Presentation at rajkot
71
A Presentation ON CONSENSUS IN PANCREAS MANAGEMENT DR. TAPAN SHAH Dr Tapan Shah, M.S, M.Ch Fellow Digestive Surgery, UPMC, USA Ph.D ( Liver transplantation) UPMC, USA SURGICAL GASTROENTEROLOGY AND HEPATOBILIARY SURGEON in AHMEDABAD AND BARODA A Prof. & Research Fellow (USA)
-
Upload
tapan-shah -
Category
Health & Medicine
-
view
68 -
download
0
Transcript of Presentation at rajkot
A Presentation
ON
CONSENSUS IN PANCREAS MANAGEMENT
DR. TAPAN SHAH
Dr Tapan Shah, M.S, M.Ch
Fellow Digestive Surgery, UPMC, USA
Ph.D ( Liver transplantation) UPMC, USA
SURGICAL GASTROENTEROLOGY AND
HEPATOBILIARY SURGEON in AHMEDABAD AND BARODA
A Prof. & Research Fellow (USA)
LETS CUDDLE IN PANCREAS MUDDLE
Discussing few cases with pancreatic pathology
• Pancreatic fistula
• Acute pancreatitis
• Chronic pancreatitis
CASE I : PANCREATIC FISTULA
• A 54 year old man presented with anasarca, later
proved to have left adrenal gland tumor on CT scan, a
laparoscopic approach was opted and during the
surgery spleen got injured, surgeon pushed ahead with
splenectomy, later on 4th day, drain shows almost bout
500-600 ml of juices that keeps increasing and
decreasing irrelevantly.
HOW TO DEFINE PANCREATIC FISTULA
• Presence of high amylase in fluid should be
consider pancreatitis almost to 5 folds
PF is surgeon’s bane, grave where you bury alive
WHAT NEXT?
• CECT 41%
• MRCP 10%
• ERCP 49%
• FLUID AMYLASE <1%
Voss and Pappas,[1] et al 2007

MANAGEMENT OF PANCREATIC FISTULA
• Conservative
• endoscopic
• Operative
• Plugs and sclerosant ( cynoacrylate or paralime)
CONSERVATIVE MANAGEMENT
• Naso Jejunostomy or feeding jejunostomy enteral feeding or total parenteral nutrition,
• nasogastric suction,
• imaging-guided percutaneous drainage of collection when necessary
• and somatostatin or its analogues.
• Correction of electrolyte imbalance
• Prophylaxis for secondary infection
ENDOSCOPIC PROCEDURES
• Cant be done
• Dislocated duct syndrome
• Island of pancreas
• Best done in
• Small disruption
• Tail disruption ( distal pancreatectomy)
WEIRD TECHNIQUES BUT WORKS
• percutaneous embolization using a sclerosing substance, prolamine, injected into the Wirsung duct via drainage catheter.
• Injection of cyanocarylate into external fistulous tracts
• Temporary fibrin glue occlusion pre operatively of main pancreatic duct
SURGERY
• RESECTION
• Generally opted
• With or without enterostomy
• ENTEROSTOMY
• Multiple
• Body generally involved or head involvement
CASE 2
• A 41 years old alcoholic male presented with
severe pain in abdomen with nausea and
vomiting. During all the investigation pateint was
found to have raised lipase , with tachcardia and
low blood volume, how would we manage him?
OVERVIEW OF ACUTE PANCREATITIS
• 85% of patients have interstitial pancreatitis; 15 (range 4 – 47%) have necrotizing pancreatitis
• Among patients with necrotizing pancreatitis, 33% (range 16-47%) have infected necrosis
• Approximately 10% of patients with interstitial pancreatitis experience organ failure, but in the majority it is transient
• Mortality in acute pancreatitis overall, is approximately 5%: 3% in interstitial pancreatitis, 17% in necrotizing pancreatitis
• In necrotizing pancreatitis, mortality 3-fold infected vs. sterile necrosis
• Mortality increases with development of organ failure ~ 3% (0-8%) and with multi-system organ failure 47% (range 28-69)
ACG Practice Guidelines in Acute Pancreatitis
Am J Gastroenterol 2006;101:2379-2400
ACUTE PANCREATITIS:WHAT SHOULD WE DO
1) Volume replacement is the foundation of therapy
2) Establish severity
Utilize initial laboratory data
standardized modalities i.e. Ranson criteria require 48 hrs
CT abnormalities correlate with severity
No need for early CT to establish severity
3) Establish etiology
Importance is to prevent recurrence
4) Biliary Pancreatitis
Utilize laboratory markers for diagnosis of retained CBD
ERCP is only for treating patients with cholangitis
5) Do not use prophylactic antibiotics
