Presentación de PowerPoint · TFST (time from randomisation to first subsequent therapy or death)...
105
BASES RACIONALES DEL USO DE TRATAMIENTOS SISTÉMICOS EN CÁNCER DE OVARIO CON BRCA MUTADOS Dr. Gonzalo H Giornelli 20 de abril, 2018. Códoba, Argentina.
Transcript of Presentación de PowerPoint · TFST (time from randomisation to first subsequent therapy or death)...

BASES RACIONALES DEL USO DE TRATAMIENTOS SISTÉMICOS EN CÁNCER DE OVARIO CON BRCA MUTADOSDr. Gonzalo H Giornelli20 de abril, 2018. Códoba, Argentina.

EN QUÉ ES DEFICIENTE EL CÁNCER DE OVARIO BRCA MUT?
DEFICIENCIA EN RECOMBINACIÓN HOMÓLOGA

Cáncer de ovario: neoplasia heterogénea

Ovarian cancer: ”caos genético”
1 2 3 4 5
6 7 8 9 10 11
12 13 14 15 16 17 18
19 20 21 22 X
1 2 3 4 5
1 2 3 4 5
6 7 8 9 10 11 12
13 14 15 16 17 18
19 20 21 22 X
1 2 3 4 5
12 13 14 15 16 17 18

DEFICIENCIA EN LA RECOMBINACIÓN HOMÓLOGA EN CÁNCER DE OVARIO
50% OF HGSOC HAVE SOME MUTATION RESULTING IN HOMOLOGOUS
RECOMBINATION DEFFICIENT (HRd) PHENOTYPE.

MECANISMOS DE REPARACIÓN DEL ADN EN CÉLULAS NORMALES

G T
A
C
G
T
A
C
G C
G
T
A
C
G
T
A
T
A
C
T
AC
GT
AC
G
G T
A
C
G
T
A
C
G C
G
T
A
C
G
T
A
T
A
C3’
5’ 3’
5’
P PP
MRN
CHK 1 CHK 2
Cdc 25
P
CHECK POINT ACTIVATION CELL-CYCLE ARREST
T
AC
GT
AC
G
P P
P
p53
p21 BAX
P
APOPTOSIS
H2AXH2AX
FAFA
FA
RAD51RAD51RAD51
RAD51 RAD51 RAD51
G
T
A
TC
T
AC
G T
A
T
AC
GG C
AGG
T
G
T
A
C
Complex senses damage
Recruitmaint/activation ATM
HOMOLOGOUS RECOMBINATION
©Dr Juan Pablo Sade

NHEJ en HRd luego de daño por CARBOPLATINO al DNA

NHEJ en HRd luego de daño por CARBOPLATINO al DNA

NHEJ en HRd luego de daño por CARBOPLATINO al DNA

DSB
BRCA defficient cell
NHEJ-loss of genetic materialgenetic instability
BRCA1
HRd creates LSST Apoptosis
KU
DNA PK
HRD EN CO BRCAmut.Consecuencias: LSST, NHEJ, TAI
©Dr Juan Pablo Sade
BRCA defficient cell

OC:” genetic chaos”
1 2 3 4 5
6 7 8 9 10 11
12 13 14 15 16 17 18
19 20 21 22 X
1 2 3 4 5
1 2 3 4 5
6 7 8 9 10 11 12
13 14 15 16 17 18
19 20 21 22 X
1 2 3 4 5
12 13 14 15 16 17 18

Por qué es importante conocer el status de BRCA?
• Consejo genético.
• Las mutaciones de BRCA 1 & 2 son pronósticas
• Comprensión de la biología de la enfermedad.
• Impacto en el tratamiento.Respuesta a platino y otros agentes
• Sensibilidad a PARPii.

Por qué es importante conocer el status de BRCA?
• Consejo genético.
• Las mutaciones de BRCA 1 & 2 son pronósticas
• Comprensión de la biología de la enfermedad.
• Impacto en el tratamiento.Respuesta a platino y otros agentes
• Sensibilidad a PARPii.

BRCA 1 & 2 ASSOCIATED OVARIAN CANCER
HEREDITARY OVARIAN CANCER






Por qué es importante conocer el status de BRCA?
• Consejo genético.
• Las mutaciones de BRCA 1 & 2 son pronósticas
• Comprensión de la biología de la enfermedad.
• Impacto en el tratamiento.Respuesta a platino y otros agentes
• Sensibilidad a PARPi.

