTI
ON
The iPad
The Internet
Genomics
TIME
15
Learning from Disruptive Innovation Cycles• Need to generate awareness and acceptance among
users and consumers before adoption happens• Adoption is based on emotional attachment and
experiences of personal value – not only a scientific or technical rationale
We need to HUMANISE AND PERSONALISE
genomics medicine

16
Hypothesis #2: Personalised Medicine is More than Genomics
• Personalised medicine/healthcare is the use of information to tailor treatment to individual groups of patients. This can include using genetic data, diagnostic tests or patient databases for segments of the population to maintain health, prevent disease, improve the outcomes of therapy and patient safety while reducing costs
“ “In effect we are looking at refining the definition of health and disease – to the point where the current definitions will be obsolete.
Ruxandra Draghia-Akli, Director-General for Research and Innovations, European Commission, “European Perspectives in Personalised Medicine, 12-13 May, 2011

17
Defining Personalized Medicine
Patient-Centricity &Empower-
ment
Drug-diagnostics
pairing
GeneticsBiomarkers
Targeted Therapies
Personal TechnologyImaging
Personal health technologieseHealth
DataKnowledge
18
Integrate personal health technologyAND
personalised medicine strategies
Leverage Personal Technologies to Drive Acceptance of Personalised Medicine
• Personal technologies – from electronic personal health records to portable smart phones – represent opportunities for empowering patients in the management of their own health by accessing genomics data
– Engage patients in the development of personalised medicine solutions: clinical trials, donations to tissue/biobanks, individual genetic tests
– Engage consumers/patients in collaboration with physicians

19
Hypothesis #3: Broader Acceptance of PM with New Health Paradigm
• Communication is more than a vehicle for educating stakeholders about the benefits of personalised medicine
• Communication is an intrinsic driver of change
• The personal and social involvement and engagement of stakeholders is the pathway to awareness, acceptance and adoption