6) CT guided aspiration is the diagnostic test for pancreatic
infection & allows directed antibiotic therapy
7) Surgical intervention in patients with infected pancreatic
necrosis but rarely in sterile necrosis
8) Early enteral feeding is safe, prevents leaky gut and is
associated with less complications than TPN
Acute Pancreatitis:Concepts 2009
CAUSES OF MORTALITYDEATH
Early (< one week)
Systemic inflammatory response syndrome (SIRS)
Multiorgan failure
Late (> one week)
Multiorgan failure
Pancreatic infections/sepsis
SYSTEMIC INFLAMMATORY RESPONSE
SYNDROME (SIRS)
Defined by two or more of the following criteria:
Pulse > 90 beats/min
Respiratory rate > 20/min or PCO2 <32 mmHg
Rectal temperature <36° C or >38°C
White blood count <4,000 or >12,000/mm3
ACG Practice Guidelines in Acute PancreatitisAm J Gastroenterol 2006;101:2379-2400
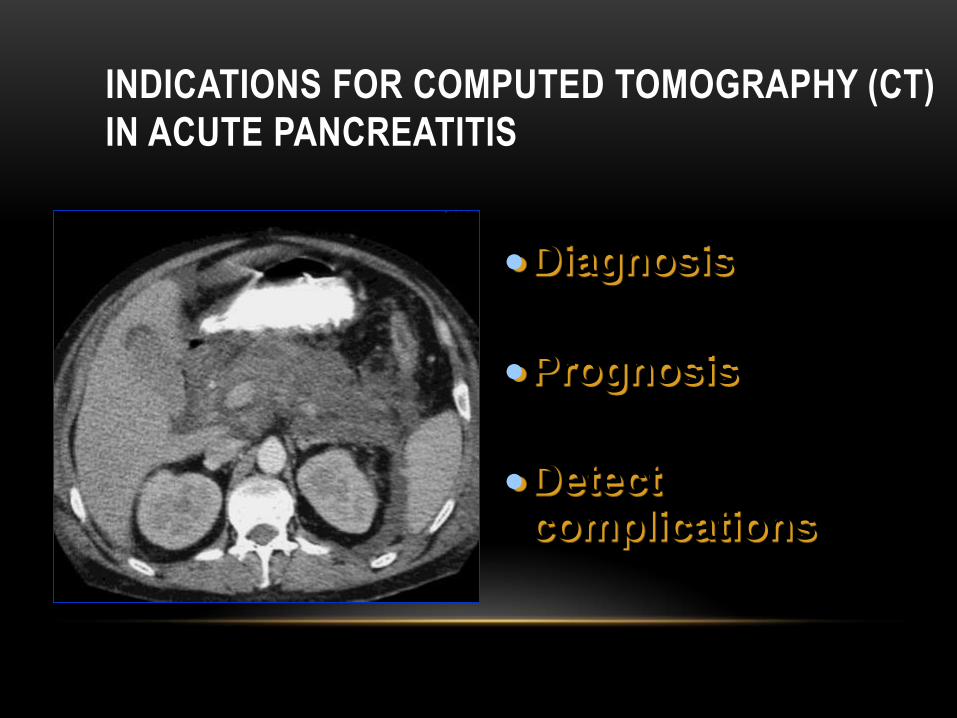
Diagnosis
Prognosis
Detect complications
INDICATIONS FOR COMPUTED TOMOGRAPHY (CT)
IN ACUTE PANCREATITIS
WHEN TO DO CT
Contrast-Enhanced CT Scan
Not on admission if diagnosis is determined -
• A few days (5-7days)after admission to distinguish interstitial
from necrotizing pancreatitis when there is clinical evidence of
increased severity. Level of Evidence III
• To guide aspiration in patients with fluid collection to determine
if infected
• When patient is deteriorating
COMPUTED TOMOGRAPHY AND MAGNETIC RESONANCE
IMAGING IN THE ASSESSMENT OF ACUTE PANCREATITIS
Method: MRI was performed with intravenous secretin and contrast medium
Results
• EQUAL RESULTS
• Costly
• To be opted when patient having contra indication of contrast dye
Arvanitakis M, et al. Gastroenterology 2004;126(3):715-23
DIAGNOSTIC GUIDELINE III
DETERMINATION OF SEVERITY DURING HOSPITALIZATION
Contrast-Enhanced CT Scan
Not on admission if diagnosis is determined -
• A few days after admission to distinguish interstitial from
necrotizing pancreatitis when there is clinical evidence of
increased severity. Level of Evidence III
• To guide aspiration in patients with fluid collection to
determine if infected ACG Practice Guidelines in Acute Pancreatitis
Am J Gastroenterol 2006;101:2379-2400
ACUTE IDIOPATHIC PANCREATITIS:
DOES IT REALLY EXIST OR IS IT A MYTH?Background:
• Gallstones and alcohol abuse are the most frequent
causes (75% of patients) of acute pancreatitis
• Consider hyperlipidemia, hypercalcemia and drugs
• In 10% to 40%, no cause is identified
Van Brummelen SE, et al. Scand J
Gastroenterol (Suppl) 2003;(239):117-22
MICROLITHIASIS IS THE MOST COMMON
CAUSE ACUTE IDIOPATHIC PANCREATITIS
Results:
• Microlithiasis or biliary sludge is an important cause of acute ‘idiopathic’ pancreatitis in up to 80% of patients
• Microlithiasis can be detected by trans-abdominal/endoscopic ultrasonography or polarizing light microscopy of bile
• Acute pancreatitis can be prevented by performing cholecystectomy and opening the sphincter of Oddi
Adapted from: Van Brummelen SE, et
al. Scand J Gastroenterol (Suppl)
2003;(239):117-22
CONTD:-
• Interstitial or necrotising, unidentified etiology based pancreatitis
are recommended to proceed for cholecystectomy
• Sphincterotomy &
• Long term use of ursodeoxycholic acid
Adapted from: Van Brummelen SE, et al. Scand J
Gastroenterol (Suppl) 2003;(239):117-22
BILIARY PANCREATITIS: WHAT HAPPENS TO
CBD STONES?
Stone or concretion is found in CBD
a) within 48 hours after admission in 62% – 75%
a) After 48 hours post admission CBD stones are found in 3% – 33%
The natural history of CBD stones is passage
TREATMENT GUIDELINE VIII
ROLE OF ERCP AND BILIARY SPHINCTEROTOMY IN
GALLSTONE PANCREATITIS
• Indicated for clearance of bile duct stones in patients with severe pancreatitis, in those with cholangitis
• ERCP should be performed primarily in patients with high suspicion of bile duct stones when therapy is indicated
• EUS or MRCP can be used to identify common bile duct stones
Level of Evidence: I
ACG Practice Guidelines in Acute Pancreatitis.