Germline BRCA ½ mutations are prognostic

Por qué es importante conocer el status de BRCA?
• Consejo genético.
• Las mutaciones de BRCA 1 & 2 son pronósticas
• Comprensión de la biología de la enfermedad.
• Impacto en el tratamiento.Respuesta a platino y otros agentes
• Sensibilidad a PARPii.

Por qué es importante conocer el status de BRCA?
• Consejo genético.
• Las mutaciones de BRCA 1 & 2 son pronósticas
• Comprensión de la biología de la enfermedad.
• Impacto en el tratamiento.Respuesta a platino y otros agentes
• Sensibilidad a PARPi.

Prediction/ comprehension on disease behaviour.

Por qué es importante conocer el status de BRCA?
• Consejo genético.
• Las mutaciones de BRCA 1 & 2 son pronósticas
• Comprensión de la biología de la enfermedad.
• Impacto en el tratamiento.Respuesta a platino y otros agentes
• Sensibilidad a PARPi.

Por qué es importante conocer el status de BRCA?
• Consejo genético.
• Las mutaciones de BRCA 1 & 2 son pronósticas
• Comprensión de la biología de la enfermedad.
• Impacto en el tratamiento.Respuesta a platino y otros agentes
• Sensibilidad a PARPi.

Respuesta a platino y otros agentes
Effect of platinum-based cemotherapy in BMOC

ORR a QT basada en platino BRCAmut vs BRCAwt

Respuesta a Trabectidina/ PLD

Respuesta a PLD (doxorrubicina liposomal)
0 10 20 30 40 50 60 70 80
ORR
PFS
ORR
PFS
BRCA wt
BRCA m
Safra et alN=40
Adams et alN=23
PFS 7,1 m

Por qué es importante conocer el status de BRCA?
• Consejo genético.
• Las mutaciones de BRCA 1 & 2 son pronósticas
• Comprensión de la biología de la enfermedad.
• Impacto en el tratamiento. Respuesta a platino y otros agentes
• Sensibilidad a PARPii.

Por qué es importante conocer el status de BRCA?
• Consejo genético.
• Las mutaciones de BRCA 1 & 2 son pronósticas
• Comprensión de la biología de la enfermedad.
• Impacto en el tratamiento. Respuesta a platino y otros agentes
• Sensibilidad a PARPii.

PARP INHIBITORSOLAPARIB-NIRAPARIB-RUCAPARIB

Clasificación de PARPi

SSB
PARP
PARP y BER
©Dr Juan Pablo Sade

SSB
PARPPARPi
PARPi.Mecanismo de acción
DSB
©Dr Juan Pablo Sade

PARP Inhibitors and Homologous Recombination repair of DNA damage
Survival
Normal cell
Repair by Homologous Recombination
During the replication process unrepaired SSBs are converted into DSBs
Replicating cells
DNA SSBs occur all the time in cells and PARP detects and repairs them
PARP
No effective repair
(No HR pathway)
Cell death
Cancer cell with HRD
Tumour specific
killing by PARP
inhibitor

OC:” genetic chaos”
1 2 3 4 5
6 7 8 9 10 11
12 13 14 15 16 17 18
19 20 21 22 X
1 2 3 4 5
1 2 3 4 5
6 7 8 9 10 11 12
13 14 15 16 17 18
19 20 21 22 X
1 2 3 4 5
12 13 14 15 16 17 18

Farmer et al Nature 2005
INHIBIDORES DEL PARPPoly(ADP-ribose) polymerase y reparación de DNA
• PARP is a key regulator of DNA damage repair
processes
• Involved in DNA base-excision repair (BER)
• Binds directly to DNA damage
• Produces large branched chains of poly(ADP-ribose)
• Attracts and assists BER repair effectors
DNA Repair Defect
Homologous Recombination Deficiency

Olaparib (AZD2281)Phase I/II trials
1. Fong et al. N Engl J Med 20092. Fong et al. J Clin Oncol 20103. Audeh et al. Lancet 2010