20
The Current Disease Paradigm
Costs
Risk factorsLife style
Pre-disease Diagnose disease
Diseaseescalation
Morbidity Mortality
Level of education and personal engagement
Health education
Earlydetection
Disease interception Therapy Palliative
care
21
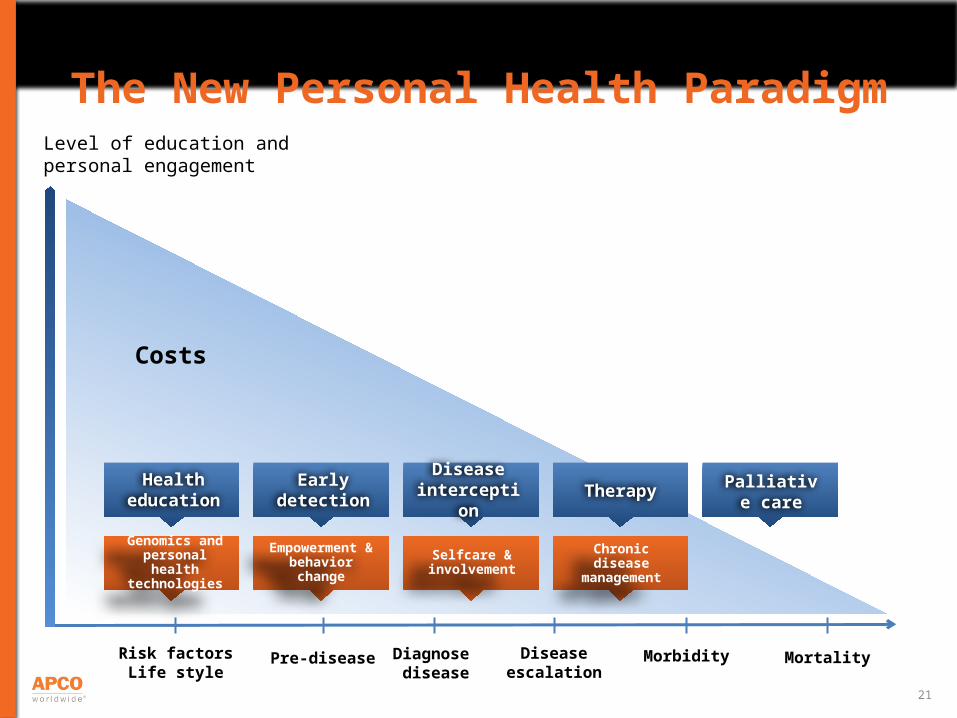
Costs
Risk factorsLife style
Pre-disease Diagnose disease
Diseaseescalation
Morbidity Mortality
Level of education and personal engagement
Health education
Earlydetection
Disease interception Therapy Palliative
care
The New Personal Health Paradigm
Empowerment & behavior change
Selfcare & involvement
Chronic disease management
Genomics and personal health
technologies
22
Leverage Genomics and Personal Technologies to Create New Health Paradigm
• Utilize technologies – genomics, personal health technologies, eHealth, etc. – to drive behavior change
• Empower patients/consumers to take more control over their own health and engage in decisions about prevention, disease interception
Improve HEALTH OUTCOMES AND QUALITY OF LIFE
while reducing costs
23
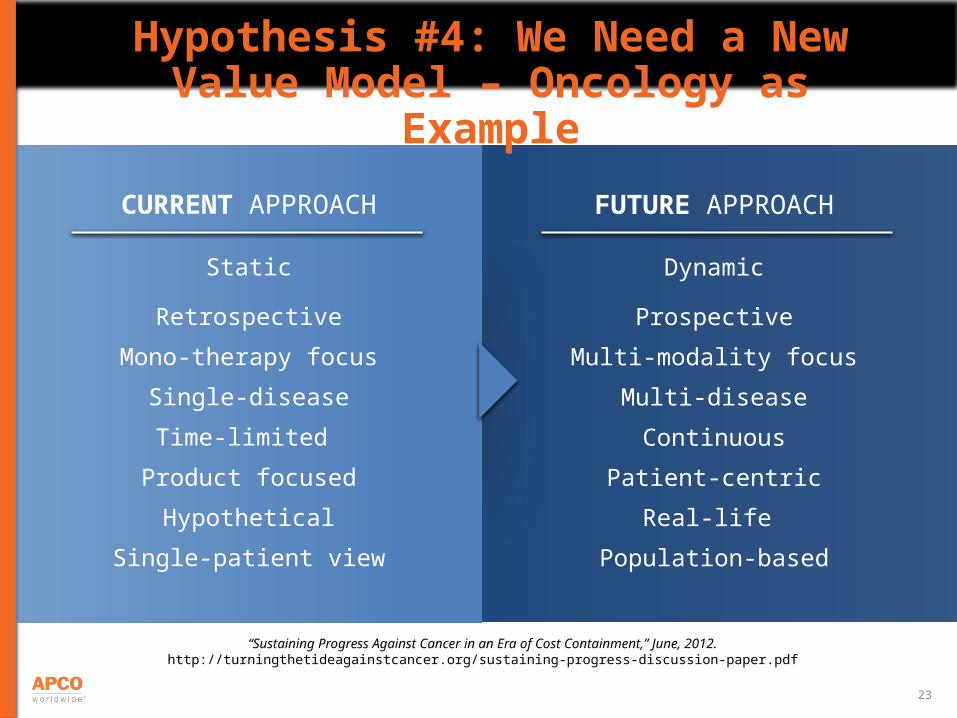
FUTURE APPROACH
Dynamic
Prospective
Multi-modality focus
Multi-disease
Continuous
Patient-centric
Real-life
Population-based
Hypothesis #4: We Need a New Value Model – Oncology as Example
CURRENT APPROACH
Static
Retrospective
Mono-therapy focus
Single-disease
Time-limited
Product focused
Hypothetical
Single-patient view
“Sustaining Progress Against Cancer in an Era of Cost Containment,” June, 2012.http://turningthetideagainstcancer.org/sustaining-progress-discussion-paper.pdf
24
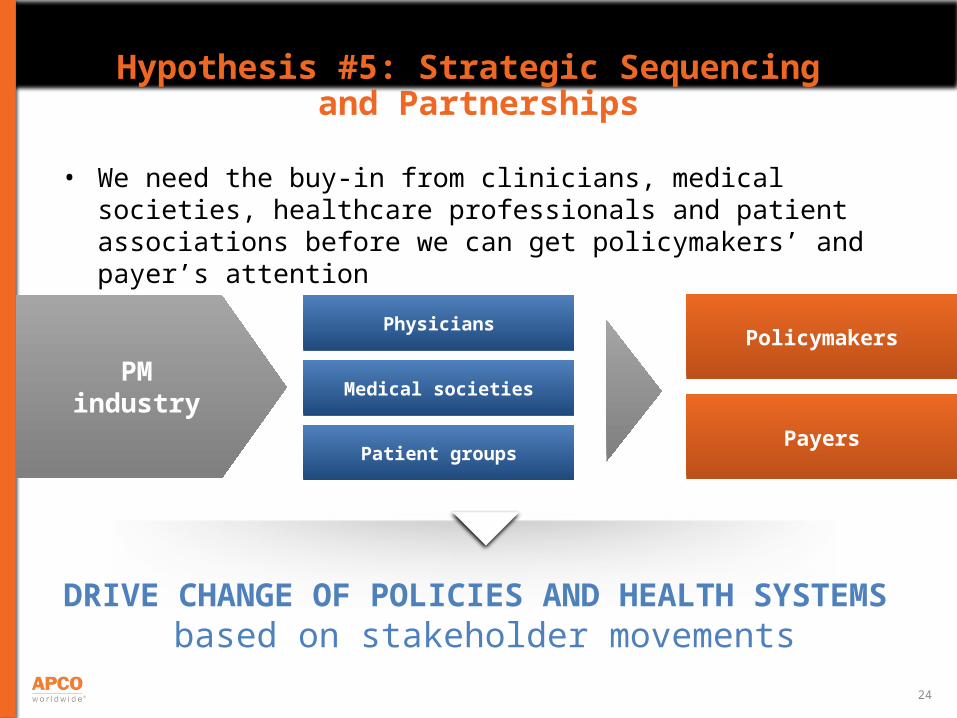
Hypothesis #5: Strategic Sequencing and Partnerships
• We need the buy-in from clinicians, medical societies, healthcare professionals and patient associations before we can get policymakers’ and payer’s attention
PM industry
Physicians
Medical societies
Patient groups
Policymakers
Payers
DRIVE CHANGE OF POLICIES AND HEALTH SYSTEMS based on stakeholder movements