Am J Gastroenterol 2006;101:2379-2400
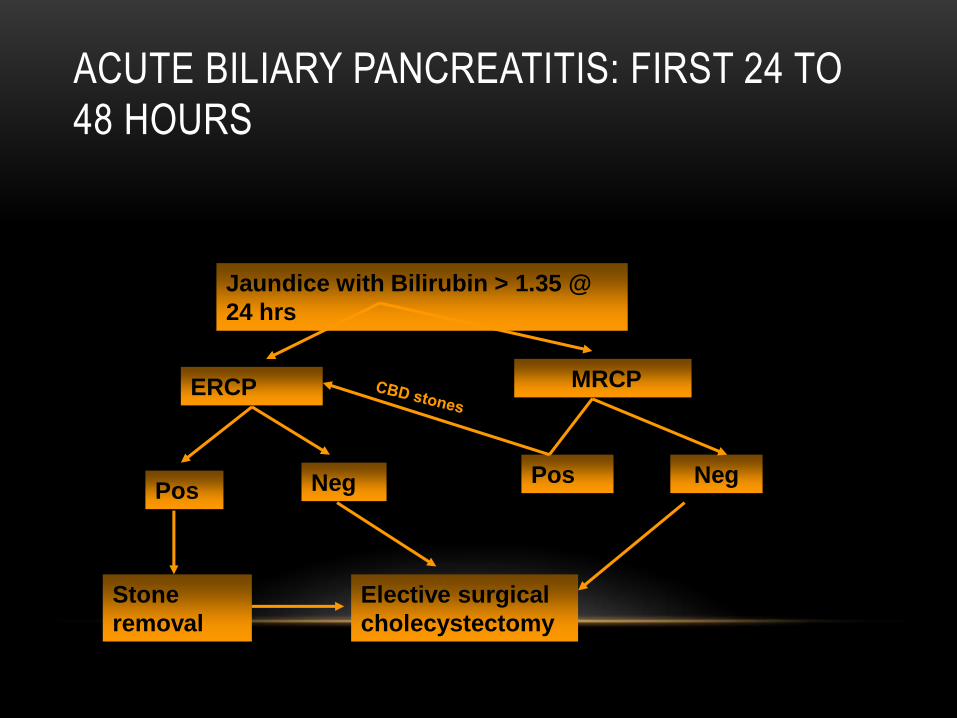
ACUTE BILIARY PANCREATITIS: FIRST 24 TO
48 HOURS
Jaundice with Bilirubin > 1.35 @
24 hrs
ERCP MRCP
PosNeg
Stone
removal
Elective surgical
cholecystectomy
Neg Pos
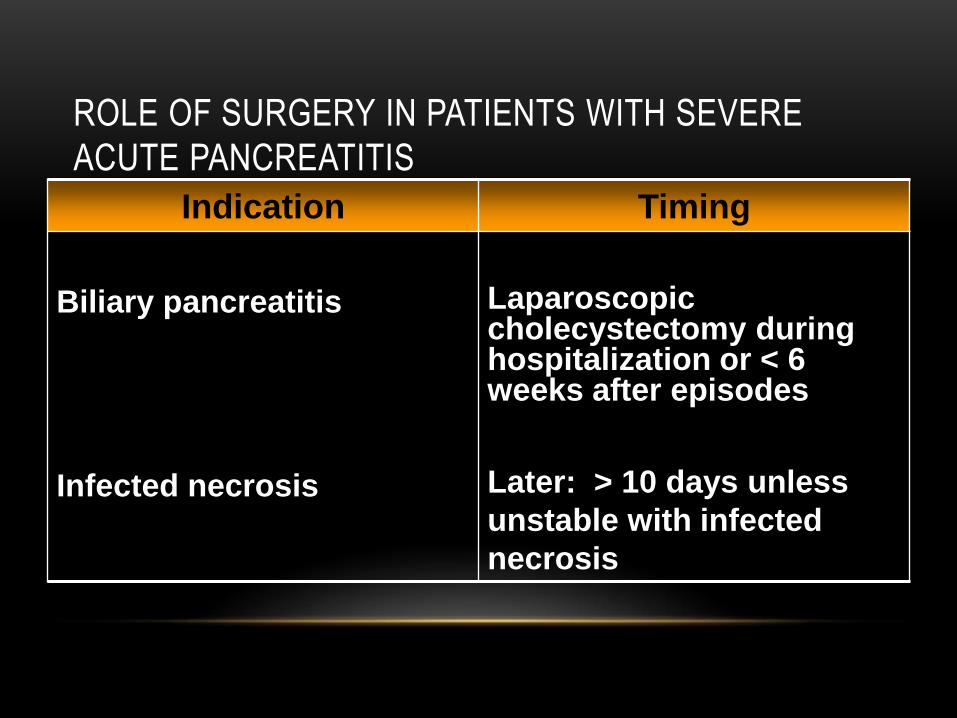
ROLE OF SURGERY IN PATIENTS WITH SEVERE
ACUTE PANCREATITIS
Indication Timing
Biliary pancreatitis
Infected necrosis
Laparoscopic cholecystectomy during hospitalization or < 6 weeks after episodes
Later: > 10 days unless
unstable with infected
necrosis
EARLY VERSUS LATE NECROSECTOMY IN SEVERE
NECROTIZING PANCREATITISPatients were randomly allocated to two treatment arms as
follows:
Group A included early necrosectomy (within 48 to 72 hours of onset)
Group B included late necrosectomy (at least 12 days after onset)
Results:
Difference in the mortality rate (58% vs. 27%) was not statistically significant, the odds ratio for mortality was much higher in the early operation group
Early surgery in severe acute pancreatitis is only required in cases with proven early infection of the pancreatic necrosis (and not stable)
Mier J, et al. Am J Surg 1997;173:71-7
Buchler MW, et al Dig Dis 1992;10:354-62
Mai G, et al Berlin, Blackwell Science 1999;475-85
ROLE OF PROPHYLACTIC
ANTIBIOTICS IN PATIENTS WITH
SEVERE ACUTE PANCREATITIS
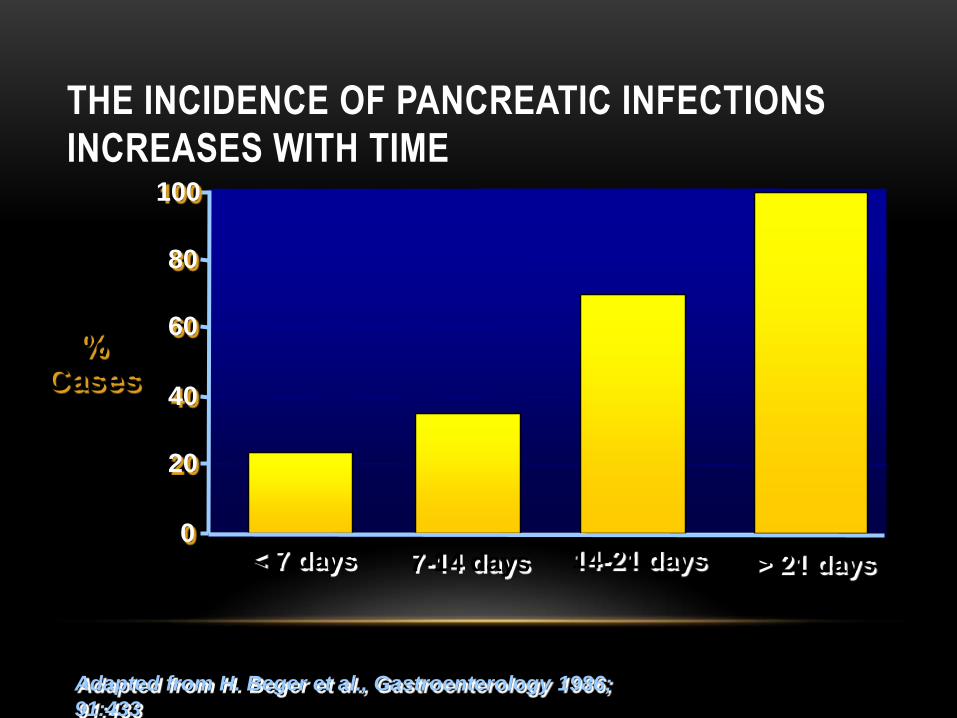
Adapted from H. Beger et al., Gastroenterology 1986;
91:433
%Cases
0
20
40
60
80
100
< 7 days 7-14 days 14-21 days > 21 days
THE INCIDENCE OF PANCREATIC INFECTIONS
INCREASES WITH TIME
LOCAL AND SYSTEMIC INFECTIONS IN ACUTE
PANCREATITIS
• After week 1, the prognosis . is mainly determined by bacterial infection of pancreatic and peripancreatic necrosis
• Mortality increases from 5% - 25% in patients with sterile necrosis to 15% - 28% in patients with infected necrosis
Rau B, et al. J Am Coll Surg 1995;181:279-288
Rau B, et al. World j Surg 1997;21:155-161
Isenmann R, et al.Br J Surg 1999;86:1020-1024
Wilson PG, et al. J Antimicrob Chemother 1998;41(suppl A):51-63
Tenner S, et al. Gastroenterology 1997;113:899-903
Buchler MW, et al. Ann Surg 2000;232:619-626
ANTIBIOTIC THERAPY FOR PROPHYLAXIS AGAINST
INFECTION OF PANCREATIC NECROSIS IN ACUTE
PANCREATITIS
Aim: to determine the effectiveness and safety of prophylactic antibiotic therapy in patients with severe acute pancreatitis who have developed pancreatic necrosis
Results
• A survival advantage for antibiotic therapy (Odds ratio 0.32, p=0.02) was demonstrated
• Pancreatic sepsis showed an advantage for therapy (Odds ratio 0.51, p=0.04)
• Extra-pancreatic infection could be evaluated in three studies, but showed no significant advantage for therapy (Odds ratio 0.47, p=0.05)
Cochrane Database Syst Rev