Olaparib en CO BRCA mutado y no-BRCA mutado
BRCA, platinum resistant or refractory
BRCA, platinum sensitive
Non-BRCA, platinum resistant or refractory
Non-BRCA, platinum sensitive
120
100
80
60
40
20
0
–20
–40
–60
–80
–100
Bes
t ch
ange
fro
m b
asel
ine
in s
ize
of
targ
et le
sio
n (
%)
120
100
80
60
40
20
0
–20
–40
–60
–80
–100
Bes
t ch
ange
fro
m b
asel
ine
in s
ize
of
targ
et le
sio
n (
%)
Ovarian BRCA
Ovarian non-BRCA
Gelmon KA, et al. Lancet Oncol 2011;12:852–61
Olaparib activity in BRCAmut
and BRCAwt
Activity greater in ‘platinum-sensitive’ compared with ‘platinum-resistant’ relapse

Mutaciones germinales y somáticas de BRCA en HGSOC
gBRCA, germline BRCA; HR, homologous recombination; sBRCA, somatic BRCA.
BRCA1 Germline
8%
BRCA2 Germline
6%
BRCA1 Somatic
3%BRCA2
Somatic3%
BRCA1 Methylation
11%
EMSY Amplification
6%PTEN Loss
5%Other HRD7%
CCNE1 Amplification
15%
MMR Germline
2%
Other 34%
HR-deficientNot HR-deficient
gBRCA-mutated14%
HR-deficient 30%
sBRCA-mutated6%
Levine, D. Personal communication;

PARP I Y SENSIBILIDAD A PLATINO

N
Plat sens 13
Plat resist 24
Plat refr 13
TOTAL 50
STUDY 9

STUDY 9

PARP I EN LA FASE DE MANTENIMIENTO

Qué es la “fase de mantenimiento”?

“ESTUDIO 19” Fase II Randomisado de mantenimiento con olaparib en CO seroso de alto grado, recaída platino-sensible.
• Aim: to assess the efficacy and safety of olaparib as a maintenance treatment
• Design: randomized, double-blind, placebo-controlled phase II maintenance study
265 patients in 82 investigational sites in 16 countries
Olaparib
400 mg po bid
Randomised 1:1
Placebo
po bid
Patients:
• Platinum-sensitive high-grade serous ovarian
cancer
• 2 previous platinum regimens
• Last chemotherapy was platinum-based, to which
they had a maintained PR or CR prior to enrolment
• Stable CA-125
Treatment
until
disease
progression
Primary end point: PFSSept 2008–Feb 2010bid, twice daily; CA-125, Cancer Antigen 125; CR, complete response; po, orally; PR, partial response.
Ledermann J et al. N Engl J Med 2012;366:1382–1392

PFS - ‘Study 19’ olaparib mantenimiento
136 104 51 23 6 0 0
129 72 23 7 1 0 0
At risk (n)
Olaparib
Placebo
0
Time from randomisation (months)
0.6
0.8
0.9
0
0.1
0.2
0.3
0.4
0.5
0.7
1.0
3 6 9 12 15 18
Placebo
Olaparib 400 mg bid
Randomised treatment
Pro
po
rtio
n o
f p
atie
nts
pro
gre
ssio
n fre
e
After 153 progression events (57.7% of
patients) the study met its primary
endpoint of a statistically significant PFS
benefit in the overall study population
CI, confidence interval; HR, hazard ratio.
Ledermann J et al. N Engl J Med 2012;366:1382–1392
Olaparib (n=74)Placebo
(n=62)
Events/total
patients (%)60/136 (44.1) 93/129 (72.1)
Median PFS,
months 8.4 4.8
HR=0.35 95% CI: 0.25, 0.49; P<0.001

PFS - ‘Study 19’ olaparib maintenanceen pacientes con BRCAm:
Olaparib BRCAm
Placebo BRCAm
74 59 34 15 5 0
62 35 13 2 0 0
0
Time from randomisation (months)
0
1.0
Pro
po
rtio
n o
f p
atie
nts
pro
gre
ssio
n-f
ree
3 6 9 12 15
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
Number at risk
Olaparib BRCAm
Placebo BRCAm
NC, not calculable.
Ledermann J et al. Lancet Oncol 2014;15:852–861
BRCAm subgroup (n=136)
Olaparib (n=74)Placebo
(n=62)
Events/total
patients (%)26/74 (35%) 46/62 (74%)
Median PFS,
months (95% CI)
11.2
(8.3, NC)
4.3
(3.0, 5.4)
HR=0.1895% CI: 0.10, 0.31; P<0.0001

