

Presentation: Evaluating the Impact of Overdose … · Prevention Education and Naloxone Rescue...
18
Evaluating the Impact of Overdose Prevention Education and Naloxone Rescue Kits in Massachusetts Alexander Y. Walley, MD, MSc Boston University School of Medicine Exploring Naloxone Uptake and Use: Measuring Progress and Impact July 2, 2015 FDA White Oak Campus
Transcript of Presentation: Evaluating the Impact of Overdose … · Prevention Education and Naloxone Rescue...

Evaluating the Impact of Overdose Prevention Education and Naloxone Rescue
Kits in Massachusetts
Alexander Y. Walley, MD, MSc
Boston University School of Medicine
Exploring Naloxone Uptake and Use:
Measuring Progress and Impact
July 2, 2015
FDA White Oak Campus
Community level impact
• Naloxone kits and overdose prevention education help save lives • The harms are few • Training should not be a barrier • Populations and venues
1. Active users • Syringe access programs • Emergency Department* • Detox programs • Criminal justice-involved* • Methadone maintenance • Pharmacy and primary care*
2. Caregivers and social networks • Community meetings and support groups • Primary care providers • Pharmacy – Behind the counter, over the counter
3. First responders • Public health-public safety partnership
* Innovation and research needed
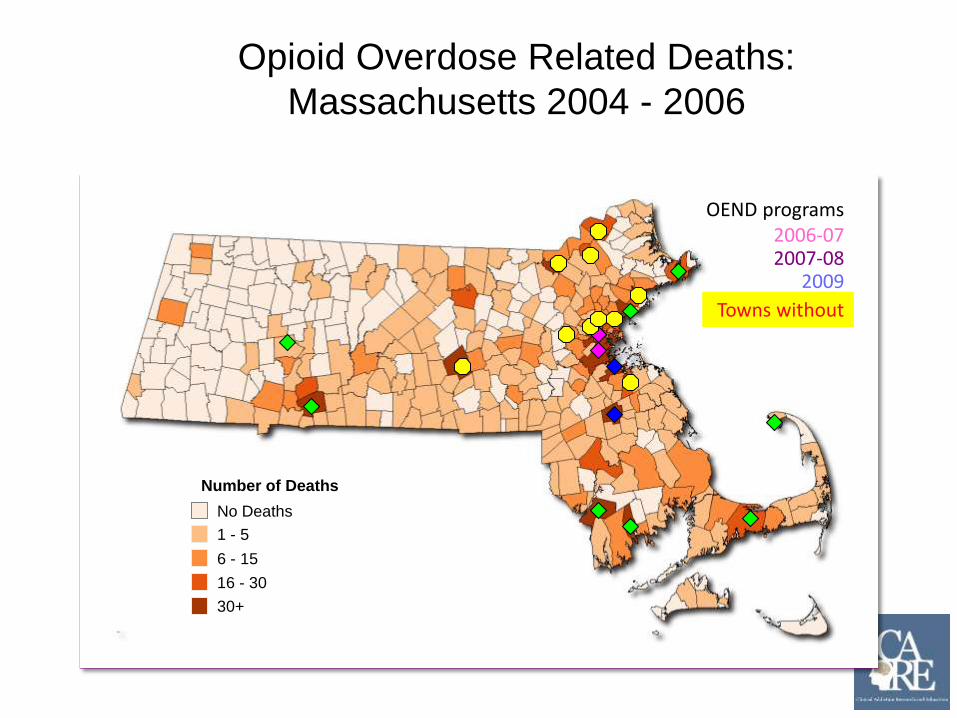
Opioid Overdose Related Deaths: Massachusetts 2004 - 2006
No Deaths
1 - 5
6 - 15
16 - 30
30+
Number of Deaths
OEND programs 2006-07 2007-08
2009
Towns without

0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
No coverage
1-100 ppl
100+ ppl
27% reduction
Fatal opioid overdose rates reduced where OEND implemented
Naloxone coverage per 100K 250
200
150
100
50
0
Opioid overdose death rate
46% reduction
Walley et al. BMJ 2013; 346: f174.