2003;(4):CD002941
ANTIBIOTIC THERAPY FOR PROPHYLAXIS AGAINST INFECTION
OF PANCREATIC NECROSIS IN ACUTE PANCREATITIS
(Cont)
• Surgery rates were not significantly reduced (Odds ratio 0.55, p=0.08)
• Fungal infections showed no strongly increased preponderance with therapy (Odds ratio o.83, p=0.7)
Reviewers’ Conclusion
• Strong evidence that intravenous antibiotic prophylactic therapy for 10 to 14 days decreased the risk of super-infection of necrotic tissue and mortality in patients with severe acute pancreatitis with proven pancreatic necrosis at CT
Cochrane Database Syst Rev 2003;(4):CD002941
TREATMENT GUIDELINE IVANTIBIOTICS IN NECROTIZING PANCREATITISLevel of Evidence III
• Not recommended at this time in patients with necrotizing pancreatitis
• During the first 7 – 10 days, patients with pancreatic necrosis may appear septic with leukocytosis, fever, and/or organ failure
• Antibiotic therapy is appropriate while an evaluation for a source of infection is undertaken
• Once blood and other cultures (including CT-guided fine needle aspiration) are found to be negative, discontinue antibiotic therapy
ACG Practice Guidelines in Acute Pancreatitis.
Am J Gastroenterol 2006;101:2379-2400
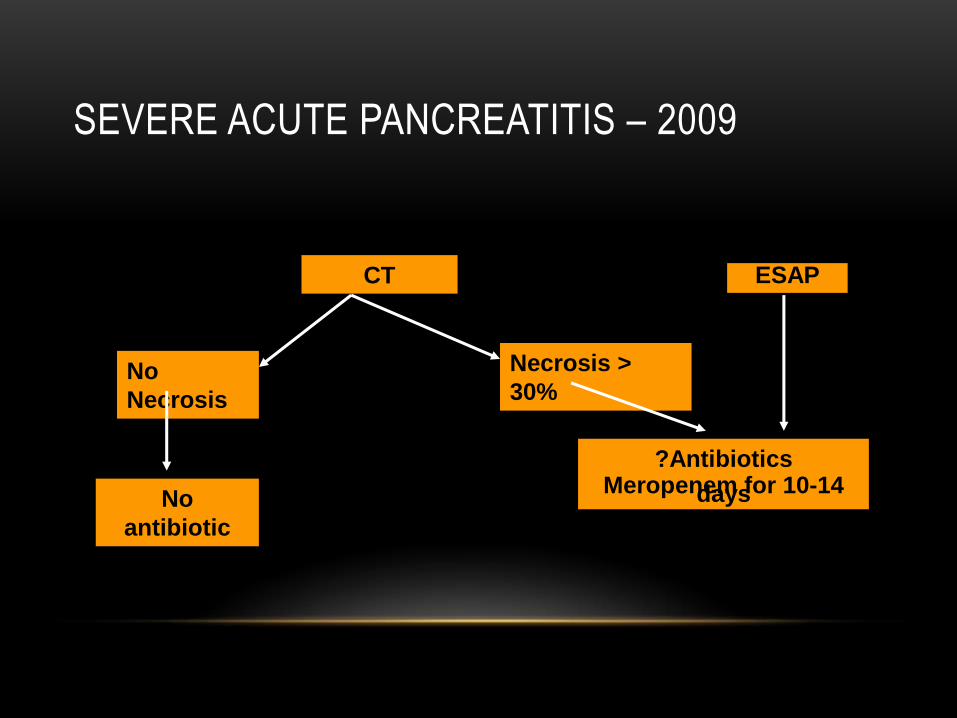
SEVERE ACUTE PANCREATITIS – 2009
CT
No
Necrosis
Necrosis >
30%
No
antibiotic
?AntibioticsMeropenem for 10-14 days
ESAP
MANAGEMENT OF PANCREATITIS PRIOR TO CT-
FNA
• The extent of leukocytosis or temperature does not
reliably distinguish severe sterile from infected
necrosis
• The development of organ failure (or multi-system
organ failure) and serum markers are not reliable
indicators of infected necrosis
Buchler MW, et al. Ann Surg 2000;232(5):619-26
Mier J, et al. Am J Surg 1997;173(2):71-5
Rau B, et al. Br J Surg 1998;85(2):179-84
SEVERE ACUTE PANCREATITIS: ROLE OF CT-GUIDED
NEEDLE ASPIRATIONInfected Necrosis
Suspicion
Tº > 100 F
elevated WBC
unresolved organ failure
Recurrence of SIRS or persistence > 7 days
Diagnosis
CT guided aspirate for gram stain and Culture and sensitivity
PERCUTANEOUS ASPIRATION OF PANCREATIC
FLUID COLLECTION – GRAM STAIN AND CULTURE
10% aspirate gram stain negative and culture positive
No history of antibiotic administered
Aspirant gram stain positive with negative cultures in 2 of
34 (6%) patients
Effect of antibiotics on aspirate
Barkin JS, et al. Dig Dis Sci 1981;26(7):585Freeny PC, et al AJR 1998;170:969-975
TREATMENT GUIDELINE V:
TREATMENT OF INFECTED NECROSIS
• CT-guided percutaneous aspiration with Gram’s stain and
culture aspirate is recommended when infected necrosis is
suspected
• Treatment of choice in infected necrosis is surgical
debridement
Level of Evidence III
ACG Practice Guidelines in Acute Pancreatitis.