Study 19 subgroupo BRCAm segundoanálisis interino de sobrevida
14 patients (23%) from the placebo arm
received post-discontinuation
PARP inhibitor treatment

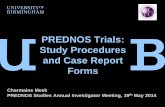
Nuevos end-pointsTFST (time from randomisation to first subsequent therapy or death)
TSST (time from randomisation to second subsequent therapy or death)
PFS2 (time from randomisation to second objective disease progression or death)*
All patients who received
treatment were included in
exploratory endpoint analyses
PFS TSSTPFS2 OS
Intermediate clinical endpoints
Olaparib maintenance monotherapy
First subsequent
treatment response
Chemo Chemo
Progression
Progression
Progression
*TSST is a surrogate for PFS2
TFST
Ledermann J et al. Lancet Oncol 2014;15:852–861

Number of patients at risk:
Olaparib 74 61 43 30 26 25 21 20 20 19 17 16 8 1 0
Placebo 62 33 16 9 7 4 4 4 2 2 2 2 2 0 0
0
10
20
30
40
50
60
70
80
90
100
No
t o
n f
irst
su
bse
qu
ent
ther
apy
(%)
Time from randomisation (months)
0 6 12 18 24 30 36 42 48 54 60 66 72 78 84
Olaparib
Placebo
BRCAm subgroup (n=136)
Olaparib (n=74)Placebo
(n=62)
TFST events, n
(%)53 (72) 59 (95)
Median TFST,
months 15.6 6.2
HR=0.3295% CI 0.22–0.48
P<0.00001
‘Study 19’ olaparib mantenimiento: pacientes BRCAm
TFST
Maturity: 82%
Updated exploratory analysis
Ledermann J et al. J Clin Oncol 34, 2016 (suppl; abstr 5501).
Slides presented at ASCO 2016

Number of patients at risk:
Olaparib 74 69 56 40 32 29 25 23 21 20 19 18 9 1 0
Placebo 62 57 42 25 18 9 6 5 5 3 3 3 3 0 0
0
10
20
30
40
50
60
70
80
90
100
No
t o
n s
eco
nd
su
bse
qu
ent
ther
apy
(%)
Time from randomisation (months)
0 6 12 18 24 30 36 42 48 54 60 66 72 78 84
Olaparib
Placebo
BRCAm subgroup (n=136)
Olaparib (n=74)Placebo
(n=62)
TSST events, n
(%)52 (70) 56 (90)
Median TSST,
months 22.0 15.3
HR=0.4195% CI 0.28–0.62
P=0.00001
‘Study 19’ olaparib mantenimiento: pacientes BRCAm
TSST
Updated exploratory analysisMaturity: 79%
Updated exploratory analysis
Ledermann J et al. J Clin Oncol 34, 2016 (suppl; abstr 5501). Slides presented at ASCO 2016
Ledermann J et al. Lancet Oncol 2014;15:852–861

STUDY 19 ANÁLISIS DE SOBREVIDA GLOBAL
OS data maturity: 77%Alpha (two-sided) = 0.95%Additional follow-up since previous analysis = 3 years
OS data maturity: 38%Alpha (two-sided) = 0.1%
HR=0.9495% CI 0.63–1.39, P=0.75
OS data maturity: 58%Alpha (two-sided) = 3%
HR=0.8895% CI 0.64–1.21, P=0.44
30 Sep 2015
DCO
CI, confidence interval; DCO, data cut-off; FSI, first subject in
28 Aug 2008 31 Oct 2011 26 Nov 2012
FSI DCO DCO
Ledermann J et al. J Clin Oncol 34, 2016 (suppl; abstr 5501). Slides presented at ASCO 2016
Ledermann J et al. New Engl J Med 2012;366:1382–1392
Ledermann J et al. Lancet Oncol 2014;15:852–861

Sobrevida global actualizada de Study 19- olaparibmantenimiento
Maturity 77 %
Maturity 70%
Ledermann et al ASCO 2016; Lancet Oncol 2016
Whole study population
BRCAm subgroup