Fatal opioid OD rates by OEND implementation
Cumulative enrollments per 100k RR ARR* 95% CI
Absolute model:
No enrollment Ref Ref Ref
Low implementation: 1-100 0.93 0.73 0.57-0.91
High implementation: > 100 0.82 0.54 0.39-0.76
* Adjusted Rate Ratios (ARR) All rate ratios adjusted for the city/town
population rates of age under 18, male, race/ ethnicity (hispanic, white,
black, other), below poverty level, medically supervised inpatient withdrawal
treatment, methadone treatment, BSAS-funded buprenorphine treatment,
prescriptions to doctor shoppers, and year
Walley et al. BMJ 2013; 346: f174.
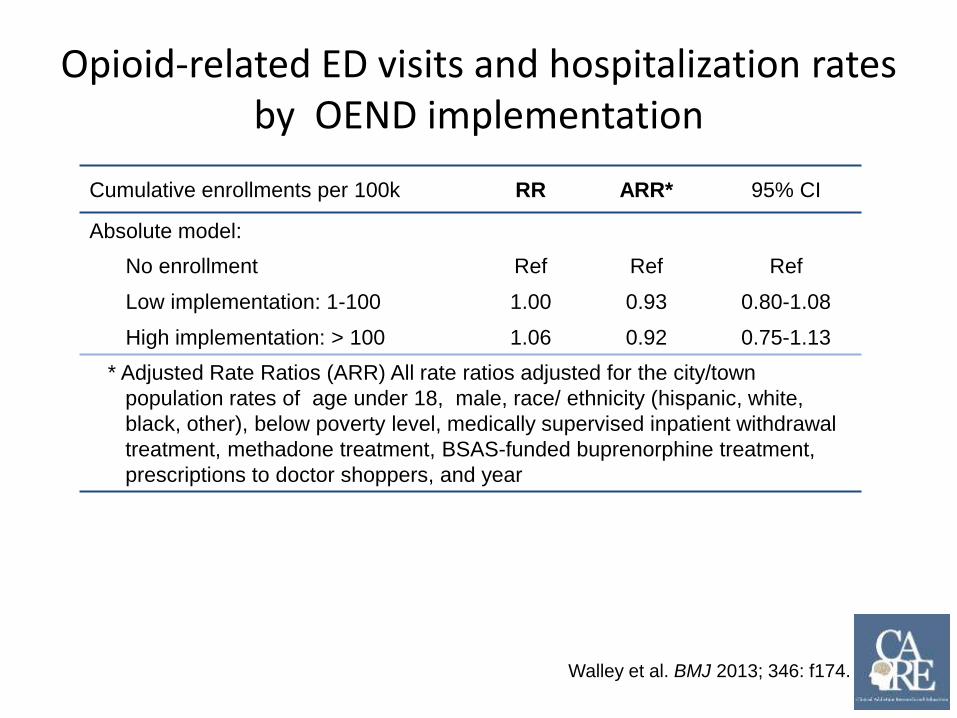
Opioid-related ED visits and hospitalization rates by OEND implementation
Cumulative enrollments per 100k RR ARR* 95% CI
Absolute model:
No enrollment Ref Ref Ref
Low implementation: 1-100 1.00 0.93 0.80-1.08
High implementation: > 100 1.06 0.92 0.75-1.13
* Adjusted Rate Ratios (ARR) All rate ratios adjusted for the city/town
population rates of age under 18, male, race/ ethnicity (hispanic, white,
black, other), below poverty level, medically supervised inpatient withdrawal
treatment, methadone treatment, BSAS-funded buprenorphine treatment,
prescriptions to doctor shoppers, and year
Walley et al. BMJ 2013; 346: f174.