Am J Gastroenterol 2006;101:2379-2400

TPN
Cost – high
No pancreas stimulation
Increased infections
Electrolyte disturbances
Detrimental to gut integrity
Enteral
Cost – moderate
May stimulate pancreas
Reduced infections
Electrolytes undisturbed
May retain gut integrity
ROUTE OF ALIMENTATION
TOTAL PARENTERAL NUTRITION (TPN) AND
ENTERAL NUTRITION (EN)
TPN – causes intestinal mucosal atrophy alterations in
the gut associated lymphoid tissue (GALT) system
and a reduction in intestinal secretory IgA (S-IgA)
levels
EN – prevents hypermetabolism, maintains immunocompetence and improves wound healing; considered to reduce septic complications, shorten hospital stay and reduce the risk of death
Levine GM, et al Gastro 1974:67:975King BK, et al. Arch Surg
Kudsk KA, et al Ann Surg 1996:223:629Mochizuk H, et al Ann Surg 1984;200:297-310
Alverdy J, et al. Ann Surg 1985;202:681Schroeder D, et al JPEN 1991;15:376
Moore FA, et al. J Trauma 1989;29:916.
TREATMENT GUIDELINE III
NUTRITIONAL SUPPORT
• Enteral feeding rather than total parenteral nutrition is
suggested for patients who require nutritional support
Level of Evidence II
• In severe necrotizing pancreatitis (especially when most or all
of the pancreas is necrotic) provide potent pancreatic
enzymes and then evaluate later in the course
• It is prudent to use a proton pump inhibitor because of the
likelihood that bicarbonate secretion by the pancreas is
severely diminished ACG Practice Guidelines in Acute Pancreatitis
Am J Gastroenterol 2006;101:2379-2400
TREATMENT GUIDELINE I:
SUPPORTIVE CARE
Level of Evidence III
1. Carefully monitored during the first 24 h of vital signs, oxygen saturation and fluid balance - hypoxemia and inadequate fluid resuscitation may be unrecognized for prolonged periods of time
Result: Early aggressive fluid resuscitation and improved delivery of
oxygen prevent or minimize pancreatic necrosis and improve
survival
2. Consequence of hypovolemia is intestinal ischemia, which increases
intestinal permeability to bacteria and endotoxin
Result: Translocation of bacteria cause secondary pancreatic infection
and contribute to on-going pancreatic injury and also to organ
failure
ACG Practice Guidelines in Acute Pancreatitis
Am J Gastroenterol 2006;101:2379-2400
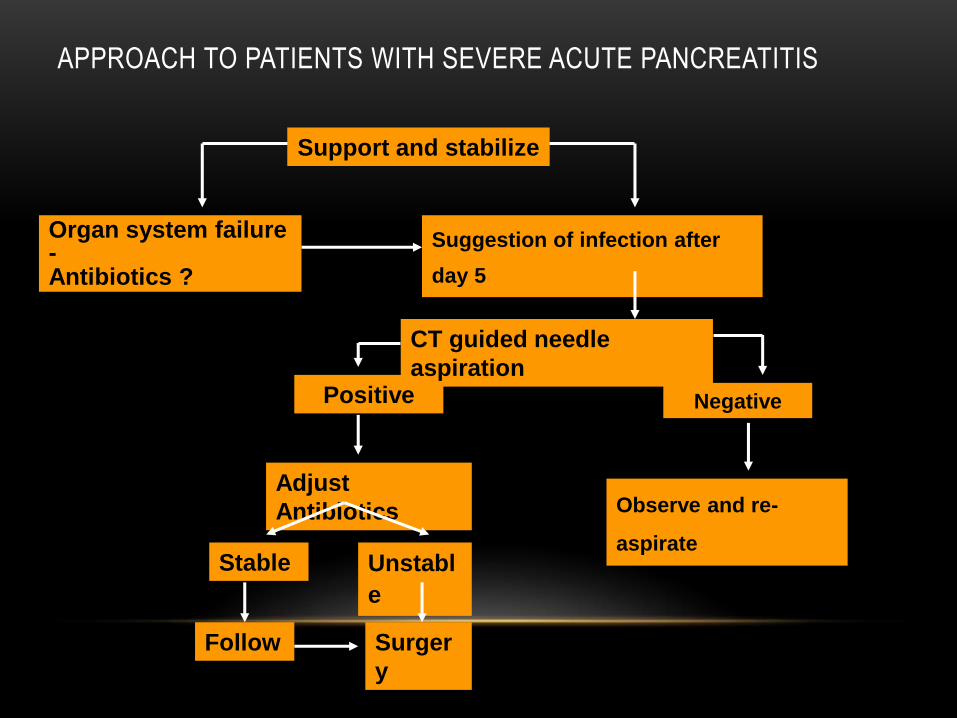
Positive
Suggestion of infection after
day 5
Support and stabilize
APPROACH TO PATIENTS WITH SEVERE ACUTE PANCREATITIS
Negative
Observe and re-
aspirate
Organ system failure -Antibiotics ?
CT guided needle
aspiration
Adjust
Antibiotics
Stable
Follow
Unstabl
e
Surger
y
CHRONIC PANCREATITIS
• Defined as chronic inflammatory condition that causes irreversible damage to pancreatic
structure and function
• Causes: ETOH abuse, malnutrition, hyperPTH, pancreas divisum, ampullary stenosis,
cystic fibrosis, hereditary, trauma, idiopathic
CHRONIC PANCREATITIS
• Chronic pancreatitis results in interstitial inflammation w/duct obstruction and dilation
leading to parenchymal loss and fibrosis.