0
5
10
15
20
25
30
35
40
45
50
≥1 ≥2 ≥3 ≥4 ≥5 ≥6
PA
TIEN
TS O
N O
LAP
AR
IB (
%)
TIME ON OLAPARIB (YEARS)
Overall study population
BRCAm subgroup
BRCAwt subgroup
40%
18%
15% 13%
5%
24%
EXPOSICIÓN PROLONGADA EN BRCA mut y wt en Estudio 19OLAPARIB COMO MANTENIMIENTO
Median follow-up of 5.9 years: 15 patients (11%) still receiving olaparib
(8 BRCAm, 7 BRCAwt); one patient (<1%) still receiving placebo (BRCAm)
Ledermann et al ASCO 2016

Overall study population
BRCAm subgroup
BRCAwt subgroup
EXPOSICIÓN PROLONGADA EN BRCA mut y wt en Estudio 19OLAPARIB COMO MANTENIMIENTO
Ledermann et al ASCO 2016
0
5
10
15
20
25
30
35
40
45
50
≥1 ≥2 ≥3 ≥4 ≥5 ≥6
PA
TIEN
TS O
N O
LAP
AR
IB (
%)
TIME ON OLAPARIB (YEARS)
46%
28%
22%
16% 15%
5%
Median follow-up of 5.9 years: 15 patients (11%) still receiving olaparib
(8 BRCAm, 7 BRCAwt); one patient (<1%) still receiving placebo (BRCAm)

Overall study population
BRCAm subgroup
BRCAwt subgroup
EXPOSICIÓN PROLONGADA EN BRCA mut y wt en Estudio 19OLAPARIB COMO MANTENIMIENTO
Ledermann et al ASCO 2016
0
5
10
15
20
25
30
35
40
45
50
≥1 ≥2 ≥3 ≥4 ≥5 ≥6
PA
TIEN
TS O
N O
LAP
AR
IB (
%)
TIME ON OLAPARIB (YEARS)
33%
19%
14% 14%12%
5%
Median follow-up of 5.9 years: 15 patients (11%) still receiving olaparib
(8 BRCAm, 7 BRCAwt); one patient (<1%) still receiving placebo (BRCAm)

30
Months
Chemo Maintenance
2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36
Primary endpoint
Secondary endpoints
Key exploratoryendpoints
TFST
TSST
PFS
OS
0 5 10 15 20 25 35
Months (median)
4.3
30.2
4.6
6.2
15.3
Placebo
HR: 0.18 (95% CI 0.10–0.31), p<0.00001
HR: 0.62 (95% CI 0.41–0.94), p=0.02480; NS
HR: 0.41 (95% CI 0.28–0.62), nominal p=0.00001
HR: 0.32 (95% CI 0.22–0.48), nominal p<0.00001
6.9 months
4.7 months
9.4 months
6.7 months Difference between arms
11.2
34.9
15.6
22
Olaparib 400 mg bid
Resúmen de END POINTS del ESTUDIO 19. Olaparib comomantenimiento
AstraZeneca. Data on file LYN/002/JUN16

Olaparib Study 19Progression-free survival in BRCAwt (excludes gBRCA & sBRCA)
Ledermann et al Lancet Oncol 2014BRCAwt, wild type (includes patients with no known BRCAm or a mutation of unknown significance)

OLAPARIB MANTENIMIENTO EN BRCA MUT SOLO 2
Eviencia FASE III

SOLO 2

SOLO 2 PFS
mPFS 19,1 meses

PARPi como tratamiento de mantenimiento
SOLO 2
STUDY 19

OLAPARIB APROBAFO POR ANMATComo mantenimiento en pacientes BRCA mut somáticas ogermnales , luego de respuesta completa o parcial a quimioterapiabasada en platino, en recaída platino-sensible.