INPEDE OD Study Summary
1. Fatal OD rates were decreased in MA cities-towns where OEND was implemented -
The more enrollment the more benefit
2. No clear impact on acute care utilization
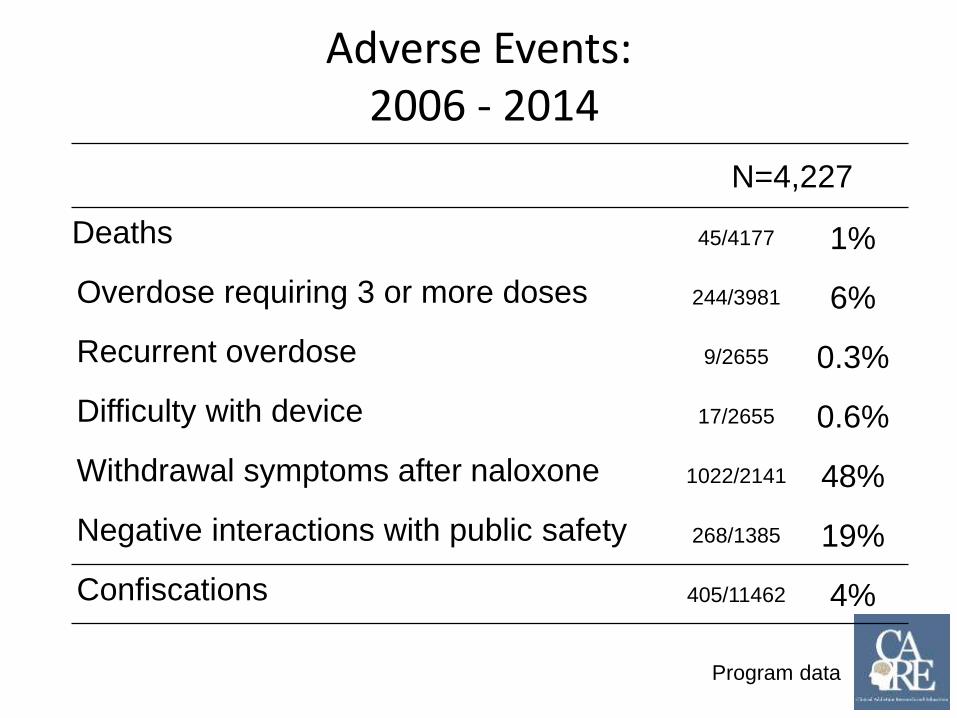
Adverse Events: 2006 - 2014
N=4,227
Deaths 45/4177 1%
Overdose requiring 3 or more doses 244/3981 6%
Recurrent overdose 9/2655 0.3%
Difficulty with device 17/2655 0.6%
Withdrawal symptoms after naloxone 1022/2141 48%
Negative interactions with public safety 268/1385 19%
Confiscations 405/11462 4%
Program data
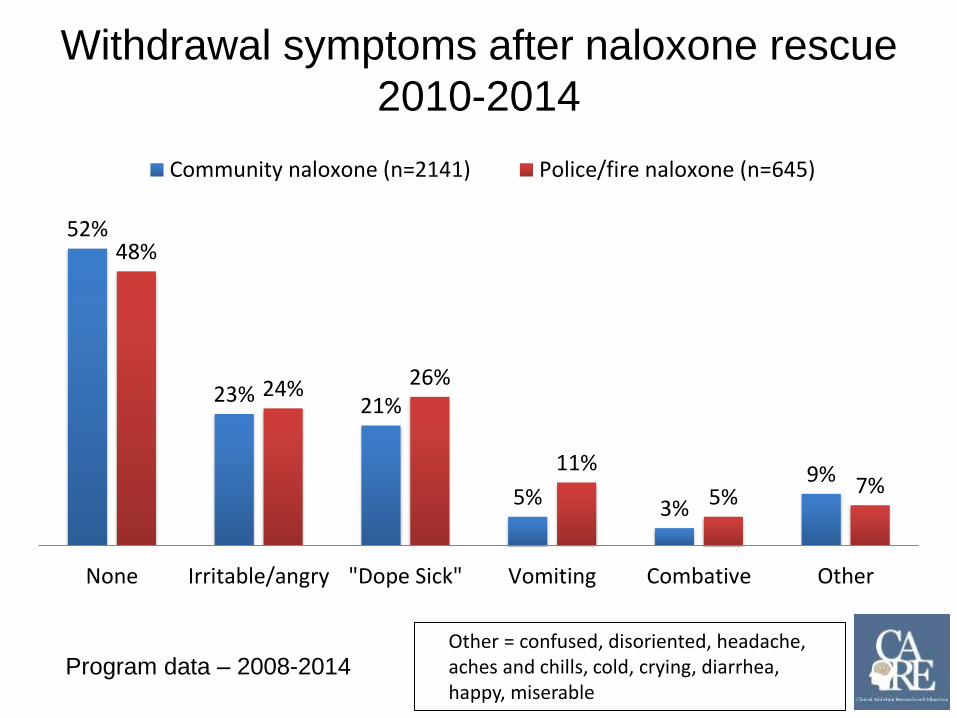
Withdrawal symptoms after naloxone rescue 2010-2014
Community naloxone (n=2141) Police/fire naloxone (n=645)
52% 48%
26%24%23% 21%
11% 9% 7%5% 5%3%
None Irritable/angry "Dope Sick" Vomiting Combative Other
Program data – 2008-2014 Other = confused, disoriented, headache, aches and chills, cold, crying, diarrhea, happy, miserable

Do trained rescuers perform differently than untrained rescuers?