• Loss of both exocrine and endocrine
• Clinicically significant malabsorption occurs when 90% of pancreas is lost.
CHRONIC PANCREATITIS
• Pathophys - irreversible parenchymal destruction leading to pancreatic dysfunction
• Persistent, recurrent episodes of severe pain
• Anorexia, nausea
• Constipation, flatulence
• Steatorrhea
• Diabetes
CHRONIC PANCREATITIS
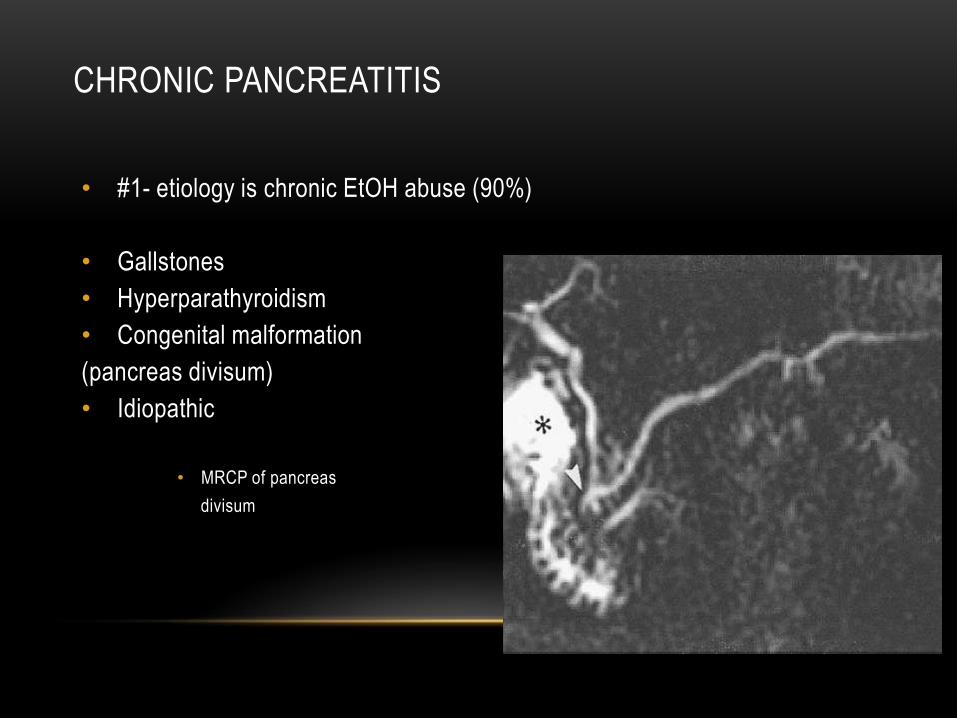
• #1- etiology is chronic EtOH abuse (90%)
• Gallstones
• Hyperparathyroidism
• Congenital malformation
(pancreas divisum)
• Idiopathic
• MRCP of pancreas
divisum
MANAGEMENT
• Medical
• Analgesic ( opiods and non opiods)
• Enzyme replacement
• Endotherapy
• Surgery
• Intraventional radiology

ENZYME REPLACEMENT
• DOES THE TYPE MATTERS?
• ACID PROTECTIVE
• SIZE OF THE DELIVERY SUBSTANCES
First, prior endoscopic treatment
SOME PRINCIPLES……..
ENDOSCOPIC TREATMENT
OF CHRONIC PANCREATITIS
PRINCIPLE 2:
TO TREAT ONLY IN CASE OF SYMPTOMS AND COMPLICATIONS
• Pain: yes
• Pseudocyst: yes if symptoms or complications
• Fistula: yes
• Biliary stenosis: +/- discussed
• Duodenal stenosis: no
• Vascular stenosis (portal vein, splenic vein): no