NOVA trial
N Engl J Med 2016;375:2154-64

Non-gBRCAmut gBRCAmut
2:1 Randomization 2:1 Randomization
Niraparib300 mg QD
PlaceboNiraparib
300 mg QDPlacebo
n=234 n=116 n=138 n=65
Primary Endpoint• PFS; >90% power to detect 4.8-month improvement (HR 0.50)• Non-gBRCAmut cohort endpoint assessed hierarchically to control type 1 error: HRD+ population first,
followed by entire population
NOVA: Niraparib maintenance en HGSOC recaído platino –sensible
• Phase III, multicenter, randomized, double-blind, placebo-controlled study
• Relapsed high-grade serous histology or known gBRCAmut
• ≥2 prior regimens of platinum-based chemotherapy
• Responded to last platinum regimen; remains in response and enrolled within
8 weeks of completion of last platinum regimen
• No measurable lesion ≥2cm
N=553

NOVA: Niraparib maintenance en HGSOC recaído platino –sensible
Treatment
PFS
Median
(95% CI)
(Months)
Hazard Ratio
(95% CI)p-value
% of Patients without
Progression or Death
12 mo
18 mo
Niraparib
(N=138)
21.0(12.9, NE)
0.27
(0.173, 0.410)
p<0.0001
62%
50%
Placebo
(N=65)
5.5(3.8, 7.2)
16%
16%
Progression-free Survival: gBRCAmut
Mirza et al ESMO 2016

Treatment
PFSMedia
n(95%
CI)(Mont
hs)
Hazard Ratio
(95% CI)p-value
% of Patients without
Progression or Death
12 mo
18 mo
Niraparib
(N=234)
9.3
(7.2, 11.2)
0.45
(0.338, 0.607)
p<0.0001
41%
30%
Placebo
(N=116)
3.9(3.7,
5.5)
14%
12%
Progression-free Survival: Non-gBRCAmut
NOVA: Niraparib maintenance en HGSOC recaídoplatino –sensible
Mirza et al ESMO 2016

Courtesy of Tesaro/Myriad Genetics
Testeo de HRD
o Loss of Heterozygosity, o Large-scale State Transitions, o Telomeric Imbalance

BRCAwt
Treatment
PFSMedia
n(95%
CI)(Mont
hs)
Hazard Ratio(95%
CI)p-
value
% of Patients without
Progression or Death12 mo
18 mo
Niraparib
(N=71)
9.3
(5.8, 15.4)
0.38
(0.231, 0.628)
p=0.0001
45%
27%
Placebo
(N=44)
3.7
(3.3, 5.6)
11%
6%
Treatment
PFSMedia
n(95%
CI)(Month
s)
Hazard Ratio(95%
CI)p-
value
% of Patients without
Progression or Death12 mo
18 mo
Niraparib
(N=35)
20.9(9.7, NR)
0.27
(0.081, 0.903)
p=0.0248
62%
52%
Placebo(N=12)
11.0(2.0, NR)
19%
19%
sBRCAmut
NR=Not reached
Treatment
PFSMedian
(95% CI)
(Months)
Hazard Ratio(95%
CI)p-
value
% of Patients without
Progression or Death12 mo
18 mo
Niraparib
(N=92)
6.9
(5.6, 9.6)
0.58
(0.361, 0.922)
p=0.0226
27%
19%
Placebo
(N=42)
3.8
(3.7, 5.6)
7% 7%
HRD-positive
NOVA: análisis exploratorio: PFS en Subgrupos
no-gBRCAmutHRD-negative
Mirza et al ESMO 2016

BRCAwt
Treatment
PFSMedia
n(95%
CI)(Mont
hs)
Hazard Ratio(95%
CI)p-
value
% of Patients without
Progression or Death12 mo
18 mo
Niraparib
(N=71)
9.3
(5.8, 15.4)
0.38
(0.231, 0.628)
p=0.0001
45%
27%
Placebo
(N=44)
3.7
(3.3, 5.6)
11%
6%
Treatment
PFSMedia
n(95%
CI)(Month
s)
Hazard Ratio(95%
CI)p-
value
% of Patients without
Progression or Death12 mo
18 mo
Niraparib
(N=35)
20.9(9.7, NR)
0.27
(0.081, 0.903)
p=0.0248
62%
52%
Placebo(N=12)
11.0(2.0, NR)
19%
19%
sBRCAmut
NR=Not reached
Treatment
PFSMedian
(95% CI)
(Months)
Hazard Ratio(95%
CI)p-
value
% of Patients without
Progression or Death12 mo
18 mo
Niraparib
(N=92)
6.9
(5.6, 9.6)
0.58
(0.361, 0.922)
p=0.0226
27%
19%
Placebo
(N=42)
3.8
(3.7, 5.6)
7% 7%
HRD-positive
NOVA: análisis exploratorio: PFS en Subgrupos
no-gBRCAmutHRD-negative
Mirza et al ESMO 2016