Naloxone rescue after training (n=508) Naloxone rescue before training (n=91)
89% 89%
63% 62%
52%48% 47%
39%
27%23%
Sternal rub >1 dose given 911 called or Rescue Breathing Stayed with the EMS present victim
Doe-Simkins et al. BMC Public Health 2014
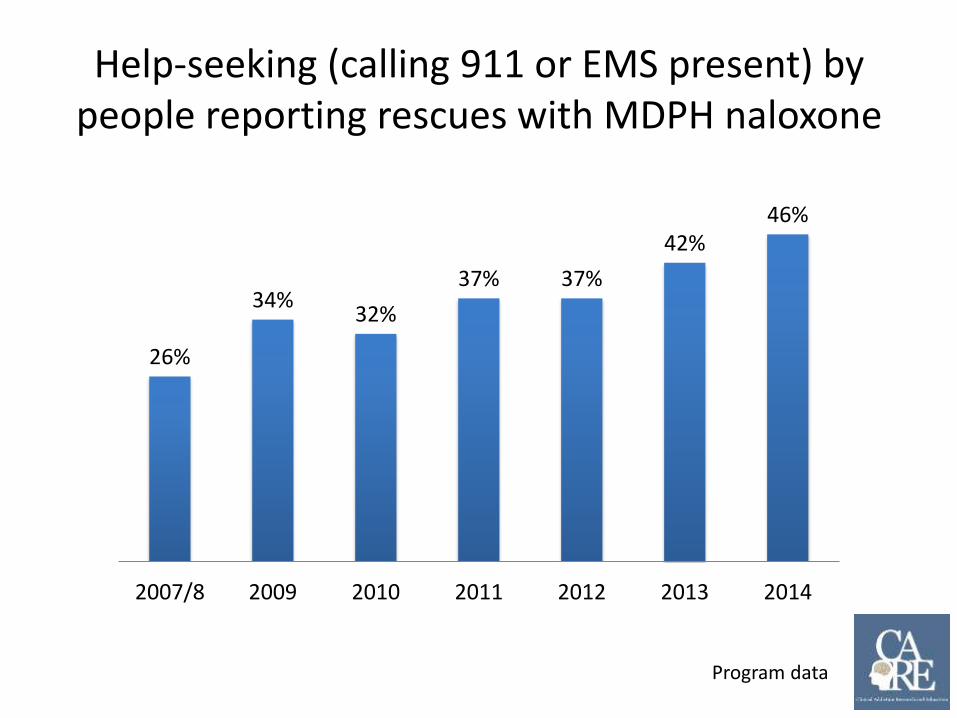
Help-seeking (calling 911 or EMS present) by people reporting rescues with MDPH naloxone
46% 42%
37% 37% 34%
32%
26%
2007/8 2009 2010 2011 2012 2013 2014
Program data

Training family members at support group meetings
Bagley et al. Overdose Education and Naloxone Rescue Kits for Family Members of Individuals Who Use Opioids: Characteristics, Motivations, and Naloxone Use. Substance Abuse 2015.

Police and Fire naloxone rescues in MA 2010-2014 Massachusetts DPH First Responder Pilot
8 67111
160
318
0
50
100
150
200
250
300
350
2010 2011 2012 2013 2014
Signsoflife,butdied Deadonarrival Rescue
Rescues and deaths, 2010-2014
Community level impact
• Naloxone kits and overdose prevention education help save lives • The harms are few • Training should not be a barrier • Populations and venues
1. Active users • Emergency Department* • Syringe access programs
• Detox programs • Criminal justice-involved*
• Methadone maintenance • Pharmacy and primary care*
2. Caregivers and social networks • Community meetings and support groups • Primary care providers • Pharmacy – Behind the counter, over the counter
3. First responders • Public health-public safety partnership

-
Evaluations of Overdose Education and Naloxone Distribution Programs
Feasibility
• Piper et al. Subst Use Misuse 2008: 43; 858-70. • Doe-Simkins et al. Am J Public Health 2009: 99: 788-791. • Enteen et al. J Urban Health 2010:87: 931-41. • Bennett et al. J Urban Health. 2011: 88; 1020-30. • Walley et al. JSAT 2013; 44:241-7. (Methadone and detox programs)
Increased knowledge and skills
• Green et al. Addiction 2008: 103;979-89. • Tobin et al. Int J Drug Policy 2009: 20; 131-6. • Wagner et al. Int J Drug Policy 2010: 21: 186-93.