THOUGHT STARTERS ABOUT COMMUNICATIONS STRATEGIES
25

26
Thought Starter #1: Humanise Genomics
• Create and tell human and emotionally powerful stories about the experiences of patients utilising genetic tests and targeted therapies
• Expand focus and education beyond oncology• Engage scientists and clinicians as partners in story telling to tell
their personal story• Utilise info graphics, animation and video to simplify and humanise
complex science around genomics
OUTCOMES Create an emotionally exciting image of what personalised
medicine means to the individual

27
Thought Starter #2: Communicate and Drive Adoption of New Value Model
• Demonstrate the benefits of personalised medicine on patients and populations
through health economic modeling– Utilize prospective modeling of future health and socioeconomic scenarios for Europe– Build on study of the value of cancer care comparing US and Europe in Health Affairs,
May 2012 - utilise data from EUROCARE registriesPhilipson et al: An Analysis Of Whether Higher Health Care Spending In The United States Versus Europe Is ‘Worth It’ In The Case Of Cancer
– http://content.healthaffairs.org/content/31/4/667.full
• Communicate the new value model to build understanding of the value of investing short-term in personalised medicine in Europe to drive significant, longer-term positive impact on the economies, productivity and patient survival – pilot in specific disease states and geographies
OUTCOMES Create tangible vision about a new,
personalised health care system in Europe

28
Thought Starter #3: Connect PM Innovation to Business Growth
• Map and identify opportunities for the development of personalised medicine, diagnostics and biomarkers as important drivers of commercialisation, business growth and jobs creation
• Highlight advances in science, innovation and technology to engage the PM industry in dialogue with industry, business leaders and policymakers about the strategic role of health innovation in the economic recovery and future growth in Europe
• Leverage the priorities of the upcoming Irish presidency of the EU to initiate new initiatives around PM, innovation and economic growth
OUTCOMESCreate urgency about enhancing a dialogue and
initiatives across health care and business sectors to drive economic growth in Europe

29
Thought Starter #4: Build Ecosystem• Take a page from the technology industry and create an open,
social eco-system for collaboration around personalised medicine (SAP, Intel, others)
• Engage all key stakeholder groups – physicians, patients, consumers, payers, policymakers – in ongoing conversations and exchange of experiences
• Stimulate Transatlantic dialogue and networking• Sponsored by industry, but with free exchange of ideas and opinions
OUTCOMESCreate a vibrant social community for innovative
collaboration between scientists, clinicians, patients/consumers and policymakers

30
DESIRED FUTURE STAKEHOLDER PERCEPTIONS

31
Personalised healthcare is a new model that gives me the choice of the right treatment for my particular needs at the right time and empowers me to take more control over my personal health
Patient Perspective

32
Physician Perspective
Personalised healthcare is a new model that gives me the professional satisfaction of helping my patient identify risks for disease and prevent, intercept and treat disease earlier so that I can help prolong my patient’s life and quality of life

33
Policymaker PerspectivePersonalised healthcare is a new model that gives me opportunity to lead the development of new policies that improve health outcomes, enhance patient safety and longer term reduce health care spending

34
Opportunities for EPEMED and Its Members
• Conduct survey among policy and opinion elites on how to communicate about personalised medicine
• Map and identify new and disruptive ways of communicating the potential benefits of personalised medicine, for example– Humanizing the benefits– Integrating PM with personal health technology revolution– Demonstrating the economic benefits of PM– Connecting PM innovation with economic growth
• Pilot new ecosystem for multi-stakeholder engagement
• Drive Transatlantic Dialogue

35
Conclusions: Escalating Momentum• A disruptive technological innovation such as personalised medicine
requires disruptive communications and social engagement
• We need to unlock the emotional drivers and barriers to achieve broader adoption
• Integrating personal health technologies and personalised medicine represents a strategic opportunity
• It will take time, and the process is not linear, but it will happen
• It will continue to be a complex process and not always as clear as we hope… But industry innovators have a huge opportunity for escalating the momentum, leading and driving change

Discussion
Contact for further questions and discussion:Stig Albinus, APCO Worldwide, New York
36


