TRIALS CON RUCAPARIB

Rucaparib: eficacia y tolerabilidad
Criteria- Diagnosis of ovarian cancer (inclusive of primary peritoneal and
fallopian tube cancer)- Enrolled at 600 mg BID dosing level and received ≥1 dose of rucaparib
600 mg
Criteria- Received ≥2 prior chemotherapies, including ≥2
platinum-based regimens- Had a deleterious germline BRCA or somatic BRCA mutation- Enrolled at 600 mg BID dosing level and received ≥1 dose of rucaparib
600 mg
Study 10(NCT01482715)
n=62
n=42
ARIEL2(NCT01891344)
n=315
n=64
Safety Population (n=377)
Efficacy Population (n=106)
Safety population visit cutoff dates: Study 10 (31 Mar 2016), ARIEL2 (29 Apr 2016).Efficacy population visit cutoff dates: Study 10 Part 2a (30 Nov 2015) and ARIEL2 (29 Feb 2016).
Study 10 and ARIEL2 parts 1 & 2
Kristeliet et al ESMO 2016


RUCAPARIB. ARIEL 2


Rucaparib: PFS en ARIEL 2 (evaluación de eficacia)
Median (months) 95% CI Range10.0 7.3–12.5 0.0–22.1+
+ Censored; Censoring rate: 47%
Progression-free at 6 months:79%
Progression-free at 12 months:41%
At risk (events) 106 (0) 93 (9) 85 (14) 69 (19) 43 (37) 31 (40) 21 (43) 14 (49) 8 (54) 3 (55) 3 (55) 2 (56) 0 (56)
• Of 106 patients, 50 did not have an event of disease progression or death at the data cutoff dates– Of these 50 patients, 32 were still on treatment, and 18 discontinued treatment for reasons other than disease
progression or death at the data cutoff dates
Efficacy population visit cutoff dates: Study 10 Part 2a (30 Nov 2015) and ARIEL2 (29 Feb 2016).CI, confidence interval.

Rucaparib: ORR según investigador, en poblaciónevaluada para eficacia.
Parameter
Study 10n=42
ARIEL2n=64
Efficacy populationn=106
n (%)[95% CI]
Investigator-assessed RECIST ORR(confirmed CR+PR)
25 (59.5)[43.3–74.4]
32 (50.0)[37.2–62.8]
57 (53.8)[43.8–63.5]
CR 4 (9.5) 5 (7.8) 9 (8.5)
PR 21 (50.0) 27 (42.2) 48 (45.3)
SD 12 (28.6) 24 (37.5) 36 (34.0)
PD 2 (4.8) 7 (10.9) 9 (8.5)
NE 3 (7.1) 1 (1.6) 4 (3.8)
Investigator-assessedRECIST/GCIG CA-125 ORR
75 (70.8)[61.1–79.2]
Efficacy population visit cutoff dates: Study 10 Part 2a (30 Nov 2015) and ARIEL2 (29 Feb 2016).CR, complete response; GCIG, Gynecologic Cancer InterGroup; NE, not evaluable; ORR, objective response rate; PR, partial response; RECIST, Response Evaluation Criteria In Solid Tumors.

Rucaparib: Mejor respuesta para lesiones target en población evaluada para eficacia
-120
-100
-80
-60
-40
-20
0
20
40
60
80
Ch
ange
fro
m B
ase
line
in S
um
of
the
Dia
met
er o
f Ta
rget
Les
ion
s†(%
)
N=103*+ = Ongoing
BRCA1
BRCA2
BRCA mutation origin uncertain
Somatic BRCA mutation
Germline BRCA mutation
*Three patients did not have a post baseline scan; †For unconfirmed responses; includes the best percent change from baseline up to and including the first overall response of progressive disease.Efficacy population visit cutoff dates: Study 10 Part 2a (30 Nov 2015) and ARIEL2 (29 Feb 2016).