No increase in use, increase in drug
treatment
• Seal et al. J Urban Health 2005:82:303-11. • Doe-Simkins et al. BMC Public Health 2014 14:297.
Reduction in overdose in
communities
• Maxwell et al. J Addict Dis 2006:25; 89-96. • Evans et al. Am J Epidemiol 2012; 174: 302-8. • Walley et al. BMJ 2013; 346: f174.
Cost-effective $438 (best)
$14,000 (worst ) per quality adjusted
life year gained
Coffin and Sullivan. Ann Intern Med. 2013 Jan 1;158(1):1-9.
16
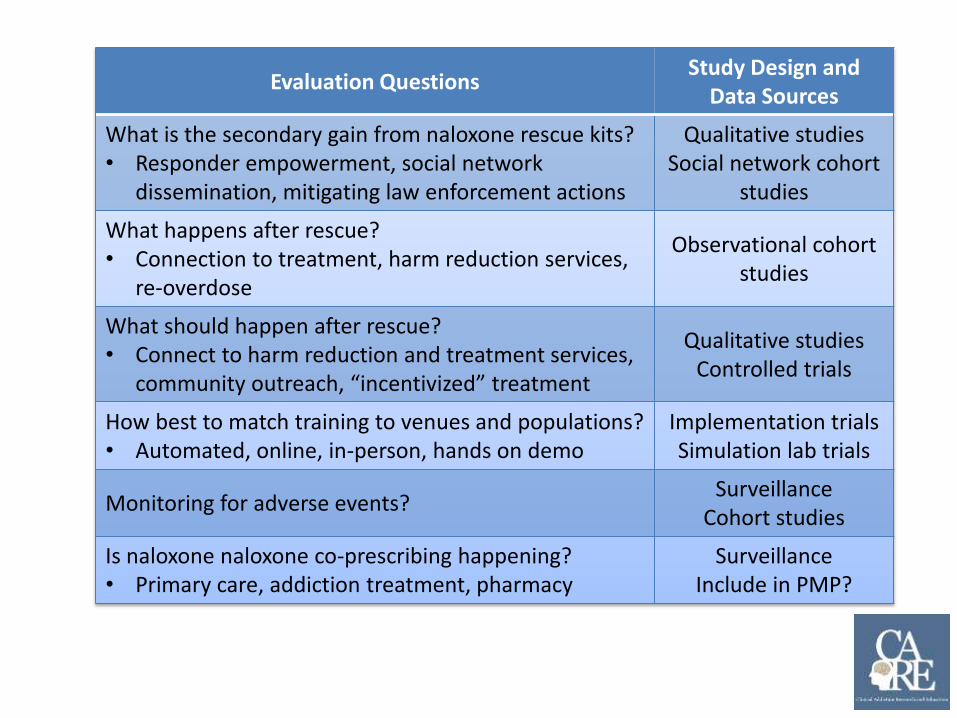
Evaluation Questions Study Design and
Data Sources
What is the secondary gain from naloxone rescue kits? • Responder empowerment, social network
dissemination, mitigating law enforcement actions
Qualitative studies Social network cohort
studies
What happens after rescue? • Connection to treatment, harm reduction services,
re-overdose
Observational cohort studies
What should happen after rescue? • Connect to harm reduction and treatment services, community outreach, “incentivized” treatment
Qualitative studies Controlled trials
How best to match training to venues and populations? • Automated, online, in-person, hands on demo
Implementation trials Simulation lab trials
Monitoring for adverse events? Surveillance
Cohort studies
Is naloxone naloxone co-prescribing happening? • Primary care, addiction treatment, pharmacy
Surveillance Include in PMP?


