• Pancreatic exocrine function: +/- discussed
• Diabetes: no
PAIN
Endoluminal Stenting
Aim: drainage of the main pancreatic duct (wirsung,santorini)
Bases: results of surgical bypass
Immediate effect on pain: 70-90%
(Sarles 82, Bradley 87, Longnecker 96, Prinz 90)
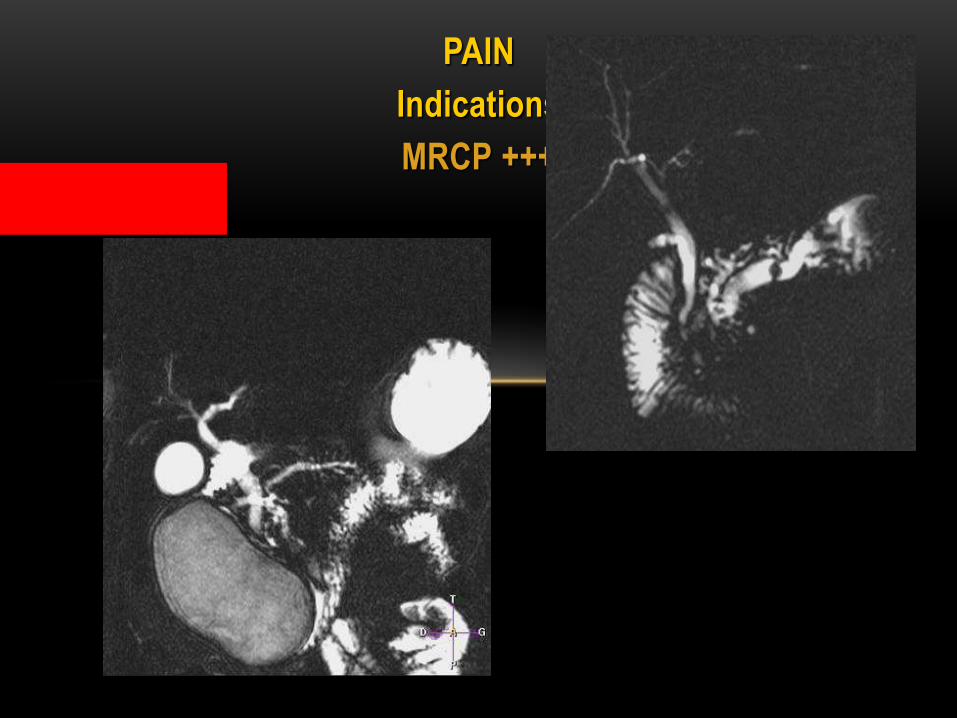
PAIN
Indications
MRCP +++
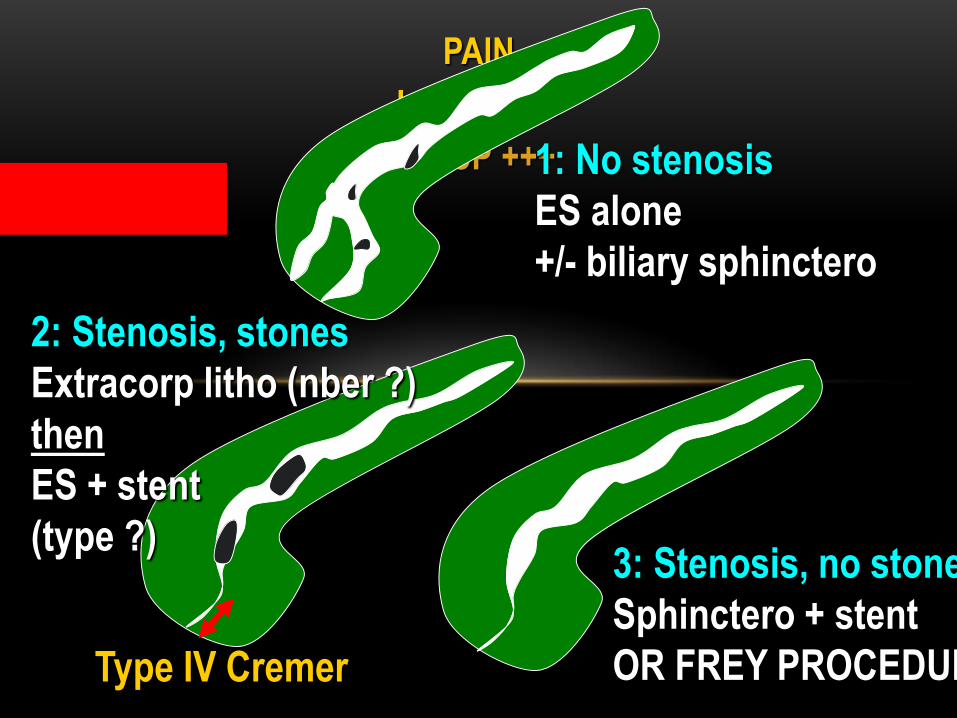
PAIN
Indications
MRCP +++1: No stenosis
ES alone
+/- biliary sphinctero
3: Stenosis, no stones
Sphinctero + stent
OR FREY PROCEDURE
2: Stenosis, stones
Extracorp litho (nber ?)
then
ES + stent
(type ?)
Type IV Cremer
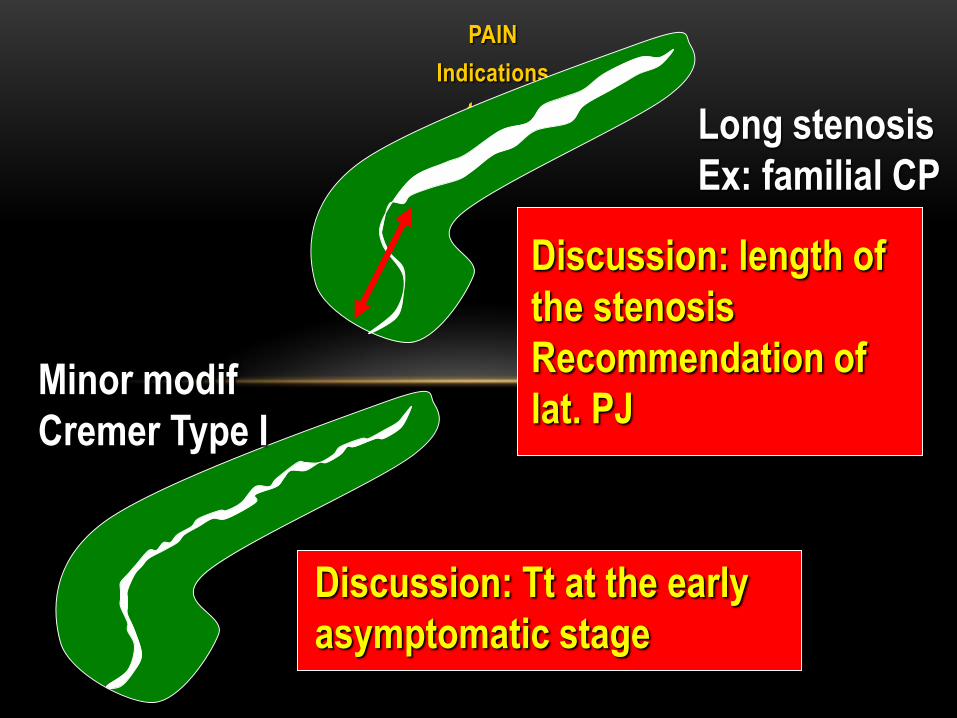
PAIN
Indications
to be
discussedLong stenosis
Ex: familial CP
Discussion: length of
the stenosis
Recommendation of
lat. PJMinor modif
Cremer Type I
Discussion: Tt at the early
asymptomatic stage
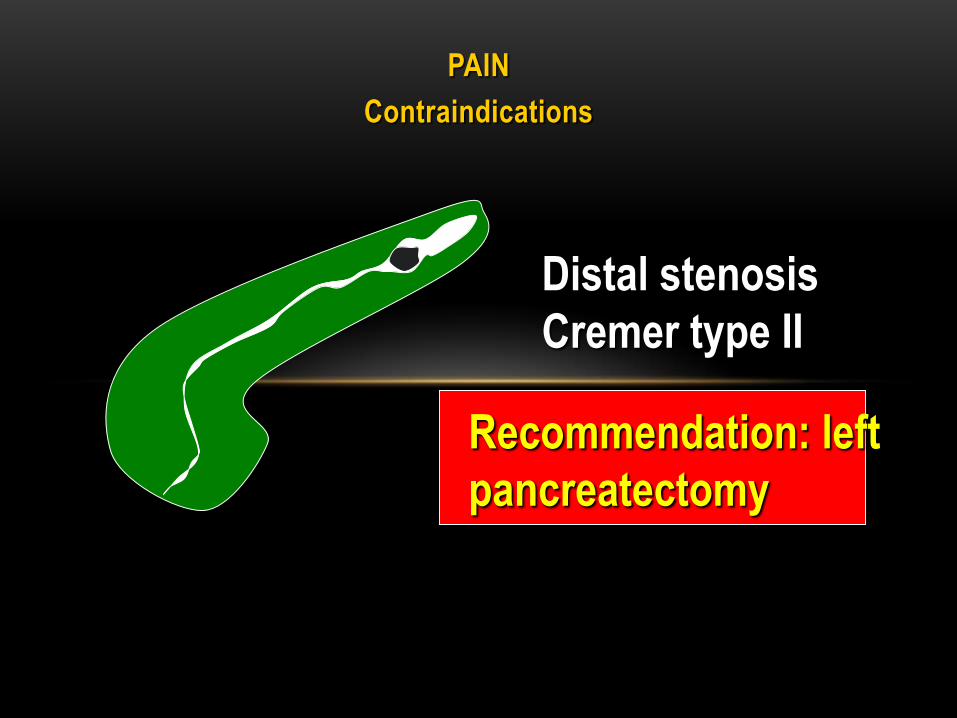
PAIN
Contraindications
Distal stenosis
Cremer type II
Recommendation: left
pancreatectomy
PAIN: ResultsIn the absence of prospective studies,
in the absence of randomized studies,
analysis of the literature is difficult:
Role of abstinence from alcohol ?