ARIEL 3- Rucaparib Maintenance Trial


TOXICIDADES DE PARPI

TOXICIDADES DE PARPI
• Key side effects
• Dose modification
• Early discontinuation due to Adverse Events
• Quality of Life measurements on maintenance therapy

Adapted from Ledermann et al Lancet Oncol 2015; ASCO 2016






Study 19: Treatment Outcome Index (TOI)cambios del basal a 6 meses
• HRQoL, as measured by TOI, was similar for olaparib and placebo and remained consistent over time
1
Time point (months)
LS
M a
nd
95%
CI
2
Olaparib
Placebo
8
–8
3 64 5
6
4
2
0
–6
–4
–2
1
Time point (months)
LSM
and
95%
CI
2
8
–8
3 64 5
6
4
2
0
–6
–4
–2
103 94 71 65 49 39Placebo
102 99 99 86 79 65Olaparib
49 45 34 31 21 19Placebo
54 52 57 48 45 42Olaparib
Patients with BRCAm (MMRM analysis)Overall population
LSM, least squares mean; MMRM, mixed model repeated measures.
Olaparib
Placebo
Ledermann J et al. ESMO, Madrid, Spain, 2014, poster
885PD

NOVA trial- Niraparib- TOXICIDADES
Mirza et al NEJM ; 2106

Event — no. (%)Niraparib(N=367)
Placebo(N=179)
Thrombocytopeniaa 124 (33.8) 1 (0.6)
Anemiab 93 (25.3) 0
Neutropeniac 72 (19.6) 3 (1.7)
Fatigued 30 (8.2) 1 (0.6)
Hypertension 30 (8.2) 4 (2.2)
NOVA Trial Niraparib:EA’S Grado 3-4 en ≤ 5% pacientes
*There were no Grade 5 events.
MDS/AML occurred in 5 of 367 (1.4%) in patients who received niraparib and 2 of 179 (1.1%) in patients who received placebo.
Mirza et al ESMO 2016

Event — no. (%)
Dose
Reductions
(N=367)
Events That Occurred After
Cycle 3(N=296)
Dose
Discontinuation
s (N=367)
Thrombocytopeniaa 148 (40.3) 7 (2.4) 12 (3.3)
Anemiab 68 (18.5) 50 (16.9) 5 (1.4)
Neutropeniac 32 (8.7) 8 (2.7) 7 (1.9)
Fatigued 20 (5.4) 9 (3.0) 12 (3.3)
Hypertension 5 (1.4) - 1
NOVA Trial Niraparib: Ajuste de dosis debido a EA’S
Mandatory dose reductions for hematology laboratory abnormalities were required for thrombocytopenia,
anemia, and neutropenia
Any Grade Grade 3/4 Any Grade
Mirza et al ESMO 2016

Olaparib study 19 y Niraparib NOVA : reducción de dosis y discontinuación por EA’s
Niraparib Placebo
SAE 110 ( 30%)
27 ( 15%)
AE leading to dose interruptions
253 (69%)
9 (5%)
AE leading to dose reduction
244 (65%)
26 (15%)
AE leading to treatment discontinuation
54 ( 15%) 4 (2%)
Olaparib Placebo
SAE 25 (18%) 11 (9%)
AE Leading to dose interruptions
49 (36%) 21 (16%)
AE leading to dose reductions
59 (43%) 29 (23%)
AE leading to treatment discontinuation
8 (6%) 2 (2%)
Ledermann et al Lancet Oncol 2016 Mirza et al NEJM 2016


CREATININA

OTROS EFECTOS ADVERSOS ESPECIALES…


CONCLUSIONES 1
• El cáncer de ovario BRCA mut
– Tiene mejor sobrevida.
– Es más quimiosensible.
– Mantenimiento con olaparib ,niraparib y ruvaparib, han demostrado prolongar significativamente el control de la enfermedad (SLP), también son activos en pts SIN BRCA mut.
– Olaparib y rucaparib son activos como mono droga en BRCA mut.

CONCLUSIONES 2
• Ofrecer el test de BRCA debe ser práctica de rutina en manejo de OC.
• Testeo de sBRCA mut y HRD van cobrando importancia a medida que las técnicas se refinan.Importancia frente a “test funcional” de sensibilidad a platino.
• La combinaciones con antiangiogénicos e inhcheck point inmunológico, muestran resultados promisorios, que pueden ampliar las indicaciones de estos agentes.

Muchas gracias…