Role of medical therapy: enzymes ?
Variable presentation of pain (chronic, attacks)
Role of the complications (pseudocyst, bile duct) ?
Fragile psychology of the patient
Different endoscopic treatments
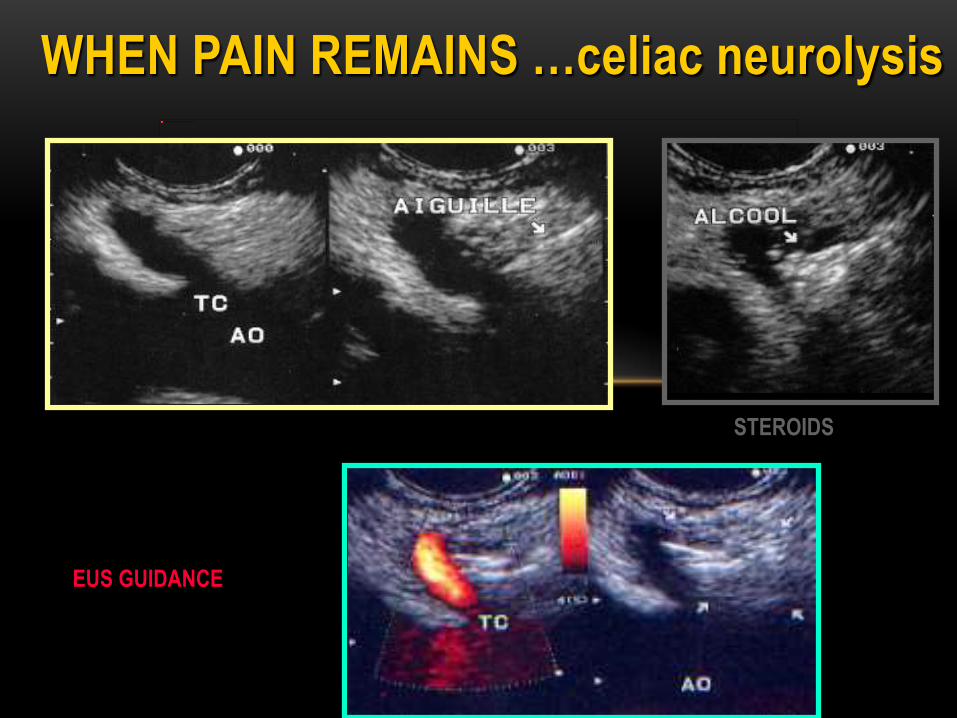
WHEN PAIN REMAINS …celiac neurolysis
EUS GUIDANCE
STEROIDS
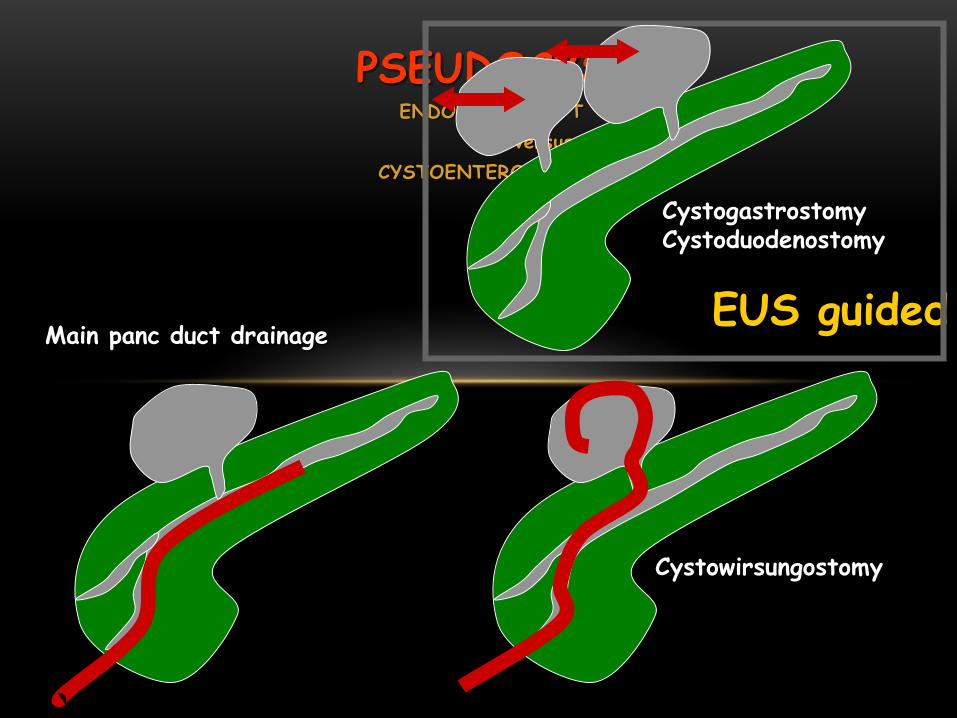
PSEUDOCYSTENDOLUMINAL TT
versus
CYSTOENTEROSTOMY
CystogastrostomyCystoduodenostomy
Cystowirsungostomy
Main panc duct drainageEUS guided

by drtapan
PANCREAS SURGERY PHOTO ALBUM


THANK
YOU!